Back to Journals » International Journal of Nanomedicine » Volume 21
Targeted Nanoboron Delivery Platform for Boron Neutron Capture Therapy in Refractory Solid Tumors
Authors Ma Z, Ma Z, Wang X, Li Y, Li L, Li L, Ji P ![]() , Yan Q
, Yan Q
Received 14 November 2025
Accepted for publication 29 January 2026
Published 6 February 2026 Volume 2026:21 581215
DOI https://doi.org/10.2147/IJN.S581215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Dong Wang
Zhenchao Ma,1,2,* Ziyan Ma,3,* Xinlin Wang,3 Yaru Li,3 Lian Li,3 Luzixuan Li,3 Peng Ji,3 Qiang Yan1
1Huzhou Central Hospital, Fifth School of Clinical Medicine of Zhejiang Chinese Medical University, Huzhou, Zhejiang Province, 313000, People’s Republic of China; 2Boron Neutron Capture Cancer Treatment Technology, Zhejiang Engineering Research Center, Huzhou, Zhejiang Province, 313000, People’s Republic of China; 3School of Pharmacy, Taizhou University, Taizhou, Jiangsu Province, 225300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peng Ji, School of Pharmacy, Taizhou University, No. 93, Jichuan East Road, Taizhou, Jiangsu Province, 225300, People’s Republic of China, Email [email protected] Qiang Yan, Huzhou Central Hospital, Fifth School of Clinical Medicine of Zhejiang Chinese Medical University, No. 1558 North Sanhuan Road, Huzhou, Zhejiang Province, 313000, People’s Republic of China, Email [email protected]
Abstract: Boron neutron capture therapy (BNCT) represents a promising binary radiotherapy for refractory solid tumors. However, its clinical translation has been historically constrained by the suboptimal pharmacokinetics of conventional boron agents (eg, BPA and BSH), characterized by low tumor selectivity and rapid clearance. This review provides a comprehensive analysis of how nanoengineered delivery platforms—including lipid-based, polymeric, inorganic, and biomimetic nanocarriers—are revolutionizing BNCT. We focus on their advanced targeting mechanisms (passive EPR effect, active ligand/receptor engagement, and nuclear localization), which collectively enable significantly enhanced tumor boron accumulation (T/N ratios of 6– 17) and prolonged intratumoral retention. Furthermore, we critically examine the integration of multimodal imaging techniques (PET, MRI) for real-time dosimetry and treatment planning, which is essential for precision-guided BNCT. Despite remarkable preclinical progress, key translational challenges persist, including the standardization of neutron sources, long-term biocompatibility of nanocarriers, and scalable GMP-compliant manufacturing. In conclusion, the convergence of targeted nanomedicine, precision imaging, and immunomodulation is forging a robust platform. This positions BNCT as an emerging, clinically viable modality within the precision oncology arsenal for refractory malignancies.
Keywords: nanodelivery system, boron neutron capture therapy, targeted controlled release, refractory tumors, boron carrier
Introduction
Refractory tumors, including glioblastoma, recurrent head and neck cancers, and hepatocellular carcinoma, present significant challenges in clinical oncology due to their aggressive growth, heterogeneity, and resistance to standard therapies.1,2 Conventional radiotherapy and chemotherapy often fail to achieve sustained therapeutic responses and are frequently associated with significant systemic toxicity and damage to healthy tissues.3
BNCT is a binary targeted radiotherapy modality whose efficacy hinges on the selective delivery of boron-10 (10B) to tumor cells followed by thermal neutron irradiation. This process generates high-linear energy transfer (LET) particles capable of inducing lethal, spatially confined DNA damage, thereby offering a unique mechanism for targeting refractory solid tumors with minimized off-target effects.4 BNCT has emerged as a promising modality for refractory solid tumors due to its dual selectivity—both biochemical (via tumor-targeted boron delivery) and radiological (via spatially confined particle emission).
Clinical evidence underscores its potential: in recurrent head and neck cancer, BNCT achieves an objective response rate of 80.5%, significantly higher than conventional therapies, and extends median survival in glioblastoma to 12–18 months versus 9–12 months with standard care.5 The transition from reactor-based to compact, hospital-accessible accelerator-based neutron sources (eg, Japan’s J-CART) is addressing historical limitations in clinical scalability and standardization, as highlighted in recent reviews.6,7
Despite decades of research, the clinical translation of BNCT has been limited by the inherent drawbacks of conventional small-molecule boron agents such as BPA and BSH. These agents exhibit limited tumor selectivity, low T/N ratios, and short retention times, which restrict their therapeutic utility.4,8
We posit that BNCT is currently evolving from a binary radiotherapy model into an integrated, platform-based strategy for precision oncology, mainly driven by advances in nanobiotechnology and imaging. Engineered nanocarriers overcome the pharmacokinetic limitations of small molecules by combining dual targeting mechanisms—the enhanced permeability and retention (EPR) effect and ligand-mediated active targeting—with multifunctional capabilities, such as imaging–therapy integration and stimuli-responsive release.9,10
This review provides a comprehensive analysis of nanoengineered boron delivery systems, with a particular focus on their targeting mechanisms and the translational challenges that impede clinical adoption. We highlight how these nanotechnological advances are forging a crucial pathway to bridge nanoscience, radiation oncology, and cancer biology, thereby repositioning BNCT as an emerging precision medicine platform for refractory solid tumors.
Nuclear Reaction Principles and Precision Implementation Techniques of BNCT
Mechanisms of the BNCT Nuclear Reaction
BNCT operates as a binary therapy where the critical first step—selective boron delivery—is spatially and temporally separated from the second step—neutron irradiation. The therapeutic effect is non-radioactive until irradiation, minimizing pre-exposure toxicity. The core reaction involves the capture of a thermal neutron by a boron-10 (10B) nucleus, which has an exceptionally high capture cross-section (~3840 barns).4,11 This fission-like reaction produces high-LET α-particles and recoiling lithium-7 (7Li) nuclei. With a combined path length of approximately 5–9 µm—comparable to a single cell diameter—these particles deposit their kinetic energy densely along their track, causing clustered, complex DNA double-strand breaks that are difficult for tumor cells to repair. This subcellular precision is the physical basis for BNCT’s ability to eradicate tumor cells while largely sparing adjacent normal tissue.
The therapeutic efficacy of BNCT highly depends on the subcellular localization of 10B. This parameter can be precisely modulated using nanoengineered delivery systems. For example, nucleus-targeted nanoliposomes (eg, DOX-CB@lipo-pDNA-iRGD) incorporate nuclear localization signals (NLS) to transport 10B within 5–9 μm of genomic DNA, corresponding to the penetration range of α-particles.12 This spatial proximity enhances the probability of inducing DNA double-strand breaks compared with cytoplasmic boron distribution, as observed with free BSH, where α-particle energy is dissipated mainly before reaching the nucleus.13 A schematic overview of this process is presented in Figure 1, depicting the sequential events from boron accumulation to radiation-induced DNA damage.
 |
Figure 1 Schematic illustration of the BNCT mechanism for precise tumor cell eradication. The process involves the accumulation of boron-10 in tumor cells, followed by thermal neutron irradiation, and the subsequent release of high-LET α-particles and lithium nuclei, which cause DNA double-strand breaks. |
Biological Consequences and Therapeutic Selectivity
Building upon the nuclear reaction principles described above, the high-LET particles (alpha particles and 7Li nuclei) deposit their energy within a very short range (5–9 μm), confining lethal damage primarily to the boron-loaded cell. This spatial confinement underpins BNCT’s therapeutic selectivity. At the cellular and molecular level, these physical events translate into distinct biological consequences. BNCT induces tumor cell death through interconnected pathways:14,15 (i) direct induction of complex DNA double-strand breaks leading to apoptotic or necrotic cell death;16–19 (ii) generation of secondary reactive species causing pronounced oxidative stress and organelle damage;20,21 and (iii) activation of cell cycle checkpoints resulting in growth arrest.22 This unique combination of targeted boron delivery and spatially confined high-LET radiation underpins BNCT’s potential to eradicate refractory tumor cells while sparing normal tissues. Nevertheless, accurately calculating boron concentration and neutron dose distribution remains a major translational challenge.
Criteria and Targeting Strategies for Boron Agents
The most widely investigated boron delivery agents for BNCT currently include boronophenylalanine (BPA), an amino acid analogue that is selectively taken up by tumor cells via overexpressed amino acid transporters, and sodium borocaptate (BSH), which primarily accumulates in tumor tissues through passive diffusion.8 An ideal boron agent for clinical BNCT should meet the following criteria:23–30 (i) high tumor selectivity, enabling preferential accumulation within malignant cells while minimising uptake in normal tissues; (ii) a high boron content per molecule to maximise the probability of neutron capture events and enhance therapeutic efficacy; (iii) favourable biodistribution to ensure homogeneous intratumoral distribution and achieve consistent cytotoxicity across the tumor mass; and (iv) excellent biocompatibility and low systemic toxicity to support safe administration and reduce off-target effects during treatment; and (v) compatibility with nanoengineering (eg, ligand conjugation, imaging moiety loading) to enable targeted delivery and real-time monitoring. A comparative overview of three fundamental targeting mechanisms—LAT1-mediated uptake, CPP-enhanced delivery, and EPR-driven passive accumulation—is provided in Figure 2.
 |
Figure 2 Illustrates three boron-based drug delivery strategies for tumor therapy: boron drug delivery targeting L-type amino acid transporter 1 (LAT1), cell-penetrating peptide (CPP)-mediated sodium borocaptate (BSH) delivery, and passive targeting mediated by the EPR effect. Exemplar A is represented by boronophenylalanine (BPA) and the poly(vinyl alcohol)-BPA (PVA-BPA) composite, which targets the LAT1 pathway. BPA can cross the blood-brain barrier and accumulate in cells via the transport function of LAT1. However, to maintain intracellular amino acid homeostasis, LAT1 pumps BPA out of cells again in exchange for extracellular amino acids, resulting in insufficient boron drug concentration in tumor cells to meet the requirements of boron neutron capture therapy (BNCT). Although traditional continuous infusion can partially maintain intracellular boron drug concentration and prolong BPA retention time, it induces adverse effects such as phlebitis. In contrast, after being transported into cells via LAT1, PVA-BPA accumulates in endosomes/lysosomes, reducing the content of free BPA in the cytoplasm, thereby slowing LAT1-mediated BPA efflux, effectively extending BPA retention time and increasing accumulation concentration, and ultimately optimizing the boron concentration ratios of tumor-to-blood (T/B) and tumor-to-normal tissue (T/N). Exemplar B is a CPP-mediated BSH delivery system represented by BSH-11R. The composite consists of 8 BSH units and a poly-11-arginine domain, with a boron content of 20.1% (mass ratio). BSH-11R enters cells through non-receptor-dependent non-classical endocytosis, can directly penetrate the cell membrane, and accumulates in the nucleus. As shown in the bar graph in Part B, BSH exhibits high-concentration accumulation in the nucleus 24 hours after administration. Exemplar C is an EPR effect-dependent passive targeting system represented by zirconium (Zr)-tetrakis (4-carboxyphenyl) porphyrin (TCPP) metal-organic nanocrystals (MNCs). These nanocrystals have a monodisperse spherical structure with an average particle size of 100.20±6.72 nm. By virtue of the EPR effect, MNCs in the bloodstream can penetrate the tumor vessel wall, retain and accumulate in tumor tissues, achieving a boron concentration ratio of 6.20±0.90 between tumor and normal tissues and 3.80±0.35 between tumor and blood, demonstrating excellent tumor-selective accumulation capability. |
Dynamic Monitoring of Boron Concentration and Multimodal Imaging Strategies
The therapeutic efficacy of BNCT is fundamentally governed by the nuclear reaction between 10B and thermal neutrons, which generates high linear energy transfer (LET) α-particles and 7Li nuclei. These reaction products induce clustered DNA double-strand breaks selectively within boron-enriched tumor cells.31–33 Because the neutron capture probability is directly proportional to the local 10B concentration, maintaining an intratumoral boron level exceeding approximately 20 μg/g is considered critical for achieving therapeutic efficacy. Conversely, excessive boron accumulation in normal tissues can result in off-target toxicity, given the limited path length of α-particles (5–9 μm). In addition, heterogeneous intratumoral boron distribution may lead to the formation of “dose-cold” regions, emphasizing the importance of achieving spatially uniform 10B localization, even at the subcellular level.
Translating these nuclear principles into clinical benefit necessitates real-time and spatially resolved monitoring of boron biodistribution. To this end, contemporary monitoring methodologies—including physical, radiochemical, and analytical approaches (Table 1)—are increasingly being integrated with advanced imaging technologies to enhance temporal and spatial resolution. Collectively, these multimodal imaging strategies not only validate whether therapeutic boron thresholds are attained but also enable individualized irradiation planning, thereby advancing BNCT toward precision-guided radiotherapy.
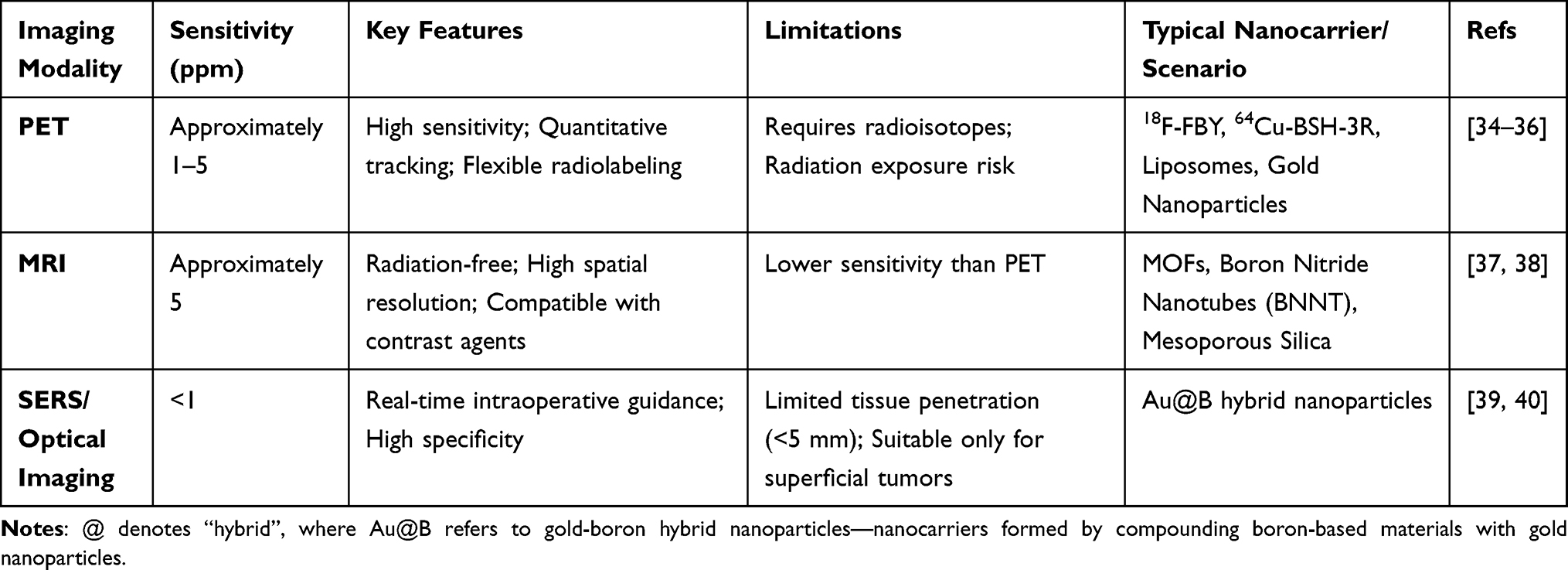 |
Table 1 Comparative Analysis of Imaging Modalities for Boron Quantification in BNCT |
Imaging Strategies and Adaptability to Nanocarriers
The emergence of nanotechnology-based boron delivery platforms has necessitated the adaptation of imaging modalities to accommodate the distinct physicochemical and pharmacokinetic characteristics of nanocarriers, including particle size, surface functionalization, and biodistribution profiles. In contrast to small-molecule agents, nanocarriers display prolonged systemic circulation and heterogeneous tumor retention, thereby requiring imaging technologies capable of simultaneously capturing both spatial distribution and temporal dynamics. Representative imaging strategies currently employed for boron quantification in BNCT are summarized in Table 1.
