Back to Journals » Local and Regional Anesthesia » Volume 16
Systemic Ropivacaine Concentrations Following Local Infiltration Analgesia and Femoral Nerve Block in Older Patients Undergoing Total Knee Arthroplasty
Authors Kazune S ![]() , Nurka I, Zolmanis M, Paulausks A, Bandere D
, Nurka I, Zolmanis M, Paulausks A, Bandere D ![]()
Received 10 June 2023
Accepted for publication 31 August 2023
Published 15 September 2023 Volume 2023:16 Pages 143—151
DOI https://doi.org/10.2147/LRA.S425353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Sigita Kazune,1,2 Inga Nurka,2 Matiss Zolmanis,2 Arturs Paulausks,3,4 Dace Bandere4,5
1Department of Anesthesiology and Intensive Care, Riga Stradins University, Riga, Latvia; 2Department of Anesthesiology, Hospital of Traumatology and Orthopedics, Riga, Latvia; 3Laboratory of Finished Dosage Forms, Faculty of Pharmacy, Riga Stradins University, Riga, Latvia; 4Baltic Biomaterials Centre of Excellence, Headquarters at Riga Technical University, Riga, Latvia; 5Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Riga Stradins University, Riga, Latvia
Correspondence: Sigita Kazune, Department of Anesthesiology, Hospital of Traumatology and Orthopaedics, 22 Duntes Street, Riga, LV-1013, Latvia, Tel +371 67399221, Fax +371 67392348, Email [email protected]
Purpose: The study examined the pharmacokinetic profile of fixed formulation mixtures comprising 225 mg of ropivacaine for local infiltration analgesia with or without epinephrine, and femoral nerve block in older patients presenting for orthopedic surgery and explored potential influences of block type, age, and body weight on this profile.
Patients and Methods: Twenty four patients scheduled for total knee arthroplasty were randomly assigned to three groups: femoral nerve block, local infiltration analgesia with epinephrine and local infiltration analgesia without epinephrine. Blood samples were collected at 10, 30, 60, and 120 min following the block and total plasma concentrations of ropivacaine were quantified by high performance liquid chromatography.
Results: The mean individual peak total plasma concentrations of ropivacaine in local infiltration analgesia with and without epinephrine, and femoral nerve block group were 0.334, 0.490 and 0.545 μg mL− 1 (p = 0.16). Local infiltration with epinephrine group had significantly lower plasma ropivacaine concentrations at 30, 60 and 120 minutes. The plasma ropivacaine concentrations exceeded 2.2 μg mL− 1 in one patient. Age, but not body weight, had a moderate correlation with peak plasma ropivacaine concentration (r = 0.37, p = 0.08).
Conclusion: Administration of a fixed 225 mg dose of ropivacaine for local infiltration analgesia with epinephrine and femoral nerve block results in plasma ropivacaine concentrations below the toxicity threshold, indicating their safety. The use of local infiltration analgesia with epinephrine provides a greater safety margin, as local infiltration analgesia without epinephrine may lead to ropivacaine concentrations associated with symptoms of local anesthetic toxicity.
Keywords: arthroplasty, anesthetic techniques, regional, anesthetics local, ropivacaine, toxicity, local anesthetics
Introduction
Regional anesthetic techniques have been shown to significantly improve patient satisfaction and reduce postoperative complications after total knee arthroplasty (TKA).1–3 While femoral nerve block (FNB) provides excellent analgesia and requires less local anesthetic compared to periarticular infiltration, it is associated with quadriceps weakness that may lead to falls.4 Local infiltration analgesia (LIA) has the advantage of preserving motor power, but the impact of a large absorption surface in the postoperative wound and large volume of local anesthetic needed can lead to unpredictable systemic absorption.5 When performing regional blocks for TKA, ropivacaine, which is less cardiotoxic than bupivacaine, is the most commonly used local anesthetic. The use of a fixed formulation for all patients is common in daily practice,6 and the recommended maximum dose of 225 mg ropivacaine is frequently used.
