Back to Journals » Research and Reports in Urology » Volume 15
Systemic Treatment-Decision Algorithms in Muscle-Invasive Bladder Cancer: Clinical Complexities and Navigating for Improved Outcomes
Received 17 April 2023
Accepted for publication 3 July 2023
Published 7 July 2023 Volume 2023:15 Pages 321—331
DOI https://doi.org/10.2147/RRU.S386549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Megan Giles,1 Simon J Crabb1,2
1Department of Medical Oncology, University Hospital Southampton NHS Foundation Trust, Southampton, UK; 2School of Cancer Sciences, University of Southampton, Southampton, UK
Correspondence: Simon J Crabb, University of Southampton, Mailpoint 824, Centre for Cancer Immunology, Southampton General Hospital, Southampton, SO16 6YD, UK, Email [email protected]
Abstract: Muscle-invasive bladder cancer has poor prognosis. If organ confined, it is potentially curable; however, across all prognostic groups, approximately half of patients will relapse. For patients with advanced disease, the median overall survival remains under two years. Systemic treatment options are centered on the use of platinum-based combination chemotherapy, with the choice of cisplatin- or carboplatin-based regimens determined on the basis of criteria including performance status and renal function. PD-1/PD-L1 checkpoint-directed immunotherapy has been established for use in advanced disease with modest overall improvements in survival outcomes. Based on current data, optimal utilization appears to be a switch maintenance strategy on completion of chemotherapy. In the curative setting, cisplatin-based chemotherapy provides modest improvements in cure rates in those fit to receive it. Data on the use of adjuvant immunotherapy are currently contradictory, with disease-free survival demonstrated for adjuvant nivolumab, but not atezolizumab, and no overall survival benefit has yet been confirmed. The Nectin-4 directed antibody drug conjugate enfortumab vedotin is an established treatment option for patients previously treated with both chemotherapy and immunotherapy. The emerging therapeutic targets under evaluation include Trop-2 with sacituzumab govitecan, fibroblast growth factor receptors, HER2, and DNA repair deficiency in biomarker-selected patients. The development of properly validated predictive biomarkers has proven challenging for this disease and should be a central priority in the future development of treatment options. This review summarizes the available systemic treatment options in both palliative and curative disease settings, and highlights the available evidence and current limitations for making treatment recommendations.
Keywords: bladder cancer, urothelial carcinoma, chemotherapy, immunotherapy, enfortumab vedotin
Introduction
Muscle-invasive bladder cancer (MIBC; urothelial carcinoma) was diagnosed in more than 570,000 patients in 2020, resulting in 210,000 deaths.1 In recent years, systemic treatment options for patients with advanced disease have increased, particularly with the introduction of programmed cell death protein 1 (PD-1)-directed checkpoint inhibitor immunotherapy and more recently, with the emergence of antibody drug conjugates (ADC). Consequently, treatment pathways and clinical decision-making have become more complex. In this review, we will highlight options for systemic treatment in both advanced disease and perioperative settings, with a focus on the evidence base and its limitations, from which key treatment decision recommendations may be made.
Palliative Treatment for Locally Advanced or Metastatic Disease
Locally advanced or metastatic MIBC (T4b, N+, and/or M1 staging) is conventionally viewed as an incurable disease. However, a small minority of long-term survivors, at least beyond 5 years, have been seen with both chemotherapy and immunotherapy.2–4 However, the majority of patients are faced with a much more limited likely prognosis and require careful selection to justify the potential toxicity of the available treatments. The standard first-line treatment in this setting, in those fit to receive it, has been cisplatin-based combination chemotherapy for more than 20 years.5 Prior to this, the median survival time is 3–6 months.6
Single-agent cisplatin has achieved remission rates of up to 40% in metastatic bladder cancer in some trials. In the early 1990s, Phase 3 trial data demonstrated that, compared to cisplatin monotherapy, combination treatment with methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) provided an improved response rate (39% vs 12%; P < 0.0001) in addition to gains in progression-free survival (10.0 v 4.3 months) and overall survival (12.5 v 8.2 months). However, this is at the expense of a greater toxicity burden, including leukopenia, mucositis, neutropenic fever, and treatment-related mortalities.7
A subsequent key multicenter, phase 3 trial compared MVAC with gemcitabine and cisplatin (GC) chemotherapy.3,6 Median overall survival was 14.8 months (95% CI, 13.2–16.8 months) with MVAC and 13.8 months (95% confidence interval [CI], 12.3–15.8 months) with GC. The time to disease progression, time to treatment failure, and response rates (MVAC, 46%; GC, 49%) were also similar.3 Although often interpreted as showing similar efficacy findings, this was, in fact, a negative study that failed to demonstrate a survival benefit for GC. However, there were clinically relevant higher rates of high-grade toxicity seen in MVAC treated patients compared to GC that included neutropenia (82% v 71%, respectively), neutropenic fever (14% v 2%), neutropenic sepsis (12% v 1%) and mucositis (22% v 1%). Quality of life outcomes also favored GC. As a result, GC has been widely adopted for use in advanced bladder cancer and is the starting point for most subsequent treatment selection choices.
