Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
TACE Combined with Targeted Immunotherapy: A Strategy for Liver Transplantation Conversion and Survival Benefits in Patients with BCLC Stage B/C HCC
Authors Zhang H, Zhang X, Zhang L ![]() , Wang S, Ma Y
, Wang S, Ma Y
Received 6 January 2026
Accepted for publication 28 April 2026
Published 20 May 2026 Volume 2026:13 588533
DOI https://doi.org/10.2147/JHC.S588533
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Hanyuan Zhang,1– 4,* Xuzhi Zhang,1– 4,* Long Zhang,1– 4,* Shuai Wang,2– 4 Yi Ma2– 4
1Sun Yat-Sen University Zhongshan School of Medicine, Guangzhou, People’s Republic of China; 2Organ Transplant Center, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 3Guangdong Provincial Key Laboratory of Organ Donation and Transplant Immunology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 4Guangdong Provincial International Cooperation Base of Science and Technology (Organ Transplantation), The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors have contributed equally to this work
Correspondence: Yi Ma, Email [email protected]
Background: Patients with BCLC stage B or C hepatocellular carcinoma (HCC) often face long waiting times. The effectiveness of different tumor control strategies remains unclear. This study evaluates preoperative conversion therapies for liver transplantation (LT).
Methods: This study retrospectively analyzed 269 patients with HCC at BCLC stage B or C from a single center from January 2015 to August 2024. All these patients underwent liver transplantation. They were divided into three groups by treatment: transcatheter arterial chemoembolization (TACE) (n = 150), TACE + tyrosine kinase inhibitor (TKI) (n = 74), and TACE + TKI+immune checkpoint inhibitors (ICI) (n = 45). Preoperative assessments included blood tests, liver and kidney function, coagulation, tumor markers, and imaging to evaluate tumor response and monitor adverse events. Data collected included baseline characteristics, lab results, surgical details, preoperative treatment response, adverse events, 1-year survival, tumor-free survival, and donor information.
Results: Baseline characteristics were well-balanced across the three groups. The TACE + TKI + ICI group showed higher DCR, ORR, and CRR than both the TACE-alone and TACE + TKI groups (all P < 0.05; χ2 = 11.592, 18.111, 17.558). It also had longer RFS versus both control groups (vs. TACE alone: P = 0.008; vs. TACE + TKI: P = 0.040). One-year OS did not differ significantly among groups (P = 0.707). Safety analyses revealed no significant differences in preoperative lab values, adverse event rates, or intraoperative liver transplant parameters (all P > 0.05), confirming prior treatments did not compromise surgical feasibility or safety. Multivariate logistic regression identified treatment regimen as an independent predictor of DCR (P=0.002), ORR (P< 0.001), and CRRP (P< 0.001). Multivariate Cox regression confirmed it as an independent predictor of RFS (P< 0.01). After a 1-month washout, rejection rates did not differ significantly among the three patient groups, and treatment method was not associated with rejection risk (P=0.549).
Conclusion: In the conversion therapy of HCC, the combination of TACE + TKI + ICI has demonstrated higher efficacy, longer recurrence-free survival, manageable safety, and does not interfere with subsequent LT.
Keywords: liver transplantation, conversion therapy, hepatocellular carcinoma
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide and the third leading cause of cancer-related death.1 Its asymptomatic onset and complex epidemiology—driven by HBV, HCV, and alcoholic cirrhosis—mean high incidence and mortality are expected over the next two decades despite prevention efforts.2 For patients with limited tumor burden who cannot undergo resection, liver transplantation (LT) is optimal, as it removes the tumor and treats underlying liver disease, offering a potential cure.3
LT is a key treatment for HCC.4 The Milan criteria define eligibility as a single tumor ≤5 cm or up to three tumors each ≤3 cm, without macrovascular invasion, lymph node involvement, or extrahepatic metastasis.5 These strict criteria limit access for patients with intermediate- to advanced-stage HCC, especially those at BCLC stage B or C.6 Extended criteria such as UCSF7 and the Hangzhou criteria8 have been proposed but have not significantly improved overall survival or substantially expanded access, leaving progress limited.9 Meanwhile, waiting-list mortality remains high: over 51,000 patients died awaiting LT in the past two decades10 and in China, only 6,170 of 14,399 transplant candidates received transplants in 2019.11 Strict criteria and high waitlist mortality continue to hinder advances in HCC care. However, recent progress shows promise. Pre-transplant downstaging therapies can reduce tumor burden and enable transplantation for select patients beyond standard criteria, achieving survival rates comparable to those within criteria.12. These protocols represent a significant advance in HCC management.
Current downstaging strategies include transcatheter arterial chemoembolization (TACE),13 tyrosine kinase inhibitors (TKIs),14 and immunotherapy.15 Conversion therapies like TACE, radiofrequency ablation, or radiotherapy are linked to 5-year survival rates of 50–60%.16 Lenvatinib, a multi-kinase inhibitor targeting VEGF receptors, improves overall and progression-free survival in unresectable HCC.17 Immune checkpoint inhibitors (ICIs), particularly anti-PD-1/PD-L1 agents, show promise in HCC treatment.18 As their role in systemic therapy grows, more transplant centers are exploring ICIs in LT recipients, though standardized protocols are lacking. ”Conversion therapy” refers to the combined comprehensive treatment of TKI, ICI, and TACE to achieve the effect of alleviating tumor progression before surgery.
For HCC patients beyond Milan criteria, multimodal preoperative therapy aims to downstage tumors and enable successful transplantation. TACE not only targets tumors directly but also modulates the tumor microenvironment and reduces immunosuppression,19 potentially enhancing systemic therapies like ICIs and TKIs.20 However, the combination of ICIs with locoregional treatments such as TACE as a neoadjuvant strategy—and its impact on post-transplant recurrence—remains unclear.21 To our knowledge, no study has yet evaluated how conversion therapy—combining TACE), TKIs, and ICIs—affects post-liver transplantation outcomes in patients with BCLC stage B or C HCC. ICIs are first-line systemic therapy for HCC and effectively control tumor progression. When combined with local therapies like TACE, they achieve >75% downstaging rates, enabling transplantation for patients initially outside transplant criteria. Although the liver is an immune-privileged site and rejection risk is relatively high, most cases respond well to intensified immunosuppression; graft loss or death from rejection remains rare (2–4%).22–24 No study has evaluated the impact of TACE + TKI + ICI conversion therapy on post-transplant outcomes in BCLC B/C HCC patients. At our center, the treatment-to-transplant washout period is 1–3 months. This is the first retrospective study to assess the safety and efficacy of pre-transplant TACE–ICI–TKI combination therapy in BCLC B/C HCC, and to examine its impact on transplantation outcomes and patient survival.
Methods
Ethics
The studies involving human participants were reviewed and approved by the Institutional Review Board of The First Affiliated Hospital of Sun Yat-sen University (Ethical Approval No. 2025-529). Our research complies with the Declaration of Helsinki. All organs were voluntarily donated, the donors signed written informed consent forms, and the organ donation process complies with the provisions of the Declaration of Istanbul. Written informed consent was obtained from all participants prior to their participation in the study. Additionally, written informed consent for the publication of any potentially identifiable images or data included in this article was obtained from the individuals involved.
Patients
A total of 312 patients with BCLC stage B or C HCC who underwent LT at the First Affiliated Hospital of Sun Yat-sen University from January 2015 to August 2024 were collected. Among them, 269 patients received TACE, TACE + TKI, or TACE + TKI + ICI before surgery. Patients who only received TACE treatment were assigned to the TACE group (n = 150), while those who received TACE combined with TKI and PD-1 inhibitor treatment were assigned to the TACE + TKI + ICI group (n = 45). Patients who received TACE combined with TKI treatment were assigned to the TACE + TKI group (n = 74).
The preoperative diagnosis of HCC is established based on the following criteria: 1. If the diameter of the liver mass is ≥2 cm, and one of the two imaging examinations (CT and MRI) shows that the liver mass has the above-mentioned characteristics of liver cancer, HCC can be diagnosed. 2. If the diameter of the liver mass is between 1 and 2 cm, both CT and MRI imaging examinations need to show that the liver mass has the above - mentioned characteristics of liver cancer to diagnose HCC. 3. Serum AFP criteria: Serum AFP ≥ 400 μg/L for 1 month or ≥200 μg/L for 2 months, and other causes of AFP elevation can be excluded. For patients with serum AFP ≥ 400 μg/L but no liver mass found by B – ultrasound, after excluding other causes of AFP elevation, multi-detector CT and/or dynamic contrast-enhanced MRI scans should be performed promptly. If the typical imaging features of HCC are presented, HCC can be diagnosed.4. For patients with chronic HBV infection without cirrhosis or high - risk factors for HCC, the diagnosis of HCC should be confirmed by pathology, because the accuracy of non - invasive imaging diagnostic criteria is insufficient in these patient populations.
The Inclusion Criteria Were as Follows
(1) age ≥18 years; (2) diagnosis of HCC confirmed by histopathological or cytological examination, or based on clinical and imaging features in accordance with the American Association for the Study of Liver Diseases (AASLD) guidelines; (3) HCC classified as stage B or C according to the BCLC staging system; (4) prior treatment with TACE alone, TACE combined with TKIs, or TACE combined with TKIs and ICIs before LT; (5) presence of at least one measurable intrahepatic lesion as defined by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.
Exclusion Criteria Were
(1) patients who received treatments other than TACE, TKI, and ICI before surgery; (2) HCC patients not in BCLC stage B or C; (3) death due to early severe complications after LT; (4) autologous LT, multiple-organ transplantation, or multiple LT; (5) presence of multiple organ dysfunction; (6) poor patient compliance (missing patient records or loss to follow-up).
