Back to Journals » International Journal of Women's Health » Volume 14
Systemic Lupus Erythematosus Management in Pregnancy
Received 15 November 2021
Accepted for publication 19 January 2022
Published 15 February 2022 Volume 2022:14 Pages 199—211
DOI https://doi.org/10.2147/IJWH.S282604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Kathryn H Dao, Bonnie L Bermas
Division of Rheumatic Diseases, UTSouthwestern Medical Center, Dallas, TX, USA
Correspondence: Kathryn H Dao, Email [email protected]
Abstract: Systemic lupus erythematosus (SLE) affects reproductive aged women. Issues regarding family planning are an important part of SLE patient care. Women with SLE can flare during pregnancy, in particular those who have active disease at conception or prior history of renal disease. These flares can lead to increased adverse pregnancy outcomes including fetal loss, pre-eclampsia, preterm birth and small for gestational aged infants. In addition, women with antiphospholipid antibodies can have thrombosis during pregnancy or higher rates of fetal loss. Women who have anti-Ro/SSA and anti-La/SSB antibodies need special monitoring as their offspring are at risk for congenital complete heart block and neonatal lupus. Ideally, SLE patients should have their disease under good control on medications compatible with pregnancy prior to conception. All patients with SLE should remain on hydroxychloroquine unless contraindicated. We recommend the addition of 81mg/d of aspirin at the end of the first trimester to reduce the risk of pre-eclampsia. The immunosuppressive azathioprine, tacrolimus and cyclosporine are compatible with pregnancy and lactation, mycophenolate mofetil (MMF)/mycophenolic acid are not. Providers should use glucocorticoids at the lowest possible dose. Methotrexate, leflunomide and cyclophosphamide are contraindicated in pregnancy and lactation. SLE patients on the biologics rituximab, belimumab and abatacept can continue these medications until conception and resume during lactation.
Keywords: systemic lupus erythematosus, fertility, pregnancy, medications
Introduction
Systemic lupus erythematosus (SLE) is a multi-organ system disorder that predominantly affects reproductive aged women. As such, issues regarding fertility and pregnancy are an important part of SLE patient care. SLE pregnancies are associated with increased incidence of disease flares as well as adverse pregnancy outcomes (Table 1). Previously, these factors combined with limited knowledge regarding medication compatibility with pregnancy led many clinicians to dissuade their SLE patients from pursuing pregnancy. However, over the past several decades, a better understanding of SLE disease course and management during pregnancy has improved maternal and fetal outcomes. In this review, we will discuss SLE management during conception, through pregnancy and the post-partum period.
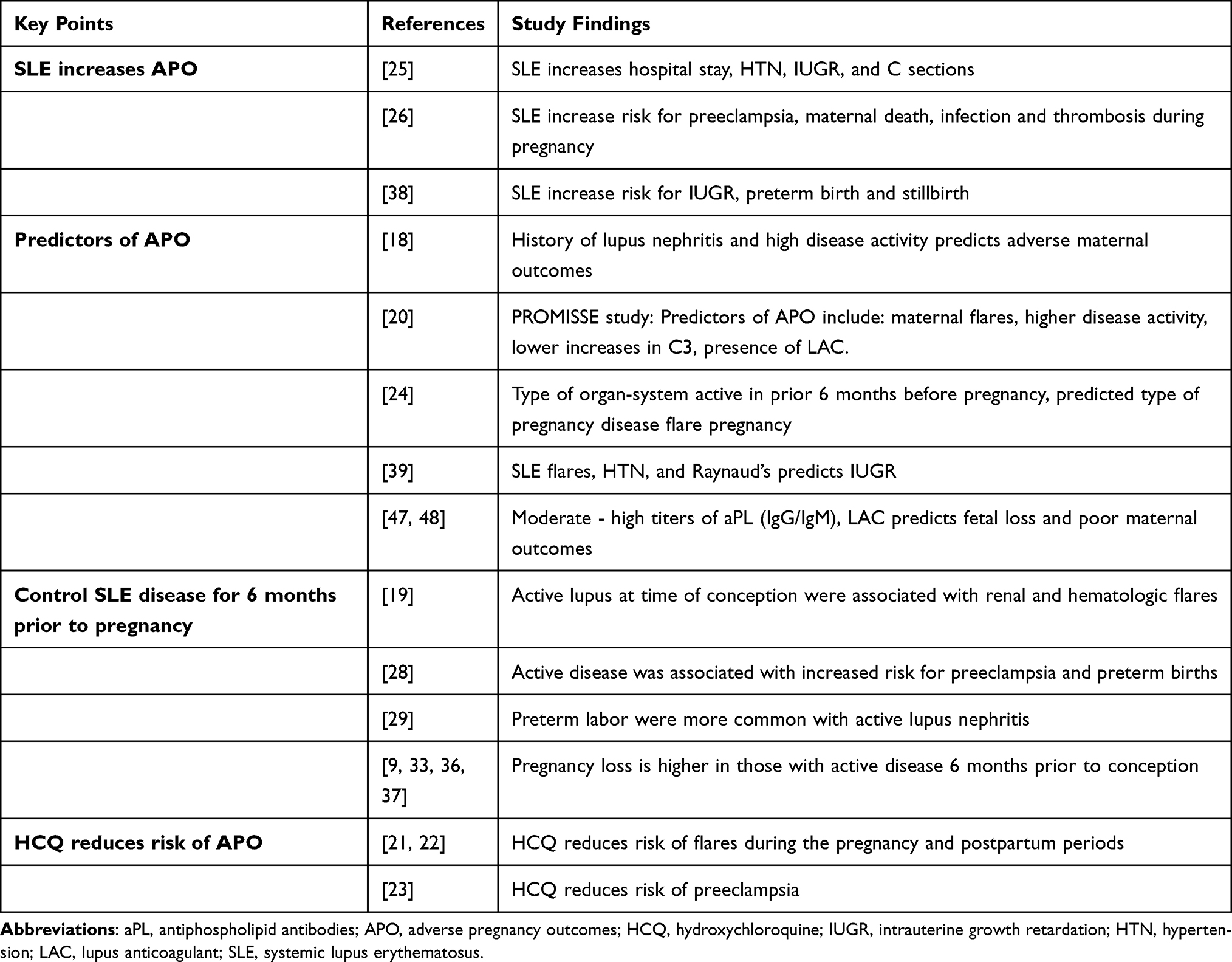 |
Table 1 Study Findings in SLE Pregnancy |
Overview of SLE
SLE is a chronic disease characterized by autoreactive T and B cells leading to pathogenic autoantibodies and immune complex deposition resulting in tissue damage.1 Diagnosing SLE can be challenging as the disease often develops slowly and evolves over time.2 Moreover, many organ symptoms can be involved including the skin, the musculoskeletal, pulmonary, cardiovascular, hematologic, renal and nervous systems. The vast majority of patients will have a positive anti-nuclear antibody and often have other autoantibodies. Diagnosis requires the presence of an ANA, and the presence of other autoantibodies and/or clinical manifestations.3 Epidemiologic studies estimate the prevalence of SLE is between 45.2 and 102.9 per 100,000 with an incidence of 2.4–7.2 per 100,000/year.4,5 The highest incidence of SLE is seen in women, peaking during their reproductive years with a female to male prevalence ratio of 7–9:1.6,7 The X chromosome and sex hormones may be responsible for the uptick in incidence among women as these have been associated with immune dysregulation. Candidate risk genes for SLE have been discovered on the X chromosome (eg, Foxp3, TLR7, IRAK1, and CD40 ligand), and estrogens have effects on B cell maturation, antibody production, Th2 responses, and survival of autoreactive cells.7 Thus, it is not surprising that pregnancy can impact SLE disease activity, and conversely SLE can impact pregnancy outcomes.
