Back to Journals » Journal of Inflammation Research » Volume 19
Systemic Immune-Inflammation Index Outperforms Conventional Inflammatory Markers in Predicting Cardiovascular Outcomes in Heart Failure with Preserved Ejection Fraction
Authors Zhu S, Li H, Ou Z, Zheng M, Yuan W
Received 25 September 2025
Accepted for publication 27 December 2025
Published 21 January 2026 Volume 2026:19 568473
DOI https://doi.org/10.2147/JIR.S568473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Chengming Fan
Shijie Zhu,1 Haiying Li,2 Zipeng Ou,3 Muhan Zheng,4 Woliang Yuan1,2
1Department of Cardiovascular Medicine, Shenshan Medical Center, Memorial Hospital of Sun Yat-Sen University, Shanwei, People’s Republic of China; 2Department of Cardiovascular Medicine, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 3Department of Cardiovascular Medicine, Fuwai Hospital, Chinese Academy of Medical Sciences, Shenzhen, People’s Republic of China; 4Department of Rheumatology and Immunology, Shenshan Medical Center, Memorial Hospital of Sun Yat-Sen University, Shanwei, People’s Republic of China
Correspondence: Woliang Yuan, Email [email protected] Muhan Zheng, Email [email protected]
Background: The systemic immune-inflammation index (SII), a novel inflammatory index integrating neutrophil, platelet, and lymphocyte counts, predicts outcomes in several cardiovascular diseases, yet its role in heart failure with preserved ejection fraction (HFpEF) remains unclear. We therefore investigated the prognostic value of SII in HFpEF patients and compares its performance against other inflammatory markers, including systemic inflammation response index (SIRI), neutrophil-to-lymphocyte ratio (NLR) and C-reactive protein (CRP).
Methods: We retrospectively analyzed a cohort of 316 patients with HFpEF diagnosed between January 2017 and January 2021. All-cause mortality, cardiovascular mortality and HF rehospitalization were assessed over a median follow-up of 24 months. Net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were employed to evaluate the comparative prognostic performance of SII against SIRI, NLR and CRP.
Results: Logistic regression models revealed that each 100-unit increase in SII was independently associated with elevated risks of cardiovascular mortality (OR:1.321, 95% CI:1.191– 1.467, P< 0.001) and HF rehospitalization (OR:1.168, 95% CI:1.098– 1.241, P< 0.001), but not with all-cause mortality (P> 0.05). SII demonstrated superior prognostic performance compared to SIRI, NLR and CRP both in cardiovascular mortality (NRI range: 0.798– 1.097; IDI range: 0.094– 0.142, all P< 0.05) and HF rehospitalization (NRI range: 0.254– 0.455; IDI range: 0.016– 0.066, all P< 0.05). However, SII provided no incremental utility for all-cause mortality (P> 0.05).
Conclusion: SII emerges as a superior predictor of adverse cardiovascular outcomes in HFpEF compared to conventional inflammatory markers, supporting its use for risk stratification and as a potential therapeutic guide. Nevertheless, its association with all-cause mortality remains limited.
