Back to Journals » Journal of Pain Research » Volume 14
Systematic Review of Systemic and Neuraxial Effects of Acetaminophen in Preclinical Models of Nociceptive Processing
Authors Hoshijima H, Hunt M ![]() , Nagasaka H, Yaksh T
, Nagasaka H, Yaksh T
Received 23 February 2021
Accepted for publication 11 September 2021
Published 12 November 2021 Volume 2021:14 Pages 3521—3552
DOI https://doi.org/10.2147/JPR.S308028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Hiroshi Hoshijima,1 Matthew Hunt,2 Hiroshi Nagasaka,1 Tony Yaksh2
1Department of Anesthesiology, Saitama Medical University Hospital, Saitama, Japan; 2Departments of Anesthesiology and Pharmacology, University of California, San Diego Anesthesia Research Laboratory, La Jolla, CA, USA
Correspondence: Tony Yaksh
Departments of Anesthesiology and Pharmacology, University of California, San Diego Anesthesia Research Laboratory 0818, 9500 Gilman Dr., La Jolla, CA, 92093, USA
Tel +1 619-543-3597
Fax +1 619-543-6070
Email [email protected]
Abstract: Acetaminophen (APAP) in humans has robust effects with a high therapeutic index in altering postoperative and inflammatory pain states in clinical and experimental pain paradigms with no known abuse potential. This review considers the literature reflecting the preclinical actions of acetaminophen in a variety of pain models. Significant observations arising from this review are as follows: 1) acetaminophen has little effect upon acute nociceptive thresholds; 2) acetaminophen robustly reduces facilitated states as generated by mechanical and thermal hyperalgesic end points in mouse and rat models of carrageenan and complete Freund’s adjuvant evoked inflammation; 3) an antihyperalgesic effect is observed in models of facilitated processing with minimal inflammation (eg, phase II intraplantar formalin); and 4) potent anti-hyperpathic effects on the thermal hyperalgesia, mechanical and cold allodynia, allodynic thresholds in rat and mouse models of polyneuropathy and mononeuropathies and bone cancer pain. These results reflect a surprisingly robust drug effect upon a variety of facilitated states that clearly translate into a wide range of efficacy in preclinical models and to important end points in human therapy. The specific systems upon which acetaminophen may act based on targeted delivery suggest both a spinal and a supraspinal action. Review of current targets for this molecule excludes a role of cyclooxygenase inhibitor but includes effects that may be mediated through metabolites acting on the TRPV1 channel, or by effect upon cannabinoid and serotonin signaling. These findings suggest that the mode of action of acetaminophen, a drug with a long therapeutic history of utilization, has surprisingly robust effects on a variety of pain states in clinical patients and in preclinical models with a good therapeutic index, but in spite of its extensive use, its mechanisms of action are yet poorly understood.
Keywords: intrathecal, paracetamol, cannabinoid, serotonin, anandamide, analgesia
Introduction
Acute and chronic pain imposes a burden on society, not only because of the associated human suffering, but also because of the cost of medical treatment, loss of productivity and disability payments, which has been estimated to be up to $650 billion per year in the USA alone. According to the recently posted National Institutes of Health (NIH) Pain Management fact sheet, pain affects more Americans than diabetes, heart disease and cancer combined.1 Opiates are widely used but are associated with a significant risk of addiction and diversion, while other types of analgesics [eg, nonsteroidal anti-inflammatory drug (NSAIDs), antidepressants and anti-epileptics] are hampered by limited efficacy and varying side effects.2–5
Acetaminophen, (also known generically as APAP or paracetamol) was synthesized by Morse in 1873 via the reduction of p-nitrophenol with tin in glacial acetic acid. It was then discovered as a metabolite of phenacetin in the 1890s.6,7 It is a small molecule (151 Da). Its commercial development occurred in the USA in the 1950s. Here, the product went on sale in the United States in 1955 under the brand name “Tylenol”.8
Unlike opioid analgesics, it was early appreciated that acetaminophen does not generate euphoria or mood alteration. It has, over decades of use, been appreciated to be without risks of sedation, addiction, dependence, tolerance and withdrawal when administered alone.9–12 The principal limitation is that in large amounts over time, acetaminophen can result in the formation of hepatotoxic metabolites.13,14 Its general tolerability, lack of abuse potential and, as discussed below, efficacy has led to its appreciation as a therapeutic with an important role in pain management. As such, it is one of the most commonly employed analgesic molecules with over 25 billion doses delivered annually in the US alone.15,16 In spite of its widespread use, its mechanisms of action remain controversial.17
This narrative review looks to consider issues related to site and mechanism of action. It is organized into three parts: 1) an overview of the clinical efficacy of acetaminophen; 2) a review of the effects of acetaminophen in animal models of acute nociception, after tissue injury and nerve injury following per os (PO), intravenous (IV), intrathecal (IT), intracerebroventricular (ICV) and peripheral routes of delivery; and 3) a summary of mechanisms by which acetaminophen (and/or its metabolites) exert its analgesic actions.
