Back to Journals » ImmunoTargets and Therapy » Volume 15
Targeting BLyS and APRIL with Telitacicept versus Conventional Immunotherapy in Generalized Myasthenia Gravis: A Comparative Study
Authors Yang Y, Kang N, Zhu Y, Ma C, Zhu R
Received 11 April 2026
Accepted for publication 19 June 2026
Published 15 July 2026 Volume 2026:15 616114
DOI https://doi.org/10.2147/ITT.S616114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jadwiga Jablonska
Yingying Yang,1– 3,* Nan Kang,1– 3,* Ying Zhu,1– 3 Chi Ma,1– 3 Ruixia Zhu1– 3
1Department of Neurology, The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China; 2Key Laboratory of Neurological Disease Big Data of Liaoning Province, Shenyang, People’s Republic of China; 3Shenyang Clinical Medical Research Center for Difficult and Serious Diseases of the Nervous System, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruixia Zhu, Email [email protected]
Background: Telitacicept is approved for acetylcholine receptor antibody-positive generalized myasthenia gravis (AChR-Ab+ gMG) in China. Although clinical trials have demonstrated its efficacy, real-world outcomes and safety require validation. This study compared telitacicept with conventional immunotherapy in a broader AChR-Ab+ GMG population, bridging the gap between RCT data and real-world practice.
Methods: This retrospective real-world study (ChiCTR2500109279) included 215 patients with AChR-Ab+ gMG, with 43 receiving telitacicept and 172 undergoing conventional immunotherapy. Propensity score matching (1:1) yielded 35 patients per group. Treatment response was assessed by changes in Quantitative Myasthenia Gravis (QMG) and Myasthenia Gravis Activities of Daily Living (ADL) scores, time to minimal symptom expression (MSE), and prednisone use.
Results: At week 4, the telitacicept group showed greater improvements than the control group in both QMG and ADL scores (QMG: 3.63± 1.48 vs 0.37± 2.76, p< 0.001; ADL: 2.80± 1.13 vs 0.46± 2.44, p< 0.001). These benefits were more pronounced at week 24 and sustained throughout follow-up (QMG: 10.30± 4.19 vs 2.86± 3.21, p< 0.001; ADL: 8.06± 3.37 vs 2.63± 2.07, p< 0.001). The telitacicept group also reached MSE earlier (median 5 months) and had more patients achieving MSE by week 24 (57.1% vs 11.4%, p< 0.001), with lower cumulative prednisone doses over 24 weeks (2325 mg vs 6525 mg, p< 0.001). A progressive decrease in IgM/IgG ratio was observed during treatment. Telitacicept was well-tolerated with no serious adverse events.
Conclusion: This real-world study demonstrates that telitacicept effectively improves symptoms and maintains stability in AChR Ab+ gMG patients, with faster onset, reduced corticosteroid dependence, and favorable safety versus conventional immunotherapy.
Keywords: generalized myasthenia gravis, telitacicept, anti-acetylcholine receptor antibody, B cells, conventional immunotherapy
Introduction
Myasthenia gravis (MG) is an autoimmune disorder mainly caused by acetylcholine receptor antibodies (AChR-Ab) that disrupt neuromuscular transmission, leading to skeletal muscle weakness and fatigability.1 These antibodies predominantly affect ocular, respiratory, and limb muscles, severely impairing patients’ quality of life. Current treatments include acetylcholinesterase inhibitors for symptomatic relief, thymectomy, and immunosuppressive therapies such as corticosteroids (CS) or non-steroidal immunosuppressive drugs (NSISTs). However, these approaches often exhibit limited efficacy, slow onset of action, and adverse effects. Notably, data from the Myasthenia Gravis Patient Registry reveal that 50% of patients maintained high Myasthenia Gravis Activities of Daily Living (MG-ADL) scores (≥6) after 12 months of treatment.2 Thus, there is a pressing need for therapies that offer rapid, durable efficacy with reduced steroid dependence.
Emerging targeted therapies, such as complement inhibitors and neonatal Fc receptor (FcRn) antagonists, act on downstream pathways and provide rapid symptom relief. However, their effects are short-lived, often requiring repeated administration or adjunct immunosuppressive therapy to prevent symptom recurrence.3–5 Recent research by the Ramirez-Valle team introduced a “sequential immunotherapy” framework aimed at achieving long-term disease control, which involves three key steps: controlling inflammation, resetting the immune system through elimination of pathogenic memory cells, and maintaining immune homeostasis.6 Therefore, deleting pathogenic immune cells is equally important.
B cells play a central role in the pathogenesis of MG, not only by producing pathogenic autoantibodies but also through their involvement in antigen presentation and the formation of immunological memory. Therefore, therapies aimed at depleting or inhibiting B cells have garnered significant interest. However, clinical responses to rituximab in MG have shown variability, which may be attributed to its inability to eliminate long-lived plasma cells (LLPCs) that do not express CD20.7,8 Telitacicept, a dual inhibitor of B lymphocyte stimulating factor (BLyS) and a proliferation-inducing ligand (APRIL), targets upstream pathogenesis by suppressing autoreactive B cells and plasma cells, thereby providing sustained clinical benefits. A Phase 2 trial of 29 AChR and Muscle-Specific Tyrosine Kinase (MuSK) antibody-positive patients with generalized MG (gMG) on various standard therapies treated for 24 weeks demonstrated that patients receiving the 160 mg dose achieved average reductions of 5.8 and 7.7 points in Quantitative Myasthenia Gravis (QMG) scores from baseline to weeks 12 and 24, respectively, indicating rapid and sustained symptomatic improvement.9 A randomized controlled Phase 3 trial of telitacicept for MG enrolled 114 participants (placebo 57, telitacicept 57). In this study, 48.1% of telitacicept-treated patients achieved a ≥3-point reduction in MG-ADL by week 4, with a significant and sustained improvement observed at week 24 (98.1% vs 12% placebo). Importantly, telitacicept showed fewer adverse events (AEs) than placebo in clinical trials. These findings have shown rapid onset of action, durable remission, and an excellent safety profile for the treatment of MG with telitacicept. However, the strict inclusion criteria of randomized controlled trials (RCTs) often exclude specific populations, such as patients with thymoma-associated MG, elderly patients, or those with comorbid autoimmune diseases, limiting the generalizability of RCT findings to real-world clinical settings. Although telitacicept has been approved based on RCT evidence, the heterogeneity and complexity of patients in real-world settings warrant further validation of its real-world outcomes and safety. To address this, we conducted this real-world study to evaluate the clinical outcomes of telitacicept in a broader population of patients with AChR-Ab+ gMG.
Methods
We conducted a retrospective study (ChiCTR2500109279) on 215 patients with AChR-Ab+ gMG aged 18 to 80 years who were treated at the First Hospital of China Medical University. All participants provided informed consent. We included patients who were diagnosed with gMG using the 2020 Chinese recommendations for MG diagnosis and treatment, tested positive for anti-AChR antibodies, and received either telitacicept or conventional immunotherapy, with a follow-up period of at least 24 weeks. Demographic and baseline clinical data were collected prospectively, including age, sex, disease duration, Myasthenia Gravis Foundation of America (MGFA) classification, QMG score, MG-ADL score, thymoma status, immunosuppressant type and dosage, and AChR antibody titers. Follow-up assessments of QMG and ADL scores were performed monthly. Patients were divided into a telitacicept group (43 cases) and a conventional immunotherapy group (172 cases). In the telitacicept group, patients received weekly subcutaneous injections of 160 mg telitacicept, with or without concurrent low-dose prednisone or NSISTs. The low-dose regimen was defined as follows: prednisolone <20 mg/day, tacrolimus <5 mg/day, azathioprine <150 mg/day, or mycophenolate mofetil <2000 mg/day.10 In the conventional immunotherapy group, treatment began with oral prednisone at an initial dose of 20 mg/day, targeting a goal dose of 0.5–1.0 mg/kg/day, combined with or without oral NSISTs. The NSISTs used in the study included tacrolimus (0.05–0.10 mg/kg/day) or mycophenolate mofetil (initial dose 0.5–1.0 g/day, maintenance dose 1.0–1.5 g/day).
