Back to Journals » Drug Design, Development and Therapy » Volume 20
Tegileridine, a Biased μ-Opioid Receptor Agonist, versus Oxycodone for Postoperative Analgesia and Postoperative Nausea and Vomiting After Total Laparoscopic Hysterectomy: A Randomized, Double-Blind, Single-Center, Controlled Trial
Authors Fu Y ![]() , Chen X
, Chen X ![]() , Gao FP, Liang Y, Wang DY, Chen CQ, Sun H
, Gao FP, Liang Y, Wang DY, Chen CQ, Sun H
Received 23 January 2026
Accepted for publication 14 May 2026
Published 21 May 2026 Volume 2026:20 598457
DOI https://doi.org/10.2147/DDDT.S598457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Solomon Tadesse Zeleke
Yu Fu, Xin Chen, Fang-Peng Gao, Yu Liang, Dong-Yu Wang, Cai-Qiao Chen, Hu Sun
Department of Anesthesia, The Second Affiliated Hospital of Hainan Medical University, Haikou, Hainan, People’s Republic of China
Correspondence: Hu Sun, Department of Anesthesia, The Second Affiliated Hospital of Hainan Medical University, No. 368 Yehai Avenue, Longhua District, Haikou, Hainan, 570311, People’s Republic of China, Tel +86 18189885268, Email [email protected]
Background: Patients undergoing total laparoscopic hysterectomy (TLH) commonly experience postoperative pain and are at relatively high risk of postoperative nausea and vomiting (PONV). Tegileridine is a recently developed biased μ-opioid receptor (MOR) agonist that may preserve analgesic efficacy while being associated with a lower incidence of opioid-related adverse effects.
Objective: To evaluate whether tegileridine, compared with oxycodone at prespecified study doses, is associated with a lower incidence of PONV while providing similar early postoperative analgesic efficacy in patients undergoing TLH.
Methods: This randomized, double-blind, single-center trial planned to enroll 66 adult women undergoing TLH. Participants were randomly assigned to the tegileridine group (group T) or the oxycodone group (group O). According to the study protocol, all patients received standardized anesthesia and surgery and were given intravenous tegileridine 0.01 mg·kg− 1 (group T) or oxycodone 0.06 mg·kg− 1 (group O) 20 minutes before the end of surgery. Data collected within 48 hours after surgery included the incidence and ordinal symptom grade of PONV, postoperative analgesic success rate, mean arterial pressure at predefined time points, the incidence of other adverse events, use of vasoactive medications, time to first patient-controlled intravenous analgesia (PCIA) demand, and the total number of PCIA demands within 24 and 48 hours.
Results: A total of 68 patients were enrolled, with comparable baseline characteristics between groups. Compared with oxycodone, tegileridine was associated with a lower incidence of PONV (27.3% vs 54.3%; RR, 0.50; 95% CI, 0.27– 0.95; P = 0.024), a lower ordinal PONV symptom grade [0 (0– 1) vs 1 (0– 3); P = 0.012], and a lower overall incidence of other adverse events (27.3% vs 60.0%; P = 0.007). Postoperative analgesic success rates were similar between groups (87.9% vs 94.3%; P = 0.615). No significant between-group differences were observed in mean arterial pressure, vasoactive medication use, time to first PCIA demand, or total PCIA demands within 24 and 48 hours.
Conclusion: In patients undergoing TLH, tegileridine was associated with a similar postoperative analgesic success rate and a lower risk of PONV compared with oxycodone.
Trial Registration: This trial was retrospectively registered at ClinicalTrials.gov after patient enrollment had begun (NCT07326683).
Keywords: biased μ-opioid receptor agonist, oxycodone, postoperative analgesia, postoperative nausea and vomiting, tegileridine, total laparoscopic hysterectomy
Introduction
Acute postoperative pain remains inadequately managed worldwide, with up to 75% of patients experiencing moderate to severe pain following surgery.1,2 Total laparoscopic hysterectomy (TLH) is a clinically relevant model for this study because hysterectomy remains a common gynecologic procedure, and laparoscopic hysterectomy is widely used for symptomatic benign uterine disease such as leiomyomas, abnormal uterine bleeding, endometriosis, and prolapse when conservative treatment is unsuccessful.3 This population is particularly suitable for evaluating postoperative analgesia and postoperative nausea and vomiting (PONV), because gynecologic laparoscopy is a recognized high-risk setting for PONV and postoperative pain after TLH still requires structured analgesic management.4–6
Oxycodone is a μ-opioid receptor (MOR) agonist widely used for perioperative analgesia. The equianalgesic dose ratio (EDR) of intravenous oxycodone relative to morphine is 1.48.7 At a morphine-equivalent analgesic dose, oxycodone has been reported to provide longer-lasting analgesia with fewer adverse effects than morphine.8,9 In addition, a dose-finding study in patients undergoing laparoscopic hysterectomy reported that the median effective dose (ED50) of a single intravenous bolus of oxycodone for postoperative analgesia was 0.060 mg·kg−1.10 However, like other MOR agonists, oxycodone remains associated with opioid-related adverse effects, including nausea, vomiting, and constipation, and placebo-controlled studies have shown higher rates of nausea and vomiting in oxycodone-treated patients.11,12
Tegileridine is a biased MOR agonist that has been shown to selectively activate G protein-coupled pathways and produce central analgesic effects. Tegileridine has been reported to have limited propensity to activate β-arrestin-2-related pathways associated with respiratory depression and gastrointestinal dysfunction, which may reduce opioid-related adverse effects, including nausea and vomiting.13 Published evidence available at the time of trial design suggested that, at a morphine-equivalent analgesic dose, tegileridine has approximately ninefold the analgesic potency of morphine, whereas oxycodone has approximately 1.5-fold the analgesic potency of morphine.14 On the basis of these indirect morphine-equivalent analgesic considerations, tegileridine 0.01 mg·kg−1 and oxycodone 0.06 mg·kg−1 were selected as the prespecified study doses for this trial. We therefore hypothesized that, in patients undergoing TLH, tegileridine at the prespecified study dose would be associated with a lower incidence of PONV while providing similar postoperative analgesic efficacy compared with oxycodone.
