Back to Journals » Advances in Medical Education and Practice » Volume 10
Teaching students to identify and document social determinants of health
Authors Lewis JH, Whelihan K ![]() , Roy D
, Roy D
Received 26 February 2019
Accepted for publication 25 July 2019
Published 20 August 2019 Volume 2019:10 Pages 653—665
DOI https://doi.org/10.2147/AMEP.S206819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Joy H Lewis,1 Kate Whelihan,1 Debosree Roy2
1Department of Public Health, A.T. Still University School of Osteopathic Medicine in Arizona, Mesa, AZ, USA; 2A.T. Still Research Institute, A.T. Still University Arizona School of Health Sciences, Mesa, AZ, USA
Correspondence: Joy H Lewis
Department of Public Health, A.T. Still University School of Osteopathic Medicine in Arizona, 5850 E. Still Circle, Mesa, AZ 85206, USA
Tel +1 307 200 7009
Fax +1 480 219 6159
Email [email protected]
Purpose: Social determinants of health (SDH) are responsible for significant health disparities, morbidity and mortality. It is important to acculturate trainees to identify and document SDH. This can elevate their perceptions related to the importance and relevance of SDH. Documentation can encourage trainees to see SDH as factors which medical providers should address.
Patients and methods: Researchers devised a novel approach to demonstrate the value of SDH to undergraduate medical students. Proprietary diagnostic codes for SDH and procedure codes for action taken to address them, were developed. Students were encouraged to log these into electronic records for clinical encounters. Students’ voluntary use of these codes was evaluated. Additionally, students were surveyed on their familiarity with the concept of SDH, their perceptions of the importance of SDH, as well as documenting SDH, twice in the study period, and results were compared. In their second year of use, proprietary codes were compared to newly available SDH related ICD-10 codes.
Results: Students utilized proprietary codes more often than SDH related ICD-10 codes. Over 20,000 codes were logged. Comparison of survey items showed modest increases in students’ positive perception about the role of SDH in patient health.
Conclusion: Students’ voluntary logging of SDH codes demonstrates they perceived these factors to be important and relevant to patient encounters. Future analyses will examine students’ knowledge, attitudes, beliefs and practice patterns related to SDH.
Keywords: social determinants of health, medical education, constructivist learning, electronic health record
Introduction
The significant health effects of social factors such as the environment, community, family structures and circumstances are well recognized.1 Known as the social determinants of health (SDH), the World Health Organization (WHO) identifies these factors as responsible for the avoidable health disparities that exist between communities. SDH are highly intersectional and continue to affect health outcomes in additive capacities.2 They are also responsible for observed rates of excess morbidity and mortality: In 2000, an estimated 119,000 deaths were due to income inequality, 162,000 to low social support, 176,000 to racial segregation and 245,000 to low levels of education.3
Given the significant impact SDH have on health and well-being, it is important for medical providers to recognize SDH and be acculturated to identify and document them like other clinical conditions. The American College of Physicians (ACP) emphasizes that health care professionals should know how to screen for and identify SDH and should work with others to address the important social factors influencing patients.4 The ACP further recommends SDH and health inequities be integrated into medical education at all levels.4 The salient goal of training medical students to identify and address SDH is to equip practitioners with the worldview necessary to alleviate disparities.5 Competency in SDH is a necessary skill for trainee doctors to possess in order for them to address all needs of their patients.6
One tool in promoting SDH competency is the Electronic Health Record (EHR), which is increasingly becoming important for individual and population health, and can be harnessed to address SDH. The National Academy of Medicine (NAM), formerly known as the Institute of Medicine, calls to incorporate at least 16 patient-reported SDH measures and one neighborhood characteristic measure in electronic health records.7 EHRs have been used to connect patients in need with necessary social services to provide care to special populations, such as homeless veterans.8 With accessibility in the EHR, SDH become part of what must be considered by health care teams. This allows providers to address SDH alongside clinical conditions. Documenting SDH in the medical record is a way to acknowledge these factors as medically relevant. It is critical to ensure medical students are proficient at documenting all important patient conditions and care, including SDH.9
Following a 2004 NAM recommendation to integrate social and behavioral science competencies in medical curriculum, the Accreditation Council for Graduate Medical Education developed SDH competencies. However, a reliable method of teaching SDH to students, which may also help transform their future practice, is yet to be determined. A literature review on the subject of methods for teaching SDH in medical curriculum yielded very few results, and none of the approaches found were evaluated for efficacy.10,11 Pedagogical approaches to teaching SDH that are innovative, collaborative, participatory and transformative are key to making future practitioners well-equipped and service-ready to face the challenges posed by health disparities.12
Practical programs are needed to train students to appreciate the importance of identifying and addressing SDH. Students at the A.T. Still Univeristy School of Osteopathic Medicine in Arizona (ATSU SOMA) are exposed to service learning opportunities from their second year of medical education when they are embedded in community health centers as student doctors serving underserved communities under the stewardship and guidance of regional directors of medical education. As such, ATSU SOMA students encounter SDH frequently in their patient encounters.
In 2015 a student wrote in a report to her professor reflecting on a particular patient encounter.
Today I had the privilege of being able to talk to a gentleman (my patient) for almost twenty minutes. When I log him into E*Value, the school’s logging program for patients, he will be reduced to ‘hypertensive crisis, sleep apnea, pacemaker, obesity, and substance abuse.’ I wish we could log ‘insufficient resources’ or ‘experiencing homelessness’ or any of a number of social challenges he faces that compromise his health. He isn’t able to hold a job because he falls asleep when he sits. Why? Because his sleep apnea is so bad he doesn’t sleep. If he had stable housing he would be on CPAP at night. But to have stable housing you have to have income.
This incentivized faculty to devise a constructivist learning method and objective for medical curriculum which would help students recognize, document and value SDH at par with medical conditions. A constructivist learning approach emphasizes that learning occurs when students are actively involved in constructing meaning.13 The objective of this intervention was to teach students to recognize SDH as independent and important factors affecting health, which are within the realm of what medical providers should address.
The teaching method which involved coding SDH in a teaching EHR, was implemented and then evaluated over two years with five cohorts of students. Primary questions that drove the evaluation were:
- How many times were SDH codes recorded?
- Are students familiar with the concept of SDH? Were there changes in their self-perception of SDH over the study period?
- Do students think that addressing the role of SDH is important while providing care? Were there changes in this value over the study period?
- Do students think that documenting SDH in EHR is important to the health of patients? Were there changes in their perception over the study period?