While several studies have shown the safety of ropivacaine up to 800 mg in younger patients, it is important to consider the potential differences in pharmacokinetics when applied to different patient populations encountered in everyday practice.7,8 This is especially relevant for older individuals or those with different body composition. The majority of patients who undergo TKA are over 65 years old, mainly women, and have a high prevalence of obesity.7,9 All of these features may alter the absorption and distribution of ropivacaine from the injection site and thus affect ropivacaine plasma concentrations. Indeed, local anesthetic toxicity remains a rare but clinically relevant complication after regional anesthesia. Specifically, in patients undergoing knee replacement surgery and receiving peripheral nerve blocks symptoms consistent with life-threatening local anesthetic systemic toxicity (LAST) occur in 0.19% of cases.10
To address safety concerns, previous efforts have been made to investigate pharmacokinetic differences. Affas et al conducted a study comparing the systemic absorption and plasma concentrations of ropivacaine when utilizing two types of regional blocks for postoperative analgesia after TKA. However, comparing the peak ropivacaine concentrations between LIA and FNB groups in this study is challenging due to differing administration methods. The LIA group received a single dose of ropivacaine, while the FNB group received repeated small doses over a 24-hour period, resulting in variations in the timing and magnitude of peak concentrations.9
In order to ensure optimal dosing and safety, further research is needed to understand the pharmacokinetic characteristics of ropivacaine in various age groups and body compositions. Therefore, the aim of this study was to examine the pharmacokinetic profile of fixed formulation mixtures containing 225 mg of ropivacaine used in local infiltration analgesia (LIA) with or without epinephrine, as well as femoral nerve block (FNB) in older patients undergoing TKA, and to assess the proximity of the resultant plasma ropivacaine concentrations to the toxic threshold. Additionally, the study aimed to explore the potential impact of block type, age, and weight on this pharmacokinetic profile.
Materials and Methods
Study Design
This single-centre prospective randomized study was conducted in a tertiary orthopedic hospital from November 1, 2020, to October 31, 2021. The study was approved by the Hospital Ethics Committee (No. 37/2020). Written informed consent was obtained before surgery from all patients who participated in the study. Participation was voluntary and patients could withdraw at any point during the study.
Recruitment
Consecutive patients scheduled for unilateral total knee arthroplasty were evaluated for inclusion into the study. Inclusion criteria were age ≥65 years and ASA ≤ III. Patients were excluded from participation in the study in case of decreased kidney function (estimated glomerular filtration rate <30 mL/min), moderate or severe liver disease, hypersensitivity to local anesthetics or revision knee replacement.
The participating patients were randomly assigned to three groups: femoral nerve block group (group F), local infiltration analgesia with epinephrine (group LIA-A) and local infiltration analgesia without epinephrine (group LIA-B) using a computer-generated random sequence.
Procedure
In all groups, surgery was performed under spinal anesthesia with 15 mg of plain bupivacaine (3 mL, 5 mg/mL), and midazolam was administered for sedation if requested. Patients were operated with insertion of a cemented posterior stabilized prosthesis, using a standard medial parapatellar approach. A tourniquet was used, and no wound drains were left at the end of the operation. After the operation, the patients were transferred to the post-anesthesia care unit for monitoring and received multimodal analgesia, tranexamic acid, and thromboembolic prophylaxis according to local protocols.
In patients randomized to group F, a femoral nerve block was performed after spinal anesthesia. Under sterile conditions, the femoral nerve was visualized at the inguinal crease using a high-frequency ultrasound 13–16 MHz probe (M-Turbo, Sonosite, Bottle, WA, USA). A 50-mm 22G stimulating needle (Stimuplex A, B-Braun, BBraun, Melsungen, Germany) was connected to a nerve stimulator (Stimuplex HNS 12; BBraun, Melsungen, Germany) set up to deliver 0.5 mA and was inserted out-of-plane to the ultrasound probe. After fascia iliaca was pierced, the proximity to the femoral nerve was confirmed by quadriceps muscle contractions. After a negative blood aspiration test, 30 mL of 7.5 mg mL−1 ropivacaine (Ropivacaine B.Braun 7.5 mg mL−1) was injected (total dose 225 mg). The end of the injection of ropivacaine was considered as time zero (T0).