Methods
Study Design, Ethics Approval, and Trial Registration
This randomized, double-blind, single-center controlled trial was conducted at the Second Affiliated Hospital of Hainan Medical University. The study protocol was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Hainan Medical University before patient enrollment (Approval No. 2025-KY82). Written informed consent was obtained from all participants before enrollment. The trial was conducted in accordance with the Declaration of Helsinki and current Good Clinical Practice guidelines.
Eligible participants were adult women who underwent TLH at the Second Affiliated Hospital of Hainan Medical University between December 17, 2025, and January 13, 2026. Patient enrollment began on December 17, 2025. Owing to an administrative coordination delay in submitting the prepared registration information to the registry, the trial was retrospectively registered at ClinicalTrials.gov after patient enrollment had begun. The trial was first submitted to ClinicalTrials.gov on December 24, 2025, and first posted on January 8, 2026 (NCT07326683). The registration was completed before database lock and final statistical analysis.
Participants
Inclusion Criteria
Patients were eligible for enrollment if they met all of the following criteria:
- Female patients scheduled to undergo TLH under general anesthesia.
- Aged 18–65 years, with a body mass index (BMI) ranging from 18 to 28 kg·m−2.
- American Society of Anesthesiologists (ASA) physical status I to III.
- Patients who consent to postoperative pain management and sign the informed consent form.
Exclusion Criteria
Patients were excluded if they met any of the following criteria:
- Known hypersensitivity to any study-related medication.
- Severe cardiovascular, respiratory, or neurological disease, including but not limited to acute myocardial infarction, cerebrovascular accident, or chronic obstructive pulmonary disease.
- Long-term use of sedatives or analgesics, or a history of opioid use disorder.
- Altered mental status, impaired communication, or inability to understand the study procedures or provide valid informed consent.
Withdrawal Criteria
Participants were withdrawn from the study under any of the following conditions:
- Occurrence of a serious adverse event (AE) requiring discontinuation of the study.
- Withdrawal of consent or loss to follow-up.
- Conversion from laparoscopic surgery to open surgery.
Anesthesia and Study Interventions
Anesthesia induction was initiated in accordance with a rapid sequence protocol, involving the intravenous administration of the following medications in preset doses: propofol at 2 mg·kg−1, cisatracurium besylate at 0.2 mg·kg−1, and remifentanil at 1 μg ·kg−1. Following the administration of the study drug, all patients were fitted with a size 7.0 ID endotracheal tube. Anesthesia was sustained using propofol at 4–12 mg·kg−1·h−1 and remifentanil at 0.02–0.2 ug·kg−1·h−1. The study drug was administered 20 minutes before the end of surgery (T1): Group T received 0.01 mg·kg−1 of tegileridine (dissolved in 10 mL of 0.9% sodium chloride injection solution and administered via continuous infusion at a rate of 60 mL·h−1 until completion). Group O received 0.06 mg·kg−1 of oxycodone (dissolved in 10 mL of 0.9% sodium chloride injection solution and administered via continuous infusion at a rate of 60 mL·h−1 until completion). Vital signs were recorded at 3 minutes (T2) and 5 minutes (T3) following the completion of the drug infusion. The infusion of maintenance anesthetics was discontinued at the conclusion of surgery (T4). Patients were subsequently transferred to the Postanesthesia care unit (PACU), and 40 mL of 0.25% ropivacaine was administered bilaterally into the transversus abdominis plane (TAP). After the patients regained consciousness (T5), the endotracheal tube was removed following confirmation of extubation criteria. Within one hour after extubation, if the patients reported no discomfort, a patient-controlled intravenous analgesia (PCIA) pump was initiated (2 μg·kg−1 sufentanil diluted in 100 mL of 0.9% saline, with no background infusion rate, a 2 mL bolus per dose, and a 20-minute lockout period), and the patients was returned to the ward. Postoperative follow-up was conducted over a period of two days, during which relevant data were collected.
During the surgical procedure, cisatracurium 0.05 mg·kg−1 was administered as needed. If severe bradycardia (heart rate < 45/min) occurred, or if hypotension (NBP decreased by 20% from baseline) happened, patients received atropine 0.3–0.5 mg or ephedrine 6–10 mg, as appropriate. If surgery was completed but the TOF ratio was <0.9, neostigmine 0.02–0.04 mg·kg−1 and atropine 0.01 mg·kg−1 were given to reverse the neuromuscular blockade. If a visual analogue scale (VAS) score of 4 or higher was observed during recovery, 5 mg of oxycodone was administered intravenously. In cases of vomiting or retching, 4 mg of Ondansetron was administered intravenously.
Outcome Measures and Data Collection
Primary Outcome
The primary outcome was the occurrence of PONV, assessed using a 4-point ordinal symptom scale (0 = none, 1 = nausea, 2 = retching, and 3 = vomiting). In the revised protocol and submitted manuscript, PONV was specified as the primary outcome, replacing the initially registered primary outcome of postoperative analgesic success in the PACU. Nausea was defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit. Retching was defined as labored, spasmodic, rhythmic contraction of the respiratory muscles without expulsion of gastric contents. Vomiting was defined as the forceful expulsion of gastric contents from the mouth.