Keywords: systemic immune-inflammation index, heart failure with preserved ejection fraction, cardiovascular outcomes
Introduction
The global burden of heart failure (HF) continues to escalate, as evidenced by epidemiological surveillance data from European cohorts indicating an annual incidence of approximately 5 cases per 1000 person-years, with an estimated 1–2% of adults currently affected by HF. Heart failure with preserved ejection fraction (HFpEF) accounts for approximately 50% of HF cases.1 Given the progressive aging of the population, coupled with improved management of cardiovascular disease, HFpEF is projected to become the predominant HF subtype globally in coming decades.2
Systemic low-grade inflammatory state is a key driver in the pathogenesis and progression of HFpEF through several classic inflammation pathways. NLRP3 inflammasome activation promotes the release of IL-1β and IL-18, whereas TNF-α/NF-κB signaling reduces nitric oxide bioavailability and protein kinase G activity, leading to titin hypophosphorylation. Simultaneously, myeloperoxidase exacerbates oxidative stress and further depletes nitric oxide further impairing endothelial function. Together, these pathways induce cardiomyocyte hypertrophy, myocardial fibrosis, endothelial and microvascular dysfunction, ultimately culminating diastolic dysfunction.3–5 Interleukin-6 (IL-6), a classic inflammatory cytokine, impairs cardiac relaxation by downregulating sarcoplasmic reticulum Ca2⁺-ATPase, thereby reducing calcium release.6 In addition, IL-6 promotes increased myocardial stiffness by inducing microvascular inflammation and reducing titin phosphorylation.7 Clinical investigations have revealed a significant association between circulating inflammatory biomarkers and HFpEF prevalence.6,8,9 Elevated levels of inflammatory biomarkers, correlate with increased risks of all-cause and cardiovascular mortality in HFpEF patients.7,10,11
Systemic immune-inflammation index (SII), as a novel and readily available inflammatory index, has been validated as a prognostic indicator for all-cause mortality in breast cancer cohorts.12 Within cardiovascular field, emerging evidence confirms the utility of SII in predicting disease severity and adverse outcomes in patients with coronary artery disease (CAD),13 as well as stratifying risks of atrial fibrillation (AF), ventricular tachycardia and bradycardia.14 However, the prognostic value of SII in HFpEF remains unexplored, representing a critical knowledge gap in cardio-inflammatory research.
To address this critical knowledge gap, we conducted a retrospective cohort study to assess SII for predicting all-cause mortality, cardiovascular mortality and HF rehospitalization in HFpEF patients, with direct comparisons to conventional inflammatory markers: C-reactive protein (CRP), systemic inflammation response index (SIRI) and neutrophil-to-lymphocyte ratio (NLR).
Methods
Study Population
This single-center retrospective study consecutively recruited patients diagnosed with HFpEF at the Department of Cardiovascular Medicine, Sun Yat-sen Memorial Hospital between January 2017 and January 2021. Inclusion criteria required: Age ≥18 years; Confirmed HFpEF diagnosis meeting ESC 2021 criteria:1 (1) Symptom and signs of HF; (2) Left ventricular ejection fraction (LVEF)≥50%; (3) Objective evidence of cardiac structural and/or functional abnormalities consistent with the presence of LV diastolic dysfunction/raised filling pressures including raised natriuretic peptide. Exclusion criteria comprised: Progression to heart failure with reduced ejection fraction (HFrEF) during follow-up; Presence of active infection at admission; Pre-existing hematological diseases that could confound the calculation of inflammatory indices; Incomplete baseline clinical data and Loss to follow-up. After screening, a total of 316 patients were included.
Clinical Data Collection and Calculation
Baseline clinical characteristics and medication regimens were collected via the electronic medical record system. SII was calculated using the first complete blood count obtained within the first 24 hours of admission, calculated as platelet count×neutrophil count/ lymphocyte count. Similarly, SIRI was derived as neutrophil count×monocyte/lymphocyte count and NLR as neutrophil count/lymphocyte count. All cell counts are reported in 109/L.
Study Endpoints
Patients were followed up for a median of 24 months (12,39). The primary endpoints were all-cause mortality, cardiovascular mortality and HF rehospitalization. Endpoint adjudication was performed independently by two clinicians blinded to the inflammatory markers, following the criteria in Supplementary Material 2. Any discrepancies were resolved by a third senior clinician.