Preoperative Treatment Plan
Prior to initiating treatment, the patient’s overall health status and liver function are assessed to exclude contraindications for the three available treatment options. Upon confirmation of diagnosis, treatment selection is guided by a multidisciplinary, expert-led clinical decision-making process that considers the patient’s clinical condition, economic burden, and personal preferences. Before making a decision, the doctor will inform the patient and their family of the potential benefits, complications and costs of each treatment option. In this center, we adopt the sequential treatment method. Some studies have shown that sequential treatment has a better effect on the prognosis of HCC. Then, TACE, TACE + TKI, and TACE + TKI + ICI treatments will be adopted. The frequency of TACE treatment is once a month. TACE is performed by puncturing the femoral artery using the Seldinger technique. Digital subtraction angiography is used to determine the blood supply arteries of liver tumors and whether there are arteriovenous fistulas, and then catheterization is carried out to the tumor blood supply branches. Tumor vascular embolization was performed using drug-loaded microspheres or 40 mg of iodized oil containing epirubicin. In patients without signs of deterioration or organ function decline, TACE was repeated “on demand” after follow-up contrast-enhanced CT or MRI confirmed tumor survival. In this study, for patients with hepatitis B, entecavir is routinely used before surgery to control the progression of the disease. After transplantation, tacrolimus and mycophenolate mofetil are routinely used in combination for anti - rejection treatment. For patients with hepatitis B, entecavir is routinely used for antiviral treatment after surgery; for patients with hepatocellular carcinoma, tyrosine kinase inhibitors (TKI) are continued to be used for anti - tumor treatment after surgery.
Both groups of patients orally took Lenvatinib (Lenvima) (initial dose, 8mg/day [<60kg] or 12mg/day [≥60kg]) within 3 days before and after the first TACE treatment. In the TACE + TKI + ICI group, the PD-1 inhibitor (Tislelizumab, initial dose 200mg, 200mg every 3 weeks) was intravenously injected. According to adverse events, the dose of Lenvatinib and PD-1 inhibitor could be halved or temporarily discontinued and then resumed after symptom relief. The treatment continued until the patient’s LT.
All enrolled patients were followed up regularly before surgery, until the day before transplantation. The follow-up included complete blood cell count, liver, kidney, thyroid and heart function tests, tumor marker detection, coagulation function tests, abdominal CT, electrocardiogram and chest X-ray before each immunotherapy. We evaluated tumor changes through regular imaging studies, with computerized tomography (MRI/CT) performed every 4 weeks, and tumor response was assessed according to RECIST v1.1 criteria. This includes complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). CR refers to the tumor of the patient being downstaged, PR indicates a significant reduction in tumor size without reaching downstaging, SD means no significant change in the tumor but the progression is controlled, and PD indicates poor tumor control, with progressive growth and deterioration of the condition. At the same time, the disease control rate (DCR [CRR + PRR + SDR]) and objective response rate (ORR [CRR + PRR]) as well as the complete response rate (CRR) are evaluated.
Clinical Data and Postoperative Follow-Up
Baseline Data of the Recipient Patients
Collect the patients’ basic information, including age, gender, recipient blood type, body mass index (BMI), etiology of liver cancer, history of previous chronic diseases (hypertension, coronary heart disease, diabetes), smoking and drinking history, as well as Child–Pugh score. Tumor - related data include the longest diameter of the tumor, the number of tumors, and tumor vascular invasion.
Donor Data
Analysis of donor age, gender, blood type, BMI, donor donation type, total bilirubin.
Preoperative Laboratory Tests for the Recipient
Preoperative laboratory tests collected include: AFP, preoperative white blood cells, hemoglobin, platelets, ALT, AST, total bilirubin, direct bilirubin, preoperative monocyte percentage, preoperative lymphocyte percentage, preoperative neutrophil percentage, albumin, prealbumin, alkaline phosphatase, GGT, cholinesterase, creatinine, prothrombin time, fibrinogen, INR.
Intraoperative Data of the Patient
Anhepatic phase time, cold ischemia time, total operation time, intraoperative plasma transfusion volume, intraoperative platelet transfusion volume, intraoperative red blood cell transfusion volume, total intraoperative fluid infusion volume, total intraoperative blood loss volume.
Preoperative Treatment Effect and Adverse Reactions
The treatment of the three groups was analyzed respectively, including the rate of ORR, DCR and CRR. The safety of the treatment was compared by contrasting adverse reactions, which included abdominal pain, fever, elevated ALT and AST, fatigue, nausea, vomiting, elevated bilirubin, rash, diarrhea, hypothyroidism, decreased white blood cell count, hand-foot syndrome, decreased appetite, and proteinuria. The grading of adverse events is based on the Clavien–Dindo system. The criterion for successful down - staging is that the tumor meets the criteria for liver transplantation after treatment. Treatment failure means the continued progression of the tumor. There should be no cases of dose reduction here. Discontinuation of the drug is due to successful down-staging.
Postoperative Follow-up
To clarify the long-term treatment effect of patients after surgery, the 1-year survival rate and tumor-free survival time of patients were collected. The calculation of recurrence-free survival (RFS) starts from the date of liver transplantation. The overall survival period refers to the survival time of patients starting from the time after liver transplantation. All patients are monitored according to the standardized follow - up protocol of our center after liver transplantation. Enhanced CT or MRI scans of the chest and abdomen are performed every three months. When a suspicious lesion is detected by imaging examination, contrast-enhanced ultrasound or PET-CT will be used for further confirmation depending on the location and characteristics of the lesion. At the same time, we collected the probabilities of postoperative rejection occurrence in three groups of patients.
Data Analysis
Statistical analysis was conducted using IBM SPSS Statistics 22.0, and graphing was performed with GraphPad Prism 9.0 (GraphPad Software). Categorical data were analyzed using Pearson’s chi-square test, and one-way ANOVA was used for comparisons across multiple groups. Data are presented as mean ± standard deviation. For non-normally distributed data, the Kruskal–Wallis H-test was applied, and results are shown as median (Mdn) and interquartile range (IQR). Binary logistic regression analysis was applied to ORR, CRR, and DCR. Multivariate analysis and Cox proportional - hazards regression were used for RFS and OS to control the interference of confounding factors. Survival curves were generated using the Kaplan–Meier method to assess 1-year overall survival (OS), and statistical significance was defined as p < 0.05.
Results
Baseline Data Characteristics of Patients
The baseline characteristics of the three patient groups were comparable, with no significant differences. Patients were similar in gender, age, blood type, Child-Pugh score, BMI, etiology, comorbidities, and smoking or drinking history. Most patients were male, and blood type O was most common. Hepatitis B virus was the primary cause of HCC, followed by hepatitis C and other causes. All patients had a Child-Pugh score of A or B. (Table 1) Donor characteristics—including age, gender, blood type, BMI, donor type, and total bilirubin—also showed no significant differences across groups. Most donors were male, with blood type O predominant and DBD the most common donor type. Pre-donation total bilirubin levels were not significantly different among the groups (TACE+TKI+ICI vs TACE+TKI vs TACE: 16.65 [11.13–30.08] vs 20.75 [11.90–33.70] vs 18.60 [12.55–25.40], P = 0.241) (Table 2).
