Back to Journals » OncoTargets and Therapy » Volume 15
Targeted Therapy for Relapsed/Refractory Follicular Lymphoma: Focus on Clinical Utility of Tazemetostat
Authors Raychaudhuri R, Ujjani C
Received 21 December 2021
Accepted for publication 12 February 2022
Published 27 February 2022 Volume 2022:15 Pages 193—199
DOI https://doi.org/10.2147/OTT.S267011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Arseniy Yuzhalin
Ruben Raychaudhuri, Chaitra Ujjani
Fred Hutchinson Cancer Research Center, University of Washington, Seattle, WA, USA
Correspondence: Chaitra Ujjani, Tel +1 206-606-1955, Email [email protected]
Abstract: The management of follicular lymphoma (FL) in the relapsed and refractory setting is challenging and an area of ongoing investigation. Epigenetic dysregulation has recently been shown to be a hallmark of FL. Mutations in histone-modifying genes are likely early, driver events in FL pathogenesis, and so are attractive targets to drug. Gain-of-function mutations in the histone methyltransferase EZH2 are common in FL and maintained through disease evolution. With mounting data supporting a critical role for EZH2 as an oncogenic driver for FL, the small molecule inhibitor, tazemetostat, was developed. Tazemetostat has shown promising activity in preclinical models and early phase trials. Importantly, responses were seen in patients with high-risk features. Based on these data, tazemetostat was approved in the US in 2020 for EZH2mut patients with FL who had received at least two prior lines of systemic therapy, or for EZH2wt patients without alternative treatment options. Here, we will review the biology of FL as it pertains to tazemetostat, the available clinical trial data, and future directions for this new therapy.
Keywords: tazemetostat, follicular lymphoma, EZH2 mutation
Introduction
Follicular lymphoma (FL) is the second most common subtype of non-Hodgkin’s lymphoma (NHL) after diffuse large B-cell lymphoma (DLCBCL). Overall, FL accounts for about 12% of all NHLs, and predominantly affects older adults, with a median age of diagnosis of 60 years.1
Most patients with FL initially present with lymphadenopathy which can often wax and wane. Further workup often demonstrates the presence of widespread disease, with bone marrow involvement in up to 80% of cases, however, patients are often asymptomatic. Only 20% of patients will have B-symptoms of fatigue, night sweats, and weight loss at presentation.2 Initial treatment is primarily determined by the stage, grade, and symptoms of the patient at the time of diagnosis. Stage is assessed by the Lugano classification and can be categorized as limited (I–II) or advanced (III–IV). Grading of FL is determined by the ratio between centroblasts and centrocytes, with an increased number of centroblasts corresponding with a higher grade. While there does not appear to be a difference in survival between grade 1 and 2 FL, grade 3a disease is associated with significantly worse overall survival and increased rate of clonal evolution to transformed disease.3
Treatment for limited stage varies; observation, radiotherapy, and anti-CD20 monoclonal antibody with or without chemotherapy may be considered. In patients with advanced stage disease, the two commonly used criteria for treatment are those developed by the Groupe d-Etude des Lymphomes Folliculaires (GELF) and the British National Lymphoma Investigation (BNLI), and include cytopenias, presence of systemic B symptoms, bulky adenopathy, and compromise of organ function due to disease. The initial treatment of advanced stage FL varies, but typically involves combination chemo-immunotherapy consisting of an anti-CD20 antibody, either rituximab or obinutuzumab. Many patients will have an excellent response to front-line therapy and experience a lengthy progression-free survival (PFS). These patients can be treated intermittently over the course of decades. Approximately 20% of patients will have progression of disease within 24 months (POD24) of first-line chemoimmunotherapy. POD24 has emerged as an important surrogate endpoint which correlates with poor survival.4 An additional population of concern is primary refractory, these patients also have a worse prognosis.5
Management of relapsed and refractory (R/R) patients is much more challenging and an area of active investigation. The observational National Lymphocare study demonstrated markedly inferior PFS with subsequent lines of therapy, highlighting the unmet need for more effective therapies with unique mechanisms of action.6 There are few novel therapies currently approved for relapsed FL patients. These include the combination of rituximab and lenalidomide, phosphoinositide 3’-kinase (PI3K) inhibitors, and anti-CD19 directed CAR T-cell therapy. There are four PI3K inhibitors approved, including idelalisib, copanlisib, duvelisib, and most recently, umbralisib. The overall response rates (ORRs) with these agents range from 40–60%, with few complete responses, and median PFS of a year.7–10 These agents are associated with significant toxicity and often require discontinuation or dose reduction. In the ZUMA-5 study, axicabtagene ciloleucel produced an impressive ORR of 94% in multiply relapsed follicular lymphoma; the median PFS has not yet been reached.11 While quite effective, the durability of CAR T-cell therapy has not yet been defined and administration is associated with significant short-term and long-term adverse events.