Ethics Statement
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University (2025-SSKY-092). Due to the retrospective nature of the study and the use of anonymized patient data, the requirement for written informed consent was waived by the ethics committee. All data were de-identified prior to analysis to ensure patient confidentiality. The reporting of this study adheres to the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) guideline, and the completed checklist is available as Supplementary Material 1.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]), with categorical variables presented as frequencies (%). Group comparisons used independent t-tests or Mann–Whitney U-tests for continuous variables, and χ2-tests for categorical variables. The primary variable of interest was SII. Based on established HFpEF prognosis literature and guideline,1,2,15 we pre-specified four key covariates for adjustment: age, sex, NT-proBNP, and LVEF All variables were included in multivariable logistic regression models without selection. Due to the non-normal distribution of SII, SIRI, and NLR, we have applied natural log-transformation to all these inflammatory markers prior to inclusion in the models. The models were used to estimate independent associations with all-cause mortality, cardiovascular mortality, and HF rehospitalization, with results reported as odds ratios (ORs) and 95% confidence intervals (CIs). Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), and goodness of fit was summarized with Nagelkerke’s R2. To assess the robustness of variable selection, we performed LASSO regression as a sensitivity analysis. Variable selection stability was evaluated across 50 repetitions of 5-fold cross-validation, with selection frequency recorded for each predictor. The final model was tuned using the lambda.min criterion. Internal validation was carried out via bootstrapping with 200 resamples to compute optimism-corrected AUC with 95% CI and quantify overfitting.
Base model incorporated baseline characteristics (age, sex, hypertension, diabetes mellitus, CAD, valvular heart disease and AF) and diagnostic parameters (NT-proBNP, left ventricular end-diastolic dimension (LVEDD), LVEF) as predictors, with the occurrence of endpoints as the outcome. To further validate the superior predictive performance of SII compared to CRP, SIRI and NLR, four models were built: Model 1 added SII as a new independent variable in the base model while Model 2–4 added SIRI, NLR and CRP respectively. Model performance was comparatively evaluated using Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI). The NRI evaluates the correct reclassification of subjects into risk categories, while the IDI reflects the overall improvement in separation between events and non-events. We applied the Benjamini–Hochberg false discovery rate (FDR) procedure to adjust P‑values for NRI and IDI, accounting for multiple comparisons across the four models and three clinical endpoints.
All analyses were conducted using R 4.4.0. The primary R packages utilized included: stats, glmnet, pROC, boot, PredictABEL, nricens, riskRegression, ggplot2 and patchwork. Statistical significance was set at two-tailed P< 0.05.
Results
Study Population and Outcomes
Among 316 enrolled patients with HFpEF (mean age 73.1 ± 10.3 years; 47.2% male), SII levels were significantly elevated in those with hypertension (63.6% prevalence), CAD (50.9%), valvular heart disease (38.3%) and diabetes mellitus (29.1%) compared to patients without these comorbidities (all P<0.05). A similar but non-significant trend was observed for AF (64.9%). Median NT-proBNP levels were elevated at 1744.0 pg/mL (820.3, 3188.0). Inflammatory markers were generally elevated: SII 630.4 (401.8, 960.6), SIRI 1.4 (0.9, 2.4), NLR:3.0 (2.0, 4.5), and CRP: 19.7 ± 12.1 mg/L. At discharge, β-blockers were the most common medication (56.0%), followed by ACEI/ARB/ANRI (44.3%), mineralocorticoid receptor antagonists (41.5%), and SGLT2 inhibitors (2.5%). Echocardiography confirmed preserved systolic function (LVEF 62.9 ± 7.2%), with LVEDD of 49.2 ± 5.9 mm.
During a median follow-up of 24 (12, 39) months, 74 patients (23.4%) experienced all-cause mortality, with cardiovascular mortality and in-hospital mortality accounting for 35.1% and 9.5%, respectively. HF rehospitalization occurred in 113 patients (35.8%).
SII and Clinical Endpoints
For cardiovascular mortality, SII demonstrated superior prognostic performance (Corrected-AUC:0.831, 95% CI: 0.739–0.905; P<0.001), with an optimal cutoff ≥826.42 providing 88.5% sensitivity and 72.8% specificity. Predictive capacity remained significant for HF rehospitalization (Corrected-AUC:0.686, 95% CI: 0.616–0.751, P<0.001; cutoff ≥808.33; sensitivity 54.0%, specificity 78.3%). In contrast, SII lacked prognostic utility for all-cause mortality (Corrected-AUC:0.532, 95% CI: 0.473–0.597; P=0.970) (Figure 1 and Table 1).