Positron Emission Tomography (PET)
PET imaging enables precise, quantitative assessment of nanocarrier biodistribution through the use of radiolabels such as 18F and 64Cu.34,35 For instance, 18F-trifluoroborate tyrosine (FBY) and 64Cu-labeled BSH-Tmr-3R—a cell-penetrating peptide–modified BSH conjugate—have shown strong correlations between PET signal intensity and actual boron concentration (R2 = 0.974 in the B16-F10 model). Owing to its high sensitivity (approximately 1 ppm) and versatility in labeling liposomes, gold nanoparticles, and polymeric micelles, PET represents the most robust modality for quantitative tracking of boron nanocarriers.36
Magnetic Resonance Imaging (MRI)
The incorporation of contrast agents such as gadolinium chelates into boron nanocarriers provides high-resolution, radiation-free anatomical and functional imaging. Although its sensitivity (approximately 5 ppm) is lower than that of PET, emerging nanoplatforms—including metal–organic frameworks (MOFs), boron nitride nanotubes (BNNTs), and mesoporous silica nanoparticles—are capable of co-loading boron and MRI contrast agents, enabling concurrent therapeutic delivery and visualization.37,38
Surface-Enhanced Raman Scattering (SERS) and Optical Imaging
The conjugation of near-infrared SERS probes or fluorescent dyes with boron nanocarriers facilitates real-time, intraoperative visualization. Despite their excellent molecular specificity, these optical approaches are limited by shallow tissue penetration depths (<5 mm), restricting their applicability to superficial or surgically accessible lesions.39,40
Beyond these in vivo modalities, advanced microscopy techniques provide unprecedented insights into nanocarrier–cell interactions at the subcellular level—an essential consideration for optimizing delivery efficiency, particularly in nuclear-targeted BNCT systems. Although predominantly employed in preclinical studies, methods such as PAINT (Point Accumulation for Imaging in Nanoscale Topography), which enables dynamic tracking of lipid nanocarriers; STORM (Stochastic Optical Reconstruction Microscopy), which achieves super-resolution mapping of cellular uptake; and STED (Stimulated Emission Depletion) microscopy, which allows targeted super-resolution fluorescence imaging, collectively offer valuable tools for validating nanocarrier design and intracellular trafficking.41–45
Collectively, PET offers unparalleled sensitivity and quantitative accuracy, MRI provides superior spatial resolution and anatomical definition, and SERS enables real-time intraoperative guidance. The complementary strengths of these modalities underscore the translational promise of integrated multimodal imaging approaches for precise, image-guided BNCT. However, translating the signals from these imaging modalities into accurate, quantitative boron concentrations within tumors—and leveraging them for clinical treatment planning—remains a significant challenge.
Imaging–Concentration Correlation and Clinical Translation
A persistent challenge in BNCT lies in establishing a quantitative correlation between imaging-derived signals and the actual intratumoral boron concentration. Positron emission tomography (PET) using 18F-labeled BPA (18F-BPA) often overestimates tumor boron accumulation—typically by 15–20%—when compared with inductively coupled plasma mass spectrometry (ICP–MS) reference values. However, the gamma camera constructed by I-Huan Chiu and his team, based on CdTe-DSD imaging technology, can accurately distinguish characteristic gamma-ray signals from background interference due to its high energy and spatial resolution, directly inverting the location and intensity of the BNCT reaction.46 The differences in accuracy from the pharmacokinetic differences between short-lived radiotracer surrogates and boron-containing therapeutic agents. In particular, radiotracers may not fully colocalize with boron retained in long-circulating nanocarriers, such as PEGylated liposomes.47–49 Consequently, standardized calibration and validation protocols are urgently needed to account for these carrier-specific pharmacokinetic disparities and to enhance the accuracy and reproducibility of imaging-guided dosimetry in BNCT. Establishing a robust, quantitative relationship between imaging signals and actual boron distribution is therefore pivotal to advancing BNCT from experimental validation toward reliable clinical implementation.
Beyond verification, the quantitative imaging of boron distribution also provides a valuable framework for optimizing drug design and delivery strategies. Such analyses reveal the intrinsic pharmacokinetic limitations of conventional small-molecule boron agents, including the short retention time and heterogeneous tumor distribution of BPA, while simultaneously offering real-time evaluation of novel formulations. For example, 18F–FBY PET imaging has demonstrated that approximately 30% of tumor regions remain below the therapeutic threshold of 20 μg/g when BPA is administered, underscoring the need for next-generation delivery systems such as polymer–boron conjugates or cell-penetrating peptide (CPP)–based constructs that prolong retention and enable subcellular targeting.
Therefore, while multimodal imaging provides indispensable, real-time guidance for BNCT, translating imaging signals into true, absolute boron concentration remains a challenge. In summary, preclinical studies have established that current imaging modalities (eg, PET, MRI) can achieve sensitivities in the range of 1–5 ppm and provide valuable semi-quantitative or correlative biodistribution data (eg, strong PET-ICP-MS correlation with R2 up to 0.974 for specific agents like FBY). However, as highlighted, discrepancies of 15–20% compared to gold-standard techniques like ICP-MS are common, underscoring the limitation of relying solely on imaging for absolute dosimetry. Future work must focus on validating imaging biomarkers against gold-standard measurements and developing carrier-specific calibration models to achieve truly quantitative, image-guided dosimetry. The design of next-generation nanoformulations, with tailored pharmacokinetics and integrated reporting functionalities (eg, co-loaded contrast agents), holds significant promise for narrowing this gap and improving the accuracy of imaging-based boron quantification.
Therefore, the development of advanced strategies for boron concentration monitoring and multimodal imaging constitutes an indispensable component of precision-guided BNCT. With these fundamental principles established, we now explore the translation of BNCT into clinical practice, beginning with its potential applications across various refractory tumor types.
Potential Applications of BNCT in Refractory Tumors
BNCT has emerged as a promising therapeutic modality for refractory malignancies such as glioblastoma and head and neck cancers, where conventional treatment regimens often result in limited efficacy and poor clinical outcomes.50 The therapeutic success of BNCT depends critically on achieving efficient intracellular accumulation of sufficient 10B atoms within tumor cells while minimizing off-target deposition in surrounding healthy tissues. Recent progress in this field has centered on two complementary directions: the refinement of small-molecule boron agents and the advancement of nanotechnology-enabled delivery systems. In particular, strategies incorporating active and subcellular (nuclear) targeting have shown significant potential in enhancing tumor selectivity and maximizing DNA damage efficiency.
Small-Molecule Boron Agents and Optimization Strategies
LAT1-Mediated Amino Acid Analogues
The L-type amino acid transporter 1 (LAT1), highly expressed in proliferating tumor cells and at the blood–brain barrier (BBB), serves as the principal uptake pathway for amino acid–based boron compounds. The first clinically approved BNCT agent, BPA (also known as Steboronine), utilizes this transporter for tumor targeting. However, the bidirectional and rapid translocation kinetics of BPA yield a modest tumor-to-normal tissue (T/N) ratio of approximately 2–3 and a short intratumoral retention time (<2 h). Although continuous infusion can maintain therapeutic plasma levels, it concurrently increases systemic exposure and toxicity.
Polymer Conjugates for Prolonged Retention
To address the limitations of rapid efflux, polymer conjugation strategies have been developed to enhance boron retention. Poly(vinyl alcohol)–BPA (PVA–BPA) accumulates within endosomes and lysosomes following LAT1-mediated uptake, thereby reducing cytoplasmic efflux and extending intracellular retention to approximately 12 h.51 Likewise, PEG–poly[Lys/Lys(fructose)]–BPA conjugates inhibit drug efflux while promoting renal clearance, resulting in substantially improved tumor-to-blood (T/B) and T/N ratios in vivo.52 These findings underscore that minimizing efflux and facilitating subcellular sequestration represent practical approaches for improving boron accumulation.
Next-Generation LAT1 Substrates
Novel amino acid analogues, such as trifluoroborate–tyrosine (FBY), exhibit a close structural similarity to endogenous tyrosine, ensuring high LAT1 affinity and efficient tumor uptake.53 In melanoma models, FBY demonstrated superior therapeutic efficacy compared with BPA. Moreover, 18F-labeled FBY PET imaging revealed a strong linear correlation between PET signal intensity and boron concentrations determined by inductively coupled plasma mass spectrometry (ICP–MS) (R2 = 0.974), highlighting its potential as a noninvasive platform for boron quantification and treatment planning.54,55
Cell-Penetrating Peptide (CPP)–Based Boron Delivery Systems
Cell-penetrating peptides (CPPs) have been utilized to enhance the intracellular delivery of sodium borocaptate (BSH). CPP–BSH conjugates achieve up to a tenfold increase in nuclear accumulation relative to free BSH, significantly amplifying BNCT-induced cytotoxicity.56–58 Radiolabeled derivatives, such as 64Cu-labeled BSH–Tmr–3R, achieve T/N ratios of up to 15.5 within 6 hours post-injection, underscoring their promise for integrated theranostic applications.38
Hybrid Designs Based on BSH Modification
Chemical modification of BSH with 2-aminocyclobutane carboxylic acid (ACBC) facilitates LAT1-mediated uptake, enhancing intracellular accumulation and prolonging tumor retention in glioma models. Concurrently, 18F–ACBC PET imaging allows real-time monitoring of boron biodistribution, demonstrating its translational potential for clinical BNCT guidance.59 Small-molecule boron agents primarily achieve tumor targeting through transporter- or peptide-mediated uptake mechanisms. Nevertheless, rapid efflux, short intratumoral retention, and systemic exposure continue to limit their therapeutic impact. Strategies involving polymer–boron conjugation, next-generation LAT1 substrates with integrated imaging tracers, and CPP-functionalized BSH derivatives show considerable promise in overcoming these limitations. In summary, the optimization of small-molecule boron agents through polymer conjugation, novel LAT1 substrates, and CPP functionalization has significantly improved tumor targeting and retention. However, their inherent constraints—particularly in boron payload capacity, tumor tissue penetration, and systemic pharmacokinetics—present fundamental barriers to further efficacy gains. To transcend these limitations, research has pivoted toward nanotechnology-based delivery platforms. The following section examines nanocarrier-based strategies, which are engineered to offer high payloads, enhanced tumor accumulation, and multifunctional integration, thereby addressing the core challenges of small-molecule agents. A comparative summary of the key agents discussed in this section is provided in Table 2.
 |
Table 2 Comparative Properties of Small-Molecule Boron Agents and Optimization Strategies |
Nanocarrier-Based Boron Delivery Strategies
While small-molecule boron agents achieve tumor accumulation primarily through transporter-mediated uptake, their therapeutic performance is limited by a constrained boron loading capacity and suboptimal intratumoral penetration. Nanocarrier-based delivery systems, with their high boron payloads, tunable surface properties, and multifunctional design, have emerged as a powerful strategy to overcome these limitations. Their design principles and performance advantages are summarized below.
Lipid- and Polymer-Based Nanocarriers
Lipid-based and polymeric nanocarriers provide biocompatible and chemically versatile platforms for boron delivery.60–62 Systems incorporating boronated porphyrins or carborane cores have achieved intratumoral boron concentrations exceeding 100 ppm, with tumor-to-normal tissue (T/N) ratios of 3–6 and tumor retention times ranging from 24 to 72 h. Many of these formulations integrate dual-modality imaging functions, such as PET and fluorescence, enabling real-time treatment planning and dosimetric assessment. However, their therapeutic efficacy remains strongly dependent on the EPR effect, which is characterized by pronounced inter- and intra-tumoral heterogeneity. Consequently, nanocarriers relying solely on passive targeting often show limited performance in poorly vascularized or fibrotic tumors.63
Inorganic and Hybrid Nanocarriers
Inorganic nanomaterials—including boron nitride nanotubes (BNNTs), boron carbide (B4C) nanoparticles, and zirconium–tetrakis(carboxyphenyl)porphyrin (Zr–TCPP) metal–organic frameworks (MOFs)—offer exceptionally high boron loading capacities (>40 wt%) and structural tunability.64 For instance, Zr–TCPP MOFs have demonstrated intratumoral boron concentrations of approximately 67 ppm and T/N ratios exceeding 6 in glioma models, while concurrently providing intrinsic fluorescence and PET imaging capabilities. BNNTs exhibit preferential nuclear localization, thereby enhancing α-particle–induced DNA double-strand break formation.65 Despite these advantages, achieving a balance between boron payload and biocompatibility remains a significant challenge. BNNTs and MOFs tend to exhibit long-term biopersistence and accumulation within the reticuloendothelial system (eg, liver and spleen), with preclinical studies indicating potential risks of chronic inflammation and fibrosis.66 The unresolved issues of biodegradability, clearance, and long-term safety continue to hinder the clinical translation of these products.
Biomimetic Nanocarriers
Concerns regarding the biosafety of inorganic materials have spurred the development of biomimetic nanocarriers with superior physiological compatibility. Biomimetic vesicles, including exosome-mimicking nanoparticles and virus-like particles (VLPs), have recently gained attention as innovative boron delivery platforms.67–69 These systems exhibit intrinsic immune evasion, barrier penetration, and enhanced biodistribution characteristics, promoting efficient tumor accumulation. Exosome-derived nanocarriers, in particular, display excellent biocompatibility and can be engineered through antibody or ligand conjugation to achieve precise targeting while minimizing nonspecific protein corona formation. Moreover, exosomes can serve as dual-function vehicles for co-delivering boron agents and immunomodulators, simultaneously enhancing tumor-specific delivery and stimulating antitumor immune responses. This integrated “delivery–immunity” paradigm offers a novel therapeutic direction for BNCT.70,71 Nonetheless, clinical translation remains limited by complex and non-standardized fabrication procedures, batch-to-batch variability, and incomplete understanding of in vivo kinetics and potential off-target effects.
Actively Targeted Nanoplatforms
Ligand-functionalized nanocarriers represent an advanced approach to improve the specificity and cellular internalization of boron delivery systems. Surface modification with molecular targeting moieties—such as transferrin, folate, or antibodies against EGFR and HER2—has been shown to significantly enhance tumor accumulation and perinuclear localization significantly, achieving intratumoral boron concentrations exceeding 200 μg/g and T/N ratios of up to 40.72 However, the clinical translation of active targeting strategies is complicated by tumor heterogeneity in receptor expression, which may result in non-uniform boron distribution and subtherapeutic “cold” zones. Additionally, the use of monoclonal antibodies presents challenges in manufacturing, immunogenicity, and scalability.73,74 Future optimization will likely focus on low–molecular–weight ligands such as peptides or affibodies, as well as pretargeting methodologies that decouple tumor recognition from payload delivery—approaches that may enhance both specificity and pharmacokinetic control. The diverse repertoire of active targeting mechanisms, including receptor-mediated and nuclear-directed strategies, is schematically illustrated in Figure 3.
 |
Figure 3 Schematic overview of active targeting strategies in tumor intervention. The figure illustrates multiple targeting approaches and their mechanisms: Part I, Cell surface receptor targeting, including folate receptor-α (FRα), transferrin receptor 1 (TfR1), epidermal growth factor receptor (EGFR), and human epidermal growth factor receptor 2 (HER2), with corresponding carriers such as folic acid (FA)-modified liposomes, transferrin (TF)-conjugated boron nitride nanotubes (TF-BNNTs), and anti-EGFR antibody-functionalized boron carbide nanoparticles (B4C-ant-EGFR). Part II, Monoclonal antibody-mediated targeting, exemplified by carcinoembryonic antigen (CEA)-targeted constructs and 123I-B-61-AuNPs. Part III, Nuclear targeting, such as CRISPR-Cas9 systems and DOX-CB@lipo-pDNA-iRGD (a liposomal system co-loading doxorubicin (DOX) and carborane (CB) with iRGD ligand and nuclear localization signal). Additional strategies include immune activation via macrophage phagocytosis of carriers like cholesteryl polyethylene glycol maleimide (Chol-PEG-Mal)-modified gold nanoparticles (GNPs), and membrane destruction mediated by Cs210B12H11SH and F-PLL-BNNTs. Various carriers (GNPs, BNNT derivatives, multifunctional nanocomposites) are employed to achieve precise tumor targeting, intracellular delivery, and tumor cell killing. |
Nuclear-Targeted Nanocarriers
Given that BNCT efficacy is dictated by the proximity of 10B atoms to genomic DNA, nanoplatforms capable of nuclear localization hold particular therapeutic importance. Nuclear localization signal (NLS)–functionalized liposomes, such as DOX–CB@lipo–iRGD, have demonstrated a sixfold increase in nuclear boron accumulation, resulting in a twofold improvement in survival in glioblastoma models. Additionally, these systems can be engineered to modulate immune checkpoints (eg, CD47 silencing), thereby combining radiotherapeutic and immunomodulatory functions.12 Despite their superior efficacy, challenges related to synthetic complexity, biosafety, and large-scale production must be addressed before clinical implementation can occur.