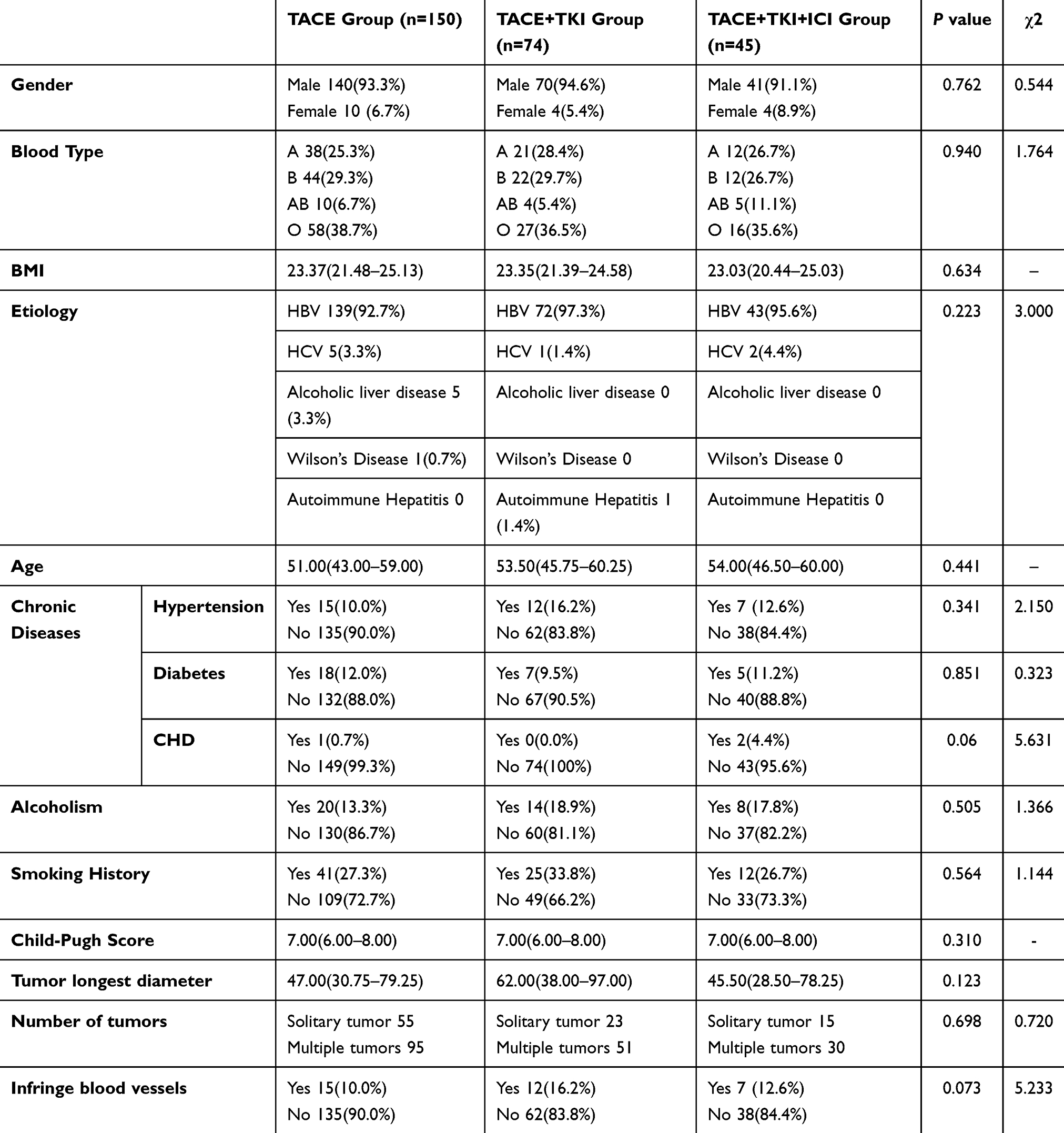 |
Table 1 Receptor Basic Information |
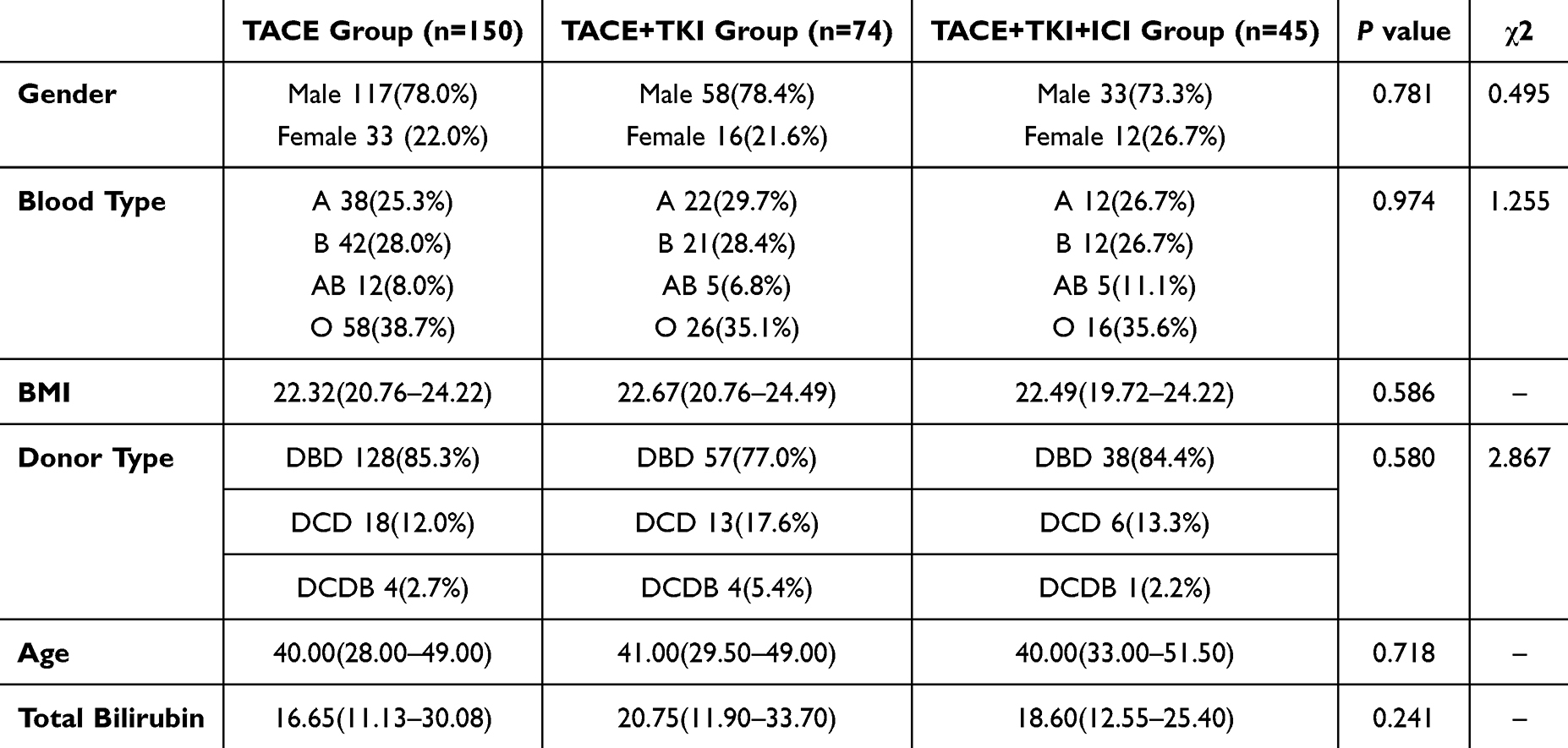 |
Table 2 Donor Clinical Data |
The Effect of Preoperative Treatment for HCC and the Prognosis of Patients After Surgery
TACE+TKI+ICI is an efficient treatment approach for primary liver cancer. After analyzing the tumor control effects of other methods, the tumor control effect of the TKI+TACE+ICI group showed a significant advantage. Compared with the other two groups, the TKI+TACE+ICI group had a DCR (TACE+TKI+ICI vs TACE+TKI vs TACE, 88.9% vs 68.9% vs 62.0%, P=0.003, χ2 =11.592), a higher ORR (TACE+TKI+ICI vs TACE+TKI vs TACE, 62.2% vs 41.9% vs 28.0%, P<0.001, χ2 =18.111), and a higher CRR (TACE+TKI+ICI vs TACE+TKI vs TACE, 28.9% vs 13.5% vs 6.0%, P<0.001, χ2 =17.558) (Table 3). In this study, we followed up on the recurrence-free survival period (RFS) and 1-year overall survival (OS) of the patients. Compared with the other two groups, the TKI+TACE+ICI group had a longer RFS (TACE+TKI+ICI vs TACE+TKI vs TACE, 222.5 (126.3–363.8) vs 257.0 (134.0–401.0) vs 701.5 (374.3–928.8), P=0.011) (Table 3), but there was no significant statistical difference in 1-year OS (TACE+TKI+ICI vs TACE+TKI vs TACE, P=0.707) (Figure 1). Binary logistic analysis shows that after excluding the influence of confounding factors, ORR, CRR, and DCR are only associated with