In this study, sex information of the participants was collected to describe the basic characteristics of the study population. Sex was determined as male or female based on birth records or self‑reported biological characteristics.
Clinical Outcome
We assessed changes in QMG and ADL scores, the time to achieve minimal symptom expression (MSE), and the proportion of patients achieving clinically meaningful improvement. Specifically, MSE was defined as an MG-ADL score of 0 or 1. A clinically meaningful improvement meant a reduction of ≥5 points in the QMG score or a decrease of ≥3 points in the ADL score from baseline. These definitions are consistent with the endpoints used in the phase 3 trial of telitacicept (NCT05737160) to ensure methodological continuity and comparability.
Safety Evaluation
All AEs were recorded and graded by severity according to the Common Terminology Criteria for Adverse Events (CTCAE). We specifically monitored drug-related reactions, including upper respiratory infections, decreased immunoglobulins, diarrhea, injection site reactions, and urinary tract infections, along with any unexpected medication-related events. Changes in the percentage of CD19+ B cells and serum immunoglobulin (IgA/IgG/IgM) levels were monitored at each follow-up visit.
Statistical Methods
We used R software version 4.5.0 for analysis. Continuous data with a normal distribution are expressed as mean ±standard deviation (SD), while non-normally distributed data are presented as median (M) with interquartile range (IQR). Continuous variables were compared between groups using the independent-samples t-test for normally distributed data and the Mann–Whitney U-test for non-normally distributed data. Categorical variables were compared using chi-squared or Fisher’s exact tests. The Bonferroni correction was used to adjust p-values for multiple comparisons. Repeated-measures ANOVA was employed to analyze within-group changes over time when parametric assumptions were met; otherwise, the Friedman test was applied. To balance baseline confounding factors between groups, we performed propensity score matching (PSM) (1:1 nearest-neighbor method with a caliper width of 0.02). The propensity scores were calculated using logistic regression incorporating age, sex, disease duration, MGFA classification, QMG score, ADL score, and thymoma status as covariates. Matching quality was evaluated using standardized mean differences (SMD), where values <0.1 indicated adequate covariate balance. We plotted survival curves using the Kaplan-Meier method and compared groups with the Log rank test. Differences were considered statistically significant with the following p-values: *p<0.05, **p<0.01, ***p<0.001.
