Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Targeted Treatment for High-Risk Early-Stage Triple-Negative Breast Cancer: Spotlight on Pembrolizumab
Authors Bagegni NA ![]() , Davis AA, Clifton KK, Ademuyiwa FO
, Davis AA, Clifton KK, Ademuyiwa FO
Received 26 December 2021
Accepted for publication 15 April 2022
Published 29 April 2022 Volume 2022:14 Pages 113—123
DOI https://doi.org/10.2147/BCTT.S293597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Nusayba A Bagegni, Andrew A Davis, Katherine K Clifton, Foluso O Ademuyiwa
Division of Oncology, Department of Medicine, Washington University in St Louis School of Medicine, St Louis, MO, 63110, USA
Correspondence: Foluso O Ademuyiwa, Division of Oncology, Department of Medicine, Washington University in St Louis School of Medicine, St Louis, MO, 63110, USA, Email [email protected]
Abstract: Triple-negative breast cancer (TNBC) is a biologically aggressive yet heterogeneous disease that disproportionately affects younger women and women of color compared to other breast cancer subtypes. The paucity of effective targeted therapies and the prevalence of chemotherapeutic resistance in high-risk, early-stage TNBC pose significant clinical challenges. Deeper insights into the genomic and immune landscape have revealed key features of TNBC, including intrinsic genomic instability, DNA repair deficiency, and potentially an immunogenic tumor microenvironment. These advances led to landmark trials with immune checkpoint inhibitors in the advanced-stage setting, which subsequently translated into immunotherapy-based clinical trials in the early-stage setting and recent promising results. Pembrolizumab, an anti-programmed death 1 (PD-1) monoclonal antibody, was investigated in combination with platinum-, taxane- and anthracycline-based neoadjuvant chemotherapy followed by adjuvant pembrolizumab monotherapy for patients with high-risk, early-stage TNBC in the randomized, double-blind, placebo-controlled phase 3 KEYNOTE-522 trial. In July 2021, the US Food and Drug Administration (FDA) granted approval for pembrolizumab based on marked improvement in pathologic complete response rate and 3-year event-free survival compared to neoadjuvant chemotherapy alone. This advance immediately altered the longstanding treatment paradigm. Here, we review the impact of pembrolizumab plus chemotherapy for the treatment of patients with high-risk, early-stage TNBC, and discuss immunotherapy-related toxicity considerations, key immunomodulatory biomarkers under active investigation, and remaining clinical questions for future research directions.
Keywords: triple-negative breast cancer, early-stage high-risk, pembrolizumab, neoadjuvant, adjuvant, immune biomarkers
Introduction
Triple-negative breast cancer (TNBC) accounts for approximately 15–20% of all breast cancers, and is clinically defined as lacking expression of estrogen receptor (ER), progesterone expression (PR), and absence of HER2-neu overexpression. In recent years, the rapidly evolving landscape of breast cancer therapeutics has contributed to the reduction in mortality associated with breast cancer, particularly reflected by key advances in targeted therapies for ER-positive and HER2-positive tumors.1,2 Although TNBC relapse rates have decreased over time with modern-era therapeutic approaches, TNBC remains associated with unfavorable prognosis due to the absence of well-defined molecular targets which are only recently beginning to be elucidated.3,4 Substantial research is underway to define biomarkers for relapse and develop more effective neoadjuvant and adjuvant treatment approaches to improve long-term outcomes in patients with early-stage TNBC.
Historically, TNBC has been managed as a single breast cancer subtype. However, comprehensive molecular analyses illustrated that TNBC encompasses a complex and biologically heterogeneous disease. Gene expression profiling of breast cancers identified five distinct intrinsic molecular subtypes; the vast majority of basal-like tumors are TNBCs (>90%).5 TNBCs are enriched for TP53 mutations.6 Lehmann et al subsequently described six unique molecular signatures of TNBC: basal-like 1 and 2, mesenchymal and mesenchymal-stem like, immunomodulatory and luminal androgen receptor groups, each with differential responses to chemotherapy, and more recently, immunotherapy.7 Additional classification efforts have reported overlapping findings.8–10 Approximately 20% of unselected TNBC patients harbor defects in BRCA1 and 2 (germline and somatic), leading to homologous recombination DNA repair deficiency and potential PARP inhibitor sensitivity.11 Dysregulation of actionable signaling pathways commonly occurs in TNBC, including altered RAS/RAF/MEK, PI3K/AKT/mTOR, and JAK/STAT3 pathways. Although these pathway alterations are not clearly established as oncogenic drivers in TNBC, early investigations suggest that multikinase inhibition strategies are promising.5,12 Thus, transcriptome analysis and molecular subtyping improved our understanding of TNBC biology and provided opportunities for translational investigation. However, these advances have not yet entered routine clinical care to guide treatment decisions for patients with early-stage TNBC.
Neoadjuvant anthracycline- and taxane-based chemotherapeutic regimens have remained the mainstay of systemic therapy for patients with high-risk, early-stage TNBC, and are largely unchanged over the last several years.13 The TNBC paradox is that patients with early-stage TNBC tend to achieve higher responses to neoadjuvant chemotherapy, yet have a higher propensity for early disease recurrence with a predilection for visceral involvement.14,15 Optimal neoadjuvant chemotherapy approaches have not been fully established, including whether the incorporation of platinum salts translates to improved long-term outcomes, and the role of adjuvant approaches beyond capecitabine.16–19 Prognosis remains poor in patients who have residual disease after standard neoadjuvant therapy, with approximately 30–40% risk of recurrence.19–21 Novel therapeutic approaches are urgently needed. The recent approval of pembrolizumab plus chemotherapy greatly expands the therapeutic armamentarium, thereby improving cure rates for patients with high-risk, early-stage TNBC.
