Back to Journals » Infection and Drug Resistance » Volume 19
Targeted Next-Generation Sequencing Reveals Distinct Pathogen Profiles in Community-Acquired Pneumonia Across Age and Disease Severity
Authors Cui S ![]() , Wen B
, Wen B ![]() , Wang Y
, Wang Y ![]() , Yang X
, Yang X ![]() , Fan F
, Fan F ![]() , Zhao M, Jiang Y, Yu X
, Zhao M, Jiang Y, Yu X ![]()
Received 9 January 2026
Accepted for publication 25 February 2026
Published 4 March 2026 Volume 2026:19 587244
DOI https://doi.org/10.2147/IDR.S587244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Shu Cui,1,* Bing Wen,1,* Ying Wang,2 XiaoJie Yang,1 FangFang Fan,3 MengQing Zhao,2 Yi Jiang,3 Xiao Yu3
1The First Clinical Medical College of Shanxi Medical University, Taiyuan, People’s Republic of China; 2The School of Public Health College of Shanxi Medical University, Taiyuan, People’s Republic of China; 3NHC Key Laboratory of Pneumoconiosis, Shanxi Key Laboratory of Chronic Respiratory Diseases and Pneumoconiosis, The First Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao Yu, NHC Key Laboratory of Pneumoconiosis, Department of Pulmonary and Critical Care Medicine, The First Hospital of Shanxi Medical University, No. 85, South Jie Fang Road, Taiyuan, 030000, People’s Republic of China, Email [email protected] Yi Jiang, NHC Key Laboratory of Pneumoconiosis, Department of Pulmonary and Critical Care Medicine, The First Hospital of Shanxi Medical University, No. 85, South Jie Fang Road, Taiyuan, 030000, People’s Republic of China, Email [email protected]
Background: Community-acquired pneumonia (CAP) represents a substantial global health burden; however, the characteristics of its etiological spectrum remain incompletely defined. Targeted next-generation sequencing (tNGS) has significantly advanced the understanding of the etiological spectrum. This study aimed to investigate the pathogen characteristics in CAP patients across different age groups and severity levels based on tNGS results.
Methods: We retrospectively analyzed the etiological test results of 272 hospitalized CAP patients at the First Hospital of Shanxi Medical University (Taiyuan, China) from 2021 to 2024. Patients were stratified by age and Pneumonia Severity Index (PSI) score, and their clinical characteristics, etiological spectrum, and infection patterns were systematically evaluated.
Results: Among the 145 patients included in the final analysis, 34.48% had simple infections, while 65.52% had multiple infections. Elderly patients (≥ 80 years) exhibited the highest proportion of mixed infections (81.82%), with the detection rates of viruses and fungi—such as Epstein-Barr virus, Human herpesvirus 5, Candida glabrata, and Candida albicans—increasing significantly with advancing age. Younger patients (18– 39 years) were more susceptible to atypical pathogen infections (eg, Mycoplasma pneumoniae). The proportion of mixed infections in severe cases was significantly higher than that in mild cases (76.92% vs 59.14%), and triple co-infections (involving bacteria, viruses, and fungi) were significantly concentrated in the severe group. Significant specific differences in the composition of the etiological spectrum were also observed among different age and severity groups; for instance, the detection rates of Klebsiella spp. and Acinetobacter baumannii were higher in the elderly and severe groups, whereas atypical pathogens were mainly concentrated in the young group.
Conclusion: The etiological spectrum of CAP exhibits significant differences across different age groups and disease severity levels. Therefore, stratified diagnosis and therapeutic strategies should be developed based on age and disease severity to optimize prognosis and reduce the misuse of antibiotics.
Keywords: community-acquired pneumonia, age stratification, disease severity, pathogen, tNGS
Introduction
Community-acquired pneumonia (CAP) is one of the most common and severe lower respiratory tract infections worldwide, with its incidence and mortality increasing markedly with age. In 2021, lower respiratory tract infections—including pneumonia and bronchiolitis—accounted for an estimated 344 million cases globally, with a mortality rate of 27.7 per 100,000 population, peaking at 224.6 per 100,000 among individuals aged ≥70 years.1 The high infection rate in individuals aged >70 years may be attributed to multiple factors, including senescence, decline in immune function, comorbidities, malnutrition, and long-term antibiotic exposure. In China, CAP poses a particularly heavy burden, with an incidence of 7.13 per 1000 person-years and over 9.5 million cases reported in 2016, most frequently affecting the elderly.2 Beyond mortality, CAP also leads to substantial healthcare expenditures in Europe, estimated at €10.1 billion annually,3 and significantly impairs post-discharge quality of life in older adults with comorbidities or recurrent disease.4
Early identification of the causative pathogen plays a critical role in guiding targeted antimicrobial therapy and improving clinical outcomes in CAP.5 Despite the emergence of molecular diagnostic technologies, conventional culture-based methods remain the most widely used approach in hospital settings due to their low cost, widespread availability, and ability to provide antimicrobial susceptibility testing. However, these methods identify pathogens in only about one-third of CAP cases, highlighting the need for more sensitive diagnostic approaches,6 owing to their low sensitivity, long turnaround times, and high false-negative rates. This diagnostic gap hampers timely initiation of appropriate therapy, particularly in patients with atypical or mixed infections. Moreover, accumulating evidence suggests that pathogen distributions in CAP vary by patient age and disease severity,7 underscoring the need for stratified diagnostic strategies.
Next-generation sequencing (NGS) technologies have emerged as powerful tools for infectious disease diagnostics, offering broader detection ranges and higher sensitivity than conventional methods.8,9 Among available approaches—metagenomic NGS (mNGS), whole-genome sequencing (WGS), and targeted NGS (tNGS)—the latter is particularly well suited for clinical practice. By enriching pathogen nucleic acids with specific primers or probes, tNGS achieves higher detection rates, reduced host background interference, and faster turnaround at lower cost compared with mNGS, while outperforming culture in sensitivity and efficiency.10 These features enable rapid (24–48 hour) results for timely treatment decisions and offer cost-effectiveness suitable for routine hospital use, positioning tNGS as an optimal balance between comprehensive pathogen detection and clinical practicality—making it an attractive method for real-world pathogen identification in CAP.