In both local infiltration analgesia groups (LIA-A, LIA-B) knee injections were performed in the same way by the orthopedic surgeon. The solution was injected sequentially; 20 mL was injected subcutaneously at the start of the operation, 50 mL was injected into the posterior capsule before cementation, and 80 mL was injected around the collateral ligaments. Patients randomized to group LIA-A periarticular infiltration was performed using 225 mg ropivacaine (0.15%; 150 mL) with epinephrine 5 μg mL−1 whereas group LIA-B received 225 mg (0.15%; 150 mL) ropivacaine. The time of tourniquet deflation was considered as time zero (T0).
Sampling and Analytical Methods
The baseline blood sample was taken at the time of peripheral venous catheterization prior to anesthesia. Blood samples for the evaluation of ropivacaine concentrations were obtained from a separate 16G peripheral venous catheter. Blood samples were collected in EDTA tubes (5 mL) at 10, 30, 60, and 120 min after time zero (T0). To avoid contamination of samples, the first 5 mL of blood drawn from the catheter were discarded at every sampling. Within 1 hour after sampling, the EDTA tubes were centrifuged at 3500 × g for 10 min to obtain blood plasma. The obtained plasma was stored at a temperature of −80°C until analysis.
To determine the total ropivacaine concentration, the plasma samples were thawed. 500 µL of plasma was added to a polypropylene tube along with 100 µL KOH 1 M and extracted with 4 mL of diethyl ether. After vortex mixing and centrifugation, the diethyl ether layer was transferred to a glass tube and evaporated to dryness at 40°C. The dry residue was reconstituted in high performance liquid chromatography (HPLC) mobile phase. HPLC analysis was performed on Thermo UltiMate 3000 HPLC-UV system (Thermo Fisher Scientific) equipped with an Ascentis C18 column (Supelco, Inc., Bellefonte, PA). The calibration was performed by spiking pooled blank patient plasma with diluted ropivacaine hydrochloride.
Demographic information from the patients was collected including age, sex, height, weight, and the American Society of Anesthesiologists (ASA) physical status.
Study Outcomes
The primary outcomes measured were peak total plasma ropivacaine concentrations (Cmax), the corresponding time to reach peak concentrations in plasma (tmax) and the area under the ropivacaine plasma concentration–time curve.
Sample Size
The selection of sample size for this study was driven by resource and ethical constraints. The study group was relatively homogenous, which allowed for the expectation of minimal inter-individual variation. A sample size of six subjects per group is consistent with established norms in pharmacokinetic research. To account for any potential attrition during the study’s duration, we chose to include a slightly larger sample size of eight subjects per group.
Statistical Analysis
Peak plasma concentrations (Cmax) and time to reach peak plasma concentrations (tmax) were obtained from the measured ropivacaine serum concentration–time curves. The area under the plasma concentration–time curve from time zero to the time of last blood sampling (AUC (0, t120)) was calculated using the linear trapezoidal rule. Data are presented as mean (standard deviation (SD)), 95% confidence interval or percentage. One-way analysis of variance (ANOVA) was performed to detect significant differences between groups, while the Fisher-Freeman-Halton test was utilized for categorical variables. Post hoc Tukey’s test was applied for multiple comparisons between groups.
The relationships between the peak plasma concentration of total ropivacaine, the time taken to reach the peak concentration, and the cumulative area under the curve at 120 minutes were analyzed using the Pearson correlation coefficient. Age and body weight were considered as potential predictors. P-values less than 0.05 were considered significant.
Data were analyzed using R Statistical Software (version 4.0.5, R foundation for Statistical Computing, Vienna, Austria).
Results
Ninety-seven patients were screened and 27 randomized to receive femoral nerve block (group F; n = 9), or infiltration with (group LIA-A; n = 9) or without epinephrine (group LIA-B; n = 9). It was not possible to draw blood from one patient in group LIA-A, making the measurement of plasma ropivacaine concentration impossible. In group LIA-B, one patient withdrew consent, and blood samples from another patient could not be analyzed due to a storage error. The number of patients included in the final analysis in each group and their demographic characteristics are shown in Table 1. Although patient characteristics did not differ between the three groups, 21 of the 24 patients recruited were women (87.5%), which is a higher proportion than reported in joint arthroplasty registries. Thirteen patients (54%) were obese (BMI ≥ 30 kg/m2).