Reproductive Potential
SLE affects fecundity (probability of conception/reproduction) and fertility (reproductive capacity). Several factors impact the number of offspring in patients with SLE, including active inflammatory disease, comorbidities (eg, renal insufficiency, lupus nephritis, and anti-phospholipid syndrome), exposure to gonadotoxic treatments, advanced maternal age, psychosocial aspects and pregnancy loss (discussed below).8–10 Lupus activity, even mild, can cause oophoritis and interrupt the hypothalamic pituitary ovarian axis.11 Flares also have been associated with hyperprolactinemia, affecting the ovulation process.12 Patients may present with amenorrhea and menstrual irregularity. Pasoto et al reported 53% of SLE patients under 40 years of age had menstrual alterations, and patients with high disease activity were more likely to endorse irregular menses.13 Anti-Mullerian hormone (AMH) levels and antral follicular count (AFC) are predictors of ovarian reserve; a reduction in levels may indicate impaired fertility. Cohort studies have found AMH and AFC levels in SLE patients were significantly lower compared to age-matched healthy controls even in those with normal menstruation.13,14
Cyclophosphamide (CYC) is an alkylating agent used in the treatment of severe manifestations of SLE (eg, class III/IV lupus nephritis, severe neurological inflammation, pulmonary alveolitis/hemorrhage). This medication can directly damage oocytes,15 however, gonadotropin-releasing hormone agonists can mitigate this toxicity.16 Women previously treated with CYC experienced greater rates of amenorrhea and early menopause. Ovarian insufficiency is more likely with age (over 30) and cumulative doses greater than 10 grams.17
Disease Activity During Pregnancy
Several studies have shown that active disease at the time of conception correlates with disease flares during pregnancy. A study of 55 pregnancies in 39 women with SLE recorded clinical and laboratory data regularly six months prior to pregnancy through the first year post-partum. In this study, history of nephritis and high disease activity, as measured by the SLE Disease Activity Index (SLEDAI), predicted adverse maternal outcome during pregnancy.18 In another study of 155 patients with lupus who became pregnant, active lupus at the time of conception was associated with renal and hematologic flares. In this cohort, 6.1% of women with active disease during pregnancy died and 15.9% developed organ failure; in addition, hypocomplementemia and anti-dsDNA at the time of conception were also associated with disease flares.19 In the prospective study, Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Antibody Syndrome and Systemic Lupus Erythematosus (PROMISSE), fewer than 10% of 318 patients with mild –moderate disease during the first trimester of pregnancy had mild flares and only 3% had severe flares.20 Several studies have shown that continuation of hydroxychloroquine during pregnancy reduces the risk of flare during pregnancy and in the post-partum period.21,22 Moreover, in a study of 316 lupus pregnancies, hydroxychloroquine reduced the risk of preeclampsia.23
Not only does disease activity in the six months preceding conception predict flare, but also the type of organ involvement in the pre-conception period predicts the type of disease flare during pregnancy. Tedeschi et al showed that the organ-system that was active in the six months prior to conception predicted the organ system involved in a pregnancy disease flare. Thus, women with hematologic manifestations prior to conception tended to have hematologic manifestations during pregnancy.24
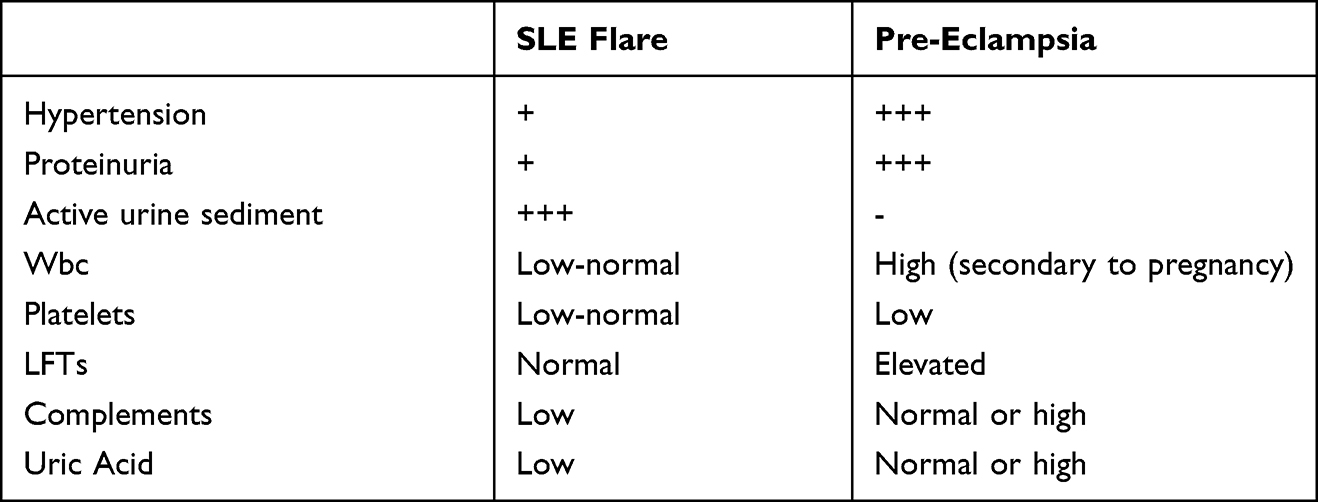 |
Table 2 Differentiating SLE Flare from Pre-Eclampsia |
Pregnancy Outcomes
Women with SLE have more adverse pregnancy outcomes than control women. In a study of the nationwide inpatient sample that included 4000 SLE pregnancies, lupus pregnancies had longer hospital lengths of stay, increased hypertension, higher rates of intrauterine growth restriction (IUGR) and C-section rate.25 The latter finding is driven by both provider and patient preference and may not reflect a medical indication. In a subsequent study using the same database but expanded years, there was a three-fold increased risk of pre-eclampsia, a 20-fold increase in maternal death, and increased rate of infections and thrombosis among SLE patients.26 More recent data has shown improvement in maternal mortality and fetal death rates, although rates are still higher than in the control population. The incidence of cesarean section rates and pre-eclampsia continues to remain higher in SLE pregnancies and have not significantly changed over time.27 In the aforementioned PROMISSE study, 19% of patients had adverse pregnancy outcomes including fetal loss after 12 weeks, neonatal death, preterm delivery and small for gestational aged infants. Baseline predictors include the presence of a lupus anticoagulant (OR 8.32, 95% CI 3.59–19.26), antihypertensive use (OR 7.05, 95% CI: 3.05–16.31), physician global assessment >1 (OR 4.02, 95% CI 1.84–8.82), thrombocytopenia (OR 1.33 per 50K decrease, 95% CI 1.09–1.63), maternal flares, higher disease activity and lower increases in C3 later in pregnancy.20 The Medical Birth Registry of Norway reported outcomes of births in women with SLE and concluded active disease was associated with increased risk for preeclampsia (OR 5.33 compared to population controls, OR 3.38 compared to inactive disease) and preterm births (OR 8.66 compared to population controls, OR 3.36 compared to inactive disease.28 A study of maternal and fetal outcomes over 3 decades by the Mayo clinic found that patients with active lupus nephritis compared to those who had quiescent disease had higher incidence of maternal complications (57% vs 11%, p < 0.001). Women with active nephritis were more likely to deliver preterm (median 34 weeks vs 40 weeks p = 0.002) and to have fetal loss (35% vs 9%, p = 0.031).29
Preeclampsia versus Lupus Flare
One of the most challenging clinical conundrums is differentiating SLE flare from pre-eclampsia. This is particularly so because up to 20% of lupus pregnancies are complicated by pre-eclampsia. This differentiation is not merely academic as pre-eclampsia is treated with immediate delivery whereas lupus flare is managed with immunosuppression. While both conditions can present with hypertension and proteinuria, urinalysis in pre-eclampsia is less likely to reveal an active sediment than in SLE flare. Thrombocytopenia is common to both but elevations of liver function tests are more suggestive of pre-eclampsia. In lupus flares, lower white blood cell counts, complement levels, and uric acid are seen than in pre-eclampsia.30,31 (Table 2)
Fetal Outcomes
Fetal Loss
Previously, fetal loss in SLE pregnancies was as high as 43%. This rate declined to 17% in 2002.32,33 In a cross-sectional study of 356 SLE pregnancies, SLE pregnancies were more than twice as likely to end in fetal death than non-SLE pregnancies.34, Another study of 148 lupus pregnancies compared to 78,905 non-lupus pregnancies found the rate of stillbirth was higher with lupus (OR 4.84 [CI, 1.72,11.08]) and associated with severe maternal disease).35 Risk factors for pregnancy loss include: the presence of antiphospholipid antibodies (aPL), lupus nephritis, renal insufficiency, and increased lupus activity in the 6 months preceding or during pregnancy.9,33,36,37
Fetal Complications
One study from Taiwan of 2059 SLE offspring reported higher rates of intrauterine growth restriction, preterm birth and stillbirth.38 Similarly, an Italian group reported higher risk of preterm delivery and small for gestational aged infants in their SLE cohort.39 This group also found SLE pregnancies were more likely to end in preterm delivery, particularly in patients with a history of lupus nephritis and hypertension. Intrauterine growth restriction was associated with hypertension, Raynaud’s, and disease flares.