Analgesic Efficacy of Acetaminophen in Humans
While acetaminophen is often times considered dismissively as a weak or minimally efficacious therapeutic, clinical studies often show that it compares favorably to other analgesic regimens in the management of a variety of pain states. Clinically, acetaminophen is available for oral, rectal and IV delivery. Not surprisingly, higher plasma concentrations are achieved with the shortest latency after IV delivery18,19 and peak cerebrospinal fluid concentrations are significantly greater with IV administration than with PO.20
Experimental Pain
The analgesic effects of acetaminophen have been studied in experimental pain models in humans. In double-blinded and placebo-controlled trials, electrical stimulation at high current densities induced spontaneous acute pain and distinct areas of hyperalgesia for painful mechanical stimuli (pinprick hyperalgesia). IV acetaminophen (650 mg), tramadol (75 mg) or a combination of both (325/37.5 mg, respectively) was administered. Tramadol led to a maximum pain reduction of 12% with negligible antihyperalgesic properties. In contrast, acetaminophen led to a similar pain reduction (10%), but surprisingly displayed a sustained antihyperalgesic effect.21
Inflammatory and Postoperative Pain
PO doses of 1000 mg of acetaminophen are reported to result in modest, but statistically significant reductions in mild to moderate acute pain states with etiologies ranging from acute soft tissue injury (sprain),22,23 major surgeries,24,25 head ache,26 total hip or knee replacements27 and hip or knee osteoarthritis.28,29 The use of IV acetaminophen has been reported to be well tolerated and efficacious in well-powered, prospective and retrospective trials and to result in significant decreases in postoperative morphine consumption and pain intensity after a variety of surgical interventions including orthopedic,30–33 dental,34 spinal fusion,35 abdominal laparoscopic interventions,36 post bariatric,37 C-section and hysterectomies,38–42 cardiac surgery,43 and head and neck cancer surgery.44 IV acetaminophen reduced the likelihood of readmission after 30 days following knee arthroscopy.45 This raises the possibility that the actions of acetaminophen reflect disease modifying actions that alter the transition from an acute to a chronic pain state hypothesized to reflect a role of innate/adaptive immune systems.46 Less promising results have also been reported,47 concerns of toxicity remain48 and the superiority of IV vs PO acetaminophen has been questioned.49
Neuropathic Pain
While there are surprisingly few studies reporting efficacy of acetaminophen alone in mono and poly neuropathic pain states, work has emphasized that opiate–acetaminophen combinations reveal synergy yielding increased utility in a variety of pain states including, not only in osteo and rheumatoid arthritis,50,51 but in diabetic neuropathy.52 In contrast, in cancer pain, addition of acetaminophen did not affect the analgesic effect of methadone or morphine.53,54
Alternate Routes in Human Acetaminophen Delivery
While meta-analyses often emphasize the lack of “high quality evidence” in many of the effects of acetaminophen (by any route), particularly for persistent pain states (eg, back pain, hip or knee osteoarthritis and cancer),28,44,55,56 IV acetaminophen has been formally approved for mild-to-moderate pain and moderate-to-severe pain with adjunctive opioid analgesics in Europe and more recently in the USA.57 Thus, the efficacy of IV acetaminophen relative to placebo has been shown in controlled postoperative trials where patient satisfaction with acute postoperative pain control was rated through 24 h after dosing. Patients receiving IV acetaminophen reported excellent satisfaction more often than those receiving placebo and was the strongest predictor of patient satisfaction.58,59 Of note, clinical trials on the use of intrathecal acetaminophen in knee and hip procedures (ClincialTrials.gov, 2016) prepared in a novel supersaturated formulation are currently registered, though no data have as yet been reported.60
Key Points Regarding Human Action of Acetaminophen
Four clinical observations are of potential significance as to the activity and mechanisms of action of acetaminophen:
1) CSF sampling after acetaminophen reveal high levels within 10 min after an IV delivery with peak concentrations being lower and delayed after PO administration.20,61
2) Acetaminophen reduced the areas of secondary hyperalgesia to pinprick and touch otherwise observed after peripheral electrical stimulation. These results suggest an effect independent of the presence of peripheral injury/inflammation leading to a hyperalgesic state and suggest an effect upon central processes underlying sensitization.62
3) Importantly, brain imaging has further confirmed the effects of analgesic doses of acetaminophen on brain responses to aversive stimulation. Human studies with fMRI have revealed that acetaminophen reduces the response to noxious thermal stimulation as compared to placebo in prefrontal cortices, insula, thalami, anterior cingulate cortex and periaqueductal gray matter, leading to the suggestion of an inhibitory effect of acetaminophen on spinothalamic outflow.29 Similarly, in subjects with knee osteoarthritis, acetaminophen reduced blood oxygenation level dependent signal activation in the sensory cortex and supramarginal gyrus, prefrontal and frontal cortex, and insula.63 Thus, while acetaminophen efficacy has been questioned in the management of osteoarthritis pain,64 it is clear that it has state dependent effects upon neuraxial processing.
