Back to Journals » Clinical Epidemiology » Volume 14
Temporary Increased LDL-C in Offspring with Extreme Elevation of Maternal Preconception Estradiol: A Retrospective Cohort Study
Authors Feng W, Zhang D, Fu L, Hu J, Gao S, Song X, Cui L ![]()
Received 19 January 2022
Accepted for publication 30 March 2022
Published 7 April 2022 Volume 2022:14 Pages 453—462
DOI https://doi.org/10.2147/CLEP.S358999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Wanbing Feng,1– 6 Di Zhang,1– 6 Linlin Fu,1– 6 Jingmei Hu,1– 6 Shanshan Gao,1– 6 Xiaocui Song,1 Linlin Cui1– 6
1Center for Reproductive Medicine, Department of Reproductive Medicine, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, People’s Republic of China; 2Research Unit of Gametogenesis and Health of ART-Offspring, Chinese Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 3Key Laboratory of Reproductive Endocrinology of Ministry of Education, Shandong University, Jinan, Shandong, People’s Republic of China; 4Shandong Key Laboratory of Reproductive Medicine, Jinan, Shandong, People’s Republic of China; 5Shandong Provincial Clinical Research Center for Reproductive Health, Jinan, Shandong, People’s Republic of China; 6National Research Center for Assisted Reproductive Technology and Reproductive Genetics, Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Linlin Cui; Xiaocui Song, Center for Reproductive Medicine, Department of Reproductive Medicine, The Second Hospital, Cheeloo College of Medicine, Shandong University, No. 157, Jingliu Road, Shizhong District, Jinan, Shandong, People’s Republic of China, 250001, Tel +86 531 85651598, Fax +86 531 87068226, Email [email protected]; [email protected]
Objective: To investigate the effect of maternal estradiol (E2) elevation on long-term metabolic manifestations in the offspring.
Study Design and Setting: This was a retrospective cohort study. Overall, 3690 children conceived by in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI) between July 2014 and December 2017 were recruited and divided into four groups categorized by maternal E2 quartiles (Q1, < 2420; Q2, 2420– 3839; Q3, 3839– 5599; and Q4, ≥ 5599 pg/mL). The metabolic profiles were measured during childhood. Linear mixed models were used to evaluate the association between maternal E2 elevation and metabolic phenotypes of the offspring.
Results: Lipoprotein cholesterol (LDL-C) was significantly higher in the highest quartile group than in the lowest quartile group during infancy (adjusted mean difference [95% confidence interval, CI]): 0.11 [0.02, 0.20], P = 0.005), but the difference disappeared in the later childhood phase. In children born after fresh embryo transfer, LDL-C showed an increasing trend with the increase in maternal E2 level (adjusted mean difference [95% CI]: Q2 vs Q1, − 0.01 [− 0.11, 0.08], Q3 vs Q1, 0.06 [− 0.04, 0.15], Q4 vs Q1, 0.10 [0, 0.20]). Other metabolic variables were comparable across increasing quartiles of maternal E2 levels.
Conclusion: This study demonstrates a temporary increase in LDL-C levels in infants with higher levels of maternal preconception E2 levels. However, the long-term safety of hyperestrogens after ovarian stimulation in the next generation is favorable. The mechanism underlying the transiently increased metabolic dysfunction risk in infants conceived by IVF/ICSI requires investigation in future studies.
Keywords: offspring, supraphysiologic estradiol, controlled ovarian hyperstimulation, assisted reproductive technology
Introduction
Previous studies, including ours, indicated that offspring conceived through in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI) showed less favorable metabolic health manifesting as differential peripheral body fat deposit,1,2 elevated blood pressure,3 deteriorate gluco-metabolism,4–6 raised triglycerides (TG),7 and decreased low-density lipoprotein cholesterol (LDL-C) levels.5 According to the DOHaD theory, metabolic changes in later life can be traced back to abnormal exposure during early life.8,9 Therefore, IVF/ICSI procedures were considered related to exposure in this population. Since infertile couples would not have babies without IVF/ICSI treatment, determining the key factors that conferred metabolic risk in the next generation was essential.
Controlled ovarian hyperstimulation (COH) is the key procedure in IVF/ICSI treatment, and the fundamental differential exposure between IVF/ICSI offspring and those nature conceived.10 Compared with the natural cycle, maternal serum estradiol (E2) levels increased more than tenfold in the COH cycle.11 It has been reported that higher maternal E2 levels on human chorionic gonadotropin (hCG) trigger days are associated with the risk of low birth weight (LBW) in the offspring not only after fresh12 but also after frozen embryo transfer (ET).13 LBW is well accepted as a risk factor for poor metabolic outcomes later in life.14 Moreover, elevated maternal serum E2 levels throughout pregnancy are directly associated with insulin resistance and dyslipidemia in newborns.15,16 However, animal studies reported that mice conceived by COH alone did not exhibit any metabolic dysfunction in childhood6 and even showed reduced lipid accumulation in the peripheral metabolic organs of old mice.16 Unfortunately, human data on the long-term metabolic profiles of offspring conceived through IVF/ICSI are limited. Only one study reported that prenatal high E2 exposure increased the fasting insulin and homeostatic model assessment for insulin resistance (HOMA-IR) index of children conceived by IVF/ICSI.15
This retrospective cohort study aimed to investigate the association between maternal E2 levels and the long-term metabolic profiles of children conceived through IVF/ICSI at ages 2–9. The results would help to target the risk factors of metabolic disturbance in IVF/ICSI offspring and provide valuable evidence on the intergenerational safety of ovarian stimulation in counseling couples with infertility before IVF/ICSI treatment.