More options are needed for patients with multiply relapsed follicular lymphoma, and in January 2020, tazemetostat, a small molecule inhibitor of the enhancer of zeste homolog 2 (EZH2) received US Food and Drug Administration (FDA) approval. In this review, we will discuss mechanism of action, the available data regarding the safety and efficacy, and future directions for tazemetostat for the treatment of FL.
Mechanism of Action of Tazemetostat
Epigenetic features such as DNA methylation, histone modifications, and chromatin structure regulation, are commonly dysregulated in cancer, and minor alterations in epigenetic regulators can have a cascade effect in promoting oncogenesis.12,13 DNA hypomethylating agents and histone deacetylation inhibitors have had remarkable efficacy in T cell lymphoma, myelodysplastic syndrome, acute myeloid leukemia, and multiple myeloma, however success with these agents in NHL have thus far been limited.14
However, next-generation sequencing studies have shown that histone-modifying genes are especially common and highly selected for in follicular lymphoma, suggesting the importance of epigenetic factors in the genesis of this condition.15 Remarkably, one study of 22 FL tumor samples identified mutations in one or more chromatin modifier genes within 96% of FL tumors and two or more in 76% of tumors.16 While the clonal hierarchy is not completely understood, some of the somatic mutations involved in epigenetic pathways are likely early, driver events in lymphomagenesis and so are conceptually attractive and rational targets to drug.17,18 Unfortunately, the two most commonly mutated epigenetic regulators, CREBBP and KMT2D, are loss-of-function events and therefore challenging to target.
EZH2, the target of tazemetostat, is another commonly mutated protein in FL involved in epigenetic regulation. Gain of function mutations in EZH2 lead to alterations in substrate specificity and trigger vast reorganization in chromatin structure and in mouse models promote tumorigenesis.19 EZH2 encodes a histone methyltransferase responsible for trimethylating Lys27 of histone H3 (H3K27).20 EZH2 is highly expressed in germinal center B-cells (GCB), facilitating cell cycle progression and preventing terminal differentiation while inactivation leads to a profound impairment in germinal center responses and memory B-cell formation.21,22 EZH2 is then considered to be a master regulator of the germinal center, with persistent expression maintaining the GCB reaction.
