Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Teamwork, Professional Identities, Conflict, and Industrial Action in Nigerian Healthcare
Received 18 June 2020
Accepted for publication 16 September 2020
Published 22 October 2020 Volume 2020:13 Pages 1223—1234
DOI https://doi.org/10.2147/JMDH.S267116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suleiman Mayaki,1 Martyn Stewart2
1Department of Pediatrics, Ahmadu Bello University Teaching Hospital, Shika-Zaria P.M.B 06, Nigeria; 2Department of Education and Training, Liverpool School of Tropical Medicine, Liverpool L3 5QA, UK
Correspondence: Suleiman Mayaki
Department of Pediatrics, Ahmadu Bello University Teaching Hospital, Shika-Zaria P.M.B 06, Nigeria
Tel +2348054919184
Email [email protected]
Purpose: Modern healthcare is delivered by teams of multidisciplinary professionals. Conflicts have been widely reported between these professionals in Nigeria. Furthermore, the health system is frequently crippled by industrial actions by trade unions representing these professionals. This study aimed to shed light on the complexities of factors perceived to cause workplace conflicts, including the extent to which these are thought to link to industrial action.
Materials and methods: Focus group discussions and in-depth interviews were conducted with nurses, doctors, and medical laboratory scientists who work in multiprofessional settings giving a total of 41 participants. Results were analyzed within the framework of the social identity theory.
Results and conclusions: The dominant themes that emerged as barriers to teamwork include professional hierarchy, role ambiguity, and poor communication. At the same time, the health sector leadership and remuneration were the main themes concerning industrial actions. The salience of professional identities was also demonstrated, providing a link between interprofessional conflict in the workplace and competitive industrial actions by trade unions representing health professionals. The implications for educational and clinical practice and the need for interprofessional education are discussed.
Keywords: interprofessional conflict, industrial action, professional identity, teamwork
Plain Language Summary
Collaboration between health professionals of different disciplines is necessary but complicated. On the one hand, teamwork can benefit patients, health systems, and the health workers themselves. On the other hand, it can lead to conflict between health workers and affect health services. This research aimed to investigate the causes of conflict between health workers in the workplace and the extent to which those conflicts are related to health worker strikes in Nigeria. Group discussions and one-on-one interviews were conducted with nurses, doctors, and medical laboratory scientists. The results were analyzed along each of these professional groups. The causes of workplace conflict identified were: issues with hierarchy, a lack of understanding of the roles of each profession, and poor communication between professionals. The reasons for strikes were: leadership of the health sector and issues with salaries. Also, the members of each professional group were actively aware of their professions. They displayed strong emotions when talking about other professional groups and continuously compared their status to those of other professions. This finding was significant and consistent, providing a link between health workers’ conflict in the workplace and competitive strikes by trade unions representing these health workers.
Introduction
The Nigerian health system is burdened by rapid population growth, scarcity of skilled workers, and infrastructural decay. These problems, which are nested within a quandary of negative social, economic, and political pressures, are major contributory factors to the country’s poor health indices.1
In recent years, there have been frequent reports of conflicts between core health professionals of different disciplines in the workplace as well. These conflicts are widespread and dysfunctional, occurring at all levels of healthcare delivery. In extreme cases, violence between cross-disciplinary professionals has been reported.2–4
There has also been an increase in the frequency of industrial actions (IAs) by groups of health professionals. In the last decade, no sector has been more affected by disputes and strikes in Nigeria than in the health sector.5 One survey estimates eight general strikes involving different health worker groups and affecting all government tertiary health centers between 2012 and 2015. These did not include local strikes in individual institutions, which are also frequent.6 In that survey, several factors were perceived by participants to be responsible for the incessant nature of IAs. Still, interprofessional disputes were ranked amongst the most important. The said IAs lasted weeks to months at a time with profound consequences on healthcare delivery. Among these, the country’s response to terrorist attacks in the North-eastern region and the Ebola epidemic (both in 2014) were affected.5,7,8 Health worker strikes have also caused an increase in medical tourism as the rich seek health services abroad.6
Two narrative reviews have proffered explanations for the recent upsurge in the frequency of health worker strikes in Nigeria. Osakede and Ijimakinwa9 suggested three themes: “changes in the organization of health services, failure of collective bargaining from previous strikes and disempowerment due to the inability of health workers to provide the best quality care.” The earlier review by Osabuohien10 is also similar, mainly focusing on more contextual issues. While these conclusions may be correct, the collapse of teamwork and reports of interprofessional conflicts that mirror IAs by trade unions suggest associations that are still unclear. Anuforo11 reports how the present situation is such that one professional group calls off an IA, only for another professional group to embark on strike.
The impact of the conflicts and frequent IAs is, however, not in doubt. To further reinforce this point, two surveys investigating maternal mortality in the North and South of the country, independently identified conflicts and strikes, amongst other factors as contributing to poor maternal health indices.12,13 Another study found that incessant health worker strikes between 2007 and 2016 accounted for 26% of the variation in infant mortality and 31% of the difference in life expectancy during the period in question.14
Background
Teamwork Origins and the Nigerian Situation
Healthcare provision is increasingly defined by biomedical and technological advancement, dynamic public perceptions, global shortages of the health workforce, rising costs, and the rising prevalence of chronic disease.15 These factors have resulted in a transformation of organizational structures with a renewed emphasis on collaboration. Consequently, there is a growing body of literature on teamwork in healthcare, particularly in the developed world.16 However, the idealization of collaboration has not been supported by research in developing countries where the push factors for collaboration may be more prevalent.17 A review conducted by the WHO study group on interprofessional education and collaborative practice illustrates this point, revealing 396 studies from 20 countries but only 8% representation from developing countries.18
Teamwork in healthcare is a complicated endeavor. It is based on the premise that professionals who have their interests are willing to work together while maintaining some degree of autonomy.19 On the one hand, teamwork provides overarching benefits to team members, patient care, and health systems.20 On the other hand, it may result in poor interpersonal relations, dysfunctional conflicts, and poor team outcomes.21 However, despite the criticisms, the driving forces for collaboration leave little alternative. Collaboration, therefore, features prominently in many aspects of healthcare in low- and high-income countries. Similarly, the Nigerian national health policy (NHP) promotes interprofessional collaboration.
Health services in Nigeria were initially modeled against the British colonial medical services, but following independence, global trends had a significant impact. Chief amongst these was the Alma-Ata declaration in 1978, on which the foundations of the current NHP were based. Those foundations were laid in 1984 with primary healthcare adopted in 1985 as the basis of the country’s health policy.22 Though interprofessional collaboration is repeatedly mentioned in these documents, they fall short of suggesting which collaborative models to adopt, with a similar trend discernable from the current NHP.1 On the backdrop of the WHO report on the global shortage of human resources in 2006,15 an independent national policy on human resources came into existence in 2007.23 While this document discusses the need for collaboration more extensively, the absence of models to be implemented in the face of interprofessional conflicts and incessant IAs persists.