Materials and Methods
Study Population
This retrospective cohort study was performed at the Center for Reproductive Medicine, Cheeloo College of Medicine, Shandong University. A total of 3690 singleton children who conceived by IVF/ICSI treatment between July 2014 and December 2017 were recruited. Children born after oocyte or embryo donation were excluded from this study. All participants were followed up at least once in their childhood (aged 2 to 9 years), which led to a total of 5238 visits. The study was approved by the Reproductive Medicine Ethics Committee of the Hospital for Reproductive Medicine Affiliated to Shandong University (Ethics approval number: NO. 2014).17 The parents signed informed consent forms with the assent of the child.
Outcome Assessment
The enrolled children were recalled at least once during their childhood phase. All the outcome assessments were performed at each visit. The height (±0.1 cm) and weight (±0.1 kg) of the offspring were measured twice using a stadiometer and electronic scale with a light cloth and no shoes. The BMI was calculated as weight (kg)/[height (m)]2. Blood samples of the offspring were collected after overnight fasting and stored at −80°C until the tests. Fasting blood glucose (FBG) levels were analyzed using the hexokinase method (Cobas c702 instrument; Roche Diagnostics, Germany). Fasting insulin was measured in the serum using an electrochemiluminescence immunoassay (Cobas e601 instrument; Roche Diagnostics, Germany). Total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and LDL-C levels were measured in serum using a homogeneous assay (Cobas c702 instrument; Roche Diagnostics, Germany). HOMA-IR was calculated as [insulin (mIU/L) FBG (mmol/L)]/22.5. HOMA of beta-cell function (HOMA-β) was calculated using the formula [20*insulin (mIU/mL)]/[FBG (mmol/L) - 3.5].
Exposure Assessment
The IVF/ICSI protocols have been described in detail in our previous study.17 Maternal E2 levels were tested using chemiluminescence immunoassays (Roche Diagnostics, Germany) on hCG trigger days, with intra- and inter-assay coefficients of variation of < 10%. All mother-offspring pairs were grouped into four quartiles: Q1 (E2 < 2420 pg/mL), Q2 (2420 ≤ E2 < 3839 pg/mL), Q3 (3839 ≤ E2 < 5599 pg/mL), and Q4 (E2 ≥ 5599 pg/mL).
Covariate Assessment
Pre-pregnancy height (±0.1 cm) and weight (±0.1 kg) of parents were measured at enrolment using a stadiometer and electronic scale to calculate BMI. Information on the parental date of birth, educational level, and parity (0 or 1) was obtained using a standardized questionnaire during a face-to-face interview. Parental age at delivery was calculated based on the date of parental birth and delivery. The IVF/ICSI procedures were extracted by reviewing the medical records. In addition to ovarian stimulation, IVF/ICSI procedures included ICSI (no or yes), cycle type (fresh or frozen), number of embryos transfer (one or more), stage of ET (cleavage or blastocyst), preimplantation genetic testing (PGT) (no or yes), and assisted hatching (no or yes). Perinatal information was recorded based on the birth certificate, including date of delivery, sex (male or female), birth weight, gestational age, and caesarean birth (no or yes). The dietary intake of the children was obtained using a standardized questionnaire completed by their parents. Energy intake was calculated based on the dietary intake when the offspring were above 4 years of age.
Statistical Analysis
All data were analyzed using R3.6.3. Categorical variables were presented as counts (proportions). For continuous variables, normality plots and the Shapiro–Wilk test were used for normality testing. Continuous variables are presented as mean ± standard deviation when normally distributed and as median (25th–75th percentile) when not normally distributed. Baseline characteristics among the four groups were compared using the Kruskal–Wallis test for non-normally distributed continuous variables and Fisher’s exact test for categorical variables. Linear mixed effects regression was used to determine the estimated mean difference (MD) and 95% confidence intervals (CIs) of outcomes for each quartile of E2 levels, with the lowest quartile (Q1) always used as a reference. A linear mixed-effects regression model was used to adjust for the confounding effect of repeated measurements in the same child at different time points.18 Model 1 tested the crude unadjusted values. Model 2 was used to control for potential confounding factors including maternal age, BMI, paternal age, BMI, cycle type, number of ET, stage of ET, offspring gestational age, birth weight, sex, and age at the visit. Since the distribution of insulin, HOMA-IR, and HOMA-β was skewed, loge transformation was performed prior to the application of regression models. A P-value <0.017 was regarded as statistically significant (Bonferroni adjustment, 0.05/3). To test the robustness of the results, we further stratified the mother-offspring pairs according to cycle type (fresh and frozen ET) and offspring age (2–3, 4–5, and 6–9 years).
