Back to Journals » Integrated Pharmacy Research and Practice » Volume 13
Telepharmacy versus Face-to-Face Approach in Providing Inhaler Technique Training Service: A Non-Inferiority Assessment Among German Pharmacy Students
Authors Ali Sherazi B ![]() , Sayyed SA, Möllenhoff K, Läer S
, Sayyed SA, Möllenhoff K, Läer S
Received 14 May 2024
Accepted for publication 28 August 2024
Published 20 September 2024 Volume 2024:13 Pages 165—180
DOI https://doi.org/10.2147/IPRP.S468881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Walid Al-Qerem
Bushra Ali Sherazi,1,2 Shahzad Ahmad Sayyed,1 Kathrin Möllenhoff,3 Stephanie Läer1
1Institute of Clinical Pharmacy and Pharmacotherapy, Heinrich Heine University, Düsseldorf, 40225, Germany; 2Institute of Pharmacy, Faculty of Pharmaceutical and Allied Health Sciences, Lahore College for Women University, Lahore, 54000, Pakistan; 3Institute of Medical Statistics and Computational Biology, Faculty of Medicine, University of Cologne, Cologne, 50924, Germany
Correspondence: Bushra Ali Sherazi, Institute of Clinical Pharmacy and Pharmacotherapy, Heinrich Heine University, Universitätsstraße 1, Düsseldorf, 40225, Germany, Email [email protected]
Background: The use of telepharmacy in delivering pharmaceutical care services has grown in the past few years; however, there are perceptions of its inappropriateness for providing medical device training among pharmacy students and practicing pharmacists.
Objective: The primary objective of this study was to determine if the telepharmacy approach for providing inhaler technique training service was non-inferior to the face-to-face approach regarding pharmacy students’ performance in simulated patient encounters. Secondary objectives were to determine students’ self-assessment of their ability to demonstrate and practice inhaler technique between the two modes of communication and their perceptions of telepharmacy.
Methods: A randomized crossover non-inferiority trial was conducted among undergraduate pharmacy students. Outcomes were measured by comparing Objective Structured Clinical Examination (OSCE) scores of participants’ performance between two modes of communication while providing inhaler technique training service. Moreover, the participants also completed self-assessment and perception questionnaires.
Results: The telepharmacy approach was non-inferior to the face-to-face approach for demonstrating and practicing the correct inhaler technique based on OSCE scores and a predefined non-inferiority margin of − 10%. The results also revealed no significant differences in student self-confidence between the two modes of communication. Moreover, participants had a largely positive perception of telepharmacy and its use in providing inhaler technique training service.
Conclusion: Considering our findings, telepharmacy is a viable alternative to traditional face-to-face consultations for providing inhaler technique training service. However, to address perceived difficulties and differences between virtual and face-to-face consultations, the pharmacy curriculum should include more telepharmacy-related didactic content with experiential learning and simulations.
Keywords: pharmacy education, digital health, eHealth, videoconferencing, clinical pharmacy services, inhaler technique
Introduction
Healthcare professionals (HCPs) are utilizing digital health (DH) technologies increasingly to deliver healthcare services,1 which has led to increased investments in telehealth and digitalization.2 Telehealth refers to using electronic information and telecommunication tools to enhance a patient’s health, including the telephone, videoconferencing, text messaging, email, internet, health applications, social media, or fax.3,4 Telehealth enables providing healthcare services to those in remote areas and has been more widely implemented and embraced over time, sometimes exceeding in-person visits.5,6 The global coronavirus disease 2019 (COVID-19) pandemic changed how healthcare was delivered, moving from in-person to telehealth, and continues to change in post-pandemic situations.7 These new digital healthcare activities and services add novel opportunities for healthcare systems and providers worldwide.5
Like others, the pharmacy profession has also embraced telehealth technologies often referred to as telepharmacy.8,9 Telepharmacy is a method used in pharmacy practice in which a pharmacist utilizes telecommunications technology to oversee aspects of pharmacy operations or to provide patient care services.8 Many examples of telepharmaceutical care and services worldwide include chronic disease management, medication review, prescription verification, dispensing, drug information, patient counseling, education, and remote monitoring.10–22 The telepharmacy approach has proven successful in various settings such as inpatient, ambulatory, nursing facility, and resident care.11,16,23–26 Moreover, patient acceptance and satisfaction with telepharmacy services have also been reported in many studies.17,20,27,28 As the overall scope of pharmacy practice expanded during the global COVID-19 pandemic, a shift from traditional care to telepharmacy also occurred rapidly in this period.29,30 Telepharmacy experiences are available in several countries worldwide.14,29 For instance, European countries such as the Netherlands, Italy, and the United Kingdom have implemented remote pharmacist consultations with patients during the pandemic using electronic means of communication.30 Similarly, telepharmacy services have also been implemented in Germany to improve patient outcomes and medication safety.31,32
The Federal Union of German Associations of Pharmacists (ABDA) prioritized DH as one of the first-level priority development goals for 2021.33 Recent years have seen many efforts to digitalize the German healthcare system.34 For instance, the electronic patient record (ePA), prescribable DH applications (DiGAs), and video consultations for HCPs are some of the notable examples.35 The 2024 symposium of the German Federal Chamber of Pharmacists (Bundesapothekerkammer, BAK) specifically focused on the topic of telepharmacy,36 and recently the position papers regarding “telepharmacy in pharmacies” have been adopted by the State Chambers of Pharmacists. These position papers define clear guidelines and standards for the first time from the pharmaceutical perspective to ensure the quality, safety, and efficiency of telepharmacy in community and hospital pharmacies.37,38 Furthermore, changes in regulatory policies such as the inclusion of telepharmacy consultations through amendments to the rules governing the operation of pharmacies (Apothekenbetriebsordnung, ApBetrO) and reimbursement for clinical pharmacy services through the On-site Pharmacy Strengthening Act (Vor-Ort-Apotheken-Stärkungsgesetz, VOASG) have created new opportunities for German pharmacists.39,40 It implies the importance of DH education and training for German pharmacy students to advance their professional development and prepare them for future pharmacy practice.31 The International Pharmaceutical Federation (FIP) reported in its global survey that pharmacy students, practitioners, and academics are interested in learning and teaching about DH tools.41 On the other hand, pharmacy professionals’ lack of interest, low comfort level, and slow adoption of DH technologies have been attributed to inadequate information and limited awareness of or training in these modalities.41–43
DH education and training for pharmacy students require the inclusion of more DH-related content into the curriculum that can be taught theoretically as well as through educational activities and simulations.42–44 In such an effort, the Institute of Clinical Pharmacy and Pharmacotherapy Heinrich Heine University, Duesseldorf has introduced DH education for pharmacy undergraduates by incorporating DH solutions such as mobile health applications (mHealth apps), high-fidelity simulators, and digital medication review tools.45–47 Students are regularly trained in basic foundational skills required for providing clinical pharmacy services in a traditional face-to-face format.48–50 One such service is the inhaler technique training service (In German: Erweiterte Einweisung in die korrekte Arzneimittelanwendung mit Üben der Inhalationstechnik) for patients from six years of age to practice their inhalation technique with a pharmacy professional according to a standardized procedure40 when a new device is prescribed, when an existing device is changed, or when patients have not practiced their inhalation technique at a doctor’s office or community pharmacy in the previous 12 months and have not participated in a disease management program for chronic obstructive pulmonary diseases (COPD) or asthma.51 This service is being reimbursed and provided in-person or through telepharmacy at German community pharmacies.52 In this instance, synchronous videoconferencing is required to demonstrate the inhaler technique and assess patient comprehension.9 It includes a real-time face-to-face encounter with a patient using a two-way interactive audio-video technology.53 Inhaler technique demonstration and practice require a three-dimensional view from the patient and provider39 and a unique set of verbal and nonverbal communication skills.54,55
Telepharmacy consultations involving pharmacist-led video telehealth and telephone calls have facilitated inhaler technique training leading to improved inhaler use and positive patient feedback,56–58 however, there are still questions raised on the practicality of this approach.39 Despite high willingness, readiness, and positive attitudes towards telepharmacy,59–63 there is also a strong perception among pharmacy students and professionals regarding the inability to provide medical device training (such as inhalers, insulin pumps, etc.) via telepharmacy.4,64 Moreover, the literature investigating the suitability of the telepharmacy approach in providing inhaler technique training in terms of the provider’s ability is scant. Therefore, to address these concerns, the primary objective of this study was to ascertain whether the telepharmacy approach is non-inferior to the traditional face-to-face format in terms of pharmacy students’ performance when providing inhaler technique training service. Secondary objectives included student self-assessment of their inhaler technique demonstration and practice skills between two modes of communication and their perceptions of telepharmacy.