4) Systematic analysis of plasma levels after acetaminophen dosing and the magnitude of the opioid sparing effects in postoperative pain point to a ceiling effect of the effect of even IV acetaminophen on postoperative pain.65
5) While acetaminophen has minimal effects other than altering nociception, recent work has suggested that, in addition, acetaminophen may have broader psychological effects. Thus, acetaminophen has been shown to reduce affective responses to both negative and positive emotional images235 and reduced the neural responses associated with experiences of acute applic pain.236,237
Analgesic Efficacy of Acetaminophen in PreClinical Models
Routes of Delivery
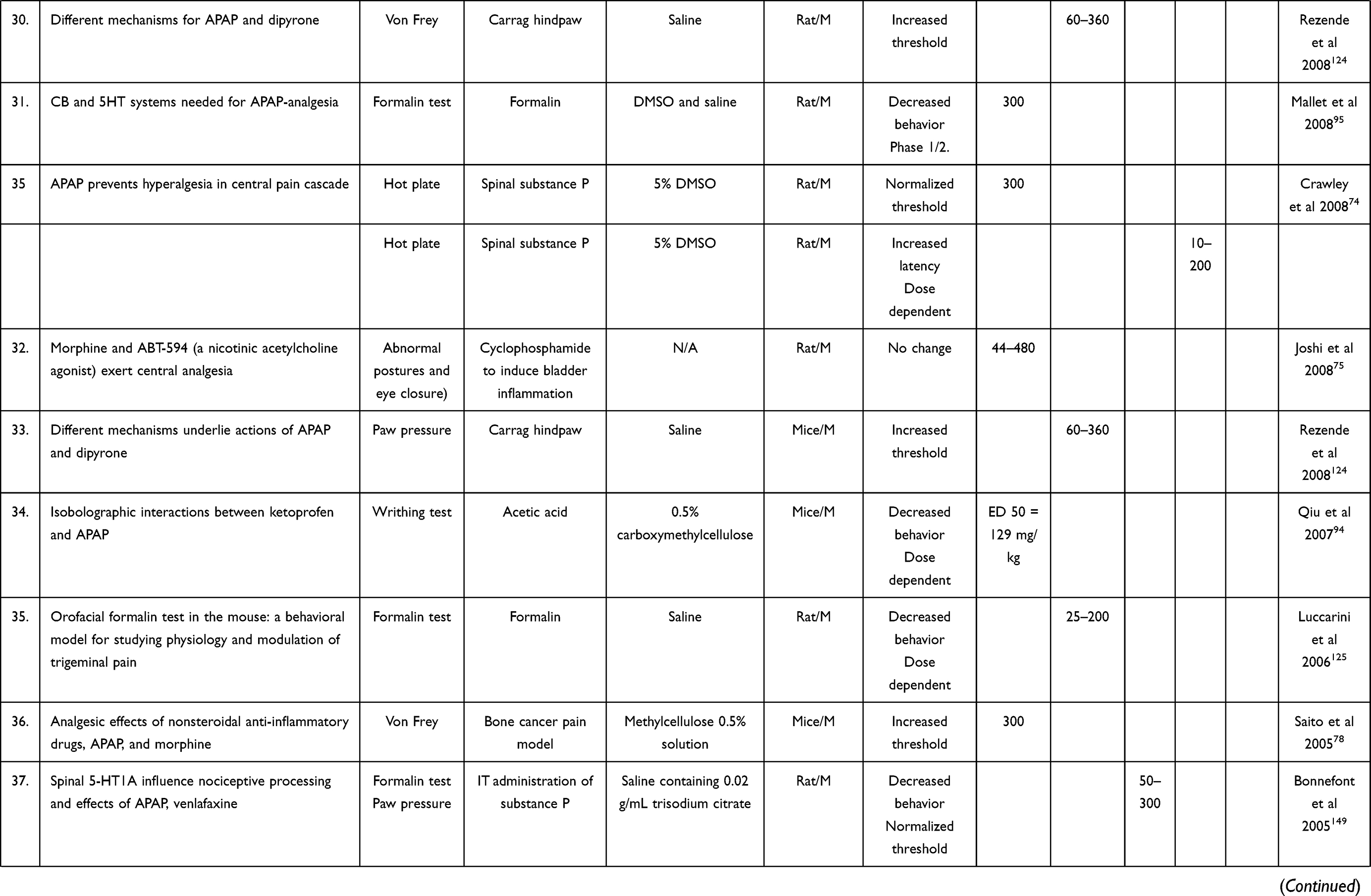
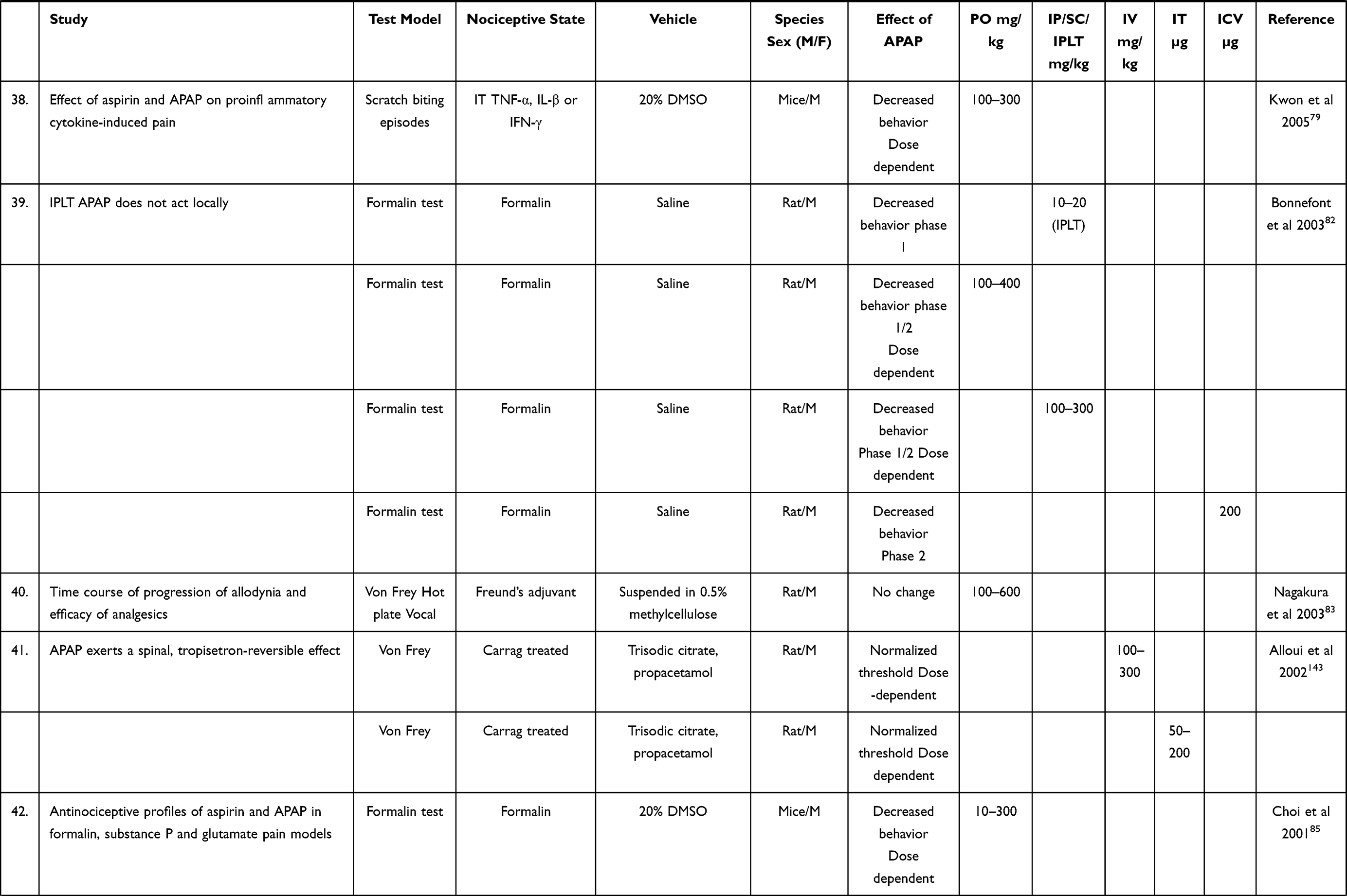
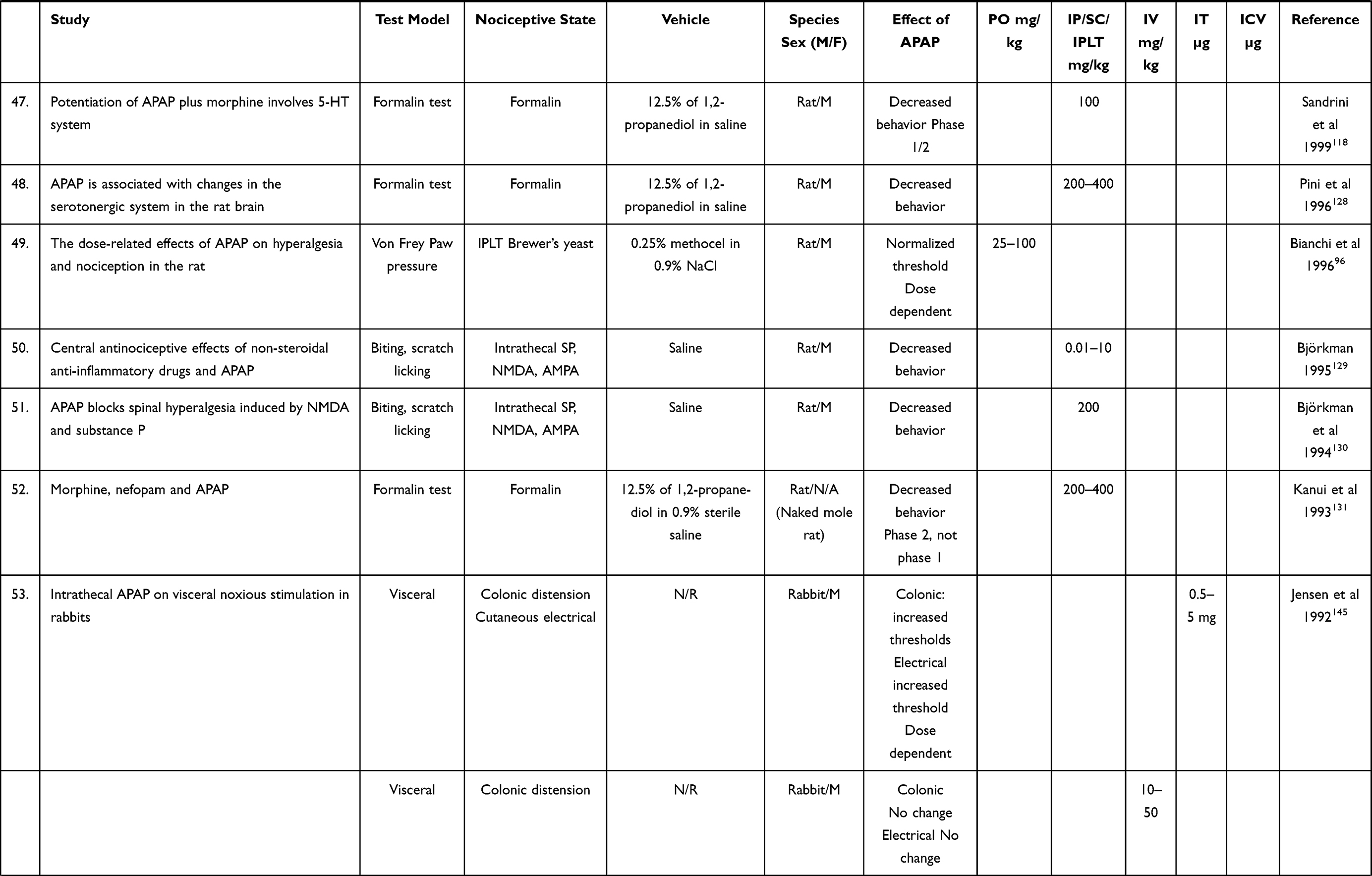