Neonatal Lupus
Approximately one-third of women with SLE will have anti-Ro/SSA and anti-La/SSB antibodies. In 10% of offspring of pregnant women with these antibodies, neonatal lupus can occur (NL). Neonatal lupus consists of cutaneous or cardiac manifestations. In cutaneous neonatal lupus, the infant has a photosensitive rash and can have elevated liver function tests. These findings disappear after six months of life. In 1–2% fetuses of mothers with anti-Ro and anti-La antibodies, congenital complete heart block (CCHB) can occur. This incidence increases to 17% if the mother has had a previous child with CCHB.40 Congenital complete heart block can lead to fetal death in 17.5% of affected fetuses most occurring before the 30th week of gestation. While no formal guidelines exist for monitoring for the development of heart block, professional societies recommend serial fetal echocardiography between 16 weeks and 26 weeks of gestation.41 Data suggest hydroxychloroquine administration during pregnancy in anti-Ro and anti-La positive mothers can reduce the reoccurrence rate of CCHB.42
Long–Term Outcome
The literature regarding long-term outcome of children of women with lupus is conflicting with some groups reporting increased usage of special educational services by children born to mothers with SLE and aPLs43 while others found that while maternal SLE is a risk factor for pre-term birth it is not a risk factor for neurological disease in children born to SLE mothers.44
Management
Patients with SLE can and do have successful pregnancies. Pregnancy outcomes are better when there is planning and close monitoring of the patient during this process.The American College of Rheumatology (ACR) published evidence-based guidelines detailing a roadmap to optimize maternal and fetal outcomes in patients with rheumatic diseases.41 A multidisciplinary team approach with close rheumatologic, obstetric, and neonatal monitoring is important from preconception to parturition. Box 1 lists good clinical practices (GCPs) for pregnancy planning for patients with SLE.
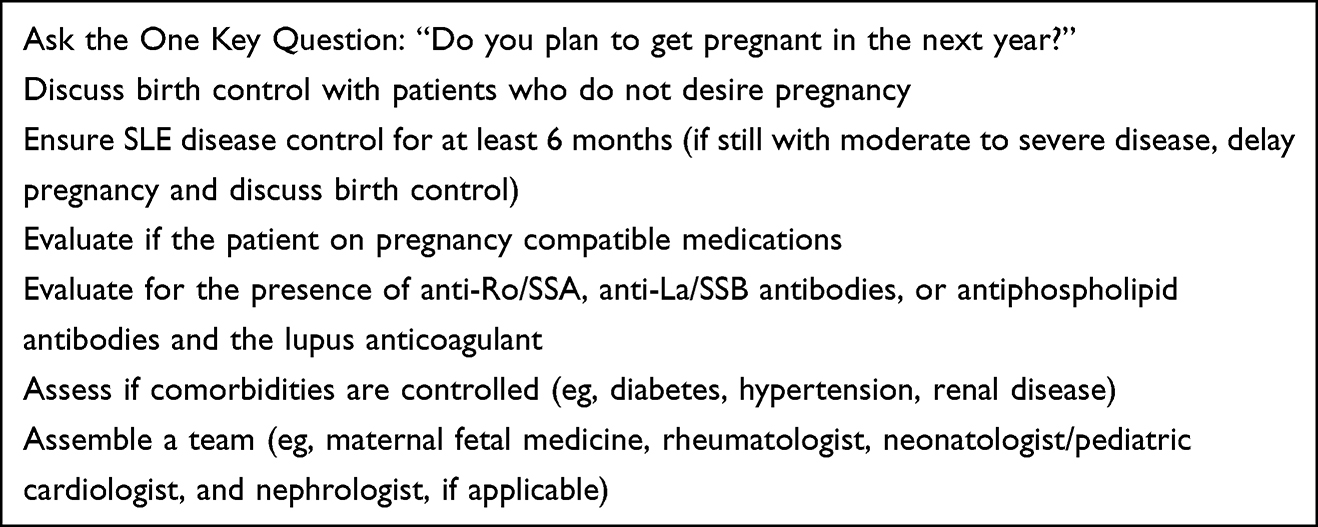 |
Box 1 Preconception Counseling: The Checklist |
Pre-Pregnancy Screening and Contraception
A planned pregnancy is important to allow time to optimize treatment and tighten disease control. End-organ damage may be a contraindication to pregnancy; examples include severe pulmonary hypertension, pulmonary fibrosis, cardiomyopathy, valvular dysfunction, severe renal insufficiency, or end stage renal disease, history of major strokes or catastrophic antiphospholipid syndrome.45,46 Patients with these conditions should avoid pregnancy. Additionally, pre-conceptual counseling will reduce risk of exposure to teratogenic medications, disease flares, and adverse pregnancy outcomes (APOs). An important part of pre-conception counseling is to ascertain the patient’s pregnancy plans. One easy way to incorporate this into clinical practice is to ask “Would you like to become pregnant in the next year?.”47 If the patient wants to avoid pregnancy, refer the patient for effective Contraception.
Preconceptual Risk Assessment
In patients desiring pregnancy, remission or low lupus disease activity state (LLDAS) is the goal before pregnancy is attempted. Active disease status will increase the risk of poor outcomes to mother and baby. Hence, to minimize risk for APOs, patients should be in LLDAS or remission for 6 months before trying to conceive on medications compatible with pregnancy. Those with moderate or severe disease activity should delay pregnancy until the disease is controlled on stable, pregnancy-compatible medications.
Biomarkers Predictive of Pregnancy Outcomes
Women with SLE anticipating pregnancy should be tested for the presence of anti-Ro/SSA, anti-La/SSB and antiphospholipid antibodies (eg, anticardiolipin IgG and IgM, b2-glycoprotein-I IgG and IgM, and the lupus anticoagulant (LAC)); these antibodies portend serious complications during pregnancy. Moderate and high titers of antiphospholipid antibodies in combination with the LAC confers the highest risk for poor fetal and maternal outcomes.47,49
Pregnancy Monitoring
Lupus pregnancies are high-risk pregnancies. A collaborative approach to monitoring the pregnant patient is essential; the team should comprise a rheumatologist, maternal fetal medicine specialist (also known as “high-risk OB”), and if applicable, a nephrologist and pediatric cardiologist. The patient should have regular assessments during pregnancy to identify potential complications and receive early intervention. Physiological pregnancy changes may resemble SLE disease activity, including arthralgias, fatigue, rashes, and swelling. Laboratory changes also occur during a healthy pregnancy. Distinguishing which changes are physiological versus pathological may be difficult, but understanding normal pregnancy physiology is essential.
Pregnancy will cause significant anatomical and physiological transformations affecting every organ system.50 Plasma volume expands by 50% and is proportional to the baby’s birthweight. With the expansion of volume cardiac output will increase by 40% during normal pregnancy Cardiac murmurs will be more evident and peripheral edema and pulmonary edema can occur. Renal changes also result from increased blood flow. A pregnant woman’s glomerular filtration rate (GFR) is increased by 50–85%.51 This in turn increases the fractional excretion of protein and uric acid.