Gain of function mutations in three recurrent hotspots (Y646, A682, A692) affecting the catalytic SET domain of the EZH2 molecule, are reported in 17–27% of patients with FL depending on the modality of assessment.23 Supporting the key role of EZH2 in maintaining the GC phenotype, EZH2 mutations are also observed in 22% of diffuse large B-cell lymphoma (DLBCL) in the GCB subtype, and not observed in the non-GCB subtype.24
Sequential mutational studies show that EZH2 mutations are often maintained throughout FL evolution, although EZH2 mutations were observed to be gained or lost in some rare, paired cases of FL and transformed FL.23,24 Interestingly, EZH2 mutations are always heterozygous in patient tumors. This is thought to be due to cooperation observed between wild-type and mutant EZH2 to promote H3K27 methylation, as the mutant allele has reduced activity in catalyzing the addition of the first and second methyl groups.25
In addition to its intrinsic role in B-cell differentiation, EZH2 is also critically important in regulating the tumor microenvironment.26 Disruption of EZH2 activity in intra-tumoral regulatory T-cells has been shown to promote cancer immunity.27 EZH2 mediated histone methylation also represses tumor production of chemokines which subsequently impairs effector T cell trafficking. In animal models of ovarian and colorectal cancer, epigenetic modulation of EZH2 activity increased effector T cell tumor infiltration and improved the efficacy of PD-L1 and CTLA-4 blockade.28,29 Mutant EZH2 in FL models also leads to profound alterations in T-follicular helper cells which further drives FL growth and tumorigenesis.30
Given the mounting data supporting a critical role for EZH2 as a common oncogenic driver in follicular lymphoma, many groups worked to identify candidate small molecule inhibitors.19,31–34 From these efforts, a candidate compound EPZ-6438 (tazemetostat) was identified with good oral bioavailability with similar potency in inhibiting both mutant and wild type EZH2. Tazemetostat led to sustained and sometimes complete tumor regression in EZH2-mutant NHL xenograft-bearing mice. The best responses were seen in xenografts bearing the EZH2 A682G mutation. Slower tumor growth was seen in EZH2 wild type xenograft models, but otherwise tumor regression was not observed, suggesting a greater role for the compound in EZH2 mutated follicular lymphoma.35
Clinical Evidence for Tazemetostat
Upon the results of these encouraging preclinical data, the first in human phase I clinical trial for tazemetostat was initiated in France in 2013.36 (Table 1). Sixty-four patients were enrolled from a variety of tumor types, including 21 patients with non-Hodgkin lymphoma, seven of whom had follicular lymphoma. The presence of an EZH2 mutation was not a requirement for enrollment. The most common grade 3 or higher adverse event was thrombocytopenia and was the primary dose-limiting toxicity. Four patients with FL had an objective response, two of which were a complete response (CR). The median time to response was about three months. EZH2 mutational analysis was performed retrospectively in using the PCR-based cobas EZH2 Mutation Test to assess for known gain-of-function mutations. One patient was identified with an EZH2 mutation and had a durable partial response before disease progression at 16 months. The investigators determined a recommended Phase 2 dose of 800 mg twice daily based upon pharmacodynamic and toxicity profiling.
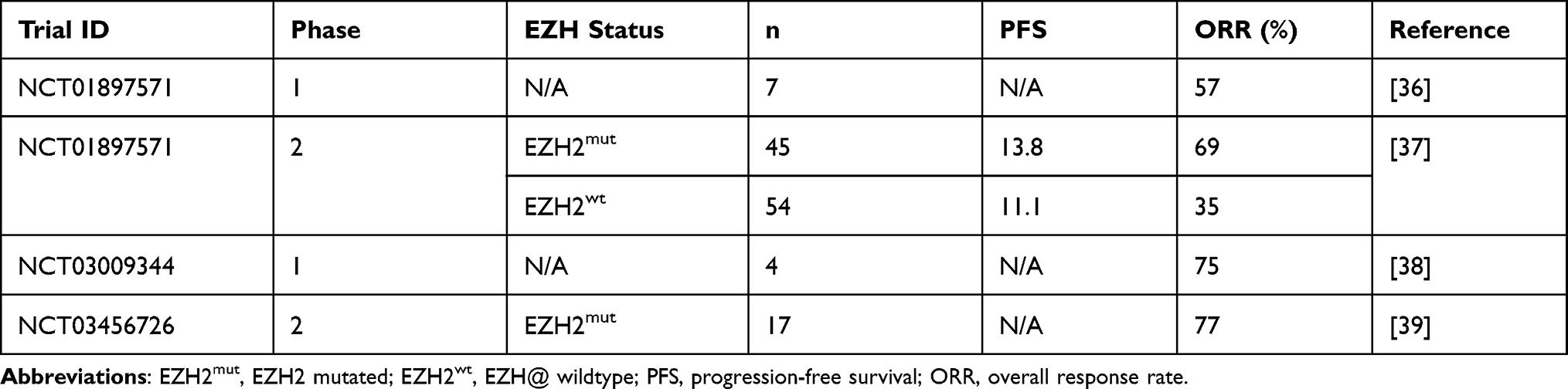 |
Table 1 Summary of Trials of Tazemetostat Monotherapy in R/R FL |
Based on this efficacy and safety data, a single-arm phase 2 trial of tazemetostat in relapsed/refractory non-Hodgkin’s lymphoma was performed.37 This study included six cohorts. Patients with either EZH2mut or EZH2wt FL were enrolled into one of two FL cohorts. Patients with any grade FL, including histologically transformed FL were eligible. Patients were required to have relapsed/refractory disease following at least two standard prior systemic treatment regimens including at least one anti-CD20 based regimen. Those with central nervous system disease or grade 3 or higher cytopenias were excluded. The primary endpoint was ORR based on IWG-NHL 2007 criteria. Secondary endpoints were duration of response, PFS, and safety and tolerability. A total of 99 patients were enrolled, 45 patients were EZHmt and 54 EZH2wt. There were several notable differences between the cohorts. The EZH2wt patient group was more heavily pre-treated (median three lines compared with two in the mutant group), and more likely to have previously received a stem-cell transplant (39% versus 9%). The wild type group also contained three patients with transformed histology, compared with zero patients in the mutant group.