During a similar timeframe, a phase 3 trial compared high-dose intensity MVAC (HD-MVAC) using two-week cycles facilitated through granulocyte colony-stimulating factor (G-CSF) support, with conventional MVAC (four-week cycles). HD-MVAC can be delivered in a shorter timeframe, with fewer delays, and, most importantly, with a reduced toxicity profile. Although the study did not reach statistical significance for the improvement in overall survival with HD-MVAC, it showed an objective benefit in response rates and progression-free survival.8,9 This led to HD-MVAC (dose-dense MVAC; dd-MVAC) becoming the preferred dosing schedule for this treatment combination.
Therefore, GC or dd-MVAC can be considered as the appropriate preferred options for first-line palliative treatment of advanced MIBC if patients are adequately fit to receive cisplatin-based combination treatment.5 To date, there have been no direct randomized comparisons of these options in advanced disease settings to guide the selection. Pretreatment factors that affect an individual’s likelihood of response to treatment and overall survival have been defined.10 They have been used to develop and validate prognostic models to predict clinical outcomes.11 The factors used within these models were performance status and the presence of visceral (lung, liver, or bone) metastases, as well as hemoglobin and albumin levels in an updated validation model.10,11
Therefore, a critical decision point for the selection of treatment options for advanced bladder cancer is the patient’s suitability for cisplatin-based combination chemotherapy. However, a substantial proportion of patients (up to approximately 50%), depending on the case mix, are deemed “ineligible” for cisplatin-based regimens. This key treatment decision is based on the multiple contributing factors discussed below.5,12
Cisplatin Eligibility and First-Line Treatment Selection
Given the benefit of cisplatin-based chemotherapy regimens, as well as the large percentage of patients who are considered ineligible, Galsky et al sought to determine parameters to define those who should be considered unfit (typically termed “ineligible”) for cisplatin-based treatment. Through consensus established via an international survey of 120 genitourinary oncologists, these criteria defined a patient as ineligible for cisplatin-based treatment if any of the following criteria were present:12
- World Health Organization (WHO)/Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) score ≥2 (Karnofsky PS score ≤70)
- Creatinine clearance (calculated or measured) <60 mL/min
- Audiometric hearing loss grade ≥2 (common terminology criteria for adverse events version 4 (CTCAE v4) grade)
- Peripheral neuropathy grade ≥2 (CTCAE v4 grade)
- New York Heart Association class III heart failure
Although the Galsky criteria are commonly used in a formal manner to determine eligibility for cisplatin-based combination chemotherapy in guidelines and trial criteria,5,13 there may be some variation in real-world routine clinical practice. In particular, regarding renal function, conventional cisplatin combinations are generally considered safe to be administered (where this is an isolated factor for considering treatment exclusion) at levels as low as approximately 50 mL/min.
A number of small Phase 2 trials have also used cisplatin-based chemotherapy in patients with a lower creatinine clearance down to a lower limit of either 35 or 40 mL/min, using split dosing schedules in either advanced or neoadjuvant bladder cancer treatment settings.14–16 These trials found that cisplatin-based chemotherapy was seemingly feasible with these lower creatinine clearance ranges, although one study’s subgroup analysis suggested that those with a creatinine clearance of ≥49 mL/min may have had better overall and progression-free survival.16 Furthermore, we lack randomized data on the relative efficacy of a split-dose cisplatin-containing regimen with carboplatin-based combinations (discussed below). The current European Association of Urology (EAU) guidelines define cisplatin-eligible patients as those with a glomerular filtration rate >50–60 mL/min if the other Galsky criteria are met.5
First-Line Treatment Options for “Cisplatin Ineligible” Patients
Gemcitabine in combination with carboplatin (GCarbo) is widely used as an alternative chemotherapeutic approach in patients deemed ineligible for cisplatin. A Phase II/III randomized EORTC study compared GCarbo to methotrexate, carboplatin, and vinblastine (M-CAVI), in patients ineligible for cisplatin.17 The study used a glomerular filtration rate (GFR) of <60 mL/min but >30 mL/min and/or a performance status of 2 to define patients as unfit for cisplatin within the trial (and thus, very similar, but not precisely, the following the Galsky criteria that are now most commonly referenced). The study did not show a statistically significant difference in overall survival (primary endpoint) or progression-free survival between the two arms. However, the response rate of 41.2% in the GCarbo arm was 30.3% in the M-CAVI arm. In addition, GCarbo-treated patients experienced fewer severe acute toxicities (defined as death, grade 4 thrombocytopenia with bleeding, grade 3 or 4 renal toxicity, neutropenic fever, or mucositis) than those treated with M-CAVI (9.3% and 21.2%, respectively).17 Therefore, GCarbo has been widely adopted as a standard of care as a carboplatin-based option for first-line treatment of patients with advanced urothelial carcinoma deemed ineligible for cisplatin-based chemotherapy.5
First-Line Combination Immunotherapy with Chemotherapy or Doublet Immunotherapy
Three Phase III trials, IMvigor130,18 KEYNOTE-36119 and DANUBE,20 tested the role of first-line immunotherapy agents in advanced urothelial carcinoma. IMvigor130 and KEYNOTE-361 compared PD-1/programmed cell death ligand 1 (PD-L1) immune checkpoint inhibitors, either as monotherapy or in combination with platinum-based chemotherapy, versus platinum-based chemotherapy alone. DANUBE is the only currently reported study to compare doublet immunotherapy (PD-L1 and cytotoxic T-lymphocyte associated protein 4 (CTLA4) inhibitors) or single-agent PD-L1 inhibitor monotherapy versus platinum-based chemotherapy. The results of these three trials comparing relevant immunotherapy combinations versus chemotherapy alone are summarized in Table 1. In summary, these three trials failed to show evidence to support the first-line use of combination immunotherapy, either combined with platinum-based chemotherapy or as doublet immunotherapy in this setting. At the time of writing, a recent press release indicated that a fourth combination immunotherapy study, CheckMate901 (NCT03036098), which tested nivolumab in combination with ipilimumab or platinum-based chemotherapy, did not meet one of the co-primary endpoints of overall survival in patients with high PD-L1 expressing cancers. At present, platinum-based, and if possible and cisplatin-based, chemotherapy remains the standard treatment options for patients fit to receive it.