Hemoglobin and platelet levels decrease in a normal pregnancy, while the erythrocyte sedimentation rate (ESR) increases. A study of more than 1000 healthy pregnant women found the ESR doubles in the second half of pregnancy from 18–48 mm/h to 30–70 mm/h; gestational age along with hemoglobin concentration will affect ESR levels.52 In contrast, C-reactive protein (CRP) levels do not rise during pregnancy; if elevated, this more likely indicates disease flare or infection. Hypercoagulability occurs in normal pregnancy; this is related to an increase of factor VIII, IX, X and fibrinogen; however, concentrations of anticoagulants, anti-thrombin and protein S are decreased contributing to thrombosis risk. This hypercoagulable state will persist from the first trimester to at least 6–12 weeks following parturition.50 Additionally, complements will rise in a healthy pregnancy; they are important in host defenses against infection and for clearing apoptotic and necrotic cells. Elevated levels of C4, C3 and activation products C4d, C3a, and SC5b-9 are common in pregnancy; however, dysregulation of the complement system can cause preeclampsia and fetal loss.53 Complement activation, likewise, is an important focus for lupus disease activity. While levels may be low in some patients with active SLE, complements can be unreliable as a biomarker of disease activity.54 Finally, physiological maternal glucose alterations occur as the pregnancy progresses to deliver glucose to the fetus and support maternal metabolism. This diabetogenic state begins in the second trimester as maternal insulin resistance peaks in the third trimester.55 Close monitoring of SLE patients who are on chronic corticosteroids is essential to evaluate for gestational diabetes. Below we discuss SLE patient monitoring by trimester (Table 3).
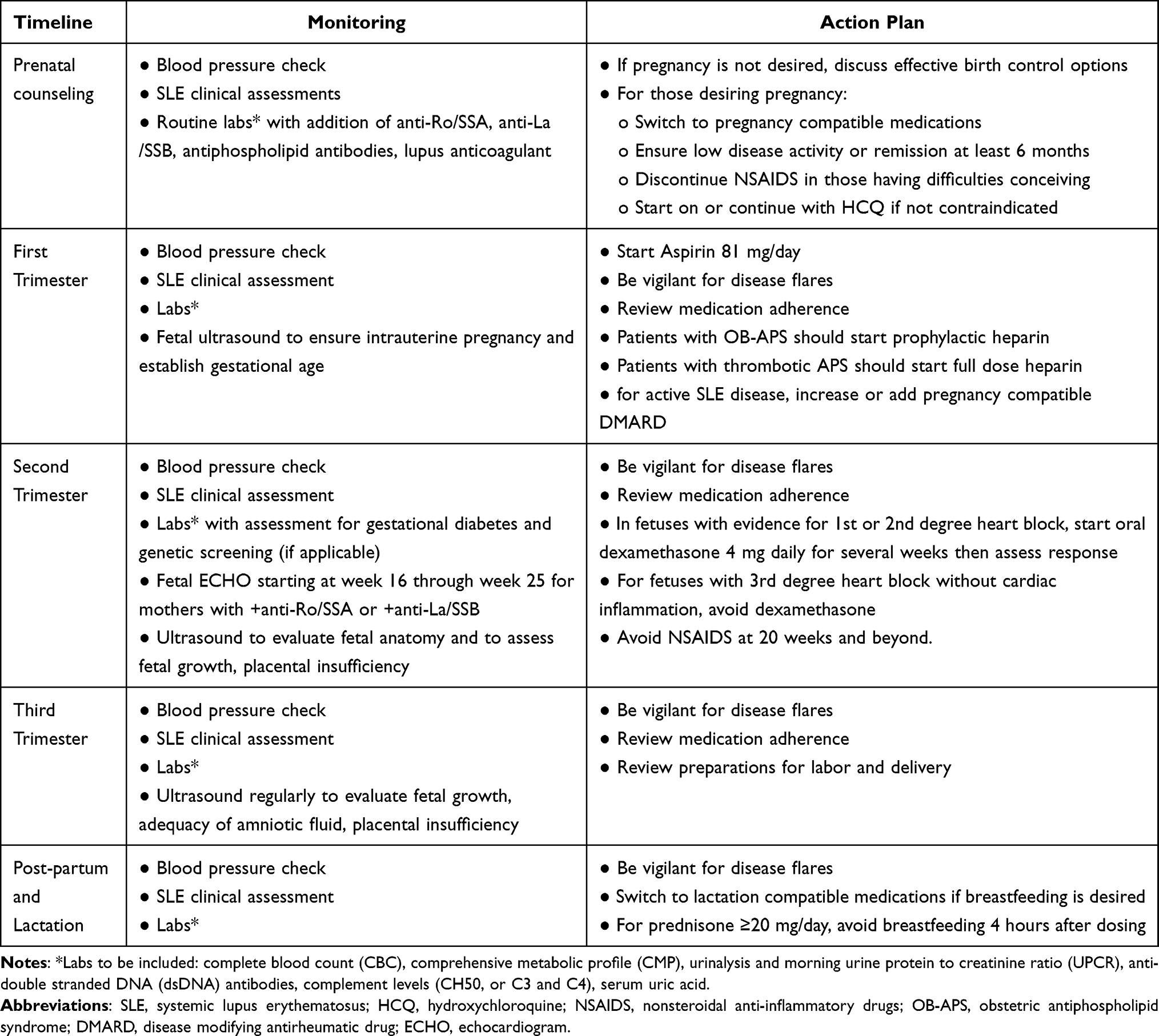 |
Table 3 Pregnancy Management |
First Trimester
Common complaints in the first trimester of a normal pregnancy will include fatigue, weight gain, nausea, and urinary frequency. At each prenatal visit, the provider should complete a careful review of systems and physical exam with blood pressure monitoring for evidence of SLE disease activity. We recommend that patients do home blood pressure monitoring as well. Practitioners familiar with validated disease measurement tools (eg, systemic lupus erythematosus disease activity index (SLEDAI, British Isles Lupus Assessment Group (BILAG)) should consider incorporating these to assess disease activity. Laboratory assessments for medication toxicity and disease activity at least once a trimester should include: a complete blood count with differential, comprehensive metabolic panel, C3, C4, double-stranded DNA, serum uric acid, urinalysis with microscopy, and a urine protein to creatinine ratio (UPCR). All patients should be on hydroxychloroquine (HCQ) unless contraindicated. Low dose aspirin (81mg/day) should be initiated early in pregnancy to reduce the risk for preeclampsia56 In patients with known obstetric antiphospholipid syndrome (OB-APS), prophylactic heparin or low dose molecular weight heparin in combination with low dose aspirin is indicated to prevent fetal loss and thromboses; anticoagulation should be continued 6 to 12 weeks post-partum. Those patients with known thrombotic APS (T-APS) should receive therapeutic doses of heparin or low molecular weight heparin with low dose aspirin.44 Frequency of follow-up will depend on the clinical status of the patient and at the provider’s discretion. The provider and/or patient should inform their obstetrician of the pregnancy. Importantly, an early fetal ultrasound to confirm an intrauterine pregnancy and to establish fetal age is crucial.
Second Trimester
Anti-Ro/SSA (in particular, anti-Ro 52 or 60 kDa) and/or anti-La/SSB antibodies may cross the placenta in the second trimester and cause neonatal cutaneous lupus or CCHB.57,58 Pregnant patients with these antibodies should undergo serial fetal echocardiography by an experienced pediatric cardiologist or a maternal fetal medicine specialist starting at the 16th week of gestation to evaluate for cardiac conduction abnormalities as the vulnerable period is between 17 and 25 weeks gestation. First-, second-, and third-degree heart block may occur, but third-degree or CCHB is a permanent condition that carries significant morbidity and mortality; infants with CCHB often require permanent pacemakers.57,58 In mothers who have had a previous infant with CCHB or cutaneous neonatal lupus, consider monitoring with weekly fetal echocardiography. When a fetus presents with first or second-degree heart block, the ACR Reproductive Health Guidelines conditionally recommends that the anti-Ro/SSA and/or anti-La/SSB mother take oral dexamethasone 4 mg daily for several weeks.44 We do not recommend dexamethasone in situations of third degree heart block without evidence for cardiac inflammation as it does not reverse the conduction abnormality. In contrast to CCHB, cutaneous neonatal lupus is typically transient; affected infants may present with a rash, abnormal liver enzymes or hematologic abnormalities. Hydroxychloroquine continued during pregnancy will reduce the risk of CCHB and NLE.