The result is teamwork in the Nigerian healthcare system being characterized by interprofessional disputes that have been described as “very intense, deep-rooted and crippling”.24 Several surveys in the country have also suggested the overwhelming recognition of interprofessional conflicts by health professionals, with perceived differential treatment between the professions, the assertion of role boundaries, and communication barriers as predominant causes.17,25–27 In terms of its impact on health workers, one survey in the North-eastern region found interprofessional conflicts to be associated with diminished motivation.28 Physical assaults and IAs have also been reported to be conventional modalities of expression of interprofessional conflicts with IAs been more likely.27
In the light of its impact on health services, the Nigerian government has made other notable but unsuccessful attempts to address interprofessional conflicts. A typical example is the “Presidential committee of experts on interprofessional relationships in the public health sector to end unhealthy rivalries,” which was inaugurated in 2013 to look into the problems. Several trade unions rejected their recommendations.8,11 Therefore, it can be surmised that healthcare teamwork in Nigeria is still in its infancy from a policy perspective. Rigorous research into the causes of dysfunctional conflict and their relationship to industrial action would be desirable to provide an evidence base for future policy direction.
Conceptual Framework: The Social Identity Theory
The social identity theory was a useful theoretical framework for this study. It is essentially the knowledge that we belong to social groups, as well as the value, and emotional implications of its membership. Developed by Henri Tajfel and John Turner, it proposes that individuals will classify themselves and others into prototype groups abstracted by their members.29 Such categorization provides members with a sense of purpose, enhancing their self-esteem while helping them deal with other groups in which they feel devalued.
An individual, therefore, expresses numerous identities as a result of membership of several groups, each identity becoming more or less prominent in different contexts.30 However, professional identities are reported to be one of the most important in the lives of individuals.31 Professional identity itself can be described as the beliefs, attitudes, and practices shared within one professional group and related to the professional roles of the members of that group. These identities develop over time, involving the internalization of the values, customs, problem-solving approaches, and even the language of the profession.32 Through these groups, the individual defines his/her location in the social environment (social identity), and systematically defines others (stereotypes), leading to an “us versus them” disposition.33 Such identities can make conflicts intractable, as any compromise on values is viewed as a threat to the group’s existence.
While conflicts can be constructive, the evidence and case reports from the literature indicate that the conflicts in Nigerian healthcare are dysfunctional and relate to tensions around professional roles. Therefore, a valuable theory to help frame and interpret the issues is the social identity theory model. This research aimed to illuminate the perceived causes of conflict in multiprofessional settings and the perceived causal interactions between interprofessional conflicts and IAs through the voices of three groups of professionals: doctors, nurses, and medical laboratory scientists (MLS). The causes of conflict in the relational domain of teamwork, according to Reeves et al,16 were identified in the local surveys reviewed, and this is where this research aimed to illuminate.
Materials and Methods
Study Architecture
The study approach was influenced by the need to understand the issues at an organizational level because of the different professional roles involved and the interactions between them. Since the interest was on illuminating different professionals’ perception of their role and those of others, a qualitative approach comprising a mix of focus group discussions (FGDs) and interviews were utilized. A case-study design was employed,34 with two case-study institutions identified to allow some contrast.
Research Design
Two case-settings (of tertiary hospitals) were purposively sampled a priori, with the selection of hospitals where the most extreme cases of interprofessional conflict were recently reported. Both hospitals have similar organizational structures and are under the auspices of the Department of Hospital Services of the Federal Ministry of Health.35 Staff of both centers also frequently embark on local strikes, in addition to the general strikes affecting all tertiary centers.
One of the hospitals is located in the North, with the other located in the South of the country. Since the North and South of the country are socio-culturally divergent, a better understanding of the participants’ cognitive construction of reality was achieved in the face of these differences.
A single FGD was conducted with each professional group (nurses, doctors, and MLS) in each case-setting, respectively, giving a total of six FGDs. One key informant interview was also conducted with heads of trade unions representing each of these professional groups in each case-setting, giving a total of six interviews.
Ethics Approvals
Ethics approvals were obtained from the Research Ethics Committees of the Liverpool School of Tropical Medicine and each of the participating hospitals. Names and addresses were avoided entirely. Pseudonyms were used for references to specific persons or places in the transcripts. Quotes were avoided when anonymization distorted messages.
Rigor and Researcher Reflexivity
The immediate challenge was to disengage the researchers’ preconceptions to ensure transparency. This was especially important given that the lead author was a practicing physician in a Nigerian tertiary hospital at the time. His experience in multidisciplinary settings in Nigeria and the United Kingdom inspired the conceptualization of this study. Both authors extensively discussed those experiences and potential preconceptions in the light of the researchers’ positionality concerning the study objectives.
To conduct the research, the authors reaffirmed the belief that for patients to benefit, there must be effective collaboration between multidisciplinary professionals. This enabled the researchers to bracket off feelings and empathize with each professional group even when responses were uncomfortable. This stance and the profession of both researchers were communicated to participants while obtaining informed consent.
A pilot run through (of interviews) was also conducted with three representatives from different professional groups. The aim was to identify, understand, and anticipate emotions during the research while avoiding any preconceptions. Both researchers also kept journals of their experiences to serve as reminders to remain objective. Additionally, analytical memos were used to record critical judgments in deciding emergent themes.
Each transcript was re-distributed to participants for up to two days for feedback before analysis. The purpose was for participants to verify the accuracy of the data. The authors have also provided thick descriptions to enable readers to understand the judgments made from the research.
Recruitment of Participants
Focus Groups
The use of FGDs enabled an understanding of how each group of participants interacted with each other and jointly interpreted the issues being discussed. Individuals irrespective of gender, working in high dependency units, who self-identified as having experienced interprofessional conflict, were sought. Though there were no restrictions on gender, no additional effort was made to ensure gender variability. Staff working in donor-funded programs were excluded. For medical doctors, residents were recruited rather than consultants on the assumption that consultants do not regularly experience interprofessional conflict.
The departmental heads acted as gatekeepers, identifying potential participants given the research objectives. A snow-balling technique was also utilized. The only other criterion was for the participant to have spent a minimum of five years in their respective roles. This was based on the premise that health workers with fewer years in their work roles may not have developed values associated with their roles.
Informed consent was obtained from nine participants for each focus group. Discussions took place in private offices and departmental libraries. There was nearly complete turnout for the MLS focus groups, with eight and nine participants in each case-setting. For nurses and doctors, there were four representatives for each, in one case-setting and five representatives for each, in the other case-setting (Table 1).