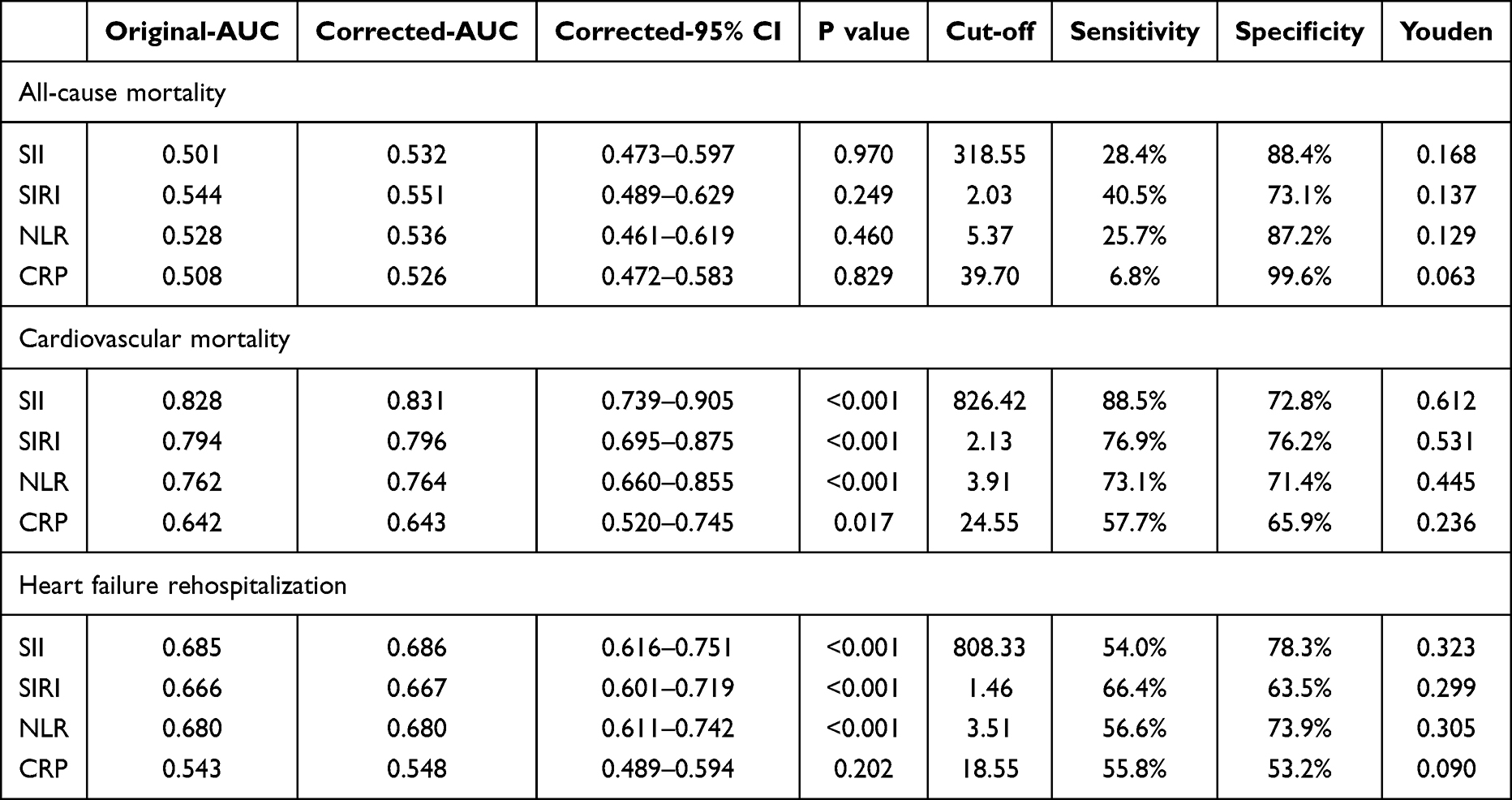 |
Table 1 Discriminatory Performance of Inflammatory Markers for Clinical Outcomes |
 |
Figure 1 Receiver operating characteristic (ROC) curves demonstrating the discriminatory capacity of the Systemic immune-inflammation index (SII), C-reactive protein (CRP), systemic inflammation response index (SIRI) and neutrophil-to-lymphocyte ratio (NLR) for (A) all-cause mortality; (B) cardiovascular mortality and (C) heart failure rehospitalization. |
Based on clinical considerations, we conducted a logistic regression model incorporating age, sex, NT-proBNP, LVEF and SII. Each 100-unit increase in SII was associated with a 32.1% higher risk of cardiovascular mortality (OR:1.321, 95% CI:1.191–1.467, P<0.001) and a 16.8% increase risk in HF rehospitalization (OR:1.168, 95% CI:1.098–1.241, P<0.001). However, no significant association was observed between SII and all-cause mortality (OR 0.996, 95% CI: 0.939–1.056, P = 0.894) (Table 2 and Figure 2A). To illustrate its clinical relevance, an increase in SII from the 25th to the 75th percentile corresponded to a higher risk of cardiovascular mortality (OR 3.325, 95% CI: 2.122–5.211) and HF rehospitalization (OR 1.951, 95% CI: 1.498–2.541).
 |
Table 2 Multivariate-Adjusted Logistic Regression Analysis for Clinical Outcomes |
 |
Figure 2 Predictive performance of the systemic immune-inflammation index (SII) in heart failure with preserved ejection fraction (HFpEF). (A) Multivariable-adjusted associations (odds ratios) of SII and clinical variables with adverse outcomes. (B) Model performance metrics, including original and bootstrap-corrected area under the curve (AUC). (C) Stability of variable selection across bootstrap resamples using LASSO regression. |
Sensitivity analyses confirmed the robustness of these findings. LASSO regression with stability selection demonstrated SII as a consistently selected predictor for both cardiovascular mortality and HF rehospitalization (Figure 2C). Bootstrap internal validation indicated minimal model overfitting, with optimism-corrected AUC values closely approximating original estimates. (Figure 2B).
Incremental Predictive Value of SII