Despite its promise, limited studies have systematically applied tNGS to delineate the etiological spectrum of CAP across different age groups and severity strata. This knowledge gap has important clinical implications, as empirical antibiotic selection remains largely based on historical data that may not reflect current pathogen distributions, particularly in the post-COVID-19 era. To address this gap, we performed tNGS on bronchoalveolar lavage fluid (BALF) samples from hospitalized CAP patients. We characterized the microbial spectrum and infection patterns, stratified by age and Pneumonia Severity Index (PSI) score, aiming to provide novel insights into age- and severity-specific pathogen distributions that could inform targeted antimicrobial strategies and personalized clinical decision-making. The findings from this study have the potential to guide stratified empirical therapy, optimize antimicrobial stewardship, and ultimately improve clinical outcomes in CAP patients.
Materials and Methods
Participant Recruitment
This retrospective cohort study was conducted with informed consent from all participants. Patients diagnosed with community-acquired pneumonia (CAP) who were admitted to the Department of Respiratory and Critical Care Medicine at the First Hospital of Shanxi Medical University between August 2021 and August 2024 were enrolled. The diagnosis of CAP was based on the Chinese Guidelines for the Diagnosis and Treatment of Community-Acquired Pneumonia in Adults (2016 Edition).11
All enrolled patients underwent bronchoscopy and bronchoalveolar lavage (BAL), and the bronchoalveolar lavage fluid (BALF) samples were subjected to targeted next-generation sequencing (tNGS). Clinical data were simultaneously collected for further analysis.
Patients were stratified into four age groups (18–39, 40–59, 60–79, and ≥80 years) and further categorized by disease severity based on the Pneumonia Severity Index (PSI), with classes I–III defined as the mild group and classes IV–V as the severe group.12 The exclusion criteria were as follows: (1) incomplete clinical data; (2) coexisting respiratory diseases such as pulmonary tuberculosis, pulmonary malignancy, non-infectious interstitial lung disease, bronchiectasis, chronic obstructive pulmonary disease (COPD), or asthma; (3) concurrent malignancies; and (4) immunosuppression resulting from bone marrow suppression, immunosuppressive therapies, or other causes. These exclusion criteria were applied to ensure the homogeneity of the study cohort and to accurately reflect the etiological characteristics of CAP in immunocompetent hosts. Patients with coexisting chronic respiratory diseases (eg, COPD, bronchiectasis) were excluded to avoid misinterpretation of chronic colonizing flora as acute causative pathogens. Patients with concurrent malignancies or immunosuppression were excluded because their underlying conditions predispose them to opportunistic infections, which would introduce significant bias into the analysis of pathogen distribution and clinical outcomes.
BALF samples were obtained under local anaesthesia using a standardised flexible bronchoscopy protocol. A minimum volume of 10 mL was collected into sterile sampling containers and transported under cold-chain conditions. Upon receipt, 2 mL of BALF was transferred into RNA-protecting tubes, and the remaining sample was aliquoted into DNA-free tubes for storage at −80 °C.13
Targeted next-generation sequencing (tNGS) was performed using ultra-multiplex PCR and sequencing technology.14 The panel covered 418 clinically relevant pathogens, including bacteria, fungi, viruses, and atypical pathogens, encompassing >95% of commonly encountered CAP-related organisms. The reported analytical sensitivity and specificity of the assay both exceeded 96% according to internal validation data.
Statistical Analysis
Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation (SD) and compared using one-way analysis of variance (ANOVA). Non-normally distributed data were reported as median with interquartile range (IQR) and compared using the Mann–Whitney U-test.
Categorical variables were presented as frequencies and percentages, with group comparisons conducted using the chi-square test or Fisher’s exact test as appropriate.
All statistical analyses were performed using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). A two-tailed P value <0.05 was considered statistically significant.
Results
Age- and Severity-Related Variations in Clinical Profiles and Outcomes of CAP
A total of 145 hospitalized patients diagnosed with CAP were included in this study. The flow of patient identification and inclusion is detailed in Figure 1. The demographic characteristics, laboratory parameters, length of stay, and mortality rates of patients stratified by age and pneumonia severity index (PSI) classification are presented in Table 1. Significant differences in inflammatory responses, physiological indicators, and clinical outcomes were observed across age groups and disease severity levels. The median age of patients in the severe group was significantly higher than in the mild group (74 vs 58 years, P < 0.01). Among the age strata, patients aged ≥80 years had the highest median age (84 years). In the severe group, the proportion of male patients was higher (76.9%), indicating a potential association between sex and disease severity. In terms of inflammatory biomarkers, levels of white blood cell count (WBC), neutrophil percentage (NEU), and procalcitonin (PCT) were markedly elevated in both the severe and elderly (≥80 years) groups, suggesting enhanced systemic inflammatory activity. Conversely, lymphocyte counts (LYM) were significantly reduced in these groups (P < 0.01), which may reflect immune suppression. Respiratory function parameters also differed by severity. Patients in the severe group exhibited lower arterial oxygen partial pressure (pO2) compared to those in the mild group (64.2 vs 74.3 mmHg, P = 0.05), indicating more severe oxygenation impairment. Additionally, patients aged ≥80 years had elevated arterial carbon dioxide partial pressure (pCO2), potentially reflecting age-related decline in ventilatory capacity. Clinical outcomes varied by disease severity. Patients in the severe group had a longer median hospital stay (14.5 vs 11 days, P < 0.01) and a significantly higher in-hospital mortality rate (17.3% vs 1.08%, P < 0.01) compared to those in the mild group. These findings highlight marked heterogeneity in the clinical profiles of CAP patients across age and severity strata, underscoring the need for age- and risk-adapted therapeutic strategies.