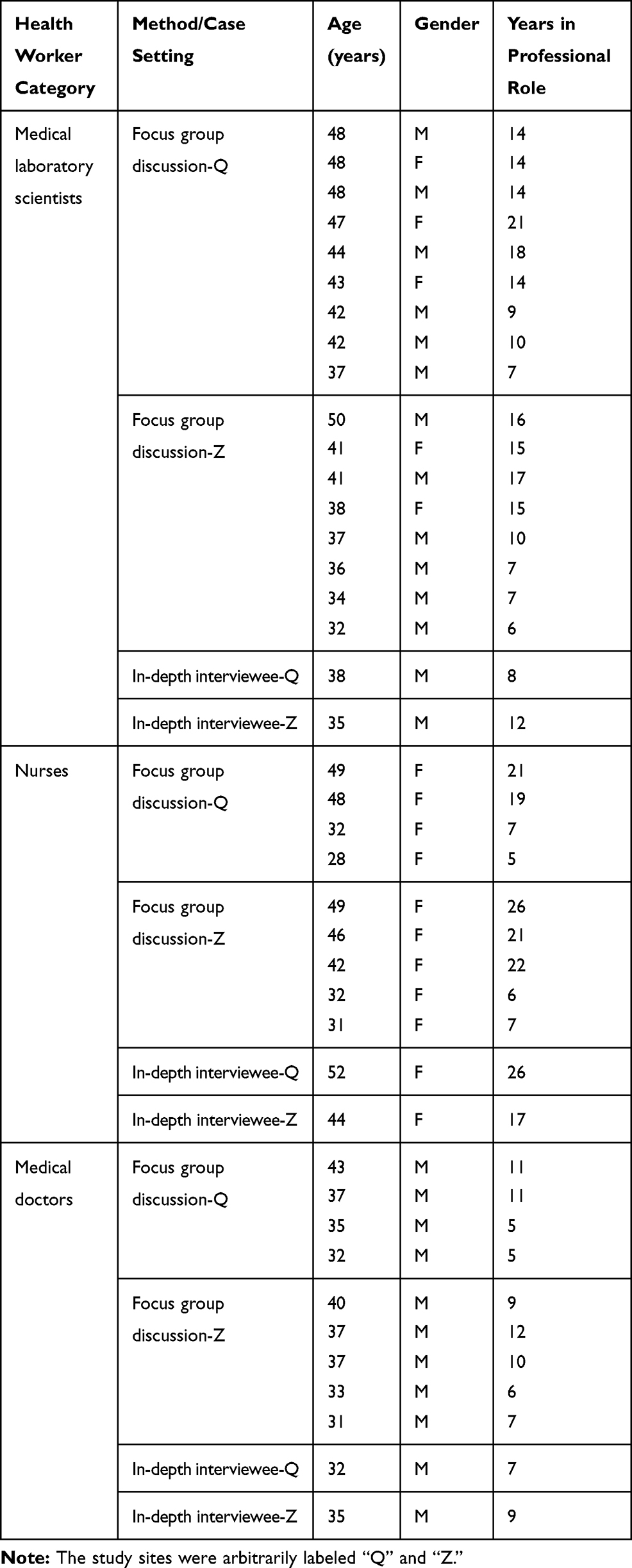 |
Table 1 Demographic Profile of the Participating Health Workers |
Key Informants
Key informants were contacted directly. The presidents or general secretaries of the local chapters of trade unions, including the Joint Health Sector Unions, the National Association of Nigerian Nurses and Midwives, and the Association of Resident Doctors, were interviewed. The aim was to obtain in-depth information regarding the motivations of their respective trade unions for embarking on industrial action. Incidentally, all the interviewees also worked in multidisciplinary settings, making them well suited to the study.
Data Collection
Data was collected between the 24th of July and the 12th of August 2016 using a digital tape recorder and transcribed verbatim. Interviews lasted between 45 and 75 minutes, while FGDs lasted between one and two hours. All discussions were in English. The same interview guide (Table 2) was utilized for both FGDs and interviews. The questions were designed to be exploratory, while the guide aided equivalence across case settings.
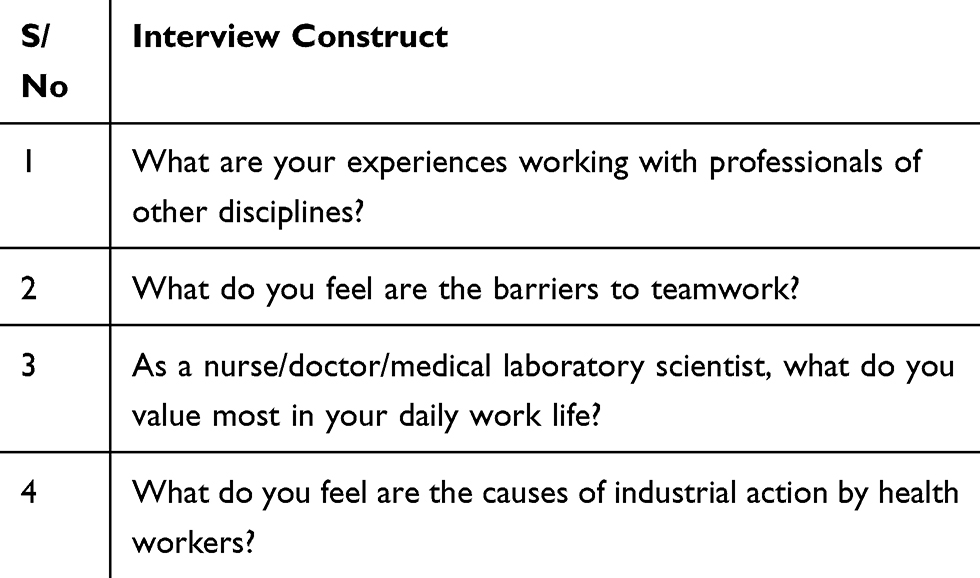 |
Table 2 Constructs of the Interview Guide |
Analysis
Analysis was approached from the perspective of each professional group and was conducted manually. Transcription and coding co-occurred with data collection. The first transcript was read in detail to identify patterns. These patterns were then aggregated into similar categories or codes. The codes were applied to new data sets and modified as data collection proceeded. With each modification, the codes were compared to the earlier transcripts to verify their initial interpretation. We always referred back to analytical memos, where we had recorded critical decisions for deciding on the codes. There was a joint consensus between the authors regarding emergent themes. The dominant themes identified from the interview and FGD of one professional group in one case-setting were compared with the same in the other context. The themes across all professional groups and case-settings were then identified and presented in the results. The social identity theory was finally used to frame the interpretation of the emergent themes and construct provisional explanations.