The study design used a two-sided alpha of 0.05 and 80% power. A Phase III study showed 24-week MSE rates of 24.1% for treatment and 4.0% for control. Based on this, we included 70 patients through 1:1 PSM for the main analysis. A post-hoc power analysis confirmed adequate power, although we acknowledge such analysis can be circular in retrospective studies.
Results
Baseline Characteristics of Patients
Our study included 215 AChR-Ab+ gMG patients, whose age at onset ranged from 18 to 80 years. The baseline characteristics of the patients treated with telitacicept (20%; n=43) and those receiving conventional immunotherapy (control group: 80%; n=172) are summarized in Table 1. A female predominance was observed in both groups (telitacicept group: 28 [65.1%] vs control group: 104 [60.5%], p=0.700), with the majority in both cohorts also receiving concomitant corticosteroid therapy (telitacicept group: 37 [86%] vs control group: 126 [73.3%], p=0.120). The proportion of patients with thymoma was similar between groups (telitacicept group: 13 [30.2%] vs control group: 48 [27.9%], p=0.910). However, the telitacicept group had more patients with severe disease (MGFA class IIIb and IVb). It also had fewer patients with mild disease (MGFA class IIa and IIb). A PSM was performed to account for baseline characteristics that differed between groups and could affect symptom improvement. After matching, 35 patients remained in each group (Table 2), and their baseline characteristics were well-balanced with no significant differences.
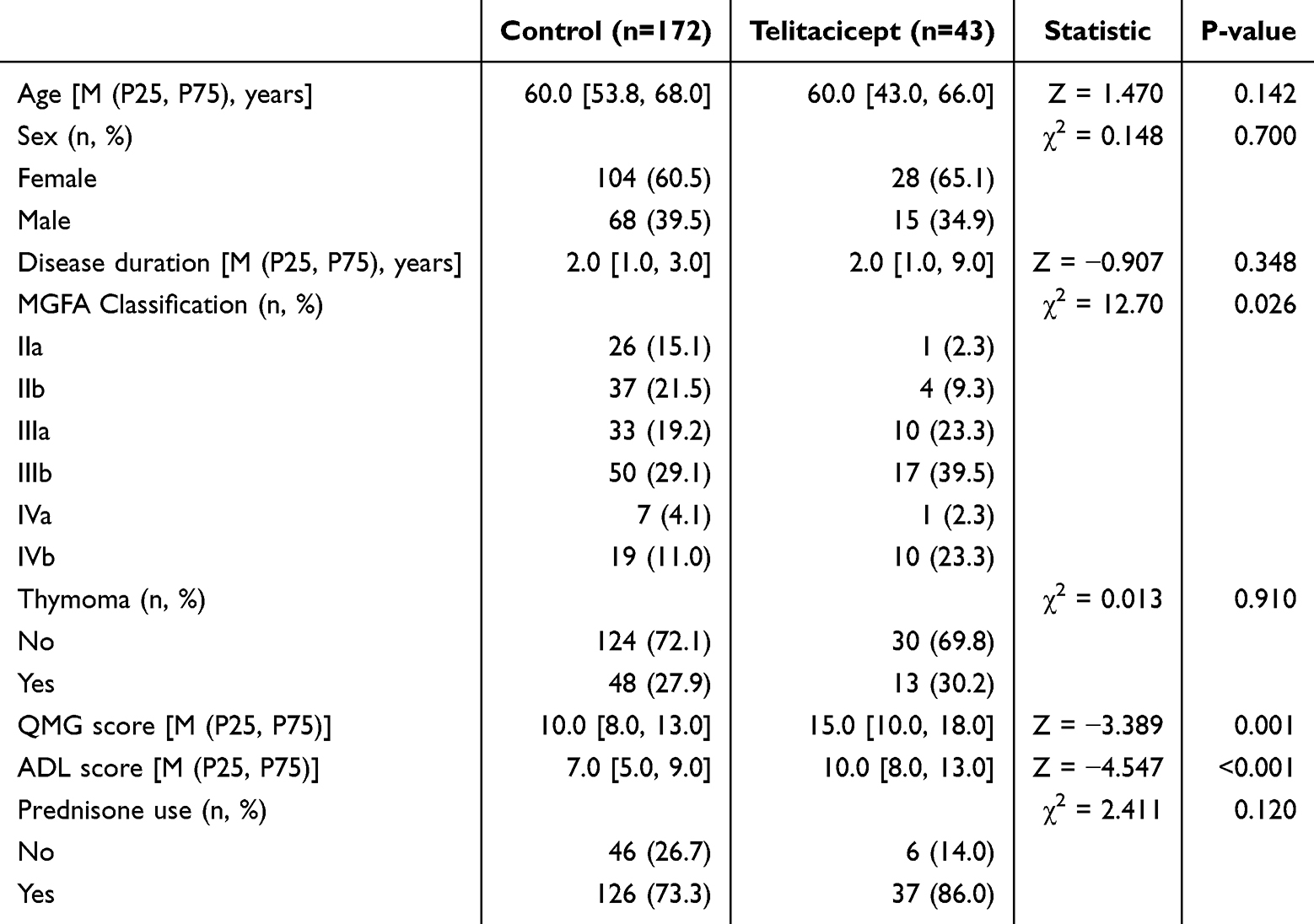 |
Table 1 Baseline Characteristics of Enrolled Patients (n = 215) |
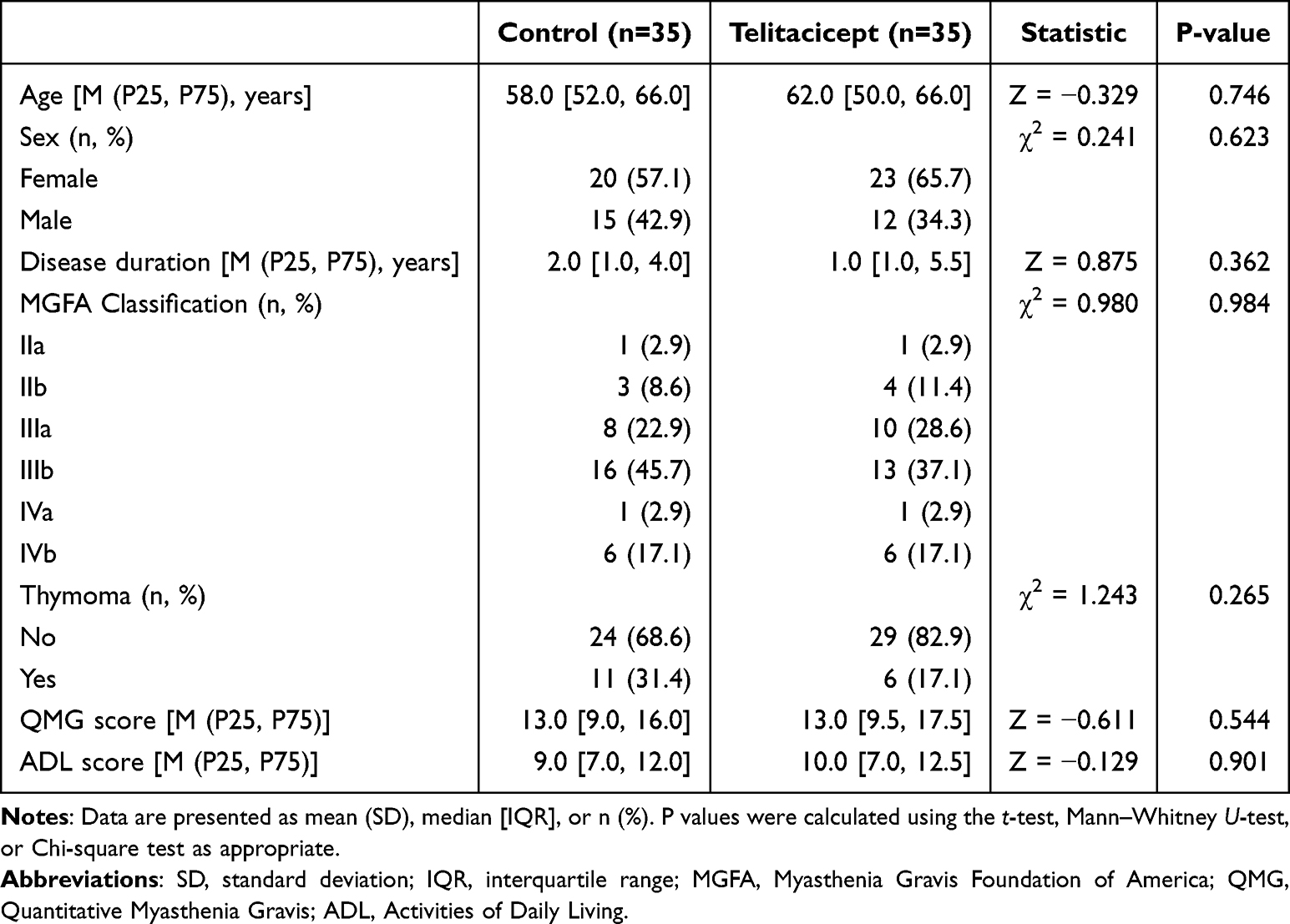 |
Table 2 Patient Characteristics After Propensity Score Matching |
Effectiveness of Telitacicept
All patients completed the 24-week follow-up. At week 24, the telitacicept group showed greater improvements from baseline in both QMG and ADL scores compared to the control group (QMG: 10.30±4.19 vs 2.86±3.21, p<0.001; ADL: 8.06±3.37 vs 2.63±2.07, p<0.001) (Figure 1a and b). More patients in the telitacicept group achieved clinically meaningful improvement, with 94.3% attaining a ≥5-point reduction in QMG score (vs 17.1% in the control group) (Figure 2a) and 97.1% achieving a ≥3-point reduction in ADL score (vs 25.7%) (Figure 2b), and these differences were statistically significant (p<0.001). The telitacicept group consistently demonstrated greater reductions in QMG and ADL scores than the control group at all follow-up points, with this decreasing trend maintained throughout the observation period. These results suggest that telitacicept offers benefits over conventional immunotherapy in the treatment of gMG.