 |
Table 1 Outcomes for the IMvigor130, KEYNOTE-361 and DAUBE Trials |
Maintenance Immunotherapy
Despite the relatively high response rates from platinum-based chemotherapy, the median progression-free survival and overall survival are only approximately 8 and 14 months, respectively, even in those able to receive cisplatin-based combinations.3 The outcomes of second-line treatments (discussed below) remain less favorable. The phase 3 JAVELIN Bladder 100 trial tested an alternative switch maintenance immunotherapy strategy to optimize the benefits achieved immediately following first-line chemotherapy.2 In this trial, patients who achieved stable disease or better following first-line treatment with gemcitabine and platinum combination chemotherapy were randomized to receive avelumab immunotherapy or best supportive care. The study demonstrated a significant overall survival benefit of 21.4 months in the avelumab group, compared to 14.3 months with best supportive care alone (hazard ratio for death 0.69; 95% CI 0.56 to 0.86; P = 0.001).2 Currently, this is the longest absolute survival gain demonstrated to date for this disease. Therefore, maintenance avelumab has been adopted as the standard of care following the completion of first-line platinum-based chemotherapy.5,13 The overall survival benefit was observed irrespective of PD-L1 status; therefore, biomarker status is not required in this setting to determine the suitability for avelumab maintenance treatment. Subsequent updates to the data from this trial have indicated treatment benefits with immunotherapy irrespective of prior use of GC or GCarbo, or whether a patient has achieved stable disease or an objective radiological response to chemotherapy.
Within the JAVELIN Bladder 100 trial, patients were deemed eligible for entry after receiving 4–6 cycles of chemotherapy with a treatment-free interval of 4–10 weeks after chemotherapy.2 The optimal number of chemotherapy cycles (4–6), as well as the timing window in which to commence avelumab following the completion of chemotherapy, is therefore relevant questions for the implementation of this treatment approach. However, subgroup analyses from JAVELIN Bladder 100 suggest that all patients gain benefit from addition of avelumab irrespective of these variables. A further randomized phase 2 trial tested maintenance of pembrolizumab in the same treatment setting (stable disease or better following platinum-based chemotherapy) versus a placebo. Progression-free survival improvement was demonstrated (5.4 months [95% CI, 3.1 to 7.3 months] v 3.0 months [95% CI; 2.7 to 5.5 months]; hazard ratio, 0.65; log-rank P5.04; maximum efficiency robust test P5.039), providing supporting evidence for avelumab.21
Single-Agent First-Line Immunotherapy
Both IMvigor13018 and KEYNOTE-36119 included a single-agent immunotherapy arm within the trials. This followed accelerated approval of single-agent atezolizumab by the United States Food and Drug Administration (FDA) in 2017, based on promising results demonstrated in IMvigor210.18,22 In this single-arm Phase II trial, cisplatin-ineligible patients received atezolizumab and demonstrated a median overall survival of 15.9 months. PD-L1 expression using the Ventana SP142 PD-L1 immunohistochemical assay scoring criteria for infiltrating immune cells (<1%, ≥1% and <5%, or ≥5%) but did not demonstrate a statistically significant difference in response to atezolizumab with respect to PD-L1 expression.22 In a similar phase II study, KEYNOTE-052 demonstrated a response rate of 24% (95% CI, 20–29) to single-agent pembrolizumab. However, KEYNOTE-052 showed improved response rates in patients with high PD-L1 expression (tumor cells, macrophages, or lymphocytes) using the 22C3 pharmDx assay with a combined positive score of >10.23
Interim assessment of IMvigor130 and KEYNOTE-361 in 2018 with analysis of PD-L1 expression subgroups within these trials produced a change in FDA and European Medicine Agency (EMA) approvals (based on data not presented at that time) for single-agent immunotherapy in the first-line setting to limit the use of PD-L1 high-expressing tumors only.18 The final published results of both trials showed contrasting results regarding the effects of PD-L1 expression status. In exploratory analyses, IMvigor130 found an increased overall survival benefit for atezolizumab monotherapy in the high PD-L1 expression subgroup, but for chemotherapy in patients with low PD-L1 expression. In comparison, KEYNOTE-361 did not show a difference in overall survival with respect to pembrolizumab monotherapy over chemotherapy in the PD-L1 high subgroups.18,19
These contrasting results have led to uncertainty regarding the role of single-agent immunotherapy as a first-line treatment in this setting, and the significance of PD-L1 expression status in treatment decisions. This has led to differences in the guidelines for first-line immunotherapy of advanced urothelial bladder carcinoma. Current EMA approvals allow the use of single-agent immunotherapy, with either atezolizumab or pembrolizumab, as first-line treatment in cisplatin-ineligible patients with high PD-L1 expression (using the relevant immunohistochemical test). However, the EAU guidelines recommend GCarbo as the preferred treatment choice over single-agent immunotherapy and restrict immunotherapy to platinum-ineligible patients (with a stronger recommendation if PD-L1 expression is high). The European Society for Medical Oncology (ESMO) guidance recommends the use of GCarbo if PD-L1 expression is low (or unknown) versus atezolizumab or pembrolizumab if PD-L1 expression is high for all cisplatin-ineligible patients (and avoids the distinction of platinum ineligibility). In those unfit for any platinum-based chemotherapy, the guidelines acknowledge the limited trial data on the treatment options in this cohort. The FDA, but not EMA, has restricted the use of single-agent immunotherapy in patients who are ineligible for platinum, regardless of PD-L1 status.5
Second-Line Chemotherapy and Immunotherapy
Data supporting second-line chemotherapy after first-line platinum-based chemotherapy have consistently demonstrated limited evidence of its clinical benefits. No study has established a survival advantage from the use of chemotherapy, and only one randomized trial has been completed that failed to demonstrate the benefit of vinflunine over supportive care.24 Single-agent paclitaxel, docetaxel, and vinflunine are commonly used but are largely based on phase II trials with PFS and OS consistently at under 6 and 12 months, respectively.5,25–28 As such, the rationale for proceeding with systemic treatment with chemotherapy in this setting requires careful consideration of a patient’s fitness and treatment goals and an honest discussion about the potential for benefit versus side effects.