We evaluated the incremental prognostic value of SII by constructing a series of models. Although the AUC for Model 1 (incorporating SII) was numerically higher for cardiovascular mortality and HF rehospitalization, the differences compared to other models did not reach statistical significance (Table 3). However, Model 1 demonstrated significantly superior performance in risk reclassification and discrimination for adverse cardiovascular outcome compared to all other models, as evidenced by statistically significant improvements in both the NRI and IDI (all P<0.05, Table 3). In contrast, Model 1 provided no significant predictive improvement for all-cause mortality compared to any of the comparison models (all P>0.05, Table 4).
 |
Table 3 Area Under the Curve (AUC) Values for the Base Model and Models Incorporating Inflammatory Markers in HFpEF |
 |
Table 4 Superior Reclassification Performance of the Systemic Immune-Inflammation Index (SII) Over Conventional Inflammatory Markers in HFpEF |
Discussion
Our study confirmed that. SII — a composite inflammatory marker derived from platelet, neutrophil, and lymphocyte counts— exhibits superior predictive capacity for cardiovascular mortality and HF rehospitalization compared to SIRI, NLR and CRP. Notably, this represents the first validation of SII’s prognostic value in HFpEF populations. However, SII shows limited predictive capacity for all-cause mortality.
A key strength of this study lies in its methodologically rigorous approach to establishing the prognostic value of SII. Unlike conventional analyses that may be susceptible to variable selection bias or overfitting, we pre-specified our adjustment variables based on established literature1,2,15 and further validated our findings through advanced statistical techniques. For cardiovascular outcomes, the consistent selection of SII by LASSO regression with stability analysis underscores its role as a robust predictor. Furthermore, the bootstrap internal validation for these endpoints demonstrated minimal overfitting, indicating that the model’s performance is likely to generalize to the real-world HFpEF populations. In summary, these comprehensive statistical strategies enhance the utility of SII as a biomarker for cardiovascular risk stratification.