Cell-Mediated Delivery Strategies
Parallel to the design of synthetic nanocarriers, the concept of cell-mediated delivery has emerged as a promising alternative approach for overcoming biological barriers. Figure 4 schematically illustrates this concept. Importantly, proof-of-concept for such a “living carrier” platform has been demonstrated in related fields: for example, stem cells loaded with therapeutic nanoparticles have been shown to traverse the BBB and home to glioblastoma (GBM) lesions in preclinical models of other therapies.75 This work provides a strong rationale and a technological blueprint for the future development of stem cells loaded with boron-containing nanoparticles as a potential delivery system for BNCT, particularly for treating intracranial tumors. Upon arrival at the tumor, such engineered cells could release their therapeutic payload, potentially facilitating trans-barrier BNCT delivery.
 |
Figure 4 Schematic illustration of the stem cell-nanoparticle delivery system for gadolinium-mediated neutron capture therapy (Gd-NCT) — a homologous strategy to boron neutron capture therapy (BNCT) — for glioblastoma (GBM).75 The system consists of umbilical mesenchymal stem cells (UMSCs) loaded with Gd-Fu@IO@PVA/Fu nanoparticles (Gd-FPFNP), which are composed of gadodiamide (Gd), fucoidan (Fu), iron oxide (Fe3O4, IO), and polyvinyl alcohol (PVA). Key processes include: 1) GBM homing and magnetic navigation of the stem cell-nanoparticle complex; 2) transport across the blood-brain barrier (BBB); 3) cell fusion between UMSCs and GBM cells, followed by release of the nanoparticle payload; 4) neutron beam irradiation triggering Gd-mediated neutron capture therapy, leading to tumor cell killing. This theranostic bio-gadolinium agent-based delivery system represents a universal targeted platform for neutron capture therapies (NCTs), including both Gd-NCT and BNCT. It demonstrates the core technical logic of NCTs: precisely delivering a neutron-capturable nucleus (Gd in this model, or boron-10 (10B) in BNCT) to tumor sites, thereby serving as a critical bridge connecting neutron capture agents, neutron beams, and tumor targets, directly determining therapeutic efficacy and safety. Used from Yen-Ho Lai, Chia-Yu Su, Hung-Wei Cheng et al. Stem cell-nanomedicine system as a theranostic bio-gadolinium agent for targeted neutron capture cancer therapy. Nature Communications. 2023;14(1):285. Permission conveyed through Copyright Clearance Centre, Inc. |
Summary and Translational Perspectives
To translate the promising preclinical potential of nanocarriers into clinical reality, it is imperative to first systematically contextualize their respective advantages and limitations. The following section will then examine the accumulated clinical evidence to validate this translational promise. Nanocarrier-based boron delivery platforms enable high payload capacity, extended tumor retention, and integration with multimodal imaging for precision-guided BNCT.76 Lipid and polymeric carriers exhibit favorable clinical adaptability but rely heavily on the EPR effect. Inorganic and hybrid systems offer ultrahigh boron content yet pose long-term biocompatibility concerns. Biomimetic nanocarriers combine immune compatibility with targeting specificity but remain in early developmental stages. Active and nuclear-targeted systems achieve unprecedented localization precision; however, tumor heterogeneity, immunogenicity, and manufacturing complexity continue to limit their translation.
The synergistic convergence of small-molecule optimization and nanotechnology-driven delivery defines the evolving landscape of BNCT for refractory malignancies. Comparative analysis reveals distinct performance profiles: small molecules such as BPA and BSH offer rapid delivery but low T/N ratios (2–3) and short retention (<2 h); polymer conjugates and amino acid analogues (eg, FBY) improve T/N ratios to approximately 10 and extend retention to 12–24 h. In contrast, nanocarriers achieve substantial advances—lipid and polymer-based systems yield T/N ratios of 3–6 with 24–72 h retention, while inorganic/hybrid and biomimetic platforms reach ratios of 6–10 and 8–10, respectively. Actively targeted and nuclear-directed platforms achieve T/N ratios as high as 40, representing the current benchmark in tumor selectivity.
As summarized in Figure 5, a spectrum of boron delivery strategies—from small molecules to multifunctional nanocarriers—has demonstrated enhanced tumor-targeted boron accumulation and therapeutic efficacy in preclinical models. Looking ahead, future progress will depend on multimodal imaging–based dosimetry validation, adaptive targeting strategies to address tumor heterogeneity, and scalable, Good Manufacturing Practice (GMP)–compliant production processes to enable clinical translation. Key physicochemical characteristics and performance metrics of representative nanocarrier systems are summarized in Table 3. The aforementioned preclinical advances systematically compare various boron delivery strategies, from traditional small molecules to multifunctional nanocarriers, highlighting the immense potential of nanotechnology in enhancing tumor targeting. While the preclinical data for nanocarrier-based BNCT are promising, their ultimate value is determined by clinical outcomes in patients. Therefore, to critically assess the translational potential of these platforms and to establish the real-world impact of BNCT, the following section shifts focus to a systematic review of exploratory studies and accumulated clinical evidence across refractory malignancies.
 |
Table 3 Comparison of Nanocarrier Platforms for BNCT |
 |
Figure 5 Overview of boron-based drugs and nanomaterial applications in boron neutron capture therapy (BNCT) for refractory tumors. (A) Applications in specific tumor types: 1) Primary central nervous system lymphoma (PCNSL): PCNSL cells express high levels of LAT1, enabling effective boron uptake via BPA; BPA/BNCT exhibits potent cytotoxicity and significantly prolongs survival in a mouse model of intracranial PCNSL. 2) High-grade glioma (GBM) and nonfunctioning pituitary adenomas (NFPA): FRα-targeted 10B-enriched carbon nanospheres are efficiently internalized by NFPAs, inducing significant apoptosis upon thermal neutron irradiation; FA-3PCB (PMAO- and PEG-modified liposomes encapsulating boron-enriched nanoparticles (3PCB) and near-infrared fluorophore Cy5) achieves a tumor boron concentration of 15.6±2.1 μg/g, surpassing non-targeted liposomes and normal brain tissue (5.2±0.9 μg/g) with a tumor-to-normal brain ratio of 6.2:1, prolonging survival. 3) Other tumors: Malignant melanoma, primary synovial sarcoma, cervical cancer, and locally recurrent colorectal cancer also benefit from BNCT. (B) Targeted Boron Delivery Strategies and Efficacy in Glioma and Other Tumor Types. 1) Schematic representation of folate receptor (FR)-targeted boron delivery system (FA-3PCB). Surface modification with folic acid enables specific recognition and internalization into FR‑overexpressing glioma cells, facilitating efficient boron accumulation within the tumor tissue. 2) Boron delivery and therapeutic efficacy in glioma models. FA‑3PCB achieves a high tumor boron concentration with a tumor‑to‑normal brain (T/N) ratio of 6.2:1. Following thermal neutron irradiation, significant apoptotic cell death is induced, resulting in prolonged survival in experimental glioma models. 3) Extension of BNCT to other refractory solid tumors. Boron‑based agents have also demonstrated promising accumulation and therapeutic potential in several other tumor types, including malignant melanoma, primary synovial sarcoma, cervical cancer, and locally recurrent colorectal cancer, supporting the broader applicability of BNCT beyond gliomas. (C) Efficacy of nanomaterials in tumor-bearing mice: 1) The A6K peptide forms a novel boron agent with BSH, achieving a tumor boron concentration of 24.8 μg/g and a T/N ratio of 2.8. 2) Parthenolide-encapsulated boron nitride nanoparticles (PTL@BNNPs) show favorable tumor accumulation (6.18%±2.18% ID/g at 24 hours post-injection) and a high tumor-to-background uptake ratio (tumor/blood: 2.71±0.96). 3) Anti-EGFR-10BPO4 NPs (boron phosphate nanoparticles enriched with 10B, modified with polyacrylic acid and anti-EGFR antibodies) achieve a tumor boron concentration of 63 μg/g and a tumor/blood ratio of 4.27 following tail vein injection. All agents meet or exceed the BNCT therapeutic threshold for effective tumor ablation. |
Exploratory Studies and Clinical Evidence of BNCT in Refractory Malignancies
Despite substantial progress in multimodal cancer therapies, many malignancies remain refractory to conventional treatment regimens. Their intrinsic anatomical complexity, aggressive invasiveness, and pronounced resistance to chemo- and radiotherapy contribute to suboptimal therapeutic outcomes and poor prognoses. For example, central nervous system (CNS) tumors are shielded by the BBB, head and neck cancers are anatomically constrained by proximity to radiosensitive organs,77 and advanced breast cancers with skeletal metastases often pose significant therapeutic and safety challenges.78
BNCT has demonstrated a favorable therapeutic index across diverse tumor types, offering highly selective cytotoxicity toward malignant cells while minimizing collateral injury to normal tissues. However, wider clinical adoption will depend on continued validation through rigorously designed trials, optimization of treatment protocols, and refinement of boron delivery platforms to ensure reproducibility, safety, and efficacy.
Recent Developments and Clinical Outcomes of Accelerator-Based BNCT (AB-BNCT)
The transition from reactor-based to accelerator-based neutron sources has significantly enhanced the clinical accessibility and scalability of BNCT, leading to an expansion of patient cohorts and the accumulation of clinical evidence. In recurrent head and neck squamous cell carcinoma (HNSCC), a multicenter Japanese trial demonstrated that AB-BNCT with borofalan (10B) achieved an objective response rate (ORR) of 71% and a complete response (CR) rate of 45% in heavily pretreated patients, with manageable cutaneous toxicity as the principal adverse event.79 Similarly, in glioblastoma, Phase II data using cyclotron-generated neutrons and BPA reported a median overall survival (OS) of 15.6 months, outperforming historical bevacizumab controls.80
Encouraging results have also been observed in other malignancies. In cutaneous melanoma and angiosarcoma, AB-BNCT achieved CR rates exceeding 80%, accompanied by favorable cosmetic preservation and functional recovery, emphasizing its suitability for superficially localized tumors.79 Early-phase investigations are also exploring its use in breast cancer skin metastases and hepatocellular carcinoma, leveraging novel boron carriers to overcome prior pharmacokinetic limitations.78 Collectively, these outcomes underscore the evolution of BNCT from an experimental approach toward a clinically translatable therapy for radioresistant cancers.
BNCT in Central Nervous System Malignancies
Since 2004, the introduction of BPA, a boron carrier capable of crossing the BBB and selectively accumulating in tumor cells, has facilitated the transition of BNCT from intraoperative to noninvasive management of glioblastoma multiforme.81 Kageji et al reported a median survival of 19.5 months and 2-, 3-, and 5-year survival rates of 31.8%, 22.7%, and 9.1%, respectively, in GBM patients treated with BNCT, representing a meaningful survival benefit.82 In a subsequent phase II study, Zhang et al demonstrated that BPA-BNCT achieved superior efficacy compared with bevacizumab monotherapy in recurrent GBM, with 1-year survival rates of 79.2% versus 34.5% and median OS of 18.9 versus 10.5 months, respectively.80
In primary CNS lymphoma (PCNSL), overexpression of the L-type amino acid transporter 1 (LAT1) enables targeted boron uptake via BPA.83 Using an intracranial PCNSL model, Yoshimura et al demonstrated efficient tumor accumulation and extended survival following BPA-BNCT, suggesting its potential utility in recurrent or refractory PCNSL.84 BNCT has also shown therapeutic promise in nonfunctioning pituitary adenomas (NFPA), utilizing dual targeting of pituitary-selective and folate receptor-α (FRα) pathways.85 Dai et al reported that FRα-targeted 10B-enriched carbon nanospheres achieved effective cellular internalization and induced marked apoptosis upon neutron irradiation, supporting BNCT’s feasibility for benign yet invasive pituitary tumors.86
BNCT in Head and Neck, Cutaneous, and Soft Tissue Malignancies
In head and neck squamous cell carcinoma, clinical studies have demonstrated the efficacy of BNCT.87 In a clinical series reported by Koivunoro et al, among 69 evaluable patients, 25 achieved CR, 22 partial response (PR), 17 stable disease, and only 5 disease progression.88 Hirose et al further reported a 2-year overall survival rate of 100% in 13 patients with recurrent or locally advanced nonsquamous carcinomas treated with BPA-BNCT.89 Using AB-BNCT, Igaki et al achieved complete remission in two cases of scalp angiosarcoma, with no dose-limiting toxicities observed during 15–20 months of follow-up.79
Beyond CNS and head and neck malignancies, BNCT has demonstrated promising efficacy in cutaneous and soft tissue tumors. Between 1987 and 2002, Cruz et al treated 22 melanoma patients with BPA-BNCT, achieving CR and PR rates of 68.2% and 23.0%, respectively, with tolerable dermatologic toxicity.90 Fujimoto et al reported partial remission of synovial sarcoma following two BNCT sessions, with complete resection and no recurrence at 6 months.91 Likewise, Fukuda et al observed complete remission in three patients with extramammary Paget’s disease (EMPD), achieving durable local control with only transient moderate skin reactions.92
BNCT in Breast Cancer and Emerging Indications
Although still in early stages of clinical evaluation, preclinical studies suggest that BNCT holds significant promise in managing metastatic breast cancer. In a murine tibial metastasis model, Andoh et al demonstrated that BPA preferentially accumulated within metastatic lesions, where BPA-BNCT effectively suppressed tumor growth, mitigated osteolytic damage, and promoted bone remodeling without injuring the surrounding normal bone.93 These findings underscore the potential of BNCT as a precision-guided treatment modality for metastatic and refractory solid tumors.
Summary and Clinical Outlook
Cumulative preclinical and clinical evidence support BNCT as a highly selective and effective therapeutic strategy for treatment-refractory malignancies. In CNS tumors, BNCT achieves durable disease control by penetrating the BBB and targeting invasive gliomas, PCNSL, and NFPA. In head and neck cancers, it provides precise tumor targeting with minimal toxicity to critical normal tissues. Promising responses in melanoma, sarcoma, EMPD, and emerging indications such as breast cancer further highlight its expanding therapeutic reach. Overall, BNCT demonstrates an encouraging balance of efficacy and safety across tumor types. However, achieving full clinical adoption requires addressing two core translational challenges: optimizing delivery systems for greater specificity and efficiency, and establishing standardized dosimetric and safety frameworks, which are the focus of the following sections. A concise summary of representative clinical and preclinical outcomes is provided in Table 4.