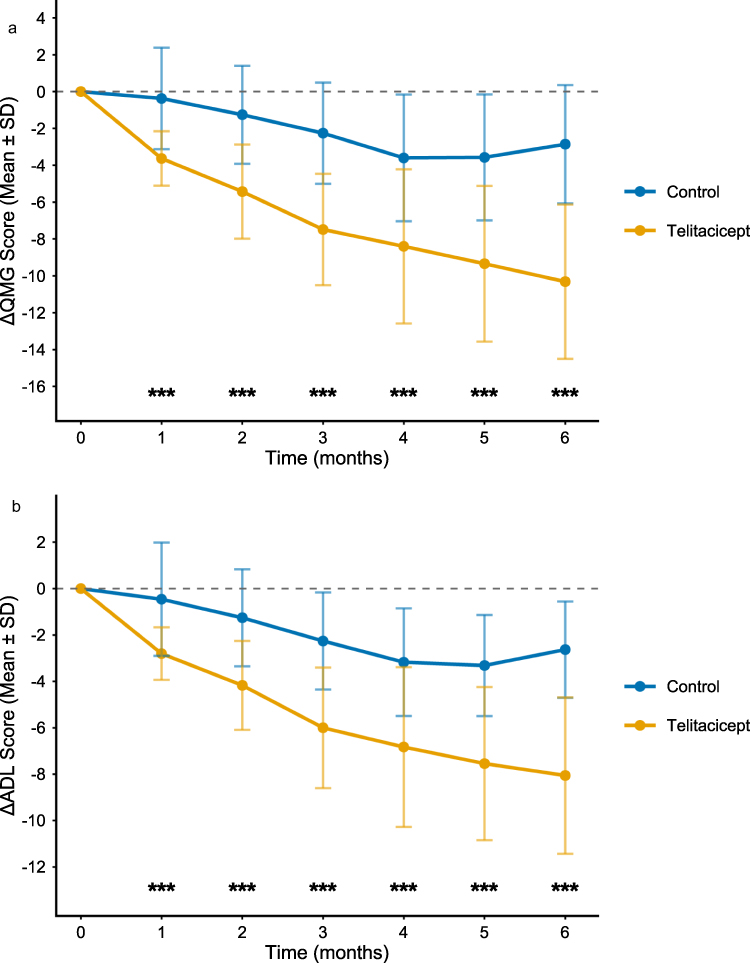 |
Figure 1 (a) ΔQMG score over time in the telitacicept group (Orange) and control group (blue). Data are mean ± SD. (b) ΔADL score over time in the telitacicept group (orange) and control group (blue). Data are mean ± SD. ***p < 0.001. |
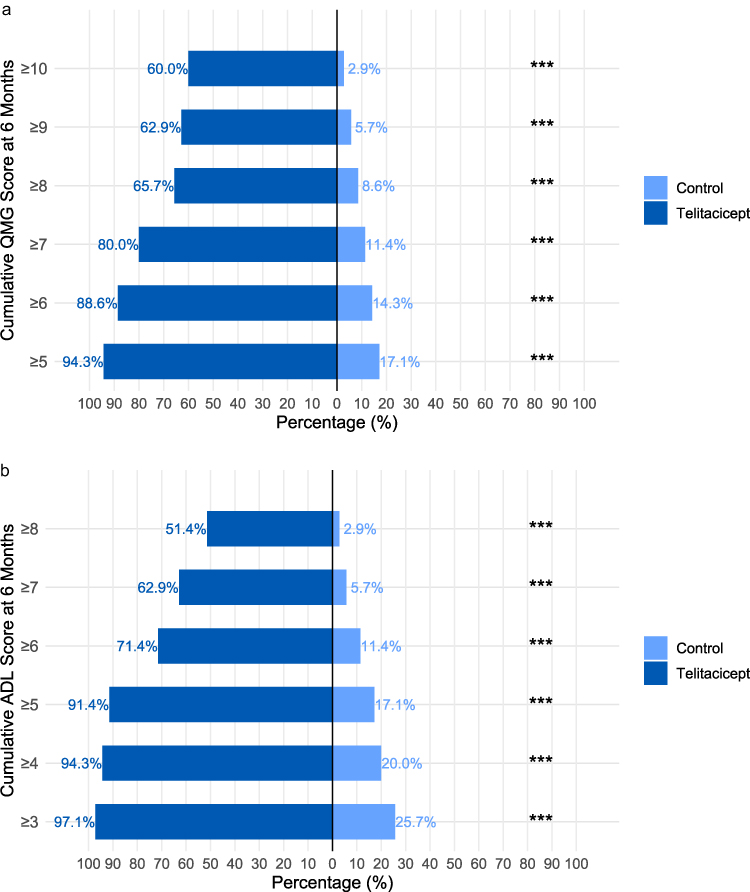 |
Figure 2 (a) Cumulative distribution of QMG scores at 6 months. Light blue: control; dark blue: telitacicept. (b) Cumulative distribution of ADL scores at 6 months. Light blue: control; dark blue: telitacicept. ***p < 0.001. |
Notably, this treatment benefit was observable as early as week 4, with patients in the telitacicept group demonstrating greater reductions in scores from baseline (QMG: 3.63±1.48 vs 0.37±2.76, p<0.001; ADL: 2.80±1.13 vs 0.46±2.44, p<0.001). By week 4, a larger proportion of telitacicept-treated patients had achieved an early clinically meaningful response (≥5-point QMG improvement: 31.4% vs 5.7%; ≥3-point ADL improvement: 48.6% vs 17.1%; both p<0.001) (Figure 3), indicating a more rapid onset of effect.
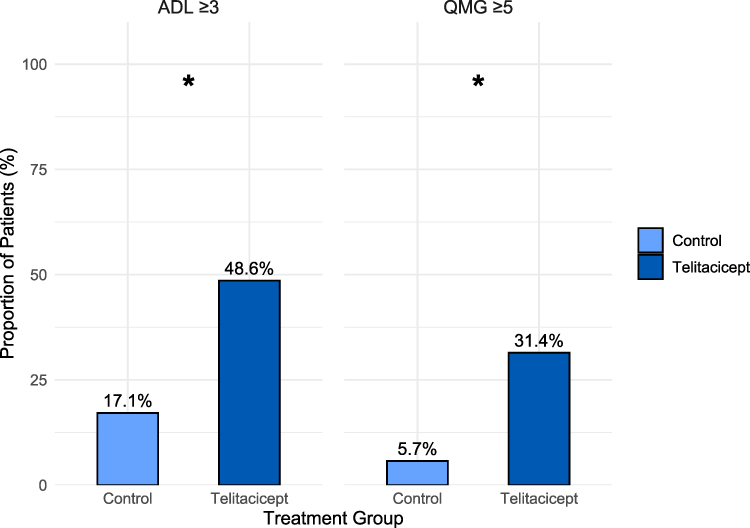 |
Figure 3 Proportion of patients achieving clinically meaningful improvement at month 1 (n=35 per group). Left: QMG improvement ≥5 points; Right: ADL improvement ≥3 points. *p < 0.05. |
Additionally, during the observation period, a higher percentage of patients in the telitacicept group achieved MSE (57.1% vs 11.4%, p<0.001). Kaplan-Meier analysis supported these findings, showing a shorter median time to MSE in the telitacicept group (5 months) (Figure 4) than in the control group.
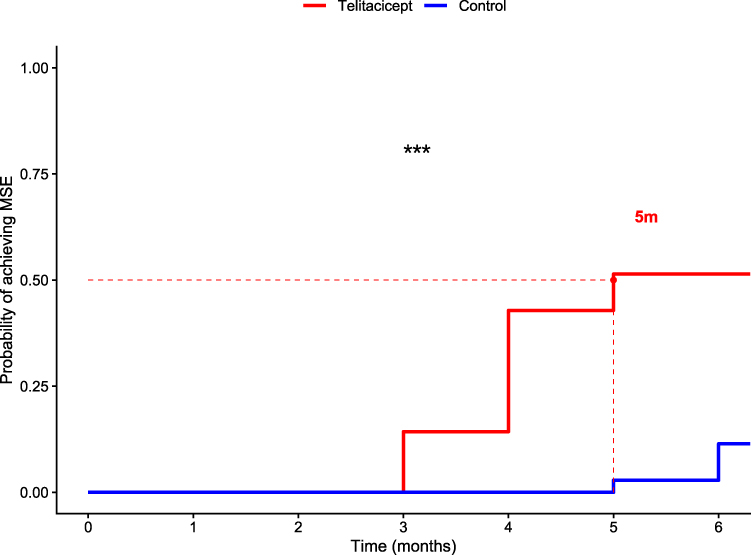 |
Figure 4 Kaplan-Meier curves for time to achieve MSE. Red: telitacicept; blue: control. Dashed lines indicate median time to MSE (telitacicept: 5 months). ***p < 0.001. |
Steroid‑Sparing Effect of Telitacicept
Among patients receiving concomitant prednisone, baseline daily doses were similar between the telitacicept (median 20.0 mg/d, IQR 20.0–30.0; n=30) and control groups (median 25.0 mg/d, IQR 20.0–32.5; n=24; P=0.217). At month 6, the median daily dose was 5.0 mg/d (IQR 5.0–10.0) with telitacicept versus 15.0 mg/d (IQR 15.0–20.0) with control therapy (P<0.001). Consequently, the 24-week cumulative prednisone exposure was 2325 mg (IQR 1575–3281) in the telitacicept group compared with 6525 mg (IQR 5231–6675) in controls (P<0.001) (Figure 5). Furthermore, all patients in the telitacicept group who completed the 12-month follow-up kept their prednisone dose at 5 mg/d or less.