Material and Methods
Study Design and Participants
The investigation was conducted as a randomized cross-over non-inferiority trial. The participants were undergraduate pharmacy students in their final semester of pharmacy studies at Heinrich Heine University, Duesseldorf, Germany. We evaluated the effect of different communication mediums on student performance, and self-assessment of their abilities to carry out the inhaler technique demonstration and practice with Standardized Patients (SP). Following the informed consent procedure, participants were randomized to two sequences of simulation, ie, Group A and Group B by using a random number generator in Microsoft Excel 2019.65 In a cross-over design, Group A was first evaluated in a face-to-face simulation followed by telepharmacy, whereas Group B was first evaluated in a telepharmacy simulation followed by a face-to-face simulated patient encounter. The complete study design is illustrated in Figure 1.
 |
Figure 1 Overview of the study design. Abbreviations: OSCE, objective structured clinical examination. |
Study Procedure
The investigation was carried out from May–June 2023 as a part of the Clinical Pharmacy course in the summer semester of 2023. The study was conducted in two stages over four days (Figure 1). Stage 1 included student recruitment during which students were informed about the study and invited to participate followed by randomization to two sequences of simulation. An introductory lecture on inhalation therapy, hands-on training with placebo inhalation devices, and a pre-simulation self-assessment survey were conducted at this stage. The second stage, the simulation encounters, consisted of telepharmacy and face-to-face consultations about the correct use of inhalers between a pharmacy student as the community pharmacist and an SP in a crossover manner. The telepharmacy simulation was conducted using the secured WebEx videoconferencing platform (Cisco Webex, Version 44.1.0.28423). To control for the possible learning effect, students were switched to the second encounter instantaneously without any feedback. For every student, both simulation encounters were identical regarding the examiner and the inhaler device, and differences were the communication medium and SP. During both encounters, the pharmacy students conducted the clinical pharmacy service according to the standard procedure described by the ABDA51 where they first demonstrated the inhaler technique to the SP and then asked the SP to redemonstrate whereby, they identified and corrected the errors made by the SP. According to the Association of Standardized Patient Educators (ASPE) Standards of Best Practice,66 the SPs were trained to act consistently and provided with written instructions to deliberately make one critical error while redemonstrating the inhaler technique. The pre-specified critical inhaler technique errors were included according to each inhaler type.54 Moreover, six different types of inhalers and their critical errors were also randomized to students. Student performance was evaluated during both simulation encounters through Objective Structured Clinical Examinations 1 and 2 (OSCE1 and OSCE2). A post-simulation survey of self-assessment was distributed after period 1 (OSCE 1) and a student perception survey after period 2 (OSCE2) of crossover design.
Objective Structured Clinical Examination (OSCE)
Participants were assessed individually during OSCE1 and OSCE2 in a crossover manner to measure any differences in performance between the two means of communication, ie face-to-face and telepharmacy. Participants were provided with individual time slots and received a brief description of the whole simulation process after registration. An OSCE lasted a maximum of 12 minutes. The eight SPs were played by four faculty members and four final-semester pharmacy students who took part in the pilot study conducted in the scope of their elective course in the winter semester of 2022/23. In total four faculty members served as observers who were different from SPs and replaced after every five students (ie after ten simulated patient encounters as every student completed two OSCEs one after the other). To minimize the variations in assessment, the same observer assessed each participant during both OSCE encounters, however SPs were replaced after each encounter. The observers were replaced purposely to avoid possible fatigue and loss of concentration. The replacement of SPs after each encounter was done to mimic the real pharmacy environment where pharmacists have to deal with different patients during each consultation.
Inhaler Technique Training
After recruitment, all the participants received a lecture on inhalation therapy. The content included background information about inhalation therapy, its history, indications, advantages/disadvantages, different types and principles of inhalation devices, critical errors in inhaler technique, an overview of the inhaler technique training service, and the role of community pharmacists in this regard. Afterward, participants were trained with different types of placebo inhaler devices including the metered dose and dry powder inhalers.
Instruments Used in the Study
Analytical Checklists for OSCE
The analytical checklist was created by faculty members based on previous literature67,68 and by incorporating the necessary steps described by the ABDA in the standard procedure for the inhaler technique training service.51 The analytical checklist was adjusted to every inhaler device type, resulting in six different analytical checklists (Supplementary Material S1-S6). The analytical checklists consisted of three stations with different total scores. Station 1 was related to the initiation of the encounter including the general preparation and introduction with a total of five points. Station 2 comprised the necessary steps of demonstration and practice of the correct inhaler technique with 12–14 points depending on the type of inhaler. Finally, Station 3 was related to communication skills, documentation, and the participant’s ability to recognize critical inhaler technique errors made by SP with a total of eight points. Regarding items performed correctly, one point was awarded, if not zero points were given. Total scores varied among the checklists for every inhaler device, therefore the assessment was based on percentage points. Before the study, the analytical checklists were pilot-tested and discussed among faculty members for comprehensibility and clarity, and necessary revisions were made as needed.