Systemic inflammation is recognized as one of the central mechanisms of HFpEF initiation and progression, with comorbidities serving as key drivers of this inflammatory state. Through impaired microvascular endothelial function, promoted myocardial fibrosis, and altered cardiomyocyte metabolism, systemic inflammation ultimately increases myocardial stiffness and leads to diastolic dysfunction.3–5,16 In line with this pathophysiological mechanism, our findings show that patients with a higher burden of comorbidities exhibit elevated SII levels. Our study demonstrates that SII exhibits strong performance in predicting cardiovascular mortality in HFpEF (AUC 0.831), significantly outperforming its predictive ability in mixed HF and CAD cohort (AUC 0.575 and 0.590, respectively).17,18 These comparisons suggest that systemic inflammation may play a more central role in adverse prognosis in HFpEF compared to HFrEF and CAD.
Conventional inflammatory indices, including CRP, SIRI and NLR, have well-established prognostic value in HFpEF.10,19–21 However, our study confirms that SII offers a distinct prognostic advantage: although its addition to the base model did not improve the AUC, it yielded statistically significant NRI and IDI for predicting adverse cardiovascular outcomes compared with conventional inflammatory markers. These results indicate that the incremental prognostic value of SII lies primarily in enhancing model calibration and enabling individualized risk stratification, underscoring its clinical relevance for personalized risk assessment and management. The SII offers a prognostic advantage by integrating three key pathological pathways. First, neutrophils induced microvascular endothelial inflammation through the release of reactive oxygen species, enzymatic cascades, and neutrophil extracellular traps.22 Second, lymphocytes coordinate antigen-specific immune responses. Th2 cell differentiation upregulate the profibrotic cytokines IL-4 and IL-13, which potently stimulate fibroblast collagen synthesis and promote myocardial fibrosis.23 Third, Aging platelets, which upregulate immunoreceptors such as CLEC-2, CD36, CD40L and ICAM-1, directly facilitate platelet-leukocyte interactions and enhance the formation of platelet-leukocyte aggregates. Concurrently, these platelets shift toward a procoagulant phenotype marked by increased phosphatidylserine (PS) exposure. The resulting PS⁺/P‑selectin⁺ platelets then act as a catalytic surface for thrombin generation, thereby functionally linking inflammation and coagulation. Furthermore, upon activation, ageing platelets release an array of bioactive mediators (eg, P‑selectin, CD40L, and chemokines such as RANTES) from their α‑granules, recruiting neutrophils and monocytes to sites of vascular injury and amplifying the inflammatory response,24,25 These mechanisms mentioned above enable SII to holistically assess the “inflammation-thrombosis-immunity” network dysregulation of HFpEF, which is not offered by SIRI or NLR (which omit platelet counts) or by CRP. Consistent with this, prior studies about CAD have also established the significantly superior predictive value of SII over SIRI, NLR and CRP.26–28
ROC analysis revealed closely aligned SII cutoffs for cardiovascular mortality (826.42) and HF rehospitalization (808.33). Patients with SII levels above this threshold should be classified as high-risk for adverse cardiovascular events. For this population, in addition to receiving guideline-directed therapies (eg SGLT2 inhibitors) and comprehensive comorbidity management, ongoing monitoring of inflammatory status and targeting anti-inflammatory interventions (eg IL-1β and IL-6 inhibition) may represent novel therapeutic strategies in HFpEF management.
Notably, SII demonstrated limited prognostic capacity for all-cause mortality, a finding potentially mediated through competing non-cardiovascular deaths prevalent in HFpEF population. These findings underscore the necessity for phenotype-specific inflammatory profiling targeting distinct mortality pathways.