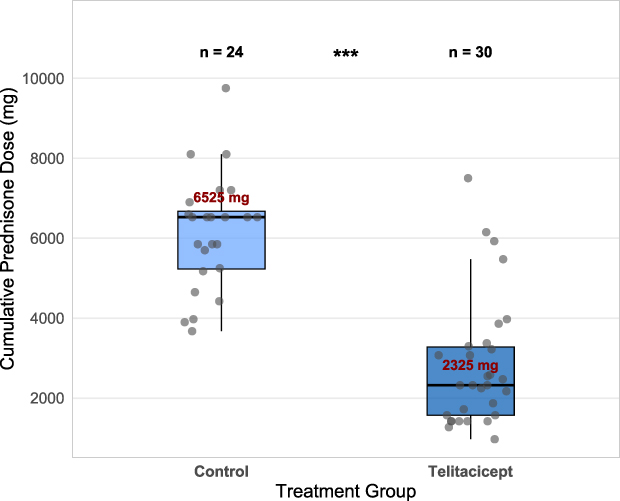 |
Figure 5 Cumulative prednisone dose over 24 weeks. Boxes represent IQR, horizontal lines indicate median. Telitacicept (dark blue, n=35); control (light blue, n=34). ***p < 0.001. |
Change in Immune Markers
We documented changes in CD19+ B-cell percentages, serum immunoglobulin levels, and anti-AChR antibody titers from baseline to week 24 for all telitacicept subjects. During treatment, the CD19+ B-cell percentage decreased from a baseline mean of 12.97% (range: 6–30%) to 8% (range: 2–13%) by week 24 (p<0.001). It is noted that no patient showed a CD19+ B-cell percentage below 1% during the observation period. Serum IgG and IgA levels also decreased by week 24, while IgM levels declined from a baseline mean of 1.11 g/L (range: 0.34–2.01) to 0.44 g/L (range: 0.14–0.75) (p<0.001, Figure 6a–c). The IgM-to-IgG ratio showed a consistent reduction, from a baseline mean of 0.093 (range: 0.04–0.19) to 0.057 (range: 0.02–0.13) at week 24 (p<0.001, Figure 6d). Additionally, anti-AChR antibody titers decreased from a baseline mean of 45.10 nmol/L to 17.91 nmol/L by week 24 (p<0.01).
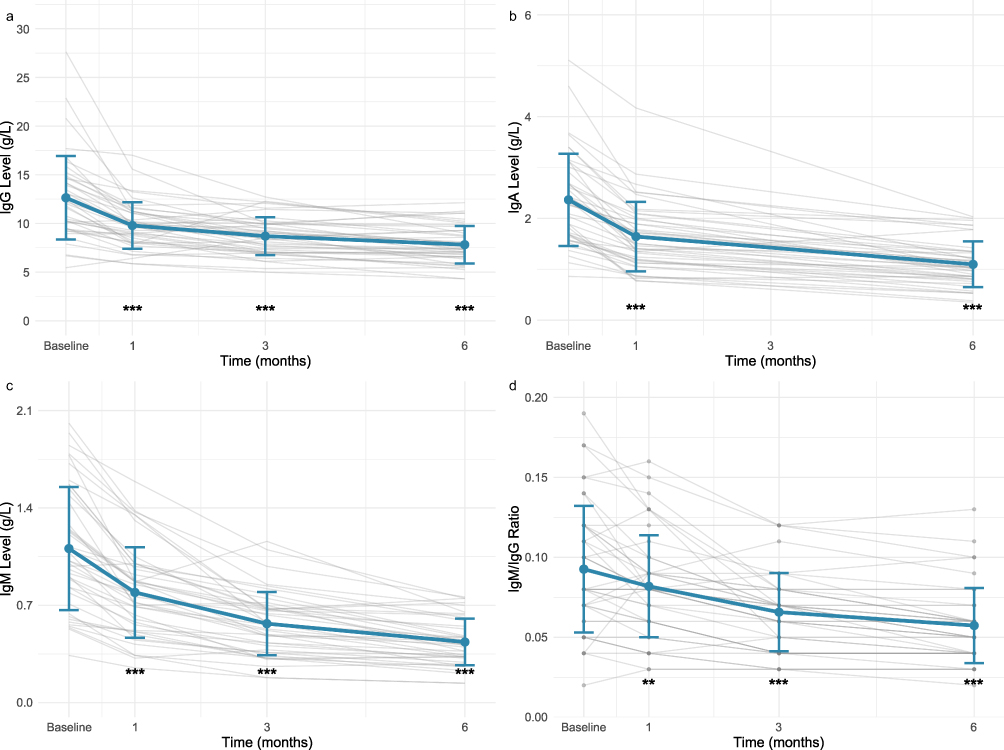 |
Figure 6 (a) Changes in serum IgG levels over time. Data are mean ± SD. Blue line: mean; grey lines: individual patients. (b) Changes in serum IgA levels over time. Data are mean ± SD. (c) Changes in serum IgM levels over time. Data are mean ± SD. (d) Changes in IgM/IgG ratio over time. Data are mean ± SD. **p < 0.01, *p < 0.001. vs baseline. |
Adverse Effects and Safety
During the observation period, 15 AEs were recorded in the telitacicept group, compared with 34 AEs in the control group (Table 3). Among patients receiving telitacicept, the most frequently reported adverse reaction was mild and transient swelling at the injection site, occurring in 6 cases, with symptoms resolving spontaneously within several days. These reactions occurred intermittently rather than after every administration and were often related to injection technique or local skin condition rather than a consistent drug effect. This was followed by 3 cases of respiratory infection during treatment, along with 2 cases of diarrhea and 1 case of urinary tract infection, all of which improved promptly with symptomatic management. Other reported events included nausea after the first injection in one patient, as well as isolated instances of dizziness and mild transient headache; these symptoms subsided by the following day. In the 35 patients treated with conventional immunosuppressive agents, the most common adverse reactions included elevated blood glucose, followed by increased blood lipids, weight gain, insomnia, osteoporosis, respiratory infections, urinary tract infections, and elevated blood pressure, consistent with their known safety profiles. No deaths were documented in either group during follow-up, and no allergic reactions or severe adverse drug reactions (SADR) occurred.