Multiple immunotherapy agents have been evaluated as second-line therapies for those progressing despite first-line platinum-based chemotherapy. Based on Phase I and II data, atezolizumab was the first FDA-approved immunotherapy in this setting. However, the phase III randomized controlled IMvigor211 trial did not meet its primary endpoint of overall survival for atezolizumab versus a physician’s choice of chemotherapy options.25 In contrast, the phase III KEYNOTE-045 trial demonstrated a significant overall survival benefit compared with chemotherapy.26 The efficacy results of these studies are summarized in Table 2.
 |
Table 2 Outcomes for the IMvigor211 and KEYNOTE-045 Second-Line Immunotherapy Trials |
Enfortumab Vedotin Following Prior Chemotherapy and Immunotherapy
Antibody-drug conjugates (ADC) against a variety of targets are currently under investigation for the treatment of this disease. Enfortumab vedotin is the most advanced in development and has become a treatment option for patients who have received both prior platinum-based chemotherapy and PD-1/PD-L1 directed immunotherapy.5 Enfortumab vedotin is a monoclonal antibody against nectin-4, a highly expressed cell adhesion molecule in urothelial malignancy that is linked to a microtubule-targeting chemotherapy agent. A phase III open-label trial randomized 608 patients to receive either enfortumab vedotin or chemotherapy (physician’s choice of vinflunine, paclitaxel, or docetaxel) after radiographic progression or relapse during or after PD-1/PD-L1 inhibitor treatment and prior platinum-containing chemotherapy. This demonstrated a significant difference in overall survival of 12.88 months in the enfortumab vedotin cohort compared to 8.97 months in the chemotherapy cohort (hazard ratio 0.70; 95% CI 0.56 to 0.89; P = 0.001). There was also a significant difference in the progression-free survival of 5.55 months in the enfortumab vedotin cohort compared to 3.71 months in the chemotherapy cohort (hazard ratio, 0.62; 95% CI, 0.51 to 0.75; P < 0.001). Although there was a similar overall incidence of toxicities, the patterns differed with more frequent rash, peripheral neuropathy, and hyperglycemia in the enfortumab vedotin group, and neutropenia and febrile neutropenia more frequently with chemotherapy.29 The sequence or combination of prior treatments was flexible; therefore, enfortumab vedotin can be considered a post-chemotherapy/post-immunotherapy treatment option.
Treatment for Potentially Curable Disease
Selection for Neoadjuvant Chemotherapy
Organ-confined and locally advanced muscle-invasive bladder cancer is a potentially curable disease that can be treated with either radical cystectomy or chemoradiotherapy. However, the risk of relapse and associated cancer-related mortality remains high, typically in the first two–three years after radical therapy.30 Decision-making between surgery and organ preservation options is complex, and we lack randomized data to support this choice of treatment. Nevertheless, there is an established survival advantage with the use of neoadjuvant systemic chemotherapy with a cisplatin-based regimen. The primary decision point for the use of neoadjuvant chemotherapy is, therefore, based on the assessment of cisplatin eligibility, and again, the Galsky criteria provide an objective approach to assessing these, in the same way as described above for advanced disease. The data to support neoadjuvant chemotherapy were primarily based on two randomized phase 3 trials that tested either cisplatin, methotrexate, and vinblastine (CMV) or conventional MVAC (Table 3), in addition to a meta-analysis of these and other smaller trials.30–33 The results of this study support a 5–6% absolute survival advantage with the addition of neoadjuvant chemotherapy to either surgery or chemoradiotherapy alone. Subset analysis from the CMV trial suggested a similar benefit of neoadjuvant chemotherapy following either cystectomy or bladder preservation with radiotherapy.33 Through extrapolation from data from the advanced disease setting, most oncologists would opt for either the GC or dd-MVAC regimen as the choice of cisplatin-based neoadjuvant treatment. We lack adequate randomized data to support the use of carboplatin-based chemotherapy or other non-cisplatin combinations, which should be reserved for future clinical trials.