The objective response rate in the EZH2mut cohort was 69% compared with 35% in the EZH2wt cohort, including complete responses in 13% and 4% in mutant and wild type groups respectively. While EZH2mut patients were more likely to respond, the response durability was similar between groups. Progression-free survival was relatively similar between groups, 13.8 months in EZH2mut and 11.1 months in EZH2wt. The median duration of response was 10.9 months in the EZH2mut cohort and 13 months in the EZH2wt cohort. Eleven patients completed two years of therapy and entered a roll-over study and continued treatment. Responses were also observed in high-risk subgroups, especially in the EZH2mut group. For instance, in patients with POD24, 63% of patients harboring an EZH2mut and 25% in the wild type cohort, had a response, with complete response rates of 11% and 3% respectively. The median time to first response was 3.7 months, similar to that seen in the Phase 1 trial. Tazemetostat was relatively well tolerated. Nine patients (9%) required dose reduction, and eight patients (8%) discontinued tazemetostat due to a treatment-emergent adverse event, five (5%) of which were considered to be treatment related. There were two secondary myeloid neoplasms seen in this trial; one case of myelodysplastic syndrome at 15.3 months and one case of acute myeloid leukemia at 25.8 months, both of which may have reflected prior chemotherapy exposure. Other events leading to drug discontinuation included oral fungal infection, prolonged QT interval, pneumonia, and thrombocytopenia. Based on the results of the results of this phase 2 trial, the FDA granted accelerated approval to tazemetostat for patients with EZH2 mutated R/R follicular lymphoma who had received at least two prior systemic therapies and for EZH2 wild type follicular lymphoma who have no satisfactory alternative treatment options.
There have been simultaneous studies performed with tazemetostat in Japan.38 In a phase I trial of seven patients, four of whom had R/R FL, no serious adverse events were observed. Three in four patients with FL had a response, one of whom had a detectable EZH2 mutation. In a multicenter phase 2 study of 17 patients with R/R follicular lymphoma with EZH2 mutations, the ORR was 76.5%, with six (35.3%) achieving CR.39 The median time to response was 3.64 months. The median PFS was not met. The most common adverse effects in this trial were dysgeusia (50%) and lymphopenia (25%); three patients discontinued the drug due to treatment emergent adverse events, namely atypical pneumonia, dysgeusia, and muscle spasticity.