Lupus flares may occur during pregnancy. For mild flares with arthralgias or myalgias, acetaminophen, topical pain creams and oral NSAIDs may be used, but at 20 weeks or later, nonsteroidal anti-inflammatory drugs (NSAIDS) should be discouraged. In instances where NSAIDS cannot be used or if the flare is more severe, pregnancy compatible disease modifying anti-rheumatic medications (DMARDS) should be added to hydroxychloroquine (see medications below). Keep prednisone at the lowest effective dose due to risk for mood changes, insomnia, infection, pregnancy-induced diabetes, macrosomia, adrenal insufficiency, and preterm delivery. During this trimester, it is necessary to remain vigilant for lupus disease activity that may not be clinically evident but can reveal itself on routine laboratory assessments. Continue to screen patients for evidence of active lupus nephritis, preeclampsia, and diabetes with blood work; assess fetal growth and anatomy, amniotic fluid level with fetal sonography. When there is a concern for placental integrity, fetal and uterine arteries with Doppler sonography should be performed.56
Third Trimester
Similar assessments should be conducted in the third trimester. Evaluate for pre-eclampsia or SLE flare regular or intrauterine growth restriction; Doppler sonography should continue at regular intervals. Mode and time of delivery will be determined by fetal and maternal conditions.
Postpartum
Mothers are at increased risk for thrombosis and disease flares during the postpartum period.59 Those who have APS should remain on anticoagulation for at least 6–12 weeks after parturition.56 Postpartum depression can be common and might be mistaken for neuropsychiatric lupus. Many medications used for SLE disease during pregnancy can be continued during lactation (see below). In mothers with anti-Ro/SSA or anti-La/SSB, observe for cutaneous lesions in the neonate; cutaneous NL may occur a few weeks after birth and can resolve spontaneously after weeks or months. These rashes are photosensitive; sun protection will help the rash resolve faster.58
Co-Existing Antiphospholipid Syndrome
Antiphospholipid syndrome (APS) is characterized as recurrent venous or arterial thromboses and pregnancy morbidity in the setting of aPL. About 29–46% of patients with SLE have evidence of aPL, but only 5–8% develop thrombotic or pregnancy complications (eg, fetal loss, preeclampsia/eclampsia, small for gestational age).60,61 The revised classification criteria for APS defines vascular manifestations and obstetric complications; APS can occur by itself or in the setting of SLE. Thrombotic APS (T-APS) is defined by: one or more episodes of arterial, venous, or small vessel thrombosis in any tissue or organ, while obstetric APS is defined by: 1. three or more consecutive spontaneous abortions before 10 weeks of gestation, 2. one or more unexplained fetal loss beyond 10 weeks of gestation, or 3. one or more premature births of a morphologically normal neonate before 34 weeks of gestation due to eclampsia or preeclampsia.62 The presence of aPL must occur on two or more occasions, separated by at least 12 weeks. Compared to other aPL, the lupus anticoagulant confers the highest risk for APO RR 12.15 (95% CI 2.92–50.54, p = 0.0006) Risk stratification and management of APS during pregnancy depends on prior thrombotic or obstetric complications.44,56 The ACR Reproductive Health Guidelines indicate prophylactic therapy is not indicated to prevent pregnancy loss for healthy, non-SLE patients with aPL but no prior history of thrombosis or pregnancy complications; however, aspirin 81–100 mg daily is conditionally recommended by the ACR Reproductive Health guidelines. We recommend, low dose aspirin with prophylactic doses of heparin (usually low molecular weight heparin) in women with obstetric APS. Continue anticoagulation for 6–12 weeks postpartum, as this is a vulnerable period for clotting. Pregnant women with T-APS should be prescribed aspirin and therapeutic dose heparin throughout pregnancy and postpartum. HCQ may help reduce the risk for thrombosis and APS-related poor outcomes. There is not enough evidence to show that prednisone, intravenous immunoglobulin, or higher doses of heparin will help APS-related outcomes.
Medications
Medication management during pregnancy must take into account any potential risk to the developing fetus (Table 4). Hydroxychloroquine is considered compatible with pregnancy.44 Reassuringly, studies of neonates exposed to hydroxychloroquine in utero have not shown retinal toxicity or prolongation of neonatal QTc intervals.63,64 Recently, there was a report of increased risk of fetal anomalies in infants exposed to hydroxychloroquine in utero; however, confounders such as alcohol, smoking, and other drugs were not assessed.65 Importantly, no particular pattern of anomaly was found, the latter being a tenet of proof of teratogenicity.66 Several studies have demonstrated that continuation of hydroxychloroquine during pregnancy decreases disease flares and reduces the risk of pre-eclampsia.21 However, claims data demonstrate that overall 16.1% of women who have lupus are filling prescriptions during pregnancy.67 Slightly higher results were found among those in Sweden, with 36% of SLE dispensed hydroxychloroquine during pregnancy.68 Given this, we emphasize to our patients the importance of staying on hydroxychloroquine during pregnancy. This medication is also compatible with breastfeeding.44
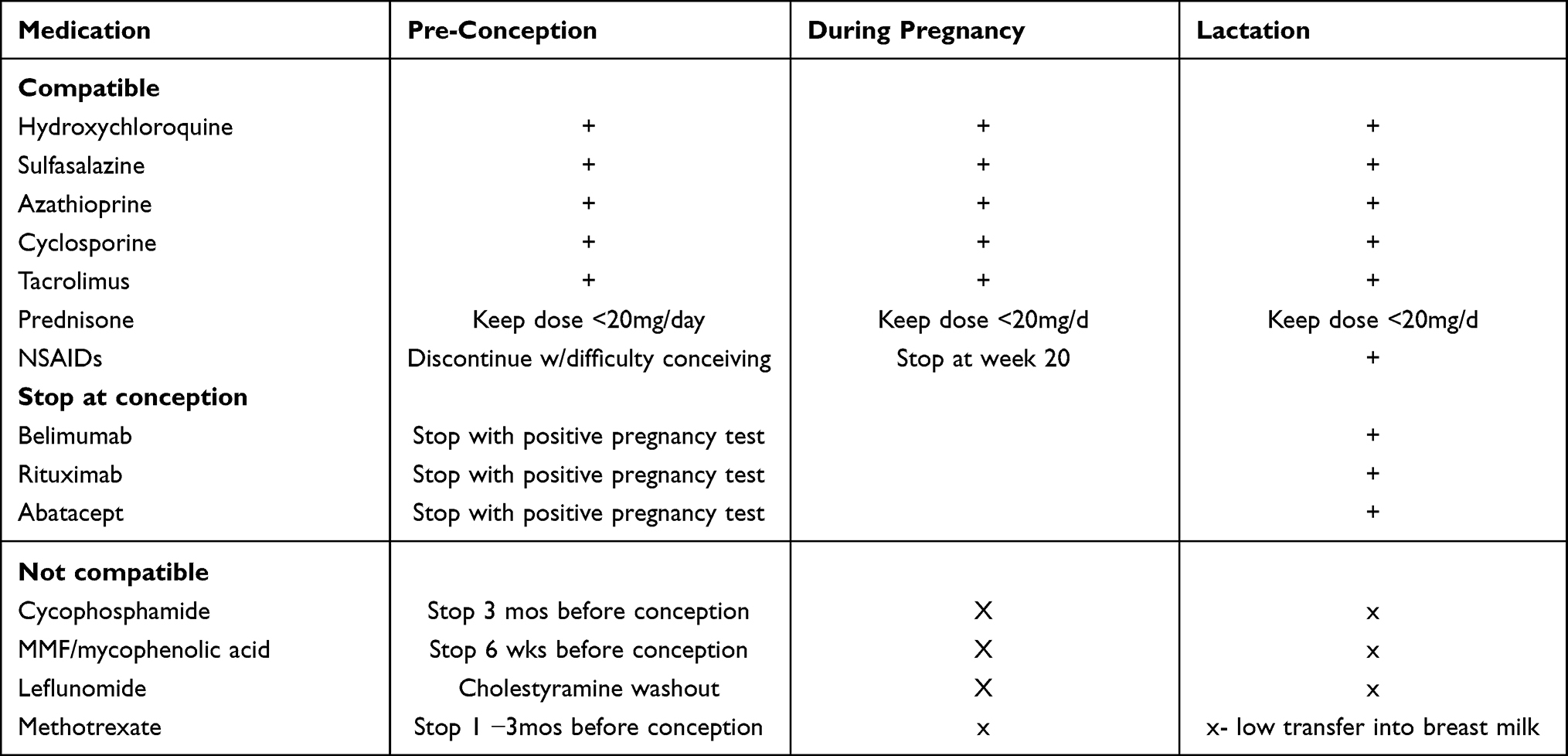 |
Table 4 Safety of Common SLE Treatments During Pregnancy and Lactation |
Non-steroidal anti-inflammatory medications (NSAIDs) help control arthralgias and arthritis in SLE patients. The Food and Drug Administration (FDA) recently issued a warning that NSAIDS as a class may cause “rare but serious kidney problems in an unborn baby” that can lead to oligohydramnios and death around 20 weeks or later.69 After 30 weeks of gestation, NSAIDs can cause premature closure of the ductus arteriosus.44 We recommend that patients stop NSAIDs after week 20 of gestation. The exception to these recommendations is low dose aspirin that can be continued for the duration of the pregnancy. NSAIDs are compatible with breastfeeding.44
Early data suggested that glucocorticoids increased the risk for cleft palate formation.70 However, in a large study from Denmark, increased rate of oral facial clefts were not found among 51,973 infants exposed to glucocorticoids in utero.71 Nonetheless, glucocorticoids can contribute to gestational hypertension and diabetes, preterm premature rupture of the membranes and small for gestational age infants. Current recommendations advise keeping prednisone dose as low as possible during pregnancy. Similarly, in women on >20mg/d of prednisone, ACR guidelines suggest discarding breast milk for four hours following dosing.44
Sulfasalazine is sometimes used to control arthritis in SLE patients. Data gleaned from the inflammatory bowel disease literature supports its use during pregnancy.72 There has been a case of diarrhea in a nursing child whose mother was taking sulfasalazine, so lactating women should consider discontinuing this medication if their infant develops diarrhea.73