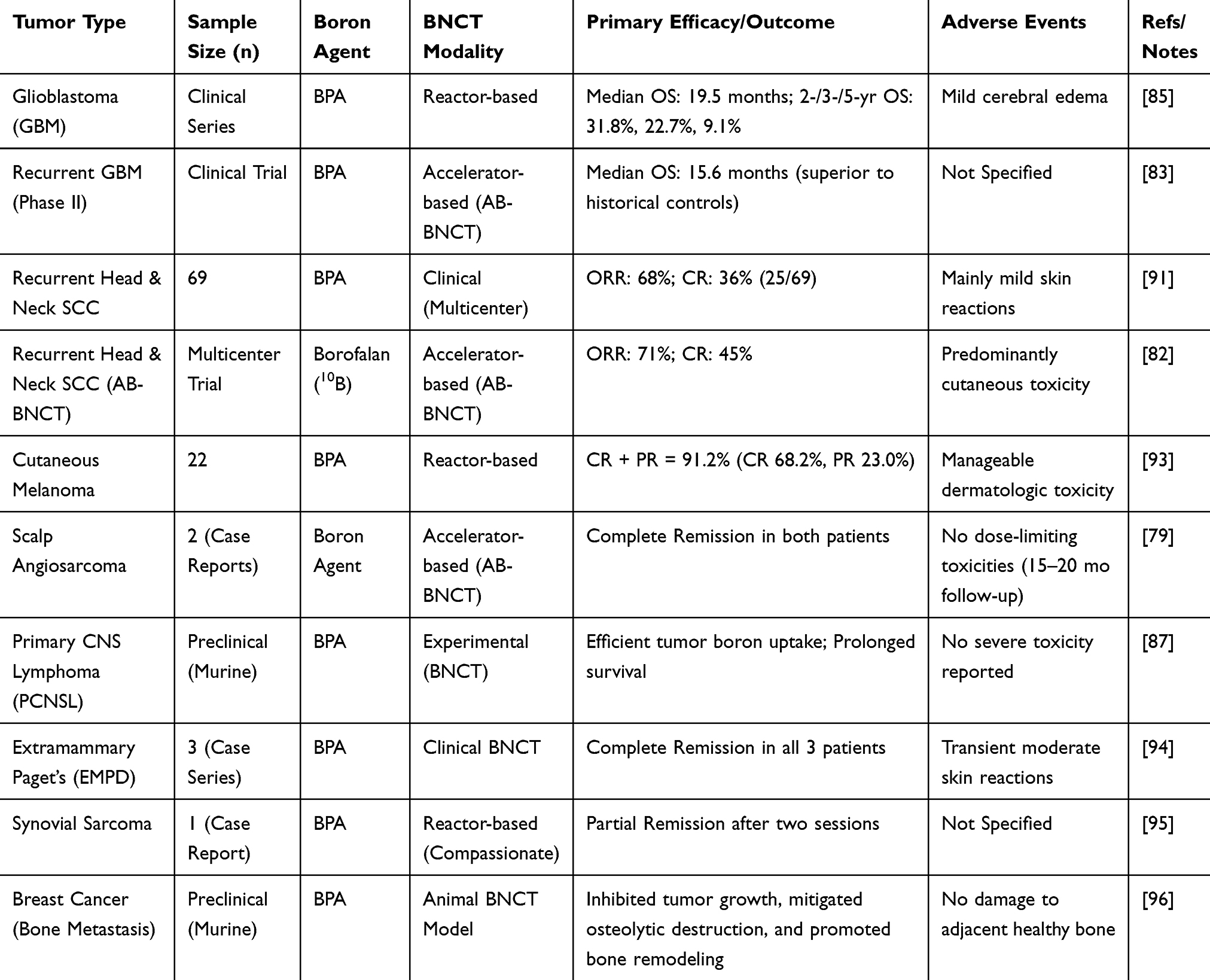 |
Table 4 Clinical and Representative Preclinical Outcomes of BNCT in Refractory Tumors |
The cumulative preclinical and clinical evidence solidly positions BNCT as a viable and selective therapy for refractory malignancies. However, its widespread adoption is contingent upon overcoming two core translational challenges: optimizing delivery systems for greater specificity and efficiency, and establishing standardized dosimetric and safety frameworks. The following sections will first delve into the optimization strategies and persisting barriers associated with BNCT delivery systems.
Optimization of BNCT Delivery Systems and Barriers to Clinical Translation
As BNCT transitions from preclinical evaluation toward broader clinical implementation, two principal challenges emerge: (1) further optimization of delivery systems, and (2) addressing system-level translational barriers. The first, encompassing strategies to enhance delivery specificity and overcome key bottlenecks, will be discussed in the section “Optimization of BNCT Delivery Systems and Barriers to Clinical Translation.” The second, which includes challenges in dosimetry, safety, and manufacturing, will be addressed in the subsequent section, “Translational Challenges and Technical Frontiers in BNCT Dosimetry and Safety.”
Optimization of Delivery Specificity
The selective accumulation of boron agents within tumor tissues is the cornerstone for maximizing therapeutic efficacy while minimizing systemic toxicity in BNCT. Enhancing tumor targeting can be achieved not only by rationally engineering the delivery vehicles themselves but also through pretargeting approaches that decouple tumor recognition from boron delivery.
Ligand-Modified Targeting Strategies
Compared with non-specific uptake pathways such as passive diffusion or phagocytosis, receptor-mediated endocytosis offers superior selectivity and cellular internalization efficiency. Covalent conjugation of tumor-specific ligands—including small molecules, peptides, antibodies, or antibody fragments—to the surface of nanocarriers enables targeted recognition of overexpressed receptors on tumor cells and facilitates enhanced boron accumulation.
For instance, Singh et al developed folic acid (FA)-modified liposomes (FA-3PCB) that exploit the overexpression of folate receptors on C6 glioma cells. This design achieved markedly improved tumor cell uptake, boron accumulation, and BBB penetration.95 Similarly, Kuthala et al engineered anti-EGFR antibody-conjugated 10B-containing phosphate nanoparticles (10BPO4 NPs), leveraging the high EGFR expression in head and neck cancers to achieve superior cytotoxicity and tumor control compared with BPA-F-mediated BNCT.94 Furthermore, Kawai K and Tsujino K demonstrated that conjugation of cyclic RGD peptides (cRGD) to boronated compounds, such as MID-BSA and MID-AC, can specifically target αvβ3 integrins, which are highly expressed in tumor cells and the neovasculature.96,97 These studies collectively affirm that ligand modification is a key strategy for enhancing BNCT selectivity, tumor penetration, and therapeutic precision.
Pretargeting Strategy
The pretargeting strategy leverages bioorthogonal click chemistry, specifically the inverse electron-demand Diels–Alder (IEDDA) reaction between trans-cyclooctene (TCO) and tetrazine (Tz).98 This reaction exhibits exceptionally rapid kinetics (with rate constants up to 103–106 M⁻1s⁻1) and high bioorthogonality, outperforming other bioorthogonal pairs.99 These properties enable the efficient anchoring of boron-loaded nanocarriers at pre-localized tumor sites.
A key advantage of this approach is the physical separation of the targeting ligand from the therapeutic payload. This decoupling allows for independent optimization of their respective pharmacokinetics, thereby enhancing overall delivery precision. An optimal pretargeting interval—defined as the time delay between antibody and nanocarrier administration—typically ranges from 24 to 72 hours.100 During this interval, unbound TCO-modified antibodies are systematically cleared from the body, primarily through renal excretion. For instance, the CC49-TCO conjugate exhibits a half-life of approximately 18 hours in mice, with its blood concentration decreasing to less than 5% of the peak level by 72 hours.100
Furthermore, administering a clearing agent (eg, Tz-functionalized dextran polymers101) before nanocarrier injection can sequester any residual circulating TCO-antibodies. This step significantly improves the tumor-to-normal tissue (T/N) boron concentration ratio. This strategy can elevate the T/N ratio to approximately 40:1, a substantial improvement over the approximately 10:1 ratio typically achieved with conventional direct targeting.101 The enhanced selectivity thereby mitigates the risk of boron-associated toxicity in normal tissues such as bone marrow and kidneys.
The pretargeting procedure involves two key steps. First, a TCO-functionalized monoclonal antibody (mAb) targeting a tumor-associated antigen is administered, facilitating its selective accumulation at the tumor site.102 For instance, in colorectal cancer models overexpressing carcinoembryonic antigen (CEA), a TCO-modified anti-CEA monoclonal antibody (mAb) demonstrated high tumor uptake, with unbound antibodies being efficiently cleared within 24 to 72 hours.103 Similarly, for targeting CA19.9 in pancreatic cancer, the TCO-functionalized 5B1 antibody achieved a tumor-to-blood concentration ratio of 15–20 at 72 hours, establishing a solid foundation for subsequent nanocarrier docking.104 In HER2-positive models, TCO-conjugated trastuzumab retained its binding affinity and was effectively internalized.105
In the second step, a tetrazine (Tz)-functionalized boron-enriched nanocarrier is administered. This modular design is compatible with diverse delivery platforms, including liposomes and polymeric nanoparticles, regardless of their intrinsic targeting capabilities. For example, cationic boron-rich liposomes can be surface-engineered with Tz groups,106 while supramolecular boron carriers may utilize Tz-functionalized cyclodextrin-boron complexes.107
Among various platforms, gold-based nanocarriers offer several advantages, including chemical inertness, low biotoxicity, and facile surface functionalization. In A431 squamous cell carcinoma models, Tz-functionalized boron-enriched gold nanoclusters resulted in an 8- to 12-fold increase in intratumoral gold content compared to passive delivery, with boron levels meeting the requirements for effective BNCT.108 Beyond gold, Tz-modified boron-doped carbon nanotubes yielded a boron concentration in HT29 colorectal xenografts 25-fold higher than in normal intestinal tissue.109,110 Similarly, Tz-functionalized HPMA copolymer-based nanoparticles demonstrated prolonged tumor retention, exceeding 72 hours, in pancreatic cancer models.111
Boron-incorporated gold nanoparticles represent a promising theranostic platform, characterized by their pronounced chemical inertness and inherent biocompatibility. Their robust resistance to oxidative degradation under physiological conditions, coupled with surface functionalization via PEGylation, effectively confers stealth characteristics by attenuating uptake by the reticuloendothelial system. Furthermore, comprehensive long-term toxicological assessments revealed no statistically significant deviations in standard hepatic and renal function biomarkers following the administration of Tz-boron-gold nanoparticles. These findings collectively support the biocompatibility of this nanoconstruct and strengthen its potential for safe clinical translation.112–114
Despite these merits, the pretargeting methodology is confronted by several translational hurdles. A primary concern is the intrinsic instability of its constituent molecules; notably, trans-cyclooctene (TCO) undergoes isomerization to its less reactive cis-cyclooctene (CCO) form, with conversion rates observed at 30–40% over 24 hours. This degradation process, which specific conjugation chemistries may further accelerate, can result in a substantial 25–30% reduction in tetrazine (Tz) binding efficiency, thereby compromising the overall efficacy of the strategy.115 Second, tetrazine probes exhibit suboptimal pharmacokinetics; hydrophobic variants are prone to hepatic sequestration, while their hydrophilic counterparts suffer from poor tumor penetration and potential ligand dissociation.116
Third, nanocarrier applications are constrained by significant reticuloendothelial system (RES) uptake and inadequate penetration into dense tumor stroma. This results in predominantly superficial accumulation and subtherapeutic boron concentrations in the tumor core.115,116 Finally, operational complexity and immunogenic risks pose additional hurdles. Clearing agents may reduce tumor uptake and can induce hypersensitivity reactions, while humanized antibodies may elicit human anti-human antibody (HAHA) responses, which can complicate repeated administration.99,117 Clinical translation is further hampered by the need to optimize multiple system-specific variables without a universal predictive model, thereby escalating the cost and duration of dose-finding studies.101,118
In summary, the continued refinement of ligand-directed and pretargeted delivery platforms is critical for advancing BNCT toward clinical translation. Future work should prioritize the stabilization of bioorthogonal components, the rational design of nanocarriers with improved tumor penetration and systemic clearance, and the establishment of standardized protocols for dosimetry and immune safety assessment.
Key Bottlenecks and Optimization Strategies for Enhancing Delivery Efficiency
Efficient delivery of boron agents to tumor sites remains the central determinant of therapeutic success in BNCT. In clinical translation, delivery efficiency is constrained by multiple factors, including achieving sufficient boron atom loading, precise control of release kinetics, and effective navigation through the complex physiological and biological barriers of the tumor microenvironment. These parameters critically influence intratumoral boron accumulation, tumor selectivity, and, ultimately, the therapeutic efficacy and safety during neutron irradiation. This section systematically discusses three major bottlenecks limiting delivery efficiency—boron loading, controlled release, and barrier penetration—and presents corresponding optimization strategies aimed at establishing a more efficient and precise BNCT delivery platform.
Increasing Boron Loading
Effective BNCT requires sufficient boron accumulation in the tumor, typically exceeding 20 μg/g of tissue, with high tumor-to-normal tissue (T/N) and tumor-to-blood (T/B) ratios. Conventional delivery systems, such as liposomes, often exhibit limited loading capacity, which makes it challenging to achieve the high boron concentrations required. Optimization strategies have focused on employing high-capacity nanocarriers, such as dendrimers or mesoporous silica nanoparticles, or designing novel boron-containing compounds.
Nakamura H et al developed a liposome-based boron delivery system (Boron Delivery System, BDS) that addresses these challenges by encapsulating boron within the aqueous core or incorporating it into the lipid bilayer. Various boron-containing liposomes designed under this framework have demonstrated substantial boron accumulation in tumor tissues and high T/B ratios, showing potential to meet the pharmacological demands of BNCT.119
Controlling Release Kinetics
Precisely regulating the release kinetics of boron agents is another key challenge for optimizing BNCT efficacy. Rapid release may result in premature clearance from circulation (eg, free 10BA exhibits a short half-life of approximately 2.1 hours). In contrast, slow release may prevent achieving effective intratumoral concentrations (≥20 μg/g) within the neutron irradiation window (typically 24–48 hours).
To address this, microenvironment-responsive release systems have been developed. For instance, Huang et al engineered PEO/PLA block copolymer nanofibers (55–100 nm in diameter) capable of dual-phase release kinetics.120 By modulating the hydrophilic-to-hydrophobic ratio (PEO/PLA = 3:2), the system released 44.4% of 10BA within 12 hours, rapidly elevating the tumor boron concentration, followed by sustained release (53.5% over the next 24 hours) to maintain therapeutic levels. The electrospun nanofiber network (porosity 78 ± 5%) combined the enzymatic degradability of PLA and the swelling behavior of PEO, achieving a tumor boron concentration of 2540 μg/g (T/B ratio 80.6) in H22 tumor-bearing mice—far exceeding the BNCT threshold. Mechanistic studies revealed that this controlled-release approach induced extensive DNA double-strand breaks, as quantified by the comet assay (TailDNA% = 78.9%, indicating severe DNA fragmentation), and mitochondrial membrane potential collapse (ΔΨm reduction 62%), yielding 3.8-fold greater efficacy and extending median survival beyond 75 days compared to free 10BA.120 This material-interface-engineered strategy effectively integrates boron loading, release modulation, and therapeutic enhancement, providing a comprehensive solution for localized BNCT applications, particularly in the treatment of postoperative residual tumors.
Overcoming Tumor Delivery Barriers
Efficient boron delivery necessitates overcoming dual-level barriers. At the tissue level, physiological constraints—such as the blood-brain barrier (BBB), dense tumor stroma, and elevated interstitial fluid pressure—impede nanoparticle penetration and accumulation in deep tumor regions. At the cellular level, limited membrane permeability, efflux pump overexpression, and endosomal entrapment further restrict intracellular retention of boron compounds.121–124
To bypass the BBB, Kusaka S et al employed a cerebrospinal fluid (CSF)-based delivery approach for boronophenylalanine (BPA) in a C6 glioma rat model.125 By harnessing CSF–interstitial fluid exchange dynamics through subdural infusion of BPA (8 mg/kg/h for 2 hours), this strategy achieved tumor boron concentrations of 2540 μg/g—comparable to intravenous administration at 350 mg/kg—while markedly reducing boron accumulation in normal tissues (eg, oral mucosa boron levels decreased by 82%). Mechanistically, CSF-mediated transport enhanced BPA penetration via aquaporin-4 (AQP4)-driven astrocytic flow. Within 24 hours post-treatment, boron levels in normal brain parenchyma declined rapidly (78% reduction vs 35% in the intravenous group), minimizing healthy tissue exposure. Both delivery routes achieved comparable tumor suppression, but CSF administration resulted in faster recovery (5% vs 20% body weight loss at one week).125 These findings establish CSF circulation delivery as a low-dose, high-selectivity method for penetrating the BBB, offering a promising paradigm for BNCT in brain tumors. Beyond pharmacological and physical circumvention strategies, biological approaches leveraging cell-based “living carriers” also represent a promising avenue to overcome the BBB, as discussed in the context of cell-mediated delivery concepts.