Results and Discussion
Three themes emerged as barriers to teamwork across both settings. These include professional hierarchy, role ambiguity, and poor communication. Concerning industrial action, the health sector leadership and remuneration were the dominant themes (Tables 3 and 4).
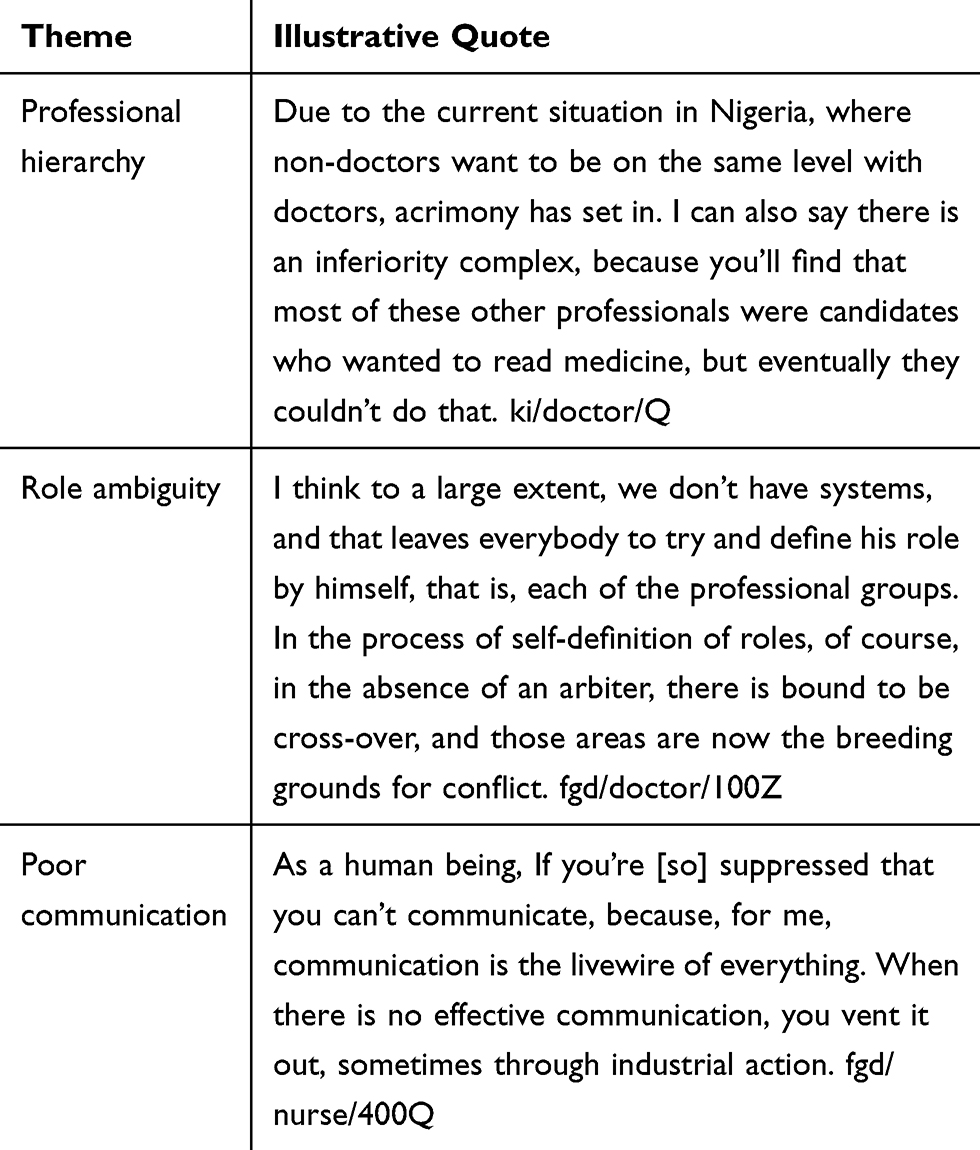 |
Table 3 Main Themes on the Causes of Conflicts Within Multiprofessional Healthcare Teams |
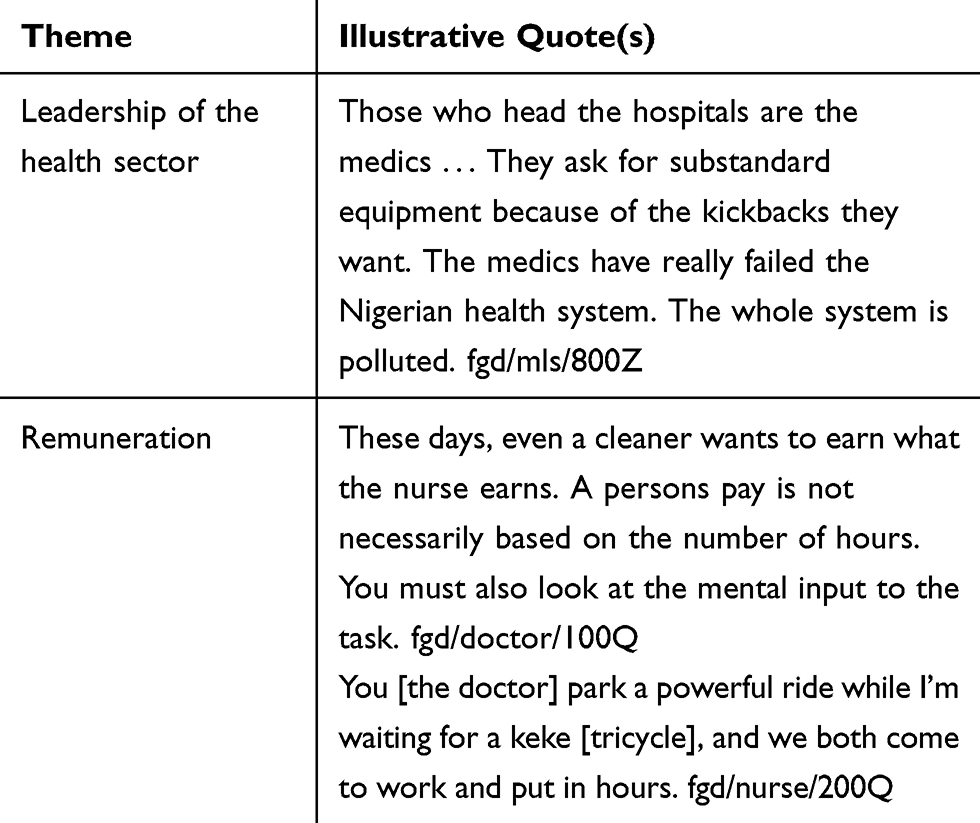 |
Table 4 Main Themes on the Causes of Industrial Actions by Health Workers |
All participants were emotionally preoccupied with the research questions. When asked about their experiences working with cross-disciplinary professionals, all but five participants across board exclusively discussed their perceived barriers to teamwork. Most went on to discuss industrial actions without prompting, sometimes linking workplace conflict directly with industrial actions. No significant differences in narratives were found between interviews and FGDs or across case-settings.