Materials and methods
ATSU SOMA uses E*Value, a MedHub product designed as both a learning tool and mechanism for ensuring standardization of instruction. Starting in their second academic-year, students are required to log diagnostic and procedure codes for all patient encounters. Procedures were logged irrespective of whether they were observed, assisted or independently performed.
Early in 2015, faculty created a list of 18 diagnosis and 7 procedure codes for SDH and added these proprietary codes to E*Value (Table 1). These were based on factors widely defined as SDH and commonly encountered in medical settings. The codes were developed from the NAM’s committee on the recommended social and behavioural measures for electronic health report,14 and the Healthy People 2020 Social Determinants of Health Framework,15 along with insight from the WHO definition of SDH.16 A list was developed from these inputs and then reviewed by clinical faculty at ATSU SOMA, who have significant experience working in health center settings. This resulted in small revisions and a comprehensive list. The list was pilot tested as part of a health center clinic-based “card study” and then further refined.17
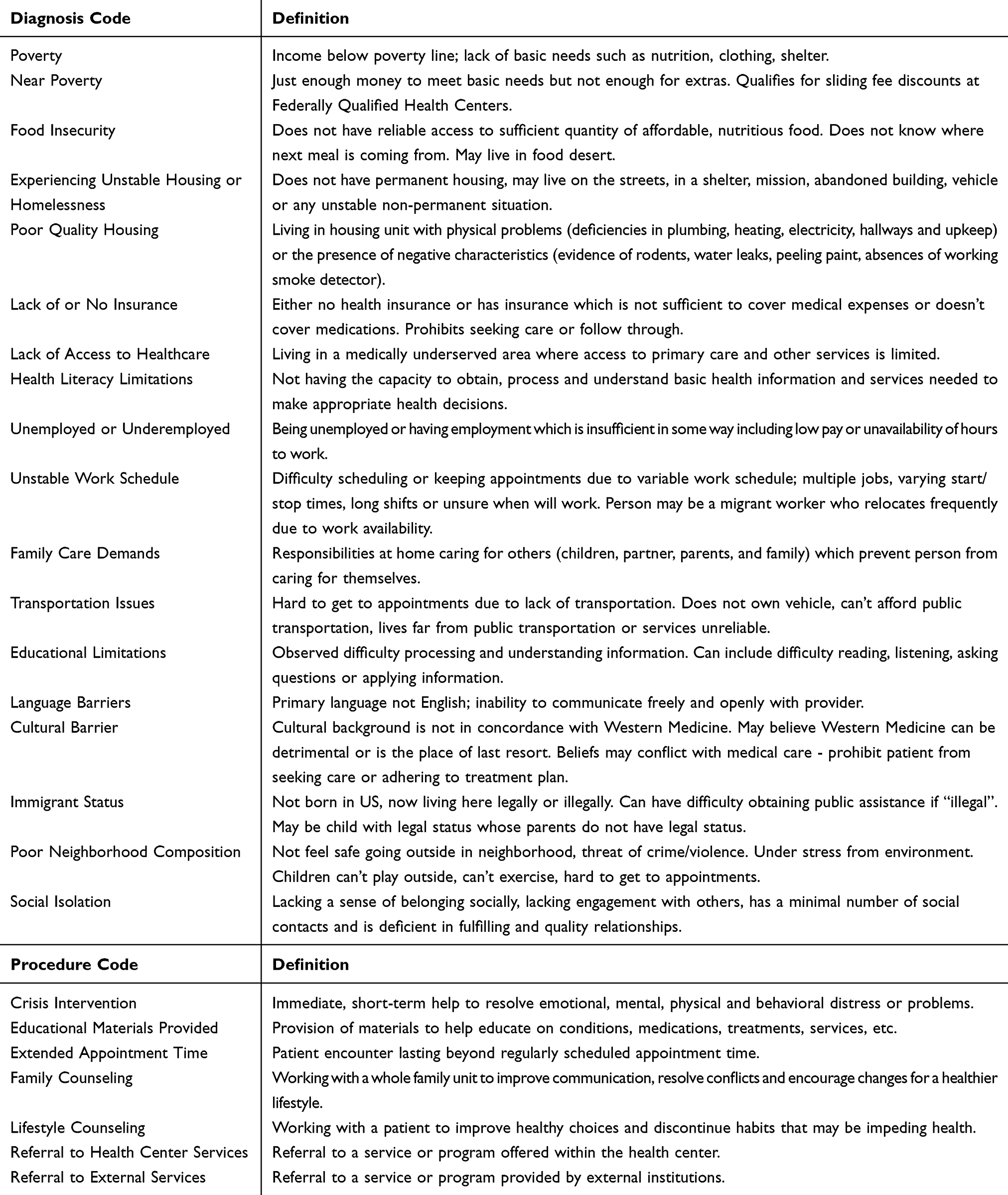 |
Table 1 Proprietary social determinants of health diagnosis and procedure codes defined |
Project year 1
Project year 1 (PY1) ran concurrently with Academic Year 2015–2016. At the start of this year, students and faculty were informed about the additional proprietary SDH codes available within E*Value. Students were given the ability to log “SDH diagnoses” and any of the corresponding procedures performed to address the SDH. A code for “other” was included. This code was to record any factors students observed and deemed to be a SDH not included in the available codes.
Project year 2
Project year 2 (PY2) began with the start of Academic Year 2016–2017. At this time, the US Department of Health and Human Services mandate for use of the ICD Tenth Revision, Clinical Modification (ICD-10-CM) came into effect. The ICD codes were now incorporated into E*Value, replacing the prior system of codes organized by body system.