Collectively, these three optimization strategies—enhanced boron loading, controlled release kinetics, and barrier circumvention—provide targeted solutions to overcome the major delivery bottlenecks in BNCT. The integration of these approaches is expected to advance the development of next-generation, high-efficiency, and precision-oriented BNCT delivery systems. The key bottlenecks and corresponding optimization strategies are summarized in Table 5.
 |
Table 5 Optimization Strategies to Enhance BNCT Delivery Efficiency |
Translational Challenges and Technical Frontiers in BNCT Dosimetry and Safety
Quality and Characteristics of Neutron Sources
The therapeutic efficacy and safety of BNCT are highly dependent on the quality and core characteristics of the neutron source, which determine the precision, safety, and clinical accessibility of treatment—a relationship validated by multiple multicenter studies. Clinically utilized neutron sources can be broadly classified into two categories: reactor-based and accelerator-based systems.126
Reactor-based neutron sources, such as Japan’s JRR-4, generate high thermal neutron fluxes (approximately 2.3 × 1012 n/(cm2 s)) via nuclear fission. These are subsequently moderated (eg, by lithium fluoride–graphite moderators) and filtered (eg, using Pb–Bi alloy filters) to produce clinical-grade epithermal neutron beams (epithermal fraction ≥85%).127 Their principal advantage lies in their high neutron flux and uniform energy spectrum, which laid the foundation for early BNCT clinical investigations. However, their inherent limitations—including large physical footprint (≥500 m2), stringent nuclear safety regulations (IAEA level 2 compliance), and extremely high capital and maintenance costs (>$30 million per system; approximately $2 million annually)—render them impractical for widespread hospital implementation, thus constraining clinical translation.
In contrast, accelerator-based BNCT (AB-BNCT) systems produce neutrons through proton–target nuclear reactions—typically by accelerating protons (15–25 MeV) to bombard beryllium (9Be) or lithium (7Li, 0.5–1 mm thick) targets, triggering (p,n) reactions [7Li(p,n)7Be or 9Be(p,n)9B].128 This approach represents the current mainstream direction of BNCT research and clinical application. AB-BNCT systems offer a compact design (footprint ≤ 150 m2), compatibility with hospital infrastructure, and superior radiation shielding (borated polyethylene + lead composites, ambient dose ≤ 0.1 μSv/h). Clinical studies have reported a 40% reduction in adverse event incidence compared to reactor-based systems, with no Grade 3 or higher events observed within 90 days post-treatment. Moreover, neutron energy spectra can be tuned to match tumor types (eg, 0.5–1 eV for breast cancer; 1–5 eV for brain tumors). Recent clinical trials demonstrated objective response rates up to 71%, highlighting the translational potential of AB-BNCT as a precision radiotherapeutic platform for refractory malignancies.
Challenges in Dosimetric Standardization
The dosimetry of BNCT is fundamentally dependent on the real-time spatiotemporal distribution of boron-10 within tissues. However, a significant clinical limitation persists due to the absence of technologies capable of online, real-time, and quantitative monitoring of boron concentration. While nano-engineered boron delivery systems have demonstrated superior tumor targeting and prolonged retention in preclinical studies, their clinical translation is hampered by several key challenges:46,129,130 (i) the lack of a unified dosimetric standard for nanocarriers; (ii) potential long-term safety and immunogenicity concerns; and (iii) difficulties in achieving scalable and compliant manufacturing processes. In response, researchers are developing boron imaging techniques, such as Prompt Gamma-ray SPECT (PG-SPECT) or MRI-based methods, for integration into treatment planning systems to enable more accurate dose control.131
It is crucial to acknowledge that the pharmacokinetics and biodistribution profiles of nanocarriers—characterized by heterogeneous intratumoral distribution, ligand-mediated cellular uptake, and prolonged retention times—are fundamentally distinct from those of small-molecule boron agents, such as BPA and BSH. Consequently, traditional BNCT dosimetric models, which assume uniform boron distribution, are inadequate for nanocarrier-based delivery systems. For instance, the dosimetry for nuclear-targeting agents (eg, DOX-CB@lipo-pDNA-iRGD) necessitates the development of subcellular-level models that correlate boron proximity to the nucleus with DNA damage efficiency, moving beyond reliance on average tissue concentration alone.130
Furthermore, the integration of quantitative boron imaging techniques—such as PET with 18F-BPA, MRI, or emerging neutron capture imaging (NCI)—into real-time treatment planning is currently impeded by a lack of standardized protocols.132 The discrepancy between imaging signals (eg, PET SUV values) and the actual boron concentration measured via gold-standard methods, such as ICP-MS, critically undermines the comparability of results across different institutions.133 Therefore, the establishment of validated, imaging-informed dosimetric protocols is imperative to realize personalized BNCT and facilitate robust multi-center clinical trials.
Long-Term Biocompatibility and Safety Considerations
Long-term biodistribution of nanocarriers poses potential risks of chronic toxicity, as many boron nanostructures—such as boron nitride nanotubes (BNNTs), metal–organic frameworks, and nondegradable polymers—tend to accumulate in reticuloendothelial system organs (liver, spleen, kidneys). Such persistence may elicit chronic inflammatory or fibrotic responses.66 For example, rodent studies using BNNTs have reported sustained inflammation and fibrosis even at therapeutic doses, underscoring the urgent need for long-term (6–12 months) toxicological evaluation. To date, comprehensive chronic safety assessments remain largely absent from BNCT nanocarrier development, representing a critical knowledge gap.
Immunogenicity
Surface engineering strategies—such as PEGylation, antibody conjugation, or peptide ligand decoration—while optimizing drug delivery properties, frequently elicit unintended immune responses. The generation of anti-drug antibodies (ADA) represents a significant clinical risk, significantly impacting therapeutic efficacy.73 Studies indicate that approximately 20% of patients receiving PEGylated liposomes develop anti-PEG antibodies, which can accelerate blood clearance and directly compromise treatment outcomes. Notably, screening of plasma samples from a German cohort revealed an anti-PEG antibody positivity rate of up to 83%. Moreover, anti-PEG antibodies are specifically enriched in the protein corona of PEGylated nanocarriers, enhancing their uptake by macrophages and thereby counteracting the intended stealth effect of PEGylation.134 Similarly, ADAs generated against engineered targeting moieties, such as cetuximab displayed on liposomal surfaces, can provoke hypersensitivity reactions or neutralize the targeting capability of the drug, further limiting therapeutic utility.74 Additionally, immunogenicity risks associated with antibody-drug conjugates (ADCs) may arise from multiple structural components, including the antibody scaffold, linker, and payload, where heterogeneity or degradation products can trigger immune activation, affecting both safety and efficacy.135
Insights from pathogen transmission interception strategies, which target “pathogen-carrier nodes,” suggest that effective immune intervention does not necessarily rely on the most immunogenic targets, but can be rationally optimized through chemical conjugation technology.136 When the pathogen carrier is immunogenic, conjugation can be designed to enhance targeted immune responses and block pathogenesis; conversely, to avoid hypersensitivity, conjugation strategies may be employed to induce immune tolerance, offering a versatile approach to immune modulation.137 This concept holds relevance for cancer immunotherapy, particularly in the context of BNCT. The high-linear energy transfer alpha particles generated during BNCT induce irreversible DNA double-strand breaks and cell membrane damage, leading to immunogenic cell death (ICD). Dying cancer cells release damage-associated molecular patterns (DAMPs)—such as ATP, HMGB1, and calreticulin—along with a spectrum of tumor-associated antigens and neoantigens. Neoantigens arising from tumor-specific mutations can be presented via human leukocyte antigen (HLA) molecules to immune cells, providing precise targets for immune recognition and helping overcome tumor immune evasion.138
However, the efficacy of conventional boron delivery agents has been limited by suboptimal tumor targeting and insufficient intracellular boron accumulation. While emerging protein-based delivery systems offer a promising solution to these bottlenecks, they face development challenges related to their intrinsic immunogenicity and the potential induction of ADAs. Such antibodies can not only reduce the bioavailability of the delivery system but also provoke immune-related adverse events.139 It is noteworthy that secondary lymphoid organs, particularly B cell follicles and germinal centers, serve as critical anatomical sites for ADA generation. The collaborative interaction between follicular helper CD4⁺ T cells and germinal center B cells dictates the magnitude and persistence of the antibody response.140 Therefore, co-delivery of immune adjuvants during BNCT could potentiate the activation of antigen-presenting cells (APCs) and T cells, amplify ICD-triggered immune signaling, and promote germinal center reactions. This approach may foster a more robust and sustained anti-tumor T cell and B cell (antibody) response, while mitigating the risks associated with nonspecific immune activation.141
The inherently low immunogenicity of cancer cells remains a central barrier in cancer immunotherapy. Enhancing tumor immunogenicity requires a balanced consideration of efficacy, specificity, and safety. Although conventional therapies can augment immunogenicity by increasing antigen expression or inducing ICD, they often suffer from inadequate targeting and significant off-target effects.142 BNCT offers the advantage of modulating ICD intensity and inflammatory levels by adjusting the neutron irradiation dose, although the long-term safety of repeated applications requires further evaluation.143 Nanomedicines provide a promising avenue for addressing these challenges. They enable the targeted delivery of tumor antigens, immune adjuvants, epigenetic modulators, or ICD inducers, thereby minimizing off-target effects. Furthermore, nanocarriers can induce ICD directly within the tumor microenvironment, releasing a broad spectrum of immune-recognition signals and awakening tumor immunogenicity. Some nanoformulations can also reduce ADA risk by optimizing the composition of the protein corona and minimizing the exposure of immunogenic components. In summary, through mechanisms such as targeted antigen delivery, in situ ICD induction, or epigenetic remodeling, nanomedicines can help overcome biological barriers in immunotherapy, efficiently present tumor antigens to the immune system, and lay the groundwork for the comprehensive eradication of tumors.
Manufacturing and Regulatory Hurdles
The scalable production of complex nanoformulations faces significant challenges, particularly in achieving batch-to-batch consistency. The inherent complexity of nanostructures, coupled with the necessity to tightly control critical quality attributes (CQAs) such as particle size, boron payload, and ligand density, complicates their precise analytical characterization.144,145 These analytical and quality control difficulties consequently hinder the reliable reproduction of in vivo targeting efficacy and safety profiles across production batches.
From a regulatory perspective, a dedicated and specific framework for nanoformulated BNCT agents is currently absent. Regulatory agencies, including the US FDA and China’s NMPA, continue to require data conforming to fundamental drug evaluation standards. For instance, the NMPA’s 2023 “Technical Guideline for Clinical Trials of Nanomedicines” stipulates that boron nanocarriers must demonstrate consistent particle size distribution (RSD < 10%), boron content (deviation < 5%), and in vitro release profiles (f2 > 50) across three pilot-scale batches. Similarly, the FDA mandates long-term toxicity studies (6 months in rats, 12 months in dogs), with particular emphasis on monitoring hepatic and splenic accumulation. While the existing regulatory framework ensures baseline safety and quality, the lack of tailored technical guidance may potentially impede the translational efficiency of innovative nanotechnologies.
Moving forward, a collaborative effort among industry, academia, and regulatory bodies is essential. Leveraging accumulated preclinical and clinical data, there is a pressing need to establish product-specific review criteria, standardized testing methodologies, and safety thresholds. This collaborative approach will be instrumental in developing specialized regulatory provisions that align with international standards while accommodating the unique technical characteristics of nanoformulated BNCT drugs. Such a pathway will not only ensure patient safety but also provide a clear and predictable route for the standardized development and clinical application of these advanced therapeutics.
In summary, the clinical translation of BNCT is a multidimensional endeavor intersecting targeting specificity, delivery efficiency, dosimetric standardization, and long-term safety. As synthesized in Table 6, a systematic analysis of these bottlenecks and their corresponding optimization pathways forms the critical roadmap for advancing BNCT from preclinical promise to clinical reality.
 |
Table 6 Significant Translational and Technical Challenges in BNCT |
Synthesis of Delivery Challenges and Optimization Pathways
The clinical translation of BNCT delivery systems is a multifaceted endeavor, confronting interconnected challenges that span targeting specificity, delivery efficiency, dosimetric standardization, and long-term safety. As systematically analyzed in Figure 6, these bottlenecks and their corresponding optimization strategies form a critical roadmap for advancing BNCT from preclinical promise to clinical reality. Beyond optimizing BNCT as a monotherapy, integrating it with other modalities like chemotherapy and immunotherapy has emerged as a powerful strategy to enhance its efficacy and address tumor heterogeneity.
 |
Figure 6 Key Bottlenecks and Optimization Pathways of Boron Neutron Capture Therapy (BNCT) Delivery Systems: As the core connecting hub between boron drugs, neutron beams, and tumor targets, this delivery system directly determines the efficacy and safety of treatment. The figure presents three major bottlenecks and their corresponding optimization strategies: Part (A) addresses the issue of low boron loading, which can be resolved using high-capacity nanostructures, such as self-assembled A6K peptide nanotubes (A6K and BSH mixed at a 1:10 molar ratio to form spherical nanocomplexes with an average particle size of 39.3±17.4 nm and a zeta potential of −38.2±1.9 mV) and folic acid-conjugated liposomes (composed of PMAO- and PEG-modified lipid bilayers with an aqueous core encapsulating 3PCB and Cy5); these liposomes exhibit a significantly improved tumor-to-normal tissue (T/N) boron concentration ratio compared to conventional formulations. Part (B) addresses the problem of uncontrolled release kinetics, which can be optimized via stimuli-responsive systems, such as PEO/PLA block copolymer nanofibers constructed by electrospinning with a PEO/PLA ratio of 3:2; the porous fiber network formed enables biphasic release (44.4% of 10BA released within 12 hours and 53.5% in the subsequent 24 hours), thereby inducing DNA double-strand breaks (DSBs) and mitochondrial membrane potential collapse in tumor cells. Part (C) addresses the challenge of tumor delivery barriers, which can be overcome by circumventing physiological barriers (including the blood-brain barrier (BBB), dense tumor stroma (DTS), and high interstitial fluid pressure (HIFP)), low tumor cell membrane permeability, overexpression of drug efflux pumps, and failure of endosomal escape; an example is the delivery of BPA via cerebrospinal fluid (CSF) circulation (subdural injection) to bypass the BBB, thereby enhancing BPA penetration into tumors, resulting in a rapid increase in tumor boron concentration within the first 12 hours followed by sustained release. |
Combinatorial Therapeutic Strategies Using Boron-Based Nanosystems
As clinical research on BNCT deepens, the limitations of standalone BNCT for highly heterogeneous and aggressive refractory tumors have become increasingly apparent. In recent years, the combined application of nanotechnology-based boron delivery systems with other treatment modalities—such as chemotherapy and immunotherapy—has emerged as a crucial direction for enhancing the efficacy of BNCT. Leveraging their advantages in co-delivery of multiple agents, controllable release, targeted delivery, and functional integration, nanocarriers provide an ideal platform for achieving spatiotemporally precise synergistic therapy. Existing research primarily focuses on the following combinatorial strategies:
Chemo-BNCT Combination Therapy
This strategy employs nanosystems to co-deliver boron agents and traditional chemotherapeutic drugs (eg, paclitaxel, doxorubicin), exploiting different mechanisms to produce synergistic effects. Huang et al fabricated PEO/PLA block‑copolymer nanofibers that co‑deliver 10B‑containing agents (10BA) and paclitaxel.120 The system exhibits sequential release: paclitaxel is released first to disrupt tumor vasculature and arrest the cell cycle, thereby sensitizing cells to the subsequently released 10BA, which upon neutron irradiation generates high‑LET particles that inflict lethal DNA damage. Another representative study is the LA‑BPA derivative-based, pH-responsive multifunctional vesicles developed by Dai et al.146 The vesicles, surface-modified with phenylboronic acid groups, target sialic acid on tumor cell surfaces, enhancing cellular uptake and lysosomal escape, and can be loaded with doxorubicin (DOX). Triggered release in the high-glutathione tumor microenvironment enables sequential chemo-BNCT therapy. In pancreatic cancer and melanoma models, these vesicles demonstrated high tumor accumulation (T/N ratio up to 6.7–7.7) and significant tumor growth inhibition coupled with extended survival following combined treatment, showcasing the feasibility of integrating targeted chemotherapy and BNCT on a single nanoplatform.
Immuno-BNCT Combination Therapy
The immunogenic cell death (ICD) induced by BNCT provides a theoretical foundation for its combination with immunotherapy. Nanocarriers can co-deliver boron agents and immunomodulators (eg, cytokines, immune checkpoint inhibitors, STING agonists), aiming to locally activate the immune microenvironment and elicit a systemic anti-tumor immune response.
One strategy involves directly harnessing BNCT byproducts for immune activation. Research shows that extracellular vesicles (EVs/BNCT-EVs) released from tumor cells following BNCT treatment are enriched with DNA fragments due to high-LET radiation. Upon uptake by dendritic cells (DCs), these EVs/BNCT-EVs potently activate DNA-sensing pathways like cGAS-STING, driving DC maturation. In a melanoma model, a DC vaccine pre-pulsed with these EVs/BNCT-EVs significantly inhibited primary tumor growth and lung metastasis while inducing long-term immune memory.147 This strategy directly converts BNCT radiation products into endogenous adjuvants for anti-tumor immunity, offering a novel paradigm for synergizing BNCT with cellular immunotherapy.