Results
We finally included 3690 mother-offspring pairs and 5238 flow-up visits in this study [maternal age, 30.8 (28.2, 34.0) years; maternal BMI, 22.7 (20.7, 25.1) kg/m2; paternal age, 31.6 (28.6, 34.9) years; paternal BMI 25.4 (22.8, 28.0) kg/m2; male offspring, 1954 (53.0%); offspring age, 4.1 (3.1, 5.6) kg/m2]. The baseline characteristics of the patients are presented in Table 1. Parental age and maternal BMI were the highest in the Q1 group. There were no significant differences in the parental education level or parity between the groups. The median maternal E2 levels were 1770, 3111, 4329, and 7043 pg/mL in the four groups. The lowest median gonadotropin dose was observed in the top quartile (Q4) group, with the highest ovarian stimulation duration. Transfer of frozen embryos, single embryos, and blastocysts was most prevalent in the Q4 group. The proportions of ICSI, PGT, and assisted hatching were similar among the four groups. The gestational age of the Q1 group was the lowest. There were no significant differences among the groups in terms of birth weight, caesarean birth, and sex. During the follow-up visits, the highest median offspring age was 4.5 years in the Q4 group. The dietary intake of the children among the groups was comparable.
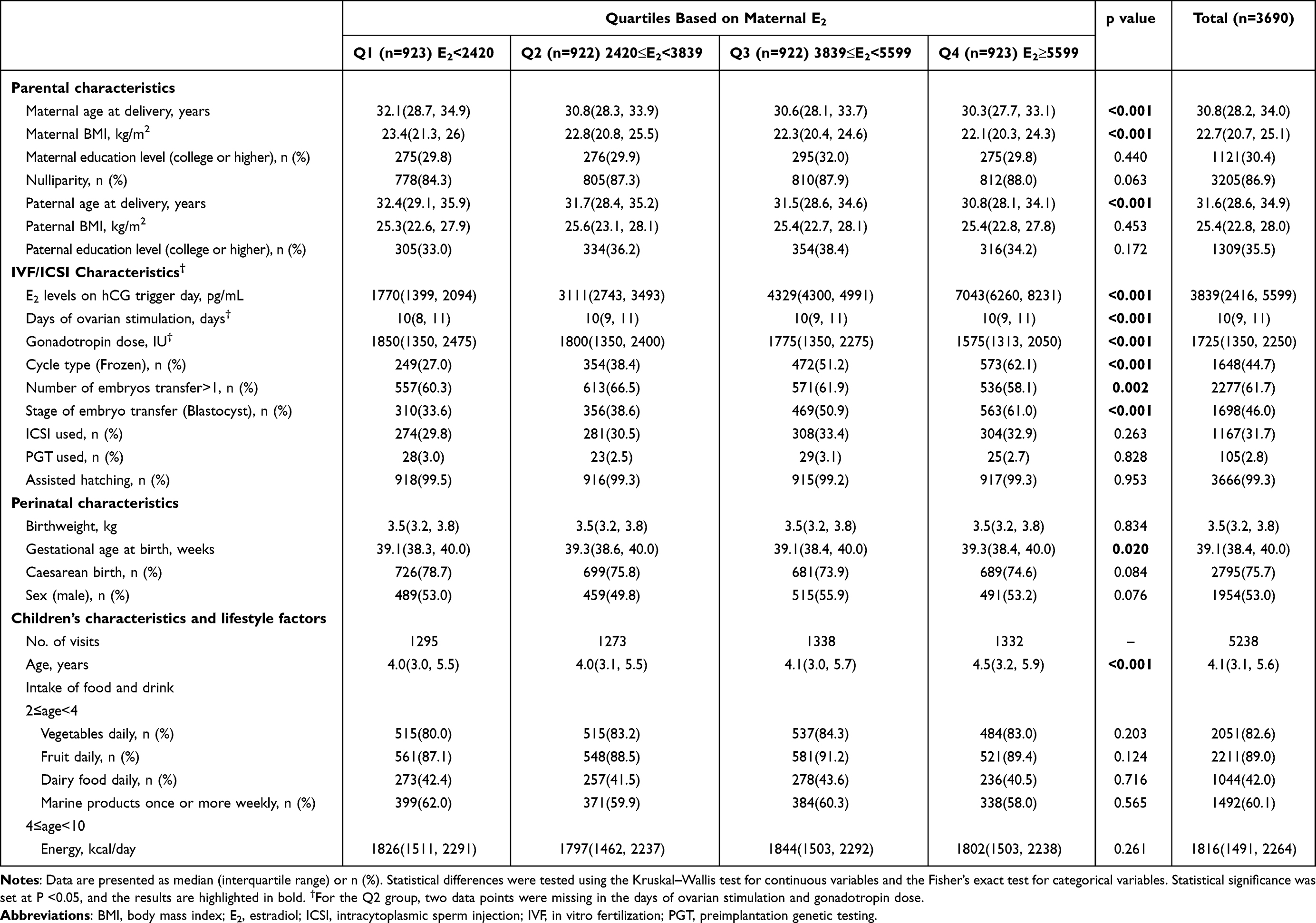 |
Table 1 Baseline Characteristics of Study Population |