the choice of treatment methods (Tables 4–6). Cox proportional hazards regression analysis, a multi-factor survival analysis, shows that there is no significant difference in the postoperative survival among the three groups of patients. The postoperative RFS results indicate that the postoperative RFS time of patients in the TKI + TACE + ICI group is significantly prolonged (Tables 7 and 8).
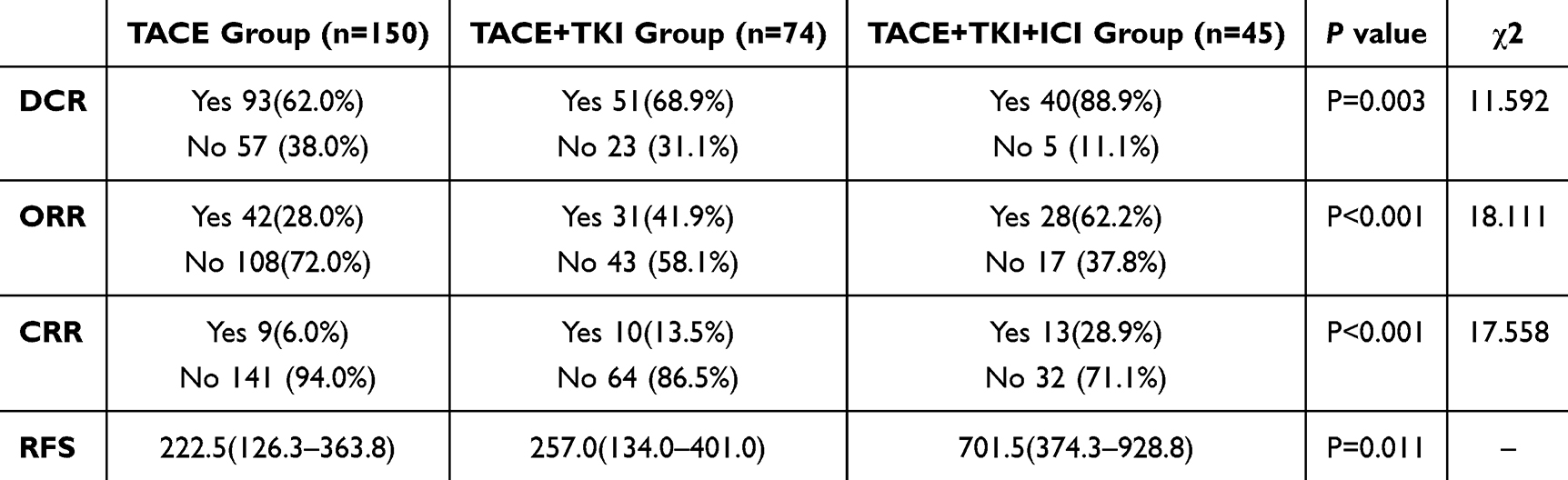 |
Table 3 Preoperative Treatment Effect |
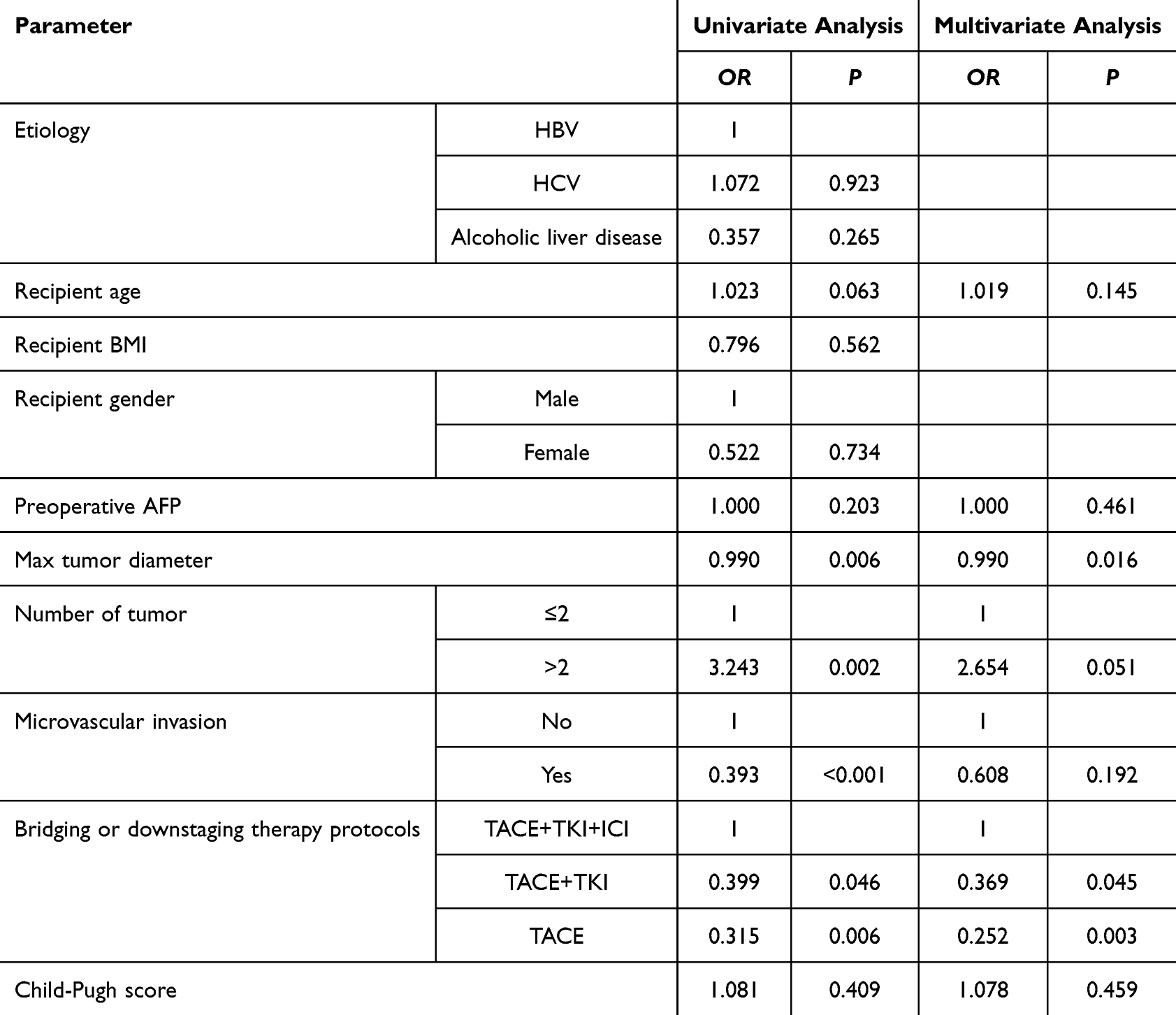 |
Table 4 Factors Associated with DCR in Multivariate Analysis |
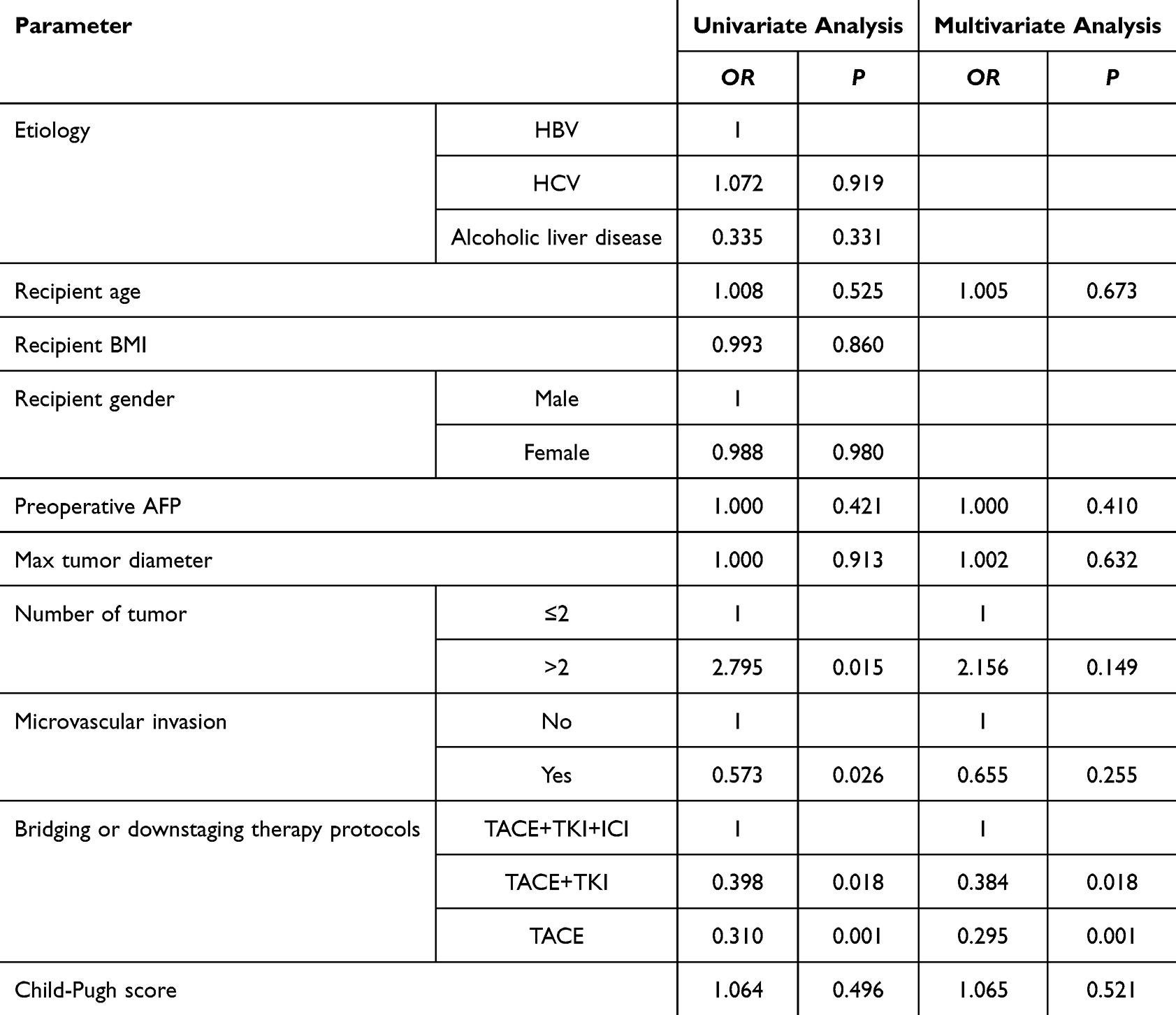 |
Table 5 Factors Associated with ORR in Multivariate Analysis |
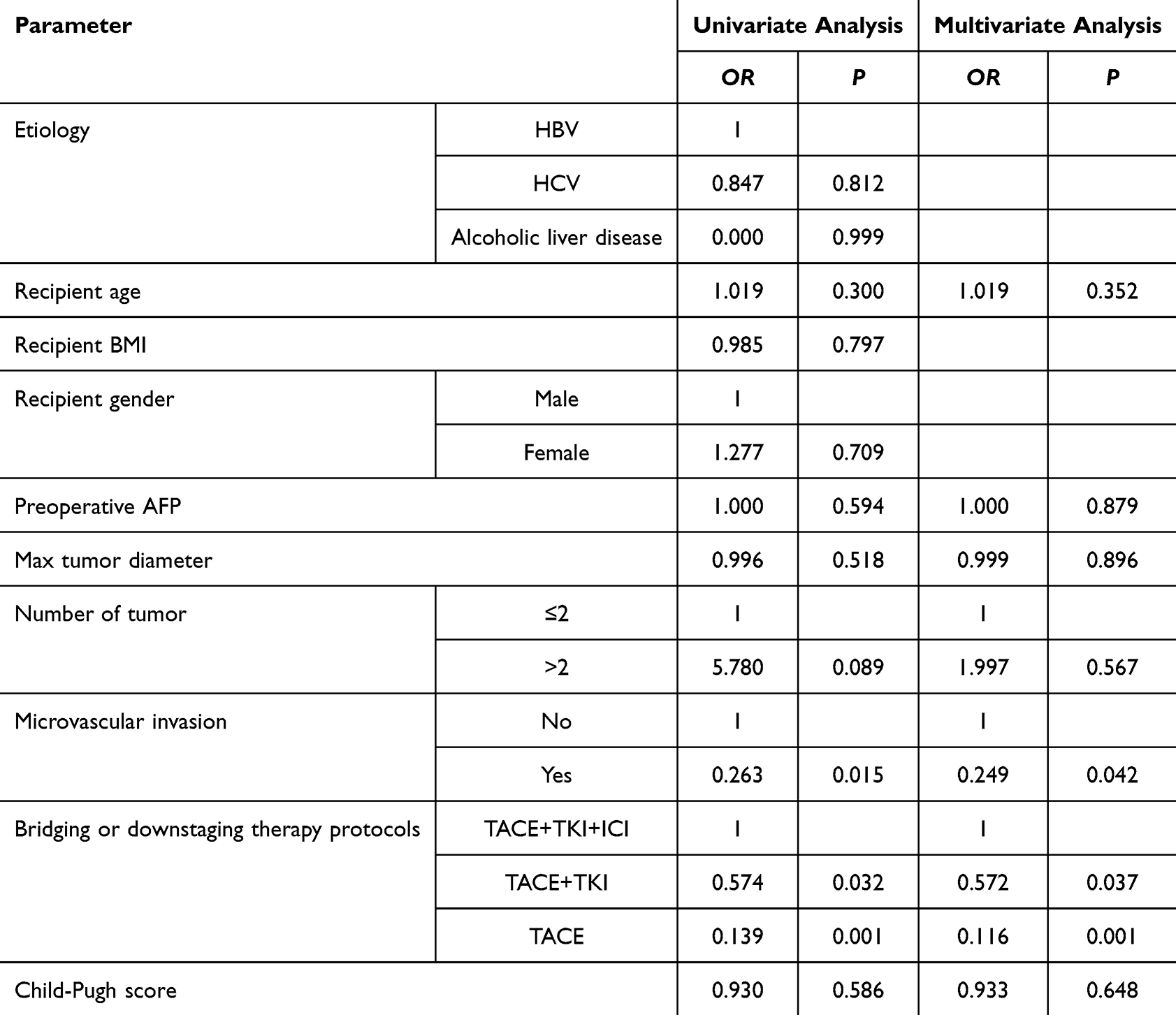 |
Table 6 Factors Associated with CRR in Multivariate Analysis |
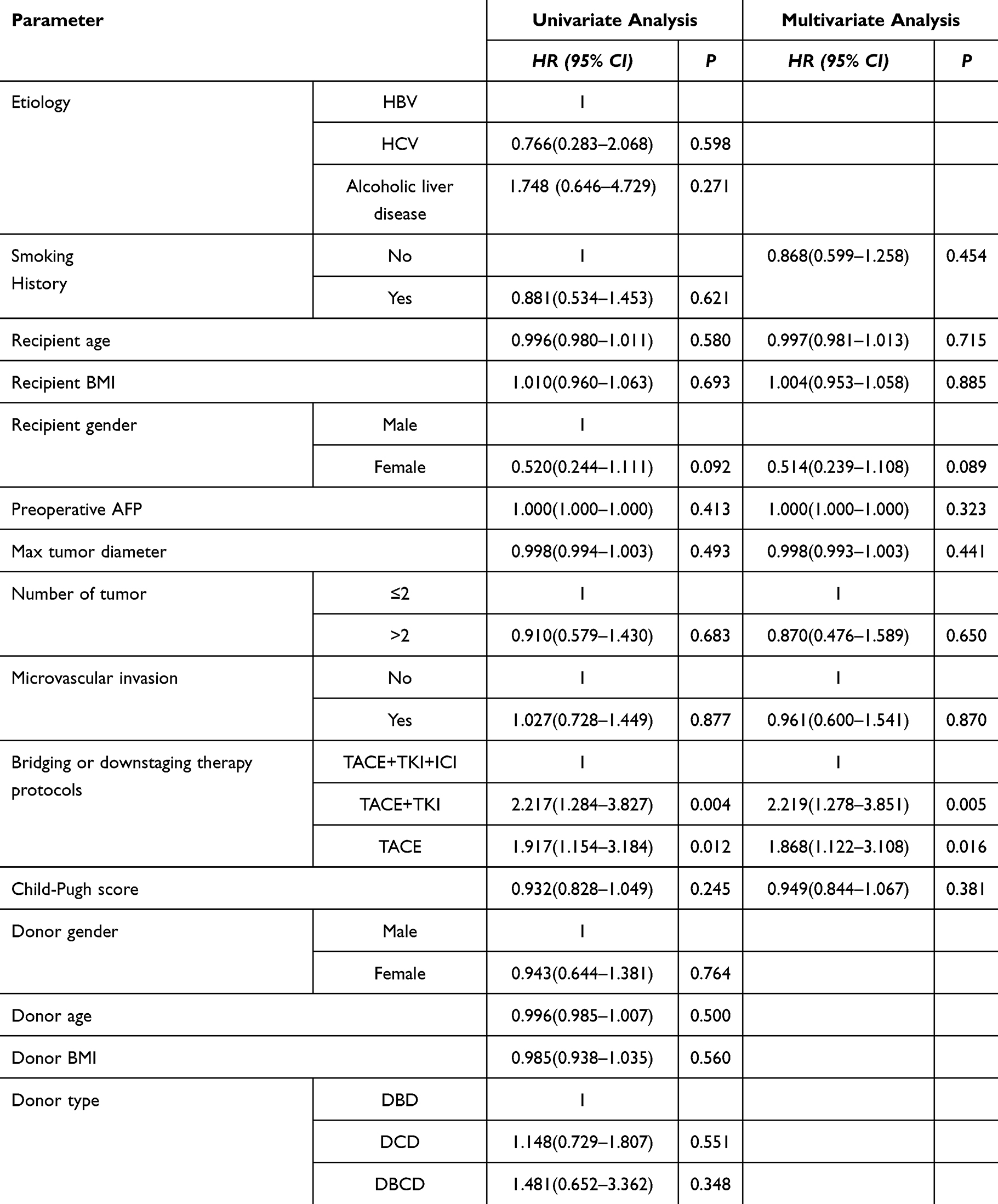 |
Table 7 COX Regression Analysis for the RFS Analysis After Liver Transplantation |
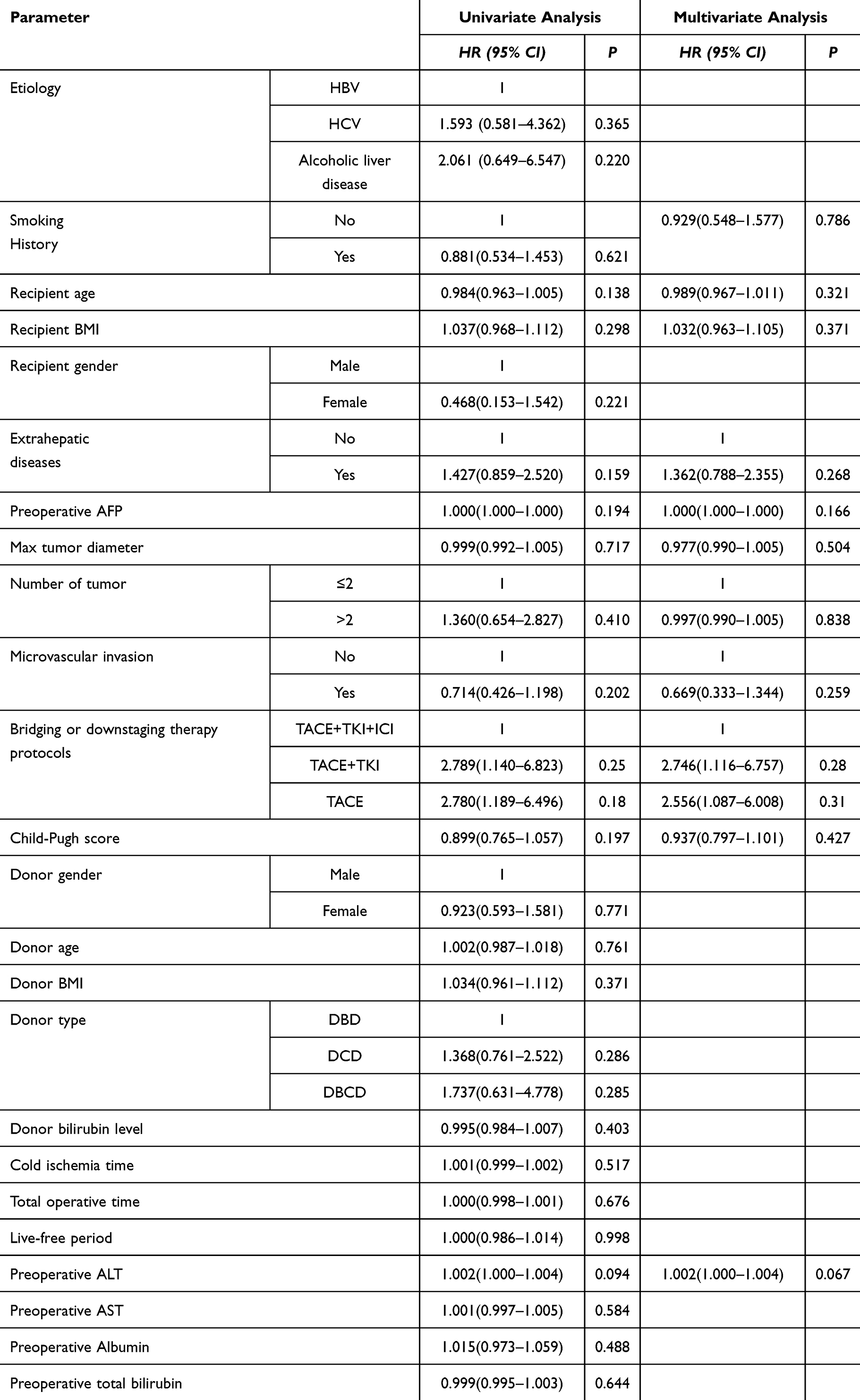 |
Table 8 COX Regression Analysis for the OS Analysis After Liver Transplantation |
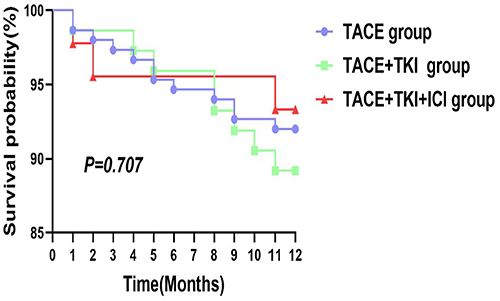 |
Figure 1 Kaplan‑Meier curve illustrating the probability of an event‑free outcome over a 12‑month follow‑up period. The numbers at selected time points indicate the percentage of patients remaining event‑free. The log‑rank test yielded a P‑value of 0.707, indicating no statistically significant difference between the compared groups. |
Analysis of Treatment Safety
Safety of Preoperative Treatment
There were no significant differences among the three groups of patients in the preoperative laboratory test results of AFP, preoperative white blood cells, hemoglobin, platelets, ALT, AST, total bilirubin, direct bilirubin, preoperative monocyte percentage, preoperative lymphocyte percentage, preoperative neutrophil percentage, albumin, prealbumin, alkaline phosphatase, GGT, cholinesterase, creatinine, prothrombin time, fibrinogen, and INR (Table 9). All three groups of patients experienced different adverse events during the treatment process. Hypothyroidism was a unique adverse event during ICI treatment, while hand-foot syndrome, leukopenia, and proteinuria were adverse events during TKI treatment. There were no significant differences among the three groups of patients in terms of abdominal pain, fever, elevated ALT and AST, fatigue, nausea, vomiting, elevated bilirubin, rash, diarrhea, and decreased appetite. This indicates that there were no significant safety differences among the three groups in treatment. Timely management after the occurrence of symptoms would not cause serious adverse reactions to the patients (Table 10). There was no statistically significant difference in the probability of postoperative rejection among the three groups of patients(Table 11).