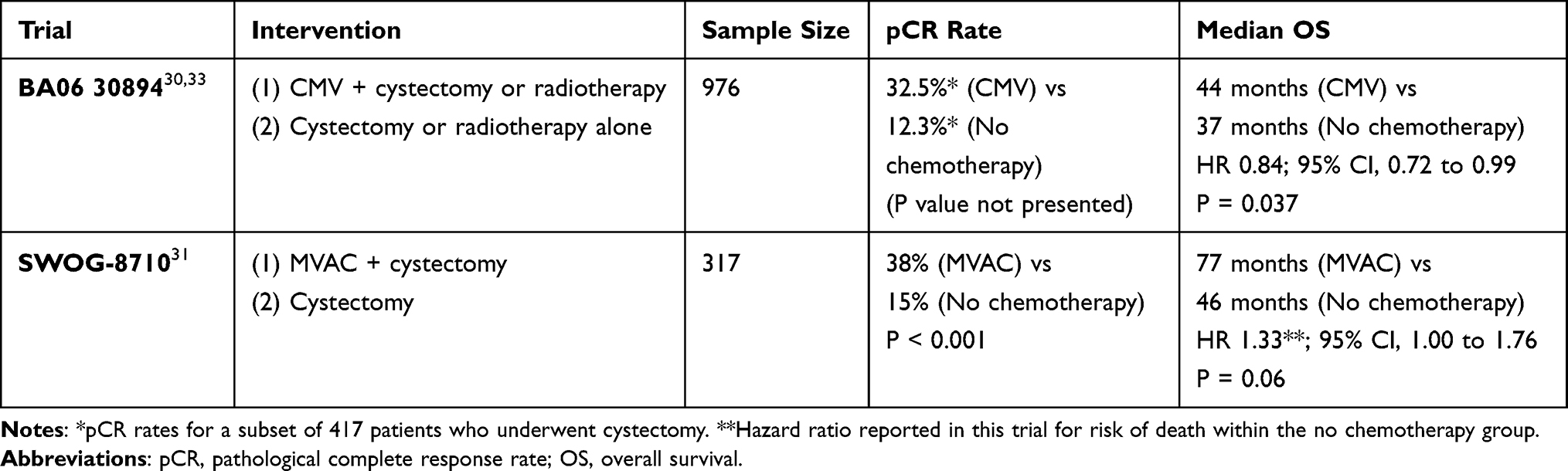 |
Table 3 Outcomes for Randomised Phase III Trials of Neoadjuvant Chemotherapy |
Recent data from the VESPER trial have provided evidence that might support the superiority of dd-MVAC over GC.34 This trial randomized between these two treatment approaches in patients receiving chemotherapy in either a neoadjuvant or an adjuvant perioperative setting. The trial did not meet its primary endpoint for progression-free survival at 3 years (64% vs 56%, respectively; hazard ratio 0.77, 95% CI, 0.57 to 1.02; P = 0.066). However, in a subset of patients who received neoadjuvant chemotherapy, there was evidence that the benefit for the dd-MVAC with PFS at 3 years was significantly higher than that for GC (66% vs 56%, hazard ratio 0.70, 95% CI, 0.51 to 0.96; P = 0.025).
Selection for Adjuvant Chemotherapy and Immunotherapy
Adjuvant chemotherapy appears to provide an approximately equivalent absolute survival advantage to that gained with neoadjuvant chemotherapy based on individual trial data and meta-analysis.35,36 However, the lack of any single fully recruited phase 3 adjuvant trial, and the fact that the number of patients included in the meta-analysis was substantially lower, supports a preference for neoadjuvant chemotherapy over adjuvant chemotherapy in general. This treatment preference is perhaps compounded if adjuvant immunotherapy is considered an option (discussed below). However, in selected patients, for example those “upstaged” to muscle invasive disease following radical cystectomy, there remains a role for adjuvant chemotherapy in some situations. Again, this should be restricted to a cisplatin-based combination approach, and the choice of regimen is typically GC or dd-MVAC.
Approximately 5% of urothelial carcinomas originate in the upper urinary tract and are potentially curable by nephroureterectomy. The POUT randomized phase III trial tested adjuvant chemotherapy, which was either cisplatin- or carboplatin-based, depending on the renal function.37 This trial found a 3-year disease-free survival rate of 71% and 46% for chemotherapy and surveillance, respectively (hazard ratio 0.45, 95% CI 0.30–0.68; P = 0.0001), and a trend toward overall survival benefit as a secondary endpoint. Therefore, adjuvant chemotherapy is an appropriate treatment option for this rare disease.
Currently available data are conflicting regarding the benefits of PD-1/PD-L1 directed immunotherapy as an adjuvant treatment following radical cystectomy. In the CheckMate274 study, patients with a pathological stage of pT3-4a or pN+ (as well as pT2 after prior neoadjuvant cisplatin-based chemotherapy) in the cystectomy sample were randomized between nivolumab immunotherapy and observation.38 Data presented to date show a 12-month disease-free survival benefit of 62.8% with nivolumab versus 46.6% with placebo (hazard ratio, 0.70; 98.22% CI, 0.55 to 0.90; P < 0.001). Overall survival was a secondary endpoint in this trial, and the data are anticipated keenly once they were suitably mature. Many investigators will reserve judgement on the routine use of adjuvant immunotherapy until overall survival data are available from this trial; however, relapse-free survival data alone have led to its implementation in many countries. Notably, in Europe, license indications were restricted to patients with high PD-L1 expression in their cystectomy samples. This subset (as a co-primary endpoint in this trial) had a 12-month disease-free survival of 67.2% with nivolumab versus 45.9% with a placebo hazard ratio of 0.55 (98.72% CI, 0.35–0.85; P < 0.001). This contrasts with the United States, where a license exists for the use of adjuvant nivolumab based on the overall intention-to-treat population data from this trial, irrespective of PD-L1 expression status.