 |
Table 1 Patient Characteristics |
Total plasma ropivacaine concentrations measured ranged from 0.03 to 2.57 μg mL −1. Median total plasma ropivacaine concentrations in the three groups over time are shown in Figure 1. One patient within group LIA-B showed large plasma concentrations of ropivacaine (ropivacaine: 2.57, 2.53 and 2.35 μg mL−1) without clinical signs of toxicity. Similarly, no other patients had symptoms of LAST. There was a significant difference in plasma ropivacaine concentrations between groups at 30, 60 and 120 minutes with group LIA-A having significantly lower concentrations than either group LIA-B (p = 0.01) or group F (p = 0.002). The systemic absorption of ropivacaine represented by the cumulative area under the curve at 120 min in group LIA-A was also significantly lower compared to both group LIA-B and F (0.183 vs 0.379 and 0.418 μg min mL −1, p = 0.04; Figure 2).
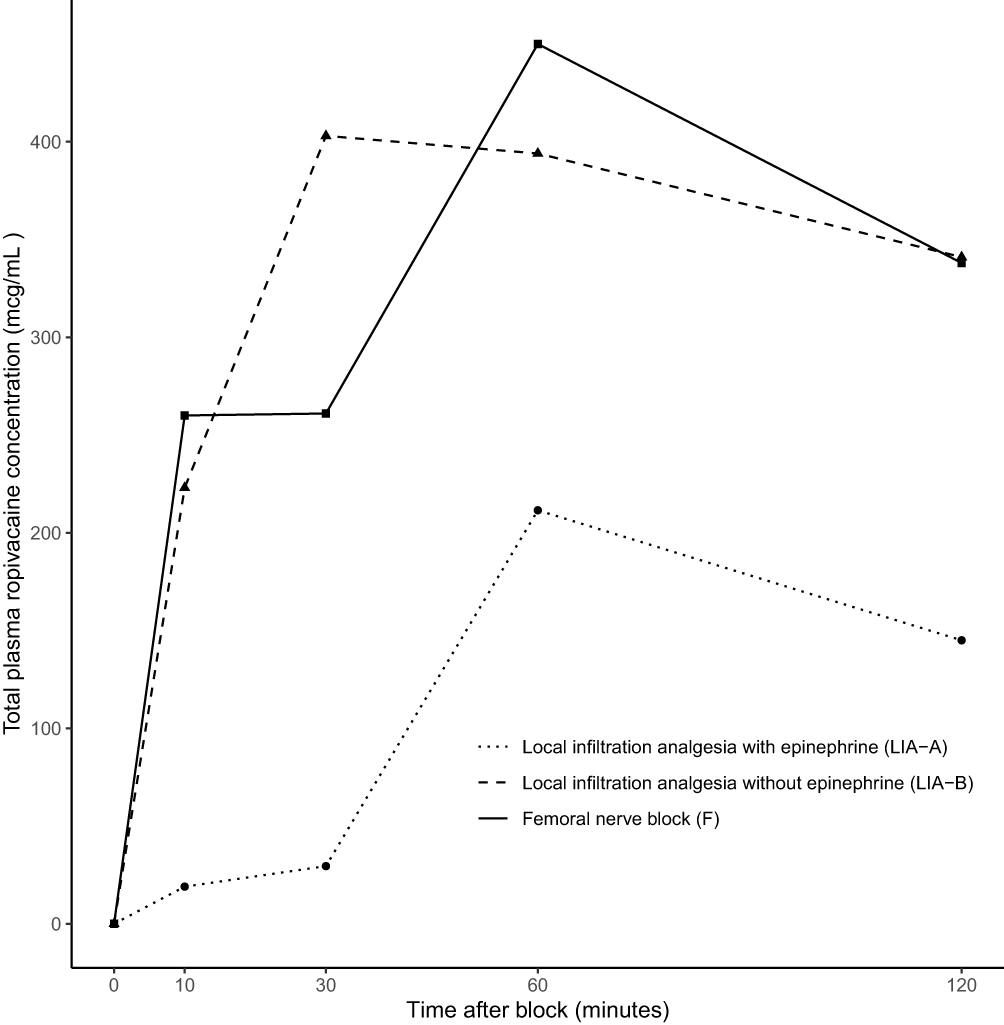 |
Figure 1 Mean total ropivacaine concentrations. |
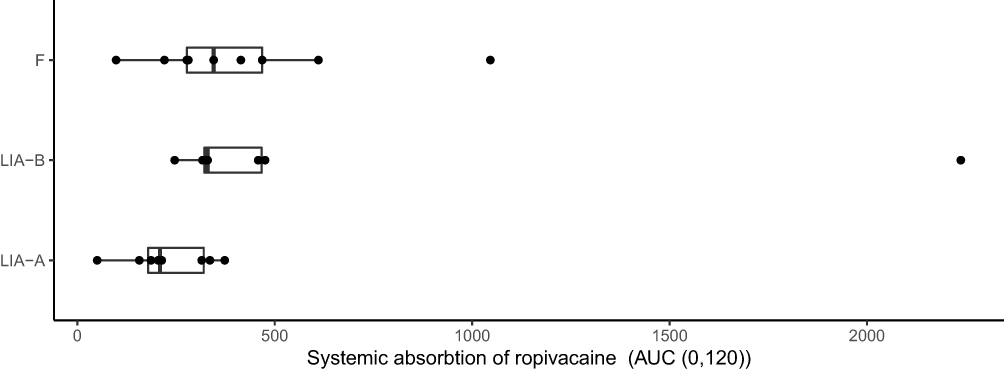 |
Figure 2 Area under the total ropivacaine concentration–time curve (AUC (0, t120)) in three groups: local infiltration analgesia with epinephrine (LIA-A), local infiltration analgesia without epinephrine (LIA-B), and femoral nerve block (F). Data are presented as median with first and third quartiles, outliers plotted as individual points. |
The mean individual peak plasma concentrations of total ropivacaine (Cmax) in groups LIA-A, LIA-B and F were 0.334 (95% CI 0.181–0.488), 0.490 (95% CI 0.395–0.584) and 0.545 (95% CI 0.309–0.782) μg mL −1 (p = 0.16). Although ropivacaine Cmax in group LIA-A was lower compared to the other groups, statistical significance was not reached, likely due to the limited sample size. The mean time to reach the maximum plasma concentration (tmax) was 36 minutes (95% CI 20–52) for group LIA-B, which was significantly shorter compared to 73 minutes (95% CI 37–108) for group LIA-A and 78 minutes (95% CI 45–111) for group F (p = 0.03).