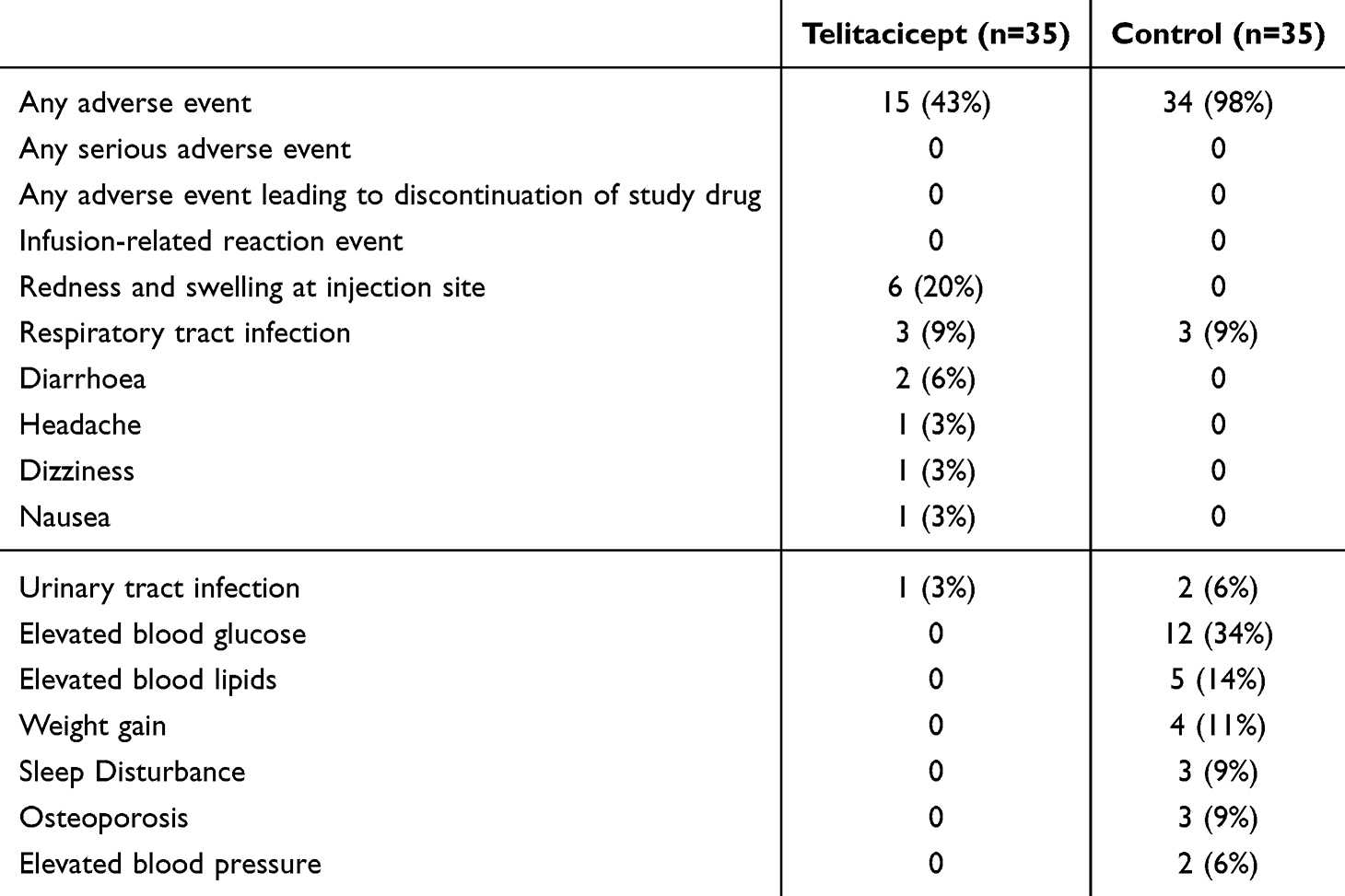 |
Table 3 Adverse Events with Telitacicept and Conventional Immunosuppressants |
Discussion
As the real-world study to directly compare telitacicept with conventional immunotherapy for gMG, our findings indicate that telitacicept, as a B-cell-modulating therapy, offers better treatment outcomes, characterized by a faster onset of action and a better tolerability profile. This pivotal evidence provides a practical reference for clinical decision-making and sets the foundation for further investigation into its role in gMG management.
The Phase 3 trial confirmed telitacicept’s efficacy, with significantly greater MG-ADL reductions than placebo. Recently, two retrospective studies have also provided supporting evidence for telitacicept’s efficacy. In a study by Bu Biao et al involving 16 patients with refractory gMG treated with telitacicept, 75% of patients demonstrated symptomatic improvement within the first 3 months11 This clinical benefit not only persisted but further increased at the 6-month follow-up. Additionally, Li et al found that sequential efgartigimod-telitacicept therapy led to sustained improvement in MG-ADL scores at week 28, indicating potential long-term symptom control12 In summary, while RCTs can minimize bias and provide the strongest evidence for causal inference, their stringent inclusion/exclusion criteria often result in study populations that may not represent the complexity of real-world clinical patients, such as those with thymoma or concurrent autoimmune diseases. Conversely, observational cohort studies frequently suffer from limitations such as lack of control groups, treatment selection bias, and small sample sizes, which compromise their reliability. To address these challenges, we employed PSM to achieve post-hoc randomization, thereby reducing confounding biases associated with potential selection effects.
In our study, the telitacicept group showed greater reductions in both QMG and ADL scores at all time periods than the conventional therapy group, indicating better treatment outcomes for gMG. These alterations were noticed as early as week four and grew more prominent by week 24. Additionally, more patients receiving telitacicept achieved MSE (57.1% vs 11.4%), with a shorter median time to MSE of 5 months. These findings suggest that telitacicept provides enhanced symptom relief compared to standard full-dose conventional immunosuppressive regimens. The rapid onset of action of telitacicept can be attributed to its favorable pharmacokinetic profile, with serum concentrations of the BLyS-telitacicept complex reaching peak levels within 5 to 29 days, facilitating prompt symptom relief.13 Its multi-target mechanism further contributes to its therapeutic effects. First, the principal mechanism of telitacicept in treating gMG is mediated through dual inhibition of BLyS and APRIL. Studies have shown elevated serum levels of BLyS and APRIL in MG patients, suggesting their involvement in disease pathogenesis.14–17 Overexpression of BLyS disrupts B-cell homeostasis and promotes the survival and proliferation of autoreactive B cells, while APRIL supports the survival of LLPCs and antibody class switching by inhibiting apoptosis-related proteins.18,19 By simultaneously targeting these two cytokines, telitacicept directly reduces autoreactive B cells and antibody production, thereby interrupting the aberrant immune response at its source, which leads to improvement in clinical symptoms. Furthermore, recent evidence suggests that telitacicept may promote the recovery of regulatory B cells (Bregs),20–23 which regulate the immune microenvironment by secreting inhibitory cytokines, further suppressing the activation and functions of autoreactive B cells.24–27 In addition, telitacicept interferes with the formation of ectopic germinal centers in MG, a process that limits the development of LLPCs, leading to a sustained reduction in autoantibody and cytokine production.28–31 Through the concerted action of these multiple mechanisms, telitacicept ultimately alleviates the clinical symptoms in MG.
Like telitacicept, the anti-CD20 monoclonal antibody rituximab represents an established therapy targeting upstream B cells. Previous studies have explored the potential of rituximab in treating MG, with clear clinical improvement observed in MuSK-Ab+ MG.8,32 However, its treatment outcome in AChR-Ab+ cases remains less consistent.33–35 This discrepancy may be attributed to the absence of CD20 on long-lived plasma cells (LLPCs), thereby limiting rituximab’s ability to target this cell population, which plays a central pathogenic role in AChR-Ab+ MG.36 Moreover, the onset of action for rituximab typically requires 6 to 8 weeks,37,38 a delay that aligns with clinical observations indicating a median time of approximately 11 weeks to maximal B-cell depletion, with some patients needing multiple treatment cycles to achieve symptomatic improvement.39 In comparison, telitacicept appears to have a more rapid onset of action. Future prospective head-to-head studies directly comparing rituximab and telitacicept will be essential to clarify their respective roles and optimal positioning in the treatment landscape of MG.
The clinical benefits of telitacicept were long-term, with sustained reductions in both QMG and ADL scores throughout at least 24 weeks of follow-up. This prolonged effect is backed by the extended presence of the BLyS-telitacicept complex, which remains detectable for up to 71 days post-administration due to a slow elimination half-life of approximately two weeks.13 Coupled with the inherently slow regeneration of mature B cells and plasma cells, these properties support persistent symptom relief and long-term immune stability even after therapy is discontinued.
