Back to Journals » Research and Reports in Urology » Volume 12
Technology Meets Tradition: CO2 Laser Circumcision versus Conventional Surgical Technique
Authors Ronchi P, Manno S, Dell'Atti L ![]()
Received 7 May 2020
Accepted for publication 24 June 2020
Published 16 July 2020 Volume 2020:12 Pages 255—260
DOI https://doi.org/10.2147/RRU.S260636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Piero Ronchi,1 Stefano Manno,2 Lucio Dell’Atti1
1Department of Urology, University Hospital “Ospedali Riuniti”, Ancona, Italy; 2Urology Unit, Hospital “Pugliese Ciaccio”, Catanzaro, Italy
Correspondence: Lucio Dell’Atti
Department of Urology, University Hospital “Ospedali Riuniti”, 71 Conca Street, Ancona 60126, Italy
Tel +39 071 5966523
Fax +39 071 5963367
Email [email protected]
Purpose: We wished to present the clinical applications and to evaluate the benefits of the use of a carbon dioxide (CO2) laser versus the conventional procedure for circumcision in adults, in terms of duration of surgery, surgical techniques, complications, pain and cosmetic appearance.
Patients and Methods: The medical records of 482 patients who had been circumcised were retrospectively evaluated. The patients were divided into two groups: 168 patients (Group A) were circumcised with traditional techniques; and 314 patients (Group B) were circumcised using a CO2 laser. All the patients were circumcised under local anesthesia. Pain was evaluated using a verbal numerical rating scale for pain assessment. Postoperative wound swelling, bleeding, infection and pain were assessed at 4 hours, 24 hours and 7 days after surgery.
Results: There were no significant differences between the two groups in terms of bleeding and infections. The difference in operating times between the groups was significant (p< 0.001). Wound disruptions occurred in one patient in Group A at 3 days and two patients in Group B at 1 week. Pain scores were low and there was less pain in Group B than in Group A during the first 4 hours (1.8 vs 3.7; p< 0.002). Compared with the conventional method, the CO2 laser technique was associated with much less pain at both 1 day (p< 0.002) and 7 days (p< 0.001) postoperatively. The cosmetic results were superior in Group B; a linear surgical scar developed in 94.9% of patients in Group B versus 61.3% in Group A (p< 0.001).
Conclusion: Our results show that the use of a CO2 laser was associated with a shorter operative time, less wound irritation and better cosmetic appearance compared with standard surgical techniques for circumcision.
Keywords: CO2 laser, circumcision, surgical technique, outcomes
Introduction
Circumcision is the oldest and the most common surgical procedure in urology.1 It comprises the removal of the skin covering the glans, and is performed for various reasons, such as medical, religious and traditional.2 The most common medical indications for circumcision are phimosis, paraphimosis, recurrent balanitis and posthitis.1,2 Many studies have observed that circumcision increases penile hygiene, and decreases the risks of penile cancer and urinary tract infections.3 Surgically, circumcision is an easy technique to learn and perform. Various surgical techniques can be used to perform this procedure, with different results and complications.2,3 The laser has been validated as being effective in the treatment of common skin diseases and aesthetic dermatology.4 Although there are various types of laser, in this article we will describe the fundamentals and clinical applications of the carbon dioxide (CO2) laser, to evaluate the benefits of its use versus the conventional procedure for circumcision in adults, in terms of duration of the operation, complications, pain and cosmetic appearance.
Patients and Methods
The medical records of 482 patients who had been circumcised were retrospectively evaluated between December 2016 and December 2019. Patients who were circumcised while undergoing another surgical procedure in the same session were not included in the study. The patients were divided into two groups. In the first group (Group A), 168 patients were circumcised with the conventional dorsal slit-sleeve method by two experienced urologists (SM and LD). In the second group (Group B), 314 patients were circumcised by an experienced surgeon (PR) using a multipulse continuous CO2 laser (MX7000®; DSE Group, Seoul, Republic of Korea) at a continuous wave power setting of 5 W. Physical examinations were performed on all patients 1 day before the operation. All of the patients were circumcised under local anesthesia. For local anesthesia, lidocaine and bupivacaine were administered together, at doses appropriate for the patient’s age, as a dorsal penile nerve block. Bleeding was controlled with a suture or bipolar cautery in Group A, and in Group B using the CO2 laser in a defocused mode (Figure 1). After the entire foreskin had been removed, the cut edges of the skin and the preputial tissue were approximated with interrupted 4/0 absorbable sutures in both groups.