Secondary Outcomes
Secondary outcomes included postoperative analgesic success rate, mean arterial pressure (MAP) at T1, T2, and T3, the occurrence of other adverse events, use of vasoactive medications during the study-drug period, time to first postoperative PCIA demand, and the total number of PCIA pump presses within 24 and 48 hours after surgery. Postoperative analgesic success was defined as a resting VAS score ≤3 during PACU stay, whereas postoperative analgesic failure was defined as a resting VAS score >3 during PACU stay. Other adverse events included hypotension, nasal congestion, dizziness, respiratory depression, delayed awakening, pruritus, muscle stiffness, convulsions, constipation, urinary retention, and severe agitation during emergence. Respiratory depression was defined as peripheral oxygen saturation (SpO2) <90% in the absence of supplemental oxygen. Delayed awakening was defined as failure to regain consciousness within 30 minutes after discontinuation of anesthetic drugs and absence of response or movement to verbal or mild external stimulation. Severe agitation during emergence was defined as a Richmond Agitation-Sedation Scale (RASS) score ≥ 3 during recovery. Time to first postoperative PCIA demand was recorded in hours; for patients who did not press the PCIA pump, the longest observation time was assigned.
Baseline Characteristics
Baseline characteristics collected included age, BMI, ASA classification, Apfel risk score, history of motion sickness, history of PONV, history of drug allergy, and smoking status.
Randomization and Blinding
Randomization was performed in a 1:1 ratio using a computer-generated block randomization sequence (block size = 4) prepared by an independent statistician who was not involved in recruitment, perioperative management, outcome assessment, or data analysis. A total of 120 sequentially numbered, opaque, sealed envelopes were prepared according to the randomization sequence and stored in a locked cabinet accessible only to a dedicated anesthesia nurse not otherwise involved in the trial. After enrollment by the principal investigator (Sun), the nurse opened the next envelope in sequence and prepared the assigned study medication by diluting the investigational drug with 0.9% sodium chloride solution to a total volume of 10 mL in an identical syringe labeled only with the study identification number. Intraoperative management and recording were performed by Fu. During PACU stay, Gao assessed PONV, VAS scores, and perioperative complications, and determined whether rescue analgesia was required according to the study protocol. Postoperative follow-up during the first 2 days was performed by Liang, who recorded AE, PCIA use, and the management of related complications. Participants, surgeons, anesthesiologists, postoperative assessors, and data analysts remained blinded to treatment allocation throughout the study. The randomization code was not broken until the database lock and completion of the final statistical analysis. In case of emergencies (eg., severe adverse events requiring unblinding), the randomization coordinator could disclose the allocation to the principal investigator, and the reason for unblinding was documented in the case report form.
Sample Size Calculation
The sample size was determined based on the revised primary outcome, PONV. After the primary outcome was revised from postoperative analgesic success in the PACU to PONV, the planned sample size was recalculated and adjusted from 96 to 66 participants. Because TLH-specific PONV data for tegileridine were not available at the time of protocol revision, the assumed event rate for the tegileridine group was set at approximately 13%, informed by the reported incidence of nausea/vomiting-related events in a published Phase 3 trial of tegileridine for postoperative pain following abdominal surgery. The assumed event rate for the oxycodone group was set at 44% based on data from patients undergoing laparoscopic hysterectomy.14,15 In PASS version 15.0, P1 was set at 0.44 and P2 at 0.13. Using a Z test for two independent proportions, with a one-sided α level of 0.05, 90% power, and a 1:1 allocation ratio, the required sample size was determined to be 66 participants.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism version 10. Normally distributed continuous variables are presented as mean ± standard deviation (SD), whereas non-normally distributed continuous or ordinal variables are presented as median with interquartile range (IQR). Categorical variables are presented as number (%). Normality was assessed using the Shapiro–Wilk test. Between-group comparisons were performed using Welch’s t test for normally distributed continuous variables, the Mann–Whitney U-test for non-normally distributed continuous or ordinal variables, and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. For key dichotomous outcomes, risk ratios (RRs) were calculated as the proportion of patients with the event in the tegileridine group divided by the corresponding proportion in the oxycodone group, and 95% confidence intervals (CIs) were estimated using the log-transformation method. A two-sided P value <0.05 was considered statistically significant. The statistical methods used for outcome analysis were not changed after trial registration, and all statistical analyses were performed only after completion of patient enrollment, data collection, and database lock.
Results
The study was reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Supplementary Material 1).16 A total of 72 patients were screened for eligibility, and 68 were finally enrolled and randomized in this trial (Figure 1). Baseline characteristics were comparable between the two groups, with no statistically significant differences in age, body weight, BMI, ASA classification, or Apfel risk score (Table 1).