General Perceptions of Teamwork
The narratives of all participants revealed uncertainty about the existence of teamwork. Only five medical doctors (the two key informants and three other participants from FGD’s) narrated some positive experiences. They nonetheless made it clear that their overall experiences were negative (see the third quote).
Furthermore, all participants directed their criticisms of inter-professional relations in the workplace to professional groups and not individuals (social categorization). To this end, references were made to two broad groups – medical doctors and a second group comprising all other core health professionals (including those who did not participate in this study). The use of “medics” and “non-medics” across both case settings to describe the doctor/non-doctor divide was noteworthy with members of the “non-medic” group frequently sympathizing with each other (see second quote).
1.There is nothing like teamwork; rather, there is a cold war in the clinical. fields. ki/nurse/Z
2.The greatest problem we have is the medics [medical doctors]. People are saying, ‘other professionals’, let us call it what it is! We don’t experience problems with nurses, pharmacists, or any other medical professional, but the medics. fgd/mls/700Z
3.My experience is a mixed one, but my first impression when I came here was that of antagonism really, especially from the laboratory scientists. fgd/doctor/400Q
Barriers to Teamwork
Hierarchy
All participants spoke about issues of hierarchy regarding the doctor/non-doctor divide. Virtually all participating nurses and MLS felt doctors saw themselves as being superior to other professionals, which they perceived as being inimical to teamwork. Both groups independently sympathized with each other while expressing disdain for doctors across both settings. Given that nurses are predominantly female, two nurses (one key informant and one participant in an FGD) also drew parallels between their perceived masculinistic attitudes of medical doctors in the workplace and the background patriarchal ideology that pervades the Nigerian social environment.
Between the nurses and MLS, the MLS were more passionate about issues of hierarchy. Of the 19 MLS who participated in the study, 13 of them went further, seeing the perceived hierarchy as an attack by doctors, not just on the dignity of their roles but also their personal dignity. In both focus groups involving the MLS, the issue of who should be the ideal team leader was discussed. The perceptions in both groups were complementary, in that it was appropriate that doctors were the team leaders. Nevertheless, having acknowledged this, they loathed a perceived non-recognition of their value as health professionals.
4.Doctors think they have big brains. Big brains should see patients, while small brains should clean the poo … during ward rounds, you may have something to say, but from past experience, also their disposition, they don’t listen to people’s suggestions; therefore, you don’t make your input. They prefer to make the mistake while the patient bears the brunt, then they correct themselves. fgd/nurse/300Q
5.There is this arrogance that ought not to be there, so there is nothing like teamwork. Like I told one doctor the other day, God did not create everyone equal, but He has a reason for putting every one of us where we are, including the cleaner. fgd/mls/700Z
The doctors also identified issues of hierarchy as a barrier to teamwork. Most of their responses were prescriptive, looking at the issues of hierarchy from the perspective of perceived poor leadership qualities of doctors being the usual team leaders (see quote 6). Other responses (see Table 3) include the doctors viewing non-doctors as envious of their status or engaging in a subjective assessment of their status with reference to doctors’ status.
6.In the postgraduate training program, there is nothing serious aiming to put the would-be consultant into the perspective of identifying what it means to be in a team, team dynamics, and how you as a doctor can manage such dynamics. fgd/doctor/100Z
Roles
All participants perceived issues surrounding role ambiguity as a significant reason for tension and conflicts. The narratives by nurses involved subtle manifestations of power. For instance, specific examples were given by the nurses across both settings regarding who should clear the field after a procedure (see quote 7).
The tendency to view issues from the lens of an individual’s profession was also evident. In the quote below, for instance, the team’s house officer was described as the “doctor’s house officer” (social identity). On this evidence, what might be surprising is that these professionals are still able to work together from time to time.
7.Sometimes, the doctor may not want to pick instruments by himself. After the procedure, he may want to leave the soiled gloves or used syringes on the patient’s bed. In fact, we had a scenario this morning where the doctor dumped everything on the ground. His house officer was about picking them up, he said no, don’t pick it, the nurses will come and pick it. He said this to the hearing of the nurses. fgd/nurse/500Q
The MLS were often passionate in describing their roles. They saw the use of the laboratory by doctors as an intrusion, and this was consistent across both settings. They also perceived doctors who worked in the laboratories as wanting to take their jobs despite having no training or laboratory license. The term “quackery” was used by five participants across both settings in reference to these doctors. They also related their experiences of tension and conflicts in the workplace directly to industrial actions.
8… we discovered that all of a sudden, they [doctors] started getting interested in our pipettes. They started getting interested in our reagents. Now they want to analyze our samples. The question is: is that what they were trained to do? The answer is no … It got so bad that if we want to carry out a strike for like a few days or one week, they quickly present themselves to the laboratory and say they are working. fgd/mls/400Z
9.What they [doctors] are after is to take everything. To control everywhere. To take everyone’s work by hook. Assuming they even want to pick the medical lab science form and read medical laboratory science, get the license, it would have been different. The problem is that from where they are, through quackery, they want to take over. Please serve as a voice if you see them. Let’s forget about this rivalry. Let’s talk about improving our health sector. Please can we talk about improving our health sector? fgd/mls/300Z
10.Sorry, I’m a Christian, so I’ll quote the Bible. Let every man stay within his own calling. fgd/mls/100Q
The doctors, on the other hand, expressed a range of opinions. Both key informants perceived a lack of role definition as a significant problem. In one case-setting, all participants in the FGD shared a similar perception, with their narratives being mainly prescriptive. The other participants perceived other professionals as being aware of their roles but rebellious at the same time.
11.It’s a situation where people [other health professionals] don’t want to do their jobs; what they are looking at is what other people [doctors] are doing. When you are working, the other person thinks you’re ordering him about. The only way we can overcome that is by insisting on people to do what they are supposed to do. fgd/doctor/100Q
Also, medical doctors tended to see their roles as being the central focus of health services with other professionals making their input exclusively to enable the doctor to diagnose, treat, and prevent disease. By seeing themselves as the focal point of health services, they sometimes accepted the responsibility for the occurrence of conflict in their various teams. At other times, their narratives suggest a frustration due to a lack of cooperation from other professionals in achieving the “doctor’s goal” of patient care. In contrast, nurses and MLS saw their roles as making direct contributions to patient care in ways in which they perceived the doctor was deficient. In so doing, they acknowledged that they were supporting the doctor in carrying out his/her role. These differences persisted across all themes and case settings. As a result, where doctors perceived poor leadership of the team and lack of job description as barriers to teamwork, non-doctors perceived a domination of power and roles by doctors as barriers.