The ICD-10-CM includes almost 92,000 codes, including a collection related to SDH (subsection Z55 – Z65); hereafter referred to as Z-codes. These Z-codes are identified as codes for persons having potential health risks related to socioeconomic and psychosocial circumstances. Some overlap was found between the proprietary SDH codes and the newly added Z-codes. A full comparison of the proprietary SDH diagnostic does and the Z-codes is provided in Table 2. While the full ICD-10-CM was available to students, the proprietary SDH codes remained as options within E*Value. Students were free to utilize all codes.
 |
Table 2 Comparison of social determinants of health (SDH) codes and ICD 10-CM Z-codes |
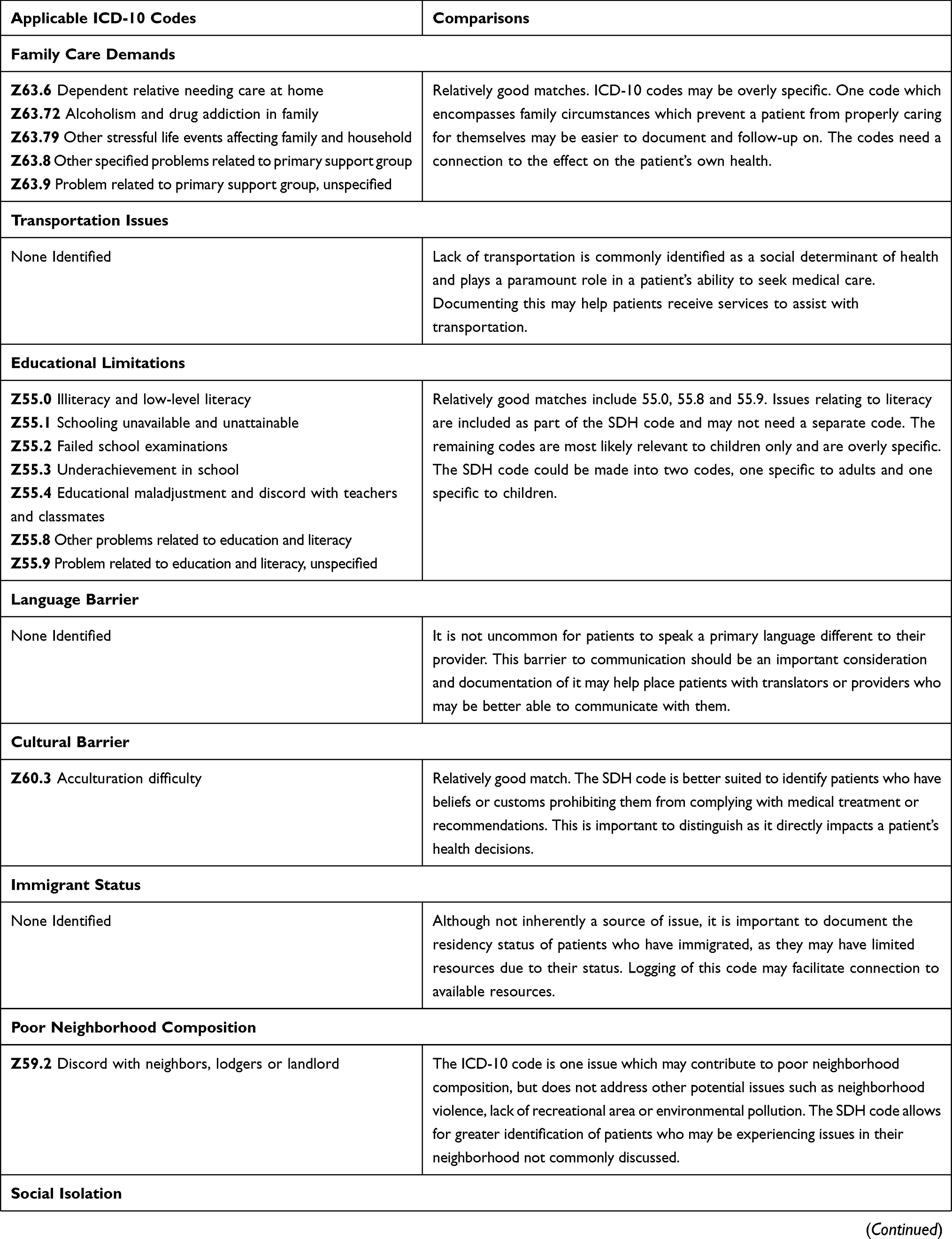 |
Table 2 (Continued). |
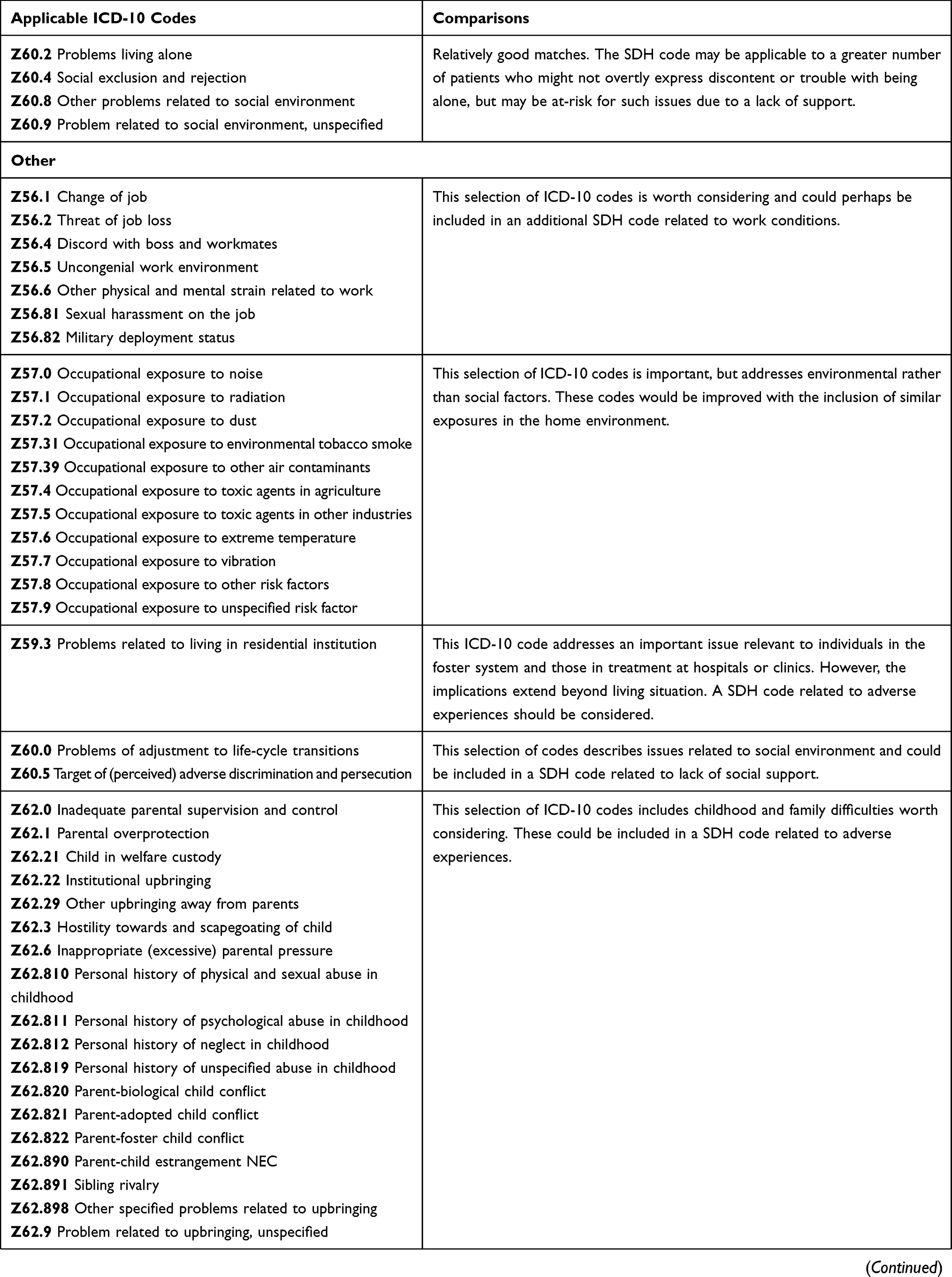 |
Table 2 (Continued). |
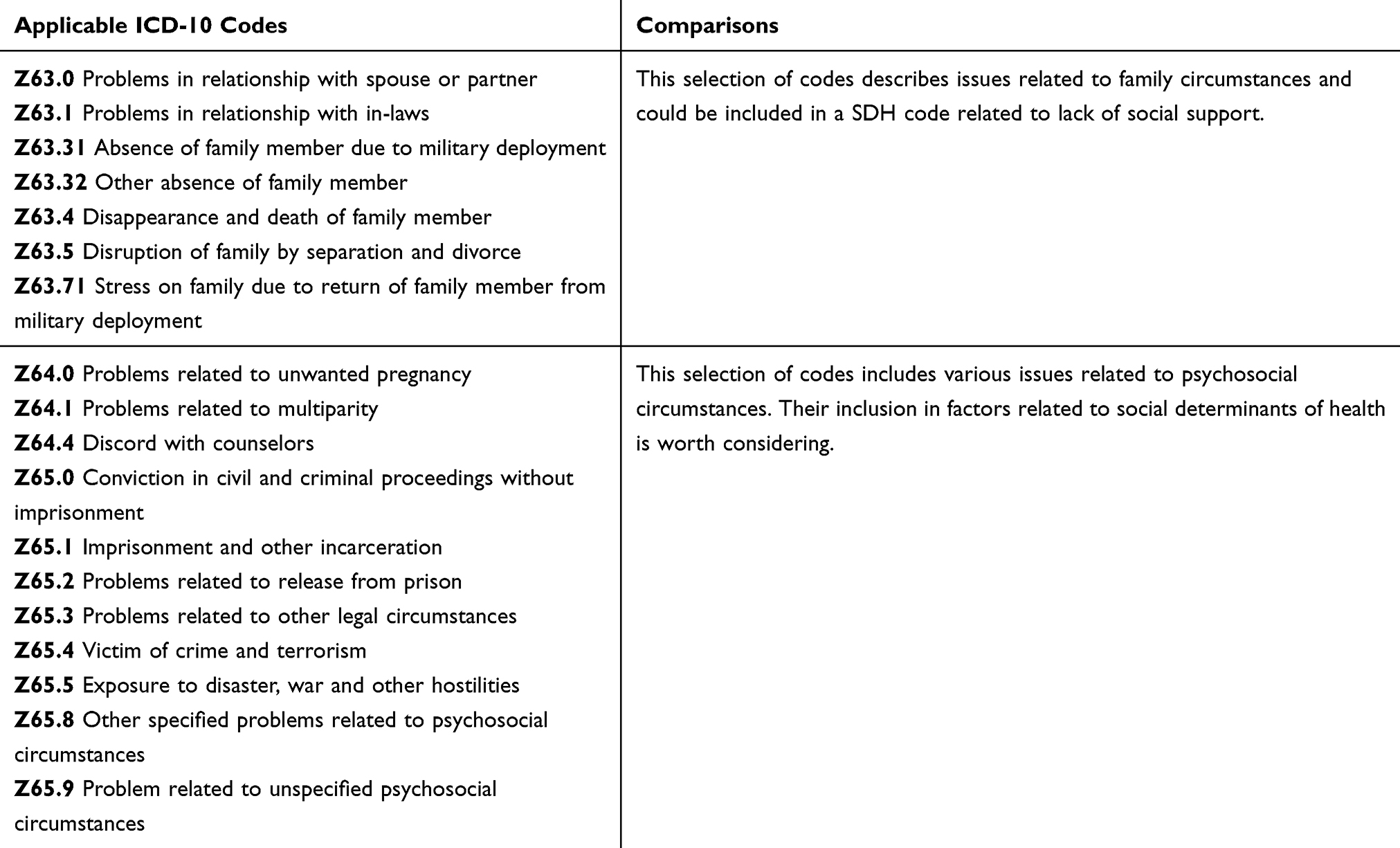 |
Table 2 (Continued). |
Measures
The first evaluation question was measured by tallying the total number of codes (any) reported on E*Value by 2nd, 3rd and 4th year students and how often they utilized SDH codes. The remaining evaluation questions were measured through a survey that was administered twice, first at the end of PY1 and again at the end of PY2.
After PY1, students in academic years 2, 3 and 4 (Classes of 2018, 2017 and 2016, respectively) had accessed the proprietary codes and were able to utilize them during clinical experiences. They were surveyed on their experience using the codes and their perceptions of the importance of SDH and the need for documenting them in the medical record.
Students in their first academic year (Class of 2019) were surveyed prior to their introduction to the codes and starting their clinical experience. This class was asked similar questions about their perceptions of the importance of SDH and addressing them during clinical encounters. This survey was used as a baseline to identify their perceptions prior to utilizing SDH codes, which could be used to compare any changes after each year of use.
The same survey was administered similarly in PY2; this time to the classes of 2017, 2018, 2019, and 2020. Students in the classes of 2018 and 2017, now 3rd and 4th year students, were responding based on 2 years of using the proprietary codes. Students in the class of 2019, 2nd years, were responding based on their first year of using the codes. As in PY1, the class of 2020 (1st year) was surveyed as a baseline measure.
Results were reported by project year and item response using descriptive statistics in order to show differences in frequency or proportion of response change over the project period.
Results
Use of codes
Table 3 shows the frequency of students logging proprietary SDH codes over the 2 project years with the addition of Z-codes in PY2. During PY1, 193 individual students utilized the SDH codes and logged a total of 12,765 SDH diagnoses and 5,040 procedures. All 18 diagnosis codes, and the option for “other” were logged. SDH codes accounted for 3.11% of the 410,142 diagnosis codes logged by all students.