Limitation
This study has several limitations. The single-center retrospective design can only identify associations but cannot establish causality between SII and adverse cardiovascular outcomes in HFpEF. In addition, the absence of serial monitoring of dynamic SII changes as well as adjustments to classes and dosages of HF medications may limit the generalizability of our findings. Future large-scale prospective clinical studies are required to validate these conclusions. Whether SII-guided anti-inflammatory strategies can improve clinical outcomes in HFpEF patients represents a critical direction for future investigations.
Conclusion
SII, integrating neutrophil, lymphocyte, and platelet counts, outperforms conventional inflammatory indices in predicting cardiovascular-specific adverse outcomes in HFpEF patients, supporting its utility for risk stratification and potential as a therapeutic target, despite its limited association with all-cause mortality.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author at [email protected] upon reasonable request.
Acknowledgment
This work was supported by the Shanwei Science and Technology Program (Grant No. 2023C011).
Author Contributions
All authors listed on this manuscript meet all five authorship criteria, having made substantial contributions to the reported work, participated in drafting, writing or revising the manuscript, agreed on the journal for submission, approved all versions of the article and accepted accountability for its contents. Individual contributions are specified as follows according to the CRediT taxonomy:
Shijie Zhu: Conceptualization, Formal analysis, Funding acquisition, Writing – original draft.
Haiying Li: Investigation, Data curation, Writing – original draft.
Zipeng Ou: Methodology, Validation, Writing – review & editing.
Muhan Zheng: Validation, Supervision. Writing – review & editing.
Woliang Yuan: Conceptualization, Investigation, Data curation, Supervision, Project administration, Writing – review & editing.
Funding
This work was supported by the Shanwei Science and Technology Program (Grant No. 2023C011).
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–11.
2. Lam CSP, Voors AA, de Boer RA, et al. Heart failure with preserved ejection fraction: from mechanisms to therapies. Eur Heart J. 2018;39(30):2780–2792. doi:10.1093/eurheartj/ehy301
3. Li C, Qin D, Hu J, et al. Inflamed adipose tissue: a culprit underlying obesity and heart failure with preserved ejection fraction. Front Immunol. 2022;13:947147. doi:10.3389/fimmu.2022.947147
4. Daou D, Gillette TG, Hill JA. Inflammatory mechanisms in heart failure with preserved ejection fraction. Physiology. 2023;38(5):217–230. doi:10.1152/physiol.00004.2023
5. Michaelsson E, Lund LH, Hage C, et al. Myeloperoxidase inhibition reverses biomarker profiles associated with clinical outcomes in HFpEF. JACC Heart Fail. 2023;11(7):775–787. doi:10.1016/j.jchf.2023.03.002
6. Chia YC, Kieneker LM, van Hassel G, et al. Interleukin 6 and development of heart failure with preserved ejection fraction in the general population. J Am Heart Assoc. 2021;10(11):e018549. doi:10.1161/JAHA.120.018549
7. Alogna A, Koepp KE, Sabbah M, et al. Interleukin-6 in patients with heart failure and preserved ejection fraction. JACC Heart Fail. 2023;11(11):1549–1561. doi:10.1016/j.jchf.2023.06.031
8. Albar Z, Albakri M, Hajjari J, et al. Inflammatory markers and risk of heart failure with reduced to preserved ejection fraction. Am J Cardiol. 2022;167:68–75. doi:10.1016/j.amjcard.2021.11.045
9. Ramirez MF, Lau ES, Parekh JK, et al. Obesity-related biomarkers are associated with exercise intolerance and HFpEF. Circ Heart Fail. 2023;16(11):e010618. doi:10.1161/CIRCHEARTFAILURE.123.010618
10. Mooney L, Jackson CE, Adamson C, et al. Adverse outcomes associated with interleukin-6 in patients recently hospitalized for heart failure with preserved ejection fraction. Circ Heart Fail. 2023;16(4):e010051.