Table 2 shows the metabolic variables of children grouped by maternal E2 levels. No differences were found in BMI, FBG, insulin, HOMA-IR, HOMA-β, TC, TG, LDL-C, or HDL-C across increasing quartiles of maternal E2 levels. The results were maintained after adjusting for confounding factors including parental age, BMI, cycle type, number, stage of ET, offspring gestational age, birth weight, sex, and age at the visit. The findings were consistent with the main results of subgroup analysis stratified by cycle type (fresh and frozen ET) (Figure 1). However, a trend of gradient increase in LDL-C along with maternal E2 was observed in children born after fresh ET [adjusted mean difference (95% CI): Q2 vs Q1, −0.01 (−0.11, 0.08); Q3 vs Q1, 0.06 (−0.04, 0.15), Q4 vs Q1, 0.10 (0, 0.20]). We further stratified the offspring into three subgroups according to age (2–3, 4–5, and 6–9 years). The infant characteristics are listed in Table 3. Compared to the Q1 group, LDL-C was significantly increased in the Q4 group after adjusting for confounding factors during infancy [adjusted mean difference (95% CI): 0.11 (0.02, 0.20), P=0.005; Table 4]. However, the parameters during childhood were comparable among the groups Tables S1–2.
 |
Table 2 Mean Differences (95% CI) for Metabolic Variables of Children Across Quartiles of Maternal E2 Levels |
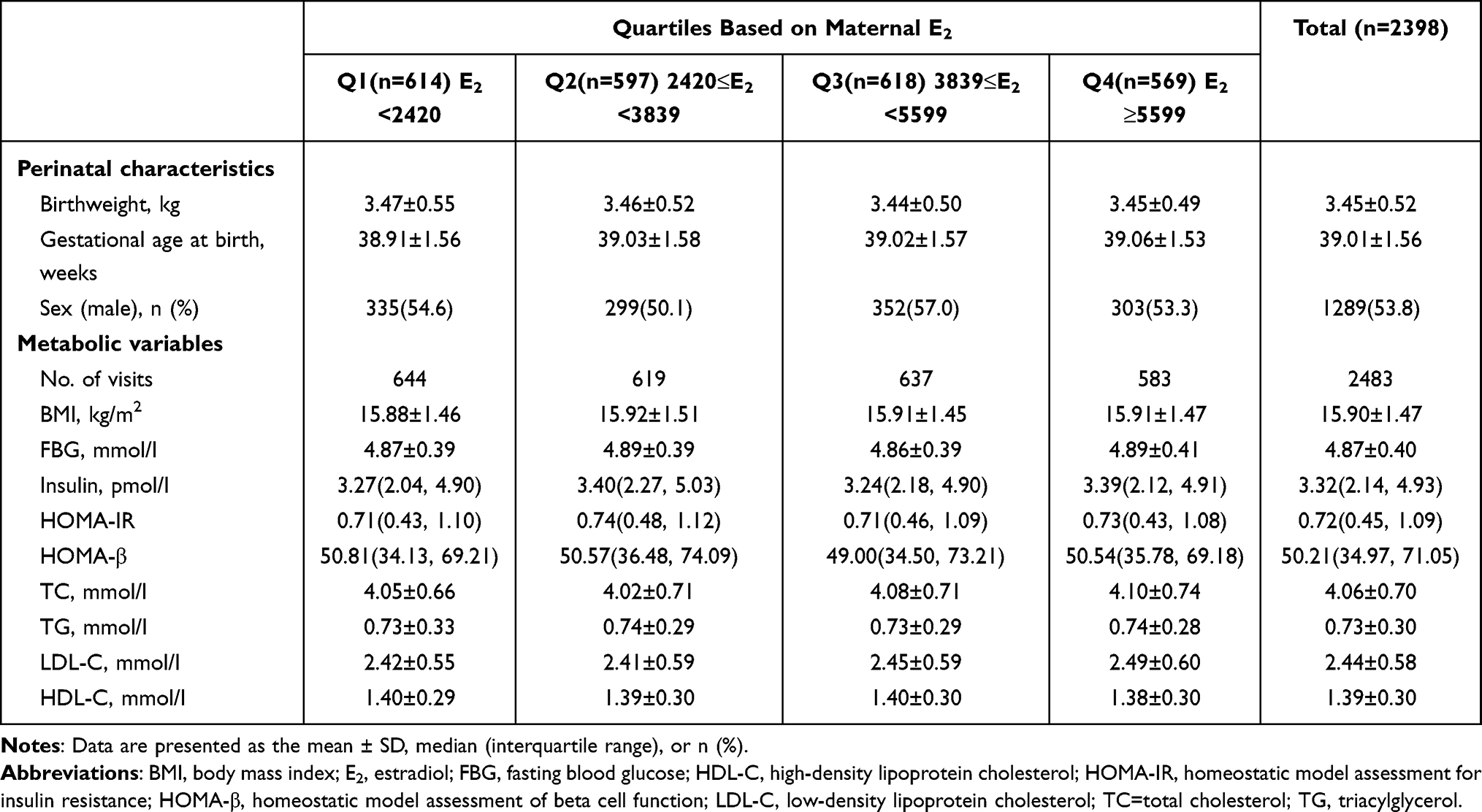 |
Table 3 Characteristics of Children Aged 2 to 3 Yrs |
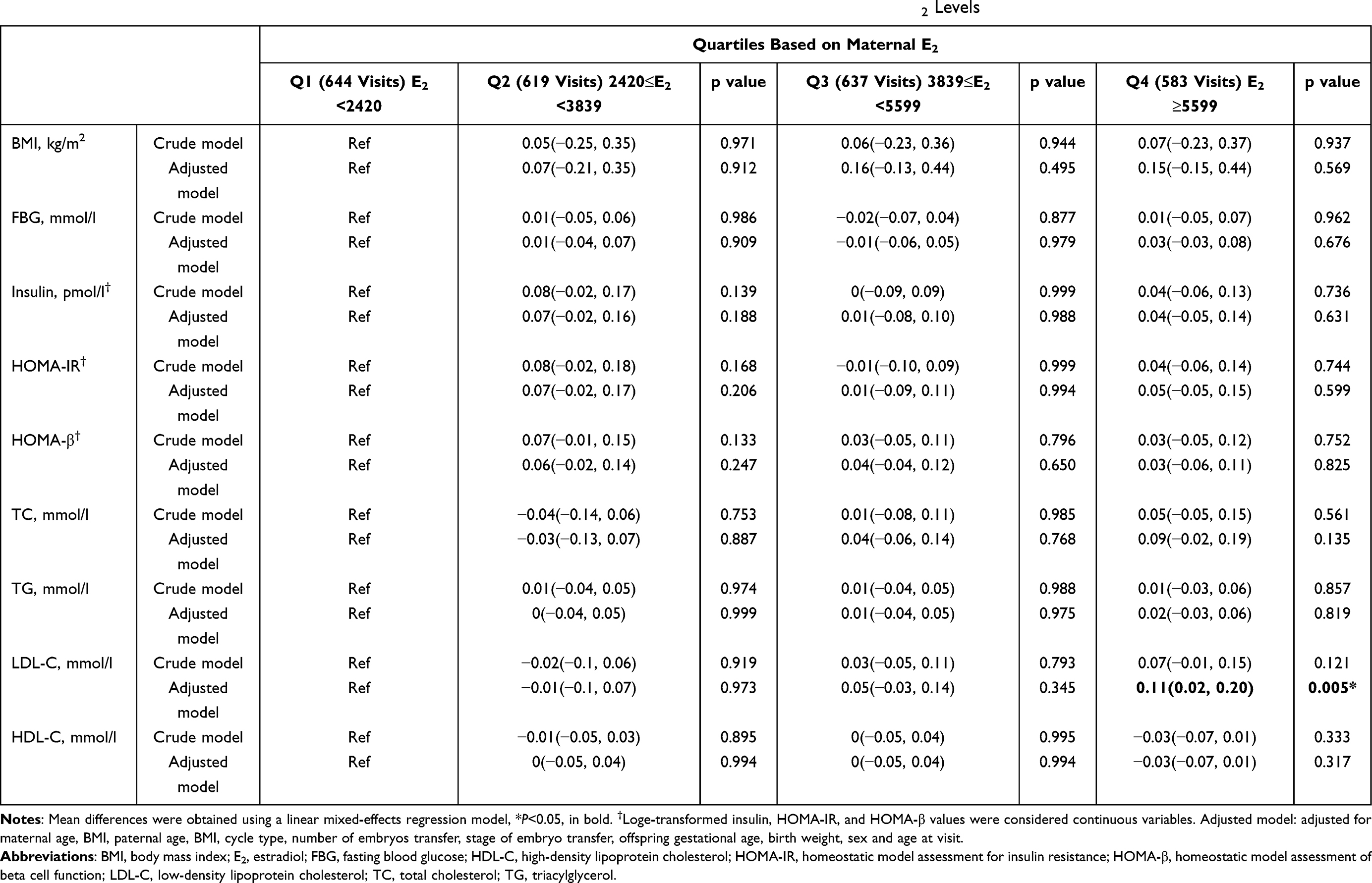 |
Table 4 Mean Differences (95% CI) for Metabolic Variables of Children Aged 2 to 3 Yrs Across Quartiles of Maternal E2 Levels |