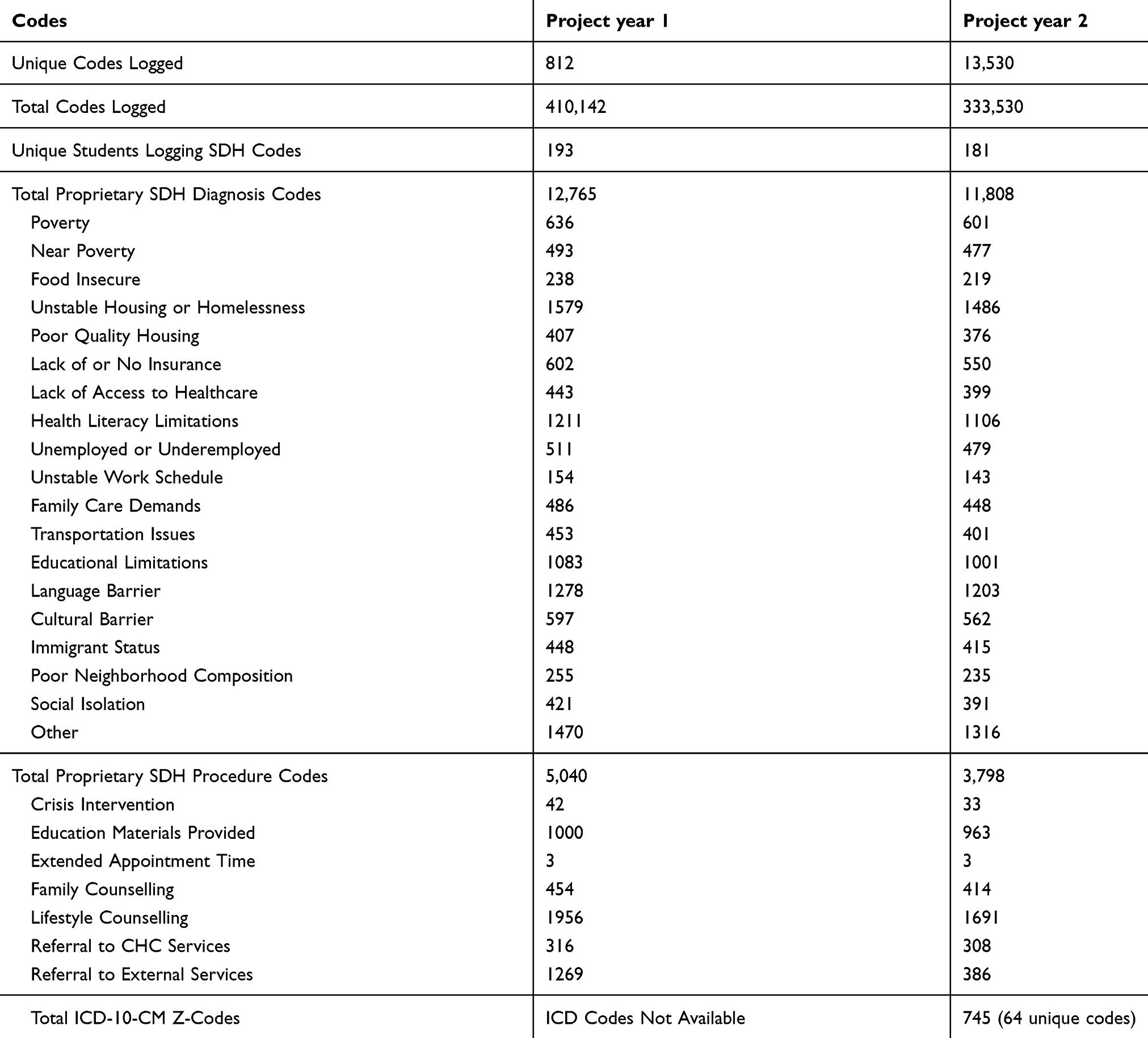 |
Table 3 Counts of all codes logged: proprietary social determinants of health (SDH) and ICD 10-CM Z-codes |
During PY2, 181 individual students utilized all SDH codes, logging a total of 11,808 diagnoses and 3,798 procedures. An additional 745 Z-codes relating to social factors were recorded. Proprietary SDH diagnosis codes accounted for 3.54% of the 333,530 diagnosis codes logged by all students. With the inclusion of Z-codes, SDH related diagnoses accounted for 3.76% of all logged codes.
Survey
At the completion of PY1, all students in each class were surveyed. A total of 318 students (73.66%) responded. Two hundred and twenty two students (51.51%) completed the survey after PY2. A complete overview of response rates is provided in Table 4.
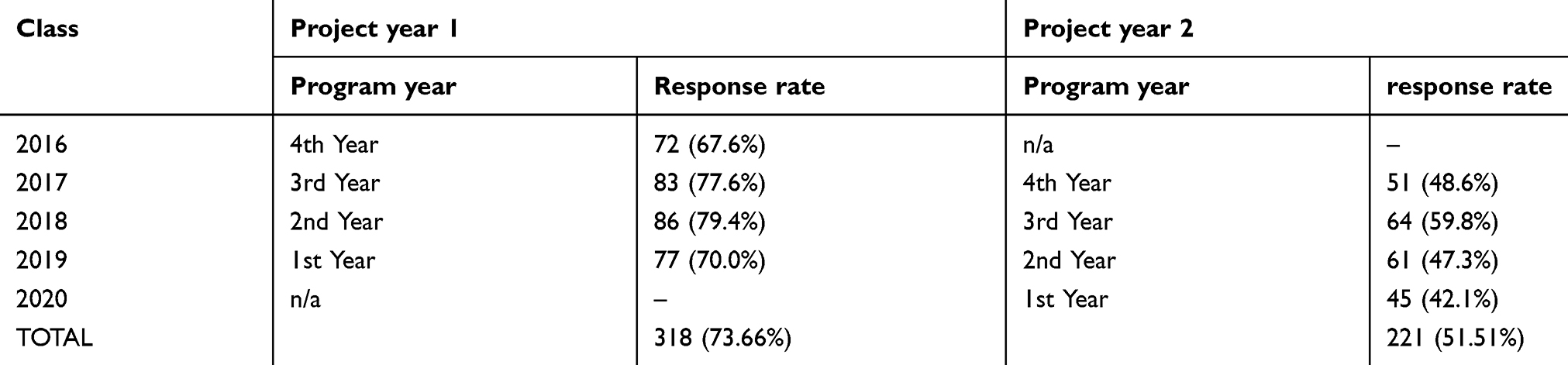 |
Table 4 Survey response rates by class and project year |
Tables 5 and 6 show results from the surveys. Table 5 presents the results for 3 survey items as the percentage of students who selected completely disagree/disagree, neutral or agree/completely agree for each.