In contrast to the data with nivolumab, in a similar phase III adjuvant study, IMvigor010, testing atezolizumab was unable to demonstrate an improvement in disease-free survival (hazard ratio 0.89; 95% CI 0.74–1.08; P = 0.24) or overall survival.39 Further data are pending from a third ongoing phase III adjuvant pembrolizumab trial (NCT03244384).
As with advanced disease, it is likely that outcomes will be optimized if suitably validated patient selection approaches for the use of neoadjuvant or adjuvant systemic therapies are developed. One of the most promising options is the use of circulating tumor DNA (ctDNA) for the selection of adjuvant immunotherapy. A post-hoc exploratory analysis of the IMvigor010 trial found that patient benefit in terms of overall and disease-free survival from adjuvant atezolizumab appears to have been restricted to a subset of patients who had detectable ctDNA post-cystectomy.40 This has led to a current randomized phase III trial (IMvigor011, NCT04660344), which is testing a surveillance strategy using ctDNA post-operatively and then randomizing those patients who become ctDNA-positive between the use of atezolizumab immunotherapy and placebo.
Emerging Systemic Treatment Approaches
Emerging treatment approaches for patients with advanced bladder cancer, following currently established treatments, include tumor-associated calcium signal transducer 2 (Trop-2)-directed antibody drug conjugate sacituzumab govitecan. Trop-2 is a transmembrane glycoprotein involved in intracellular calcium signal transduction. It is differentially expressed in several solid malignancies, including bladder cancer. Sacituzumab govitecan is a humanized anti-Trop2 monoclonal antibody linked to the topoisomerase inhibitor, SN-38. Phase 2 data from 113 patients with locally advanced or unresectable UC who had progressed after prior platinum-based chemotherapy and immunotherapy showed an objective response rate of 27% (95% CI, 19.5 to 36.6) and 77% had a decrease in measurable disease. Treatment-related adverse events included neutropenia, leukopenia, anemia, diarrhea, and febrile neutropenia (10%).41 Phase 3 evaluation in this setting (NCT04527991) and the development of immunotherapy combinations are ongoing.
Fibroblast growth factor receptor (FGFR) mutations affect up to 20% of advanced urothelial carcinomas. Erdafitinib, a tyrosine kinase pan-inhibitor of FGFR 1–4, has shown a response rate in patients with FGFR mutations or fusions in advanced urothelial carcinoma of the bladder.42 The BLC2001 study was a phase II study in which patients with a prespecified FGFR alteration (FGFR3 mutation or FGFR2/3 fusion) who received erdafitinib had progressed on previous treatment or those who had received no previous chemotherapy if they were cisplatin-ineligible. The overall objective response rate was 40%, and an additional 39% of the patients had stable disease.42 This has led to the FDA-approved of erdafitinib as a second-line treatment following platinum-containing chemotherapy in patients with specific FGFR2 or FGFR3 alterations.5 Phase III investigations of erdafitinib are ongoing (NCT03390504), and other FGFR inhibitors are in development.
Encouraging phase 2 data were obtained with a combination of pembrolizumab and enfortumab vedotin. Among 45 cisplatin-ineligible, treatment-naive patients, the confirmed objective response rate was 73.3%, with a complete response rate of 15.6%.43 The median durations of response and overall survival were 25.6 months and 26.1 months, respectively. These exciting results require validation but have led to an ongoing phase 3 trial testing this combination against first-line platinum-based chemotherapy (NCT04223856). Further therapeutic targets with initial phase 2 data to support further investigation (in biomarker selected subsets) include HER2 (human epidermal growth factor receptor 2) and PARP (poly-ADP ribose polymerase) inhibition.44–46
Conclusion
Despite a substantial change in the systemic treatment options available for muscle-invasive bladder cancer, there remains a significant unmet need in terms of the relatively high risk of relapse in the curative disease setting and short prognosis for advanced disease. Chemotherapy is effective in inducing clinical response in some patients. However, the toxicity of platinum-based chemotherapy limits its utility in many patients, and the disease progression is relatively rapid in most patients. Immunotherapy, particularly as a post-induction maintenance strategy, and enfortumab vedotin have advanced outcomes; however, the overall survival gain remains relatively modest. Areas for medium-term progress potentially include pending phase 3 data for FGFR inhibition, sacituzumab govitecan, and ADC combinations (in particular, for enfortumab vedotin combined with pembrolizumab). Systemic neoadjuvant chemotherapy provides modest improvements in the cure rates for this disease. The role of perioperative immunotherapy remains to be fully elucidated, with conflicting results between current data. One of the challenges in improving systemic treatment is the development and validation of predictive biomarkers for treatment selection. Ideally, biomarker hypotheses should be prospectively incorporated into all therapeutic trials, but these are logistically challenging and expensive.