 |
Figure 1 Illustration of the surgical procedure of circumcision using a CO2 laser. (A) Phimosis. (B) The laser beam is used in focused mode to delimit the circumferential mark incision over the penile skin just proximal to the corona. The preputial skin is resected leaving a 0.5 cm sleeve proximal to the corona. (C) Using the laser beam, incisions are made along the marked lines, taking care to cut through the skin to the subcutaneous tissue but no deeper. (D) Between the two top artery forceps (at 11 o’clock and 1 o’clock), the dissecting laser beam is used to make a cut along the middle of the crushed foreskin up to the previously marked incision line. |
Pain was evaluated using a verbal numerical rating scale for pain assessment.5 Patient’s age, indications for surgery and operative time were recorded. Postoperative wound swelling, bleeding, infection (wound with pus and separation) and pain were assessed at 4 hours, 24 hours and 7 days after surgery. After the circumcision, the wounds were dressed, with application of an antibiotic lotion three times a day, and the use of tablet therapy with ibuprofen 8mg/kg two to three times a day to be taken “only as needed”. Wound dressings were removed 24 hours after the circumcision, either by the family members at home or by the physicians at the hospital. Antibiotic prophylaxis was dispensed routinely 60 minutes prior to incision (amoxicillin–clavulanate 875–125 mg). No postoperative antibiotics were prescribed in any of the patients.
Statistical Analysis
The data were analyzed in a common database. Qualitative variables were described using absolute frequencies and percentages. Quantitative variables were described using the mean, standard deviation, median and quartiles. All statistical analyses were conducted using SPSS version 23 (IBM Corp., Armonk, NY).
Results