The steroid-sparing benefit of telitacicept emerged as a key finding in this study. Although CS serve as first-line immunotherapy for MG, their long-term use is limited by considerable adverse effects.40 Standard prednisone regimens typically maintain an average daily dose above 30 mg/d over 15 months.41 In the study by Sharshar et al, a rapid tapering regimen resulted in a substantially lower total prednisone dose over one year compared to a slow tapering schedule (7890 mg vs 9060 mg).42 Their findings demonstrated that rapid prednisone reduction was not only well-tolerated but also associated with more patients achieving corticosteroid-free remission at 12 months. Similarly, in our cohort, telitacicept supported faster prednisone reduction. At week 24, the median daily prednisone dose was lower in the telitacicept group (5.0 mg/d, IQR 5.0–10.0) than in controls (15.0 mg/d, IQR 15.0–20.0; P<0.001). Consistent with this reduction, the 24-week cumulative exposure was 2325 mg (IQR 1575–3281) with telitacicept compared with 6525 mg (IQR 5231–6675) in the control group (P<0.001). These results together indicate that telitacicept helps lessen reliance on steroids in MG treatment.
In our study, telitacicept demonstrated a favorable safety and tolerability profile in patients with gMG. No SADRs occurred, and no patients discontinued therapy due to AEs. The most common issue was mild, transient injection site reactions. Other AEs were infrequent and resolved rapidly with appropriate care. This safety record is consistent with prior studies and stands in marked contrast to conventional therapy, which was frequently associated with long-term AEs such as increased blood glucose, dyslipidemia, and osteoporosis.43 Furthermore, the convenience of subcutaneous administration resulted in high patient compliance. Collectively, these features establish telitacicept as a safe and manageable long-term treatment strategy for gMG.
We performed a detailed analysis of dynamic changes in immune biomarkers. Initially, CD19⁺ B cells demonstrated a mild upward trend during the early phase, likely related to telitacicept’s inhibition of BLyS and APRIL, which impedes B-cell maturation and leads to the discharge of immature, functionally deficient B cells into peripheral blood. Reduced BLyS levels may further contribute to this increase in B-cell counts. Second, serum levels of IgM, IgG, and IgA decreased to differing degrees, in keeping with earlier research. Notably, a sustained decrease in the IgM-to-IgG ratio was observed, which earlier research has suggested may be connected with elevated levels of the BLyS-telitacicept complex.18 This leads us to propose that the IgM-to-IgG ratio could potentially serve as a serological biomarker for predicting clinical response, though further research remains necessary to identify reliable biomarkers for accurately assessing treatment outcomes with telitacicept.
This study has certain limitations. As a retrospective single-center study, it is inherently subject to selection bias and may limit generalizability. Although PSM was used, the approach was still less stringent than that of an RCT and reduced the sample size from 215 to 70, which may decrease statistical power and generalizability. The limited sample also prevented comparisons between the effectiveness of telitacicept and that of individual conventional regimens, as well as identification of the optimal patient subgroups. Additionally, thymic hyperplasia could not be reliably analyzed due to the lack of pathological confirmation in non-surgical patients. Therefore, future large-scale RCTs with extended follow-up are needed to clarify the optimal target population for telitacicept and to compare its long-term outcomes with those of different conventional immunotherapies in MG.
Conclusion
In summary, this study provides real-world evidence supported through PSM, demonstrating that compared with conventional immunotherapy, telitacicept enables patients with gMG to achieve symptom control and attain MSE within 5 months, along with improved therapeutic benefits and a favorable safety and tolerability profile. In addition, the application of telitacicept helps reduce steroid dosage, which may support long-term management. The sustained decline in the IgM to IgG ratio observed during the treatment suggests its potential as a serological biomarker for predicting gMG disease activity. These results serve as a valuable reference for clinical decision-making and help pave the way for advancing gMG treatment strategies toward more individualized and precise approaches. Regrettably, we did not directly measure the serum levels of BLyS and APRIL. In the future, a multi-center, large-sample prospective cohort study for verification will remain an indispensable next step.
Abbreviations
QMG, Quantitative Myasthenia Gravis; SD, standard deviation; ADL, activities of daily living; MSE, minimal symptom expression; IgG, immunoglobulin G; IgA, immunoglobulin A; IgM, immunoglobulin M; *p < 0.05, **p < 0.01, ***p < 0.001.
Data Sharing Statement
Due to patient privacy and ethical restrictions, the raw clinical data are not publicly available. The de-identified data underlying the findings can be obtained from the corresponding author upon reasonable request, subject to approval by the Ethics Committee of The First Affiliated Hospital of China Medical University (Approval No. 2025-690-2).
Ethics Approval
This study was approved by the Ethics Committee of The First Affiliated Hospital of China Medical University (No. 2025-690-2). The study followed the Declaration of Helsinki and its amendments.
Consent to Participate
Informed consent was obtained from all individuals included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (81501006) and Natural Science Foundation of Liaoning province (2023-MSLH-406).
Disclosure
Yingying Yang and Nan Kang are co-first authors for this study. The authors declare no conflicts of interest in this work.
References
1. Gilhus NE, Tzartos S, Evoli A, Palace J, Burns TM, Verschuuren JJGM. Myasthenia gravis. Nat Rev Dis Primers. 2019;5(1):30. doi:10.1038/s41572-019-0079-y
2. Cutter G, Xin H, Aban I, et al. Cross-sectional analysis of the myasthenia gravis patient registry: disability and treatment. Muscle Nerve. 2019;60(6):707–13. doi:10.1002/mus.26695
3. McConville J. C5 complement inhibition and FcRn modulation in generalized myasthenia gravis. Fast-acting but short-lived therapies the use of which should prompt assertive escalation of conventional treatments. J Neurol Neurosurg Psychiatry. 2025;96(4):309. doi:10.1136/jnnp-2024-334584
4. Pane C, Di Stefano V, Cuomo N, et al. A real-life experience with eculizumab and efgartigimod in generalized myasthenia gravis patients. J Neurol. 2024;271(9):6209–6219. doi:10.1007/s00415-024-12588-7
5. Ulrichts P, Guglietta A, Dreier T, et al. Neonatal Fc receptor antagonist efgartigimod safely and sustainably reduces IgGs in humans. J Clin Invest. 2018;128(10):4372–4386. doi:10.1172/JCI97911
6. Ramírez-Valle F, Maranville JC, Roy S, Plenge RM. Sequential immunotherapy: towards cures for autoimmunity. Nat Rev Drug Discov. 2024;23(7):501–524. doi:10.1038/s41573-024-00959-8
7. Nelke C, Schroeter CB, Stascheit F, et al. Eculizumab versus rituximab in generalised myasthenia gravis. J Neurol Neurosurg Psychiatry. 2022;93(5):548–554. doi:10.1136/jnnp-2021-328665
