Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Tarsus-Orbicularis-Septum Fixation in Double-Eyelid Blepharoplasty: A Reliable and Flexible Technique
Authors Sun Y, Liu R, Yu N, Zhang D, Chen J, Huang J, Long X
Received 24 March 2022
Accepted for publication 9 June 2022
Published 21 June 2022 Volume 2022:15 Pages 1125—1132
DOI https://doi.org/10.2147/CCID.S367202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Video abstract of "TOS Fixation in Double-Eyelid Blepharoplasty" [ID 367202].
Views: 306
Yixin Sun,1,* Runzhu Liu,1,* Nanze Yu,1 Dingyue Zhang,2 Juan Chen,3 Jiuzuo Huang,1 Xiao Long1
1Division of Plastic Surgery, Department of Surgery, Peking Union Medical College Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Clinical Medicine, Peking Union Medical College & Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 3Institute of Medical Information/Medical Library, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiuzuo Huang; Xiao Long, Division of Plastic Surgery, Department of Surgery, Peking Union Medical College Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, No. 1, Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel/Fax +86-1069158730, Email [email protected]; [email protected]
Purpose: Incisional double eyelid blepharoplasty is the most common cosmetic operation in East Asia. Although numerous articles on surgical techniques have been published, complications, such as fold loss, asymmetry, and visible scars, still exist. To create a stable and dynamic double-eyelid crease, the author has introduced a modified technique of double-eyelid blepharoplasty.
Patients and Methods: The authors introduced a new surgical technique to reduce complications and create reliable and dynamic double eyelids. The orbicularis oculi muscle of the lower flap was anchored on the tarsus and sutured with the distal part of the septal flap. The skin incision was closed by skin–septal flap–skin suture. Postoperative evaluations were assessed at the twelfth postoperative month.
Results: One hundred ninety-three patients underwent double eyelidplasty with the TOS fixation technique. The mean follow-up duration was 18.6 months (range, 12– 30 months). In the aesthetic outcome evaluation, 88 (45.6%) patients had very much improved results, 56 (29.0%) had much improved results, 29 (15.0%) had improved results, 8 (4.1%) had no change and 12 (6.2%) had worse results. Complications included crease asymmetry (n=7, 3.6%), partial fold loss (n=8, 4.1%) and complete fold loss (n =5, 2.6%).
Conclusion: Tarsus-orbicularis-septum (TOS) fixation is a reliable and flexible surgical technique for creating stable and dynamic double-eyelid creases.
Keywords: double eyelidplasty, primarily blepharoplasty, orbital septum, tarsus
Introduction
As one of the most important aesthetic units in the face, eyes with fine-defined upper lid creases can visually enlarge palpebral fissures and increase facial attractiveness.1 However, almost half of individuals of East Asian descent do not own this crease.2 Among those with a single eyelid, epicanthus and ptosis are also common, which make the palpebral fissure look narrower. For these reasons, double eyelidplasty has been the most common aesthetic operation in East Asia.3
The ideal outcome after double eyelidplasty is creating a long-lasting dynamic upper eyelid fold with suitable height and depth without a visible scar or hollow appearance when the eyes are closed or gazing down.4 Compared with nonincisional techniques, incisional double eyelid blepharoplasty is more widely performed. The classic incisional technique involves overresection of pretarsal tissue and dermis-tarsus fixation, which usually creates a static fold.4,5 The features of a static fold include deep fold formation when the eye is open and a still, sunken line in the previous incision when the eye is closed or looking downward.3 Dynamic double eyelids can be created with flexible tissues such as orbicularis-levator fixation,6 septoaponeurosis junctional thickening (SAJT),3 and septal extension.7 However, certain complications still exist, such as fold loss or asymmetry. To achieve a more reliable and dynamic outcome, a novel approach called tarsus-orbicularis-septum (TOS) fixation was proposed.