The influence of individual patient characteristics (age, weight) on the peak plasma concentrations of ropivacaine, the time to reach it and the cumulative area under the curve at 120 minutes was assessed. It was found that age, but not weight, had a moderate positive correlation with both peak plasma concentration of ropivacaine (Pearson correlation coefficient R = 0.37, p = 0.08) and the time taken to reach it (Pearson correlation coefficient R = 0.33, p = 0.12). There was no significant effect of demographic variables on the cumulative area under the curve.
Discussion
This randomized study compared the systemic absorption of ropivacaine in three commonly used regional techniques: femoral nerve block and local infiltration analgesia with or without epinephrine using fixed formulation mixtures containing 225 mg of ropivacaine. Group LIA-A was found to have lower total plasma ropivacaine concentrations than either of the other two groups at 30, 60, and 120 minutes. However, caution must be exercised when inferring significant differences in peak plasma ropivacaine concentrations from these measurements due to a mismatch in the time at which the peak is reached. Group LIA-B demonstrated peak plasma concentrations at around 30 minutes, while the other two groups reached their peak concentrations at around 90 minutes. Although the study did not find significant differences in peak total plasma ropivacaine concentration between the three groups, it must be highlighted that the cumulative area under the curve at 120 minutes was significantly lower in Group LIA-A compared to both Groups LIA-B and F. Taking all these findings into consideration, Group LIA-A exhibited slower ropivacaine absorption and overall lower plasma ropivacaine concentrations. The small sample size may have contributed to the absence of a significant difference in peak total plasma ropivacaine concentrations between the groups.