Patients with significant organ involvement may require ongoing immunosuppression during pregnancy. Leflunomide, methotrexate and cyclophosphamide are either suspected or confirmed teratogenic medications and should be discontinued prior to conception. Leflunomide has a long half-life; women should undergo a drug elimination procedure with cholestyramine prior to conception; metabolite blood levels <0.03 μg/mL has been regarded as safe for pregnancy.74 Methotrexate should be stopped one to three months prior to anticipated conception and cyclophosphamide treatment should be discontinued three months prior to conception.44,55
Mycophenolate mofetil/mycophenolic acid, are now the most commonly prescribed medication for lupus nephritis, is teratogenic and increases the risk for pregnancy loss in the first trimester.75 A review of cumulative mycophenolate data in pregnancy showed the frequency of malformations is 22% and for spontaneous abortions to be 45%; inhibition of purine synthesis by mycophenolic acid is believed to be the cause of genotoxicity76 Mycophenolate should be stopped six weeks respectively prior to conception.
Fortunately, azathioprine, cyclosporine and tacrolimus are compatible with pregnancy and can be substituted for the aforementioned potential teratogens.44,55 The biologics rituximab, belimumab, and abatacept do not significantly cross the placenta until the 15th week of gestation; these medications can be continued through conception. In patients who are dependent on these biologics for disease control, discussing the potential risks of and benefits of these medications and through shared decision-making one can consider continuing these medications during pregnancy.
The Federal Drug Administration (FDA) recently approved voclosporin for the treatment of SLE nephritis; current recommendations are to avoid this medication in pregnant and lactating women.77
Treatment Approach
All women with SLE who are pregnant should continue hydroxychloroquine. Given the risk of pre-eclampsia, we recommend adding low dose aspirin at the end of the first trimester. Transition women who need ongoing immunosuppression for disease control to an immunosuppressive agent compatible with pregnancy (eg, tacrolimus, azathioprine or cyclosporine) and observe for four to six months to make certain that disease is stable prior to conception. For non-renal flares during pregnancy, treat with the lowest possible dose of prednisone. For renal flares, we recommend combination therapy of azathioprine with tacrolimus.
Many medications used for lupus management are compatible with lactation. Hydroxychloroquine, NSAIDs, sulfasalazine, and the immunosuppressive agents cyclosporine, azathioprine and tacrolimus are all compatible with breastfeeding. Biologics such as rituximab, and belimumab and likely abatacept are also compatible with lactation as these medications are all large molecules and do not readily get transferred into breast milk. Current recommendations are to avoid methotrexate in lactating women although there is growing evidence that little of this medication gets secreted in breast milk. Mycophenolate mofetil, cyclophosphamide and leflunomide should not be taken by lactating women.44,55
Conclusion
Systemic lupus erythematosus is a disease of reproductive aged women. Whereas formerly, providers counseled SLE patients to avoid pregnancy, improved disease management and a better understanding of medication safety render pregnancy a possibility for most SLE patients. Careful pregnancy planning for when disease is under good control with pregnancy compatible medications is crucial. Assembling a team that includes a maternal fetal medicine provider or obstetrician who is familiar with caring for SLE patients is likewise important. All patients with SLE should remain on hydroxychloroquine during pregnancy unless contraindicated. We encourage patients at high risk for developing pre-eclampsia (older or younger age, primigravida, patients with hypertension, prior renal disease, presence of antiphospholipid antibodies) to initiate aspirin therapy (81mg/day) during the first trimester. Sulfasalazine, and the immunosuppressive agents cyclosporine, azathioprine, and tacrolimus are compatible with pregnancy. Rituximab, belimumab and other biologic agents can continue through conception. Glucocorticoids can help manage flares but providers should use the lowest dose possible for disease control. All of the aforementioned medications are compatible with breast- feeding. Cyclophosphamide, leflunomide, methotrexate, mycophenolate mofetil, and voclosporin should be stopped prior to pregnancy and avoided in lactating women. Women with anti-Ro and anti-La antibodies will need fetal screening for the development of congenital complete heart block. Successful pregnancies in patients with SLE are possible with close monitoring and a collaborative framework.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choi J, Kim ST, Craft J. The pathogenesis of systemic lupus erythematosus—an update. Curr Opin Immunol. 2012;24(6):651–657. doi:10.1016/j.coi.2012.10.004
2. Bertsias GK, Pamfil C, Fanouriakis A, Boumpas DT. Diagnostic criteria for systemic lupus erythematosus: has the time come? Nat Rev Rheumatol. 2013;9(11):687–694. doi:10.1038/nrrheum.2013.103
3. Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. 2019;71(9):1400–1412. doi:10.1002/art.40930
4. Gergianaki I, Bortoluzzi A, Bertsias G. Update on the epidemiology, risk factors, and disease outcomes of systemic lupus erythematosus. Best Pract Res Clin Rheumatol. 2018;32(2):188–205. doi:10.1016/j.berh.2018.09.004
5. Stojan G, Petri M. Epidemiology of systemic lupus erythematosus: an update. Curr Opin Rheumatol. 2018;30(2):144–150. doi:10.1097/BOR.0000000000000480
6. Gaudreau M-C, Johnson BM, Gudi R, Al-Gadban MM, Vasu C. Gender bias in lupus: does immune response initiated in the gut mucosa have a role? Clin Exp Immunol. 2015;180(3):393–407. doi:10.1111/cei.12587
7. Tedeschi SK, Bermas B, Costenbader KH. Sexual disparities in the incidence and course of SLE and RA. Clin Immunol. 2013;149(2):211–218. doi:10.1016/j.clim.2013.03.003
8. Hickman RA, Gordon C. Causes and management of infertility in systemic lupus erythematosus. Rheumatology. 2011;50(9):1551–1558. doi:10.1093/rheumatology/ker105
9. Bermas BL, Sammaritano LR. Pregnancy and fertility in systemic lupus erythematosus. In: Systemic Lupus Erythematosus. Elsevier; 2016:441–449. doi:10.1016/B978-0-12-801917-7.00050-4
10. Clowse MEB, Chakravarty E, Costenbader KH, Chambers C, Michaud K. Effects of infertility, pregnancy loss, and patient concerns on family size of women with rheumatoid arthritis and systemic lupus erythematosus. Arthritis Care Res. 2012;64(5):668–674. doi:10.1002/acr.21593
11. Oktem O, Yagmur H, Bengisu H, Urman B. Reproductive aspects of systemic lupus erythematosus. J Reprod Immunol. 2016;117:57–65. doi:10.1016/j.jri.2016.07.001
12. Blanco-Favela F, Quintal-Alvarez G, Leaños-Miranda A. Association between prolactin and disease activity in systemic lupus erythematosus. Influence of statistical power. J Rheumatol. 1999;26(1):55–59.