As presented in Tables 1–3, we found 99 preclinical studies on analgesia of acetaminophen when retrieved on an electronic database using the following search phrases: ((“acetaminophen”[MeSH Terms] OR “acetaminophen”[All Fields] OR “paracetamol”[All Fields]) OR (“acetaminophen”[MeSH Terms] OR “acetaminophen”[All Fields])) NOT (“liver”[MeSH Terms] OR “liver”[All Fields]) AND “animals”[MeSH Terms: noexp]. The systematic search was undertaken through 9 September 2019. These are summarized by pain models in the tables. Among them, 41 studies involved oral administration of acetaminophen,66–105 38 studies with intraperitoneal injection,73,76,86,102,106–140 13 studies with intrathecal administration,74,87,121,132,141–147 12 studies with intravenous administration,82,87,107,134,143,145,148–153 5 studies with intracerebroventricular administration89,126,135,146,154 and with local subcutaneous in the paw,82,126,135,155,156 7 studies with subcutaneous administration124,141,157–161 and 1 study with rectal administration.98
 |
 |
 |
 | |
Table 1 Preclinical Analgesic Effect of Acetaminophen by PO, IT, IP/SC, IV, IT, ICV Administration in Acute Nociception |
 |
 |
 |
 |
 |
 |
 |
 |
 |
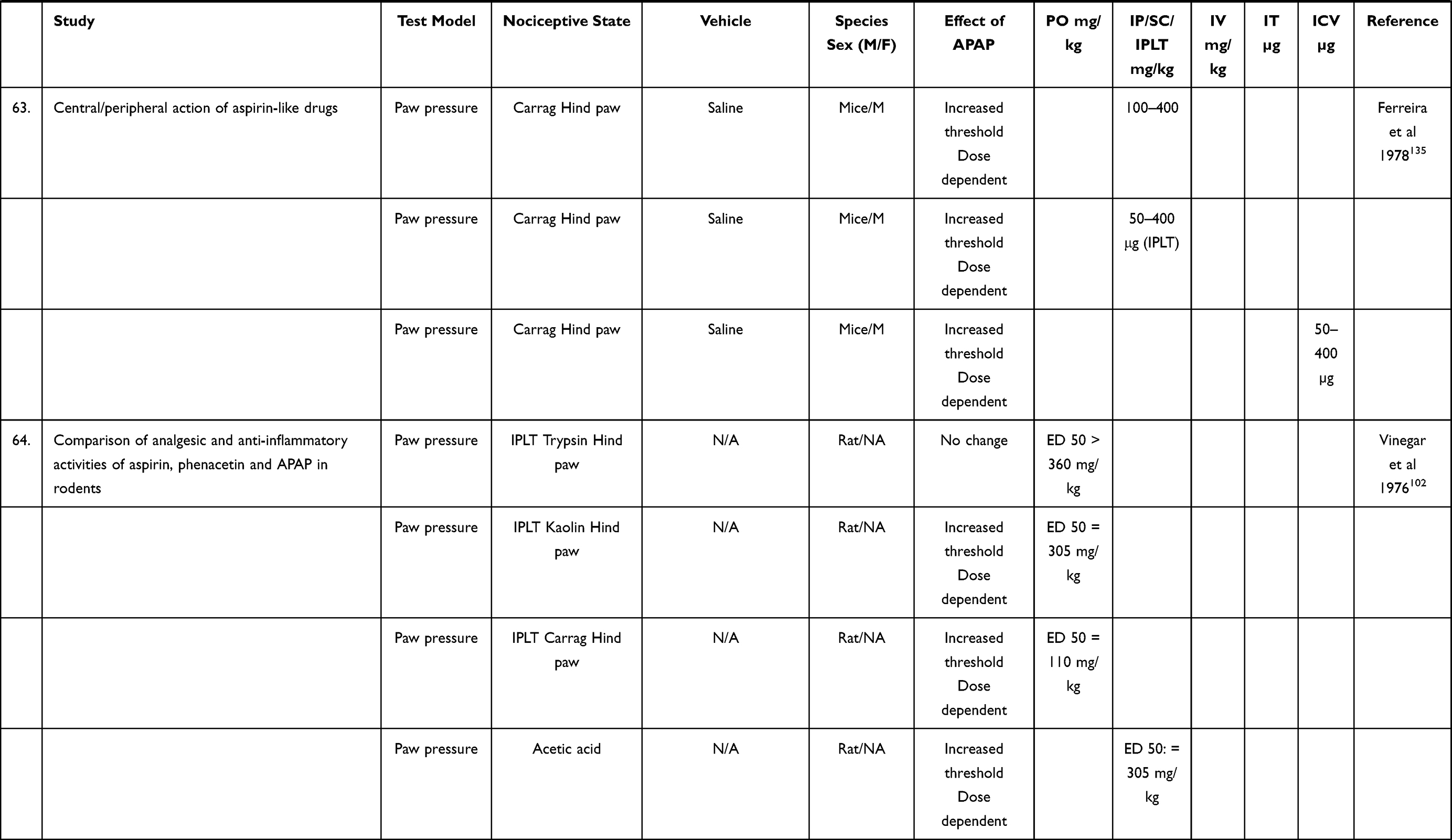 |
Table 2 Preclinical Analgesic Effect of Acetaminophen by PO, IT, IP/SC, IV, IT, ICV Administration in Tissue Injury and Inflammation |
 |
Table 3 Preclinical Analgesic Effect of Acetaminophen by PO, IT, IP/SC, IV, IT, ICV Administration in Neuropathic Models |
Formulation
Acetaminophen is freely soluble in alcohol; soluble in methanol, ethanol, dimethylformamide, ethylene dichloride, acetone, ethyl acetate; slightly soluble in ether; and practically insoluble in petroleum ether, pentane, and benzene.162 Solubility in water at 25 °C is 14 mg/mL, and water solubility is markedly increased with heat.162,163 While acetaminophen is very stable at room temperature, acetaminophen degrades rapidly to p-aminophenol and undergoes oxidative modifications at elevated temperatures in the presence of oxygen.164–166 The development of a stable supersaturated concentration of acetaminophen has been described.60 The normal limited solubility of acetaminophen in water typically has required utilization in preclinical studies of a variety of vehicles and additive to increase solubility or wettability including dimethyl sulfoxide (DMSO), dimethylformamide (DMF), propylene glycol (PG), ethanol, Cremophor and Tween 20 with varying degrees of biological compatibility and typically with poorly described pharmacokinetics. Control data, baseline responses were typically examined with the respective vehicle.167
Acute Nociception
The acute application of thermal or mechanical stimulus above a threshold intensity will evoke a homotopic withdrawal or escape response (eg, stimulation of the left hind paw will result in a withdrawal of the left hind paw). The effects of APAP delivered by various routes are summarized in Table 1.