Several other studies have reported the pharmacokinetics of similar doses of ropivacaine without adrenaline for lower extremity blocks. Hubler11 administered 150 mg of ropivacaine into the psoas compartment, resulting in individual peak total ropivacaine concentrations 0.422 to 1.249 μg mL −1. In the study by Affas the FNB group received 60 mg of ropivacaine after spinal anesthesia with repeated injections 4 hourly up to a total of 240 mg.9 Cmax was between 0.122 and 1.151 μg mL −1 observed 24 hours after initial injection. The concentrations reported by these studies are similar to those observed in group F of this study (0.303 to 1.157 μg mL −1). Zhang et al12 used 3.5 mg/kg of ropivacaine (mean dose 210 mg) to perform fascia iliaca block, and reported substantially higher Cmax of 2.17 ± 0.56 μg mL −1. In our study, the doses of ropivacaine ranged from 1.9 to 3.75 mg/kg, and only 4 patients received doses exceeding 3 mg/kg, so a lower Cmax would be expected.
In their studies, Koniuch et al observed Cmax of 0.23 to 0.75 μg mL −1 after using LIA mixture with 270 mg ropivacaine and Miller et al reported Cmax of 0.42 to 0.83 μg mL −1 after LIA using 300 mg ropivacaine with epinephrine.13,14 We found that infiltration 225 mg of ropivacaine with and without epinephrine resulted in a similar Cmax (range with adrenaline, 0.1–0.58 μg mL −1; range without epinephrine, 0.38 −0.65 μg mL −1).
Similar to our study, Affas et al compared the pharmacokinetic profile of 300 mg of ropivacaine used in LIA with epinephrine and FNB after TKA and found significant overlap between all groups. The peak plasma concentrations of ropivacaine ranged from 0.12 to 1.74 mg/mL.9 The similar Cmax achieved while using different doses and administration protocols and wide inter-individual variability mean that patient-related factors, such as age, weight and gender, play a significant role in ropivacaine pharmacokinetics after lower extremity blocks.
None of the patients in this study showed signs of cardiac or central nervous system toxicity. However, one patient in the IA-B group had Cmax levels of more than 2.2 μg mL −1. According to research in volunteers, this total venous plasma ropivacaine concentration value exceeds the threshold for neurotoxicity.15 The finding of an asymptomatic high Cmax is consistent with a number of studies in which ropivacaine doses of up to 800 mg have been used and Cmax of 3 μg mL −1 have been documented without adverse effects.7,16 On the other hand, 30% of published reported cases of local anesthetic toxicity are related to ropivacaine and several reports of LAST describe weight appropriate dosing.17,18 Elderly patients constitute a group at increased risk of LAST due to the high proportion of surgeries that involve regional anesthesia and patient-related factors can substantially influence pharmacokinetics. Although there is a general recommendation to calculate maximum safe ropivacaine doses according to weight, it is widely accepted that further personalization of ropivacaine doses could be needed.19,20
In our study, older patients had higher Cmax after injection of the same dose of ropivacaine regardless of weight. These results are partially supported by the results of other studies of ropivacaine pharmacokinetics in older patients. Miller et al investigated the pharmacokinetics of 300 mg of ropivacaine with epinephrine used for LIA and showed a positive correlation between patient age, female sex, and Cmax.14 Similarly, Gaudreault et al identified age as a covariate for the first-order absorption rate constant of ropivacaine in femoral nerve blocks.21 Analysis of hospitalization data for patients undergoing arthroplasty has also shown that patients older than 73 years are at increased risk of having LAST.22 These age-related effects on Cmax are probably explained by changes in tissue composition that lead to accelerated release of ropivacaine into the systemic circulation in elderly patients. The higher ropivacaine Cmax in female patients may be due to reduced activity of CYP1A2, the most important isozyme for the metabolism of ropivacaine.23
Previous studies have identified an effect of weight on ropivacaine Cmax.14,21 In contrast, our study found no significant correlation between weight and ropivacaine Cmax in the dose range 1.9 to 3.75 mg/kg. The reasons for this difference might be the longer blood sampling protocols (up to 96 h) in other studies. On the other hand, Cmax occurred between 60 and 90 minutes after tourniquet release, and ropivacaine concentration declined in all patients after this point.
Mean ropivacaine plasma concentrations were significantly lower when LIA containing epinephrine was used. This confirms findings from studies of other regional blocks that adding epinephrine to ropivacaine slows tissue uptake during the rapid absorption phase.24 Delaying ropivacaine absorption by addition of epinephrine could be a useful strategy to reduce the risk of systemic ropivacaine toxicity in patients at risk of LAST.