Materials and Methods
A total of 193 patients underwent double-eyelid blepharoplasty from February 2018 to January 2021. The patients were aged 18–45 years with an average age of 22.3 years. This study adhered to the tenets of the Declaration of Helsinki and was approved by the institutional ethical committee. All participants signed informed consent form.
Preoperative Design
A preoperative marking line was drawn based on the patient’s preference and the surgeon’s experience. Generally, the distance between the incisional line and ciliary margin at the midpapillary point was 6–8 mm for women and 4–6 mm for men.
A pair of forceps were used to clamp the skin above the marking line. When the upper eyelid skin was tight and the eyelash began to move, the upper incision line was determined. Because gravity can change the eyelid skin distribution, it was important to make necessary adjustments with the patients in a sitting position.
Anesthesia, Incision and Dissection
Local anesthesia was completed with 2% lidocaine and 1:100,000 epinephrine. A strip of skin was excised along the preoperative marking lines. A small strip of orbicularis oculi muscle above the upper border of the lower flap was trimmed. The orbital septum was transversely opened from the lateral to medial direction, resulting in herniation of preaponeurotic fat (Figure 1). Redundant preaponeurotic fat was conservatively removed. Care must be taken to not remove too much fat, otherwise it is easy to show a sunken appearance or multiple creases postoperatively. Meticulous hemostasis was achieved with bipolar electrocoagulation during the operation to minimize postoperative edema.
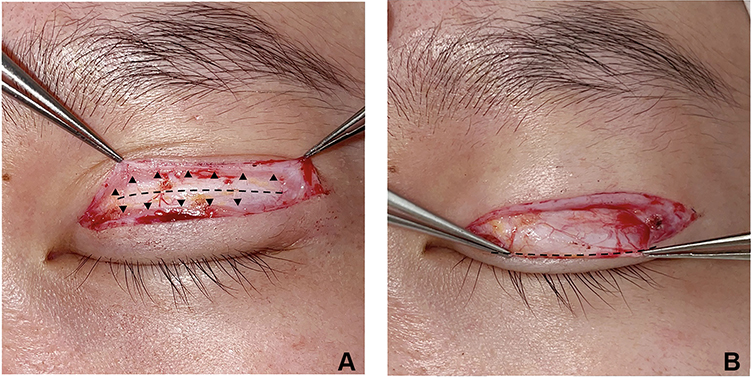 |
Figure 1 Open the orbital septum. (A) Exposing the orbital septum. The upper and lower black triangles show the orbicularis oculi muscle of the upper flap and lower flap, respectively. The whitish tissue underlying the middle black dotted line is the untapped orbital septum. (B) Opening the orbital septum. The tissue held by the forceps is the downward-turned distal septal flap, the edge of which is shown by the black dotted line. |
TOS Fixation
After grabbing the pretarsal fascia and superficial tarsal plate with forceps, the upper eyelid could be firmly elevated. Then, 7–0 nylon suture was used to pass through the pretarsal fascia and partial thickness of the tarsal plate. The second bite passed through the orbicularis oculi muscle of the lower flap, and the third bite passed through the distal part of the septal flap (Figures 2 and 3). The suture usually started from the mid-pupillary point, followed by the lateral and medial points. TOS fixation was made at 3–5 points. During the operation, it is important to ensure that the suture does not pass through the full thickness of the tarsus to prevent corneal injury.