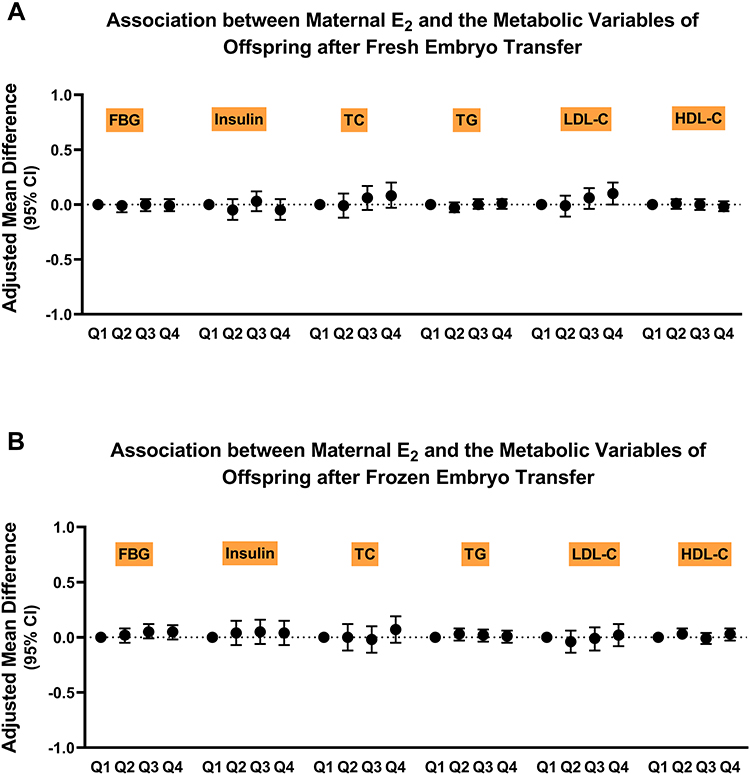 |
Figure 1 Differences in metabolic variables of children across quarters of maternal E2 levels stratified by embryo frozen Association between maternal E2 and metabolic variables in offspring after Fresh (A) and Frozen (B) embryo transfer.Abbreviations: FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triacylglycerol. |
Discussion
Our study indicated that children with higher maternal E2 levels before conception manifested temporary increases in LDL-C levels during infancy. However, in childhood, those with different maternal E2 levels before conception showed similar metabolic profiles. This indicates that maternal COH does not affect the long-term metabolic health of the children.
Ovarian stimulation was one of the necessary key procedures in IVF/ICSI treatment.19 In a COH cycle of normal ovarian response, more than 5–8 mature follicles would develop and produce supraphysiological E2 levels,11 which is only 100–300 pg/mL in natural conceived women.20 A previous study indicated that the elevation of steroid hormones could persist through the first trimester in women who underwent COH.21 Maternal E2 enters fetal circulation through the placenta.22 Accumulating evidence suggests that children exposed to a higher maternal E2 displayed poor neonatal outcomes,12,13 deregulated cardiovascular functions,23 and a less favorable thyroid hormone profile,24 neurodevelopment,25,26 and neonatal metabolism.15,16
In this study, we also found a temporary increase in LDL-C levels in children within the highest quartile of maternal E2 levels during the infancy phase. This may be affected by their mothers, whose serum LDL-C, TG, and Apo-B levels were reported to increase after ovarian stimulation.26 Intrauterine exposure to elevated maternal lipid levels may upregulate genes involved in de novo lipogenesis, cholesterol synthesis, and dysregulation of genes related to lipid metabolism in offspring.27,28 In addition, increased E2 levels after ovarian stimulation could occur throughout the gestation period in fresh cycles and could be distributed into the fetal bloodstream.16,23 Furthermore, it was demonstrated that E2 could stimulate the synthesis of LDL-C and TC via increased expression of the cholesterol synthesis rate-limiting enzyme 3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR) in fetal livers,16 which was supported by the increasing trend of LDL-C in fresh ET. Moreover, higher maternal E2 levels indicate a higher dose of exogenous gonadotropin, which was suggested to affect the next generation through epigenetic modification and oxidative stress status of oocytes, embryos, and their microenvironment.29–34 However, it should be noted that according to our data, the difference vanished in the later childhood phase. This suggests that adverse effects on neonates may be auto-adjusted with age.