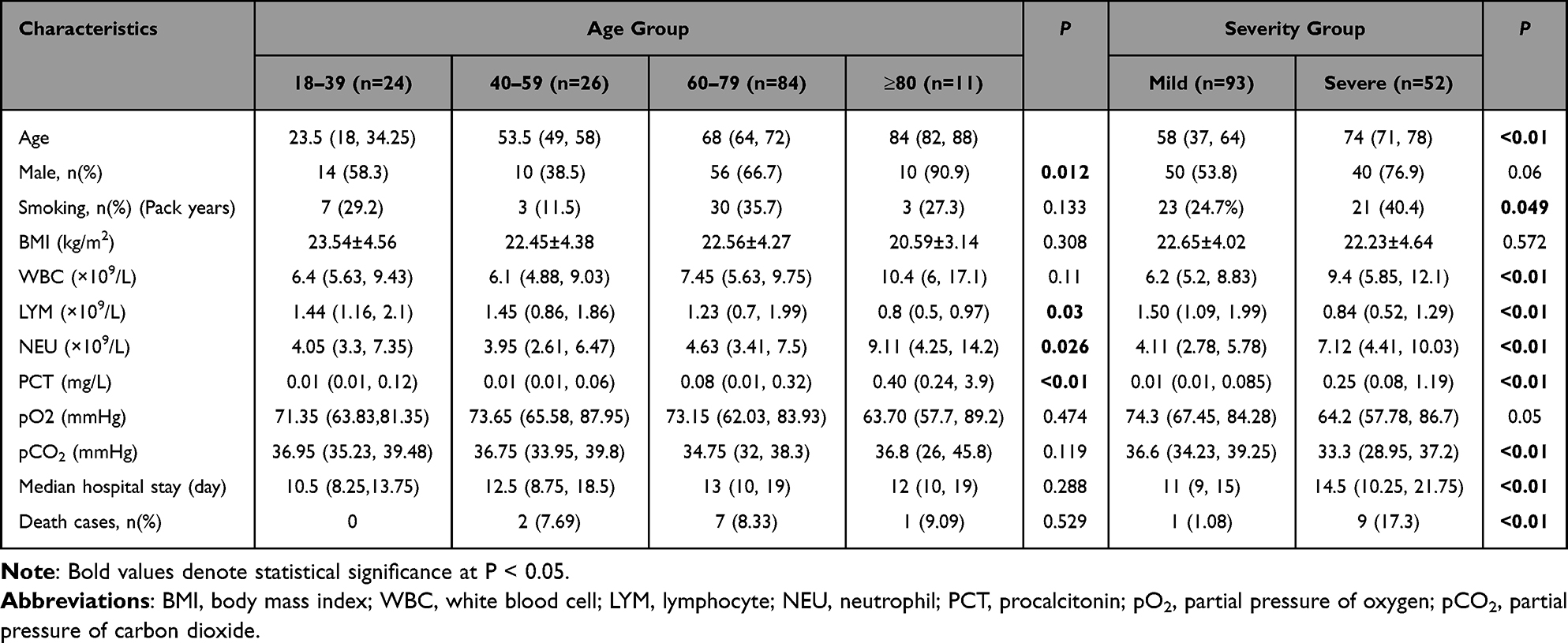 |
Table 1 Clinical Characteristics |
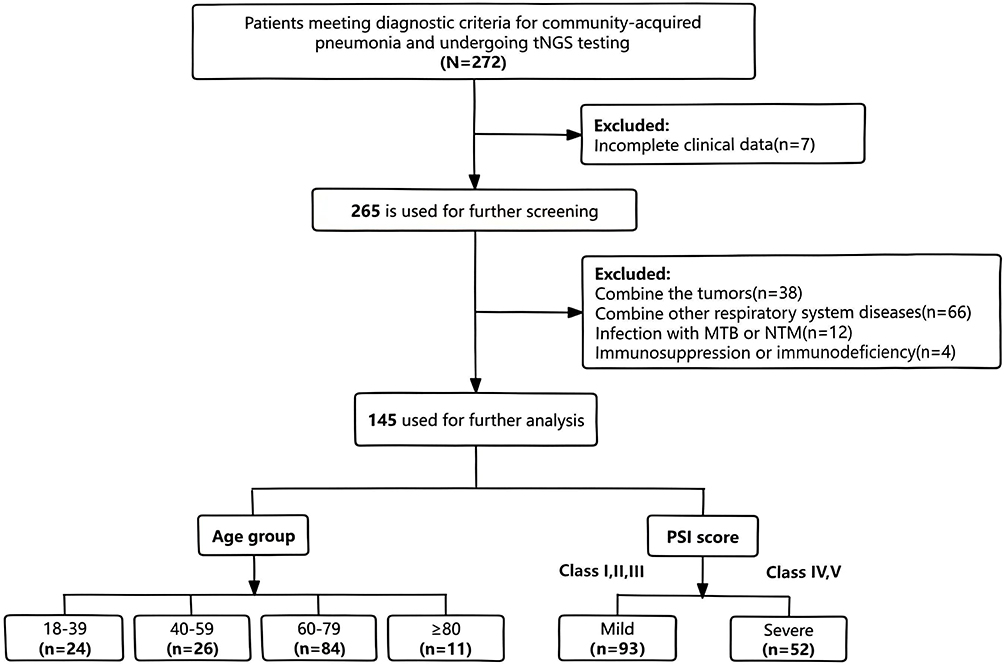 |
Figure 1 Flow diagram of study identification and inclusion. |
Infection Patterns and Pathogen Spectrum in CAP Patients
Among the 145 CAP patients, 50 cases (34.48%) had simple infections, while 95 cases (65.52%) had multiple infections. Among simple infections, bacterial pathogens were the most prevalent, accounting for 78%. Within multiple infections, bacterial-viral co-infections were the most common, representing 46.32% of cases, followed by co-infections involving bacteria, viruses, and fungi, which accounted for 26.31% (Figure 2A and B). In bronchoalveolar lavage fluid samples from 145 patients with community-acquired pneumonia (CAP), a total of 106 pathogenic microorganisms were detected (Figure 2C), including 64 bacterial species (60.4%), 24 viral species (22.5%), 14 fungal species (13.2%), and 4 atypical pathogens (3.8%).