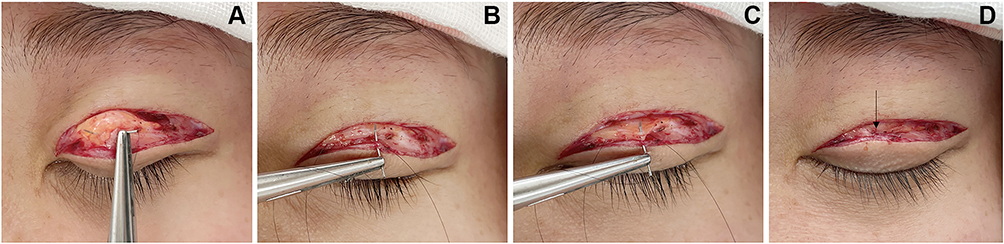 |
Figure 2 TOS fixation. (A) The first bite is in the pretarsal tissue and superficial tarsus. (B) The second bite is in the orbicularis oculi muscle of the lower flap. (C) The third bite is in the downward turned orbital septum. (D) The black arrow shows the stitch position for the TOS fixation. |
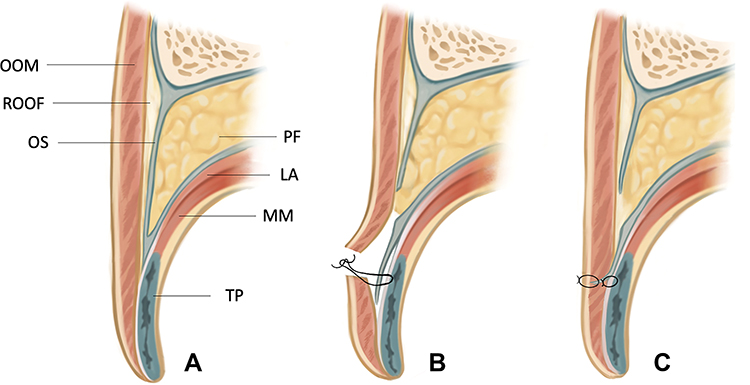 |
Figure 3 Schematic illustration of TOS technique. (A) Normal upper eyelid anatomy. (B) TOS fixation. The OOM of the lower flap is sutured to the pretarsal fascia and partial thickness of the tarsal plate and then sutured with the downward-turned distal septal flap. (C) Incision closure. The skin incision was closed by skin-orbital septum-skin sutures to facilitate double-eyelid crease formation. Abbreviations: OOM, orbicularis oculi muscle; ROOF, retro-orbicularis oculi fat; OS, orbital septum; PF, preaponeurotic fat; LA, levator aponeurosis; MM, Mu ̈ller’s muscle; TP, tarsal plate. |
Skin Suture
Since the downward-turned orbital septum had been fixed with the pretarsal tissue and superficial tarsus at 3–5 points, the orbital septum could be sutured with skin to facilitate double eyelid formation. Three to five skin-septum-skin sutures were usually performed. The patients were asked to open and close their eyes in a sitting position, and necessary adjustments were made. Skin closure was then performed with interrupted 7–0 nylon sutures (Figure 3).
Postoperative Care
After thin antibiotic ointment application, the incision was covered with sterile gauze for 24 hours. For the first 48 hours, intermittent cool compression with ice packs was helpful to reduce swelling. Suture removal was performed on the fifth to seventh postoperative day.
Outcome Evaluation
Efficacy evaluation was accomplished by the patients at the twelfth postoperative month based on the Global Aesthetic Improvement Scale.7 The results were classified into five levels: worse, no change, improved, much improved, and very much improved. Complications such as scar formation, asymmetric or multiple folds, partial and complete fold loss, and sunken upper eyelid were recorded as well.
Results
A total of 179 females and 14 males with a single eyelid received double-eyelid blepharoplasty with TOS fixation. All the patients were primary cases. Patients diagnosed with blepharoptosis were excluded. The follow-up period ranged between 12 months and 30 months, with a mean duration of 18.6 months. Twenty-four patients with epicanthus simultaneously underwent epicanthoplasty. Typical cases are presented in Figures 4–6.