The strength of this study is the inclusion of patients within the age (65 to 89 years) and weight (60 to 121 kg) range of patients undergoing routine TKA and the use of fixed formulation mixture which is common in clinical practice.
There are three main limitations to this study. Firstly, the conclusions that can be reached from the results of our study are limited by the small number of patients. Secondly, there is a possibility that peak concentrations beyond 2 hours were missed. The decision to limit the sampling period to 120 minutes was based on existing literature, which indicated that the expected tmax occurs between 1 and 2 hours. Finally, although measuring unbound ropivacaine could have strengthened the results, the administration of a single bolus and the short sampling period suggest that significant changes in ropivacaine protein binding are unlikely to have occurred.25
Conclusion
This study shows that administration of a fixed dose of 225 mg of ropivacaine for local infiltration analgesia with epinephrine and femoral nerve block results in peak plasma ropivacaine concentrations that remain below the established toxicity threshold, indicating that these techniques are safe. However, the use of local infiltration analgesia with epinephrine offers a greater safety margin. While no clinical signs of toxicity were observed, local infiltration analgesia without epinephrine may produce ropivacaine plasma concentrations associated with symptoms of local anesthetic toxicity. The potential association between age and plasma concentrations of ropivacaine needs to be further investigated.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Scientific Research Ethics Committee of the Hospital of Traumatology and Orthopedics (26/23.02.2017). Informed consent was obtained from all the patients or their next of kin involved in the study.
Funding
The authors acknowledge support from the European Union’s Horizon 2020 research and innovation program under grant agreement No. 857287 (Baltic Biomaterials Centre of Excellence).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. 2008;33(6):510–517. doi:10.1097/00115550-200811000-00002
2. Duncan CM, Moeschler SM, Horlocker TT, Hanssen AD, Hebl JR, Self-Paired A. Comparison of Perioperative Outcomes Before and After Implementation of a Clinical Pathway in Patients Undergoing Total Knee Arthroplasty. Reg Anesth Pain Med. 2013;38(6):533. doi:10.1097/AAP.0000000000000014
3. Kelley TC, Adams MJ, Mulliken BD, Dalury DF. Efficacy of multimodal perioperative analgesia protocol with periarticular medication injection in total knee arthroplasty: a randomized, double-blinded study. J Arthroplasty. 2013;28(8):1274–1277. doi:10.1016/j.arth.2013.03.008
4. Kwofie MK, Shastri UD, Gadsden JC, et al. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med. 2013;38(4):321–325. doi:10.1097/AAP.0b013e318295df80
5. Wasudev G, Smith BE, Limbird TJ. Blood levels of bupivacaine after arthroscopy of the knee joint. Arthroscopy. 1990;6(1):40–42. doi:10.1016/0749-8063(90)90095-u
6. Albrecht E, Guyen O, Jacot-Guillarmod A, Kirkham KR. The analgesic efficacy of local infiltration analgesia vs femoral nerve block after total knee arthroplasty: a systematic review and meta-analysis. British Journal of Anaesthesia. 2016;116(5):597–609. doi:10.1093/bja/aew099
7. Gromov K, Grassin-Delyle S, Foss NB, et al. Population pharmacokinetics of ropivacaine used for local infiltration anaesthesia during primary total unilateral and simultaneous bilateral knee arthroplasty. Br J Anaesth. 2021;126(4):872–880. doi:10.1016/j.bja.2020.11.038
8. Brydone AS, Souvatzoglou R, Abbas M, Watson DG, McDonald DA, Gill AM. Ropivacaine plasma levels following high-dose local infiltration analgesia for total knee arthroplasty. Anaesthesia. 2015;70(7):784–790. doi:10.1111/anae.13017