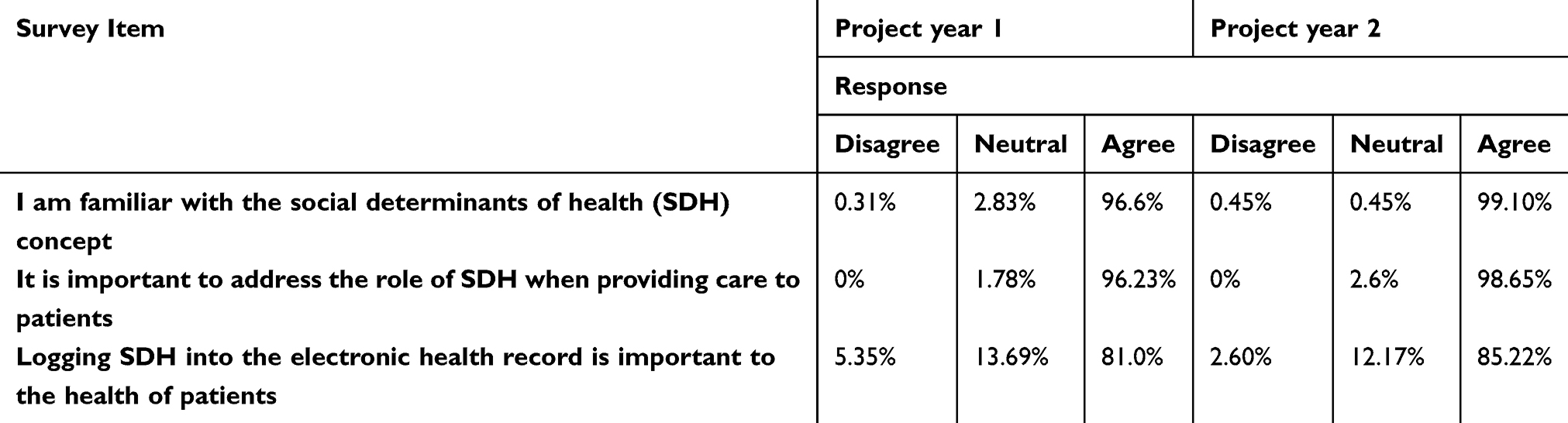 |
Table 5 Survey items and response proportions by project year |
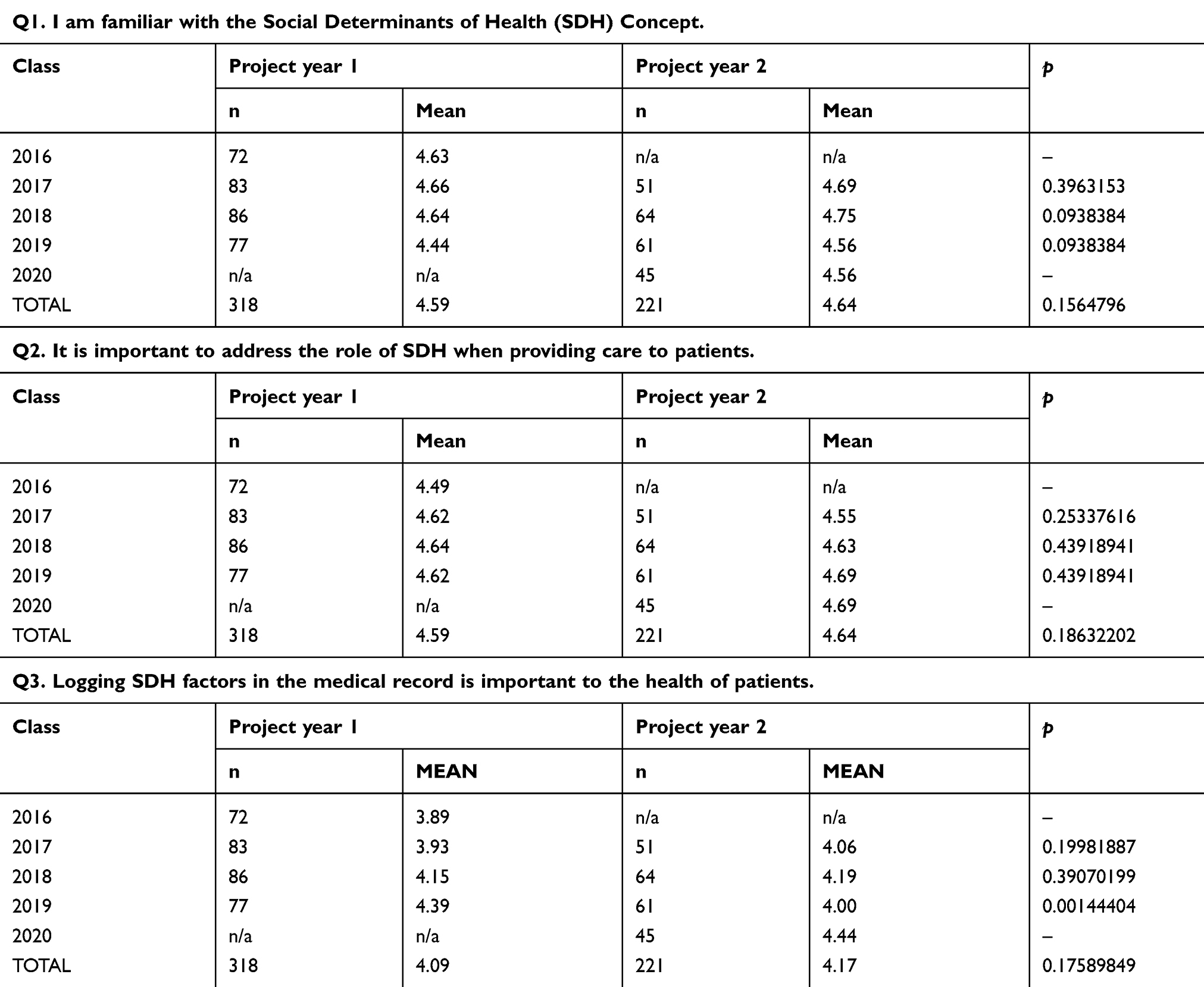 |
Table 6 Survey items and response means by class and project year |
A majority of students who responded (96.6% in PY1 and 99.1% PY2) felt that they were familiar with the concept of SDH. Additionally, the majority of responding students (96.23% in PY1 and 98.65% in PY2) felt it was important to address the role of SDH when providing care to patients. They also felt that logging SDH into EHR is important to the health of patients (81% in PY1 and 85.22% in PY2).