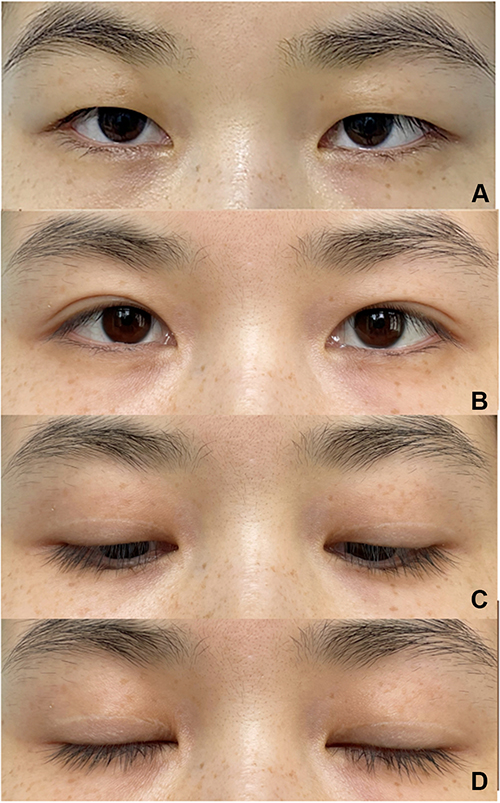 |
Figure 4 Patient 1. (A) Preoperative view of a 28-year-old female with puffy upper eyelids who underwent double-eyelid blepharoplasty with TOS fixation. Postoperative views at twelfth month with her eyes open (B), eyes gazing downward (C), and eyes closed (D). |
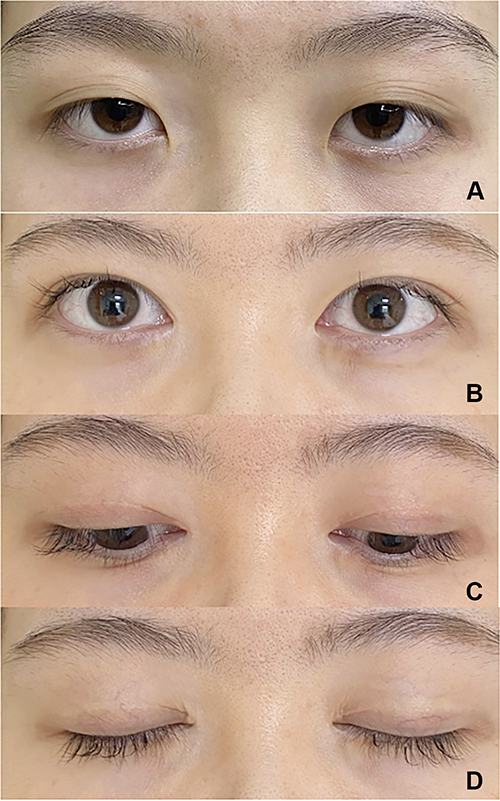 |
Figure 5 Patient 2. (A) Preoperative view of a 22-year-old female who underwent double-eyelid blepharoplasty with TOS fixation and epicanthoplasty. Postoperative views at twelfth month with her eyes open (B), eyes gazing downward (C), and eyes closed (D). |
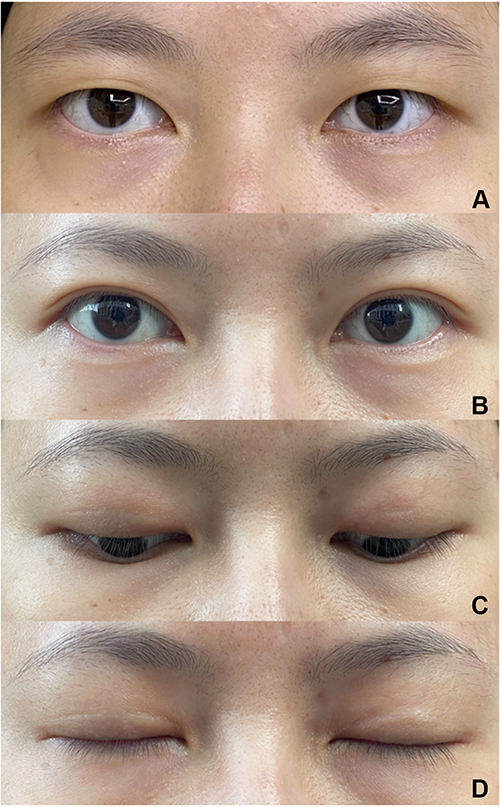 |
Figure 6 Patient 3. (A) Preoperative view of a 25-year-old female who underwent double-eyelid blepharoplasty with TOS fixation. Postoperative views at eighteenth month with her eyes open (B), eyes gazing downward (C), and eyes closed (D). |
The postoperative evaluation received from the patients showed that 88 (45.6%) patients had very much improved results, 56 (29.0%) had much improved results, 29 (15.0%) had improved results, 8 (4.1%) had no change and 12 (6.2%) had worse results. Complications recorded during the follow-up included fold asymmetry (n=7, 3.6%), partial double-eyelid crease loss (n=8, 4.1%) and complete double-eyelid crease loss (n=3, 1.6%). All these patients underwent revision surgery and were satisfied with the results. There were no depressed scars or sunken eyelids reported.