Immune Checkpoint Inhibitor Studies in Early-Stage TNBC
Recent approvals in the metastatic setting have provided promising therapeutic strategies for patients with advanced TNBC, including PARP inhibitors for tumors associated with germline BRCA1/2 mutations, the antibody-drug conjugate (ADC) sacituzumab govitecan, and immune checkpoint inhibitor combinations. In March 2019, atezolizumab plus nab-paclitaxel became the first checkpoint inhibitor to be granted accelerated FDA approval for the treatment of patients with PD-L1–positive advanced TNBC (as measured by the VENTANA SP-142 companion diagnostic) based on results from the Phase III IMpassion130 trial.22,23 The continued FDA approval of atezolizumab in this setting was contingent upon results from the IMpassion131 trial, a postmarketing requirement. The phase III IMpassion 131 trial of atezolizumab plus paclitaxel versus paclitaxel in a similar patient population failed to demonstrate an improvement in progression-free survival with the addition of atezolizumab.24 Although the results of both trials were reviewed by the FDA Oncology Drugs Advisory Committee and initially voted in favor of maintaining this accelerated approval of atezolizumab plus nab-paclitaxel, due to a shift in treatment landscape, the FDA no longer supported accelerated approval, and the manufacturer subsequently voluntarily withdrew this indication in the United States.25,26 In November 2020, the FDA approved pembrolizumab in combination with taxane or platinum chemotherapy for the treatment of patients with PD-L1–positive advanced TNBC [PDL-1 combined positive score (CPS) ≥10 according to the DAKO 22C3 companion diagnostic] based on the phase III KEYNOTE-355 study.27
These promising advances in metastatic TNBC therapeutics paved the way for designing clinical trials utilizing immune checkpoint inhibitors in the early-stage setting with varying findings [Table 1]. The phase III IMpassion031 trial demonstrated that administration of atezolizumab every 2 weeks plus anthracycline-cyclophosphamide and taxane-based chemotherapy improved the pathologic complete response (pCR) rate [58% (95% confidence interval (CI), 50 to 65) with atezolizumab versus 41% (95% CI, 34 to 49) with placebo in the intention-to-treat (ITT) population (∆ 17%, 95% CI, 6 to 27; one-sided p=0.0044 (significance boundary 0.0184))].28 By contrast, the NeoTRIPaPDL1 trial of neoadjuvant carboplatin plus nab-paclitaxel with or without atezolizumab, followed by surgery and adjuvant anthracycline-based regimen, did not improve the pCR rate in the ITT analysis (48.6% pCR with atezolizumab versus 44.4% without atezolizumab, odds ratio (OR) 1.18; 95% CI, 0.74 to 1.89; p=0.48).29 In the Phase II TONIC trial, anthracycline chemotherapy induction in patients with metastatic TNBC prior to administration of nivolumab yielded the highest response rate to immunotherapy (objective response rate of 35%) compared to other immunomodulating strategies, including other chemotherapeutic agents.30 Collectively, these data suggest that anthracyclines may serve as key chemotherapeutic agents to prime the immune response. In the phase II GeparNuevo trial, 117 patients treated with an initial 2-week “window” of single-agent durvalumab prior to neoadjuvant chemotherapy had a more pronounced improvement in pCR rate than those who received combination therapy alone (pCR 61.0% with durvalumab versus 41.4% with placebo, OR 2.22, 95% CI, 1.06 to 4.64, p=0.035).31,32
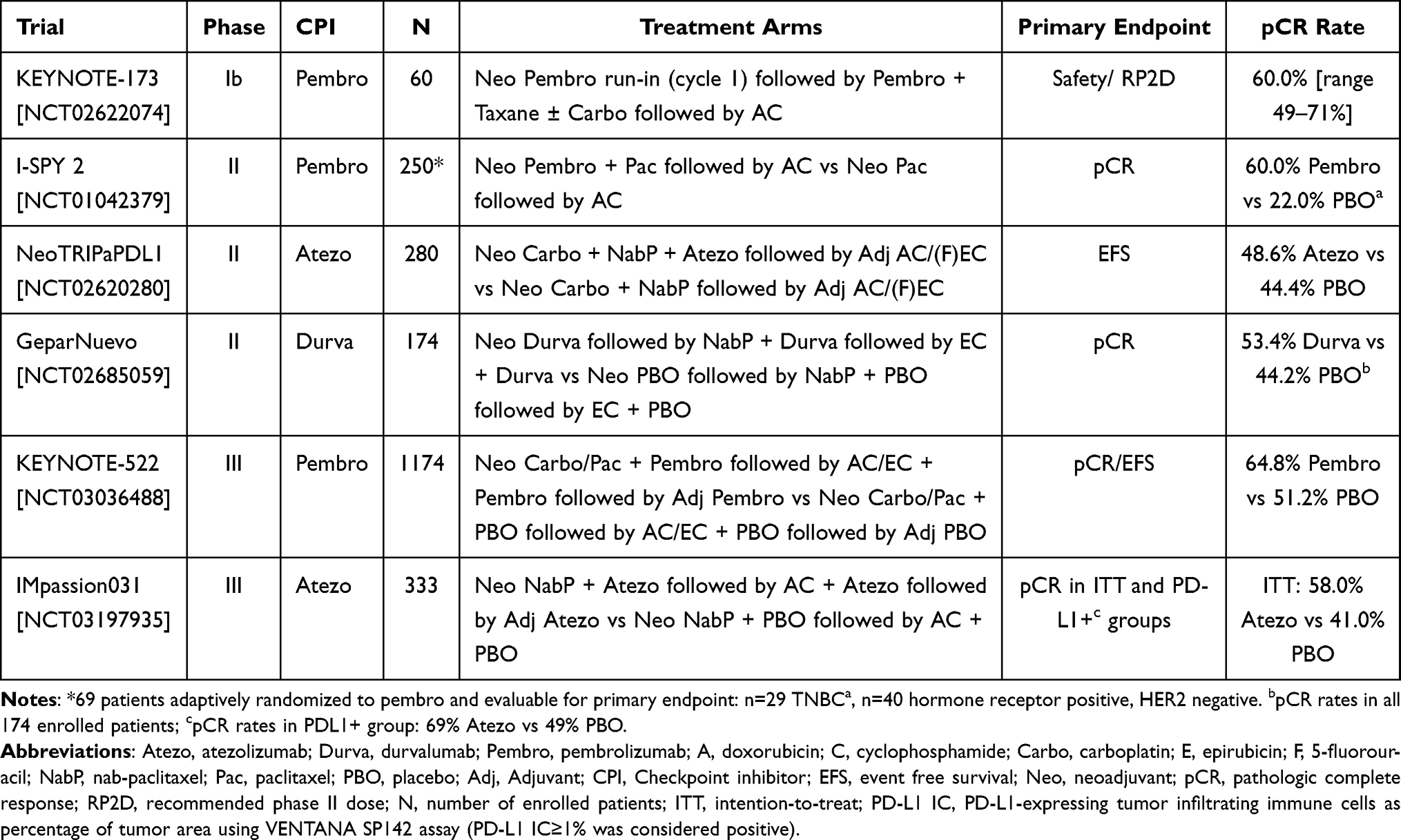 |
Table 1 Key Neoadjuvant Immune Checkpoint Inhibitor Trials in Stage II/III TNBC |
Early trials of neoadjuvant pembrolizumab plus chemotherapy showed manageable toxicity and improved antitumor activity in patients with early-stage TNBC. Pembrolizumab combined with neoadjuvant chemotherapy approximately doubled pCR rates and shifted residual cancer burden distribution to lower disease burden for evaluated cohorts in the randomized I-SPY 2 trial.33 These results supported the need for further investigation of pembrolizumab in a larger clinical trial. The phase Ib KEYNOTE-173 trial treated patients with pembrolizumab run-in for cycle 1, followed by taxane with or without carboplatin, followed by doxorubicin and cyclophosphamide (AC), similar to the GeparNuevo study design, and demonstrated promising anti-tumor activity (as assessed by pCR rate, event-free survival (EFS) and overall survival (OS)) and manageable toxicity profile.34 These trials established the basis for the FDA Breakthrough Therapy designation of pembrolizumab, and ultimately for the pivotal KEYNOTE-522 trial.