9. Affas F, Stiller CO, Nygårds EB, Stephanson N, Wretenberg P, Olofsson C. A randomized study comparing plasma concentration of ropivacaine after local infiltration analgesia and femoral block in primary total knee arthroplasty. Scand J Pain. 2012;3(1):46–51. doi:10.1016/j.sjpain.2011.09.001
10. Mörwald EE, Zubizarreta N, Cozowicz C, Poeran J, Memtsoudis SG. Incidence of local anesthetic systemic toxicity in orthopedic patients receiving peripheral nerve blocks. Reg Anesth Pain Med. 2017;42(4):442–445. doi:10.1097/AAP.0000000000000544
11. Hübler M, Planitz MC, Vicent O. Early pharmacokinetic of ropivacaine without epinephrine after injection into the psoas compartment. Br J Anaesth. 2015;114(1):130–135. doi:10.1093/bja/aeu363
12. Zhang F, Lv C, Yang L, Wang S, Zhang M, Guo X. Pharmacokinetics of ropivacaine in elderly patients receiving fascia iliaca compartment block. Exp Ther Med. 2019;18(4):2648–2652. doi:10.3892/etm.2019.7838
13. Koniuch KL, Buys MJ, Campbell B, et al. Serum ropivacaine levels after local infiltration analgesia during total knee arthroplasty with and without adductor canal block. Reg Anesth Pain Med. 2019;44(4):478–482. doi:10.1136/rapm-2018-100043
14. Miller RJ, Cameron AJ, Dimech J, Orec RJ, Lightfoot NJ. Plasma Ropivacaine Concentrations Following Local Infiltration Analgesia in Total Knee Arthroplasty: a Pharmacokinetic Study to Determine Safety Following Fixed-Dose Administration. Reg Anesth Pain Med. 2018;43(4):347–351. doi:10.1097/AAP.0000000000000727
15. Knudsen K, Beckman Suurküla M, Blomberg S, Sjövall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997;78(5):507–514. doi:10.1093/bja/78.5.507
16. Bakker SMK, Fenten MGE, Touw DJ, et al. Pharmacokinetics of 400 mg locally infiltrated ropivacaine after total knee arthroplasty without perioperative tourniquet use. Reg Anesth Pain Med. 2018;43(7):699. doi:10.1097/AAP.0000000000000816
17. Vasques F, Behr AU, Weinberg G, Ori C, Di gregorio GA. Review of local anesthetic systemic toxicity cases since publication of the American Society of Regional Anesthesia recommendations: to whom it may concern. Reg Anesth Pain Med. 2015;40(6):698–705. doi:10.1097/AAP.0000000000000320
18. Waldinger R, Weinberg G, Gitman M. Local anesthetic toxicity in the geriatric population. Drugs Aging. 2020;37(1):1–9. doi:10.1007/s40266-019-00718-0
19. Williams DJ, Walker JD. A nomogram for calculating the maximum dose of local anaesthetic. Anaesthesia. 2014;69(8):847–853. doi:10.1111/anae.12679
20. Rosenberg PH, Veering BT, Urmey WF. Maximum recommended doses of local anesthetics: a multifactorial concept. Reg Anesth Pain Med. 2004;29(6):564–575. doi:10.1016/j.rapm.2004.08.003
21. Gaudreault F, Drolet P, Fallaha M, Varin F. A population pharmacokinetic model for the complex systemic absorption of ropivacaine after femoral nerve block in patients undergoing knee surgery. J Pharmacokinet Pharmacodyn. 2012;39(6):635–642. doi:10.1007/s10928-012-9275-z
22. Rubin DS, Matsumoto MM, Weinberg G, Roth S. Local Anesthetic Systemic Toxicity in Total Joint Arthroplasty: incidence and Risk Factors in the United States From the National Inpatient Sample 1998–2013. Reg Anesth Pain Med. 2018;43(2):131–137. doi:10.1097/AAP.0000000000000684
23. Ekström G, Gunnarsson UB. Ropivacaine, a new amide-type local anesthetic agent, is metabolized by cytochromes P450 1A and 3A in human liver microsomes. Drug Metab Dispos. 1996;24(9):955–961.
24. Karmakar MK, Ho AMH, Law BK, Wong ASY, Shafer SL, Gin T. Arterial and venous pharmacokinetics of ropivacaine with and without epinephrine after thoracic paravertebral block. Anesthesiology. 2005;103(4):704–711. doi:10.1097/00000542-200510000-00008
25. Scott DA, Emanuelsson B-M, Mooney PH, Cook RJ, Junestrand C. Pharmacokinetics and efficacy of long-term epidural ropivacaine infusion for postoperative analgesia. Anesthesia & Analgesia. 1997;85(6):1322–1330. doi:10.1213/00000539-199712000-00026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.