Discussion
An obvious supratarsal crease is often regarded as an ethnic identity of Caucasians. The characteristic of Asian upper lids is a single eyelid or a very low crease appearing droopy.8 The anatomical differences between Caucasians and Asians are as follows:9 (1) There is a firm connection between the orbicularis oculi muscle and levator aponeurosis in Caucasians; however, in Asians, subcutaneous and retro-orbicularis oculus fat is abundant, thereby interrupting the insertion of levator tissue into the orbicularis oculi muscle and subdermal tissue. (2) In Caucasian double eyelids, the levator aponeurosis is found to fuse with the orbital septum above the supratarsal margin; however, the fusion level of the levator aponeurosis and the orbital septum is below the upper border of the tarsus in Asians and sometimes near the lower margin of the eyelid. This situation makes the orbital fat extend nearer to the eyelid edge, limiting the attachment between the levator tissue and the subdermal tissue. The primary mechanism of double eyelid blepharoplasty is to mimic the physiological anatomy of people with congenital double eyelids. For these reasons, building reliable adhesion between the posterior lamella and the anterior lamella is the key point of double eyelidplasty. An ideal procedure should create reliable and dynamic double eyelids with minimal invasiveness.
Fixation to the tarsus is important for double-eyelid blepharoplasty, as it creates reliable results. Since the classic tarsal fixation technique involves skin-tarsus-skin fixation, it is reliable.10 However, too much resection of pretarsal tissue can cause a depressed scar and a static fold, which need revision.4 A modified technique called the orbicularis-tarsus fixation approach was proposed, which was similar to the classic method, but the pretarsal fascia and pretarsal orbicularis oculi muscle are preserved.11
To create a dynamic fold, flexible connecting tissue is of great importance. In 1999, Park proposed levator aponeurosis-orbicularis muscle fixation to create a dynamic fold.8 Crease fixation with flexible connecting tissue (including levator aponeurosis and other related tissue) has been widely performed, and many modifications have been published, such as the septo-aponeurosis junctional thickening (SAJT) to dermis technique,3 pretarsal levator aponeurosis flap technique (in which the pretarsal levator aponeurosis flap is dissected and sutured with upper eyelid skin),12 orbital septal flap technique13 (in which the distal part of the septal flap is sutured with the pretarsal fascia and the lower flap), flexible suspension technique7 (in which the lower flap is fixed with the septal extension), hinge technique14 (in which the orbital septal flap is fixed to the pretarsal dermis), and kiss technique15 (in which the orbicularis oculi muscle and ROOF of the lower flap is sutured with white line). The aforementioned techniques transmit the force of the levator aponeurosis to the upper eyelid skin and create a dynamic fold. However, without tarsal fixation, the results of these techniques with flexible connecting tissues are not reliable, and complications such as partial fold loss and complete fold loss occur.