Communication
The narratives of the nurses regarding poor communication generally had a hint of subtle manifestations of power. However, three of the participants overall also talked about a complete absence of communication concerning patient care.
12…Where a doctor does not communicate with the nurse, he comes and writes and throws the folder, or communicates directly with only the patient, there are bound to be problems. fgd/nurse/200Z
For the MLS, it was instead a question of doctors not treating them respectfully or blaming them when errors occurred with laboratory results.
13.What you see is that a consultant just appears one day and he starts shouting on everyone. He starts making noise everywhere. You don’t see him on a regular basis, but once he’s around, he ferments trouble. fgd/mls/600Q
14.When they make a mistake, our medics don’t acknowledge that the mistake is clearly from them. Instead, they seek to push the blame either to the nurses or the laboratory scientists or they cover it up.“-fgd/mls/800Z “Especially the lab”-fgd/mls/200Z
All the doctors in the focus group in one case-setting and one doctor in the second case-setting also identified communication issues as a barrier. Without exception, their narratives were prescriptive. The following extract is illustrative of the narratives:
15.I think we are not interacting enough. We are not taking active measures to talk to each other … what happens is that everybody works like an island. fgd/doctor/300Q
Values Around Roles
All participants perceived their contribution to patient care and learning on the job as being what they valued. The narratives of nurses and MLS were often in line with helping the doctor carry out his/her role. However, their descriptions were generally more detailed, listing specific instances where they derived value. For example, particular situations were given by the MLS in one FGD concerning their value in veterinary research, water purification, and public health. The following quotes are illustrative of the responses:
16.You see a dying child coming out of that condition and getting better. In the process, you continue to learn and improve on your knowledge and skill. That’s the height of joy for me. fgd/doctor/500Z
17.By virtue of this profession, we are able to proffer diagnosis regarding any ailment. We are like the searchlight. We throw light into the darkness. fgd/mls/100Z
The differences in perspective have also resulted in a subjective re-assessment of qualifications in comparison with other professionals. For instance, in talking about values associated with roles, the MLS in one FGD went to great lengths to explain their primary undergraduate courses and diploma. It is noteworthy that this was less about a demonstration of competence and more about comparing with doctors, with the perceived significant difference being that doctors are awarded their degree after six years of undergraduate study as opposed to five years for MLS in Nigeria (social comparison). This observed closeness is likely contributing to the intensity of the rivalry between MLS and doctors.
General Perceptions of Industrial Action
All participants denounced industrial actions, sometimes with a gloomy perception of what the future holds, as illustrated by the following quote:
18.During the last strike, I lost my mom. If the government had done the right thing, the strike should not have taken place. She would get adequate attention … It [industrial action] can affect anybody. fgd/mls/500Z
Causes of Industrial Action
Leadership of the Health Sector
All participants, including key informants, perceived poor leadership as a reason for incessant industrial actions. However, while the doctors recommended leadership training, nurses and MLS were independently unified in suggesting hospital administrators rather than medical doctors, to lead government hospitals.
19.As doctors, we claim to be, or we are the head of the medical team … But there has not been any formal training on leadership on our curriculum. Maybe our elders too, have not really shown or lead by examples. fgd/doctor/200Q
20.These problems will remain a recurring decimal until the hospital system is restructured ….it should be manned by administrators where every professional comes to do his work and people go to make issues known to the administrator. fgd/nurse/200Q
Nurses and MLS were keen to suggest a change in the management of hospitals because they perceived the doctors as promoting only their interests akin to their perceptions of teamwork. Their reason for this was less about poor leadership and more about having a perceived neutral arbiter at the helm. The MLS went further, viewing the doctors as corrupt and responsible for the health system’s failure (see Table 4). These stereotypes are contributing to conflicts and industrial actions being more frequent.
Remuneration
A similar pattern is discernible from the narratives of participants. All participants perceived a hierarchy concerning remuneration. While doctors viewed this to be directly proportional to input, nurses and MLS understood it to be unfair. The evidence also suggests that doctors were keen to maintain the status quo while other professionals were keen to offset the status quo.
21.Everybody in the health sector should have one salary scale, so to speak. So that in the ladder, everybody knows where they fall. If there are going to be adjustments, it should happen across board, but a relativity regarding your profession is maintained. The different salary scales are putting us in a lot of mess. fgd/doctor/300Z
22.One major reason for strikes is the obvious dichotomy. When the NMA [Nigerian Medical Association] negotiates an upward review of their salaries, the government should know that there are nurses, lab scientists, radiographers, and all that. A situation where you address it for person A, but close the chapter for persons B, C, and D will result in industrial action. fgd/nurse/300Q
What also comes across as striking is that the feelings between professionals are intense, and the resentment is deep. Strong personal pronouns, interrogatives, intense nouns, and adverbs were used to delineate boundaries or discriminate. Feelings were most intense with the MLS who were often philosophical while giving their narratives, their interest partly reflected in their willingness to participate in this research (Table 1). The lead author was not spared by one of the participants, as demonstrated by the following quote:
23.Just the singular fact that you were a doctor, I didn’t want to participate in this discussion because of the problems with doctors that has been hammered. fgd/mls/300Q
Within the context of the social identity theory, there is evidence to suggest self-categorization and social categorization by health professionals (eg quotes 21, 22, and 23). There was also a recognition by participants of a shared identity between the members of two broad groups: doctors and non-doctors (eg quotes 2, 7, 11, 14, and 22). The apparent cohesion of the non-doctor group despite this group comprising professionals with heterogenous roles is evidence of the centrality of their values and the emotional implications of group membership. There is also evidence to suggest that this categorization had caused each group to regard the other as stereotypes (eg quotes 5 and 11). Through stereotypes, each group interpreted the actions and expectations of the other in turn with regards to interprofessional relationships and other contextual issues.
The evidence explains the frequency and intensity of both interprofessional conflicts and IAs and provides a link between the two. The cognitive construction of these identities cuts across the different socio-cultural milieu where both case settings are located. Similarities in narratives were evident across both settings, sometimes akin to reading from the same script. Across both settings, some participants in each professional group cited similar examples from individual personal experiences and, in some cases, used the same wording while narrating these experiences. This was surprising, especially with the focus group discussions given the improbability of participants across case settings discussing the issues before this study. It also suggests deeply held values straddling the doctor/non-doctor divide concerning interprofessional relationships. Doctors generally viewed the issues from a position of positive identity, positive esteem, and a need to preserve the status quo. In contrast, nurses and MLS saw the problems from a place of negative identity, negative esteem, and a need to offset the status quo.