Baseline characteristics of the patients are shown in Table 1. There were no significant differences between the two groups. Operative outcomes and adverse events are shown in Table 2. There were no intraoperative complications. There was no significant difference between the two groups in terms of bleeding and infections. Comparison of the patients in the two groups demonstrated a significant decrease in terms of operative time in the laser-treated group (12.8±0.9 vs 23.1±2.8 minutes; p<0.001). Wound disruptions occurred in one patient in Group A at 3 days and two patients in Group B at 1 week. Wound disruptions were not more than 5 mm in width, and none required surgical closure. Pain scores were low and there was less pain in Group B than in Group A during the first 4 hours (1.8 vs 3.7 on a 10-point scale; p<0.002). The CO2 laser technique was associated with much less pain at both 1 day (p<0.002) and 7 days (p<0.001) postoperatively. Postoperative pain scores are shown in Table 3. The cosmetic results were superior in Group B; a linear surgical scar developed in 94.9% of patients in Group B versus 61.3% in Group A (p<0.001) (Figure 2). There were no differences in healing time at 4 weeks. Three patients in Group A required a secondary operation because of fibrosis and scar tissue.
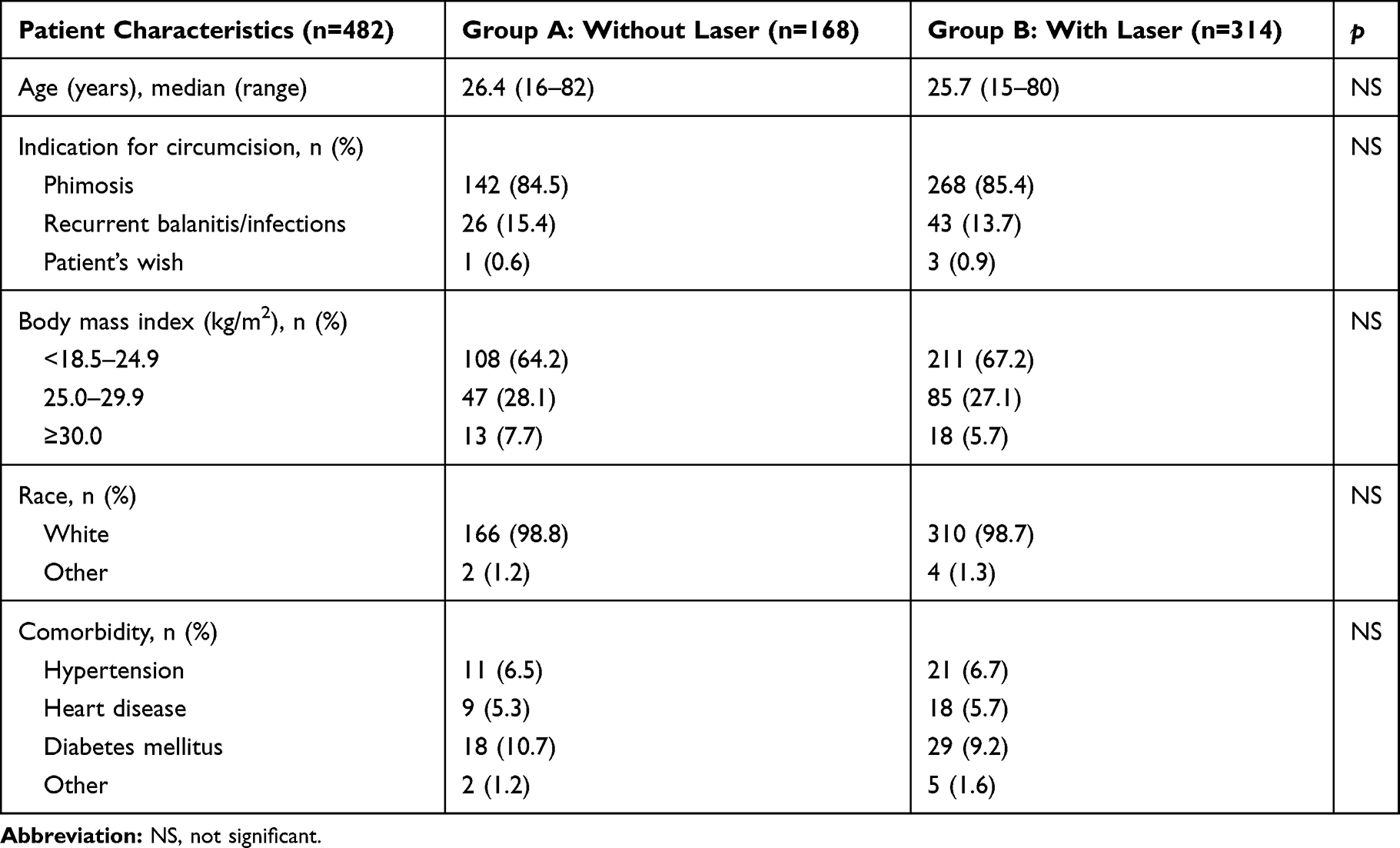 |
Table 1 Distribution of Preoperative Clinical Characteristics in Patients Undergoing Circumcision |
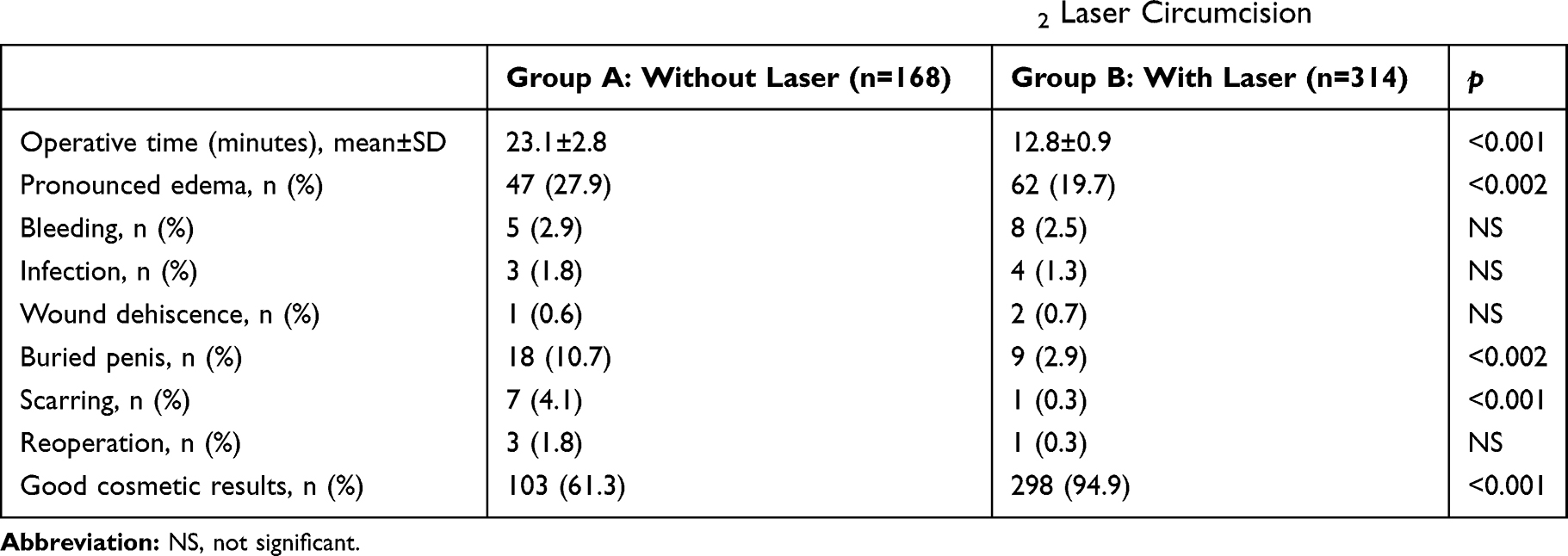 |
Table 2 Comparison of Outcomes for Conventional Circumcision versus CO2 Laser Circumcision |
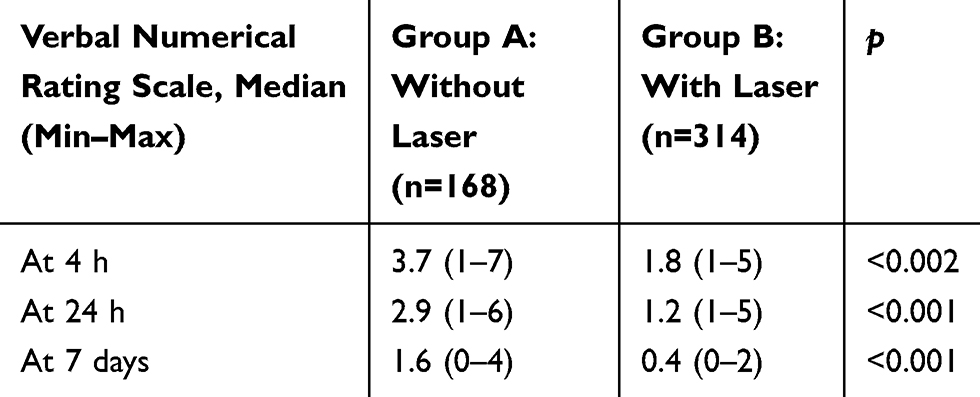 |
Table 3 Details of Pain Scores in the Two Groups of Patients |
 |
Figure 2 (A) Postoperative wound after CO2 laser circumcision. (B) Postoperative wound at 1 month after CO2 laser circumcision. |
Discussion
The benefits of circumcision include a reduced risk of urinary tract infections and sexually transmitted diseases; protection against penile cancer, and cervical cancer in female sexual partners; and prevention of balanitis, posthitis, phimosis and paraphimosis.6 Numerous studies since the 1980s have noted a lower risk of HIV infection in circumcised men, as well as lower HIV prevalence in populations where male circumcision is common.7 