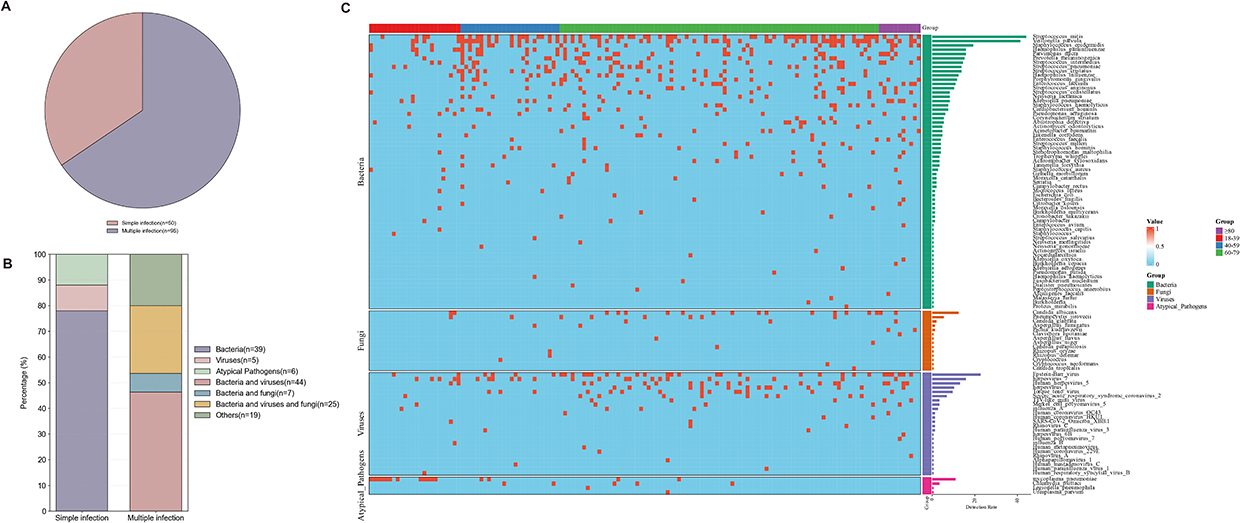 |
Figure 2 Microbial distribution in patients with CAP. (A) Infection patterns in 145 CAP patients. (B) Categorization of pathogenic infections and the proportion of each category. (C) Distribution of microbial infection among patients with CAP. |
Age-Stratified Differences in the Pathogen Spectrum of CAP
Age was also closely associated with the composition of the pathogen spectrum in CAP patients. A total of 38 pathogen species were detected in the 18–39 years group, 4 of which were unique to this group; 50 pathogen species (7 unique ones) were detected in the 40–59 years group; the 60–79 years group had the most abundant pathogens, with 84 species detected (29 unique ones); and 44 pathogen species (9 unique ones) were detected in the ≥80 years group (Figure 3A). The detection rates of some bacteria, such as Klebsiella pneumoniae, Klebsiella oxytoca, Staphylococcus aureus, and Enterococcus faecium, were relatively higher in the ≥80 years population. Certain pathogens, including Acinetobacter baumannii and Corynebacterium striatum, were only detected in patients over 60 years old, with their detection rates gradually increasing with age. Regarding viruses, multiple viruses such as Human coronavirus OC43, Human metapneumovirus, Human coronavirus HKU1, and Human mastadenovirus C were only detected in populations over 60 years old, while Human respiratory syncytial virus B and Influenza B virus were only found in patients aged 18–39 years. Influenza A virus and Severe acute respiratory syndrome coronavirus 2 were detected in all age groups, with relatively uniform distribution. Atypical pathogens (eg, Mycoplasma pneumoniae) were mainly concentrated in the young groups; the detection rate in patients aged 18–39 years was significantly higher than that in other age groups, and it decreased significantly with increasing age, with no detection in the ≥80 years group. Other pathogens such as Chlamydia psittaci and Legionella pneumophila were only occasionally detected in middle-aged and elderly groups.
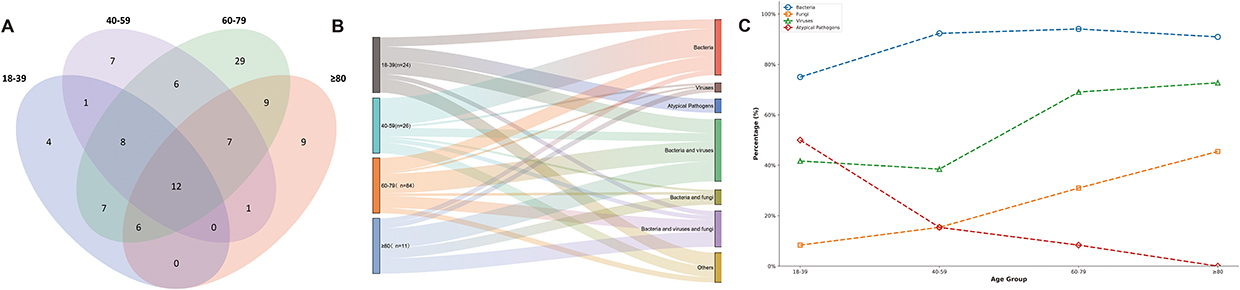 |
Figure 3 Microbial distribution among CAP patients in different age groups. (A) Venn diagram showing unique and shared pathogen species across age groups. (B) Categorization of pathogenic infections and the proportion of each category. (C) Detection rates of different pathogen categories. |
Age-Related Patterns of Bacterial, Viral, and Atypical Pathogen Infections in CAP
There were significant differences in the distribution of infection types among different age groups (Figure 3B). The proportion of simple infections was relatively higher in the 18–39 years and 40–59 years age groups, accounting for 41.67% and 53.85%, respectively. In contrast, multiple infections dominated in the 60–79 years and ≥80 years age groups, with proportions reaching 71.43% and 81.82%, respectively. Among all simple infections, bacterial infections were the most common, with the highest proportion in the 40–59 years group (41.67%) and the lowest in the ≥80 years group (9.09%). Notably, monoviral infections had the highest proportion in elderly patients (≥80 years, 9.09%), while no monoviral infections were observed in patients aged 18–39 years. In contrast, monotypic atypical pathogen infections only occurred in the 18–39 years group, accounting for 25%, indicating that atypical pathogens may specifically affect young populations.