Several surveys conducted in Nigeria have documented the widespread nature of tensions and conflict, their causes, and implications. The study by Olajide et al27 identified limited staff interaction and “a desire for power” by health professionals as causes of conflict. For Ogbimi and Adebamowo,36 poor social interaction, activist unionism, “disregard for one’s profession,” amongst other factors were perceived to be associated with the occurrence of workplace conflict. In the study by Akpabio et al,37 discriminatory issues were identified as being contributory to workplace conflict. In contrast, the results of this research suggest that professional identities are salient in the Nigerian health care system with issues of hierarchy, role ambiguity, and poor communication identified from these surveys as potential fault lines. There is a need for further research into the contribution of these fault lines to workplace conflict from the perspective of professional identities in Nigeria.
The relative “fitness” of the individual in a social category depends on the expectations from the observed similarity or difference from other groups.30 To this end, the narratives promulgated along the doctor/non-doctor divide are also reflected at the contextual level in Nigeria. The perceived hegemony of health care by doctors has seen the formation of several new trade unions comprising other core health professionals and cutting across disciplinary lines. The “Joint Health Sector Unions” and the “Assembly of Healthcare Professional Associations” of Nigeria are two of such alliances that exclude medical doctors from their membership. The interprofessional boundaries within these trade unions have been blurred, while the alliances themselves have become the vanguard for resisting the perceived dominion of doctors in Nigerian healthcare.11,38 However, their existence and actions stimulate an identity threat on the part of doctors leading to further chaos.
A discussion of professional identities must also be done within the historical context. Individuals often have strong attachments to historical events, which can deepen stereotypical perceptions.39 Concerning this, two past events are worth mentioning. The first is the restructuring of the Nigerian health system in 1985 by the now-infamous decree 10.40 This decree established the appointment of boards and medical directors of the country’s tertiary institutions, specifying that medical directors be “medically” qualified. Non-doctors oft perceive the decree as discriminatory. The second event was the appointment of Professor Eyitayo Lambo-a health economist, as minister of health in 2003. While medical doctors are generally viewed to have been opposed to his appointment, the relative stability in the health sector during his tenure is regularly used as justification by non-doctors to make their case for more open leadership.5,11
The apparent complexity of the problems notwithstanding, there is good evidence to suggest that interprofessional education (IPE) improves team outputs within the context of integrated health care.20 It generally achieves this by providing health workers with the knowledge and skills required for working collaboratively. Such practices have been demonstrated to reduce communication failures, promote role clarification, change existing cultures, and diminish the adverse effects of professional identities. Since identities tend to develop early and are strengthened over time, the goal of IPE in this context should be to start early in an individual’s professional development to foster a dual professional and team identity. However, these measures are by no means straightforward. Nonetheless, if properly adapted, IPE can also hypothetically reduce the potential for health workers’ competitive industrial actions. For such measures to be incorporated into policy, collaboration between the health and education ministries will be crucial. Also, institutional support will need to be provided, while models on patient safety and service delivery will need to be studied and adapted to the Nigerian setting. To this end, this research should provide a pedestal for directing future research and policy concerning teamwork in the Nigerian health care system.
Conclusions
This study brings the salience of professional identities and, potentially, fault lines in the Nigerian healthcare system into focus. The negativity of the findings can be explained by the recruitment of subjects who self-identified as having experienced cross-disciplinary conflict, and their focus on teamwork barriers. The lack of attention to ensuring gender variability, evident during analysis, and the non-inclusion of other core health professionals are potential limitations of this study. While the findings must be placed in the context of the selection of critical case-settings and participants’ characteristics (eg residents rather than consultants), the inclusion of two case settings and richness of the data adds to the credibility of the results. It has also contributed to theory by proposing that professional identities may provide a link between conflicts in the workplace and industrial actions by health workers.
In the Nigerian context, the social identity theory provides a robust framework to understand how health workers think and how it contributes to the problems of interprofessional disputes. These identities are not universally negative, as studies have shown that group identification provides a basis for members to give and receive social support from one another.41 However, the success of solutions to salient professional identities and interprofessional disputes may lie in the ability to question emanating assumptions, and incorporate the understanding into meaningful health policies. There remains a need for further research in this area, as well as the impact of IPE practices in enhancing teamwork in the face of salient professional identities in Nigeria.
Abbreviations
FGD, focus group discussion; IA, industrial action; IPE, interprofessional education; MLS, medical laboratory scientist; NHP, national health policy; WHO, World Health Organization.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Federal Ministry of Health. The Nigerian national strategic health development plan frame-work 2009–2015. Available from: https://www.uhc2030.org/fileadmin/uploads/ihp/Documents/Country_Pages/Nigeria/Nigeria%20National%20Strategic%20Health%20Development%20Plan%20Framework%202009-2015.pdf.
2. Olatinwo A. Managing inter-professional relationships in the health sector. The Nation. 2014. Available from: http://thenationonlineng.net/managing-inter-professional-relationships-health-sector/.
3. Medical News Nigeria. Nigeria medical association FCT press release on assault/attack of doctors at their duty posts by JOHESU members. Medical World Nigeria. 2015. Available from: https://medicalworldnigeria.com/post/medical-and-dental-consultants-association-of-nigeria-mdcan-national-executive-council-nec-meeting-communique?pid=30145.
4. News Agency of Nigeria. JOHESU strike: NMA decries attacks on doctors, patients in Enugu. The guardian. 2018. Available from: https://guardian.ng/features/johesu-strike-nma-decries-attacks-on-doctors-patients-in-enugu/.
5. Ihekweazu C Three reasons strikes will continue in Nigeria’s health sector. Nigeria Health Watch. 2015. Available from: http://nigeriahealthwatch.com/three-reasons-strikes-will-continue-in-nigerias-health-sector/.
6. Oleribe OO, Ezieme IP, Oladipo O, Akinola EP, Udofia D, Taylor-Robinson SD. Industrial action by healthcare workers in Nigeria in 2013–2015: an inquiry into causes, consequences and control—a cross-sectional descriptive study. Hum Resour Health. 2016;14(1):46. doi:10.1186/s12960-016-0142-7
7. Oleribe OO, Salako BL, 25Ka MM, et al. Ebola virus disease epidemic in West Africa: lessons learned and issues arising from West African countries. Clin Med. 2015;15(1):54–57. doi:10.7861/clinmedicine.15-1-54
8. Nigerian Health Watch Admin. Why strikes are killing the public health sector and why it may be difficult to reclaim. Nigeria Health Watch. 2015. Available from:. http://nigeriahealthwatch.com/how-strikes-are-killing-the-public-healthcare-sector-and-why-it-may-be-difficult-to-reclaim/.