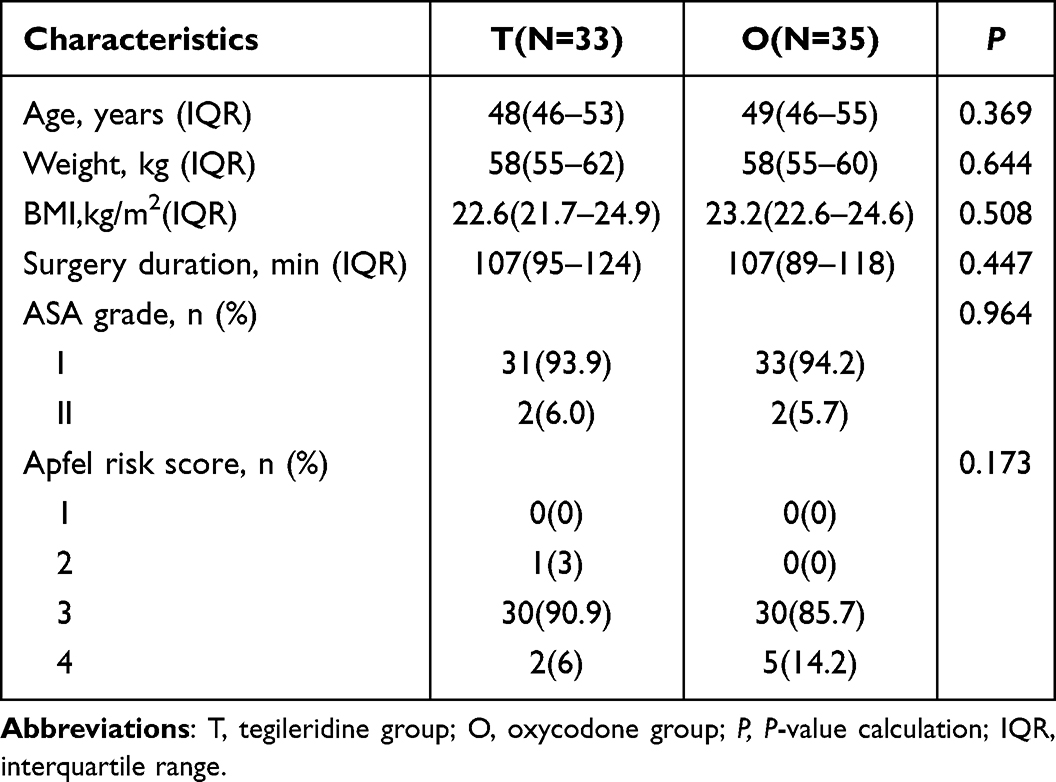 |
Table 1 General Baseline Characteristics of the Subjects |
 |
Figure 1 The flowchart of the participants in the study. |
The incidence of PONV was significantly lower in the tegileridine group than in the oxycodone group (27.3% vs 54.3%; RR, 0.50; 95% CI, 0.27–0.95; P = 0.024) (Figure 2). In addition, the median PONV grade was lower in the tegileridine group than in the oxycodone group [0 (0–1) vs 1 (0–3); P = 0.012] (Figure 3).
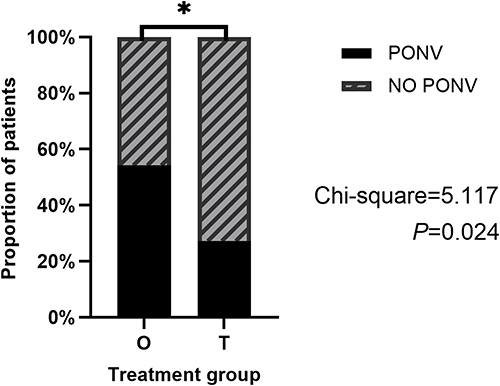 |
Figure 2 Incidence of PONV. Abbreviations: PONV postoperative nausea and vomiting; T, tegileridine group; O, oxycodone group. Note: *p<0.05. |
 |
Figure 3 Distribution of PONV grades in the two groups. Abbreviations: T, tegileridine group; O, oxycodone group; PONV postoperative nausea and vomiting. Notes: PONV was graded as 0 = none, 1 = nausea, 2 = retching, and 3 = vomiting. Nausea was defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit. Retching was defined as labored, spasmodic, rhythmic contraction of the respiratory muscles without expulsion of gastric contents. Vomiting was defined as the forceful expulsion of gastric contents from the mouth. |
Postoperative analgesic success was similar between the tegileridine and oxycodone groups (87.9% vs 94.3%; P = 0.615) (Figure 4).
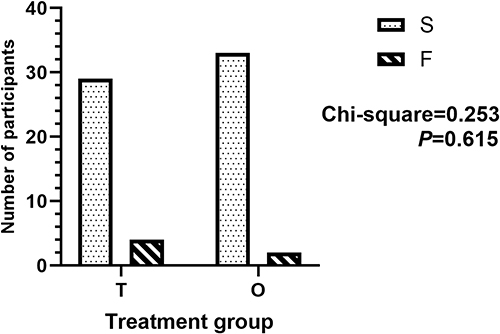 |
Figure 4 Postoperative analgesic success and failure in the two groups. Abbreviations: T, tegileridine group; O, oxycodone group; S, postoperative analgesic success; F, postoperative analgesic failure. |
The overall incidence of adverse events, defined as the proportion of patients experiencing at least one adverse event during the observation period, was lower in the tegileridine group than in the oxycodone group (27.3% vs 60.0%; P = 0.007). The detailed distribution of adverse events is presented in Table 2.