11. Fu Z, Liu P, Gao X, et al. Association of systemic inflammatory markers with clinical adverse prognosis and outcomes in HFpEF: a systematic review and meta-analysis of cohort studies. Front Cardiovasc Med. 2024;11:1461073. doi:10.3389/fcvm.2024.1461073
12. Li Y, Yu M, Yang M, et al. The association of systemic immune-inflammation index with incident breast cancer and all-cause mortality: evidence from a large population-based study. Front Immunol. 2025;16:1528690. doi:10.3389/fimmu.2025.1528690
13. Zhao Z, Zhang X, Sun T, et al. Prognostic value of systemic immune-inflammation index in CAD patients: systematic review and meta-analyses. Eur J Clin Invest. 2024;54(2):e14100. doi:10.1111/eci.14100
14. Yang X, Zhao S, Wang S, et al. Systemic inflammation indicators and risk of incident arrhythmias in 478,524 individuals: evidence from the UK biobank cohort. BMC Med. 2023;21(1):76. doi:10.1186/s12916-023-02770-5
15. Pfeffer MA, Shah AM, Borlaug BA. Heart failure with preserved ejection fraction in perspective. Circ Res. 2019;124(11):1598–1617. doi:10.1161/CIRCRESAHA.119.313572
16. Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62(4):263–271. doi:10.1016/j.jacc.2013.02.092
17. Zheng Z, Shi S, Liu Z, et al. The predictive and prognostic value of the systemic immune-inflammation index for congestive heart failure. Rev Cardiovasc Med. 2024;25(11):417. doi:10.31083/j.rcm2511417
18. Gao Y, Bai G, Li Y, et al. Prognosis impact of multiple novel lymphocyte-based inflammatory indices in patients with initially diagnosed coronary artery disease. Immun Inflamm Dis. 2024;12(9):e1340. doi:10.1002/iid3.1340
19. Lai W, Zhao X, Gao Z, et al. Association of systemic inflammation level on admission with total and cardiovascular‑specific death in heart failure with preserved ejection fraction: a large multi‑center retrospective longitudinal study. J Inflamm Res. 2024;17:5533–5542. doi:10.2147/JIR.S462848
20. Lakhani I, Wong MV, Hung JKF, et al. Diagnostic and prognostic value of serum C-reactive protein in heart failure with preserved ejection fraction: a systematic review and meta-analysis. Heart Fail Rev. 2021;26(5):1141–1150. doi:10.1007/s10741-020-09927-x
21. Tamaki S, Nagai Y, Shutta R, et al. Combination of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as a novel predictor of cardiac death in patients with acute decompensated heart failure with preserved left ventricular ejection fraction: a multicenter study. J Am Heart Assoc. 2023;12(1):e026326. doi:10.1161/JAHA.122.026326
22. Ling S, Xu JW. NETosis as a pathogenic factor for heart failure. Oxid Med Cell Longev. 2021;2021:6687096. doi:10.1155/2021/6687096
23. Kong P, Christia P, Frangogiannis NG. The pathogenesis of cardiac fibrosis. Cell Mol Life Sci. 2014;71(4):549–574. doi:10.1007/s00018-013-1349-6
24. Anjum A, Mader M, Mahameed S, et al. Aging platelets shift their hemostatic properties to inflammatory functions. Blood. 2025;145(14):1568–1582. doi:10.1182/blood.2024024901
25. Lordan R, Tsoupras A, Zabetakis I. Platelet activation and prothrombotic mediators at the nexus of inflammation and atherosclerosis: potential role of antiplatelet agents. Blood Rev. 2021;45:100694. doi:10.1016/j.blre.2020.100694
26. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
27. Yilu Z, Zhanglong W, Fanke H, et al. The progression of non-culprit coronary lesion is related to higher SII, SIRI, and PIV in patients with ACS. Medicine. 2024;103(52):e41094. doi:10.1097/MD.0000000000041094
28. Ren Z, Liu J. Influence of systemic immunoinflammatory index on major adverse cardiovascular events in patients with coronary heart disease with heart failure as assessed by propensity score matching. Eur J Med Res. 2025;30(1):766. doi:10.1186/s40001-025-03028-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.