Given the relatively encouraging safety signal and single agent activity, there have been several small studies examining tazemetostat in combination with other agents. Tazemetostat was combined with R-CHOP in a phase I study in older patients with newly diagnosed DLBCL with high-risk disease. This trial did not reveal any new concerning safety signals, and there was no significant additional hematologic toxicity. Patients tolerated the 800 mg twice-daily dose used for monotherapy.40 In another phase 1 study, tazemetostat was combined with the anti-programmed death-ligand 1 (PD-L1) atezolizumab in patients with R/R DLBCL. 35% of patients had a serious adverse event, most commonly anemia, neutropenia, or thrombocytopenia. The median PFS was 1.9 months, and the ORR was 16%. EZH2 mutations were identified in 17% of patients, and 60% of EZHmt did have a response.41
Combination studies are also being conducted in R/R FL, including two trials that were presented at the American Society of Hematology 2021 annual meeting. Based on preclinical data demonstrating synergy between tazemetostat and lenalidomide and the well-established efficacy data with rituximab with lenalidomide, a phase 1b/3 study evaluating the triplet was performed in patients who had received at least one prior therapy.42,43 In the phase 1b portion of the study, three dose levels of tazemetostat were explored: 400 mg (n = 4), 600 mg (n = 4), and 800 mg (n = 6) twice daily. Patients received rituximab 375 mg/m2 on days 1, 8, 15, and 22 of cycle 1 and day 1 of cycles 2–5 and lenalidomide 20 mg on days 1–21 of cycles 1–12. Each cycle was 28 days. There were no dose-limiting toxicities. Grade 3 or higher adverse events were reported in 50% of patients; the most frequent was neutropenia in 21%. The most common all grade adverse events were nausea in 43% and headache in 36%. Of the 12 patients who were evaluable for response assessment, the ORR was 92% with a CR rate of 42%. The median duration of exposure was 17 weeks (range 8–28). The single arm phase II study of tazemetostat in combination with rituximab in R/R FL is also ongoing.44 As part of this single arm study, patients will receive rituximab 375 mg/m2 weekly during cycle 1 and on day 1 of cycles 3–6 for a total of 8 cycles and tazemetostat 800 mg twice daily for 24 cycles (28 days each).
Discussion
The novel EZH2 inhibitor, tazemetostat, is an important addition to the armamentarium for relapsed/refractory follicular lymphoma. By providing a mechanism of action distinct from other agents currently approved in this space, patients have an opportunity for improved outcomes, including those with high-risk features such as POD24 and double-refractory disease. The FDA granted accelerated approval based upon phase II data which demonstrate anti-tumor efficacy in patients refractory to two or greater lines of chemo-immunotherapy. This approval has been incorporated into the NCCN guidelines for treatment of R/R FL. It is important to note that there appears to be clinical benefit regardless of EZH2 status, providing disease control even in EZH2wt patients.
Given the relatively comparable PFS curves between EZH2mut and EZH2wt FL, one may consider molecular testing to be primarily academic for these heavily pretreated patients. In addition, EZH2mut appears to be a positive prognostic factor for response to cyclophosphamide-containing regimens such as CHOP/CVP as opposed to bendamustine regimens.45 Regardless, these trials were not designed to compare these cohorts and there were many differences in patient characteristics, and so we feel there is a role for EZH2 analysis to be useful in terms of patient education and expectations, especially in light of the disparate response rates.
The median time to response with tazemetostat was greater than three months, a finding which was reproduced in both phase 2 studies. Response assessments were undertaken every eight weeks, and so this result is unlikely to be an artifact of the trial design. As responses can often deepen with longer exposure, sufficient time should be permitted if clinically appropriate before changing regimens.
Further clinical investigation of tazemetostat is needed to better define its place in the increasingly complex landscape of the treatment of R/R FL. Given the modest PFS, questions remain regarding how best to sequence this agent and whether there is a role for combination with other agents. Although head to head trials are not available, the drug appears a reasonable option after chemoimmunotherapy and rituximab in combination with lenalidomide in patients who are not candidates for cellular therapy, including autologous stem cell transplant and/or CAR T-cell therapy. As tazemetostat is well tolerated, it may be considered over PI3K inhibitors in patients who are EZH2mut or EZH2wt patients with certain comorbidities. Given tazemetostat’s novel mechanism of action and tolerable safety profile, results from ongoing and future combination studies may allow for earlier administration. It is an ideal agent for combination with other targeted therapies.
Tazemetostat is the product of an improved understanding of the pathogenesis of follicular lymphoma over the past decade. The data for its use in patients with EZH2 mutations, especially in high-risk patients with few other options, are encouraging. Further studies are needed to define its impact on overall survival, its place in the sequence of therapies, and its role in combination with other agents.