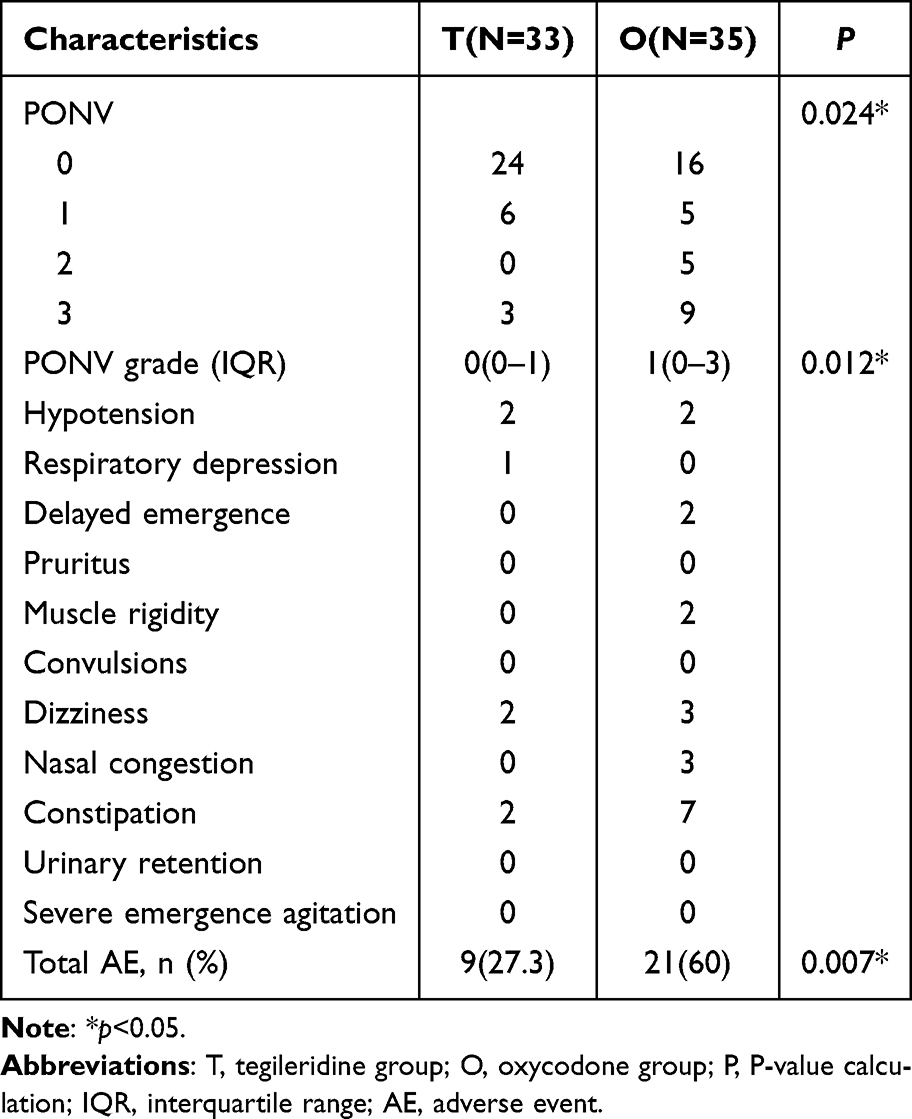 |
Table 2 Number of AE in the Two Groups |
Hemodynamic changes before and after administration of the study drug are summarized in Table 3. No statistically significant differences in MAP were observed between the tegileridine and oxycodone groups at any predefined time point. Use of vasoactive drugs during the study-drug period was also similar between the tegileridine and oxycodone groups (6.0% vs 5.7%; P = 1.000). Total intraoperative remifentanil consumption was comparable between the tegileridine and oxycodone groups [989 (957–1006) vs 986 (948–1004); P = 0.585] (Table 3).
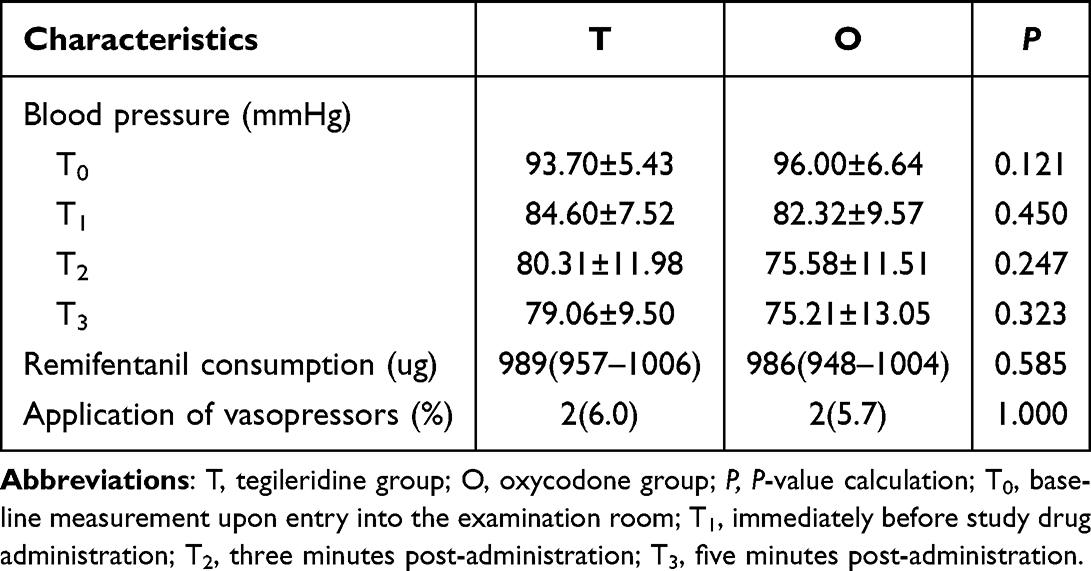 |
Table 3 Other Perioperative Variables in the Two Groups |
Postoperative PCIA-related outcomes are shown in Table 4. Time to first PCIA use was similar between the tegileridine and oxycodone groups [5 (4–6.5) vs 5 (4–6); P = 0.936]. The total number of PCIA pump presses within 24 hours [3 (2–4) vs 3 (2–5); P = 0.291] and within 48 hours [4 (3–6) vs 6 (4–8); P = 0.082] also did not differ significantly between the tegileridine and oxycodone groups.
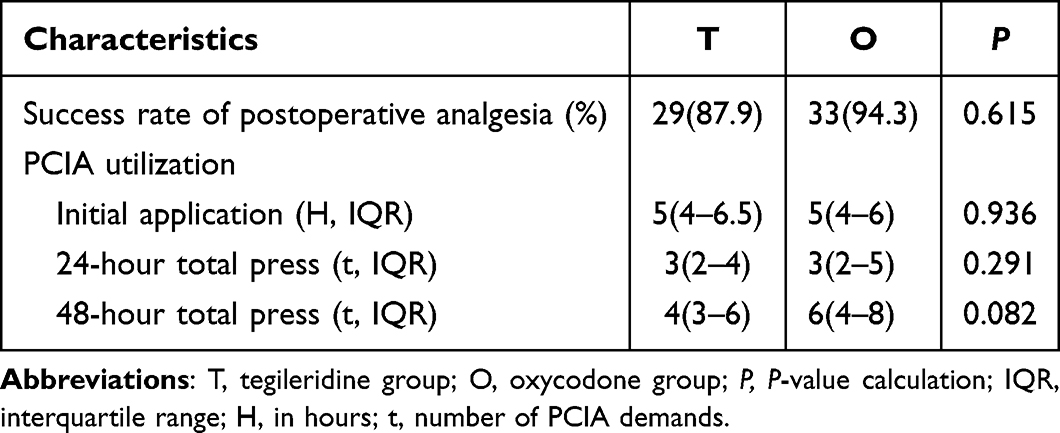 |
Table 4 Comparison of Postoperative Analgesia Between the Two Groups |
Discussion
This randomized, double-blind, controlled trial compared tegileridine and oxycodone at prespecified study doses for postoperative analgesia and PONV after TLH.