Thermal
Behavioral Model
Thermal responsivity may be assessed by applying a thermal stimulus to the body surface and assessing the latency to withdraw the stimulated part or escape. Application of heat to the rodent tail leads to a “tail flick”, a model with a strong reflex component.168 Withdrawal of the hind paw is typically assessed by the placing of the animal on a uniformly heated surface (hot plate) maintained at a surface temperature typically between 48* and 55 °C with the measured end point being latency to a licking of the hind paw or a jumping from the surface.169 An alternate model, referred to as the Hargreaves model, employs focusing a light source under one or the other hind paws of an animal placed on a glass plate, with the latency to withdrawal of that paw being the measured end point.170 These thermal models are considered to reflect the acute activation of high threshold nociceptive afferents.171
Drug Effect
Significant increases in hind paw thermal escape latencies over baseline were observed over a range of dose 500–850 mg/kg in the rat or mouse.68,73,76,77 Tail flick latencies were significantly elevated in mice after PO administration of acetaminophen (400 mg/kg).66 Orally administered acetaminophen inhibited tail flick in a concentration-dependent manner (97–772 mg/kg).98 IT acetaminophen (50 and 100 μg/rat) showed significant elevations in hind paw escape latencies on the hot plate test.74,141
Mechanical
Behavioral Model
Mechanical compression of the paw is accomplished by a progressively increasing pressure progressively applied through a blunt probe to the paw situated on a non-compliant surface. This model referred to as the Randall–Selitto test is a classical way to measure mechanical thresholds.172 The pressure which leads to hind paw withdrawal is the measured end point. In this case, the threshold response generated by the blunt stimulus surface is considered to be mediated by high threshold nociceptors lying in the muscle and bone of the compressed tissue.171 A variant stimulus involves the application of a small diameter probe (von Frey hairs) to the plantar surface and the stimulus resulting in withdrawal is considered to be the threshold. In the absence of inflammation it is considered that the withdrawal, in contrast to the Randall–Selitto paradigm, is mediated by the activation of superficial terminals of high threshold cutaneous afferents.172
Drug Effect
Pressures leading to paw withdrawal were significantly elevated in mice and rats with acetaminophen in doses in the range of 200–800 mg/kg.76,81,84,87,173 Increases in thresholds were found in rats at 200 mg/kg.73 IV acetaminophen (22–724 mg/kg) did not alter by mechanical stimulation thresholds in rats,150 and IV acetaminophen (50–300 mg/kg) resulted in a dose dependent elevation in the compression required to produce a withdrawal response.87,149 Similar results were observed in rats after a single IV dose of acetaminophen (200 mg/kg).151 IT acetaminophen (100 or 200 μg/rat) produced a significant increase in baseline paw compression thresholds,87 a finding confirmed at lower IT acetaminophen doses (50 and 100 μg/rat).141
Electrical Stimulation
Behavioral Model
An electrical stimulus may be applied through subcutaneous electrodes (typically in the paw). The threshold electrical stimulus which evokes one of several specified responses (vocalization, flinch, escape) is the measured variable.171
Drug Effect
The stimulus evoked vocalization was reduced by PO (50,400 mg/kg) and ICV (50–400 µg) acetaminophen in both normal and adjuvant arthritic rats. The equipotent doses were less in the inflamed than the normal rat.89 ICV administration of acetaminophen at 25–400 μg dose-dependently inhibited the withdrawal initiated by hind paw stimulation electrical stimulation in both normal rats and adjuvant arthritic rats.89 Consistent with these effects of acetaminophen, experiments were carried out on rats under urethane anesthesia in which neuraxial activation was elicited by supramaximal electrical stimulation of sural nociceptive afferents and the activation of single neurons in the dorsomedial part of the ventral nucleus (VDM) of the thalamus was observed. IV acetaminophen (5–25 mg/kg) reduced nociceptive-evoked activation of these neuron in the VDM thalamus.174 ICV administration of acetaminophen displayed potent analgesic actions in rats.89
Facilitated States of Nociceptive Processing
A common observation is that certain interventions may lead to an enhanced response to mildly noxious stimuli (hyperalgesia) or a significant pain response to an otherwise innocuous stimulus (allodynia). In the latter case, the common end point is the behavioral response to a low intensity tactile stimulus (as applied through application of von Frey hairs) and hence referred to as tactile allodynia. These facilitated states may occur as a result of direct central sensitization (as with an intrathecal or neuraxial treatment) or after tissue inflammation or nerve injury.
Neuraxially Evoked Spontaneous and Facilitated Behavioral Pain States
Spontaneous Behaviors
Behavioral Model
The intrathecal (spinal) delivery of a variety of afferent transmitters (eg, substance P and glutamate) and pro-inflammatory cytokines (TNF-α, IL-β or IFN-γ) will initiate acute pain behaviors as biting of the body surface, agitation or vocalization as well as robust facilitated states. The behavioral relevance of these facilitated states is evidenced by an increased sensitivity to mechanical (touch) and thermal stimulation. As this enhanced responsiveness is initiated by an action within the spinal cord, systemic drugs blocking that hyperalgesia are considered to reflect their central effect upon neuraxial mechanisms of nociceptive processing.