The strength of our present study was the long duration of follow-up, which extended the confirmation of the safety of COH and subsequent E2 elevation in the next generation, the large sample size, which provided preferably statistical power and allowed the subgroup analysis to confirm the robustness of the conclusions, and the high homogeneity of the participants. However, this study has several limitations. First, the ideal control should be offspring born after natural cycle ART. However, this was difficult to obtain because the natural cycle was most suitable for women with diminished ovarian reserve (DOR) or older age, which would be an important confounding factor. Second, the metabolic profiles examined in the present study were only general tests that could not sufficiently represent the metabolic status in detail. Metabolomic analysis should be confirmed in future studies.
Conclusion
In conclusion, the elevation of E2 levels after COH in mothers did not seem to affect their offspring in terms of metabolism, except for a temporary change in LDL-C levels during infancy. The long-term safety of COH in the next generation was favorable, at least during childhood. However, the trend of gradient increase in LDL-C suggests the need for close monitoring in the later life of those born after fresh ET.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This work was supported by the National Key Research and Development Program of China (2018YFC1004301), Research Unit of Gametogenesis and Health of ART-Offspring, Chinese Academy of Medical Sciences (2020RU001), Shandong Provincial Key Research and Development Program (2018YFJH0504), Natural Science Foundation of Shandong Province of China (ZR2020MH065), and Taishan Scholars Program for Young Experts of Shandong Province (tsqn201909195).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ceelen M, van Weissenbruch MM, Roos JC, Vermeiden JP, van Leeuwen FE, Delemarre-van de Waal HA. Body composition in children and adolescents born after in vitro fertilization or spontaneous conception. J Clin Endocrinol Metab. 2007;92(9):3417–3423. doi:10.1210/jc.2006-2896
2. Belva F, Painter R, Bonduelle M, Roelants M, Devroey P, De Schepper J. Are ICSI adolescents at risk for increased adiposity? Hum Reprod. 2012;27(1):257–264. doi:10.1093/humrep/der375
3. Cui L, Zhao M, Zhang Z, et al. Assessment of cardiovascular health of children ages 6 to 10 years conceived by assisted reproductive technology. JAMA network open. 2021;4(11):e2132602. doi:10.1001/jamanetworkopen.2021.32602
4. Ceelen M, van Weissenbruch MM, Vermeiden JP, van Leeuwen FE, Delemarre-van de Waal HA. Cardiometabolic differences in children born after in vitro fertilization: follow-up study. J Clin Endocrinol Metab. 2008;93(5):1682–1688. doi:10.1210/jc.2007-2432
5. Guo XY, Liu XM, Jin L, et al. Cardiovascular and metabolic profiles of offspring conceived by assisted reproductive technologies: a systematic review and meta-analysis. Fertil Steril. 2017;107(3):622–631.e625. doi:10.1016/j.fertnstert.2016.12.007
6. Chen M, Wu L, Zhao J, et al. Altered glucose metabolism in mouse and humans conceived by IVF. Diabetes. 2014;63(10):3189–3198. doi:10.2337/db14-0103
7. Sakka SD, Loutradis D, Kanaka-Gantenbein C, et al. Absence of insulin resistance and low-grade inflammation despite early metabolic syndrome manifestations in children born after in vitro fertilization. Fertil Steril. 2010;94(5):1693–1699. doi:10.1016/j.fertnstert.2009.09.049
8. Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: physiology or pathophysiology? Physiol Rev. 2014;94(4):1027–1076. doi:10.1152/physrev.00029.2013
9. Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–417. doi:10.1111/j.1365-2796.2007.01809.x
10. Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27(2):170–207. doi:10.1210/er.2005-0015
11. Liu Y, Li J, Zhang W, Guo Y. Association between serum oestradiol level on the hCG administration day and neonatal birthweight after IVF-ET among 3659 singleton live births. Sci Rep. 2021;11(1):6084. doi:10.1038/s41598-021-85692-7
12. Pereira N, Elias RT, Christos PJ, et al. Supraphysiologic estradiol is an independent predictor of low birth weight in full-term singletons born after fresh embryo transfer. Hum Reprod. 2017;32(7):1410–1417. doi:10.1093/humrep/dex095
13. Cai J, Liu L, Xu Y, et al. Supraphysiological estradiol level in ovarian stimulation cycles affects the birthweight of neonates conceived through subsequent frozen-thawed cycles: a retrospective study. Bjog. 2019;126(6):711–718. doi:10.1111/1471-0528.15606
14. Patti ME. Intergenerational programming of metabolic disease: evidence from human populations and experimental animal models. Cell Mol Life Sci. 2013;70(9):1597–1608. doi:10.1007/s00018-013-1298-0
15. Wang HH, Zhou CL, Lv M, et al. Prenatal high estradiol exposure induces sex-specific and dietarily reversible insulin resistance through decreased hypothalamic INSR. Endocrinology. 2018;159(1):465–476. doi:10.1210/en.2017-03017
16. Meng Y, Lv PP, Ding GL, et al. High maternal serum estradiol levels induce dyslipidemia in human newborns via a hepatic HMGCR estrogen response element. Sci Rep. 2015;5(1):10086. doi:10.1038/srep10086
17. Zhang B, Meng Y, Jiang X, et al. IVF outcomes of women with discrepancies between age and serum anti-Müllerian hormone levels. Reprod Biol Endocrinol. 2019;17(1):58. doi:10.1186/s12958-019-0498-3
18. Gill PS. A robust mixed linear model analysis for longitudinal data. Stat Med. 2000;19(7):975–987. doi:10.1002/(SICI)1097-0258(20000415)19:7<975::AID-SIM381>3.0.CO;2-9
19. Holzer H, Casper R, Tulandi T. A new era in ovulation induction. Fertil Steril. 2006;85(2):277–284. doi:10.1016/j.fertnstert.2005.05.078
20. Audebert AJ, Emperaire JC, Ruffie A. [Steroids and the prediction of ovulation]. Contracept Fertil Sex. 1984;12(2):411–419. Romanian.