8. Piehl F, Eriksson-Dufva A, Budzianowska A, et al. Efficacy and safety of rituximab for new-onset generalized myasthenia gravis: the RINOMAX randomized clinical trial. JAMA Neurol. 2022;79(11):1105–1112. doi:10.1001/jamaneurol.2022.2887
9. Yin J, Zhao M, Xu X, et al. A multicenter, randomized, open-label, phase 2 clinical study of telitacicept in adult patients with generalized myasthenia gravis. Eur J Neurol. 2024;31(8):e16322. doi:10.1111/ene.16322
10. Hehir MK, Hobson-Webb LD, Benatar M, et al. Rituximab as treatment for anti-MuSK myasthenia gravis: multicenter blinded prospective review. Neurology. 2017;89(10):1069–1077. doi:10.1212/WNL.0000000000004341
11. Lin J, Li Y, Gui M, Bu B, Li Z. Effectiveness and safety of telitacicept for refractory generalized myasthenia gravis: a retrospective study. Ther Adv Neurol Disord. 2024;17:17562864241251476. doi:10.1177/17562864241251476
12. Zhang Y, Fang Z, Liu Y, et al. Efgartigimod followed by telitacicept in adult generalized myasthenia gravis: a retrospective case series. J Inflamm Res. 2025;18:4831–4842. doi:10.2147/JIR.S513986
13. Chen X, Hou Y, Jiang J, et al. Pharmacokinetics, pharmacodynamics, and tolerability of single ascending doses of RCT-18 in Chinese patients with rheumatoid arthritis. Clin Pharmacokinet. 2014;53(11):1033–1044. doi:10.1007/s40262-014-0175-9
14. Yi JS, Guptill JT, Stathopoulos P, Nowak RJ, O’Connor KC. B cells in the pathophysiology of myasthenia gravis. Muscle Nerve. 2018;57(2):172–184. doi:10.1002/mus.25973
15. Scuderi F, Alboini PE, Bartoccioni E, Evoli A. BAFF serum levels in myasthenia gravis: effects of therapy. J Neurol. 2011;258(12):2284–2285. doi:10.1007/s00415-011-6092-z
16. Kang SY, Kang CH, Lee KH. B-cell-activating factor is elevated in serum of patients with myasthenia gravis. Muscle Nerve. 2016;54(6):1030–1033. doi:10.1002/mus.25162
17. Thangarajh M, Masterman T, Helgeland L, et al. The thymus is a source of B-cell-survival factors-April and BAFF-in myasthenia gravis. J Neuroimmunol. 2006;178(1–2):161–166. doi:10.1016/j.jneuroim.2006.05.023
18. Halliley JL, Tipton CM, Liesveld J, et al. Long-lived plasma cells are contained within the CD19(-)CD38(hi)CD138(+) subset in human bone marrow. Immunity. 2015;43(1):132–145. doi:10.1016/j.immuni.2015.06.016
19. Jourdan M, Cren M, Robert N, et al. IL-6 supports the generation of human long-lived plasma cells in combination with either April or stromal cell-soluble factors. Leukemia. 2014;28(8):1647–1656. doi:10.1038/leu.2014.61
20. Blair PA, Noreña LY, Flores-Borja F, et al. CD19(+)CD24(hi)CD38(hi) B cells exhibit regulatory capacity in healthy individuals but are functionally impaired in systemic lupus erythematosus patients. Immunity. 2010;32(1):129–140. doi:10.1016/j.immuni.2009.11.009
21. Iwata Y, Matsushita T, Horikawa M, et al. Characterization of a rare IL-10-competent B-cell subset in humans that parallels mouse regulatory B10 cells. Blood. 2011;117(2):530–541. doi:10.1182/blood-2010-07-294249
22. Knippenberg S, Peelen E, Smolders J, et al. Reduction in IL-10 producing B cells (Breg) in multiple sclerosis is accompanied by a reduced naïve/memory Breg ratio during a relapse but not in remission. J Neuroimmunol. 2011;239(1–2):80–86. doi:10.1016/j.jneuroim.2011.08.019
23. Catalán D, Mansilla MA, Ferrier A, et al. Immunosuppressive mechanisms of regulatory B cells. Front Immunol. 2021;12:611795. doi:10.3389/fimmu.2021.611795
24. Lundy SK. Killer B lymphocytes: the evidence and the potential. Inflamm Res. 2009;58(7):345–357. doi:10.1007/s00011-009-0014-x
25. Ullah MA, Mackay F. The BAFF-april system in cancer. Cancers. 2023;15(6):1791. doi:10.3390/cancers15061791
26. Chen X, Hu L, Zhu L, et al. Prospective analysis of B cell subset dynamics following telitacicept treatment in systemic lupus erythematosus. Arthritis Res Ther. 2025;27(1):126. doi:10.1186/s13075-025-03584-x
27. den Hartog G, van Osch TLJ, Vos M, et al. BAFF augments IgA2 and IL-10 production by TLR7/8 stimulated total peripheral blood B cells. Eur J Immunol. 2018;48(2):283–292. doi:10.1002/eji.201646861
28. Furuya T, Tando S, Ogi H, et al. Distribution of ectopic germinal centers in thymic epithelial tumors and their relationship with thymic involution. Cancer Sci. 2025;116(11):3209–3219. doi:10.1111/cas.70183
29. Silver J, Zuo T, Chaudhary N, et al. Stochasticity enables BCR-independent germinal center initiation and antibody affinity maturation. J Exp Med. 2018;215(1):77–90. doi:10.1084/jem.20171022
30. Brink R. The imperfect control of self-reactive germinal center B cells. Curr Opin Immunol. 2014;28:97–101. doi:10.1016/j.coi.2014.03.001
31. Seyler TM, Park YW, Takemura S, et al. BLyS and April in rheumatoid arthritis. J Clin Invest. 2005;115(11):3083–3092. doi:10.1172/JCI25265
32. Brauner S, Eriksson-Dufva A, Hietala MA, Frisell T, Press R, Piehl F. Comparison between rituximab treatment for new-onset generalized myasthenia gravis and refractory generalized myasthenia gravis. JAMA Neurol. 2020;77(8):974–981. doi:10.1001/jamaneurol.2020.0851
33. Verschuuren JJ, Palace J, Murai H, Tannemaat MR, Kaminski HJ, Bril V. Advances and ongoing research in the treatment of autoimmune neuromuscular junction disorders. Lancet Neurol. 2022;21(2):189–202. doi:10.1016/S1474-4422(21)00463-4
34. Zhao C, Pu M, Chen D, et al. Effectiveness and safety of rituximab for refractory myasthenia gravis: a systematic review and single-arm meta-analysis. Front Neurol. 2021;12:736190. doi:10.3389/fneur.2021.736190
35. Nowak RJ, Coffey CS, Goldstein JM, et al. Phase 2 trial of rituximab in acetylcholine receptor antibody-positive generalized myasthenia gravis: the BeatMG study. Neurology. 2022;98(4):e376–e389. doi:10.1212/WNL.0000000000013121
36. Huda R. New approaches to targeting B cells for myasthenia gravis therapy. Front Immunol. 2020;11:240. doi:10.3389/fimmu.2020.00240
37. Howard JF, Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol. 2017;16(12):976–986. doi:10.1016/S1474-4422(17)30369-1
38. Nowak RJ, Dicapua DB, Zebardast N, Goldstein JM. Response of patients with refractory myasthenia gravis to rituximab: a retrospective study. Ther Adv Neurol Disord. 2011;4(5):259–266. doi:10.1177/1756285611411503
39. Fichtner ML, Jiang R, Bourke A, Nowak RJ, O’Connor KC. Autoimmune pathology in myasthenia gravis disease subtypes is governed by divergent mechanisms of immunopathology. Front Immunol. 2020;11:776. doi:10.3389/fimmu.2020.00776
40. Rice JB, White AG, Scarpati LM, Wan G, Nelson WW. Long-term systemic corticosteroid exposure: a systematic literature review. Clin Ther. 2017;39(11):2216–2229. doi:10.1016/j.clinthera.2017.09.011
41. Palace J, Newsom-Davis J, Lecky B; Myasthenia Gravis Study Group. A randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Neurology. 1998;50(6):1778–1783. doi:10.1212/wnl.50.6.1778
42. Sharshar T, Porcher R, Demeret S, et al. Comparison of corticosteroid tapering regimens in myasthenia gravis: a randomized clinical trial. JAMA Neurol. 2021;78(4):426–433. doi:10.1001/jamaneurol.2020.5407
43. Mantegazza R, Antonini G, Gastaldi M, et al. Use of corticosteroids in myasthenia gravis: expert opinion for daily management. Neurol Ther. 2025;14(5):2063–2081. doi:10.1007/s40120-025-00796-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.