13. Pasoto SG, Mendonça BB, Bonfá E. Menstrual disturbances in patients with systemic lupus erythematosus without alkylating therapy: clinical, hormonal and therapeutic associations. Lupus. 2002;11(3):175–180. doi:10.1191/0961203302lu163oa
14. Ma W, Zhan Z, Liang X, Chen J, Huang X, Liao C. Subclinical impairment of ovarian reserve in systemic lupus erythematosus patients with normal menstruation not using alkylating therapy. J Womens Health. 2013;22(12):1023–1027. doi:10.1089/jwh.2013.4255
15. Nguyen QN, Zerafa N, Liew SH, Findlay JK, Hickey M, Hutt KJ. Cisplatin- and cyclophosphamide-induced primordial follicle depletion is caused by direct damage to oocytes. Mol Hum Reprod. 2019;25(8):433–444. doi:10.1093/molehr/gaz020
16. Kado R, McCune WJ. Ovarian protection with gonadotropin-releasing hormone agonists during cyclophosphamide therapy in systemic lupus erythematosus. Best Pract Res Clin Obstet Gynaecol. 2020;64:97–106. doi:10.1016/j.bpobgyn.2019.10.008
17. Slater CA, Liang MH, McCune JW, Christman GM, Laufer MR. Preserving ovarian function in patients receiving cyclophosphamide. Lupus. 1999;8(1):3–10. doi:10.1191/096120399678847335
18. Kwok L-W, Tam L-S, Zhu T, Leung YY, Li E. Predictors of maternal and fetal outcomes in pregnancies of patients with systemic lupus erythematosus. Lupus. 2011;20(8):829–836. doi:10.1177/0961203310397967
19. Yang H, Liu H, Xu D, et al. Pregnancy-related systemic lupus erythematosus: clinical features, outcome and risk factors of disease flares–a case control study. PLoS One. 2014;9(8):e104375. doi:10.1371/journal.pone.0104375
20. Buyon JP, Kim MY, Guerra MM, et al. Predictors of pregnancy outcomes in patients with lupus: a cohort study. Ann Intern Med. 2015;163(3):153–163. doi:10.7326/M14-2235
21. Clowse MEB, Magder L, Witter F, Petri M. Hydroxychloroquine in lupus pregnancy. Arthritis Rheum. 2006;54(11):3640–3647. doi:10.1002/art.22159
22. Eudy AM, Siega-Riz AM, Engel SM, et al. Effect of pregnancy on disease flares in patients with systemic lupus erythematosus. Ann Rheum Dis. 2018;77(6):855–860. doi:10.1136/annrheumdis-2017-212535
23. Saavedra MÁ, Miranda-Hernández D, Lara-Mejía A, et al. Use of antimalarial drugs is associated with a lower risk of preeclampsia in lupus pregnancy: a prospective cohort study. Int J Rheum Dis. 2020;23(5):633–640. doi:10.1111/1756-185X.13830
24. Tedeschi SK, Guan H, Fine A, Costenbader KH, Bermas B. Organ-specific systemic lupus erythematosus activity during pregnancy is associated with adverse pregnancy outcomes. Clin Rheumatol. 2016;35(7):1725–1732. doi:10.1007/s10067-016-3270-5
25. Chakravarty EF, Nelson L, Krishnan E. Obstetric hospitalizations in the United States for women with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Rheum. 2006;54(3):899–907. doi:10.1002/art.21663
26. Clowse MEB, Jamison M, Myers E, James AH. A national study of the complications of lupus in pregnancy. Am J Obstet Gynecol. 2008;199(2):
27. Mehta B, Luo Y, Xu J, et al. Trends in maternal and fetal outcomes among pregnant women with systemic lupus erythematosus in the United States: a cross-sectional analysis. Ann Intern Med. 2019;171(3):164–171. doi:10.7326/M19-0120
28. Skorpen CG, Lydersen S, Gilboe I-M, et al. Influence of disease activity and medications on offspring birth weight, pre-eclampsia and preterm birth in systemic lupus erythematosus: a population-based study. Ann Rheum Dis. 2018;77(2):264–269. doi:10.1136/annrheumdis-2017-211641
29. Wagner SJ, Craici I, Reed D, et al. Maternal and foetal outcomes in pregnant patients with active lupus nephritis. Lupus. 2009;18(4):342–347. doi:10.1177/0961203308097575
30. Buyon JP, Cronstein BN, Morris M, Tanner M, Weissmann G. Serum complement values (C3 and C4) to differentiate between systemic lupus activity and pre-eclampsia. Am J Med. 1986;81(2):194–200. doi:10.1016/0002-9343(86)90251-2
31. Bellos I, Pergialiotis V, Loutradis D, Daskalakis G. The prognostic role of serum uric acid levels in preeclampsia: a meta-analysis. J Clin Hypertens. 2020;22(5):826–834. doi:10.1111/jch.13865
32. Clark CA, Spitzer KA, Laskin CA. Decrease in pregnancy loss rates in patients with systemic lupus erythematosus over a 40-year period. J Rheumatol. 2005;32(9):1709–1712.
33. Al Arfaj AS, Khalil N. Pregnancy outcome in 396 pregnancies in patients with SLE in Saudi Arabia. Lupus. 2010;19(14):1665–1673. doi:10.1177/0961203310378669
34. Molokhia M, Maconochie N, Patrick A, Doyle P. Cross-sectional analysis of adverse outcomes in 1029 pregnancies of Afro-Caribbean women in Trinidad with and without systemic lupus erythematosus. Arthritis Res Ther. 2007;9(6):R124. doi:10.1186/ar2332
35. Dhar JP, Essenmacher LM, Ager JW, Sokol RJ. Pregnancy outcomes before and after a diagnosis of systemic lupus erythematosus. Am J Obstet Gynecol. 2005;193(4):1444–1455. doi:10.1016/j.ajog.2005.02.104
36. Smyth A, Oliveira GHM, Lahr BD, Bailey KR, Norby SM, Garovic VD. A systematic review and meta-analysis of pregnancy outcomes in patients with systemic lupus erythematosus and lupus nephritis. Clin J Am Soc Nephrol. 2010;5(11):2060–2068. doi:10.2215/CJN.00240110
37. Chakravarty EF, Colón I, Langen ES, et al. Factors that predict prematurity and preeclampsia in pregnancies that are complicated by systemic lupus erythematosus. Am J Obstet Gynecol. 2005;192(6):1897–1904. doi:10.1016/j.ajog.2005.02.063
38. Chen Y-J, Chang J-C, Lai E-L, et al. Maternal and perinatal outcomes of pregnancies in systemic lupus erythematosus: a nationwide population-based study. Semin Arthritis Rheum. 2020;50(3):451–457. doi:10.1016/j.semarthrit.2020.01.014
39. Moroni G, Doria A, Giglio E, et al. Fetal outcome and recommendations of pregnancies in lupus nephritis in the 21st century. A prospective multicenter study. J Autoimmun. 2016;74:6–12. doi:10.1016/j.jaut.2016.07.010
40. Brito-Zerón P, Izmirly PM, Ramos-Casals M, Buyon JP, Khamashta MA. The clinical spectrum of autoimmune congenital heart block. Nat Rev Rheumatol. 2015;11(5):301–312. doi:10.1038/nrrheum.2015.29
41. Sammaritano LR, Bermas BL, Chakravarty EE, et al. 2020 American College of Rheumatology Guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Rheumatol. 2020;72(4):529–556. doi:10.1002/art.41191
42. Izmirly PM, Costedoat-Chalumeau N, Pisoni CN, et al. Maternal use of hydroxychloroquine is associated with a reduced risk of recurrent anti-SSA/Ro-antibody-associated cardiac manifestations of neonatal lupus. Circulation. 2012;126(1):76–82. doi:10.1161/CIRCULATIONAHA.111.089268