21. Xu GF, Zhou CL, Xiong YM, et al. Reduced intellectual ability in offspring of ovarian hyperstimulation syndrome: a cohort study. E Bio Med. 2017;20:263–267. doi:10.1016/j.ebiom.2017.05.020
22. Gude NM, Roberts CT, Kalionis B, King RG. Growth and function of the normal human placenta. Thromb Res. 2004;114(5–6):397–407. doi:10.1016/j.thromres.2004.06.038
23. Xu GF, Zhang JY, Pan HT, et al. Cardiovascular dysfunction in offspring of ovarian-hyperstimulated women and effects of estradiol and progesterone: a retrospective cohort study and proteomics analysis. J Clin Endocrinol Metab. 2014;99(12):E2494–E2503. doi:10.1210/jc.2014-2349
24. Lv PP, Meng Y, Lv M, et al. Altered thyroid hormone profile in offspring after exposure to high estradiol environment during the first trimester of pregnancy: a cross-sectional study. BMC Med. 2014;12(1):240. doi:10.1186/s12916-014-0240-0
25. Zhou CL, Xu GF, Yang Q, et al. Diminished verbal ability among children conceived through ART with exposure to high serum estradiol in utero. J Assist Reprod Genet. 2020;37(8):1931–1938. doi:10.1007/s10815-020-01835-1
26. Brizzi P, Dessole S, Tonolo G, et al. Effect of ovarian stimulation on plasma lipid and apolipoprotein concentrations in a population of infertile women undergoing IVF/embryo transfer. Reprod Biomed Online. 2003;7(3):309–312. doi:10.1016/S1472-6483(10)61869-X
27. Zhou Y, Peng H, Xu H, et al. Maternal diet intervention before pregnancy primes offspring lipid metabolism in liver. Lab Invest. 2020;100(4):553–569. doi:10.1038/s41374-019-0344-4
28. Jacometo CB, Schmitt E, Pfeifer LF, et al. Linoleic and α-linolenic fatty acid consumption over three generations exert cumulative regulation of hepatic expression of genes related to lipid metabolism. Genes Nutr. 2014;9(4):405. doi:10.1007/s12263-014-0405-7
29. Uysal F, Ozturk S, Akkoyunlu G. Superovulation alters DNA methyltransferase protein expression in mouse oocytes and early embryos. J Assist Reprod Genet. 2018;35(3):503–513. doi:10.1007/s10815-017-1087-z
30. Huo Y, Yan ZQ, Yuan P, et al. Single-cell DNA methylation sequencing reveals epigenetic alterations in mouse oocytes superovulated with different dosages of gonadotropins. Clin Epigenetics. 2020;12(1):75. doi:10.1186/s13148-020-00866-w
31. Yu B, Smith TH, Battle SL, Ferrell S, Hawkins RD. Superovulation alters global DNA methylation in early mouse embryo development. Epigenetics. 2019;14(8):780–790. doi:10.1080/15592294.2019.1615353
32. Tang SB, Yang LL, Zhang TT, et al. Multiple superovulations alter histone modifications in mouse early embryos. Reproduction. 2019;157(6):511–523. doi:10.1530/REP-18-0495
33. de Waal E, Yamazaki Y, Ingale P, Bartolomei MS, Yanagimachi R, McCarrey JR. Gonadotropin stimulation contributes to an increased incidence of epimutations in ICSI-derived mice. Hum Mol Genet. 2012;21(20):4460–4472. doi:10.1093/hmg/dds287
34. Pérez-Ruiz I, Meijide S, Ferrando M, Larreategui Z, Ruiz-Larrea MB, Ruiz-Sanz JI. Ovarian stimulated cycles reduce protection of follicular fluid against free radicals. Free Radic Biol Med. 2019;145:330–335. doi:10.1016/j.freeradbiomed.2019.10.004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.