Pulmobox Training Material
Pulmobox was used as the training material for inhaler technique training. The Pulmobox contains around 17 different placebo inhaler devices for demonstration purposes, a manual on counseling aids for inhalation therapy, and information sheets for patient counseling and inhaler technique.54,68
Self-Assessment Questionnaire
To ascertain the impact of different modes of communication on the participant’s self-assessment of their competency in demonstrating and practicing the correct inhaler technique, a pre- and post-simulation self-assessment questionnaire was developed. The pre-survey was conducted before OSCE1, and the post-survey was conducted after OSCE1 where every participant passed through only one format of simulation either face-to-face or telepharmacy therefore they were asked to rate the statements by keeping in mind the communication medium they have recently used for the OSCE1 encounter. The questionnaire consisted of 8 items rated by a six-point Likert-type scale from “strongly disagree” to “strongly agree”. The participant demographic characteristics such as age, gender, additional education as a pharmaceutical technician assistant, current or former work in a community pharmacy, and previous provision of the inhaler technique training service were also included in the self-assessment questionnaire.
Perception Questionnaire
A perception survey was conducted at the end of the study consisting of 10 items rated on a six-point Likert-type scale ranging from “strongly disagree” to “strongly agree”. These items were related to students’ perceptions of; telepharmacy in general, the difference between telepharmacy and face-to-face encounters, and the provision of inhaler technique service through telepharmacy. Additionally, one item was included where the participants were required to rate their experience of telepharmacy simulation. The items were worded based on previous studies of student perceptions regarding telepharmacy.44,69
Statistical Analysis
All the data were collected in pseudonymous form and were anonymized after data analysis. Descriptive statistical analyses were conducted for quantitative survey and analytical checklist data. The Mann–Whitney U-test was used to evaluate student performance and self-assessment regarding inhaler technique demonstration and practice between different mediums of communication. The non-inferiority of the telepharmacy medium compared to the face-to-face medium between groups and per group in terms of the OSCE checklist scores was examined. We defined a non-inferiority margin of −10% based on a previous study.70 To rule out any learning effect from period 1 to period 2 we applied a linear mixed model (LMM) incorporating the intra-individual variation for the non-inferiority analysis, given by

where S0 corresponds to the random intercept of the participants, ß0 (intercept) and ß1 (slope) denote the fixed effects, ITele equals 1 if the participant was assigned to telepharmacy and is 0 otherwise, and e is the residual error of the model. The non-inferiority test was performed as a one-sided t-test based on ß1, ie non-inferiority was concluded at a significance level of alpha = 0.05 if the lower bound of the two-sided 90% confidence interval for ß1 was larger than the non-inferiority margin of −10%. A corresponding p-value was deduced from the one-sided t-test. The model mentioned above was applied in total four times: for the total scores and for each of the three individual stations of OSCEs. Microsoft Excel 201965 was used for data entry, whereas Origin Pro 202171 and R statistical software72 were used for statistical analysis. To account for multiple testing, the Bonferroni-Holm correction was applied. For all statistical analyses, p-values below 0.05 were considered significant.
Ethical Approval
Approval for this study was granted by the responsible Ethics Commission of the Faculty of Medicine, Heinrich Heine University, Duesseldorf (Number: 2023–2401). The participation was voluntary, and all participants provided signed informed consent before the start of the study.
Results
Participant Characteristics
Of 44 students in the last semester of their pharmacy studies, 40 provided informed consent and participated in the study, excluding those four students who took part in the pilot study and served as SPs. A total of 40 participants were randomized to the two sequences (Group A and Group B) of simulation resulting in 20 participants per group; however, one participant from Group A remained absent on the day of OSCE evaluation resulting in a total of 19 participants in Group A. All 39 students participated in the self-assessment and perception surveys. Table 1 provides further details regarding participant characteristics.
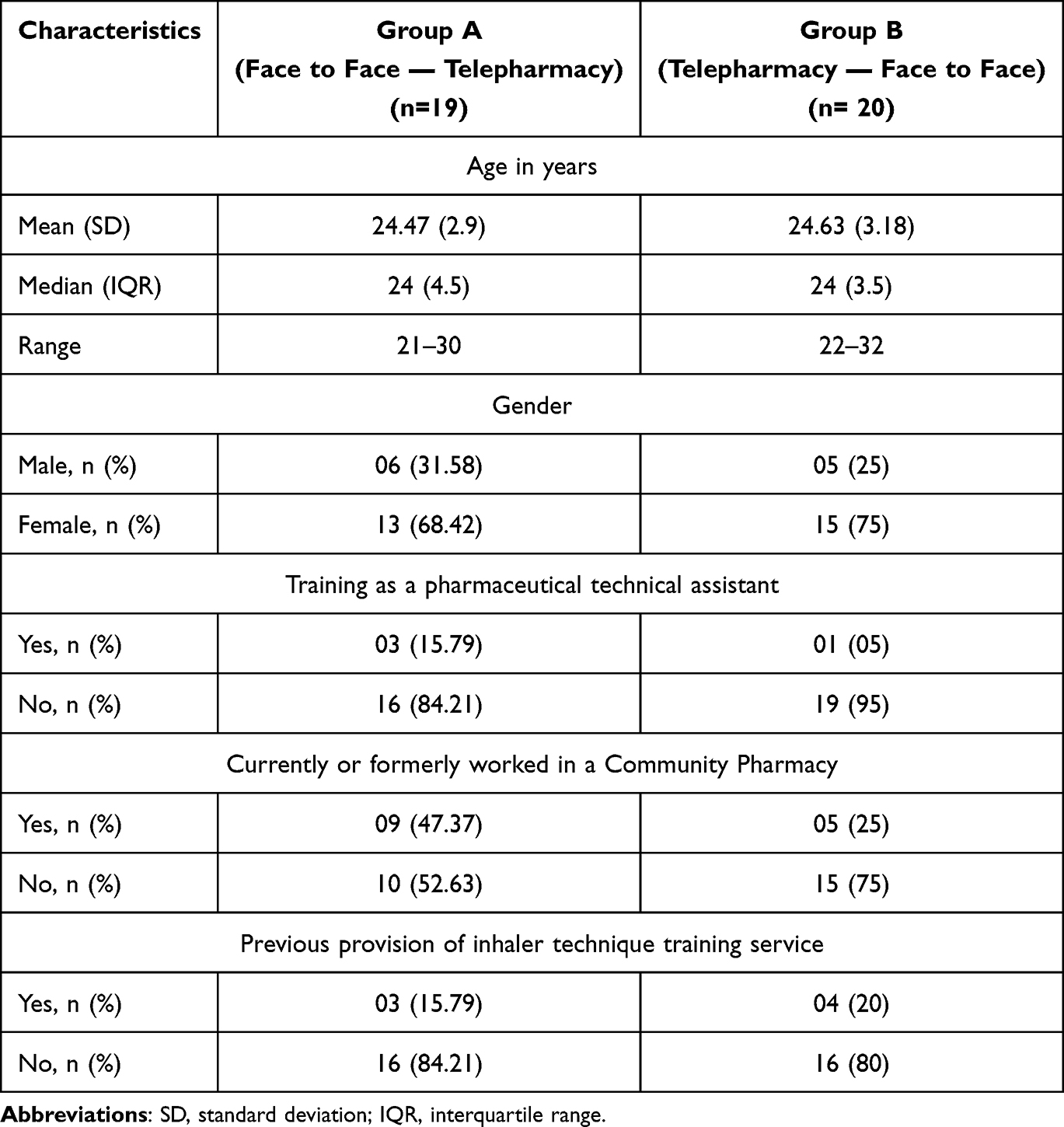 |
Table 1 Participant Characteristics (N = 39) |
OSCE Scores
The total OSCE scores did not differ significantly between the two groups for OSCE1 (p = 0.79) and OSCE2 (p = 0.65). Similarly, the total OSCE scores at two OSCE encounters did not differ significantly within group A (p = 0.23) and group B (p = 0.13). The detailed results for the OSCE scores are depicted in Table 2 and Figure 2. Moreover, on average, the time to complete the simulated patient encounter was 10 minutes for the telepharmacy and 10.2 minutes for the face-to-face consultation formats. Regarding the LMM and non-inferiority analysis in terms of the student performance between different communication mediums, all tests are significant and, consequently, non-inferiority of telepharmacy format in terms of student performance can be concluded at all OSCE stations and for the total OSCE scores, also after adjusting for multiple comparisons. Table 3 summarizes the estimated coefficients, the confidence intervals for ß1, and the p-values of the corresponding non-inferiority tests (unadjusted and adjusted).