Disclosure
Professor Simon Crabb reports grants, personal fees from AstraZeneca, grants, personal fees from Roche, grants, personal fees from Clovis Oncology, grants, personal fees from Astex Pharmaceuticals, personal fees from Merck, personal fees from MSD, personal fees from Janssen, personal fees from BMS, personal fees from Bayer, personal fees from Pfizer, personal fees from Amgen, personal fees from Amphista Therapeutics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Powles T, Park SH, Voog E, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med. 2020;383(13):1218–1230. doi:10.1056/NEJMoa2002788
3. Von Der Maase H, Sengelov L, Roberts JT, et al. Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. J Clin Oncol. 2005;23(21):4602–4608. doi:10.1200/JCO.2005.07.757
4. Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30(6):970–976. doi:10.1093/annonc/mdz127
5. European Association of Urology. EAU guidelines on muscle-invasive and metastatic bladder cancer; 2022. Available from: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Muscle-Invasive-And-Metastatic-Bladder-Cancer-2022.pdf.
6. von der Maase H, Hansen SW, Robers JT, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, Phase III study. J Clin Oncol. 2000;17(17):3069–3077.
7. Loehrer PJ, Einhorn LH, Elson PJ, et al. A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: a cooperative group study. J Clin Oncol. 1992;10(7):1066–1073. doi:10.1200/JCO.1992.10.7.1066
8. Sternberg CN, de Mulder PHM, Schornagel JH, et al. Randomized phase III trial of high-dose-intensity methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) chemotherapy and recombinant human granulocyte colony-stimulating factor versus classic MVAC in advanced urothelial tract tumors: European Organization for Research and treatment of cancer protocol no. 30924. J Clin Oncol. 2001;19(10):2638–2646. doi:10.1200/JCO.2001.19.10.2638
9. Sternberg CN, de Mulder P, Schornagel JH, et al. Seven year update of an EORTC phase III trial of high-dose intensity M-VAC chemotherapy and G-CSF versus classic M-VAC in advanced urothelial tract tumours. Eur J Cancer. 2006;42(1):50–54. doi:10.1016/j.ejca.2005.08.032
10. Bajorin DF, Dodd PM, Mazumdar M, et al. Long-term survival in metastatic transitional-cell carcinoma and prognostic factors predicting outcome of therapy. J Clin Oncol. 1999;17(10):3173–3181. doi:10.1200/JCO.1999.17.10.3173
11. Apolo AB, Ostrovnaya I, Halabi S, et al. Prognostic model for predicting survival of patients with metastatic urothelial cancer treated with cisplatin-based chemotherapy. J Natl Cancer Inst. 2013;105(7):499–503. doi:10.1093/jnci/djt015
12. Galsky MD, Hahn NM, Rosenberg J, et al. Treatment of patients with metastatic urothelial cancer “Unfit” for cisplatin-based chemotherapy. J Clin Oncol. 2011;29(17):2432–2438. doi:10.1200/JCO.2011.34.8433
13. Powles T, Bellmunt J, Comperat E, et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(3):244–258. doi:10.1016/j.annonc.2021.11.012
14. Hussain SA, Palmer DH, Lloyd B, et al. A study of split-dose cisplatin-based neo-adjuvant chemotherapy in muscle-invasive bladder cancer. Oncol Lett. 2012;3(4):855–859. doi:10.3892/ol.2012.563
15. Hussain SA, Stocken DD, Riley P, et al. A phase I/II study of gemcitabine and fractionated cisplatin in an outpatient setting using a 21-day schedule in patients with advanced and metastatic bladder cancer. Br J Cancer. 2004;91(5):844–849. doi:10.1038/sj.bjc.6602112
16. Morales-Barrera R, Bellmunt J, Suárez C, et al. Cisplatin and gemcitabine administered every two weeks in patients with locally advanced or metastatic urothelial carcinoma and impaired renal function. Eur J Cancer. 2012;48(12):1816–1821. doi:10.1016/j.ejca.2012.04.002
17. De Santis M, Bellmunt J, Mead G, et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer who are unfit for cisplatin-based chemotherapy: EORTC study 30986. J Clin Oncol. 2012;30(2):191–199. doi:10.1200/JCO.2011.37.3571
18. Galsky MD, Arija JÁA, Bamias A, et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10236):1547–1557. doi:10.1016/S0140-6736(20)30230-0
19. Powles T, Csőszi T, Özgüroğlu M, et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(7):931–945. doi:10.1016/S1470-2045(21)00152-2
20. Powles T, van der Heijden MS, Castellano D, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (Danube): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020;21(12):1574–1588. doi:10.1016/S1470-2045(20)30541-6
21. Galsky MD, Mortazavi A, Milowsky MI, et al. Randomized double-blind Phase II study of maintenance pembrolizumab versus placebo after first-line chemotherapy in patients with metastatic urothelial cancer. J Clin Oncol. 2020;38(16):1797–1806. doi:10.1200/JCO.19.03091
22. Balar AV, Galsky MD, Rosenberg JE, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017;389(10064):67–76. doi:10.1016/S0140-6736(16)32455-2
23. Balar AV, Castellano D, O’Donnell PH, et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. Lancet Oncol. 2017;18(11):1483–1492. doi:10.1016/S1470-2045(17)30616-2