Bacterial–Viral and Triple Infections as Dominant Patterns in Elderly CAP
With increasing age, the types of infections in patients tended to be more diverse and complex. multiple infections were particularly prevalent in populations over 60 years old, mainly consisting of bacterial-viral co-infections, which accounted for 35.71% in the 60–79 years group and 36.36% in the ≥80 years group, respectively. The proportion of triple infections (bacteria + virus + fungus) also increased significantly in the elderly groups, reaching 27.28% in the ≥80 years group (Figure 3B). These findings suggest that elderly CAP patients face a higher risk of co-pathogenicity by multiple pathogens, and a more comprehensive assessment of potential pathogens is required during clinical diagnosis and treatment.
Age-Dependent Trends in Pathogen Detection
With the change in age, the detection rates of different types of pathogens also varied among age groups. The overall detection rate of bacteria remained high, with no significant changes across different age groups. The detection rates of viruses and fungi generally increased with age. However, the detection rate of atypical pathogens was the highest in the 18–39 years age group, and then gradually decreased with increasing age (Figure 3C).
In conclusion, the distribution of infection types and pathogen spectrum in CAP patients shows a significant age dependence. Particularly in the elderly population, the risks of multiple infections and viral/fungal infections are significantly increased, which requires attention in clinical prevention and control.
Severity-Stratified Differences in Clinical Characteristics and Outcomes
There were differences in pathogen composition between patients with different disease severities. Analysis based on the Venn diagram (Figure 4A) showed that a total of 81 pathogen species were detected in the mild group, 31 of which were unique to this group; 74 pathogen species were detected in the severe group, with 24 being unique; and 50 pathogen species were shared between the two groups. These findings suggest distinct differences in the infection spectrum between the two groups, emphasizing the need for targeted optimization of pathogen screening strategies for each group.
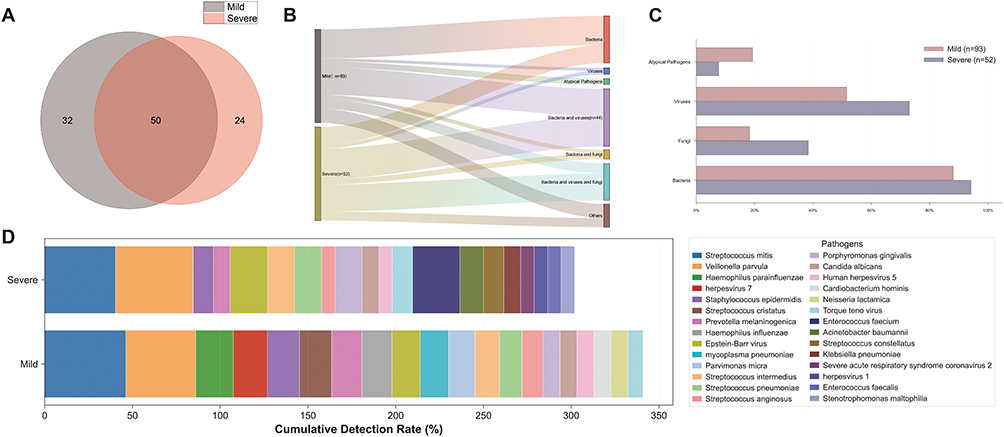 |
Figure 4 Microbial distribution in mild versus severe CAP groups. (A) Venn diagram showing unique and shared pathogen species between severity groups. (B) Categorization of pathogenic infections and the proportion of each category. (C) Detection rates of different pathogen categories. (D) Top 20 microorganisms ranked by detection frequency. |
This study found that the severity of CAP was closely associated with the type of infection. The proportion of simple infections was 40.86% in the mild group, while it decreased to 23.08% in the severe group. Correspondingly, multiple infections were the dominant type in both groups, but their proportion increased significantly in the severe group, rising from 59.14% in the mild group to 76.92% in the severe group. This indicates a positive correlation between disease progression and the complexity of infection.
Increased Prevalence of Multiple and Triple Infections in Severe CAP
Further analysis revealed that bacterial infections were the most common among simple infections, accounting for 31.18% in the mild group. Monoviral infections had a slightly higher proportion in the severe group (3.85%), while monotypic infections caused by atypical pathogens were only observed in the mild group (6.45%). Among multiple infections, bacterial-viral co-infections were the most frequent combination, accounting for 29.03% in the mild group and 32.69% in the severe group. Notably, the proportion of triple co-infections (involving bacteria, viruses, and fungi) increased significantly in the severe group, reaching 28.85%, which was much higher than the 10.75% in the mild group (Figure 4B).
Severity-Associated Trends in Pathogen Detection
As shown in Figure 4C, with the aggravation of CAP, the composition of pathogens underwent a structural change. The detection rates of fungi and viruses in the severe group were significantly higher than those in the mild group, whereas the mild group showed a higher proportion of infections caused by atypical pathogens. This change suggests that in clinical practice, pathogen screening directions and anti-infective strategies should be reasonably adjusted according to the severity of patients’ conditions. In particular, the risk of multiple mixed infections in severe patients requires heightened vigilance.