Pembrolizumab in Early-Stage TNBC
The phase III KEYNOTE-522 trial was the first randomized, double-blind, placebo-controlled study of pembrolizumab in early-stage TNBC in the neoadjuvant and adjuvant settings.35 Eligible patients included those with newly diagnosed, high-risk, early-stage TNBC (defined as cT1c, N1-2 or cT2-4, N0-2 according to the American Joint Committee on Cancer, 7th edition). Patients with active autoimmune disease requiring systemic treatment within the previous 2 years, clinically significant comorbid condition or immunodeficiency, or requiring immunosuppressive therapy were excluded. In the neoadjuvant setting, a total of 1174 patients were randomized (2:1 fashion) and received pembrolizumab (200 mg intravenously every 3 weeks) or placebo combined with carboplatin (weekly or every 3 weeks) plus weekly paclitaxel for 4 cycles (first neoadjuvant treatment), followed by anthracycline (doxorubicin or epirubicin) plus cyclophosphamide every 3 weeks for 4 cycles (second neoadjuvant treatment). This was followed by definitive surgery, radiation therapy (if clinically indicated), and adjuvant pembrolizumab or placebo to complete one full year of treatment. If radiation therapy was indicated per standard of care, adjuvant pembrolizumab or placebo was initiated either concurrently with radiation therapy, or at least 2 weeks post-radiation therapy. Adjuvant capecitabine was not permitted. The primary endpoints included pCR (defined as ypT0/Tis ypN0) and EFS in the ITT population. Key secondary endpoints included safety, OS and pCR in the PD-L1–positive population. PD-L1 expression was tested using the PD-L1 IHC 22C3 pharmDx assay; tumor specimens with CPS ≥ 1 were considered PD-L1 positive.
The first interim analysis, among the first 602 patients undergoing randomization showed that pCR rate was 64.8% [95% CI, 59.9 to 69.5] with pembrolizumab-chemotherapy versus 51.2% (95% CI, 44.1 to 58.3) with placebo-chemotherapy (∆ 13.6%, 95% CI, 5.4 to 21.8, p=0.00055). Pembrolizumab-chemotherapy increased pCR rates across all subgroups irrespective of PD-L1 status in the KEYNOTE-522 trial, unlike in the metastatic setting where PD-L1 status was predictive of pembrolizumab benefit. The pCR rate in the PD-L1–positive population was 68.9% with pembrolizumab-chemotherapy versus 54.9% with placebo-chemotherapy. By contrast, the pCR rate in the PD-L1–negative population was 45.3% with pembrolizumab-chemotherapy versus 30.3% with placebo-chemotherapy. The 3-year EFS rate, first reported at the 2021 European Society for Medical Oncology (ESMO) Virtual Meeting and subsequently published in the New England Journal of Medicine, was 84.5% with pembrolizumab-chemotherapy versus 76.8% with placebo-chemotherapy, a 7.7% absolute improvement in EFS with addition of pembrolizumab.36,37 In the pembrolizumab-treated group, 15.7% (n=123 of 784) of patients experienced any disease-related event or death compared to 23.8% (n=93 of 390) in the placebo-treated group [hazard ratio (HR) 0.63, 95% CI, 0.48 to 0.82, p=0.00031]. The distant recurrence rate was 7.7% (n=60 of 784) in the pembrolizumab-treated group versus 13.1% (n=51 of 390) in the placebo-treated group. Patients who achieved pCR had 94.4% EFS rate with pembrolizumab-containing regimen and 92.5% EFS with placebo, whereas patients with residual disease after neoadjuvant therapy had 67.4% EFS rate with pembrolizumab and 56.8% EFS with placebo. This suggests that adjuvant pembrolizumab is potentially most critical in the non-pCR setting. In the PD-L1–positive population, EFS events occurred in 14.9% of pembrolizumab-treated group versus 21.5% of placebo-treated group (HR 0.67, 95% CI, 0.49 to 0.92). In the PD-L1 negative population, EFS events occurred in 19.5% of pembrolizumab-treated group versus 36.2% of placebo-treated group (HR 0.48, 95% CI, 0.28 to 0.85). There was a trend toward OS improvement with the addition of pembrolizumab (89.7% versus 86.9%), although the data remain immature. Distant progression- or recurrence-free survival (RFS) was 87.0% with pembrolizumab versus 80.7% with placebo. On July 26, 2021, the FDA approved pembrolizumab for the treatment of patients with high-risk, early-stage TNBC.38
The incidence of treatment-related adverse events (TRAEs) of grade ≥3 across all treatment phases was 77.1% in the pembrolizumab-chemotherapy group and 73.3% in the placebo-chemotherapy group, including death in 0.5% (n=4 patients) treated with pembrolizumab and 0.3% (n=1 patient) treated with placebo. Deaths in the pembrolizumab group were attributed to sepsis, pneumonitis, pulmonary embolism, and autoimmune encephalitis. Most TRAEs and adverse events (AEs) of interest occurred in the neoadjuvant phase, were of low grade, and were largely attributed to chemotherapy. AEs of interest occurred in 38.9% of patients treated with pembrolizumab and 18.3% of patients treated with placebo. AEs of interest that were grade ≥3 occurred in 12.9% and 1.8% of patients treated with pembrolizumab and placebo, respectively, and commonly included severe skin reactions (3.8%), infusion reactions (2.6%), and adrenal insufficiency (1.3%) in the pembrolizumab-treated group. TRAEs that led to treatment discontinuation of any therapy occurred in 27.7% in the pembrolizumab-treated group and 14.1% in the placebo-treated group. Specifically, grade 3–5 immune-related AEs (irAEs) occurred in 14.9% of the pembrolizumab-treated group and 2.1% of the placebo-treated group, and led to treatment discontinuation in 10.9% and 2.6% of patients, respectively. In the adjuvant setting, grade 3–5 irAEs occurred in 2.9% and 0.3% of patients in the pembrolizumab- and placebo-treated groups, respectively. The incorporation of an additional chemotherapy drug (carboplatin) in the neoadjuvant setting, as well as neoadjuvant followed by adjuvant immunotherapy drug (pembrolizumab) requires that improved efficacy must be considered in the context of added toxicity, and comprehensive patient education of irAEs will be an essential aspect of clinical care. Therefore, rare and potentially long-lasting irAEs will need to be closely monitored in the future.