Another strategy focuses on designing multifunctional nanosystems co-delivering immunomodulatory components. For example, Chen et al developed a nucleus-targeting liposomal system (DOX-CB@lipo-iRGD) for the co-delivery of carborane and a CRISPR-Cas9 plasmid targeting CD47.12 In glioblastoma models, this design leveraged the nuclear translocation property of DOX to efficiently accumulate boron within tumor cell nuclei, thereby significantly enhancing BNCT-mediated DNA damage. Simultaneously, the CRISPR-Cas9 system knocked out the “don’t-eat-me” signal CD47 on tumor cells, promoting macrophage phagocytosis and impairing cancer stem-cell phenotypes. The combination of BNCT and immunotherapy synergistically inhibited tumor growth, reduced stemness, and decreased recurrence risk, leading to improved survival—demonstrating a compelling integrated therapeutic strategy. Similarly, Deng et al developed PD-L1 siRNA-loaded boron nanoparticles (10B/siPD-L1).148 This system achieves tumor-selective uptake via cRGD targeting ligands and releases 10B polymers and siRNA in the highly reductive tumor cytosol. The PD-L1 siRNA not only inhibits BNCT-induced PD-L1 upregulation to activate T-cell immunity but also enhances BNCT’s DNA damage effect by suppressing PD-L1-mediated DNA repair protein expression, thereby inducing stronger ICD and anti-tumor immune responses. In a breast cancer model, this combinatorial therapy demonstrated promising synergistic tumor suppression and anti-metastatic potential.
Multimodal Synergistic Therapy
Beyond chemotherapy and immunotherapy, BNCT can also be combined with other physical treatment modalities—such as photothermal therapy (PTT)—to form multimodal synergistic therapy platforms. A representative example is the Au@BNNT (gold-boron nitride nanotube) platform.65 This hybrid nanocarrier leverages the innate high boron-loading capacity of BNNTs for BNCT, while the incorporated gold components confer strong near-infrared photothermal conversion efficiency. The sequential application of local PTT prior to neutron irradiation can disrupt the dense tumor stroma, enhance vascular permeability and blood perfusion, thereby significantly improving the penetration and homogeneous distribution of boron agents throughout the tumor mass. By leveraging the intersecting actions of different mechanisms, these multimodal strategies hold promise for overcoming the single-agent resistance caused by tumor heterogeneity, reducing the required dose of each treatment modality, and thereby mitigating toxic side effects.
In summary, existing research robustly demonstrates the significant potential of boron-based nanosystem combinatorial strategies—primarily including chemo-BNCT, immuno-BNCT, and multimodal synergistic therapy (eg, with photothermal or sonodynamic modalities)—in enhancing therapeutic outcomes for refractory tumors. These strategies leverage the precise control offered by nanotechnology to achieve optimized spatiotemporal synergy between different therapies. Chemo- and immuno-BNCT strategies not only improve local tumor eradication but also hold promise for eliciting systemic anti-tumor immunity to control distant metastases. Multimodal approaches aim to overcome physiological barriers and tumor heterogeneity through complementary mechanisms. Future research should focus on further optimizing combinatorial regimen design (eg, sequencing, timing) and advancing these innovative strategies toward standardized, reproducible clinical translation. Looking beyond these incremental optimizations, several emerging and potentially disruptive technologies are poised to redefine the future landscape of BNCT, as discussed in the next section.
Emerging Frontiers and Disruptive Technologies
Looking beyond the incremental optimization of existing platforms, several emerging technologies hold the potential to redefine the future of BNCT.
mRNA and In vivo Boron Programming
Inspired by the success of mRNA-LNP (lipid nanoparticle) vaccines, a groundbreaking approach involves transiently programming tumor cells to synthesize their own boron-capturing proteins. By delivering mRNA encoding for boron-affinity proteins or transporters directly to the tumor site, this strategy could shift the paradigm from delivering boron drugs to engineering the tumor itself to sequester boron, potentially achieving unprecedented levels of intracellular concentration and specificity.
Artificial Intelligence and Digital Twins for Treatment Planning
The complexity of BNCT dosimetry, which depends on real-time, spatial boron distribution, is a primary challenge for AI. Machine learning models can integrate patient-specific data—including prior PET/MRI scans, tumor genomics, and pharmacokinetic models—to predict optimal timing for neutron irradiation and forecast 3D dose distribution. Furthermore, creating a “digital twin” of the patient’s treatment using Monte Carlo simulations allows for the virtual testing and optimization of BNCT plans in silico, ensuring maximum efficacy and safety before the actual treatment begins.
In situ Vaccination and Systemic Immunomodulation
BNCT is uniquely potent at inducing immunogenic cell death (ICD). The next frontier is to systematically harness this effect to turn the tumor into an in situ vaccine. This involves rationally combining BNCT with immunomodulatory agents (eg, checkpoint inhibitors, STING agonists) that are co-delivered via nanocarriers. The key lies in optimizing the sequence and timing—administering immunotherapies when the “danger signals” from BNCT are at their peak—to convert a localized treatment into a robust, systemic anti-tumor immune response capable of attacking distant metastases.
In summary, these emerging frontiers—ranging from in vivo programming to AI-driven planning and systemic immunomodulation—collectively highlight a transformative potential for BNCT, moving beyond incremental improvements toward novel therapeutic paradigms. The integration of these concepts forms the basis for the concluding outlook on the field.
Conclusions and Outlook
This review delineates the evolution of boron neutronron capture therapy (BNCT) from a promising yet pharmacokinetically constrained binary radiotherapy into an integrative precision oncology platform, a transformation fundamentally catalyzed by advances in nanotechnology-enabled boron delivery. The advent of smart nanocarriers—featuring high payload capacity, active targeting, controlled release, and nuclear localization—has directly overcome the historical limitations of low tumor selectivity and rapid clearance inherent to conventional small-molecule agents.
Looking ahead, the clinical translation of BNCT depends on concerted advances along two complementary axes: next-generation technological integration and system-level translational enablers. On the technological front, future efforts must focus on developing multifunctional theranostic platforms that seamlessly combine real-time imaging, tumor-microenvironment-responsive drug release, and co-delivery of immunomodulators to potentiate BNCT-induced immunogenic cell death into a systemic anti-tumor immune response. Concurrently, the integration of artificial intelligence and digital twin technology is crucial for harnessing complex multimodal data to achieve truly personalized dosimetry and dynamic treatment planning.
To translate these technological promises into clinical reality, addressing system-level challenges is imperative. This includes the standardization of neutron sources and dosimetric protocols, the establishment of robust, scalable, and GMP-compliant manufacturing processes, and a comprehensive understanding of the long-term biocompatibility and immunogenicity of novel nanocarriers. Proactive collaboration among academia, industry, and regulatory bodies will be key to developing tailored evaluation frameworks and accelerating clinical adoption.
In summary, the synergy of nanomedicine, advanced imaging, radiation physics, and immuno-oncology is maturing BNCT into a powerful and versatile therapeutic modality. By systematically navigating the outlined roadmap—from smart nanocarrier design and AI-driven personalization to standardization and safety validation—BNCT is poised to transition from a promising experimental approach into a cornerstone of personalized therapy for refractory solid tumors, ultimately ushering in a new era of precision cancer radiotherapy.
Abbreviations
3D-CRT, three-dimensional conformal radiotherapy; AB-BNCT, accelerator-based boron neutron capture therapy; ACBC, 2-aminocyclobutane carboxylic acid; ADA, anti-drug antibodies; AI, artificial intelligence; ALI, acute lung injury; APCs, antigen-presenting cells; AQP4, aquaporin-4; ARDS, acute respiratory distress syndrome; BBB, blood-brain barrier; BNCT, boron neutron capture therapy; BDS, boron delivery system; BPA, boronophenylalanine; BSH, sodium borocaptate; BUN, blood urea nitrogen; CEA, carcinoembryonic antigen; CNS, central nervous system; CPP, cell-penetrating peptide; CR, complete response; CQAs, critical quality attributes; CSF, cerebrospinal fluid; DAMPs, damage-associated molecular patterns; DNA, deoxyribonucleic acid; EMPD, extramammary Paget’s disease; EPR, enhanced permeability and retention; FA, folic acid; FBY, trifluoroborate–tyrosine; FDA, Food and Drug Administration; FRα, folate receptor-α; GBM, glioblastoma multiforme; GMP, Good Manufacturing Practice; HAHA, human anti-human antibody; HLA, human leukocyte antigen; HNSCC, head and neck squamous cell carcinoma; HPMA, N-(2-hydroxypropyl) methacrylamide; ICD, immunogenic cell death; IEDDA, inverse electron-demand Diels–Alder; LAT1, L-type amino acid transporter 1; LET, linear energy transfer; LNP, lipid nanoparticle; mAb, monoclonal antibody; MOF, metal–organic framework; MRI, magnetic resonance imaging; NFPA, nonfunctioning pituitary adenoma; NLS, nuclear localization signal; NMPA, National Medical Products Administration; ORR, objective response rate; OS, overall survival; PAINT, point accumulation for imaging in nanoscale topography; PCNSL, primary central nervous system lymphoma; PET, positron emission tomography; PEG, polyethylene glycol; PLA, polylactic acid; PVA, poly(vinyl alcohol); RES, reticuloendothelial system; SERS, surface-enhanced Raman scattering; STED, stimulated emission depletion; STORM, stochastic optical reconstruction microscopy; T/B, tumor-to-blood ratio; T/N, tumor-to-normal tissue ratio; TCO, trans-cyclooctene; TfR1, transferrin receptor 1; Tz, tetrazine; VLPs, virus-like particles.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Joint TCM Science &Technology Project of National Demonstration Zone for Comprehensive TCM Reform under Grant No. GZY-KJS-ZJ-2025-064; National Natural Science Foundation of China (32401196); Public Welfare Technology Application Research Program of Huzhou (No. 2025GY095); Zhejiang Provincial Natural Science Foundation of China under Grant No.LTGD24H220001 and LQ24H300001; Zhejiang Province First Batch of “Small yet Strong” Clinical Innovation Team Project; Zhejiang Provincial “Jianbing” and “Lingyan” R & D Program (No.2024C03174); Natural Science Foundation of Hangzhou (2024SZRYBH090001); Natural Science Foundation of Jiangsu Province for Universities (24KJB350011); Natural Science Foundation Project of Taizhou Science and Technology Support Programme (Social Development) (TS202402); Qinglan Project of Jiangsu Province of China (2024).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barth RF, Mi P, Yang W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018;38(1):35. doi:10.1186/s40880-018-0299-7
2. Suzuki M. Boron neutron capture therapy (BNCT): a unique role in radiotherapy with a view to entering the accelerator-based BNCT era. Int J Clin Oncol. 2020;25(1):43–32. doi:10.1007/s10147-019-01480-4
3. Wang S, Zhang Z, Miao L, Li Y. Boron Neutron Capture Therapy: current Status and Challenges. Front Oncol. 2022;12:788770. doi:10.3389/fonc.2022.788770
4. Barth RF, Coderre JA, Vicente MG, Blue TE. Boron neutron capture therapy of cancer: current status and future prospects. Clin Cancer Res. 2005;11(11):3987–4002. doi:10.1158/1078-0432.Ccr-05-0035
5. Takeno S, Yoshino Y, Aihara T, et al. Preliminary outcomes of boron neutron capture therapy for head and neck cancers as a treatment covered by public health insurance system in Japan: real-world experiences over a 2-year period. Cancer Med. 2024;13(11):e7250. doi:10.1002/cam4.7250
6. Donya H, Umer M. Optimization of DD-110 Neutron Generator Output for Boron Neutron Capture Therapy Using Monte Carlo Simulation. Quantum Beam Sci. 2025;9(2):12.
7. Donya H, Alzahrani NM, Abdulsalam A, Umer M. Boron neutron capture therapy: a promising radiation treatment modality. Radiat Environment Biophys. 2025;64(3):339–353. doi:10.1007/s00411-025-01134-2
8. Barth RF, Gupta N, Kawabata S. Evaluation of sodium borocaptate (BSH) and boronophenylalanine (BPA) as boron delivery agents for neutron capture therapy (NCT) of cancer: an update and a guide for the future clinical evaluation of new boron delivery agents for NCT. Review. Cancer Commun. 2024;44(8):893–909. doi:10.1002/cac2.12582
9. Ariztia J, Solmont K, Moïse NP, et al. PET/Fluorescence Imaging: an Overview of the Chemical Strategies to Build Dual Imaging Tools. Review. Bioconjugate Chem. 2022;33(1):24–52. doi:10.1021/acs.bioconjchem.1c00503
10. Wang S, Ren WX, Hou J-T, et al. Fluorescence imaging of pathophysiological microenvironments. Review. Chem Soc Rev. 2021;50(16):8887–8902. doi:10.1039/d1cs00083g
11. Provenzano C, Marra M, Caricato AP, et al. Development of a High-Efficiency Device for Thermal Neutron Detection Using a Sandwich of Two High-Purity 10B Enriched Layers. Sensors. 2023;23(24):9831. doi:10.3390/s23249831
12. Chen J, Dai Q, Yang Q, et al. Therapeutic nucleus-access BNCT drug combined CD47-targeting gene editing in glioblastoma. J Nanobiotechnol. 2022;20(1):102. doi:10.1186/s12951-022-01304-0
13. Li J, Sun Q, Lu C, et al. Boron encapsulated in a liposome can be used for combinational neutron capture therapy. Nat Commun. 2022;13(1):2143. doi:10.1038/s41467-022-29780-w
14. Kashihara T, Nakamura S, Yamazaki N, et al. Boron neutron capture therapy for cutaneous angiosarcoma and malignant melanoma: first in-human Phase I clinical trial. Radiother Oncol. 2025;202:110607. doi:10.1016/j.radonc.2024.110607
15. Kankaanranta L, Seppälä T, Koivunoro H, et al. Boron neutron capture therapy in the treatment of locally recurred head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;69(2):475–482. doi:10.1016/j.ijrobp.2007.03.039
16. Aghevlian S, Boyle AJ, Reilly RM. Radioimmunotherapy of cancer with high linear energy transfer (LET) radiation delivered by radionuclides emitting α-particles or Auger electrons. Review. Adv Drug Deliv Rev. 2017;109:102–118. doi:10.1016/j.addr.2015.12.003
17. Helm A, Fournier C. High-LET charged particles: radiobiology and application for new approaches in radiotherapy. Review Strahlenther Onkol. 2023;199(12):1225–1241. doi:10.1007/s00066-023-02158-7
18. Jezkova L, Zadneprianetc M, Kulikova E, et al. Particles with similar LET values generate DNA breaks of different complexity and reparability: a high-resolution microscopy analysis of γH2AX/53BP1 foci. Nanoscale. 2018;10(3):1162–1179. doi:10.1039/c7nr06829h
19. Nikitaki Z, Velalopoulou A, Zanni V, et al. Key biological mechanisms involved in high-LET radiation therapies with a focus on DNA damage and repair. Review. Expert Rev Mol Med. 2022;24:15. doi:10.1017/erm.2022.6
20. Guan SQ, Liu XJ, Li CL, et al. Intracellular Mutual Amplification of Oxidative Stress and Inhibition Multidrug Resistance for Enhanced Sonodynamic/Chemodynamic/Chemo Therapy. Small. 2022;18(13):2107160. doi:10.1002/smll.202107160
21. Jaganjac M, Milkovic L, Zarkovic N, Zarkovic K. Oxidative stress and regeneration. Free Radic Biol Med. 2022;181:154–165. doi:10.1016/j.freeradbiomed.2022.02.004
22. Feril Jr LB, Yamaguchi K, Ikeda-Dantsuji Y, et al. Low-intensity ultrasound inhibits melanoma cell proliferation in vitro and tumor growth in vivo. J Med Ultrason. 2021;48(4):451–461. doi:10.1007/s10396-021-01131-0
23. Coderre JA, Morris GM. The radiation biology of boron neutron capture therapy. Radiation Research. 1999;151(1):1–18.
24. Boedtkjer E, Pedersen SF. The Acidic Tumor Microenvironment as a Driver of Cancer. Annu Rev Physiol. 2020;82:103–126. doi:10.1146/annurev-physiol-021119-034627
25. Shiba S, Shimo T, Yamanaka M, et al. Increased cell killing effect in neutron capture enhanced proton beam therapy. Sci Rep. 2024;14(1):28484. doi:10.1038/s41598-024-79045-3
26. Takemori M, Nakamura S, Sofue T, et al. Failure modes and effects analysis study for accelerator-based Boron Neutron Capture Therapy. Med Phys. 2023;50(1):424–439. doi:10.1002/mp.16104
27. Martínez-Torró C, Alba-Castellón L, Carrasco-Díaz LM, et al. Lymphocyte infiltration and antitumoral effect promoted by cytotoxic inflammatory proteins formulated as self-assembling, protein-only nanoparticles. Biomed Pharmacother. 2023;164:114976. doi:10.1016/j.biopha.2023.114976
28. Rawls K, Dougherty BV, Papin J. Metabolic Network Reconstructions to Predict Drug Targets and Off-Target Effects. Methods Mol Biol. 2020;2088:315–330. doi:10.1007/978-1-0716-0159-4_14
29. Kumar R, Dkhar DS, Kumari R, et al. Ligand conjugated lipid-based nanocarriers for cancer theranostics. Biotechnol Bioeng. 2022;119(11):3022–3043. doi:10.1002/bit.28205
30. Lawal IO, Abubakar SO, Ndlovu H, Mokoala KMG, More SS, Sathekge MM. Advances in Radioligand Theranostics in Oncology. Mol Diagn Ther. 2024;28(3):265–289. doi:10.1007/s40291-024-00702-4
31. Liu HL, Nan H, Zhao WW, Wan XB, Fan XJ. Phase separation in DNA double-strand break response. Review. Nucleus. 2024;15(1):2296243. doi:10.1080/19491034.2023.2296243
32. Zhang T, Xu D, Yi Y, et al. Chitosan-lactobionic acid-thioctic acid-modified hollow mesoporous silica composite loaded with carborane for boron neutron capture therapy of hepatocellular carcinoma. Mater Design. 2022;223:111196.