Table 6 presents the mean score for the same survey items, as calculated using a 1 to 5 scale (1= completely disagree, 3= neutral, 5= completely agree). The table further shows the calculated significance for the 3 survey items by class and project year and additionally, the significance for overall survey. Although the differences were not statistically significant, each item showed a slight increase in average score and the proportion of students in agreement over the 2 project years.
Results were analyzed from two open-response questions. First year students (class of 2019 in PY1 and class of 2020 in PY2) were asked if they felt it important to learn about SDH during medical education. Open-ended responses were reviewed and categorized into positive, neutral and negative responses. Percentages in each category were calculated. Forty five students from the class of 2020 responded to this question with 97.8% responding positively that they do feel it is important and 2.2% responding negatively. Similarly, 75 students from the class of 2019 responded to this question with 94.7% responding positively and 5.3% responding negatively. There were no comments categorized as neutral.
Second, third and fourth year students were all asked if they felt coding SDH was beneficial to their undergraduate medical education. For the responses to this item repeat themes were identified and condensed into summary statements. Statements representing the results for question two are presented in Table 7.
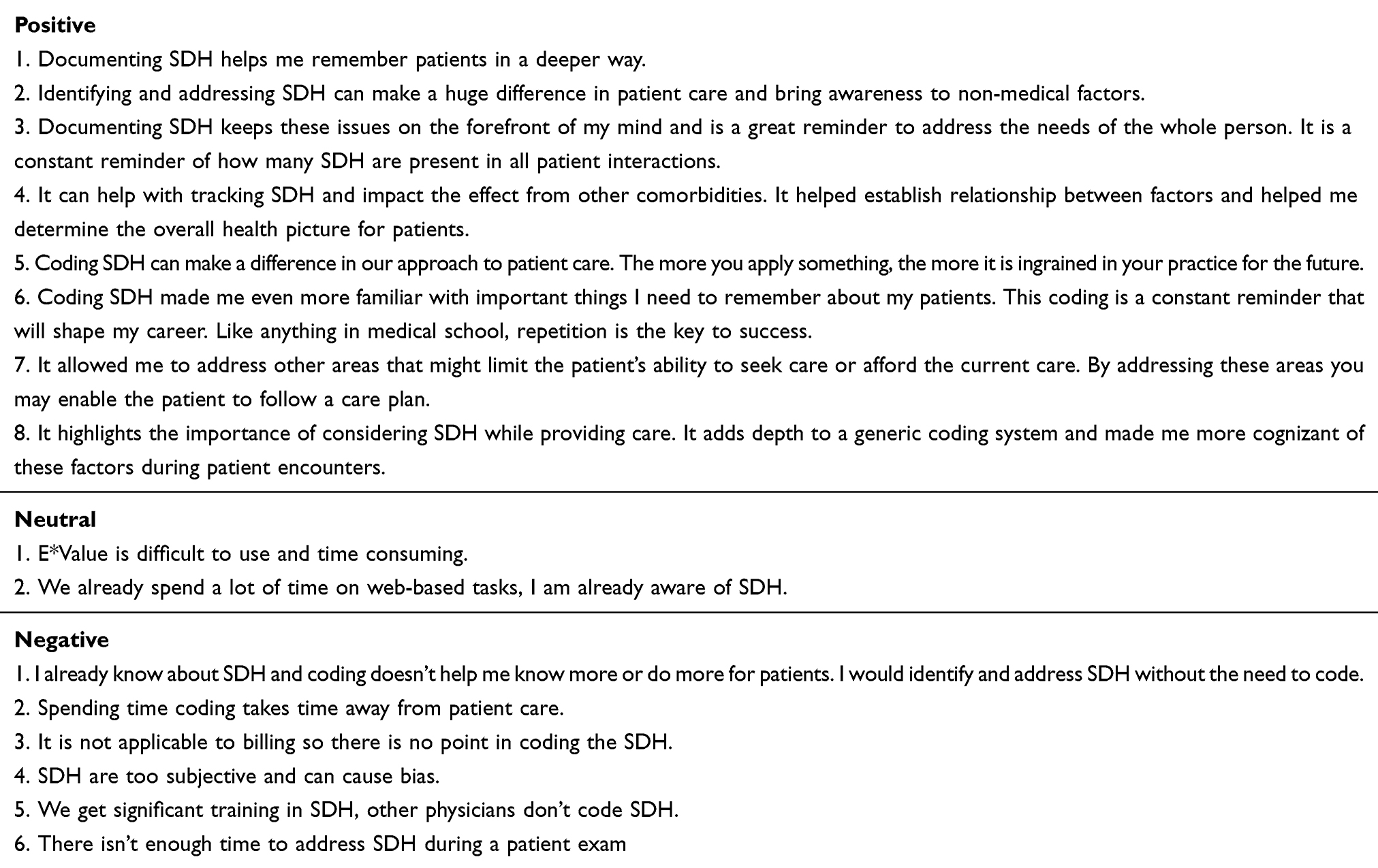 |
Table 7 Open-ended responses to the question “Do you feel the request for you to code SDH was beneficial to your undergraduate medical education?” |
Responses from second, third and fourth year students related to the benefit of coding SDH were varied. The positive comments included statements indicating that logging made a difference in patient care, helped students remember their patients better, and that the codes were a great tool to help keep SDH on the forefront of the visit. Negative comments were directed more towards external issues, rather than the use of SDH codes. Many students were frustrated with the E*Value platform, finding it to be difficult to use. Other students questioned the practice as SDH codes are not applicable to billing and most doctors they shadow do not record social factors. Some students who responded negatively to the question indicated their negative feelings were more about the requirement for them to log their patient encounters with codes and not about their feelings about the importance of identifying and addressing SDH.