43. Marder W, Romero VC, Ganser MA, et al. Increased usage of special educational services by children born to mothers with systemic lupus erythematosus and antiphospholipid antibodies. Lupus Sci Med. 2014;1(1):e000034. doi:10.1136/lupus-2014-000034
44. Davidov D, Sheiner E, Wainstock T, Miodownik S, Pariente G. Maternal Systemic Lupus Erythematosus (SLE) high risk for preterm delivery and not for long-term neurological morbidity of the offspring. J Clin Med. 2021;10(13). doi:10.3390/jcm10132952
45. Sammaritano LR, Bermas BL, Chakravarty EE, et al. 2020 American College of Rheumatology Guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Care Res. 2020;72(4):461–488. doi:10.1002/acr.24130
46. Petri M. Pregnancy and systemic lupus erythematosus. Best Pract Res Clin Obstet Gynaecol. 2020;64:24–30. doi:10.1016/j.bpobgyn.2019.09.002
47. Allen D, Hunter MS, Wood S, Beeson T. One key question®: first things first in reproductive health. Matern Child Health J. 2017;21(3):387–392. doi:10.1007/s10995-017-2283-2
48. Yelnik CM, Laskin CA, Porter TF, et al. Lupus anticoagulant is the main predictor of adverse pregnancy outcomes in aPL-positive patients: validation of PROMISSE study results. Lupus Sci Med. 2016;3(1):e000131. doi:10.1136/lupus-2015-000131
49. Yelnik CM, Porter TF, Branch DW, et al. Brief report: changes in antiphospholipid antibody titers during pregnancy: effects on pregnancy outcomes. Arthritis Rheumatol. 2016;68(8):1964–1969. doi:10.1002/art.39668
50. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89–94. doi:10.5830/CVJA-2016-021
51. Cheung KL, Lafayette RA. Renal physiology of pregnancy. Adv Chronic Kidney Dis. 2013;20(3):209–214. doi:10.1053/j.ackd.2013.01.012
52. van den Broe NR, Letsky EA. Pregnancy and the erythrocyte sedimentation rate. BJOG. 2001;108(11):1164–1167. doi:10.1016/S0306-5456(01)00267-4
53. Chighizola CB, Lonati PA, Trespidi L, Meroni PL, Tedesco F. The complement system in the pathophysiology of pregnancy and in systemic autoimmune rheumatic diseases during pregnancy. Front Immunol. 2020;11. doi:10.3389/fimmu.2020.02084.
54. Weinstein A, Alexander RV, Zack DJ. A review of complement activation in SLE. Curr Rheumatol Rep. 2021;23(3):16. doi:10.1007/s11926-021-00984-1
55. Butte NF. Carbohydrate and lipid metabolism in pregnancy: normal compared with gestational diabetes mellitus. Am J Clin Nutr. 2000;71(5Suppl):1256S–61S. doi:10.1093/ajcn/71.5.1256s
56. Andreoli L, Bertsias GK, Agmon-Levin N, et al. EULAR recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum Dis. 2017;76(3):476–485. doi:10.1136/annrheumdis-2016-209770
57. Friedman DM, Rupel A, Buyon JP. Epidemiology, etiology, detection, and treatment of autoantibody-associated congenital heart block in neonatal lupus. Curr Rheumatol Rep. 2007;9(2):101–108. doi:10.1007/s11926-007-0003-4
58. Lun Hon K, Leung AKC. Neonatal lupus erythematosus. Autoimmune Dis. 2012;2012:1–6. doi:10.1155/2012/301274
59. Aoki S, Yamamoto Y. Systemic lupus erythematosus: strategies to improve pregnancy outcomes. Int J Womens Health. 2016;8:265–272. doi:10.2147/IJWH.S90157
60. Mok CC, Tang SSK, To CH, Petri M. Incidence and risk factors of thromboembolism in systemic lupus erythematosus: a comparison of three ethnic groups. Arthritis Rheum. 2005;52(9):2774–2782. doi:10.1002/art.21224
61. Petri M. Antiphospholipid syndrome. Transl Res. 2020;225:70–81. doi:10.1016/j.trsl.2020.04.006
62. Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295–306. doi:10.1111/j.1538-7836.2006.01753.x
63. Motta M, Tincani A, Faden D, et al. Follow-up of infants exposed to hydroxychloroquine given to mothers during pregnancy and lactation. J Perinatol. 2005;25(2):86–89. doi:10.1038/sj.jp.7211208
64. Friedman DM, Kim M, Costedoat-Chalumeau N, et al. Electrocardiographic QT intervals in infants exposed to hydroxychloroquine throughout gestation. Circ Arrhythmia Electrophysiol. 2020;13(10). doi:10.1161/CIRCEP.120.008686
65. Huybrechts KF, Bateman BT, Zhu Y, et al. Hydroxychloroquine early in pregnancy and risk of birth defects. Am J Obstet Gynecol. 2021;224(3):
66. Bermas BL, Chambers C. Hydroxychloroquine early in pregnancy and risk of birth defects: don’t throw out the baby with the bathwater. Am J Obstet Gynecol. 2021;224(5):548–549. doi:10.1016/j.ajog.2020.12.1218
67. Bermas BL, Kim SC, Huybrechts K, et al. Trends in use of hydroxychloroquine during pregnancy in systemic lupus erythematosus patients from 2001 to 2015. Lupus. 2018;27(6):1012–1017. doi:10.1177/0961203317749046
68. Palmsten K, Simard JF, Chambers CD, Arkema EV. Medication use among pregnant women with systemic lupus erythematosus and general population comparators. Rheumatology. 2016;kew448. doi:10.1093/rheumatology/kew448
69. Available from: Https://www.fda.gov/safety/medical-product-safety-information/nonsteroidal-anti-inflammatory-drugs-nsaids-drug-safety-communication-avoid-use-nsaids-pregnancy-20.
70. Park-Wyllie L, Mazzotta P, Pastuszak A, et al. Birth defects after maternal exposure to corticosteroids: prospective cohort study and meta-analysis of epidemiological studies. Teratology. 2000;62(6):385–392. doi:10.1002/1096-9926(200012)62:6<385::AID-TERA5>3.0.CO;2-Z
71. Hviid A, Mølgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ. 2011;183(7):796–804. doi:10.1503/cmaj.101063
72. Mogadam M, Dobbins WO, Korelitz BI, Ahmed SW. Pregnancy in inflammatory bowel disease: effect of sulfasalazine and corticosteroids on fetal outcome. Gastroenterology. 1981;80(1):72–76. doi:10.1016/0016-5085(81)90193-1
73. Branski D, Kerem E, Gross-Kieselstein E, Hurvitz H, Litt R, Abrahamov A, Bloody diarrhea–a possible complication of sulfasalazine transferred through human breast milk. J Pediatr Gastroenterol Nutr. 1986;5(2):316–317. doi:10.1097/00005176-198605020-00028
74. Chambers CD, Johnson DL, Robinson LK, et al. Birth outcomes in women who have taken leflunomide during pregnancy. Arthritis Rheum. 2010;62(5):1494–1503. doi:10.1002/art.27358
75. Sifontis NM, Coscia LA, Constantinescu S, Lavelanet AF, Moritz MJ, Armenti VT. Pregnancy outcomes in solid organ transplant recipients with exposure to mycophenolate mofetil or sirolimus. Transplantation. 2006;82(12):1698–1702. doi:10.1097/01.tp.0000252683.74584.29
76. Kim M, Rostas S, Gabardi S. Mycophenolate fetal toxicity and risk evaluation and mitigation strategies. Am J Transplant. 2013;13(6):1383–1389. doi:10.1111/ajt.12238
77. Available from: Https://d1io3yog0oux5.cloudfront.net/auriniapharma/files/pages/lupkynis-prescribing-information/FPI-0011+Approved+USPI++MG.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.