33. Zhao YC, Chen SY. Targeting DNA Double-Strand Break (DSB) Repair to Counteract Tumor Radio-resistance. Review. Curr Drug Targets. 2019;20(9):891–902. doi:10.2174/1389450120666190222181857
34. Awan UA, Naeem M, Saeed RF, Mumtaz S, Akhtar N. Smart Nanocarrier-Based Cancer Therapeutics. Cancer Treat Res. 2023;185:207–235. doi:10.1007/978-3-031-27156-4_11
35. Guo DD, Ji XT, Luo JT. Rational nanocarrier design towards clinical translation of cancer nanotherapy. Review Biomed Mater. 2021;16(3):032005. doi:10.1088/1748-605X/abe35a
36. Rajora MA, Leung C, Chen J, Zheng G. Fabricating and Labeling Microbubbles with Fluorescent and Radioactive Tracers. J Vis Exp. 2025;37(215):e67431. doi:10.3791/67431
37. Frankl J, Rajamohan N, Yang J, Sibley RC. PET/MRI evaluation of hepatobiliary tumors. Q J Nucl Med Mol Imaging. 2024;68(4):259–269. doi:10.23736/s1824-4785.24.03607-0
38. Schwenck J, Sonanini D, Cotton JM, et al. Advances in PET imaging of cancer. Nat Rev Cancer. 2023;23(7):474–490. doi:10.1038/s41568-023-00576-4
39. Li L, Jiang R, Shan B, Lu Y, Zheng C, Li M. Near-infrared II plasmonic porous cubic nanoshells for in vivo noninvasive SERS visualization of sub-millimeter microtumors. Nat Commun. 2022;13(1):5249. doi:10.1038/s41467-022-32975-w
40. Lu YX, Shan BB, Li LH, Jiang RT, Li M. Tumor-Homing Biomimetic Near-Infrared II SERS Probes for Targeted Intraoperative Resection Guidance of Orthotopic Glioblastoma. Nano Lett. 2025;25(6):2325–2333. doi:10.1021/acs.nanolett.4c05622
41. Chen H, Wang J, Feng X, et al. Mitochondria-targeting fluorescent molecules for high efficiency cancer growth inhibition and imaging. Chem Sci. 2019;10(34):7946–7951. doi:10.1039/c9sc01410a
42. Tarbali S, Dadkhah M, Saadati H. Lipophilic fluorescent products as a potential biomarker of oxidative stress: a link between central (brain) and peripheral (blood). Review. J Res Med Sci. 2024;29(1):38. doi:10.4103/jrms.jrms_671_23
43. Xia Y, Fu BM. Investigation of Endothelial Surface Glycocalyx Components and Ultrastructure by Single Molecule Localization Microscopy: stochastic Optical Reconstruction Microscopy (STORM). Yale J Biol Med. 2018;91(3):257–266.
44. Hou WH, Wei YJ. Evaluating the resolution of conventional optical microscopes through point spread function measurement. Review. iScience. 2023;26(10):107976. doi:10.1016/j.isci.2023.107976
45. Tran MT, Oldenbourg R. Point spread function of the polarized light field microscope. J Opt Soc Am A-Opt Image Sci Vis. 2022;39(6):1095–1103. doi:10.1364/josaa.458034
46. Chiu IH, Osawa T, Sumita T, Ninomiya K, Takeda S, Takahashi T. Evaluation of a CdTe semiconductor-based gamma camera for real-time dose dosimetry in boron neutron capture therapy. Med Phys. 2025;52(10):e70062. doi:10.1002/mp.70062
47. Men YZ, Peng SJ, Yang P, et al. Biodegradable Zwitterionic Nanogels with Long Circulation for Antitumor Drug Delivery. ACS Appl Mater Interfaces. 2018;10(28):23509–23521. doi:10.1021/acsami.8b03943
48. Wang YQ, Huang C, Ye PJ, et al. Prolonged blood circulation outperforms active targeting for nanocarriers-mediated enhanced hepatocellular carcinoma therapy in vivo. J Control Release. 2022;347:400–413. doi:10.1016/j.jconrel.2022.05.024
49. Zheng YS, Guo WF, Hu LW, et al. Long Circulating Cancer Cell-Targeted Bionic Nanocarriers Enable Synergistic Combinatorial Therapy in Colon Cancer. ACS Appl Mater Interfaces. 2023;15(19):22843–22853. doi:10.1021/acsami.3c00469
50. Kanai Y. Amino acid transporter LAT1 (SLC7A5) as a molecular target for cancer diagnosis and therapeutics. Review. Pharmacol Ther. 2022;230:107964. doi:10.1016/j.pharmthera.2021.107964
51. D’Souza AA, Shegokar R. Polyethylene glycol (PEG): a versatile polymer for pharmaceutical applications. Review. Expert Opin Drug Deliv. 2016;13(9):1257–1275. doi:10.1080/17425247.2016.1182485
52. Nomoto T, Yao Y, Inoue Y, et al. Fructose-functionalized polymers to enhance therapeutic potential of p-boronophenylalanine for neutron capture therapy. J Control Release. 2021;332:184–193. doi:10.1016/j.jconrel.2021.02.021
53. Lopez-Nieves S, El-Azaz J, Men Y, et al. Two independently evolved natural mutations additively deregulate TyrA enzymes and boost tyrosine production in planta. Plant J. 2022;109(4):844–855. doi:10.1111/tpj.15597
54. Kong ZR, Li Z, Chen JY, et al. Metabolic characteristics of 18F fluoroboronotyrosine (FBY) PET in malignant brain tumors. Nucl Med Biol. 2022;106:80–87. doi:10.1016/j.nucmedbio.2022.01.002
55. Li JY, Shi YX, Zhang ZZ, et al. A Metabolically Stable Boron-Derived Tyrosine Serves as a Theranostic Agent for Positron Emission Tomography Guided Boron Neutron Capture Therapy. Bioconjugate Chem. 2019;30(11):2870–2878. doi:10.1021/acs.bioconjchem.9b00578
56. Desale K, Kuche K, Jain S. Cell-penetrating peptides (CPPs): an overview of applications for improving the potential of nanotherapeutics. Biomater Sci. 2021;9(4):1153–1188. doi:10.1039/d0bm01755h
57. Zorko M, Langel Ü. Cell-Penetrating Peptides. Methods Mol Biol. 2022;2383:3–32. doi:10.1007/978-1-0716-1752-6_1
58. Yadav S, Singh P. Advancement and application of novel cell-penetrating peptide in cancer management. 3 Biotech. 2023;13(7):234. doi:10.1007/s13205-023-03649-1
59. Jang SI, Pan TS, Li Y, et al. Spach Transformer: spatial and Channel-Wise Transformer Based on Local and Global Self-Attentions for PET Image Denoising. IEEE Trans Med Imaging. 2024;43(6):2036–2049. doi:10.1109/tmi.2023.3336237
60. Alavi M, Nokhodchi A. Micro- and nanoformulations of paclitaxel based on micelles, liposomes, cubosomes, and lipid nanoparticles: recent advances and challenges. Drug Discovery Today. 2022;27(2):576–584. doi:10.1016/j.drudis.2021.10.007
61. Gibot L, Demazeau M, Pimienta V, et al. Role of Polymer Micelles in the Delivery of Photodynamic Therapy Agent to Liposomes and Cells. Cancers. 2020;12(2):384. doi:10.3390/cancers12020384
62. Mukhopadhyay D, Sano C, AlSawaftah N, El-Awady R, Husseini GA, Paul V. Ultrasound-Mediated Cancer Therapeutics Delivery using Micelles and Liposomes: a Review. Recent Patents Anti-Cancer Drug Disc. 2021;16(4):498–520. doi:10.2174/1574892816666210706155110
63. Lozada J, Merkens H, Froelich J, et al. Synthesis and Preclinical Evaluation of Dual-Mode Fluorescent (18)F-PET Tracers Targeting PSMA. J Med Chem. 2025;68(15):16645–16665. doi:10.1021/acs.jmedchem.5c01480
64. Nakamura S, Igaki H, Ito M, et al. Characterization of the relationship between neutron production and thermal load on a target material in an accelerator-based boron neutron capture therapy system employing a solid-state Li target. PLoS One. 2019;14(11):e0225587. doi:10.1371/journal.pone.0225587
65. Kleynhans J, Sathekge M, Ebenhan T. Obstacles and Recommendations for Clinical Translation of Nanoparticle System-Based Targeted Alpha-Particle Therapy. Materials. 2021;14(17):4784. doi:10.3390/ma14174784
66. Silva WM, Ribeiro H, Taha-Tijerina JJ. Potential Production of Theranostic Boron Nitride Nanotubes (64Cu-BNNTs) Radiolabeled by Neutron Capture. Nanomaterials. 2021;11(11):2907. doi:10.3390/nano11112907
67. Li J, Peng K, Li YM, et al. Exosome-Mimetic Supramolecular Vesicles with Reversible and Controllable Fusion and Fission. Angew Chem Int Edit. 2020;59(48):21510–21514. doi:10.1002/anie.202010257
68. Nicolini A, Ferrari P. Involvement of tumor immune microenvironment metabolic reprogramming in colorectal cancer progression, immune escape, and response to immunotherapy. Review Front Immunol. 2024;15:1353787. doi:10.3389/fimmu.2024.1353787
69. Rayamajhi S, Nguyen TDT, Marasini R, Aryal S. Macrophage-derived exosome-mimetic hybrid vesicles for tumor targeted drug delivery. Acta Biomater. 2019;94:482–494. doi:10.1016/j.actbio.2019.05.054
70. Dai XM, Lu LS, Deng SK, et al. USP7 targeting modulates anti-tumor immune response by reprogramming Tumor-associated Macrophages in Lung Cancer. Theranostics. 2020;10(20):9332–9347. doi:10.7150/thno.47137
71. Mellman I, Chen DS, Powles T, Turley SJ. The cancer-immunity cycle: indication, genotype, and immunotype. Review. Immunity. 2023;56(10):2188–2205. doi:10.1016/j.immuni.2023.09.011
72. Troendle EP, Khan A, Searson PC, Ulmschneider MB. Predicting drug delivery efficiency into tumor tissues through molecular simulation of transport in complex vascular networks. J Control Release. 2018;292:221–234. doi:10.1016/j.jconrel.2018.11.010
73. Benne N, ter Braake D, Stoppelenburg AJ, Broere F. Nanoparticles for Inducing Antigen-Specific T Cell Tolerance in Autoimmune Diseases. Review. Front Immunol. 2022;13:864403. doi:10.3389/fimmu.2022.864403
74. Mosch R, Guchelaar HJ. Immunogenicity of Monoclonal Antibodies and the Potential Use of HLA Haplotypes to Predict Vulnerable Patients. Review. Front Immunol. 2022;13:885672. doi:10.3389/fimmu.2022.885672
75. Lai YH, Su CY, Cheng HW, et al. Stem cell-nanomedicine system as a theranostic bio-gadolinium agent for targeted neutron capture cancer therapy. Nat Commun. 2023;14(1):285. doi:10.1038/s41467-023-35935-0
76. Fang H, Zheng L, Tian J, et al. Multimodal Mass Spectrometry Imaging with a Metal-Based Alignment Tool Enables Targeted Single-Cell Boronophenylalanine Uptake and Metabolic Profiling in Glioblastoma Tumors. Anal Chem. 2025;97(49):27122–27132. doi:10.1021/acs.analchem.5c04402
77. Morgan RJ, Synold T, Mamelak A, et al. Plasma and cerebrospinal fluid pharmacokinetics of topotecan in a phase I trial of topotecan, tamoxifen, and carboplatin, in the treatment of recurrent or refractory brain or spinal cord tumors. Cancer Chemother Pharmacol. 2010;66(5):927–933. doi:10.1007/s00280-010-1242-z
78. Zhang L, Li WB, Chen XH, et al. Morusin inhibits breast cancer-induced osteolysis by decreasing phosphatidylinositol 3-kinase (PI3K)-mTOR signalling. Chem Biol Interact. 2024;394:110968. doi:10.1016/j.cbi.2024.110968
79. Igaki H, Murakami N, Nakamura S, et al. Scalp angiosarcoma treated with linear accelerator-based boron neutron capture therapy: a report of two patients. Clin Transl Radiat Oncol. 2022;33:128–133. doi:10.1016/j.ctro.2022.02.006
80. Zhang S, Wei Y, Gu W, et al. Uptakes of boronophenylalanine in the in vitro and in situ glioblastoma and the potential efficacy of boron neutron capture therapy. IBRO Neurosci Rep. 2025;19:192–197. doi:10.1016/j.ibneur.2025.06.014
81. Xiang J, Ma L, Tong JF, et al. Boron-peptide conjugates with angiopep-2 for boron neutron capture therapy. Front Med. 2023;10:1199881. doi:10.3389/fmed.2023.1199881
82. Kageji T, Nagahiro S, Mizobuchi Y, Matsuzaki K, Nakagawa Y, Kumada H. Boron neutron capture therapy (BNCT) for newly-diagnosed glioblastoma: comparison of clinical results obtained with BNCT and conventional treatment. J Med Invest. 2014;61(3–4):254–263. doi:10.2152/jmi.61.254
83. Watanabe T, Sanada Y, Hattori Y, Suzuki M. Correlation between the expression of LAT1 in cancer cells and the potential efficacy of boron neutron capture therapy. J Radiat Res. 2023;64(1):91–98. doi:10.1093/jrr/rrac077
84. Yoshimura K, Kawabata S, Kashiwagi H, et al. Efficacy of Boron Neutron Capture Therapy in Primary Central Nervous System Lymphoma: in Vitro and In Vivo Evaluation. Cells. 2021;10(12):3398. doi:10.3390/cells10123398
85. Zhang ZZ, Chong YZ, Liu YH, et al. A Review of Planned, Ongoing Clinical Studies and Recent Development of BNCT in Mainland of China. Review. Cancers. 2023;15(16):4060. doi:10.3390/cancers15164060
86. Dai CX, Cai F, Hwang KC, et al. Folate receptor-mediated boron-10 containing carbon nanoparticles as potential delivery vehicles for boron neutron capture therapy of nonfunctional pituitary adenomas. Sci China-Life Sci. 2013;56(2):163–173. doi:10.1007/s11427-012-4433-5
87. Igawa K, Izumi K, Sakurai Y. Development of the Follow-Up Human 3D Oral Cancer Model in Cancer Treatment. BioTech. 2023;12(2):35. doi:10.3390/biotech12020035
88. Koivunoro H, Kankaanranta L, Seppälä T, Haapaniemi A, Mäkitie A, Joensuu H. Boron neutron capture therapy for locally recurrent head and neck squamous cell carcinoma: an analysis of dose response and survival. Radiother Oncol. 2019;137:153–158. doi:10.1016/j.radonc.2019.04.033
89. Hirose K, Konno A, Hiratsuka J, et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan (10B) for recurrent or locally advanced head and neck cancer (JHN002): an open-label phase II trial. Radiother Oncol. 2021;155:182–187. doi:10.1016/j.radonc.2020.11.001
90. Cruz GAS, González SJ, Bertotti J, Marín J. First application of dynamic infrared imaging in boron neutron capture therapy for cutaneous malignant melanoma. Med Phys. 2009;36(10):4519–4529. doi:10.1118/1.3218760