Biomarkers for Immunotherapy in TNBC
TNBC has been considered to have the highest immunogenic potential of all breast cancers, with enrichment for BRCA germline mutations and higher somatic mutational load and tumor-associated neoantigens, but are rarely associated with microsatellite instability.39,40 Thus, TNBC is a target for immune-modulating therapies.41 Early- and advanced-stage breast cancers differ in their tumor and immune cell microenvironments that may impact immunogenicity and offer therapeutic opportunities for the incorporation of checkpoint inhibitors. The predictive potential of conventional immune-based biomarkers to immunotherapy response also differ (eg, by disease stage). In the preclinical setting, high levels of tumor-specific CD8+ T cells soon after neoadjuvant immunotherapy exposure were predictive of long-term survival.42 Adjuvant immunotherapy resulted in lower tumor-specific CD8+ T cells compared to neoadjuvant-treated mice with intact tumor. Additionally, PD-L1 mRNA expression is higher in TNBC, and is associated with improved clinical outcomes.43 PD-L1 status is an established predictive biomarker of immune checkpoint inhibitor therapy response in metastatic TNBC. By contrast, the clinical benefit of immunotherapy-based treatment exists independently of PD-L1 expression for patients with early-stage TNBC, although patients with PD-L1–positive tumors achieved numerically higher pCR rates to immunotherapy-based treatment in the KEYNOTE-522 trial. Approximately 80% of patients in each treatment arm of the KEYNOTE-522 trial had PD-L1–positive disease according to the PD-L1 IHC 22C3 pharmDX assay.36 PD-L1 expression in tumor cells versus immune cells resulted in varying treatment responses to immunotherapy in early-stage TNBC.32,44 Specifically, data from the phase II GeparNuevo trial of neoadjuvant durvalumab plus chemotherapy suggested a trend for pCR rates in PD-L1 positive tumors, which was significant for PD-L1 expression in tumor cells in the durvalumab arm (p=0.045) and for PDL-1 expression in immune cells in the placebo arm (p=0.040). Tumor mutational burden (TMB) combined with immune gene expression profile also predicted pCR in this study.45
Tumor infiltrating lymphocytes (TILs) are a promising immunologic biomarker for response to neoadjuvant chemotherapy in early-stage TNBC.46–51 The presence of stromal TILs (sTILs) is prognostic in TNBC and associated with higher pCR rates to neoadjuvant therapy. A pooled analysis of 3771 patients treated with neoadjuvant therapy indicated that a 10% increase in sTILs was associated with longer disease-free survival (DFS) in TNBC patients.52 The phase III BIG 02–98 trial showed that both sTILs and intratumoral TILs (iTILs) were highest in highly proliferative tumors, and were associated with ER and HER2 negativity.53 Increasing lymphocytic infiltration in the tumor and stroma at the time of diagnosis was significantly associated with favorable prognosis in the ER-negative/HER2-negative subgroup regardless of the chemotherapy backbone. This was particularly observed in the lymphocyte-predominant breast cancer (LPBC) subgroup, defined by approximately 50–60% of TILs in the tumor specimen. Higher TIL levels in residual disease also were associated with improved RFS and OS in TNBC.54 Interestingly, some studies have reported heterogeneity in the predictive nature of TILs on treatment effect by TIL distribution - stromal versus intratumoral location. Specifically, in the GeparNuevo trial, although the presence of sTILs was associated with pCR, iTILs on pretreatment baseline biopsy did not seem to predict pCR.32 This highlights the importance of further investigation of spatial immunophenotyping in TNBC given pre-treatment tumor microenvironment composition, as well as dynamic changes in TIL composition in response to therapy, may have key implications on therapeutic strategies necessary to promote immune cell recruitment and anti-tumor immune response.51
Despite this deeper understanding of TNBC immunobiology, further development of suitable biomarkers for immunotherapy response and benefit in patients with early-stage TNBC remains an area of significant need. The standardization of biomarker assay implementation and interpretation methodologies before introducing novel biomarkers into the clinical setting will be required. Strategies to identify and target key immune suppression regulators within the tumor microenvironment that could contribute to immunotherapy resistance or predict benefit to checkpoint inhibition and optimize tumor immunogenicity will achieve a more personalized therapeutic approach and balance the risks of immunotherapy-related toxicity.
Ongoing Immunotherapy-Based Clinical Trials in Early-Stage TNBC
There are multiple ongoing clinical trials incorporating pembrolizumab and other immune-modulating strategies in early-stage TNBC [Table 2]. The NeoPACT trial is a phase II neoadjuvant study of pembrolizumab with carboplatin and docetaxel in early-stage TNBC, with pCR as the primary outcome and RFS as the secondary outcome (NCT03639948). Another ongoing study evaluates neoadjuvant pembrolizumab in combination with decitabine followed by standard neoadjuvant chemotherapy in early-stage TNBC (NCT02957968), which uses changes in lymphocyte infiltration into tumor and/or tumor stroma as the primary outcome. A phase Ib/II trial is currently evaluating the safety and efficacy of nivolumab plus cabiralizumab (anti-colony stimulating factor 1 receptor (CSF-1R) antibody) combined with neoadjuvant chemotherapy in early-stage TNBC to enhance TILs and reduce tissue-associated macrophages (NCT04331067). One phase II trial evaluates neoadjuvant pembrolizumab plus chemotherapy and immunotherapy induction regimen with IRX-2 in patients with early-stage TNBC (NCT04373031). IRX-2 is a cell-derived biologic agent that increased intratumoral T cell infiltration, improved dendritic cell function and resulted in radiologic tumor response in patients with previously untreated, surgically resectable head and neck cancer.55,56 Another window trial in the neoadjuvant setting explores the use of one cycle of pembrolizumab plus multikinase inhibitor lenvatinib in untreated TNBC before surgery (NCT04427293). Lenvatinib has demonstrated antitumor activity when paired with pembrolizumab in advanced TNBC.57
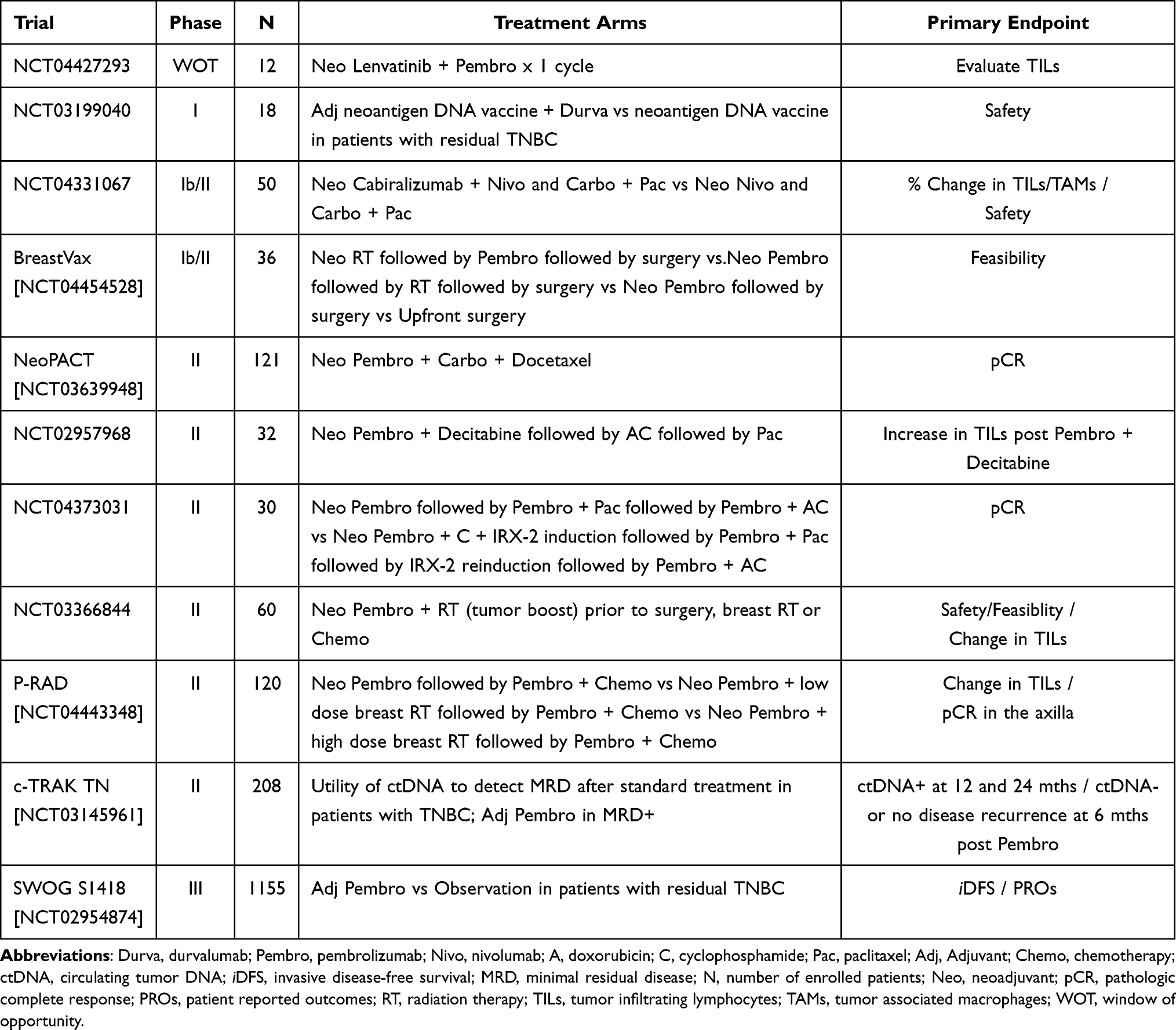 |
Table 2 Ongoing Immunotherapy-Based Clinical Trials in Early-Stage TNBC |
Several ongoing trials (NCT03366844, NCT04443348, NCT04454528) are evaluating neoadjuvant pembrolizumab and standard radiation before patients undergo chemotherapy or surgery. These trials are testing whether radiation generates antitumor effects when combined with immunotherapy.58 Other investigations are testing the effects of personalized neoantigen DNA vaccines combined with immunotherapy in residual TNBC (NCT03199040). The results from the SWOG S1418 trial of adjuvant pembrolizumab versus placebo in patients with residual disease after neoadjuvant chemotherapy are eagerly anticipated (NCT02954874). Additional studies incorporating precision medicine including next-generation sequencing are designed to guide adjuvant therapy. The c-TRAK TN phase II trial assesses serial circulating tumor DNA (ctDNA) to screen for minimal residual disease (MRD) after standard neoadjuvant therapy for early-stage TNBC (NCT03145961). Patients with positive ctDNA are randomized to receive adjuvant pembrolizumab versus observation alone.
Future Directions