Pathogen Spectrum Differences Between Mild and Severe CAP
In terms of microbial composition, there were significant differences in the distribution of the top 20 pathogens between mild and severe CAP patients (Figure 4D). For bacteria, Moraxella catarrhalis and Haemophilus haemolyticus were only detected in the mild group; the detection rates of Haemophilus influenzae, Haemophilus parainfluenzae, Prevotella melaninogenica, Micromonas micros, and Staphylococcus haemolyticus were also higher in the mild group than in the severe group. In contrast, Acinetobacter baumannii, Klebsiella oxytoca, Enterococcus avium, Bacteroides fragilis, Pseudomonas putida, and Klebsiella aerogenes were only detected in the severe group, showing a strong association with disease severity.
For viruses, Human rhinovirus A, Human parainfluenza virus 1, and Human coronavirus OC43 were exclusively found in the severe group; the detection rates of Severe acute respiratory syndrome coronavirus 2 (including its variant XXB.1), Human rhinovirus C, Human parainfluenza virus 3, and Influenza A virus were also higher in the severe group than in the mild group. On the contrary, Influenza B virus, Human metapneumovirus, Human coronavirus 229E, Human mastadenovirus C, Human respiratory syncytial virus B, and Human coronavirus HKU1 were only detected in the mild group.
In addition, the distribution of atypical pathogens also differed between groups: the detection rate of Mycoplasma pneumoniae was significantly higher in the mild group than in the severe group, while Chlamydia psittaci and Legionella spp. were more frequently detected in severe patients.
Discussion
Previous studies have identified Streptococcus pneumoniae and respiratory viruses, such as human rhinovirus and influenza virus, as the most common pathogens of CAP,15,16 with other pathogens including Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus, and atypical microorganisms such as Legionella spp., Mycoplasma pneumoniae, and Chlamydophila pneumoniae.17 However, in recent years, the etiology of CAP has been constantly changing due to the extensive use of antibiotics, changes in climate and environment, and particularly the outbreak of the coronavirus disease 2019 (COVID-19) pandemic. Non-pharmaceutical interventions during the COVID-19 pandemic—including stay-at-home orders, school and community closures, and mask mandates—suppressed the circulation of common respiratory viruses such as influenza, RSV, and human metapneumovirus, while the subsequent relaxation of these measures led to a re-increase in infections, particularly rhinovirus.18 Additionally, COVID-19 has been associated with a higher propensity for bacterial co-infections, further complicating clinical management.19 These shifts underscore the need for continuous monitoring of CAP etiology in the post-pandemic era. The development of sequencing technologies has also provided new tools for further identifying pathogenic bacteria. In this study, tNGS was used to systematically analyze the infection types and pathogen spectrum of 145 patients with CAP, revealing significant differences across different age groups and disease severity levels. The results showed that both age and disease severity were closely associated with infection complexity and pathogen distribution, indicating that the etiological characteristics of CAP exhibit obvious age dependence and stratified features.
We found that with increasing age, the infection type of CAP patients showed a trend of transitioning from simple infection to multiple infection. Particularly in the population aged ≥80 years, patients were more prone to multiple infections, and the infection types were more complex—among these, bacterial-viral co-infections accounted for the highest proportion, and the proportion of triple infections (involving bacteria, viruses, and fungi) also increased significantly with age. This phenomenon may be related to factors such as immunosenescence, comorbid chronic underlying diseases, and long-term medical exposure. Notably, the detection rates of viruses and fungi were significantly higher in elderly patients, while young populations were more susceptible to infections caused by atypical pathogens such as Mycoplasma pneumoniae. The high prevalence of M. pneumoniae in young patients may be attributed to multiple factors, including transmission dynamics favoring close-contact settings such as schools and workplaces, age-related immunity differences whereby older adults acquire partial protection from prior infections while younger individuals lack such antibodies,20 and high macrolide resistance rates in China (>90%) that may prolong illness and pathogen shedding, thereby increasing transmission opportunities in socially active young populations.21,22 This suggests that age may be a key factor influencing susceptibility to atypical pathogens; therefore, when formulating anti-infective treatment regimens for young patients, more attention should be paid to infections caused by atypical pathogens, especially Mycoplasma pneumoniae. This finding is consistent with some previous epidemiological studies, but it also implies that early detection and intervention of viruses and fungi should be strengthened during the diagnosis and treatment of elderly populations to reduce the risks of diagnostic delay and insufficient treatment.
This study also revealed age-specific trends in the pathogen spectrum of CAP patients across different age groups. The 60–79 years group had the most abundant pathogens, with significantly more unique species than other groups; in contrast, young populations showed high susceptibility to atypical pathogens. Such differences may reflect variations in immune response, respiratory microbiota, and pathogen exposure patterns among populations of different ages. Clinically, these results suggest that patient age should be fully considered when developing diagnosis and treatment strategies to optimize etiological detection and anti-infective treatment regimens.
It is important to note that 3 cases of Pseudomonas aeruginosa were detected in young patients in this study, and none of these 3 patients were admitted to the intensive care unit (ICU), had structural lung disease, or were immunocompromised. Studies have shown that the incidence of CAP caused by Pseudomonas aeruginosa is 2% in patients with no prior Pseudomonas aeruginosa infection/colonization and no chronic lung diseases such as bronchiectasis or chronic obstructive pulmonary disease (COPD).23 We speculate that Pseudomonas aeruginosa infection in these patients may be related to the previous irregular use of broad-spectrum antibiotics, highlighting the need for greater caution in antibiotic use.