 |
Table 2 Achieved OSCE Scores |
 |
Table 3 Coefficients of the Linear Mixed Model and Corresponding Non-Inferiority Analysis |
 |
Figure 2 Box plots of total OSCE scores. Abbreviations: OSCE, objective structured clinical examination. Note: OSCE scores (%) of Group A and Group B during two periods of assessment OSCE1 and OSCE2 showing per group (A) and between-groups (B) comparisons; the p-values were obtained by Mann–Whitney U-tests per group (paired tests) and between groups; p-values below 0.05 were considered significant; Black diamonds = outliers. |
Self-Assessment Score
The self-assessment scores did not differ significantly between groups at baseline (p = 0.75) and after the first simulation activity (p = 0.42). Similarly, there were no significant differences in self-assessment scores from pre- to post-simulation within the telepharmacy group (p = 0.21) and the face-to-face group (p = 1). The detailed results of the self-assessment scores are depicted in Table 4. Regarding individual statements of the post-simulation self-assessment questionnaire, only the statement that concerns the participant’s ability to identify the inhaler technique errors made by patients showed a statistically significant difference (p = 0.03) between telepharmacy and face-to-face formats (Figures 3 and 4).
 |
Table 4 Achieved Scores by Group A and Group B in Pre- and Post-Simulation Self-Assessment Survey |
 |
Figure 3 Box plots of post-self-assessment scores (statements 1–4). Note: post-self-assessment scores of Group A (face-to-face) and Group B (telepharmacy) showing between-group comparisons; Responses were rated on a six-point Likert scale where 1 = strongly disagree and 6 = strongly agree; Black diamonds = outliers; All p-values were obtained from Mann–Whitney U-tests; p-values below 0.05 were considered significant. |
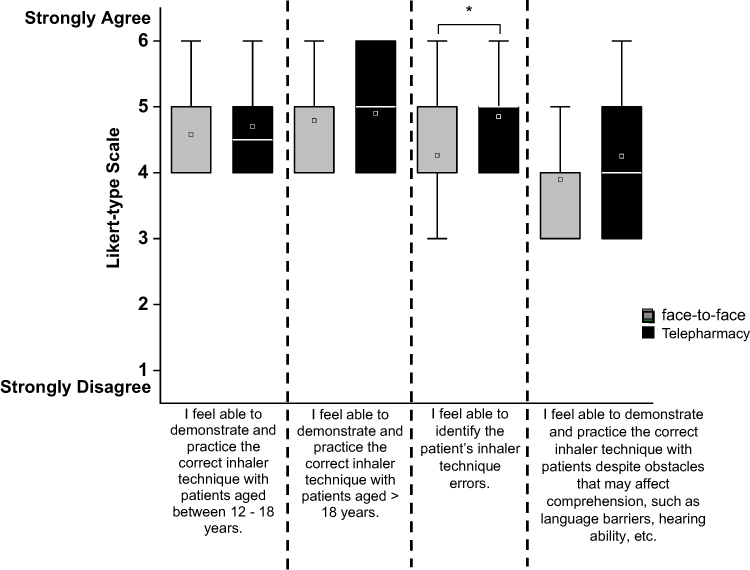 |
Figure 4 Box plots of post-self-assessment scores (statements 5–8). Note: post-self-assessment scores of Group A (face-to-face) and Group B (telepharmacy) showing between-group comparisons; Responses were rated on a six-point Likert scale where 1 = strongly disagree and 6 = strongly agree; Black diamonds = outliers; * p value = 0.03; All p-values were obtained from Mann–Whitney U-tests; p-values below 0.05 were considered significant. |
Perception Survey
The participants reported an overall positive perception of telepharmacy and its use for the provision of inhaler technique training service (Figure 5). All the participants (100%) perceived telepharmacy as another option for patient consultations in the future. A large majority agreed that telepharmacy is future-oriented (92.3%), a suitable approach (92.3%), and a good alternative to face-to-face consultations for providing inhaler technique training service (82.1%). On the other hand, 51.2% of participants found telepharmacy more difficult than face-to-face consultation and found a difference in their verbal (69.2%), and non-verbal (82.1%) communication and their interaction with the patients (64.1%) between the two formats. Most of the participants (79.5%) tend to disagree with the statement that telepharmacy is time-consuming, and all of them (100%) found the educational activity helpful in getting an insight into telepharmacy consultations. These responses are illustrated in Figure 5. The detailed results of the perception survey are also presented in the supplementary Table 1.
 |
Figure 5 Responses to the perception survey (N=39). Note: Responses were rated on a six-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = rather disagree, 4 = rather agree, 5 = agree, 6 = strongly agree); strongly disagree, disagree and rather disagree = disagreement; rather agree, agree, and strongly agree = Agreement. |
Discussion
The randomized cross-over study demonstrates that, based on OSCE scores and a non-inferiority margin of −10%, the telepharmacy approach was non-inferior to the traditional face-to-face approach for demonstrating and practicing the correct inhaler technique. Referring to equally good consultation, whether face-to-face or via telepharmacy for patients living in remote localities or unable to visit the community pharmacy for various reasons. The results also revealed that there are no significant differences in student self-confidence and perceived competence between the two modes of communication. Moreover, participants had a largely positive perception of telepharmacy and its use in providing inhaler technique training service.