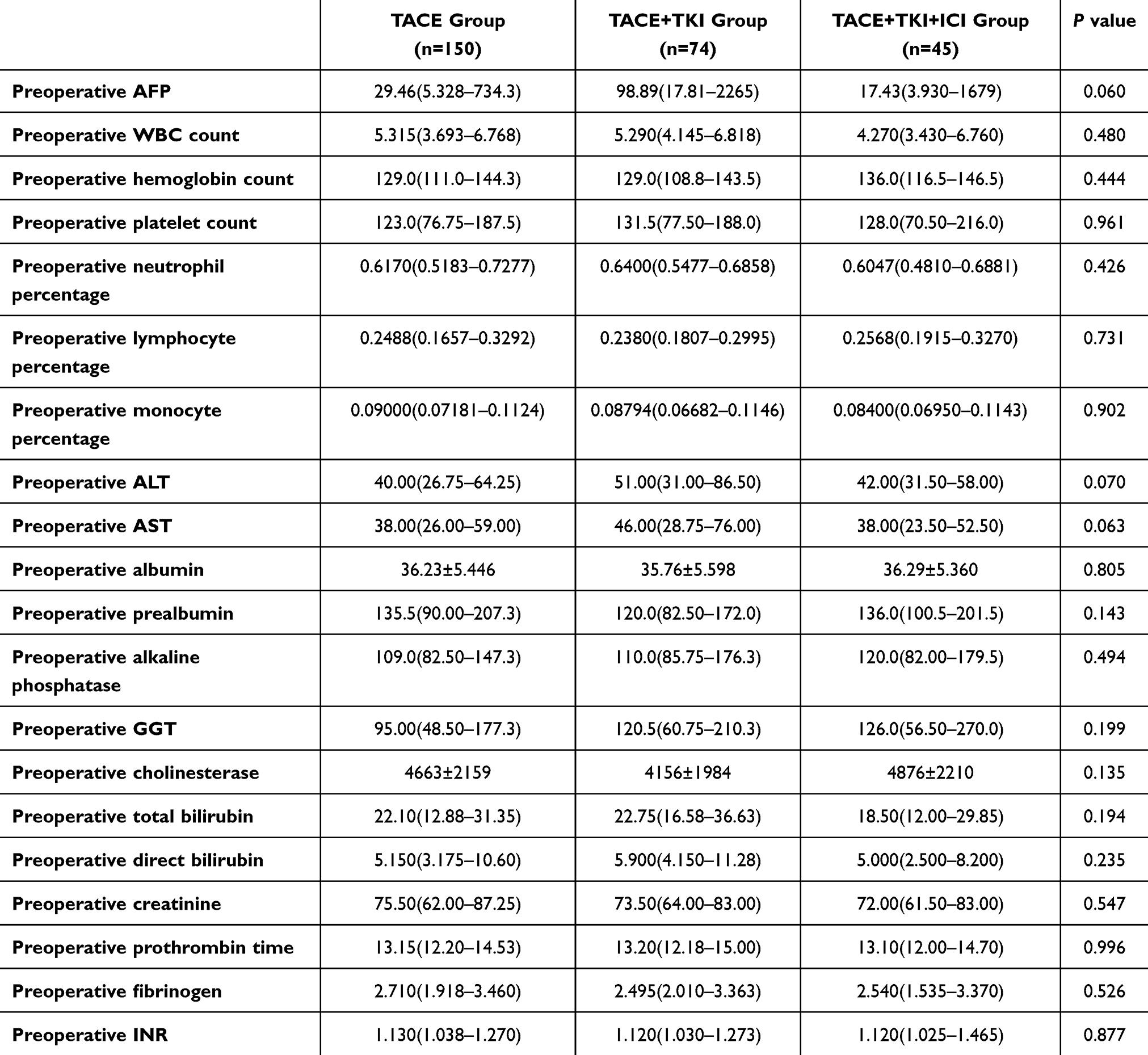 |
Table 9 Preoperative Laboratory Test Results |
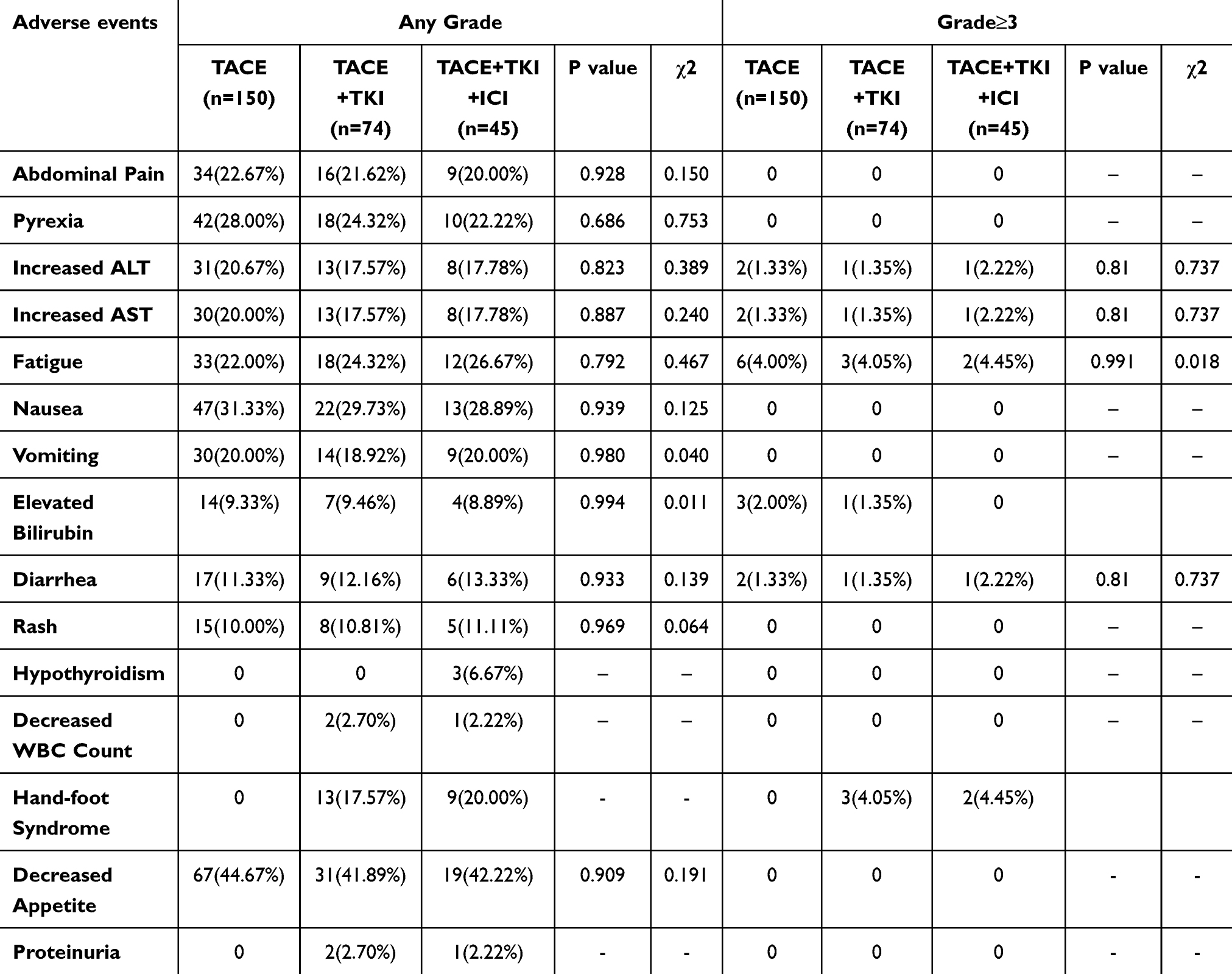 |
Table 10 Adverse Event Assessment |
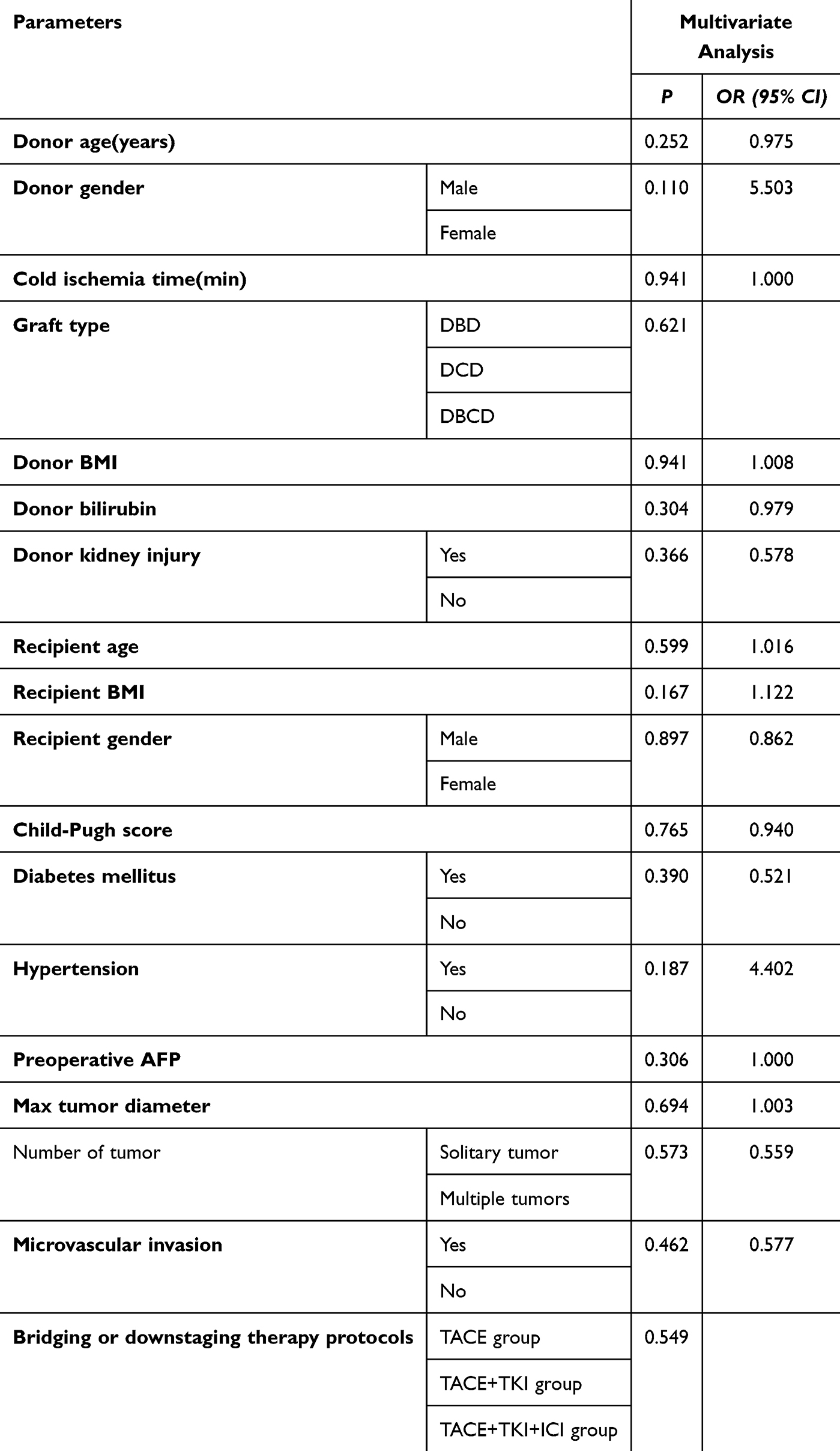 |
Table 11 Factors Associated with Transplant Rejection in Multivariate Analysis |
Safety Analysis of Treatment for Transplantation Surgery
To investigate the impact of preoperative treatment on LT surgery, we analyzed the anhepatic phase time, cold ischemia time, total operation time, intraoperative plasma transfusion volume, intraoperative platelet transfusion volume, intraoperative red blood cell transfusion volume, intraoperative total fluid infusion volume, and intraoperative total blood loss volume. After preoperative treatment, there was no significant difference in the transplantation process among the three groups of patients. This indicates that different treatments have little effect on the surgical process (Table 12).
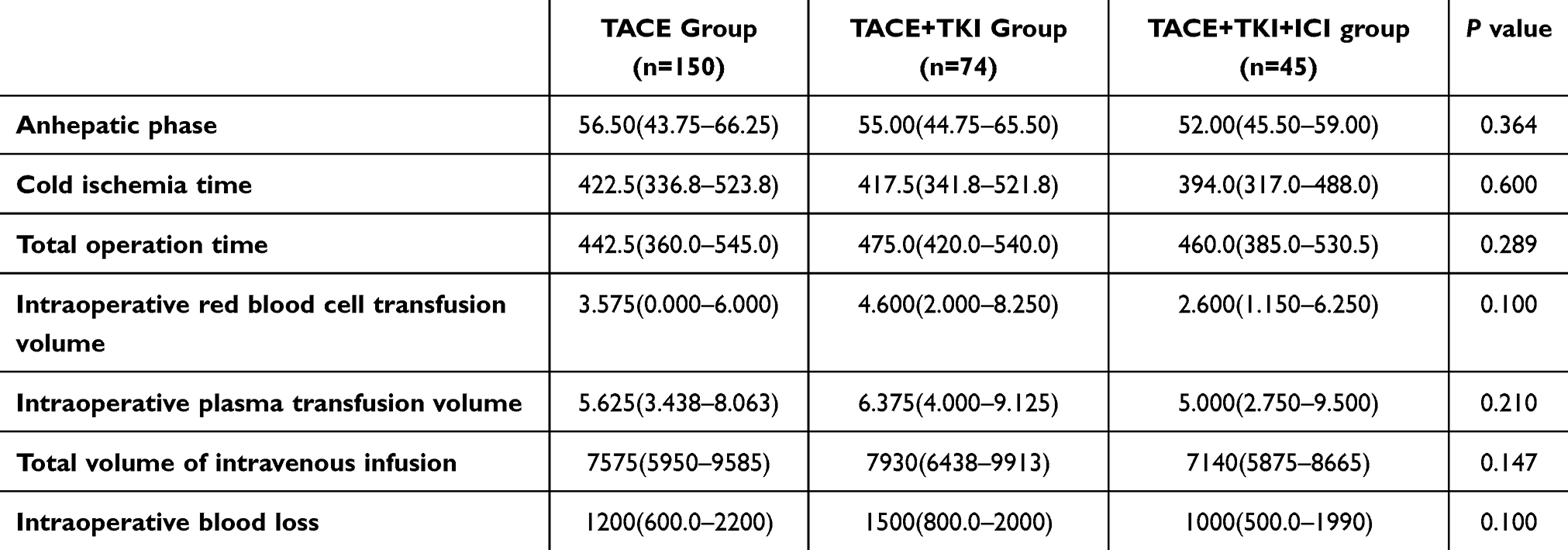 |
Table 12 Surgical Data |
Discussion
In recent years, advances in understanding HCC molecular mechanisms and treatment strategies have enhanced the potential of combining TACE, TKIs, and ICIs as preoperative therapy for LT22. This study systematically evaluates their role in downstaging HCC and enabling successful transplant conversion.
TACE, a core local therapy, induces ischemic necrosis by embolizing tumor-feeding arteries and increases localized chemotherapy concentration, effectively controlling intrahepatic disease progression.23 However, as monotherapy, its efficacy is limited. Complete arterial occlusion is difficult in larger tumors, and some patients fail to achieve downstaging.24 TKIs, such as lenvatinib and sorafenib, inhibit tumor angiogenesis and delay disease progression by targeting multiple tyrosine kinases, but their use is limited by significant adverse effects and unclear optimal agent selection.25 ICIs, including PD-1 and PD-L1 inhibitors, restore T-cell function and induce systemic anti-tumor immunity26 yet are contraindicated after transplantation due to the risk of graft rejection and show high inter-patient variability in efficacy. Notably, combining TACE, TKI, and ICI has a clear synergistic