Funding
There is no funding to report.
Disclosure
CU reports consulting for Epizyme, AbbVie, Atara, Pharmacyclics, Gilead, Janssen, Beigene, Lilly, and Incyte. The authors report no other conflicts of interest in this work.
References
1. Teras LR, Desantis CE, Cerhan JR, et al. 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J Clin. 2016;66(6):443–459. doi:10.3322/CAAC.21357
2. Freedman A. Follicular lymphoma: 2018 update on diagnosis and management. Am J Hematol. 2018;93(2):296–305. doi:10.1002/AJH.24937
3. Swerdlow SH; International Agency for Research on Cancer, World Health Organization. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. International Agency for Research on Cancer; 2008.
4. Casulo C, Byrtek M, Dawson KL, et al. Early relapse of follicular lymphoma after rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone defines patients at high risk for death: an analysis from the national lymphocare study. J Clin Oncol. 2015;33(23):2516. doi:10.1200/JCO.2014.59.7534
5. Alonso-Álvarez S, Manni M, Montoto S, et al. Primary refractory follicular lymphoma: a poor outcome entity with high risk of transformation to aggressive B cell lymphoma. Eur J Cancer. 2021;157:132–139. doi:10.1016/J.EJCA.2021.08.005
6. Link BK, Day BM, Zhou X, et al. Second-line and subsequent therapy and outcomes for follicular lymphoma in the United States: data from the observational National Lymphocare Study. Br J Haematol. 2019;184(4):660–663. doi:10.1111/BJH.15149
7. Gopal AK, Kahl BS, de Vos S, et al. PI3Kδ inhibition by idelalisib in patients with relapsed indolent lymphoma. N Engl J Med. 2014;370(11):1008–1018. doi:10.1056/NEJMOA1314583
8. Matasar MJ, Capra M, Özcan M, et al. Copanlisib plus rituximab versus placebo plus rituximab in patients with relapsed indolent non-Hodgkin lymphoma (CHRONOS-3): a double-blind, randomised, placebo-controlled, Phase 3 trial. Lancet Oncol. 2021;22(5):678–689. doi:10.1016/S1470-2045(21)00145-5
9. Flinn IW, Miller CB, Ardeshna KM, et al. DYNAMO: a Phase II study of duvelisib (IPI-145) in patients with refractory indolent non-hodgkin lymphoma. J Clin Oncol. 2019;37(11):912–922. doi:10.1200/JCO.18.00915
10. Fowler NH, Samaniego F, Jurczak W, et al. Umbralisib, a dual PI3Kδ/CK1ε inhibitor in patients with relapsed or refractory indolent lymphoma. J Clin Oncol. 2021;39(15):1609–1618. doi:10.1200/JCO.20.03433
11. Jacobson C, Chavez JC, Sehgal AR, et al. Primary analysis of zuma-5: a phase 2 study of Axicabtagene ciloleucel (Axi-Cel) in patients with Relapsed/refractory (R/R) indolent non-Hodgkin lymphoma (iNHL). Blood. 2020;136(Supplement1):40–41. doi:10.1182/BLOOD-2020-136834
12. Lawrence MS, Stojanov P, Mermel CH, et al. Discovery and saturation analysis of cancer genes across 21 tumour types. Nature. 2014;505(7484):495–501. doi:10.1038/nature12912
13. Cao J, Yan Q. Cancer epigenetics, tumor immunity, and immunotherapy. Trends Cancer. 2020;6(7):580–592. doi:10.1016/J.TRECAN.2020.02.003
14. Bennett RL, Licht JD. Targeting epigenetics in cancer. Annu Rev Pharmacol Toxicol. 2018;58:187–207. doi:10.1146/ANNUREV-PHARMTOX-010716-105106
15. Morin RD, Mendez-Lago M, Mungall AJ, et al. Frequent mutation of histone-modifying genes in non-Hodgkin lymphoma. Nature. 2011;476(7360):298–303. doi:10.1038/nature10351