We evaluated the student performance between different mediums of communication (face to face and telepharmacy). Students performed equally well regardless of the communication medium during both simulation encounters, the additional practice and previous evaluation during OSCE 1 did not influence their performance in OSCE2 for both groups, and allocation to group A or group B did not advantage or disadvantage them. Students’ ability to conduct telepharmacy consultations without prior practice could be explained by their extensive experience with videoconferencing both during and after COVID-19, a period of digital transformation in education.73,74 Moreover, demographic characteristics showed that the participants of this study belong to Generation Z (persons born between 1997 and 2012) or digital natives who are quite comfortable and expert in using Information and communication technology (ICT).75,76 The present study builds on previous research, which demonstrated that pharmacy students successfully provided consultations via telepharmacy without prior practice, but they were more successful during face-to-face consultations.44 However, that study did not include medical device training and was conducted before the pandemic with minimal exposure to online teaching formats.
Students demonstrated the stepwise standard procedure of the inhaler technique training service equally well using both mediums of communication as shown by the scores at station 2 of relevant OSCEs. Studies have reported the effectiveness of pharmacist-led home video telehealth inhaler training programs in improving inhaler techniques and other patient outcomes.56,57 However, no study evaluated the provider’s abilities in using video telehealth technology to provide inhaler technique training. OSCE scores were also comparable at station 3 which was related to verbal and non-verbal communication skills as well as identification of critical inhaler technique errors made by patients during the encounter. Concerning communication skills Skoy et al found no significant differences in pharmacy students’ verbal communication during face-to-face and telepharmacy consultations, however, there were inappropriate nonverbal cues for the telepharmacy format.44 Another study cited student comments about differences in body language and in developing a relationship with the patient between both formats of consultation.64
The secondary objective of this study was to enhance our understanding of participants’ self-assessment and perceptions of telepharmacy. The simulation activity minimally impacted students’ self-assessment of their abilities to carry out the inhaler technique training service for both mediums of communication. In the post-self-assessment survey, students rated their self-confidence after the first simulation activity where each group had an experience of only one mode of communication, ie either face-to-face or telepharmacy. The self-assessment survey results demonstrate that the telepharmacy format is a viable alternative to the face-to-face format for the provision of inhaler technique training service as participants in both groups rated their competence equally in all aspects of their self-confidence. However, there was a statistically significant difference in participants’ self-assessment of their ability to recognize critical inhaler technique errors made by patients. These findings are interesting as the participants in the telepharmacy group felt more confident in recognizing the critical errors than in the face-to-face group (mean scores 4.85 vs 4.26). Similarly, Porter et al demonstrated that all the pharmacy students who participated in their study were able to identify errors during telepharmacy-based prescription verification activities.69
In our study, participants had an overall positive perception of telepharmacy. Many studies have pointed out the positive perceptions and good acceptance of telepharmacy among pharmacy students and practicing pharmacists.59–63,77 Despite their equivalent performance, most of the participants perceived differences between telepharmacy and face-to-face SP encounters and found telepharmacy as more difficult than the face-to-face approach. In previous studies, pharmacy students have reported perceived differences in their abilities to counsel patients using telepharmacy vs in-person.44,64,69 In our study, this perception could also be attributed to the first formal telepharmacy consultation experience of students during their pharmacy studies. Students agreed to the suitability of telepharmacy for providing inhaler technique training service and found it an alternative to face-to-face format, whereas a previous study conducted with 390 pharmacy students in two pharmacy programs reported perceived difficulties in providing medical device training through telepharmacy; however, the authors of that study suggested that these perceptions could be addressed with extra practice and training in telepharmacy.64
We believe that the simulated telepharmacy encounter with SPs also provided the students with an opportunity to practice their foundational consultation skills in new ways of pharmacy practice as students agreed to the statement that the simulation gave them an insight into telepharmacy consultations. It has also previously been reported that simulated telehealth encounters improved communication skills and enhanced learning among medical and nursing students.78,79 This experience is also shared by pharmacy students, who felt that telepharmacy simulations improved their comfort and confidence in utilizing this technology in the future.69 International telepharmacy guidelines and professional pharmacy associations emphasize the importance of training for all involved persons in topics of communication, telepharmacy technology, service delivery processes and staff expectations, privacy and security issues, and requirements for documentation.80,81 Among other means of electronic communication, videoconferencing is becoming popular for patient consultations, and previously videoconferencing systems have been used to train online consultation skills among healthcare professional students.82 In the future, this research could lead to more adoption of the telepharmacy approach for providing inhaler technique training service and other pharmaceutical care services at community pharmacies in Germany. It could also help in taking academic initiatives aimed at incorporating more telepharmacy practice models into the professional development of the future pharmacy workforce.
Our study is subjected to certain limitations. First, the present study was conducted at a single university and involved a small sample size thereby limiting the generalizability of the results. Secondly, there may be a learning effect from OSCE1 to OSCE2, however, to minimize it, students were immediately switched from one format to the other without any feedback in between and further, the statistical analysis ruled out this effect during data analysis. Thirdly, we did not collect data about students’ previous experience with telepharmacy during their internships or other experiential education that may have affected the results. Finally, the SP encounters did not represent all patient populations (different age groups, language barriers, digital literacy, etc.) and consultation scenarios students could face while providing inhaler technique training service through videoconferencing such as technical issues, low-video quality, etc. Further research could be conducted with real patients and practicing pharmacists in real-world scenarios to determine the non-inferiority of the telepharmacy format over the face-to-face medium of communication and to further explore the acceptance of telepharmacy in this regard.
Conclusion
The results from the study suggest that telepharmacy is as effective as traditional face-to-face consultation for providing inhaler technique training service. The anticipated comparable OSCE scores, self-confidence, and positive perceptions about telepharmacy supported the idea that implementation may occur and be delivered as routine clinical pharmacy services. The successful telepharmacy implementations worldwide, in particular during the COVID-19 pandemic unearthed new possibilities for providing specialized pharmaceutical care services through telepharmacy. However, to address the special training needs of the pharmacy workforce such as those related to verbal and non-verbal communication skills, telepharmacy technology, etiquette, and other related requirements when performing telepharmacy services, the pharmacy curriculum should include more telepharmacy-related didactic content along with experiential learning and simulations.