mechanism: TACE-induced tumor necrosis releases antigens and enhances tumor immunogenicity; TKIs inhibit angiogenesis and modulate the tumor microenvironment to reverse immunosuppression; ICIs further activate cellular immunity, enabling a systemic anti-tumor response. Thus, the triple therapy may promote substantial tumor shrinkage and increase pathological complete response rates, potentially improving eligibility for LT. However, its safety remains controversial.
A total of 269 liver transplant recipients were divided into three groups based on preoperative treatment. Baseline characteristics were comparable across groups, with no significant differences in gender, age, blood type, Child-Pugh score, BMI, etiology (mainly HBV), medical history, or smoking and drinking status. Donor characteristics were also similar, including gender, age, blood type, BMI, donor type (mostly DBD), and pre-donation bilirubin levels, supporting reliable intergroup comparisons.
The key finding is that triple therapy significantly outperformed TACE alone or TACE + TKI in DCR, ORR, and CRR. This supports the synergistic effect of local and systemic therapies: TACE induces tumor necrosis and antigen release, altering the immune microenvironment;27 TKI inhibits angiogenesis and modulates immunity;28 ICI relieves immune suppression and enhances anti-tumor responses.29 Together, they enable multidimensional tumor control, improving downstaging success and conversion rates. Patients receiving triple therapy had significantly longer RFS after LT, suggesting not only local tumor reduction but also elimination of undetectable micrometastases. As post-transplant recurrence often originates from such micrometastases, preoperative immune activation may provide long-term protection beyond surgery, enabling a shift from “transplantable” to “long-term tumor-free after transplant.” Despite these benefits, there was no significant difference in 1-year OS among groups. This may be due to several factors: LT itself greatly improves outcomes for all bridged patients, potentially masking differences; the follow-up period may be too short to detect OS differences; and post-recurrence treatments may influence OS results.