Secondly, CAP patients with different severity levels exhibited distinct infection characteristics. Atypical pathogens are more common in patients with mild disease severity,7,24 which is consistent with the results of our study, suggesting that CAP caused by Mycoplasma pneumoniae is relatively mild. Severe CAP is associated with more complex infection types, higher detection rates of viruses and fungi, and a higher prevalence of multiple infections. Studies have shown that the inflammatory pattern of CAP patients with multiple infections differs from that of patients with simple infections, with a more intense inflammatory response,25 which may be related to Interferon (IFN)-γ-induced protein 10.26 A Spanish study demonstrated that among the microbial etiologies of CAP, Gram-negative Enterobacteriaceae, Staphylococcus aureus, and mixed etiologies were associated with the highest mortality rates.7 A 2022 Chinese study on severe community-acquired pneumonia showed that influenza viruses, Streptococcus pneumoniae, and Enterobacteriaceae bacteria were the main causes of severe pneumonia.27 Another multicenter study found that influenza viruses, Klebsiella pneumoniae, Staphylococcus aureus, and respiratory syncytial virus (RSV) were closely associated with severe infections, and Klebsiella pneumoniae was linked to poor outcomes.28 In our study, Acinetobacter baumannii, Stenotrophomonas maltophilia, Corynebacterium striatum, and Escherichia coli were associated with severe CAP; in addition, the detection rates of Enterococcus avium, Enterococcus faecium, and Staphylococcus aureus in the severe group were significantly higher than those in the mild group. This suggests that these pathogens may cause more severe pneumonia, which requires further research for verification. Regarding viral infections, the detection rates of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), Influenza A virus, parainfluenza virus, and rhinovirus C in patients with severe pneumonia were significantly higher than those in patients with mild pneumonia, and these viruses were mostly accompanied by bacterial co-infections. Therefore, more attention should be paid to viral infections when screening pathogens and formulating anti-infective regimens for patients with severe CAP.
Current perspectives suggest that in addition to the previously recognized pathogenic microorganisms, the etiology of CAP may also include certain normal respiratory flora, which also have potential pathogenicity.29 However, these normal respiratory flora are usually not identified by traditional microbiology laboratories. A study by Daniel M Musher found that the previously reported normal respiratory flora appeared to play a pathogenic role in 25.8% of CAP cases, causing CAP under certain conditions such as aspiration, decreased immunity, and disruption of respiratory microbiota.30 In our study, the detection rate of normal respiratory microorganisms was relatively high: the detection rate of Streptococcus mitis was as high as 44.14%, Veillonella parvula was 41.38%, and Streptococcus intermedius and Streptococcus cristatus were both around 14%. Previous studies have shown that Streptococcus mitis shares the same molecular characteristics as Streptococcus pneumoniae, can also form capsules, and can cause severe infections in humans.31,32 Therefore, we have reason to include these normal respiratory flora in the pathogen spectrum of CAP, and further studies are needed to clarify their potential role in the development of CAP.
This study still has certain limitations. First, the sample size was relatively small, and the study subjects were limited to a single center; thus, the generalizability of the results to other regions and populations needs to be verified. Second, bronchoalveolar lavage fluid (BALF) was used as the detection sample in this study. Although BALF can well reflect the pathogen spectrum of the lower respiratory tract, it may still be affected by sampling depth, background flora, and the sensitivity of detection technologies. In addition, the inference of pathogenicity for some pathogens was mainly based on detection results, lacking further activity verification and correlation analysis with host responses. Therefore, future multicenter studies with larger cohorts are needed to validate our findings across diverse populations. Standardization of BALF sampling protocols is also warranted to minimize procedural variability and guide precision diagnostic strategies for CAP.
Conclusion
For elderly patients, clinical practice should prioritize the risk of multiple infections, particularly early identification of viruses and fungi; for young patients, screening for atypical pathogens should be emphasized; and for severe patients, rapid multi-pathogen detection and optimized empirical anti-infective strategies are essential to reduce mortality.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Xiao Yu) upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the First Hospital of Shanxi Medical University (Approval No. KYLL-2023-091. All samples and data were collected with the informed consent of the participants.
Acknowledgments
We thank all patients for participating in the study.
Author Contributions
Shu Cui and Bing Wen share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Fundamental Research Program of Shanxi Province (202503021211269) and the Shanxi Provincial University Young Teachers’ Sci-Tech Innovation Support Program (2025Q012).
Disclosure
The authors declare no competing interests.
References
1. Bender RG, Sirota SB, Swetschinski LR. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies, 1990–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2024;24(9):974–13. doi:10.1016/s1473-3099(24)00176-2
2. Sun Y, Li H, Pei Z, et al. Incidence of community-acquired pneumonia in urban China: a national population-based study. Vaccine. 2020;38(52):8362–8370. doi:10.1016/j.vaccine.2020.11.004
3. Tsoumani E, Carter JA, Salomonsson S, Stephens JM, Bencina G. Clinical, economic, and humanistic burden of community acquired pneumonia in Europe: a systematic literature review. Expert Rev Vaccines. 2023;22(1):876–884. doi:10.1080/14760584.2023.2261785