Complication rates following male circumcision are very low when it is performed by trained health-care providers. The complication rate due to this type of surgery was reported as nearly 5%.8 The rate of complications depends upon multiple factors, including anatomical abnormalities, medical comorbidities, surgical technique, sterility of the conditions and the patient’s age, and increases when the surgery is performed by inexperienced people.9 The most common complication is bleeding, with an incidence that varies from 0.1% to 3.1%.8,9 Bleeding from larger blood vessels can be controlled easily by ligature or electrocoagulation, although excessive electrocoagulation carries the risk of electrical burns and necrosis.10
The CO2 laser was one of the earliest types of laser systems to be found.11 It was first created in 1964 by Patel and collaborators.12 It was quickly recognized as an ideal surgical laser because of its high-water absorption. Its thermocoagulation cauterizes small blood vessels with the surrounding tissue, achieving hemostasis and therefore a dry field. In the hands of an appropriately trained practitioner, the CO2 laser offers a large range of dermatological indications, with great precision for techniques involving incision, excision, vaporization and coagulation.11,13 However, few authors have used a CO2 laser instead of a lancet. Gorgulu et al14 showed that the use of a CO2 laser shortened the operating time and reduced complications related to bleeding, in comparison with the conventional guillotine method, in a series of 150 patients. Xu et al10 observed similar outcomes. They investigated the safety and efficacy of a modified CO2 laser technique for circumcision in adult males compared with the conventional dorsal slit-sleeve method. Data were analyzed from a prospective randomized controlled clinical study comparing two different operative techniques. Compared with the conventional group, there were shorter operative times, less blood loss and lower postoperative complication rates in the laser group.