Acknowledgments
The authors thank all the study participants; the faculty members Jutta Tins, Anke Bartel, Florian Andreas Kinny, and Ahmed Reda Sharkas for taking over the role of standardized patients; the final year pharmacy students Natalie Beckmann, Sakineh Asgari, Bijeng Urun, and Iman Mortga for taking over the role of standardized patients; the faculty members Armin Dabidian, Melina Steichert, and Sabina Schlottau for taking over the role of raters during the OSCEs. The authors would also like to acknowledge that Heinrich Heine University Düsseldorf funded the publication fees. The research work of B.A.S. was supported by a scholarship from the Higher Education Commission (HEC), Pakistan in collaboration with the German Academic Exchange Service (DAAD), Germany.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Turner A, Morris R, Rakhra D, et al. Unintended consequences of online consultations: a qualitative study in UK primary care. Br J Gen Pract. 2022;72(715):e128–e137. doi:10.3399/BJGP.2021.0426
2. Raja M, Bjerkan J, Kymre IG, Galvin KT, Uhrenfeldt L. Telehealth and digital developments in society that persons 75 years and older in European countries have been part of: a scoping review. BMC Health Serv Res. 2021;21(1):1157. doi:10.1186/s12913-021-07154-0
3. Cao DX, Tran RJC, Yamzon J, Stewart TL, Hernandez EA. Effectiveness of telepharmacy diabetes services: a systematic review and meta-analysis. Am J Health Syst Pharm. 2022;79(11):860–872. doi:10.1093/ajhp/zxac070
4. Lobkovich A, Javed S, Hammoud R, Habhab A, Lipari M. Pharmacist perceptions of delivering patient care through telehealth. Am J Health Syst Pharm. 2024;81:539–545. doi:10.1093/ajhp/zxae020
5. Golinelli D, Boetto E, Carullo G, Nuzzolese AG, Landini MP, Fantini MP. Adoption of digital technologies in health care during the COVID-19 pandemic: Systematic review of early scientific literature. J Med Internet Res. 2020;22(11):e22280. doi:10.2196/22280
6. Tuckson RV, Edmunds M, Hodgkins ML. Telehealth. N Engl J Med. 2017;377(16):1585–1592. doi:10.1056/NEJMsr1503323
7. Lewinski AA, Walsh C, Rushton S, et al. Telehealth for the longitudinal management of chronic conditions: Systematic review. J Med Internet Res. 2022;24(8):e37100. doi:10.2196/37100
8. Alexander E, Butler CD, Darr A, et al. ASHP Statement on Telepharmacy. Am J Health Syst Pharm. 2017;74(9):e236–e241. doi:10.2146/ajhp170039
9. Killeen RM, Grindrod K, Ong SW. Innovations in practice: Telepharmacy’s time has arrived. Can Pharm J. 2020;153(5):252–255. doi:10.1177/1715163520945732
10. Manuel FC, Wieruszewski ED, Brown CS, Russi CS, Mattson AE. Description of telepharmacy services by emergency medicine pharmacists. Am J Health Syst Pharm. 2022;79(11):873–880. doi:10.1093/ajhp/zxac027
11. Niznik JD, He H, Kane-Gill SL. Impact of clinical pharmacist services delivered via telemedicine in the outpatient or ambulatory care setting: a systematic review. Res Social Adm Pharm. 2018;14(8):707–717. doi:10.1016/j.sapharm.2017.10.011
12. Nkemdirim Okere A, Balogun A, Smith A, Stevens J. Association between pharmacist-led telehealth services and improvements in cardiovascular outcomes among patients with cardiovascular risk factors: a scoping review. Int J Cardiol Cardiovasc Risk Prev. 2023;19:200206. doi:10.1016/j.ijcrp.2023.200206
13. Cohen LB, Taveira TH, Wu WC, Pirraglia PA. Pharmacist-led telehealth disease management program for patients with diabetes and depression. J Telemed Telecare. 2020;26(5):294–302. doi:10.1177/1357633X18822575
14. Baldoni S, Amenta F, Ricci G. Telepharmacy Services: present Status and Future Perspectives: a Review. Medicina. 2019;55(7):327. doi:10.3390/medicina55070327
15. Brown W, Scott D, Friesner D, Schmitz T. Impact of telepharmacy services as a way to increase access to asthma care. J Asthma. 2017;54(9):961–967. doi:10.1080/02770903.2017.1281292
16. Win AZ. Telepharmacy: time to pick up the line. Res Social Adm Pharm. 2017;13(4):882–883. doi:10.1016/j.sapharm.2015.06.002
17. You A, Kawamoto J, Smith JP. A pharmacist-managed telemedicine clinic for hepatitis C care: a descriptive analysis. J Telemed Telecare. 2014;20(2):99–101. doi:10.1177/1357633X13519043
18. Lertsinudom S, Tiamkao S, Mungmanitmongkol S, Dilokthornsakul P. Telepharmacy services to support patients with epilepsy in Thailand: a descriptive study. Heliyon. 2023;9(2):e13361. doi:10.1016/j.heliyon.2023.e13361
19. Omboni S, Tenti M, Coronetti C. Physician-pharmacist collaborative practice and telehealth may transform hypertension management. J Hum Hypertens. 2019;33(3):177–187. doi:10.1038/s41371-018-0147-x
20. Rothwell M, Hogan A Clinical pharmacists connecting with patients in rural and remote towns via telehealth.
21. Cigolle C, Phillips K. Telepharmacy Model of Care. Clin Ther. 2023;45(10):935–940. doi:10.1016/j.clinthera.2023.08.009
22. Poudel A, Nissen LM. Telepharmacy: a pharmacist’s perspective on the clinical benefits and challenges. Integr Pharm Res Pract. 5:75–82. doi:10.2147/IPRP.S101685
23. Kane-Gill SL, Niznik JD, Kellum JA, et al. Use of Telemedicine to Enhance Pharmacist Services in the Nursing Facility. Consult Pharm. 2017;32(2):93–98. doi:10.4140/TCP.n.2017.93
24. McFarland R. Telepharmacy for remote hospital inpatients in north-west Queensland. J Telemed Telecare. 2017;23(10):861–865. doi:10.1177/1357633X17732367
25. Keeys C, Kalejaiye B, Skinner M, et al. Pharmacist-managed inpatient discharge medication reconciliation: a combined onsite and telepharmacy model. Am J Health Syst Pharm. 2014;71(24):2159–2166. doi:10.2146/ajhp130650
26. Erickson AK, Yap D. On the line: telepharmacy technology expands hospital pharmacists’ reach. Pharm Today. 2016;22(4):4–5. doi:10.1016/j.ptdy.2016.10.038
27. Margusino-Framiñán L, Fernández-Llamazares CM, Negro-Vega E, et al. Outpatients’ Opinion And Experience Regarding Telepharmacy During The COVID-19 Pandemic: the Enopex Project. J Multidiscip Healthc. 2021;14:3621–3632. doi:10.2147/JMDH.S343528
28. Al Ammari M, AlThiab K, AlJohani M, et al. Tele-pharmacy Anticoagulation Clinic During COVID-19 Pandemic: patient Outcomes. Front Pharmacol. 2021;12:652482. doi:10.3389/fphar.2021.652482
29. Sarasmita MA, Sudarma IW, Jaya MKA, Irham LM, Susanty S. Telepharmacy Implementation to Support Pharmaceutical Care Services during the COVID-19 Pandemic: a Scoping Review. Can J Hosp Pharm. 2024;77(1):e3430. doi:10.4212/cjhp.3430
30. Merks P, Jakubowska M, Drelich E, et al. The legal extension of the role of pharmacists in light of the COVID-19 global pandemic. Res Social Adm Pharm. 2021;17(1):1807–1812. doi:10.1016/j.sapharm.2020.05.033
31. Koeck JA, Dohmen SM, Marx G, Eisert A. Comparison of Drug-Related Problems in COVID-19 and Non-COVID-19 Patients Provided by a German Telepharmacy Service for Rural Intensive Care Units. J Clin Med. 2023;12(14):4739. doi:10.3390/jcm12144739
32. Amkreutz J, Lenssen R, Marx G, Deisz R, Eisert A. Medication safety in a German telemedicine centre: implementation of a telepharmaceutical expert consultation in addition to existing tele-intensive care unit services. J Telemed Telecare. 2020;26(1–2):105–112. doi:10.1177/1357633X18799796
33. International Pharmaceutical Federation (FIP). The FIP Development Goals Report 2021: setting goals for the decade ahead The Hague: International Pharmaceutical Federation; 2022. Available from: https://developmentgoals.fip.org/global-report-2021/.