24. Bellmunt J, Théodore C, Demkov T, et al. Phase III trial of vinflunine plus best supportive care compared with best supportive care alone after a platinum-containing regimen in patients with advanced transitional cell carcinoma of the urothelial tract. J Clin Oncol. 2009;27(27):4454–4461. doi:10.1200/JCO.2008.20.5534
25. Powles T, Durán I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2018;391(10122):748–757. doi:10.1016/S0140-6736(17)33297-X
26. Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376(11):1015–1026. doi:10.1056/NEJMoa1613683
27. Jones RJ, Hussain SA, Protheroe AS, et al. Randomized Phase II study investigating pazopanib versus weekly paclitaxel in relapsed or progressive urothelial cancer. J Clin Oncol. 2017;35(16):1770–1777. doi:10.1200/JCO.2016.70.7828
28. Petrylak D, de Wit R, Chi KN, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel in patients with locally advanced or metastatic urothelial carcinoma after platinum-based therapy (RANGE): a randomised, double-blind, phase 3 trial. Lancet. 2017;390(10109):2266–2277. doi:10.1016/S0140-6736(17)32365-6
29. Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N Engl J Med. 2021;384(12):1125–1135. doi:10.1056/NEJMoa2035807
30. International Collaboration of Trialists. Neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: a randomised controlled trial. Lancet. 1999;354(9178):533–540. doi:10.1016/S0140-6736(99)02292-8
31. Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859–866. doi:10.1056/NEJMoa022148
32. Vale CL; Advanced Bladder Cancer (ABC) Meta-analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol. 2005;48(2):202–206. doi:10.1016/j.eururo.2005.04.006
33. International Collaboration of Trialists. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long-term results of the BA06 30894 trial. J Clin Oncol. 2011;29(16):2171–2177. doi:10.1200/JCO.2010.32.3139
34. Pfister C, Gravis G, Echon F, et al. Dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin or gemcitabine and cisplatin as perioperative chemotherapy for patients with nonmetastatic muscle-invasive bladder cancer: results of the GETUG-AFU V05 VESPER trial. J Clin Oncol. 2022;40(18):2013–2022. doi:10.1200/JCO.21.02051
35. Advanced Bladder Cancer (ABC) Meta-analysis Collaboration. Adjuvant chemotherapy in invasive bladder cancer: a systematic review and meta-analysis of individual patient data. In: European Urology. Vol. 48. Elsevier; 2005: 189–201.
36. Sternberg CN, Skoneczna I, Kerst JM, et al. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): an intergroup, open-label, randomised phase 3 trial. Lancet Oncol. 2015;16(1):76–86. doi:10.1016/S1470-2045(14)71160-X
37. Birtle A, Johnson M, Chester J, et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): a phase 3, open-label, randomised controlled trial. Lancet. 2020;395(10232):1268–1277. doi:10.1016/S0140-6736(20)30415-3
38. Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102–2114. doi:10.1056/NEJMoa2034442
39. Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525–537. doi:10.1016/S1470-2045(21)00004-8
40. Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021;595(7867):432–437. doi:10.1038/s41586-021-03642-9
41. Tagawa ST, Balar AV, Petrylak DP, et al. TROPHY-U-01: a Phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol. 2021;39(22):2474–2485. doi:10.1200/JCO.20.03489
42. Loriot Y, Necchi A, Park SH, et al. Erdafitinib in locally advanced or metastatic urothelial carcinoma. N Engl J Med. 2019;381(4):338–348. doi:10.1056/NEJMoa1817323
43. Hoimes CJ, Flaig TW, Milowsky MI, et al. Enfortumab vedotin plus pembrolizumab in previously untreated advanced urothelial cancer. J Clin Oncol. 2022;41(1):22–31. doi:10.1200/JCO.22.01643
44. Scherrer E, Kang A, Bloudek LM, Koshkin VS. HER2 expression in urothelial carcinoma, a systematic literature review. Front Oncol. 2022;12. doi:10.3389/fonc.2022.1011885
45. Rosenberg JE, Park SH, Kozlov V, et al. Durvalumab plus olaparib in previously untreated, platinum-ineligible patients with metastatic urothelial carcinoma: a multicenter, randomized, Phase II trial (BAYOU). J Clin Oncol. 2022;41(1):43–53. doi:10.1200/JCO.22.00205
46. Crabb SJ, Hussain S, Soulis E, et al. A randomized, double-blind, biomarker-selected, Phase II clinical trial of maintenance poly ADP-ribose polymerase inhibition with rucaparib following chemotherapy for metastatic urothelial carcinoma. J Clin Oncol. 2023;41(1):54–64. doi:10.1200/JCO.22.00405
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Options for Metastatic Urothelial Carcinoma After First-Line Chemotherapy
Tassinari E, Mollica V, Nuvola G, Marchetti A, Rosellini M, Massari F
Cancer Management and Research 2022, 14:1945-1960
Published Date: 13 June 2022
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Chiang RS, Glover MJ, Khaki AR, Srinivas S
OncoTargets and Therapy 2022, 15:1259-1269
Published Date: 20 October 2022
Nanoparticles for Chemoimmunotherapy Against Triple-Negative Breast Cancer
Liu S, Li J, Gu L, Wu K, Xing H
International Journal of Nanomedicine 2022, 17:5209-5227
Published Date: 7 November 2022
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Diagnosis, Prognosis, and Treatment of Triple-Negative Breast Cancer: A Review
Jie H, Ma W, Huang C
Breast Cancer: Targets and Therapy 2025, 17:265-274
Published Date: 17 March 2025