PONV remains one of the most important early postoperative outcomes in gynecologic laparoscopy.17 A substantial correlation has been established between the administration of opioids during anesthesia and the occurrence of PONV.18 The evaluation of PONV risk in study participants utilizing the APFEL scoring system demonstrated no notable difference between the two groups in this investigation. Apfel et al previously proposed the hypothesis that the use of volatile anesthetics during surgical procedures is the primary cause of early postoperative nausea and vomiting (ePONV). Total intravenous anesthesia (TIVA) has been postulated to reduce the incidence of PONV by curbing the use of inhaled anesthetics in comparison to combined intravenous-inhalation anesthesia (CIVIA).19
In this study, the incidence rate within the O group (57.6%), achieved through TIVA, was comparable to that observed in Dr. Comelon’s TIVA trial (44%).15 However, when contrasted with the findings reported by Dr. Wu’s group, which documented a PONV incidence rate of approximately 20% in the O group, our group exhibited a higher rate.10 This difference may be attributable to the administration of 8 mg of dexamethasone during surgery in Dr. Wu’s group. The disparity in outcomes between the two groups, as evidenced by the contrasting results observed in Dr. Comelon’s and Dr. Wu’s studies, indicates a divergence in the effects of TIVA and IIA on PONV, which contradicts earlier clinical research results.10,15,18 The discrepancy observed between the groups receiving TIVA and those receiving CIVIA suggests that the influence of these anesthesia techniques on PONV may not be consistent with previous findings. Therefore, the present results should be interpreted within the specific anesthetic and antiemetic context of this trial, in which CIVIA and intraoperative dexamethasone may be considered protective factors against PONV.
A plausible reason for the lower incidence of PONV in the tegileridine group is its unique pharmacologic profile compared to traditional MOR agonists. Opioid-induced recruitment of β-arrestin-2 has been associated with several adverse effects, including nausea, vomiting, constipation, and respiratory depression.20 In contrast, β-arrestin-2 knockout models have shown enhanced and prolonged morphine analgesia with attenuation of some opioid-related adverse effects.21 Against this background, the development of biased ligands at G protein-coupled receptors has attracted considerable attention over the past decade.22 Tegileridine has been reported to show limited β-arrestin-2 recruitment, which may partly account for the lower rate of PONV observed in the present study. Nevertheless, this mechanistic interpretation should remain cautious, because the present trial was designed to evaluate clinical outcomes rather than directly test signaling pathways.
The analgesic findings of the present trial should also be interpreted within the context of the multimodal analgesic strategy employed. Previous dose-finding work has shown that 0.06 mg·kg−1 intravenous oxycodone can provide satisfactory postoperative analgesia after laparoscopic hysterectomy.10 A similar outcome was observed in this trial. The single intravenous opioid drug dose utilized in this trial was minimal. However, as demonstrated in the trial conducted by Dr. Wang, pain resulting from surgical incision is principally alleviated through local anesthetic wound infiltration. Ropivacaine was administered following TAP, covering the site of laparoscopic perforation, and maintained a sensory blockade effect of 87% over a duration of six hours.23 The analgesic duration provided by a nerve block is comparable to that of opioid medications. It is confirmed that a combined TAP nerve block reduces opioid consumption and enhances the potential benefits for the trial participant.15 Therefore, the present study should not be interpreted as evaluating single-agent analgesia in isolation, but rather as comparing two systemic opioid strategies on top of an established multimodal analgesic background.
The similar early postoperative analgesic success observed between groups suggests that both study regimens were able to maintain adequate analgesia during PACU stay. This study employed remifentanil as the agent for anesthesia induction, thereby ensuring that the opioids present in the patient during their stay in the PACU were exclusively the administered intervention drugs. This methodological approach facilitated a more precise distinction of the effects attributable to each intervention. The preliminary trial results demonstrate no statistically significant difference in postoperative analgesia success rates between the two groups, indicating that the analgesic effects at prespecified study doses were consistent with expectations. The occurrence of postoperative analgesic failure was attributed to inadequate analgesic medication. At the study dose used in this trial, oxycodone did not ensure maintenance of a resting VAS score ≤3 in all patients during PACU stay. This discrepancy can be attributed to the fact that the trial designed by Professor Wu employed an UP-DOWN Dose-Finding protocol, whereas the current trial utilizes the median dose provided by him.10 The research team contemplated the potential for postoperative hyperalgesia resulting from the utilization of high-dose short-acting opioids for the induction and maintenance of anesthesia. Subsequent postoperative follow-up results demonstrated an absence of this phenomenon. This discrepancy may partly reflect the observed variation in the recommended dosage of remifentanil for the induction of hyperalgesia, which has been reported as 0.4 μg·kg−1·min−1, a level significantly exceeding that used in this study.24,25
The postoperative analgesic trajectory beyond PACU was further supported by the PCIA-related findings. Our team set the PCIA pump parameters based on experimental reports from the southeastern region of China.26 Preliminary trials in Tegileridine demonstrated that the duration of analgesia was comparable to that observed in the main trial (5,4 to 6.5 hours). Additionally, no statistically significant differences were observed between Tegileridine group and the Oxycodone group with respect to the timing of the initial PCIA dose or the total postoperative PCIA dosage. This finding indicates that prespecified study doses of the two interventions provide consistent analgesic benefits to patients during the first two days postoperatively.