The emergence of pembrolizumab in combination with chemotherapy has changed the treatment paradigm for patients with high-risk, curative-intent TNBC as it led to a statistically significant and clinically meaningful improvement in pCR rate and EFS. However, it is necessary to balance reduced risk of recurrence while minimizing potential toxicity, both treatment-related and financial, as we implement this regimen into routine clinical practice. When interpreting trial findings, it is important to note that the control arm in the KEYNOTE-522 trial did not receive dose-dense administration of anthracycline-based chemotherapy (doxorubicin and cyclophosphamide). Furthermore, no adjuvant capecitabine was provided to non-pCR patients, which may potentially magnify separation of the EFS curves between pembrolizumab-treated and placebo-treated patients. Future studies are necessary to determine the optimal chemotherapy backbone and dosing frequency as multiple clinical questions remain. First, dose-dense administration of AC in patients treated with adjuvant anthracycline-based chemotherapy followed by paclitaxel have shown modest benefit on DFS, particularly in those with ER-negative tumors.59 The IMpassion031 trial treated early-stage TNBC patients with neoadjuvant dose-dense anthracycline-based therapy combined with atezolizumab.28 The potential impact of dosing every 2 weeks versus every 3 weeks when anthracycline-based therapy is combined with immune checkpoint inhibition should be explored. Second, the incorporation of platinum agents into neoadjuvant treatment was controversial before the KEYNOTE-522 trial given the lack of consistent long-term benefit and the potential for increased myelosuppression despite improved pCR rates.16,17,60 It is currently unknown whether all patients require the addition of carboplatin to taxane, particularly now with the incorporation of immunotherapy.61 Third, additional work is necessary to examine whether anthracycline-sparing regimens could be utilized in some patients to avoid cardiotoxicity and short- and long-term hematologic toxicity. Recent modified neoadjuvant regimens have yielded encouraging pCR rates, including platinum–based regimens such as docetaxel plus carboplatin.62,63 Ongoing trials are combining immunotherapy plus platinum compounds. The chemotherapy backbone likely matters for optimal immune response. Lastly, future trials should investigate upfront immunotherapy to prime the immune response before administering chemotherapy.
There are opportunities to explore de-escalation and escalation strategies in adjuvant TNBC treatment. First, patients who achieved pCR in KEYNOTE-522 had less benefit to adjuvant pembrolizumab compared to non-pCR patients based on early EFS data. Future studies should explore biomarkers for eliminating adjuvant pembrolizumab in patients who achieve a pCR because some of the benefits may be attributed to the neoadjuvant phase of immune checkpoint inhibition. Second, the optimal choice and sequence of adjuvant systemic therapy for non-pCR patients is unknown. Future work should establish how to optimally incorporate capecitabine, a current adjuvant standard-of-care chemotherapy that improves OS in the residual disease setting.18 Clinical data in other tumor settings suggest capecitabine plus pembrolizumab is a safe combination, but future trials are needed to assess the safety and efficacy of concurrent pembrolizumab with capecitabine versus sequential therapy for TNBC patients without a pCR.64,65 Third, the PARP inhibitors olaparib and talazoparib have been approved as an additional therapeutic option for patients with germline BRCA1/2-mutant HER-2–negative metastatic breast cancer.66,67 One year of olaparib as adjuvant treatment following neoadjuvant or adjuvant chemotherapy in patients with high risk of recurrence significantly improved 3-year invasive DFS compared to placebo.68 It remains unclear whether PARP inhibitors should be used as monotherapy or combined with pembrolizumab in this setting. PARP inhibitors are DNA-damaging agents that potentially boost immune response to immunotherapy by increasing tumor-specific neoantigen release, increasing TMB, and promoting PD-L1 expression.69 The non-pCR setting also provides opportunities to explore novel investigational agents and additional combination therapies. This includes trials combining immunotherapy plus agents with novel mechanisms of action that have been approved or remain in active investigation in the metastatic setting, such as the anti-Trop2 monoclonal ADC sacituzumab govitecan, which improves OS compared to conventional chemotherapy in metastatic TNBC, or datopotamab deruxtecan.70–73 Novel HER2-directed ADCs, such as trastuzumab-deruxtecan with membrane-permeable topoisomerase I inhibitor payload, have promising activity in patients with advanced HER2-low expressing, HER2-negative breast cancer.74 Preliminary data support further investigations for combining anti-HER2 therapies with immune checkpoint inhibition in HER2-low metastatic TNBC.75
It is crucial to consider toxicity in the curative-intent setting because some survivors develop lifelong toxicities. Short- and long-term effects related to irAEs will need to be closely monitored with the addition of pembrolizumab, including some rare and potentially life-threatening toxicities that have been observed with immune checkpoint inhibition in the metastatic setting across multiple tumor types. Clinicians must remain vigilant and promptly manage immune-related toxicities leading up to definitive surgery for unrecognized irAEs such as adrenal insufficiency, which may be life-threatening, and during survivorship care planning in the curative-intent setting. It is recommended that blood cortisol levels be monitored at time of pembrolizumab therapy initiation, prior to surgery, and as clinically indicated thereafter.76 Some patients are cured with anthracycline- and taxane-based chemotherapy alone. Thus, this novel regimen overtreats a subset of patients, thereby adding additional toxicity risk without further clinical benefit. Future stratified analyses will be required to optimize patient selection for the inclusion of immunotherapy. Finally, financial toxicity from the rising cost of cancer therapeutics is an important consideration for patients, while access to this novel regimen in resource-limited countries may further magnify cancer care disparities. Strategies to improve the availability of cutting-edge treatments in these populations must be explored.77
Moving forward, it is uncertain whether pCR is the best surrogate biomarker for EFS and OS following chemo-immunotherapy. Recent studies indicate that minimal (or molecular) residual disease (MRD) may serve as a more prognostic biomarker for future clinical relapse. Early data indicate that non-pCR but MRD-negative patients may have similar outcomes to patients who achieve pCR and are MRD-negative.78 Further studies are needed to confirm this result. Thus, MRD status rather than pCR status alone may better stratify patients at higher risk of recurrence and who may benefit from adjuvant immune checkpoint inhibition. This hypothesis was recently confirmed in a retrospective analysis of the IMvigor010 study of patients with urothelial cancer.79 Although the study did not meet its primary endpoint in the overall population, improved DFS and OS was observed for MRD-positive patients who were treated with adjuvant atezolizumab. By contrast, MRD-negative patients treated with atezolizumab did not experience improved outcomes. Other biomarkers may help to refine adjuvant treatment strategies, including TMB, gene expression profiling, tumor microenvironment composition, and circulating immune cells. Future studies should investigate whether immune-based biomarkers can distinguish “hot” vs “cold” immune phenotypes to select patients who may benefit from combination immunotherapy to recruit additional T cells into the immune milieu and those who may not require immune checkpoint inhibition.