How et al15 compared the costs associated with the operating time between CO2 lasers and the conventional technique. They found that the median operating time was 20 (range 16–21) minutes using the conventional technique and 15 (range 13–17) minutes using a CO2 laser. In our study, the comparison of the patients in the two groups demonstrated a 10-minute decrease in the operative time in the laser-treated group.
Another advantage of CO2 laser surgery is the large decrease in postoperative pain, which increases the comfort of the patients.16 Our study showed that patients treated with the CO2 laser had significantly less postoperative pain than did those who had conventional surgery, at 4 hours, 1 day and 7 days postoperatively.
Although previous studies valued sutureless circumcision techniques, we believe that this type of technique should not be used because of the increased risk of wound breakdown following an occasional penile erection.17–19 In this study, although the tissues around the wound edges were exposed to the thermal effects of the CO2 laser, there were two cases of wound separation at 1 week in Group B, but the patients had practiced sexual masturbation at 6 days postoperatively, despite our instruction to avoid sexual intercourse for 6 weeks. However, in our study more cases of pronounced edema were observed among patients treated by the conventional technique (27.9%) than among the laser group (19.7%). This observation is probably due to the excessive thermal damage to the preputial tissues caused by the electrocautery used for hemostasis in the conventional group. Thermal transmission to surrounding tissue by the CO2 laser is minimal, whereas the mean depth of damage produced by electrosurgery is much greater than that created by a CO2 laser.13
The cosmetic appearance and wound edge regularity, as assessed by both the medical personnel and each patient, were better in Group B (94.9%) than in Group A (61.3%). The residual thermal damage deposited by the CO2 laser beam helps to ensure a dry field and swiftly induces the wound healing and remodeling process. More extensive and irregular necrosis is found after electrocautery, resulting in a more severe inflammatory reaction than with the CO2 laser.11 The necrosis may result in an irregular wound edge and a poor cosmetic outcome.
The retrospective nature of our study may have resulted in unrecognized biases. This study was conducted by a single experienced surgeon at only one institution. A selection bias existed because the surgical approach was selected by the surgeon based on patient characteristics and according to his experience. The relatively small sample size is a significant limitation, as well as the lack of long-term outcomes, and our data must be validated with future multicenter studies.
Conclusion
Our results demonstrate that the use of a CO2 laser was associated with a shorter operative time, less wound irritation and better cosmetic appearance compared with standard surgical techniques for circumcision. Moreover, the CO2 laser technique was not associated with significant postoperative pain. Surgically, circumcision is an easy technique to learn and perform. A surgical laser ideal for cutting soft tissue must be able to vaporize the tissues and cauterize the surgical margins at the same time, and the CO2 laser can achieve both of these criteria. Not all laser wavelengths are suitable to comply with both requirements. To solve this laser controllability problem, virtual scalpel systems have been developed. Such systems assess the fundamental processes involved in laser–tissue interaction, analyzing graphically and mathematically how deeply a laser beam cuts, and how far coagulation and hemostasis extend into the surgical margins, further demonstrating the importance of laser selection for a given procedure. The system allows surgery to be safely and precisely performed using a graphics pen directly over a live video from the surgical site. This has been shown to eliminate the hand–eye coordination problems that affect other microsurgery systems and to make full use of the operator’s manual dexterity without the need for extra training.20
The main obstacles to performing circumcision using a CO2 laser are the high cost of the CO2 laser machine and the surgical skills required to use the laser. This surgical approach may be used for a variety of cases in an andrology outpatient surgery setting, and may be helpful in reducing surgical waiting lists and preventing postoperative morbidity. We plan to use the present results to counsel future patients who intend to undergo circumcision surgery.