The overall incidence of adverse events differed significantly between the two groups. However, this difference was driven predominantly by PONV. Therefore, the clinical interpretation of several isolated postoperative events should remain cautious. A comparative analysis of blood pressure variations prior to and following the administration of intervention drugs between the two groups indicates the presence of potential statistical differences; however, the clinical significance of these differences is negligible. Consequently, an additional comparison concerning the utilization of vasoactive agents was conducted, which revealed no statistically significant differences in their use between the two groups.
Constipation is related to gastric emptying and intestinal peristalsis; activation of MOR receptors by opioid drugs leads to disruption of the intestinal barrier, increased intestinal permeability, reduced water and electrolyte secretion in the intestinal lumen, which in turn causes constipation.27 However, there is no clear evidence of a relationship between β-arrestin recruitment and constipation.
Delayed awakening was observed in a small number of patients in this trial. Although high intraoperative opioid exposure has been reported to increase the risk of delayed awakening, the remifentanil dose used in the present study was approximately 0.16 μg·kg−1·min−1, which was lower than the dose commonly discussed in relation to opioid-induced postoperative hyperalgesia.28 In addition, total intraoperative remifentanil consumption was comparable between the two groups. Therefore, the delayed awakening events observed in this trial are unlikely to be explained by between-group differences in remifentanil exposure alone.
Two patients developed transient postoperative muscle rigidity after recovery of consciousness in the PACU, which was considered more likely attributable to postoperative shivering. Respiratory depression constitutes one of the most grave complications associated with anesthesia and it is a primary cause of mortality in patients receiving opioid medications. Research has shown that opioid-induced respiratory depression results from MOR activation; β-arrestin-2 recruitment may not be involved in respiratory depression.29–32 Agents with slower MOR binding, such as morphine, may be safer than those with faster binding, like alfentanil and remifentanil, despite having similar pain-relief effects.29 It has also been demonstrated that rapid increases in opioid receptor occupancy following intravenous bolus can trigger apnea. Conversely, slower receptor binding is less prone to respiratory depression. As demonstrated in the extant research, Tegileridine exhibits a significantly higher affinity for MOR than oxycodone.8,14 However, receptor affinity alone may not fully explain respiratory safety in clinical practice, and other factors, including binding kinetics, administration profile, and perioperative context, may also contribute.
This study has several limitations. It was a single-center trial with a small sample size and a 48-hour follow-up period, which may limit generalizability and preclude assessment of longer-term outcomes. In addition, only patients undergoing TLH were included, and the single-dose study-drug design was applied within a multimodal analgesic framework including TAPB and postoperative PCIA. Therefore, the findings should be interpreted cautiously, and larger multicenter studies are needed to further clarify the role of tegileridine in postoperative analgesic strategies.
Conclusion
In patients undergoing TLH, tegileridine was associated with a similar postoperative analgesic success rate and a lower risk of PONV compared with oxycodone.
Trial Registration
This trial was retrospectively registered at ClinicalTrials.gov after patient enrollment had begun because of an administrative coordination delay in submitting the prepared registration information to the registry. The trial was first submitted on December 24, 2025, and first posted on January 8, 2026 (NCT07326683). The registration was completed before database lock and final statistical analysis.
Data Sharing Statement
Deidentified data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Hainan Medical University (Approval number: 2025-KY82), and all subjects provided written informed consent.
Funding
This research was supported by the Hainan Provincial Natural Science Foundation of China (No.823RC592).
Disclosure
The authors declare no conflicts of interest.
References
1. Glare P, Aubrey K, Myles P. Transition from acute to chronic pain after surgery. Lancet. 2019;393:1537–12. doi:10.1016/S0140-6736(19)30352-6
2. Yi K, Sun W, Yu W, Chen S. Overview and prospects of the clinical application of oliceridine. drug design, development and therapy. Drug Design Develop Ther. 2025;19:5415–5430. doi:10.2147/dddt.S525471
3. Wright MA, Kinlaw AC, McClurg AB, et al. Appropriateness of hysterectomy as treatment for benign gynecological conditions. J Women’s Health. 2024;33(10):1358–1366. doi:10.1089/jwh.2024.0142
4. Luo D, Huang Z, Tang S, et al. Risk analysis of postoperative nausea and vomiting in patients after gynecologic laparoscopic surgery. BMC Anesthesiol. 2024;24(1):345. doi:10.1186/s12871-024-02727-y
5. Lirk P, Thiry J, Bonnet MP, Joshi GP, Bonnet F. Pain management after laparoscopic hysterectomy: systematic review of literature and PROSPECT recommendations. Reg Anesth Pain Med. 2019;44(4):425–436. doi:10.1136/rapm-2018-100024
6. Zhao K, Gao Y, Zhang J, et al. Penehyclidine for prevention of postoperative nausea and vomiting in patients undergoing gynecological laparoscopic surgery under combined intravenous and inhalation anesthesia: a randomized, double-blind, placebo-controlled trial. Drug Des Devel Ther. 2024;18:685–697. doi:10.2147/dddt.S453327
7. Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose ratios for opioids. a critical review and proposals for long-term dosing. J Pain Sympt Manage. 2001;22(2):672–687. doi:10.1016/s0885-3924(01)00294-9
8. Kalso E. Oxycodone. J Pain Sympt Manage. 2005;29(5 Suppl):47–56. doi:10.1016/j.jpainsymman.2005.01.010
9. Barrett JE, Inan ASS. Oxycodone: a current perspective on its pharmacology, abuse, and pharmacotherapeutic developments. Pharmacol Rev. 2023;75(6):1062–1118. doi:10.1124/pharmrev.121.000506
10. Yu W, Wu X, Liu L, et al. The median effective dose of one intravenous bolus of oxycodone for postoperative analgesia after myomectomy and hysterectomy with local ropivacaine wound infiltration: an up–down dose-finding study. Anesthesia Analg. 2020;131(5):1599–1606. doi:10.1213/ANE.0000000000005011
11. Ferreira DH, Louw S, McCloud P, et al. Controlled-Release oxycodone vs. placebo in the treatment of chronic breathlessness-a multisite randomized placebo controlled trial. J Pain Symptom Manage. 2020;59(3):581–589. doi:10.1016/j.jpainsymman.2019.10.017
12. Yang GW, Cheng H, Song XY, et al. Effect of oxycodone-based multimodal analgesia on visceral pain after major laparoscopic gastrointestinal surgery: a randomised, double-blind, controlled trial. Drug Des Devel Ther. 2024;18:1799–1810. doi:10.2147/dddt.S464518
13. Shi R, Chai Y, Feng H, et al. Study of the mass balance, biotransformation and safety of [14C]SHR8554, a novel μ-opioid receptor injection, in healthy Chinese subjects. Front Pharmacol. 2023;14(000):14. doi:10.3389/fphar.2023.1231102
14. Wang T, Wang Y, Xie H, et al. Tegileridine for moderate-to-severe acute pain following abdominal surgery: a randomized, double-blind, phase 3 clinical trial. Cell Rep Med. 2025;6(12):102477. doi:10.1016/j.xcrm.2025.102477
15. Comelon M, Raeder J, Drægni T, Lieng M, Lenz H. Tapentadol versus oxycodone analgesia and side effects after laparoscopic hysterectomy A randomised controlled trial. Eur J Anaesthesiol. 2021;38(9):995–1002. doi:10.1097/eja.0000000000001425
16. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. BMJ. 2025;389:e081123. doi:10.1136/bmj-2024-081123
17. Liu ZY, Yang XY, Lv C, et al. Effect of high maintenance dose versus low dose of remifentanil on incidence of Postoperative Nausea and Vomiting (PONV) in patients under gynecological laparoscopic procedure: a pilot study. Drug Des Devel Ther. 2025;19:4885–4894. doi:10.2147/dddt.S518291
18. Gan TJ, Belani KG, Bergese S, Chung F, Philip BK. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesthesia Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
19. Apfel CC. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth. 2002;88. doi:10.1093/bja/88.5.659
20. Gillis A, Gondin AB, Kliewer A, et al. Low intrinsic efficacy for G protein activation can explain the improved side effect profiles of new opioid agonists. Sci Signaling. 2020;13(625):eaaz3140. doi:10.1126/scisignal.aaz3140
21. Raehal KM, Walker JKL, Bohn LM. Morphine side effects in beta-arrestin 2 knockout mice. J Pharmacol Exp Ther. 2005;314(3):1195–1201. doi:10.1124/jpet.105.087254
22. Violin JD, Crombie AL, Soergel DG, Lark MW. Biased ligands at G-protein-coupled receptors: promise and progress. Trends Pharmacol Sci. 2014;35(7):308–316. doi:10.1016/j.tips.2014.04.007
23. Chen Y, Shi KJ, Xia Y, et al. Sensory assessment and regression rate of bilateral oblique subcostal transversus abdominis plane block in volunteers. Reg Anesth Pain Med. 2018;43(2):174–179. doi:10.1097/aap.0000000000000715
24. Hansen EG, Duedahl TH, Rmsing J, Hilsted KL, Dahl JB. Intra-operative remifentanil might influence pain levels in the immediate post-operative period after major abdominal surgery. Acta anaesthesiologica Scandinavica. 2005;49(10):1464–1470. doi:10.1111/j.1399-6576.2005.00861.x
25. Maurtua MA, Deogaonkar A, Bakri MH, et al. Dosing of remifentanil to prevent movement during craniotomy in the absence of neuromuscular blockade. J Neurosurg Anesthesiol. 2008;20(4):221. doi:10.1097/ANA.0b013e3181806c4a
26. Qingqing Y, Xianwen H, Yun L, et al. Effect of different dose of nalbuphine combined with sufentanil for patient-controlled intravenous analgesia after laparoscopic hysterectomy(in Chinese). J Clin Anesthesiol. 2020;36(02):140–143. doi:10.12089/jca.2020.02.008
27. Lacy BE, Cangemi DJ. Opioids and the gastrointestinal tract: the role of peripherally active μ-opioid receptor antagonists in modulating intestinal permeability. Am J Gastroenterol. 2024;119(10):1970–1978. doi:10.14309/ajg.0000000000002887
28. Wang BY, Peng GF, Chen L, et al. Effect of transcutaneous electrical acupoint stimulation on remifentanil dosage during craniotomy aneurysm clipping: a prospective, randomized controlled study. BMC Complement Med Therap. 2023;23(1):453. doi:10.1186/s12906-023-04297-x
29. Pattinson KTS. Opioids and the control of respiration. Br J Anaesth. 2008;100(6):747–758. doi:10.1093/bja/aen094
30. Bateman JT, Saunders SE, Levitt ES. Understanding and countering opioid-induced respiratory depression. British J Pharmacol. 2023;180(7):813–828. doi:10.1111/bph.15580
31. Kliewer A, Schmiedel F, Sianati S, et al. Phosphorylation-deficient G-protein-biased μ-opioid receptors improve analgesia and diminish tolerance but worsen opioid side effects. Nat Commun. 2019;10367. doi:10.1038/s41467-018-08162-1
32. Kliewer A, Gillis A, Hill R, et al. Morphine-induced respiratory depression is independent of β-arrestin2 signalling. Br J Pharmacol. 2020;177(13):2923–2931. doi:10.1111/bph.15004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.