Conclusions
Recent clinical advances in the management of early-stage TNBC make cure a reality to more patients with early-stage, high-risk TNBC. This is a significant breakthrough for patients with the deadliest subtype of breast cancer. The approval of pembrolizumab based on the KEYNOTE-522 regimen marks a new era of neoadjuvant immunotherapy entering the clinic. The challenge moving forward is how to incorporate biomarkers and precision medicine approaches to define who will benefit from pembrolizumab rather than chemotherapy alone, and determine the optimal immunotherapy duration to balance the potential risks of toxicity. Adjuvant treatment trials are already planned or underway to better understand adaptive escalation or de-escalation strategies based on pCR and MRD status. Ultimately, the incorporation of pembrolizumab in the curative-intent setting is a significant step forward for patients with TNBC, and an opportunity for future studies to refine precision medicine approaches and optimize neoadjuvant and/or adjuvant immune checkpoint inhibition. These efforts will improve long-term outcomes for patients with TNBC.
Disclosure
Dr Nusayba A Bagegni reports Institutional research funding for clinical trial conduction from Sermonix Pharmaceuticals Inc, AstraZeneca, Daiichi Sankyo, Xcovery Holding Company LLC, Pfizer Inc, Ambrx Inc, Sarah Cannon Development Innovations LLC, Seattle Genetics Inc, Biovica International AB and Novartis Pharmaceuticals Inc, outside the submitted work.
Dr Foluso O. Ademuyiwa reports consulting for Eisai, Immunomedics, Astra Zeneca, Athenex, Cardinal Health, Pfizer, AbbVie, Best Doctors, and Advance Medical. Foluso O Ademuyiwa reports contracted research for Immunomedics, Pfizer, Seattle Genetics, NeoImmuneTech, RNA Diagnostics, and Astellas. The authors declare that they have no competing interests relevant to this work.
References
1. Plasilova ML, Hayse B, Killelea B, et al. Features of triple-negative breast cancer: analysis of 38,813 cases from the national cancer database. Medicine. 2016;95(35):e4614. doi:10.1097/MD.0000000000004614
2. Bagegni NA, Tao Y, Ademuyiwa FO. Clinical outcomes with neoadjuvant versus adjuvant chemotherapy for triple negative breast cancer: a report from the National Cancer Database. Plos One. 2019;14(9):e0222358.
3. Cossetti RJD, Tyldesley SK, Speers CH, et al. Comparison of breast cancer recurrence and outcome patterns between patients treated from 1986 to 1992 and from 2004. J Clin Oncol. 2015;33(1):65–73. doi:10.1200/JCO.2014.57.2461
4. Diana A, Carlino F, Franzese E, et al. Early triple negative breast cancer: conventional treatment and emerging therapeutic landscapes. Cancers. 2020;12(4):819. doi:10.3390/cancers12040819
5. Bianchini G, Balko J, Mayer I, et al. Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat Rev Clin Oncol. 2016;13(11):674–690. doi:10.1038/nrclinonc.2016.66.
6. Shah SP, Roth A, Goya R, et al. The clonal and mutational evolution spectrum of primary triple-negative breast cancers. Nature. 2012;486(7403):395–399. doi:10.1038/nature10933
7. Lehmann BD, Bauer JA, Chen X, et al. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Investig. 2011;121(7):2750–2767. doi:10.1172/JCI45014
8. Masuda H, Baggerly KA, Wang Y, et al. Clin Cancer Res. Differential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypes. Clin Cancer Res. 2013;19(19):5533–5540. doi:10.1158/1078-0432.CCR-13-0799
9. Burstein MD, Tsimelzon A, Poage GM, et al. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin Cancer Res. 2015;21(7):1688–1698. doi:10.1158/1078-0432.CCR-14-0432.
10. Liu YR, Jiang YZ, Xu XE, et al. Comprehensive transcriptome analysis identifies novel molecular subtypes and subtype-specific RNAs of triple-negative breast cancer. Breast Cancer Res. 2016;18(1):33. doi:10.1186/s13058-016-0690-8.
11. Gonzalez-Angulo AM, Timms KM, Liu S, et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin Cancer Res. 2011;17(5):1082–1089. doi:10.1158/1078-0432.CCR-10-2560
12. Toft DJ, Cryns VL. Minireview: basal-like breast cancer: from molecular profiles to targeted therapies. Mol Endocrinol. 2011;25(2):199–211. doi:10.1210/me.2010-0164
13. Costa RLB, Gradishar WJ. Triple-negative breast cancer: current practice and future directions. J Oncol Practice. 2017;13(5):301–303.
14. Fornier M, Fumoleau P. The paradox of triple negative breast cancer: novel approaches to treatment. Breast J. 2012;18(1):41–51. doi:10.1111/j.1524-4741.2011.01175.x
15. Von Minckwitz G, Untch M, Blohmer J-U, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30(15):1796–2180. doi:10.1200/JCO.2011.38.8595
16. Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13–21. doi:10.1200/JCO.2014.57.0572
17. Von Minckwitz G, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto, GBG 66): a randomized Phase 2 trial. Lancet Oncol. 2014;15(7):747–756. doi:10.1016/S1470-2045(14)70160-3
18. Masuda N, Lee S, Ohtani S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. 2017;376(22):2147–2159. doi:10.1056/NEJMoa1612645.