Ethical Approval
Ethical approval was given by Hospital “Pugliese Ciaccio” – Catanzaro (Italy) ethics committee for reporting this case series.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent
We have obtained written informed consent from these patients for all of the anonymized information to be published.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dunsmuir WD, Gordon EM. The history of circumcision. BJU Int. 1999;83:1–12.
2. Gargollo PC, Kozakewich HP, Bauer SB, et al. Balanitis xerotica obliterans in boys. J Urol. 2005;174:1409–1412. doi:10.1097/01.ju.0000173126.63094.b3
3. Hirji H, Charlton R, Sarmah S. Male circumcision: a review of the evidence. JMHG. 2005;2:21–30.
4. Ohshiro T. The laser apple: a new graphic representation of medical laser applications. Laser Ther. 1995;8:185–190. doi:10.5978/islsm.8.185
5. Jensen MP, Castarlenas E, Roy R, et al. The utility and construct validity of four measures of pain intensity: results from a University-Based Study in Spain. Pain Med. 2019;20:2411–2420. doi:10.1093/pm/pny319
6. Tobian AA, Gray RH. The medical benefits of male circumcision. JAMA. 2011;306:1479–1480. doi:10.1001/jama.2011.1431
7. Kim HH, Goldstein M. High complication rates challenge the implementation of male circumcision for HIV prevention in Africa. Nat Clin Pract Urol. 2009;6:64–65. doi:10.1038/ncpuro1279
8. Dell’Atti L, Polito M, Galosi AB. Is degloving the best method to approach the penile corporoplasty with Yachia’s technique? Urology. 2019;126:204–208. doi:10.1016/j.urology.2018.12.040
9. Weiss HA, Larke N, Halperin D, Schenker I. Complications of circumcision in male neonates, infants and children: a systematic review. BMC Urol. 2010;10:2. doi:10.1186/1471-2490-10-2
10. Xu Y, Li F, Li Z, et al. A prospective, randomized controlled trial of circumcision in adult males using the CO2 laser: modified technique compared with the conventional dorsal-slit technique. Photomed Laser Surg. 2013;31(9):422–427. doi:10.1089/pho.2013.3550
11. Kaplan I. The CO2 surgical laser. Photomed Laser Surg. 2010;28:847–848. doi:10.1089/pho.2010.9926
12. Omi T, Numano K. The role of the CO2 laser and fractional CO2 laser in dermatology. Laser Ther. 2014;23:49–60. doi:10.5978/islsm.14-RE-01
13. Kaplan I. The CO2 laser as a versatile surgical modality. Laser Ther. 2007;16:25–38. doi:10.5978/islsm.16.25
14. Gorgulu T, Olgun A, Torun M, et al. A fast, easy circumcision procedure combining a CO2 laser and cyanoacrylate adhesive: a non-randomized comparative trial. Int Braz J Urol. 2016;42:113–117. doi:10.1590/S1677-5538.IBJU.2015.0284
15. How AC, Ong CC, Jacobsen A, et al. Carbon dioxide laser circumcisions for children. Pediatr Surg Int. 2003;19:11–13. doi:10.1007/s00383-002-0894-0
16. Tuncer I, Ozcakir–Tomruk C, Sencift K, et al. Comparison of conventional surgery and CO2 laser on intraoral soft tissue pathologies and evaluation of the collateral thermal damage. Photomed Laser Surg. 2010;28:75–79. doi:10.1089/pho.2008.2353
17. Kelly BD, Lundon DJ, Timlin ME, et al. Paediatric sutureless circumcision – an alternative to the standard technique. Pediatr Surg Int. 2012;28:305–308. doi:10.1007/s00383-011-3015-0
18. Lane V, Vajda P, Subramaniam R. Paediatric sutureless circumcision: a systematic literature review. Pediatr Surg Int. 2010;26:141–144. doi:10.1007/s00383-009-2475-y
19. D’Arcy FT, Jaffry SQ. A review of 100 consecutive sutureless child and adult circumcisions. Ir J Med Sci. 2011;180:51–53. doi:10.1007/s11845-010-0545-8
20. Mattos LS, Deshpande M, Barresi G, et al. A novel computerized surgeon-machine interface for robot-assisted laser phonomicrosurgery. Laryngoscope. 2014;128:1887–1894. doi:10.1002/lary.24566
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.