The adverse event profile in this study was consistent with the known safety profiles of the drugs. Hypothyroidism in the ICI group30 and hand-foot syndrome and proteinuria in the TKI group were target-specific, reflecting expected drug activity.31 Despite increased drug use with triple therapy, the incidence of common adverse events after TACE and systemic treatment—such as abdominal pain, fever, transient transaminase elevation, and nausea/vomiting—did not differ significantly across groups, indicating that intensified treatment did not worsen common toxicities.32 Safety data show that the TACE + TKI + ICI regimen improves tumor outcomes—including conversion rate, ORR, and RFS—while maintaining manageable safety. Most adverse reactions can be controlled through standard prevention, symptomatic management, and timely dose adjustments, without irreversible effects or impact on LT eligibility. Thus, in transplant centers with experienced multidisciplinary teams, this regimen offers favorable clinical feasibility and a positive risk-benefit profile. Based on prior and current efficacy and safety results, this study further supports TACE + TKI + ICI as a preferred pre-transplant strategy. It enhances tumor conversion and RFS without compromising transplant feasibility, alleviating surgical concerns about treatment-related risks, and encourages broader use of effective downstaging or bridging therapies under multidisciplinary care to improve long-term outcomes. This study is a retrospective study, and there is a selection bias. Meanwhile, the follow - up time is relatively short. In the future, we will collect more data to make the results more widely applicable. As a first-line drug for the treatment of hepatocellular carcinoma (HCC), the application of immune checkpoint inhibitors (ICI) before liver transplantation is controversial. However, current research also shows that the reasonable and standardized application of ICI before surgery can minimize the occurrence of postoperative rejection. In this study, there was no statistically significant difference in the probability of postoperative rejection among the three groups of patients included.
Conclusion
This study found that combining TACE, TKI, and ICI yielded the best DCR, ORR, and CRR, demonstrating strong synergy between local therapy and systemic immunotherapy and targeted therapy. The regimen significantly prolonged RFS after LT, reduced tumor stage, and provided long-term benefits without delaying transplantation. Adverse events were controllable and did not increase common side effects, indicating good safety under standardized management. No significant difference in 1-year OS was observed across groups, likely due to high LT efficacy, short follow-up, and subsequent therapies; long-term survival benefits require further evaluation. As a single-center study with limited follow-up, future research will extend follow-up duration and include multi-center data to enhance validity and clinical relevance.
Funding
This study was supported by grants from the Natural Science Foundation of Guangdong Province (2023A1515011805 and 2022A1515011052), the National Natural Science Foundation of China (81873591), the Science and Technology Planning Project of Guangdong Province (2018A050506030), the Science and Technology Program of Guangzhou (201704020073), the Guangdong Provincial Key Laboratory Construction Projection on Organ Donation and Transplant Immunology (2013A061401007, 2017B030314018, and 2020B1212060026), and the Guangdong Provincial International Cooperation Base of Science and Technology (Organ Transplantation) (2015B050501002 and 2020A0505020003).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–17. doi:10.1002/hep.28431
2. Huang DQ, Mathurin P, Cortez-Pinto H, et al. Global epidemiology of alcohol-associated cirrhosis and HCC: trends, projections and risk factors. Nat Rev Gastroenterol Hepatol. 2022;20(1):37–49. doi:10.1038/s41575-022-00688-6
3. Lai JC, Roberts JP. ABO-nonidentical liver transplantation in the United States. Am J Transplant. 2016;16(8):2430–2436. doi:10.1111/ajt.13763
4. Li M, Bhoori S, Mehta N, et al. Immunotherapy for hepatocellular carcinoma: the next evolution in expanding access to liver transplantation. J Hepatol. 2024;81(4):743–755. doi:10.1016/j.jhep.2024.05.037
5. Yao FY. Liver transplantation for hepatocellular carcinoma: beyond the milan criteria. Am J Transplant. 2008;8(10):1982–1989. doi:10.1111/j.1600-6143.2008.02351.x
6. Tsai MC, Yong -C-C, Lin -C-C, et al. Living donor liver transplantation for Barcelona clinic liver cancer (BCLC) intermediate-stage hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2023;12(2):169–182. doi:10.21037/hbsn-21-196
7. Victor DW, Monsour HP, Boktour M, et al. Outcomes of liver transplantation for hepatocellular carcinoma beyond the university of california san francisco criteria: a single-center experience. Transplantation. 2020;104(1):113–121. doi:10.1097/TP.0000000000002835
8. Ling S, Feng T, Zhan Q, et al. Sirolimus-based immunosuppression improves outcomes in liver transplantation recipients with hepatocellular carcinoma beyond the Hangzhou criteria. Ann translat Med. 2020;8(4):80. doi:10.21037/atm.2020.01.10
9. Kim WR, Mannalithara A, Heimbach JK, et al. MELD 3.0: the model for end-stage liver disease updated for the modern era. Gastroenterology. 2021;161(6):1887–1895.e4. doi:10.1053/j.gastro.2021.08.050
10. Kulik L, Heimbach JK, Zaiem F, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis. Hepatology. 2017;67(1):381–400. doi:10.1002/hep.29485
11. Yuan M, Zhou X, Luo R, et al. Real needs of end-stage kidney disease patients awaiting kidney transplantation in China: a qualitative study. Patient Educ Couns. 2025;135:108717. doi:10.1016/j.pec.2025.108717
12. Marzi L, Mega A, Turri C, et al. Immune checkpoint inhibitors in the pre-transplant hepatocellular carcinoma setting: a glimpse beyond the liver. Int J Mol Sci. 2024;25(21):11676. doi:10.3390/ijms252111676
13. Otto G, Schuchmann M, Hoppe-Lotichius M, et al. How to decide about liver transplantation in patients with hepatocellular carcinoma: size and number of lesions or response to TACE? J Hepatol. 2013;59(2):279–284. doi:10.1016/j.jhep.2013.04.006
14. Liu C-Y, Chen K-F, Chen P-J. Treatment of liver cancer. cold spring harbor perspectives in medicine. Blood Cancer J. 2015;5(9). doi:10.1038/bcj.2015.59
15. Tabrizian P, Abdelrahim M, Schwartz M. Immunotherapy and transplantation for hepatocellular carcinoma. J Hepatol. 2024;80(5):822–825. doi:10.1016/j.jhep.2024.01.011
16. Chiang CL, Chiu KWH, Chan KSK, et al. Sequential transarterial chemoembolisation and stereotactic body radiotherapy followed by immunotherapy as conversion therapy for patients with locally advanced, unresectable hepatocellular carcinoma (START-FIT): a single-arm, Phase 2 trial. Lancet Gastroenterol Hepatol. 2023;8(2):169–178. doi:10.1016/S2468-1253(22)00339-9
17. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
18. Pinter M, Scheiner B, Pinato DJ. Immune checkpoint inhibitors in hepatocellular carcinoma: emerging challenges in clinical practice. Lancet Gastroenterol Hepatol. 2023;8(8):760–770. doi:10.1016/S2468-1253(23)00147-4
19. Lee EW, Khan S. Recent advances in transarterial embolotherapies in the treatment of hepatocellular carcinoma. Clin Mol Hepatol. 2017;23(4):265–272. doi:10.3350/cmh.2017.0111
20. Wang Z, et al. Conversion therapy with TACE, TKIs, and ICIs for unresectable BCLC stage B and C hepatocellular carcinoma. Front Immunol. 2025;16.
21. Chen W, Yan H-T, Zhang J-X, et al. Transarterial chemoembolization combined with molecular targeted agents plus immune checkpoint inhibitors for unresectable hepatocellular carcinoma beyond the up-to-seven criteria: a propensity score-matching analysis. Ann Med. 2024;56(1). doi:10.1080/07853890.2024.2419993.
22. Zhu X-D, Li K-S, Sun H-C. Adjuvant therapies after curative treatments for hepatocellular carcinoma: current status and prospects. Genes Dis. 2020;7(3):359–369. doi:10.1016/j.gendis.2020.02.002
23. Tsurusaki M, Murakami T. Surgical and Locoregional Therapy of HCC: TACE. Liver Cancer. 2015;4(3):165–175. doi:10.1159/000367739
24. Kuroda H, Oikawa T, Ninomiya M, et al. Objective response by mrecist to initial lenvatinib therapy is an independent factor contributing to deep response in hepatocellular carcinoma treated with lenvatinib-transcatheter arterial chemoembolization sequential therapy. Liver Cancer. 2022;11(4):383–396. doi:10.1159/000522424
25. Mahaki H, Nobari S, Tanzadehpanah H, et al. Targeting VEGF signaling for tumor microenvironment remodeling and metastasis inhibition: therapeutic strategies and insights. Biomed. Pharmacother. 2025;186:118023. doi:10.1016/j.biopha.2025.118023
26. Xia L, Liu Y, Wang Y. PD-1/PD-L1 blockade therapy in advanced non-small-cell lung cancer: current status and future directions. oncologist. 2019;24(S1):S31–S41. doi:10.1634/theoncologist.2019-IO-S1-s05
27. Wang C, Leng B, You R, et al. A transcriptomic biomarker for predicting the response to tace correlates with the tumor microenvironment and radiomics features in hepatocellular carcinoma. J Hepatocell Carcinoma. 2024;11:2321–2337. doi:10.2147/JHC.S480540
28. Zhao Y, Zhang YN, Wang KT, et al. Lenvatinib for hepatocellular carcinoma: from preclinical mechanisms to anti-cancer therapy. Biochim. Biophys. Acta Rev. Cancer. 2020;1874(1):188391. doi:10.1016/j.bbcan.2020.188391
29. Das S, Johnson DB. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J Immunother Cancer. 2019;7(1). doi:10.1186/s40425-019-0805-8
30. Khoja L, Day D, Wei-Wu Chen T, et al. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–2385. doi:10.1093/annonc/mdx286
31. Zhou C, Wang W, Mu Y, et al. Efficacy and safety of a novel TKI (anlotinib) for the treatment of advanced digestive system neoplasms: a systematic review and meta-analysis. Front Immunol. 2024;15: 1393404
32. Fan W, Zhu B, Chen S, et al. Survival in patients with recurrent intermediate-stage hepatocellular carcinoma. JAMA Oncol. 2024;10(8):1047. doi:10.1001/jamaoncol.2024.1831
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.