19. Mayer J, Zhao F, Arteaga C, et al. Randomized phase III postoperative trial of platinum-based chemotherapy versus capecitabine in patients with residual triple-negative breast cancer following neoadjuvant chemotherapy: ECOG-ACRIN EA1131. J Clin Oncol. 2021;39(23):2539–2551. doi:10.1200/JCO.21.00976
20. Liedtke C, Mazouni C, Hess MR, et al. response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–1281. doi:10.1200/JCO.2007.14.4147
21. Symmans WF, Ya C, Chen Y, et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY2 randomized clinical trial. JAMA Oncol. 2021;16:e213690. doi:10.1001/jamaoncol.2021.3690
22. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379(22):2108–2121. doi:10.1056/NEJMoa1809615
23. Schmid P, Rugo HS, Adams S, et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectable, locally advanced or metastatic triple-negative breast cancer (IMpassion 130): updated efficacy results from a randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2020;21(1):44–59.
24. Miles D, Gligorov J, Cameron AF, et al. Primary results from IMpassion 131, a double-blind, placebo-controlled, randomized phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32(8):994–1004. doi:10.1016/j.annonc.2021.05.801.
25. Virgil H. Atezolizumab TNBC indication withdrawn by manufacturer after talks with FDA; 2021. Available from: https://www.cancernetwork.com/view/atezolizumab-tnbc-indication-withdrawn-by-manufacturer-after-talks-fda.
26. Update on U.S. indication for atezolizumab in PD-L1-positive metastatic triple-negative breast cancer. The ASCO Post; 2021. Available from: https://ascopost.com/issues/september-25-2021/update-on-us-indication-for-atezolizumab-in-pd-l1-positive-metastatic-triple-negative-breast-cancer/#:~:text=Atezolizumab%20was%20granted%20accelerated%20approval,be%20approved%20in%20this%20setting.
27. Cortes J, Cescon DW, Rugo HS, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomized, placebo-controlled, double-blind, phase 3 clinical trial. Lancet. 2020;396(10265):1817–1828. doi:10.1016/S0140-6736(20)32531-9
28. Mittendorf EA, Zhang H, Barrios CH, et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomized, double-blind, phase 3 trial. Lancet. 2020;396(10257):1090–1100. doi:10.1016/S0140-6736(20)31953-X
29. Gianni L, Huang CS, Egle D, et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple negative, early high-risk and locally advanced breast cancer. NeoTRIP Michelangelo randomized study. Ann Oncol. 2022. doi:10.1016/j.annonc.2022.02.004
30. Voorwerk L, Slagter M, Horlings HM, et al. Immune induction strategies in metastatic triple-negative breast cancer to enhance the sensitivity to PD-1 blockade: the TONIC trial. Nat Med. 2019;25(6):920–928. doi:10.1038/s41591-019-0432-4
31. Loibl S, Untch M, Burchardi N, et al. Randomized phase II neoadjuvant study (GeparNuevo) to investigate the addition of durvalumab to a taxane-anthracycline containing chemotherapy in triple negative breast cancer (TNBC). J Clin Oncol. 2018;3615_suppl:104. doi:10.1200/JCO.2018.36.15_suppl.104
32. Loibl S, Untch M, Burchardi N, et al. A randomized phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol. 2019;30(8):1279–1288. doi:10.1093/annonc/mdz158
33. Nanda R, Liu MC, Yau C, et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing phase 2 adaptively randomized I-SPY2 trial. JAMA Oncol. 2020;6(5):676–684. doi:10.1001/jamaoncol.2019.6650
34. Schmid P, Salgado R, Park YH, et al. Pembrolizumab plus chemotherapy as neoadjuvant treatment of high-risk, early-stage triple-negative breast cancer: results from the Phase 1b open-label, multicohort KEYNOTE-173 study. Ann Oncol. 2020;31(5):569–581. doi:10.1016/j.annonc.2020.01.072
35. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
36. Schmid P, Cortes J, Dent R, et al. KEYNOTE-522: phase III study of neoadjuvant pembrolizumab plus chemotherapy versus placebo plus chemotherapy, followed by adjuvant pembrolizumab versus placebo for early-stage triple-negative breast cancer. ESMO Virtual Plenary. Abstract VP7-2021. Ann Oncol. 2021;32(9):1198–1200. doi:10.1016/j.annonc.2021.06.014
37. Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556–567. doi:10.1056/NEJMoa2112651
38. Food and Drugs Administartion. FDA approves pembrolizumab for high-risk early-stage triple-negative breast cancer. US: Food & Drug Administration; 2021. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-high-risk-early-stage-triple-negative-breast-cancer.
39. Heimes A, Schmidt M. Immuno-oncology in triple-negative breast cancer. J Cancer Metastasis Treat. 2021;7:9. doi:10.20517/2394-4722.2020.124
40. O’Meara TA, Tolaney SM. Tumor mutational burden as a predictor of immunotherapy response in breast cancer. Oncotarget. 2021;12(5):394–400. doi:10.18632/oncotarget.27877
41. DiCosimo S. Advancing immunotherapy for early-stage triple-negative breast cancer. Lancet. 2020;396(10257):1046–1048. doi:10.1016/S0140-6736(20)21962-0
42. Liu J, Blake SJ, Yong MCR, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov. 2016;6(12):1382–1399. doi:10.1158/2159-8290.CD-16-0577
43. Sabatier R, Finetti P, Mamessier E, et al. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget. 2015;6(7):5449–5464. doi:10.18632/oncotarget.3216
44. Planes-Laine G, Rochigneux P, Bertucci F, et al. PD-1/PD-L1 targeting in breast cancer: the first clinical evidences are emerging – a literature review. Cancers. 2019;1197:1033. doi:10.3390/cancers11071033
45. Karn T, Denkert C, Weber KE, et al. Tumor mutational burden and immune infiltration as independent predictors of response to neoadjuvant immune checkpoint inhibition in early TNBC in GeparNuevo. Ann Oncol. 2020;31:1215–1222. doi:10.1016/j.annonc.2020/05/015
46. Ibrahim EM, Al-Foheidi ME, Al-Mansour MM, et al. The prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancer: a meta-analysis. Breast Cancer Res Treat. 2014;148(2):467–476. doi:10.1007/s10549-014-3185-2
47. Denkert C, Loibl S, Noske A, et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J Clin Oncol. 2010;28(1):105–113. doi:10.1200/JCO.2009.23.7370
48. Denkert C, von Minckwitz G, Brase JC, et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J Clin Oncol. 2015;33(9):983–991. doi:10.1200/JCO.2014.58.1967
49. Brown LC, Salgado R, Luen SJ, et al. Tumor-infiltrating lymphocytes in triple-negative breast cancer: update for 2020. Cancer J. 2021;27(1):25–31. doi:10.1097/PPO.0000000000000501