34. Driving the digital transformation of Germany’s healthcare system for the good of patients. Digital Healthcare Act (DVG). Federal Ministry of Health. Available from: https://www.bundesgesundheitsministerium.de/en/digital-healthcare-act.
35. Telemedicine on the rise – the legal framework and potential for development; 2022. Available from: https://www.gleisslutz.com/en/telemedicine_on_the_rise.html.
36. BAK-Symposium “Telepharmazie-Chancen und Grenzen” [“Telepharmacy-Opportunities and limitations”]. ABDA. Available from: https://www.abda.de/aktuelles-und-presse/veranstaltungen/detail/bak-symposium-telepharmazie-chancen-und-grenzen/.
37. Statt „irgendwie so” auf fundierter Basis die Chancen der Digitalisierung in der Apotheke nutzen [Using the opportunities of digitalisation in pharmacies on a sound basis instead of ‘just like that’]. Apothekerkammer Nordrhein. Available from: https://www.aknr.de/presse/pressemitteilungen/positionspapier-telepharmazie-ausschuss-fuer-digitalisierung-aknr.
38. Positionspapiere zur Telepharmazie verabschiedet [Position papers on telepharmacy adopted]. ABDA. Available from: https://www.abda.de/aktuelles-und-presse/newsroom/detail/positionspapiere-zur-telepharmazie-verabschiedet/.
39. Bettina M, Sarah W. Telepharmazie Arbeitshilfe Für Die Apotheke [Telepharmacy Guide for the Pharmacy]. Stuttgart: Deutscher Apotheker Verlag; 2023.
40. Schulz M, Griese-Mammen N, Müller U. Clinical pharmacy services are reimbursed in Germany: challenges of real world implementation remain. Int J Clin Pharm. 2023;45(1):245–249. doi:10.1007/s11096-022-01492-7
41. International Pharmaceutical Federation (FIP). FIP Digital health in pharmacy education. The Hague: International Pharmaceutical Federation; 2021. Available from: https://www.fip.org/file/4958.
42. Frenzel J, Porter A. The Need to Educate Pharmacy Students in Telepharmacy and Telehealth. Am J Pharm Educ. 2021;85(8):8566. doi:10.5688/ajpe8566
43. International Pharmaceutical Federation (FIP). Advancements in digital pharmacy post COVID-19: report from the FIP Technology Advisory Group. The Hague: International Pharmaceutical Federation, 2023. Available from: https://www.fip.org/file/5528.
44. Skoy ET, Eukel HN, Frenzel JE, Schmitz TM. Performance and Perceptions: evaluation of Pharmacy Students’ Consultation via Telepharmacy. J Pharm Technol. 2015;31(4):155–160. doi:10.1177/8755122514568123
45. Obarcanin E, Ali-Sherazi B, Dabidian A, Schlottau S, Deters MA, Läer S. Introducing m-Health and Digital Diabetes Apps in Clinical Pharmacy Education in Germany. J Diabetes Clin Res. 2022;4:17–19.
46. Dabidian A, Obarcanin E, Ali Sherazi B, Schlottau S, Schwender H, Laeer S. Impact of a Digital Tool on Pharmacy Students’ Ability to Perform Medication Reviews: a Randomized Controlled Trial. Healthcare. 2023;11(13):1968. doi:10.3390/healthcare11131968
47. Sayyed SA, Sharkas AR, Ali Sherazi B, Dabidian A, Schwender H, Laeer S. Development and Assessment of Innovative High-Fidelity Simulation Vaccination Course Integrating Emergency Cases for Pharmacy Undergraduates-A Randomized Controlled Study. Vaccines. 2023;11(2):324. doi:10.3390/vaccines11020324
48. Farahani I, Laeer S, Farahani S, Schwender H, Laven A. Blended learning: improving the diabetes mellitus counseling skills of German pharmacy students. Curr Pharm Teach Learn. 2020;12(8):963–974. doi:10.1016/j.cptl.2020.04.016
49. Farahani I, Farahani S, Deters MA, Schwender H, Laeer S. Training Pharmacy Students in Self-Medication Counseling Using an Objective Structured Clinical Examination-Based Approach. J Med Educ Curric Dev. 2021;8:23821205211016484. doi:10.1177/23821205211016484
50. Farahani I, Farahani S, Deters MA, Schwender H, Laeer S. Efficacy of an Objective Structured Clinical Examination Training Approach for Training Pharmacy Students in Diabetes Mellitus Counseling: a Randomized Controlled Trial. Pharmacy. 2020;8(4):229. doi:10.3390/pharmacy8040229
51. Erweiterte Einweisung in die korrekte Arzneimittelanwendung mit Üben der Inhalationstechnik [extended instruction in the correct use of medication with practice of the inhalation technique]. ABDA. Available from: https://www.abda.de/pharmazeutische-dienstleistungen/inhalativa/.
52. Neuer Weg: telepharmazie der Apotheken [New path: telepharmacy in pharmacies]. ABDA. Available from: https://www.abda.de/aktuelles-und-presse/newsroom/detail/neuer-weg-telepharmazie-der-apotheken/.
53. Badowski ME, Walker S, Bacchus S, et al. Providing Comprehensive Medication Management in Telehealth. Pharmacotherapy. 2018;38(2):e7–e16. doi:10.1002/phar.2071
54. Jaeschke R, Spindler T. Handbuch Beratungshilfen Zur Inhalationstherapie [Handbook of Counseling Aids for Inhalation Therapy]. Stuttgart: Deutscher Apotheker Verlag; 2019.