9. Osakede KO, Ijimakinwa SA. The effect of public sector healthcare workers strike: the Nigeria experience. Rev Pub Admin Mgt. 2014;3(6):154–161.
10. Osabuohien E. Industrial conflicts and health care provision in Nigeria. In: Ninalowo A, Badru FA, Akinyemi, editors. An Interdisciplinary Discourse on the Human Condition. Lagos: University of Lagos; 2010:64–95.
11. Anuforo E Leeway to industrial harmony in the health sector by MDCAN. The Guardian. 2015. Available from: http://guardian.ng/features/natural-health/leeway-to-industrial-harmony-in-health-sector-by-mdcan/.
12. Ozumba BC, Nwogu-Ikojo EE. Avoidable maternal mortality in Enugu, Nigeria. Pub Health. 2008;122(4):354–360. doi:10.1016/j.puhe.2007.04.018
13. Sabitu K, Alti-Mu’azu M, Musa AA, et al. The effect of improving maternity services in a secondary facility, Zaria, Nigeria. Int J Gynecol Obstet. 1997;59(2):S99–S106. doi:10.1016/S0020-7292(97)00153-7
14. Kalu I, Udeorah SA. Labor crises in the health sector and economic development in Nigeria. Int J Sci Res. 2018;III(2):84–95.
15. World Health Organization. Working Together for Health, 2006. Available from: https://www.who.int/whr/2006/whr06_en.pdf?ua=1.
16. Reeves S, Lewin S, Espin S, Zwarenstein M. Interprofessional Teamwork for Health and Social Care. Barr H ed. John Wiley and Sons; 2011.
17. Iyoke CA, Lawani LO, Ugwu GO, et al. Knowledge and attitudes towards interdisciplinary team working among obstetricians and gynecologists in teaching hospitals in Southeast Nigeria. J Multidiscip Healthc. 2015;8:237–244. doi:10.2147/JMDH.S82969
18. Yan J, Gilbert J, Hoffman S, Rodger S, Ishikawa Y. WHO study group on interprofessional education and collaborative practice. J Interprof Care. 2007;21(6):587–589.
19. D’Amour D, Goulet L, Labadie J, Martín-Rodriguez LS, Pineault R. A model and typology of collaboration between professionals in healthcare organizations. BMC Health Serv Res. 2008;8(1):1–14.
20. Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013;3:CD002213.
21. Brown J, Lewis L, Ellis K, Stewart M, Freeman TR, Kaspersky JM. Conflict on interprofessional primary healthcare teams–can it be resolved? J Interprof Care. 2011;25(1):4–10. doi:10.3109/13561820.2010.497750
22. Health Reform Foundation of Nigeria. Nigerian Health Review: Primary Healthcare in Nigeria: 30 Years After Alma Ata. Abuja: Author; 2007.
23. Federal Ministry of Health. National human resources for health strategic plan 2008 to 2012. Available from: https://www.who.int/workforcealliance/countries/Nigeria_HRHStrategicPlan_2008_2012.pdf.
24. Adeniji O. Groupthink among health workers: the Nigerian perspective. Researcher. 2010;2(5):1–4.
25. Ogbonnaya LU, Ogbonnaya CE, Adeoye-Sunday IM. The perception of health professions on causes of interprofessional conflict in a tertiary health institution in Abakaliki, southeast Nigeria. Nig J Med. 2007;16(2):161–168. doi:10.4314/njm.v16i2.37300
26. Lorngurum T, Godowoli A. The nature of competition and conflicts among health professionals in Nigeria. Nig Hosp. 2008;2(2):42–48.
27. Olajide AT, Asuzu MC, Obembe TA. Doctor-nurse conflicts in Nigerian hospitals: causes and modes of expression. Br J Med Med Res. 2015;9(10):1–12. doi:10.9734/BJMMR/2015/15839
28. Chirdan O, Akosu JT, Ejembi CL, Bassi AP, Zoakah AI. Perceptions of working conditions amongst health workers in state-owned facilities in north-eastern Nigeria. Ann Afr Med. 2009;8(4):243–249. doi:10.4103/1596-3519.59579
29. Tajfel H, Turner JC. An integrative theory of intergroup conflict. Soc Psychol Intergroup Rel. 1979;33(47):74.
30. Burford B. Group processes in medical education: learning from social identity theory. Med Educ. 2012;46(2):143–152. doi:10.1111/j.1365-2923.2011.04099.x
31. Haslam AS, Jetten J, Postmes T, Haslam C. Social identity, health, and well‐being: an emerging agenda for applied psychology. Appl Psychol. 2009;58(1):1–23. doi:10.1111/j.1464-0597.2008.00379.x
32. Nancarrow SA, Borthwick AM. Dynamic professional boundaries in the healthcare workforce. Social Health Illn. 2005;27(7):897–919. doi:10.1111/j.1467-9566.2005.00463.x
33. Ashforth BE, Mael F. Social identity theory and the organization. Acad Manage Rev. 1989;14(1):20–39. doi:10.5465/amr.1989.4278999
34. Seawright J, Gerring J. Case selection techniques in case study research: a menu of qualitative and quantitative options. Pol Res Q. 2008;61(2):294–308. doi:10.1177/1065912907313077
35. Federal Ministry of Health. Agencies under the Federal Ministry of Health. Available from: https://www.health.gov.ng/index.php?option=com_content&view=article&id=129&Itemid=495.
36. Ogbimi RI, Adebamowo CA. Questionnaire survey of working relationships between nurses and doctors in university teaching hospitals in southern Nigeria. BMC Nurs. 2006;5(1):2. doi:10.1186/1472-6955-5-2
37. Akpabio I, John ME, Akpan MI, Akpabio F, Uyanah DA. Work-related conflict and nurses’ role performance in a tertiary hospital in South-South Nigeria. J Nurs Educ Pract. 2016;6(2):106.
38. Adeloye D, David RA, Olaogun AA, et al. Health workforce and governance: the crisis in Nigeria. Hum Resour Health. 2017;15(1):32. doi:10.1186/s12960-017-0205-4
39. McNeil KA, Mitchell RJ, Parker V. Interprofessional practice and professional identity threat. Health Social Rev. 2013;22(3):291–307. doi:10.5172/hesr.2013.22.3.291
40. Federal Government of Nigeria. University Teaching Hospitals (Reconstitution of Boards e.t.c,) Act (No. 10) 1985. Available from: http://lawsofnigeria.placng.org/laws/U15.pdf.
41. Haslam SA, O’Brien A, Jetten J, Vormedal K, Penna S. Taking the strain: social identity, social support, and the experience of stress. Br J Soc Psychol. 2005;44(Pt 3):355–370. doi:10.1348/014466605X37468
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.