Several techniques have been reported that utilize both tarsal fixation and flexible connecting tissue, including the pretarsal levator mini-flap technique16 (in which several mini-flaps derived from pretarsal levator aponeurosis are fixed with the tarsus and the lower flap) and bridge technique17 (in which a levator aponeurosis-orbital septum flap is fixed with the tarsal plate and the lower flap). Although these techniques could produce reliable and flexible results, the pretarsal levator should be dissected from the tarsus, which is relatively invasive and technically demanding. It is also possible to damage the levator aponeurosis during pretarsal levator dissection, causing iatrogenic blepharoptosis.
To make good use of tarsal fixation and flexible connecting tissue, as well as minimize damage to the pretarsal levator aponeurosis, a new technique called tarsus-orbicularis-septum (TOS) fixation was proposed. There are several advantages of the TOS technique. First, there is no dissection of the pretarsal levator aponeurosis, so the damage is less than that with the mini-flap16 and bridge techniques.17 Second, tarsal fixation is performed, which is more reliable than fixation techniques with only flexible connecting tissue. Third, the septal flap was utilized as flexible connecting tissue to create dynamic double-eyelid folds.
Certain key points should be taken into consideration when performing TOS fixation blepharoplasty. The first key point is related to the management of pretarsal tissue. For most of the patients without pretarsal tissue hypertrophy, the pretarsal tissue and the superficial tarsus could be fixed together with 7–0 nylon. However, for patients with bulky pretarsal tissue, it is difficult to perform tarsal fixation. In this case, small pretarsal holes were created to expose the pretarsal levator aponeurosis, which facilitated tarsal fixation.18
The second key point is manipulation of the septal flap. After the transverse dissection, the distal part of the septal flap was turned downward using SAJT as a pedicle. The orbital septal flap was then fixed with the tarsus and the lower flap, so the orbital septal flap was tightly connected to the levator aponeurosis, making it the flexible connecting tissue.
The third key point is the skin-septal flap-skin suturing. After this layer of suture, the septal flap could act as flexible connecting tissue, which transmits the power of the levator aponeurosis to the skin, contributing to the formation of a double-eyelid crease. Since the tarsus was changed into supporting ligaments at both the lateral and medial canthi, the lower flap could not be effectively fixed with the tarsus directly. However, there is orbital septum at both the lateral and medial canthi. Since the downward-turned orbital septum had been fixed with the pretarsal tissue and superficial tarsus, the orbital septal flap could be sutured with the skin at both the medial and lateral canthi to facilitate double-eyelid formation.
Several limitations exist in this study. First, this study was conducted retrospectively. A prospective trial is required to demonstrate the effect of this technique in the future. Second, a control group is absent in this study. It would be better to conduct a randomized controlled study to compare the postoperative evaluation and complication rate with other techniques. Third, an objective measurable assessment was not performed to evaluate the outcome of the TOS fixation, which might lead to some subjective bias.
Conclusion
Tarsus-orbicularis-septum (TOS) fixation is a reliable and flexible surgical technique for creating stable and dynamic double-eyelid creases.
Data Sharing Statement
There is no additional unpublished data from this study.