Discussion
This project addresses the need to integrate SDH into medical education. This is a step towards developing best practices for utilizing EHRs to improve individual and population health and toward using SDH data to assist with clinical decision making.4
In the first project year, 870 diagnosis codes were available to students for logging clinical encounters. In year two, students had access to over 92,000 codes. Despite this increase, there was no significant change in overall representation of SDH codes recorded. Students utilized the proprietary codes more often than the Z-codes. This could be because of their familiarity with the proprietary codes, or it could be that the proprietary codes were more straight forward and relevant to the clinical encounters.
Students’ voluntary logging of SDH codes demonstrates they perceived these factors to be important. Additionally, the survey provided evidence that an overwhelming portion of ATSU SOMA students (who participated in the survey) are familiar with the SDH concept, feel that addressing SDH is important while providing care, and also feel that documenting SDH in EHRs is important to the health of patients. Modest increases in responses agreeing to items studied could be attributed to our intervention. This correlation does not imply causation. However, the combined evidence supports the fact that students value the ability to identify and address SDH. Thereby, we plan to continue to foster these beliefs in our undergraduate medical students and to continue to teach them to formally document and address SDH.
This study is limited to one learning institution, the results cannot be generalized to other education programs. These codes are one part of a curriculum with an emphasis on identifying the SDH and addressing health disparities. The proprietary codes were introduced into the curriculum before the ICD-10 codes were available. This sequence could have affected the differential use of the codes for the cohort of students who first logged patient encounters using the proprietary codes and then logged with the option of the proprietary codes and the ICD-10. However, the class of 2019 students were introduced to the proprietary codes and the ICD-10 SDH codes at the same time and showed a similar preference for the use of the proprietary codes as that shown by the other classes. There is evidence the tools we provided our students to track and quantify SDH diagnoses and procedures were well utilized and can add value to the education environment.
Table 2 should be useful for clinical educators and students to use as a reference for ICD-10 SDH coding. We provide the SDH category, relevant codes and the authors’ evaluation of how the Z-codes compare to the proprietary codes.
Future research can evaluate practicing physician’s views of the proprietary SDH codes in comparison to the Z-codes. Most importantly, students and providers of all levels could be queried to discover their perceptions of the clinical relevance of the two sets of codes and the ease of use. Additionally, future work will involve evaluating and documenting clinical practices and partnerships which can be used to address identified SDH.
Conclusion
We aim to positively affect practice culture by encouraging future providers to work towards addressing SDH and alleviating health inequities. SDH need to be included as integral parts of the health record. Only then will SDH be considered within the realm of what should be addressed by all medical providers. Coding of SDH will allow for evaluation and documentation of the significant impact of SDH on individual and population health. This can also lead to development of more mechanisms to address the SDH.
In clinical medicine, we evaluate the etiology of disease, disease characteristics, and the effects of the disease and treatment modalities. It is time to heighten the importance of SDH and to teach students how to evaluate these factors in the same manner we teach them to evaluate disease. Including SDH in the formal student documentation of medical encounters is an effective approach, easily replicable by other clinical educators.
Acknowledgments
Authors would like to acknowledge Helen Hill, DO, MPH for her inspiration for this work.
Disclosure
The authors reports no conflicts of interest in this work.
References
1. Cantor MN, Chandras R, Pulgarin C. FACETS: using open data to measure community social determinants of health. J Am Med Inf Assoc. 2018;25(4):419–422.
2. Krieger N, Waterman PD, Spasojevic J, Li W, Maduro G, Van Wye G. Public health monitoring of privilege and deprivation with the index of concentration at the extremes. Am J Public Health. 2016;106(2):256–263. doi:10.2105/AJPH.2015.302955
3. Galea S, Tracy M, Hoggatt KJ, DiMaggio C, Karpati A. Estimated deaths attributable to social factors in the United States. Am J Public Health. 2011;101(8):1456–1465. doi:10.2105/AJPH.2010.300086
4. Daniel H, Bornstein SS, Kane GC. Addressing social determinants to improve patient care and promote health equity: an American College of physicians position paper. Ann Intern Med. 2018;168(8):577–578. doi:10.7326/M17-2441
5. Sharma M, Pinto AD, Kumagai AK. Teaching the social determinants of health: a path to equity or a road to nowhere? Acad Med. 2018;93(1):25–30. doi:10.1097/ACM.0000000000001689
6. Siegel J, Coleman DL, James T. Integrating social determinants of health into graduate medical education: a call for action. Academic Medicine. 2018;93(2):159–162. doi:10.1097/ACM.0000000000002054
7. Nancy EA, William WS. Patients in context — EHR capture of social and behavioral determinants of health. N Engl J Med. 2015;372(8):698–701.
8. Gottlieb LM, Tirozzi KJ, Manchanda R, Burns AR, Sandel MT. Moving electronic medical records upstream: incorporating social determinants of health. Am J Prev Med. 2015;48(2):215–218. doi:10.1016/j.amepre.2014.07.009
9. Welcher CM, Hersh W, Takesue B, Stagg Elliott V, Hawkins RE. Barriers to medical students’ electronic health record access can impede their preparedness for practice. Academic Medicine. 2018;93(1):48–53. doi:10.1097/ACM.0000000000001829
10. O’Brien MJ, Garland JM, Murphy KM, Shuman SJ, Whitaker RC, Larson SC. Training medical students in the social determinants of health: the health scholars program at puentes de salud. Adv Med Educ Pract. 2014;5:307. doi:10.2147/AMEP.S67480
11. Ambrose AJH, Andaya JM, Yamada S, Maskarinec GG. Social justice in medical education: strengths and challenges of a student-driven social justice curriculum. Hawai’i J Med Publ Health. 2014;73(8):244.
12. Rooks RN, Rael CT. Enhancing curriculum through service learning in the social determinants of health course. J Scholarship Teach Learn. 2013;13(2):84–100.
13. Bada SO, Olusegun S. Constructivism learning theory: a paradigm for teaching and learning. J Res Method Educ. 2015;5(6):66–70.
14. Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records; Board on Population Health and Public Health Practice; Institute of Medicine. Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2. Washington, DC: National Academies Press; 2015.ISBN-10:0-309-31242-6
15. Office of Disease Prevention and Health Promotion. Social Determinants of Health. 2020 Topics & Objectives; 2016. Avaialable from: healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health.
16. WHO. Social Determinants of Health. 2016. Avaialable from: http://www.who.int/topics/social_determinants/en/.
17. Lewis JH, Whelihan K, Navarro I, Boyle KR. Community health center provider ability to identify, treat and account for the social determinants of health: a card study. BMC Fam Pract. 2016;17(1):121. doi:10.1186/s12875-016-0526-8
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.