4. Andrade LF, Saba G, Ricard JD, et al. Health related quality of life in patients with community-acquired pneumococcal pneumonia in France. Health Qual Life Outcomes. 2018;16(1):28. doi:10.1186/s12955-018-0854-6
5. Messacar K, Parker SK, Todd JK, Dominguez SR, Kraft CS. Implementation of rapid molecular infectious disease diagnostics: the role of diagnostic and antimicrobial stewardship. J Clin Microbiol. 2017;55(3):715–723. doi:10.1128/jcm.02264-16
6. Carugati M, Aliberti S, Reyes LF, et al. Microbiological testing of adults hospitalised with community-acquired pneumonia: an international study. ERJ Open Res. 2018;4(4):00096–2018. doi:10.1183/23120541.00096-2018
7. Cillóniz C, Ewig S, Polverino E, et al. Microbial aetiology of community-acquired pneumonia and its relation to severity. Thorax. 2011;66(4):340–346. doi:10.1136/thx.2010.143982
8. Deurenberg RH, Bathoorn E, Chlebowicz MA, et al. Application of next generation sequencing in clinical microbiology and infection prevention. J Biotechnol. 2017;243:16–24. doi:10.1016/j.jbiotec.2016.12.022
9. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14(1):319–338. doi:10.1146/annurev-pathmechdis-012418-012751
10. Li S, Tong J, Liu Y, Shen W, Hu P. Targeted next generation sequencing is comparable with metagenomic next generation sequencing in adults with pneumonia for pathogenic microorganism detection. J Infect. 2022;85(5):e127–e129. doi:10.1016/j.jinf.2022.08.022
11. Qu JM, Cao B. [Guidelines for the diagnosis and treatment of adult community acquired pneumonia in China (2016 Edition)]. Zhonghua Jie He He Hu Xi Za Zhi. 2016;39(4):241–242. Danish. doi:10.3760/cma.j.issn.1001-0939.2016.04.001
12. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336(4):243–250. doi:10.1056/nejm199701233360402
13. Chinese Thoracic Society. [Consensus of clinical pathways of metagenomic next-generation sequencing test in diagnosis of lower respiratory tract infections in China]. Zhonghua Jie He He Hu Xi Za Zhi. 2023;46(4):322–335. Danish. doi:10.3760/cma.j.cn112147-20220701-00553
14. Society of Clinical Microbiology of China International Exchange and Promotion Association for Medical and Healthcare. [Expert consensus on the application and practice of targeted next-generation sequencing in infectious diseases]. Zhonghua Yi Xue Za Zhi. 2024;104(48):4375–4383. Danish. doi:10.3760/cma.j.cn112137-20240927-02208
15. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med. 2015;373(5):415–427. doi:10.1056/NEJMoa1500245
16. Johansson N, Kalin M, Tiveljung-Lindell A, Giske CG, Hedlund J. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis. 2010;50(2):202–209. doi:10.1086/648678
17. Aliberti S, Dela Cruz CS, Amati F, Sotgiu G, Restrepo MI. Community-acquired pneumonia. Lancet. 2021;398(10303):906–919. doi:10.1016/s0140-6736(21)00630-9
18. Redlberger-Fritz M, Kundi M, Aberle SW, Puchhammer-Stöckl E. Significant impact of nationwide SARS-CoV-2 lockdown measures on the circulation of other respiratory virus infections in Austria. J Clin Virol. 2021;137:104795. doi:10.1016/j.jcv.2021.104795
19. Menis AA, Gerovasileiou E, Mantzarlis K, et al. The effect on mortality of bacterial co-infections on critically ill patients with community-acquired COVID-19 and influenza pneumonia: a systematic review. Viruses. 2025;17(6):851. doi:10.3390/v17060851
20. Waites KB, Talkington DF. Mycoplasma pneumoniae and its role as a human pathogen. Clin Microbiol Rev. 2004;17(4):697–728, table of contents. doi:10.1128/cmr.17.4.697-728.2004
21. Dekyi, Xiao Y, Wang X, et al. Predominance of A2063G mutant strains in the Mycoplasma pneumoniae epidemic in children: a clinical and epidemiological study in 2023 in Wuhan, China. Int J Infect Dis. 2024;145:107074. doi:10.1016/j.ijid.2024.107074
22. Li Y, Wu M, Liang Y, et al. Mycoplasma pneumoniae infection outbreak in Guangzhou, China after COVID-19 pandemic. Virol J. 2024;21(1):183. doi:10.1186/s12985-024-02458-z
23. Restrepo MI, Babu BL, Reyes LF, et al. Burden and risk factors for Pseudomonas aeruginosa community-acquired pneumonia: a multinational point prevalence study of hospitalised patients. Eur Respir J. 2018;52(2). doi:10.1183/13993003.01190-2017
24. Gramegna A, Sotgiu G, Di Pasquale M, et al. Atypical pathogens in hospitalized patients with community-acquired pneumonia: a worldwide perspective. BMC Infect Dis. 2018;18(1):677. doi:10.1186/s12879-018-3565-z
25. Bello S, Mincholé E, Fandos S, et al. Inflammatory response in mixed viral-bacterial community-acquired pneumonia. BMC Pulm Med. 2014;14(1):123. doi:10.1186/1471-2466-14-123
26. Hoffmann J, Machado D, Terrier O, et al. Viral and bacterial co-infection in severe pneumonia triggers innate immune responses and specifically enhances IP-10: a translational study. Sci Rep. 2016;6(1):38532. doi:10.1038/srep38532
27. Qu J, Zhang J, Chen Y, et al. Aetiology of severe community acquired pneumonia in adults identified by combined detection methods: a multi-centre prospective study in China. Emerg Microbes Infect. 2022;11(1):556–566. doi:10.1080/22221751.2022.2035194
28. Zhang L, Xiao Y, Zhang G, et al. Identification of priority pathogens for aetiological diagnosis in adults with community-acquired pneumonia in China: a multicentre prospective study. BMC Infect Dis. 2023;23(1):231. doi:10.1186/s12879-023-08166-3
29. Gadsby NJ, Musher DM. The microbial etiology of community-acquired pneumonia in adults: from classical bacteriology to host transcriptional signatures. Clin Microbiol Rev. 2022;35(4):e0001522. doi:10.1128/cmr.00015-22
30. Musher DM, Jesudasen SS, Barwatt JW, Cohen DN, Moss BJ, Rodriguez-Barradas MC. Normal respiratory flora as a cause of community-acquired pneumonia. Open Forum Infect Dis. 2020;7(9):ofaa307. doi:10.1093/ofid/ofaa307
31. Shelburne SA, Sahasrabhojane P, Saldana M, et al. Streptococcus mitis strains causing severe clinical disease in cancer patients. Emerg Infect Dis. 2014;20(5):762–771. doi:10.3201/eid2005.130953
32. Kilian M, Riley DR, Jensen A, Brüggemann H, Tettelin H, Russell M. Parallel evolution of Streptococcus pneumoniae and Streptococcus mitis to pathogenic and mutualistic lifestyles. mBio. 2014;5(4):e01490–14. doi:10.1128/mBio.01490-14
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.