50. Adams S, Gray RJ, Demaria S, et al. Prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin Oncol. 2014;32(27):2959–2966. doi:10.1200/JCO.2013.55.0491
51. Adams S, Goldstein LJ, Sparano JA, et al. Tumor infiltrating lymphocytes (TILs) improve prognosis in patients with triple negative breast cancer (TNBC). Oncoimmunology. 2015;4(9):e985930. doi:10.4161/2162402X.2014.985930
52. Denkert C, von Minckwitz G, Darb-Esfahani S, et al. Tumor-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. doi:10.1016/S1470-2045(17)30904-X
53. Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltration lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02–98. J Clin Oncol. 2013;31(7):860–867. doi:10.1200/JCO.2011.41.0902
54. Luen SJ, Salgado R, Dievi MV, et al. Prognostic implications of residual disease tumor-infiltrating lymphocytes and residual cancer burden in triple-negative breast cancer patients after neoadjuvant chemotherapy. Ann Oncol. 2019;30(2):236–242. doi:10.1093/annonc/mdy547
55. Wolf GT, Moyer JS, Kaplan MJ, et al. IRX-2 natural cytokine biologic for immunotherapy in patients with head and neck cancers. Onco Targets Ther. 2018:3731–3746. doi:10.2147/OTT.S165411
56. Schilling B, Harasymczuk M, Schuler P, et al. IRX-2, a novel immunotherapeutic, enhances functions of human dendritic cells. PLoS One. 2013;8(2):e47234. doi:10.1371/journal.pone.0047234
57. Chung HC, Saada-Bouzid E, Munoz FL, et al. Abstract PS12-07: lenvatinib plus pembrolizumab for previously treated, advanced triple-negative breast cancer: early results from the multicohort phase 2 LEAP-005 study. Cancer Res. 2021;81(4). doi:10.1158/1538-7445.SABCS20-PS12-07
58. Ho AY, Wright JL, Blitzlau RC, et al. Optimizing radiation therapy to boost systemic immune responses in breast cancer: a critical review for breast radiation oncologists. Int J Radiat Oncol Biol Phys. 2020;108(1):227–241. doi:10.1016/j.ijrobp.2020.05.011
59. Citron ML, Berry DA, Cirrincione C, et al. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of intergroup trial C9741/cancer and leukemia group B trial 9741. J Clin Oncol. 2003;21(8):1431–1439. doi:10.1200/JCO.2003.09.081
60. Petrelli F, Coinu A, Borgonovo K, et al. The value of platinum agents as neoadjuvant chemotherapy in triple-negative breast cancers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2014;144(2):223–232. doi:10.1007/s10549-014-2876-z
61. Garufi G, Palazzo A, Paris I, et al. Neoadjuvant therapy for triple-negative breast cancer: potential predictive biomarkers of activity and efficacy of platinum chemotherapy, PARP- and immune-checkpoint-inhibitors. Expert Opin Pharmacother. 2020;21(6):687–699. doi:10.1080/14656566.2020.1724957
62. Sharma P, Lopez-Tarruella S, Garcia-Saenz JA, et al. Pathological response and survival in triple-negative breast cancer following neoadjuvant carboplatin plus docetaxel. Clin Cancer Res. 2018;24(23):5820–5829. doi:10.1158/1078-0432.CCR-18-0585
63. Ademuyiwa FO, Chen I, Luo J, et al. Immunogenomic profiling and pathological response rates from a clinical trial of docetaxel and carboplatin in triple-negative breast cancer. Breast Cancer Res Treat. 2021;189(1):187–202. doi:10.1007/s10549-021-06307-3
64. Shah AN, Flaum L, Helenowski I, et al. Phase II study of pembrolizumab and capecitabine for triple negative and hormone receptor-positive, HER2-negative endocrine-refractory metastatic breast cancer. J Immunother Cancer. 2020;8(1):e000173. doi:10.1136/jitc-2019-000173
65. Bocobo AG, Wang R, Behr S, et al. Phase II study of pembrolizumab plus capecitabine and bevacizumab in microsatellite stable (MSS) metastatic colorectal cancer (mCRC): interim analysis. J Clin Oncol. 2021;393. doi:10.1200/JCO.2021.39.3_suppl.77
66. Robson M, Im S, Senkus E, et al. Olaparib for metastatic breast cancer in patients with germline BRCA mutation. N Engl J Med. 2017;377(6):523–533. doi:10.1056/NEJMoa1706450
67. Litton JK, Rugo HS, Ettl J, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018;379(8):753–763. doi:10.1056/NEJMoa1802905
68. Tutt AN, Garber JE, Kaufman B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2- mutated breast cancer. N Engl J Med. 2021;384(25):2394–2405. doi:10.1056/NEJMoa2105215
69. Vikas P, Borcherding N, Chennamadhavuni A, et al. Therapeutic potential of combining PARP inhibitor and immunotherapy in solid tumors. Front Oncol. 2020;10. doi:10.3389/fonc.2020.00570
70. Bardia A, Hurvitz S, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529–1541. doi:10.1056/NEJMoa2028485
71. Bardia A. Datopotamab deruxtecan (Dato-DXd), a TROP2-directed antibody-drug conjugate (ADC), for triple-negative breast cancer (TNBC): preliminary results from an ongoing phase 1 trial. Ann Oncol. 2021;322:S60–S78. doi:10.1016/annonc/annonc508
72. Krop I, Juric D, Shimizu T, et al. Datopotamab deruxtecan (Dato-DXd) in advanced/metastatic HER2 negative breast cancer: triple negative breast cancer results from the phase 1 TROPION-PanTumor01 study.
73. Schmid P, Nunes AT, Dry H, et al. BEGONIA: phase 1b/2, open-label, platform study of the safety and efficacy of durvalumab (D) ± paclitaxel (P) with novel oncology therapies for first-line metastatic triple-negative breast cancer (mTNBC): addition of arm 7, D + datopotamab deruxtecan (Dato-DXd; DS-1062). J Clin Oncol. 2021;39(15). doi:10.1200/JCO.2021.39.15_suppl.TPS1105
74. Modi S, Park H, Murth RK, et al. Antitumor activity and safety of trastuzumab deruxtecan in patients with HER2-low-expressing advanced breast cancer: results from a phase Ib study. J Clin Oncol. 2020;38(17):1887–1896. doi:10.1200/JCO/19.02318
75. Eiger D, Agostinetto E, Saúde-Conde R, et al. The exciting new field of HER2-low breast cancer treatment. Cancers. 2021;13(5):1015. doi:10.3390/cancers13051015
76. Guide for KEYTRUDA. Pembrolizumab prescribing information. Available from: https://www.merckaccessprogram-keytruda.com/static/pdf/guide-for-keytruda.pdf.
77. Osarogiagbon RU, Sineshaw HM, Unger JM, et al. Immune-based cancer treatment: addressing disparities in access and outcomes. Am Soc Clin Oncol Educ Book. 2021;41:1–13. doi:10.1200/EDBK_323523
78. Magbanua MJM, Swigart LB, Wu H-T, et al. Circulating tumor DNA in neoadjuvant-treated breast cancer reflects response and survival. Ann Oncol. 2021;32(2):229–239. doi:10.1016/j.annonc.2020.11.007
79. Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021;595(7867):432–437. doi:10.1038/s41586-021-03642-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.