16. Green MR, Kihira S, Liu CL, et al. Mutations in early follicular lymphoma progenitors are associated with suppressed antigen presentation. Proc Natl Acad Sci U S A. 2015;112(10):E1116–E1125. doi:10.1073/PNAS.1501199112/-/DCSUPPLEMENTAL
17. Green MR, Gentles AJ, Nair RV, et al. Hierarchy in somatic mutations arising during genomic evolution and progression of follicular lymphoma. Blood. 2013;121(9):1604. doi:10.1182/BLOOD-2012-09-457283
18. Korfi K, Ali S, Heward JA, Fitzgibbon J. Follicular lymphoma, a B cell malignancy addicted to epigenetic mutations. Epigenetics. 2017;12(5):370. doi:10.1080/15592294.2017.1282587
19. Qi W, Chan H, Teng L, et al. Selective inhibition of Ezh2 by a small molecule inhibitor blocks tumor cells proliferation. Proc Natl Acad Sci. 2012;109(52):21360–21365. doi:10.1073/PNAS.1210371110
20. Margueron R, Reinberg D. The polycomb complex PRC2 and its mark in life. Nature. 2011;469(7330):343–349. doi:10.1038/nature09784
21. Caganova M, Carrisi C, Varano G, et al. Germinal center dysregulation by histone methyltransferase EZH2 promotes lymphomagenesis. J Clin Invest. 2013;123(12):5009. doi:10.1172/JCI70626
22. Béguelin W, Popovic R, Teater M, et al. EZH2 is required for germinal center formation and somatic EZH2 mutations promote lymphoid transformation. Cancer Cell. 2013;23(5):677. doi:10.1016/J.CCR.2013.04.011
23. Bödör C, Grossmann V, Popov N, et al. EZH2 mutations are frequent and represent an early event in follicular lymphoma. Blood. 2013;122(18):3165–3168. doi:10.1182/BLOOD-2013-04-496893
24. Morin RD, Johnson NA, Severson TM, et al. Somatic mutations altering EZH2 (Tyr641) in follicular and diffuse large B-cell lymphomas of germinal-center origin. Nat Genet. 2010;42(2):181–185. doi:10.1038/ng.518
25. Green MR. Chromatin modifying gene mutations in follicular lymphoma. Blood. 2018;131(6):595. doi:10.1182/BLOOD-2017-08-737361
26. Wang X, Brea LT, Yu J. Immune modulatory functions of EZH2 in the tumor microenvironment: implications in cancer immunotherapy. Am J Clin Exp Urol. 2019;7(2):85. PMC6526357/.
27. Wang D, Quiros J, Mahuron K, et al. Targeting EZH2 reprograms intratumoral regulatory T cells to enhance cancer immunity. Cell Rep. 2018;23(11):3262. doi:10.1016/J.CELREP.2018.05.050
28. Peng D, Kryczek I, Nagarsheth N, et al. Epigenetic silencing of Th1 type chemokines shapes tumor immunity and immunotherapy. Nature. 2015;527(7577):249. doi:10.1038/NATURE15520
29. Nagarsheth N, Peng D, Kryczek I, et al. PRC2 epigenetically silences Th1-type chemokines to suppress effector T-cell trafficking in colon cancer. Cancer Res. 2016;76(2):275–282. doi:10.1158/0008-5472.CAN-15-1938
30. Béguelin W, Teater M, Meydan C, et al. Mutant EZH2 induces a pre-malignant lymphoma Niche by reprogramming the immune response. Cancer Cell. 2020;37(5):655–673.e11. doi:10.1016/J.CCELL.2020.04.004
31. Garapaty-Rao S, Nasveschuk C, Gagnon A, et al. Identification of EZH2 and EZH1 small molecule inhibitors with selective impact on diffuse large B cell lymphoma cell growth. Chem Biol. 2013;20(11):1329–1339. doi:10.1016/J.CHEMBIOL.2013.09.013
32. Diaz E, Machutta CA, Chen S, et al. Development and validation of reagents and assays for EZH2 peptide and nucleosome high-throughput screens. J Biomol Screen. 2012;17(10):1279–1292. doi:10.1177/1087057112453765