55. Jaeschke R, Spindler T. Inhalativa. Standardisierte, erweiterte Einweisung in die korrekte Arzneimittelanwendung und Üben der Inhalationstechnik – Arbeitshilfe für die Apotheke [Inhalers. Standardised, extended instruction in the correct use of medicines and practicing the inhalation technique - a guide for pharmacies]. Stuttgart: Deutscher Apotheker Verlag; 2023.
56. Locke ER, Thomas RM, Woo DM, et al. Using Video Telehealth to Facilitate Inhaler Training in Rural Patients with Obstructive Lung Disease. Telemed J E Health. 2019;25(3):230–236. doi:10.1089/tmj.2017.0330
57. Thomas RM, Locke ER, Woo DM, et al. Inhaler Training Delivered by Internet-Based Home Videoconferencing Improves Technique and Quality of Life. Respir Care. 2017;62(11):1412–1422. doi:10.4187/respcare.05445
58. Margolis A, Young H, Lis J, Schuna A, Sorkness CA. A telepharmacy intervention to improve inhaler adherence in veterans with chronic obstructive pulmonary disease. Am J Health Syst Pharm. 2013;70(21):1875–1876. doi:10.2146/ajhp120241
59. Alfian SD, Khoiry QA, Pratama AA, et al. Knowledge, perception, and willingness to provide telepharmacy services among pharmacy students: a multicenter cross-sectional study in Indonesia. BMC Med Educ. 2023;23(1):800. doi:10.1186/s12909-023-04790-4
60. Tegegne MD, Wubante SM, Melaku MS, et al. Tele-pharmacy perception, knowledge and associated factors among pharmacy students in northwest Ethiopia: an input for implementers. BMC Med Educ. 2023;23(1):130. doi:10.1186/s12909-023-04111-9
61. Elnaem MH, Akkawi ME, Al-Shami AK, Elkalmi R. Telepharmacy knowledge, perceptions, and readiness among future Malaysian pharmacists amid the COVID-19 pandemic. Indian J Pharm Educ Res. 2022;56:9–16. doi:10.5530/ijper.56.1.2
62. Ahmed NJ, Almalki ZS, Alsawadi AH, et al. Knowledge, perceptions, and readiness of telepharmacy among community pharmacists. Saudi Pharm J. 2023;31(9):101713. doi:10.1016/j.jsps.2023.101713
63. Ahmed NJ, Almalki ZS, Alsawadi AH, et al. Knowledge, Perceptions, and Readiness of Telepharmacy among Hospital Pharmacists in Saudi Arabia. Healthcare. 2023;11(8):1087. doi:10.3390/healthcare11081087
64. Frenzel JE, Porter AL. Design and Assessment of Telepharmacy and Telehealth Training in Two Pharmacy Programs. Am J Pharm Educ. 2023;87(2):ajpe8800. doi:10.5688/ajpe8800
65. Microsoft Corporation. Microsoft Excel. Redmond, WA, USA: Microsoft Corporation; 2019.
66. Lewis KL, Bohnert CA, Gammon WL, et al. The Association of Standardized Patient Educators (ASPE) Standards of Best Practice (SOBP). Adv Simul. 2:10. doi:10.1186/s41077-017-0043-4
67. Basheti IA, Qunaibi EA, Hamadi SA, Reddel HK. Inhaler technique training and health-care professionals: effective long-term solution for a current problem. Respir Care. 2014;59(11):1716–1725. doi:10.4187/respcare.02671
68. Jaeschke R, Spindler T. Pulmobox – Demogeräte Und Beratungshilfen [Pulmobox - Demo Devices and Counseling Aids]. Stuttgart: Deutscher Apotheker Verlag; 2019.
69. Porter AL, Frenzel JE, Siodlak MM. Assessment of a two-school collaborative telepharmacy simulation. Curr Pharm Teach Learn. 2022;14(2):215–221. doi:10.1016/j.cptl.2021.11.020
70. Farahani S, Farahani I, Burckhardt BB, Schwender H, Laeer S. Self-Instruction Video Versus Face-to-Face Instruction of Pharmacy Students’ Skills in Blood Pressure Measurement. Pharmacy. 2020;8(4):217. doi:10.3390/pharmacy8040217
71. OriginLab Corporation. Origin(Pro); OriginLab Corporation Northampton, MA, USA; 2021
72. Team R. RStudio: integrated Development Environment for R. RStudio, PBC, Boston, MA. 2021. Available from: http://www.rstudio.com/.
73. Camilleri MA, Camilleri AC. The Acceptance of Learning Management Systems and Video Conferencing Technologies: lessons Learned from COVID-19. Tech Know Learn. 2022;27:1311–1333. doi:10.1007/s10758-021-09561-y
74. Gorina L, Gordova M, Khristoforova I, Sundeeva L, Strielkowski W. Sustainable Education and Digitalization through the Prism of the COVID-19 Pandemic. Sustainability. 2023;15(8):6846. doi:10.3390/su15086846
75. Silva ROS, de Araújo DCSA, Dos Santos MPW, Neves ERZ, de Lyra DPJ. Digital pharmacists: the new wave in pharmacy practice and education. Int J Clin Pharm. 2022;44(3):775–780. doi:10.1007/s11096-021-01365-5
76. Shorey S, Chan V, Rajendran P, Ang E. Learning styles, preferences and needs of generation Z healthcare students: scoping review. Nurse Educ Pract. 2021;57:103247. doi:10.1016/j.nepr.2021.103247
77. Siddiqua A, Makki S, Siddiqui S, et al. Community Pharmacists’ Knowledge and Perception towards Telepharmacy Services and Willingness to Practice It in Light of COVID-19. Int J Clin Pract. 2024:6656097. doi:10.1155/2024/6656097
78. Liu C, Lim RL, McCabe KL, Taylor S, Calvo RA. A Web-Based Telehealth Training Platform Incorporating Automated Nonverbal Behavior Feedback for Teaching Communication Skills to Medical Students: a Randomized Crossover Study. J Med Internet Res. 2016;18(9):e246. doi:10.2196/jmir.6299
79. Smith TS, Watts P, Moss JA. Using Simulation to Teach Telehealth Nursing Competencies. J Nurs Educ. 2018;57(10):624–627. doi:10.3928/01484834-20180921-10
80. Morillo-Verdugo R, Margusino-Framiñán L, Monte-Boquet E, et al. Spanish Society of Hospital Pharmacy Position Statement on Telepharmacy: recommendations for its implementation and development. Farm Hosp. 44(4):174–181. doi:10.7399/fh.11515
81. Canadian Society of Hospital Pharmacist. Telepharmacy Guidelines. Ottawa. 2018. Available from: https://www.telemedecine-360.com/wpcontent/uploads/2019/03/2018-CSHP-Telepharmacy-Guidelines.pdf.
82. Kyyhkynen R, Peltonen LM, Smed J. Videoconferencing Applications for Training Professionals on Nonverbal Communication in Online Clinical Consultations. Healthc Inform Res. 2023;29(4):394–399. doi:10.4258/hir.2023.29.4.394
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.