91. Fujimoto T, Suzuki M, Kuratsu S, et al. BNCT for primary synovial sarcoma. Appl Radiat Isot. 2021;169:109407. doi:10.1016/j.apradiso.2020.109407
92. Fukuda H, Hiratsuka J, Kobayashi T, et al. Boron neutron capture therapy (BNCT) for malignant melanoma with special reference to absorbed doses to the normal skin and tumor. Australas Phys Eng Sci Med. 2003;26(3):97–103. doi:10.1007/bf03178777
93. Andoh T, Fujimoto T, Satani R, et al. Preclinical study of boron neutron capture therapy for bone metastasis using human breast cancer cell lines. Article; Proceedings Paper. Appl Radiat Isot. 2020;165(6):1009257. doi:10.1016/j.apradiso.2020.109257
94. Kuthala N, Shanmugam M, Yao CL, Chiang CS, Hwang KC. One step synthesis of 10B-enriched 10BPO4 nanoparticles for effective boron neutron capture therapeutic treatment of recurrent head-and-neck tumor. Biomaterials. 2022;290:121861. doi:10.1016/j.biomaterials.2022.121861
95. Singh A, Kim BK, Mackeyev Y, et al. Boron-Nanoparticle-Loaded Folic-Acid-Functionalized Liposomes to Achieve Optimum Boron Concentration for Boron Neutron Capture Therapy of Cancer. J Biomed Nanotechnol. 2019;15(8):1714–1723. doi:10.1166/jbn.2019.2800
96. Kawai K, Nishimura K, Okada S, et al. Cyclic RGD-Functionalized closo-Dodecaborate Albumin Conjugates as Integrin Targeting Boron Carriers for Neutron Capture Therapy. Mol Pharm. 2020;17(10):3740–3747. doi:10.1021/acs.molpharmaceut.0c00478
97. Tsujino K, Kashiwagi H, Nishimura K, et al. Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model. Biology-Basel. 2023;12(3):377. doi:10.3390/biology12030377
98. Chen J, Ji P, Gnawali G, et al. Building bioorthogonal click-release capable artificial receptors on cancer cell surface for imaging, drug targeting and delivery. Acta Pharm Sin B. 2023;13(6):2736–2746. doi:10.1016/j.apsb.2022.12.018
99. Rondon A, Degoul F. Antibody Pretargeting Based on Bioorthogonal Click Chemistry for Cancer Imaging and Targeted Radionuclide Therapy. Review Bioconjugate Chem. 2020;31(2):159–173. doi:10.1021/acs.bioconjchem.9b00761
100. Patra M, Zarschler K, Pietzsch H-J, Stephan H, Gasser G. New insights into the pretargeting approach to image and treat tumours. Review. Chem Soc Rev. 2016;45(23):6415–6431. doi:10.1039/c5cs00784d
101. Cheal SM, Chung SK, Vaughn BA, Cheung N-KV, Larson SM. Pretargeting: a Path Forward for Radioimmunotherapy. J Nucl Med. 2022;63(9):1302–1315. doi:10.2967/jnumed.121.262186
102. Staudt M, Hvass L, Müller M, et al. Development of Polar BODIPY-Tetrazines for Rapid Pretargeted Fluorescence Imaging. ACS Omega. 2024;9(41):42498–42505. doi:10.1021/acsomega.4c06570
103. Nittka S, Krueger MA, Shively JE, et al. Radioimmunoimaging of Liver Metastases with PET Using a 64Cu-Labeled CEA Antibody in Transgenic Mice. PLoS One. 2014;9(9):e106921. doi:10.1371/journal.pone.0106921
104. Meyer J-P, Houghton JL, Kozlowski P, et al. 18 F-Based Pretargeted PET Imaging Based on Bioorthogonal Diels–Alder Click Chemistry. Bioconjugate Chem. 2016;27(2):298–301. doi:10.1021/acs.bioconjchem.5b00504
105. Takayama Y, Kusamori K, Nishikawa M. Click Chemistry as a Tool for Cell Engineering and Drug Delivery. Molecules. 2019;24(1):172. doi:10.3390/molecules24010172
106. Matsumoto Y, Fukumitsu N, Ishikawa H, Nakai K, Sakurai H. A Critical Review of Radiation Therapy: from Particle Beam Therapy (Proton, Carbon, and BNCT) to Beyond. Review. J Pers Med. 2021;11(8):825. doi:10.3390/jpm11080825
107. Hapuarachchige S, Si G, Huang CT, et al. Dual-Modality PET-SPECT Image-Guided Pretargeting Delivery in HER2(+) Breast Cancer Models. Biomacromolecules. 2021;22(11):4606–4617. doi:10.1021/acs.biomac.1c00918
108. Nejati K, Dadashpour M, Gharibi T, Mellatyar H, Akbarzadeh A. Biomedical Applications of Functionalized Gold Nanoparticles: a Review. Review J Clust Sci. 2022;33(1):1–16. doi:10.1007/s10876-020-01955-9
109. Lesnikowski ZJ, Ekholm F, Hosmane NS, et al. Early Stage In Vitro Bioprofiling of Potential Low-Molecular-Weight Organoboron Compounds for Boron Neutron Capture Therapy (BNCT)-Proposal for a Guide. Cells. 2024;13(10):798. doi:10.3390/cells13100798
110. Wellum GR, Zamenhof RG, Tolpin EI. Boron neutron capture radiation therapy of cerebral gliomas: an analysis of the possible use of boron-loaded tumor-specific antibodies for the selective concentration of boron in gliomas. Int J Radiat Oncol Biol Phys. 1982;8(8):1339–1345. doi:10.1016/0360-3016(82)90584-3
111. Klepac D, Kostková H, Petrova S, et al. Interaction of spin-labeled HPMA-based nanoparticles with human blood plasma proteins - the introduction of protein-Corona-free polymer nanomedicine. Nanoscale. 2018;10(13):6194–6204. doi:10.1039/c7nr09355a
112. Zhang Y, Liu AT, Cornejo YR, Van Haute D, Berlin JM. A Systematic comparison of in vitro cell uptake and in vivo biodistribution for three classes of gold nanoparticles with saturated PEG coatings. PLoS One. 2020;15(7):e0234916. doi:10.1371/journal.pone.0234916
113. Wang J, Bai R, Yang R, et al. Size- and surface chemistry-dependent pharmacokinetics and tumor accumulation of engineered gold nanoparticles after intravenous administration. Metallomics. 2015;7(3):516–524. doi:10.1039/c4mt00340c
114. Qiu L, Lin QY, Si Z, et al. A Pretargeted Imaging Strategy for EGFR-Positive Colorectal CarcinomaviaModulation of Tz-Radioligand Pharmacokinetics. Mol Imaging Biol. 2021;23(1):38–51. doi:10.1007/s11307-020-01539-z
115. Rondon A, Ty N, Bequignat JB, et al. Antibody PEGylation in bioorthogonal pretargeting with trans-cyclooctene/tetrazine cycloaddition: in vitro and in vivo evaluation in colorectal cancer models. Sci Rep. 2017;7:14918. doi:10.1038/s41598-017-15051-y
116. Wang J, Tian Y, Duan X, et al. Synthesis, radiolabeling and biodistribution studies of [99mTc(CO)3(MN-TZ-BPA)]+ in tumor-bearing mice. J Radioanal Nucl Chem. 2012;292(1):177–181. doi:10.1007/s10967-011-1396-0
117. Handula M, Chen KT, Seimbille Y. IEDDA: an Attractive Bioorthogonal Reaction for Biomedical Applications. Molecules. 2021;26(15):4640. doi:10.3390/molecules26154640
118. Liu G, Hnatowich DJ. A semiempirical model of tumor pretargeting. Bioconjug Chem. 2008;19(11):2095–2104. doi:10.1021/bc8002748
119. Nakamura H. Liposomal boron delivery system for neutron capture therapy. Yakugaku zasshi. 2008;128(2):193–208. doi:10.1248/yakushi.128.193
120. Huang W, Yang Y, Pan Y, Jing S, Qi Y, Huang Y. Enhanced boron neutron capture therapy (BNCT) through controlled drug release via boron-loaded nanofiber mats. Nano Res. 2024;17(8):7479–7492. doi:10.1007/s12274-024-6721-3
121. Ding S, Khan AI, Cai X, et al. Overcoming blood-brain barrier transport: advances in nanoparticle-based drug delivery strategies. Mater Today. 2020;37:112–125. doi:10.1016/j.mattod.2020.02.001
122. Shen X, Pan D, Gong Q, Gu Z, Luo K. Enhancing drug penetration in solid tumors via nanomedicine: evaluation models, strategies and perspectives. Bioact Mater. 2024;32:445–472. doi:10.1016/j.bioactmat.2023.10.017
123. Nance E, Pun SH, Saigal R, Sellers DL. Drug delivery to the central nervous system. Nat Rev Mater. 2022;7(4):314–331. doi:10.1038/s41578-021-00394-w
124. Yi X, Jin X, Hu Y, et al. Drug Delivery Systems for Overcoming Physical Barriers in Cancer Therapy. Mol Pharm. 2025;22(11):6413–6429. doi:10.1021/acs.molpharmaceut.5c00474
125. Kusaka S, Voulgaris N, Onishi K, et al. Therapeutic Effect of Boron Neutron Capture Therapy on Boronophenylalanine Administration via Cerebrospinal Fluid Circulation in Glioma Rat Models. Cells. 2024;13(19):1610.
126. Matsubayashi N, Hu N, Takata T, et al. Characterization of acrylic phantom for use in quality assurance of BNCT beam output procedure. J Radiat Res. 2024;66(1):10–15. doi:10.1093/jrr/rrae089
127. He H, Li J, Jiang P, et al. The basis and advances in clinical application of boron neutron capture therapy. Radiat Oncol. 2021;16(1):216. doi:10.1186/s13014-021-01939-7
128. Tanaka H, Sakurai Y, Suzuki M, et al. Improvement of dose distribution in phantom by using epithermal neutron source based on the Be(p,n) reaction using a 30 MeV proton cyclotron accelerator. Appl Radiat Isot. 2009;67(7–8):S258–S261. doi:10.1016/j.apradiso.2009.03.096
129. Kawabata S, Goto H, Narita Y, et al. Extended follow-up of recurrent glioblastoma patients treated with boron neutron capture therapy (BNCT): long-term survival from a Phase II trial (JG002) using Cyclotron Neutron Source and Boronophenylalanine. Appl Radiat Isot. 2025;226:112118. doi:10.1016/j.apradiso.2025.112118
130. Seneviratne DS, Saifi O, Mackeyev Y, Malouff T, Krishnan S. Next-Generation Boron Drugs and Rational Translational Studies Driving the Revival of BNCT. Review. Cells. 2023;12(10):1398. doi:10.3390/cells12101398
131. Zhou P, Li XJ, Zhou H, et al. Support Vector Machine Model Predicts Dose for Organs at Risk in High-Dose Rate Brachytherapy of Cervical Cancer. Front Oncol. 2021;11:619384. doi:10.3389/fonc.2021.619384
132. Hu CR, Lai YQ, Cao Y, et al. MRI and 18F-BPA PET-guided targeting in boron neutron capture therapy. Sci Rep. 2025;15(1):31285. doi:10.1038/s41598-025-14642-4
133. Carré A, Battistella E, Niyoteka S, Sun R, Deutsch E, Robert C. AutoComBat: a generic method for harmonizing MRI-based radiomic features. Sci Rep. 2022;12(1):12762. doi:10.1038/s41598-022-16609-1
134. Zhu X, Luo WZ, Zhang DH, Liu RH. An Assay for Immunogenic Detection of Anti-PEG Antibody. ChemBioChem. 2024;25(16):7. doi:10.1002/cbic.202400316
135. Chang CA, Emberley E, D’Souza AL, et al. ABBV-319: a CD19-targeting glucocorticoid receptor modulator antibody-drug conjugate therapy for B-cell. Blood. 2024;144(7):757–770. doi:10.1182/blood.2024023849
136. Reshetnikov VV, Chirinskaite AV, Sopova JV, Ivanov RA, Leonova EI. Cas-Based Systems for RNA Editing in Gene Therapy of Monogenic Diseases: in Vitro and in Vivo Application and Translational Potential. Review. Front Cell Dev Biol. 2022;10:903812. doi:10.3389/fcell.2022.903812
137. Irais CM, María-de-la-Luz SG, Dealmy DG, et al. Plant Phenolics as Pathogen-Carrier Immunogenicity Modulator Haptens. Review. Curr Pharm Biotechnol. 2020;21(10):897–905. doi:10.2174/1389201021666200121130313
138. Li Y, Chen HQ, Shen QF, et al. Fragment Autoantigens Stimulated T-Cell-Immunotherapy (FAST) as a Fast Autologous Cancer Vaccine. Adv Sci. 2025;12(26):16. doi:10.1002/advs.202502937
139. Gogtay M, Aimalla N, Thirugnanasambandam RP, Ganti AK. Therapeutic Potential of Datopotamab Deruxtecan in the Treatment of Advanced Non-Small Cell Lung Cancer: evidence to Date. Onco Targets Ther. 2025;18:575–584. doi:10.2147/ott.S466220
140. Hait SH, Hogge CJ, Rahman MA, et al. TFH Cells Induced by Vaccination and Following SIV Challenge Support Env-Specific Humoral Immunity in the Rectal-Genital Tract and Circulation of Female Rhesus Macaques. Front Immunol. 2021;11:608003. doi:10.3389/fimmu.2020.608003
141. Yi M, Li Y, Jie H, Deng S. Nanotechnology-Driven Drug Delivery Systems for Lung Cancer: computational Advances and Clinical Perspectives. Thorac Cancer. 2025;16(14):e70134. doi:10.1111/1759-7714.70134
142. Tang L, Xiao Q, Mei Y, et al. Insights on functionalized carbon nanotubes for cancer theranostics. J Nanobiotechnol. 2021;19(1):423. doi:10.1186/s12951-021-01174-y
143. Gao Y, Liu J, Wu M, et al. Photosensitive Hybrid γδ-T Exosomes for Targeted Cancer Photoimmunotherapy. ACS Nano. 2025;19(4):4251–4268. doi:10.1021/acsnano.4c11024
144. Mahmud MM, Pandey N, Winkles JA, Woodworth GF, Kim AJ. Toward the scale-up production of polymeric nanotherapeutics for cancer clinical trials. Nano Today. 2024;56:102314. doi:10.1016/j.nantod.2024.102314
145. Sorrentino C, Ciummo SL, Fieni C, Di Carlo E. Nanomedicine for cancer patient-centered care. MedComm. 2024;5(11):e767. doi:10.1002/mco2.767
146. Dai L, Liu J, Yang T, et al. Lipoic acid-boronophenylalanine-derived multifunctional vesicles for cancer chemoradiotherapy. Nat Commun. 2025;16(1):1329. doi:10.1038/s41467-025-56507-4
147. Lv L, Zhang J, Wang Y, et al. Boron Neutron Capture Therapy-Derived Extracellular Vesicles via DNA Accumulation Boost Antitumor Dendritic Cell Vaccine Efficacy. Adv Sci. 2024;11(35):e2405158. doi:10.1002/advs.202405158
148. Deng S, Hu L, Chen G, et al. A PD-L1 siRNA-Loaded Boron Nanoparticle for Targeted Cancer Radiotherapy and Immunotherapy. Adv Mater. 2025;37(13):e2419418. doi:10.1002/adma.202419418
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.