33. Bradley WD, Arora S, Busby J, et al. EZH2 inhibitor efficacy in non-Hodgkin’s lymphoma does not require suppression of H3K27 monomethylation. Chem Biol. 2014;21(11):1463–1475. doi:10.1016/J.CHEMBIOL.2014.09.017
34. McCabe MT, Ott HM, Ganji G, et al. EZH2 inhibition as a therapeutic strategy for lymphoma with EZH2-activating mutations. Nature. 2012;492(7427):108–112. doi:10.1038/nature11606
35. Knutson SK, Kawano S, Minoshima Y, et al. Selective inhibition of EZH2 by EPZ-6438 leads to potent antitumor activity in EZH2-mutant non-Hodgkin lymphoma. Mol Cancer Ther. 2014;13(4):842–854. doi:10.1158/1535-7163.MCT-13-0773
36. Italiano A, Soria JC, Toulmonde M, et al. Tazemetostat, an EZH2 inhibitor, in relapsed or refractory B-cell non-Hodgkin lymphoma and advanced solid tumours: a first-in-human, open-label, phase 1 study. Lancet Oncol. 2018;19(5):649–659. doi:10.1016/S1470-2045(18)30145-1
37. Morschhauser F, Tilly H, Chaidos A, et al. Tazemetostat for patients with relapsed or refractory follicular lymphoma: an open-label, single-arm, multicentre, phase 2 trial. Lancet Oncol. 2020;21(11):1433–1442. doi:10.1016/S1470-2045(20)30441-1
38. Munakata W, Shirasugi Y, Tobinai K, et al. Phase 1 study of tazemetostat in Japanese patients with relapsed or refractory B‐cell lymphoma. Cancer Sci. 2021;112(3):1123. doi:10.1111/CAS.14822
39. Izutsu K, Ando K, Nishikori M, et al. Phase II study of tazemetostat for relapsed or refractory B‐cell non‐Hodgkin lymphoma with EZH2 mutation in Japan. Cancer Sci. 2021;112(9):3627. doi:10.1111/CAS.15040
40. Sarkozy C, Morschhauser F, Dubois S, et al. A LYSA phase Ib study of tazemetostat (EPZ-6438) plus R-CHOP in patients with newly diagnosed diffuse large B-cell lymphoma (DLBCL) with poor prognosis features. Clin Cancer Res. 2020;26(13):3145–3153. doi:10.1158/1078-0432.CCR-19-3741
41. Palomba ML, Cartron G, Popplewell L, et al. Safety and clinical activity of atezolizumab in combination with tazemetostat in relapsed or refractory diffuse large B-cell lymphoma: primary analysis of a phase 1B study. Hematol Oncol. 2019;37:517–519. doi:10.1002/HON.203_2631
42. Tong KI, Yoon S, Isaev K, et al. Combined EZH2 inhibition and IKAROS degradation leads to enhanced antitumor activity in diffuse large B-cell lymphoma. Clin Cancer Res. 2021;27(19):5401–5414. doi:10.1158/1078-0432.CCR-20-4027
43. Batlevi C, Park S, Nastoupil L, et al. Interim analysis of the randomized Phase 1b/3 study evaluating the safety and efficacy of tazemetostat plus lenalidomide and rituximab in patients with relapsed/refractory follicular lymphoma. Blood. 2021;138(Supplement 1):2207. doi:10.1182/blood-2021-148199
44. Patel K, Bailey N, Miller K, et al. A phase 2, single-arm, open-label, multicenter study of tazemetostat in combination with rituximab for the treatment of relapsed or refractory follicular lymphoma. Blood. 2021;138(Supplement 1):3571. doi:10.1182/blood-2021-148199
45. Jurinovic V, Passerini V, Oestergaard MZ, et al. Evaluation of the m7-FLIPI in patients with follicular lymphoma treated within the Gallium trial: EZH2 mutation status may be a predictive marker for differential efficacy of chemotherapy. Blood. 2019;134(Supplement_1):122. doi:10.1182/BLOOD-2019-130208
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.