Ethical Approval and Informed Consent
This study was in accordance with the ethical standards formulated in the Declaration of Helsinki. This study was approved by the Research Ethics Board of Peking Union Medical College Hospital. Informed consent was obtained from all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This manuscript is funded by the CAMS Innovation Fund for Medical Sciences (CIFMS), No. 2020-I2M-C&T-A-004 and the National Key R&D Program of China, Key Project of the Strategic International Science and Technology Innovation Cooperation, Ministry of Science and Technology, grant No. 2020YFE0201600.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hwang HS, Spiegel JH. The effect of “single” vs “double” eyelids on the perceived attractiveness of Chinese women. Aesthet Surg J. 2014;34(3):374–382. doi:10.1177/1090820X14523020
2. McCurdy JA. Upper lid blepharoplasty in the Oriental eye. Facial Plast Surg. 1994;10(1):53–66. doi:10.1055/s-2008-1064556
3. Kim HS, Hwang K, Kim CK, Kim KK. Double-eyelid surgery using septoaponeurosis junctional thickening results in dynamic fold in asians. Plast Reconstr Surg Glob Open. 2013;1(2):1–9. doi:10.1097/GOX.0b013e318293dc69
4. Huang J, Feng S, Dong R, et al. Secondary upper blepharoplasty: converting static folds into dynamic folds. Aesthetic Surgery Journal. 2021;41(5):NP188–NP195. doi:10.1093/asj/sjaa334
5. Boo-Chai K. Plastic construction of the superior palpebral fold. Plast Reconstr Surg. 1963;31:74–78. doi:10.1097/00006534-196301000-00010
6. Park JI, Park MS. Double-eyelid operation: orbicularis oculi-levator aponeurosis fixation technique. Facial Plast Surg Clin North Am. 2007;15(3):315–26, vi. doi:10.1016/j.fsc.2007.04.002
7. Pan L, Sun Y, Yan S, et al. A flexible suspension technique of blepharoplasty: clinical application and comparison with traditional technique. Aesthetic Plast Surg. 2019;43(2):404–411. doi:10.1007/s00266-019-01317-5
8. Park JI. Orbicularis-levator fixation in double-eyelid operation. Arch Facial Plast Surg. 1999;1(2):
9. Jeong S, Lemke BN, Dortzbach RK, Park YG, Kang HK. The Asian upper eyelid: an anatomical study with comparison to the Caucasian eyelid. Arch Ophthalmol. 1999;117(7):907–912. doi:10.1001/archopht.117.7.907
10. Sayoc BT. Plastic construction of the superior palpebral fold. Am J Ophthalmol. 1954;38(4):556–559. doi:10.1016/0002-9394(54)90707-2
11. Sun W, Wang Y, Song T, Wu D, Li H, Yin N. Orbicularis-tarsus fixation approach in double-eyelid blepharoplasty: a modification of park’s technique. Aesthetic Plast Surg. 2018;42(6):1582–1590. doi:10.1007/s00266-018-1218-7
12. Lu L, Zhu M, Luo X, et al. Using levator aponeurosis to create physiologically natural double eyelid: a new reconstruction technique based on three key factors in double eyelid formation. Ann Plast Surg. 2017;78(5):487–491. doi:10.1097/SAP.0000000000000951
13. Li G, Ding W, Tan J, et al. Method for double-eyelid blepharoplasty using orbital septum. Ann Plast Surg. 2018;81(6):633–636. doi:10.1097/SAP.0000000000001650
14. Wong CH, Hsieh MKH, Wei FC. Asian upper blepharoplasty with the hinge technique. Aesthetic Plast Surg. 2022;3:1–9.
15. Zhou X, Wang H. Orbicularis-white line fixation in asian blepharoplasty: kiss technique. Aesthetic Plast Surg. 2019;43(6):1553–1560. doi:10.1007/s00266-019-01454-x
16. Choi Y, Eo S. A new crease fixation technique for double eyelidplasty using mini-flaps derived from pretarsal levator tissues. Plast Reconstr Surg. 2010;126(3):1048–1057. doi:10.1097/PRS.0b013e3181e3b72a
17. Jin R, Shen Y, Yu W, et al. Tarsal-fixation with aponeurotic flap linkage in blepharoplasty: bridge technique. Aesthet Surg J. 2020;40(12):Np648–np654. doi:10.1093/asj/sjaa195
18. Huang J, Feng Y, Li Z, et al. Double-eyelid blepharoplasty: dermis-outer orbicularis fascia-orbicularis-levator fixation technique with preorbicular venous network preservation. Aesthetic Plast Surg. 2021;46:231–236. doi:10.1007/s00266-021-02627-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.