Drug Effect
Biting and scratching in the rat after intrathecal substance P and glutamate and the response time were reduced in a dose dependent fashion by PO acetaminophen (10–300 mg/kg).85 The scratching and biting episodes evoked in the mice by IT TNF-α, IL-β or IFN-γ were reduced in a dose dependent fashion by PO acetaminophen (100–300 mg/kg).79
Facilitated Pain States
Behavioral Model
The intrathecal delivery of agents such as substance P will evoke an increased response to an otherwise innocuous or mildly aversive stimulus.
Drug Effect
Thermal hyperalgesia evoked by IT substance P examined in rats was significantly reduced after PO acetaminophen (30–300 mg/kg).74 These results support the assertion that a component of the effects of systemic acetaminophen reflect an effect upon neuraxial nociceptive processing.
Inflammation Induced Facilitated States in Somatic Tissues
Generation of inflammation in soft tissue and joints routinely leads to a hyperalgesic state. This enhanced responsiveness reflects the appearance of a variety of proinflammatory products in the local injury milieu. These products, often acting through eponymous receptors expressed on the terminals of the primary afferent, serve to depolarize the terminal and through the activation of local kinases enhance the sensitivity of the terminal to subsequent stimulation.175,176 These changes lead to ongoing afferent traffic, which leads to the initiation of a state of spinal sensitization. Such a state leads to an enhanced input–output function of the dorsal horn and a state of spinal facilitation.177 This scenario is common to virtually all of the inflammatory motifs in soft tissue and joint.
Local Inflammation and Somatic Pain
Behavioral Model
Intraplantar or intra-articular injections of carrageenan, uric acid or injections of adjuvants such as complete Freund’s adjuvant (CFA) result in a robust ipsilateral (if local) or bilateral, if systemic, inflammation and an associated thermal and mechanical hyperalgesia and tactile allodynia.
Drug Effect
The hyperpathia, but not the inflammation, is significantly reduced by PO acetaminophen.8 In rats rendered hyperalgesic with adjuvant arthritis, PO acetaminophen (50–400 mg/kg) attenuated the withdrawal response otherwise evoked by stimulation of electrical stimulation in adjuvant arthritic rats.89 In rats rendered arthritic with intra-articular injection of uric acid in the knee, PO acetaminophen (178–562 mg/kg) resulted in a significant analgesic effect, quantified as the recovery of a functionality index.88 On the other hand, PO acetaminophen (100–600 mg/kg) had only modest effects in the CFA-induced arthritic rat model, as measured by tactile or thermal escape latencies.83,104 IV acetaminophen (100–300 mg/kg) showed a significant reduction in the tactile with no change in paw swelling, for about 60 minutes compared to the control (vehicle). After ICV delivery, acetaminophen produced a dose dependent (50–400 µg) reduction in the hyperalgesia evoked by intraplantar carrageenan in mice.135 IT acetaminophen (50–200 μg) resulted in a dose dependent normalization of tactile allodynia in the carrageenan rat paw.143 Intraplantar acetaminophen (50 and 400 μg) of acetaminophen in mice rendered hyperalgesic with intraplantar carrageenan reversed the hyperalgesia in a dose dependent manner in the paw pressure test.135
Plantar Incision
Behavioral Model
The creation of an incision of the plantar surface of the rodent is considered to mimic a postoperative state where there has been a skin incision and an underlying muscle retraction with an associated inflammation secondary to the wounding.178
Drug Effect
PO acetaminophen resulted in a robust dose dependent analgesic effect in mice (200–600 mg/kg)72 and rats (30–180 mg/kg) after plantar incision.69
Formalin Evoked Flinching
Behavioral Model
Injection of a small volume of formalin into the dorsum of the rodent paw results in a biphasic flinching. The first phase is considered to reflect behavior evoked by the acute afferent drive from the injected paw while the second phase represents a response mediated by the low-level input arising from the injected paw and a state of spinal facilitation initiated by the first conditioning barrage.179
Drug Effect
Systemic acetaminophen typically results in a robust dose dependent suppression of phase II formalin and to a lesser degree phase I in mice (10–300 mg/kg)73 (60) and rats (100–400 mg/kg)82 but71 IV acetaminophen shows analgesic effect in phase I only at high concentration (300 mg/kg) in rats. Phase II shows analgesic effects at doses of 100–300 mg/kg.82,149 ICV acetaminophen had no effect upon phase I but significantly reversed phase II in rats.126 IT administration of acetaminophen (4.5–45 µg) in the rat was observed to be effective in phase II.132 IPL acetaminophen (5–200 μg) had no effect upon either phase I or phase II formalin flinching in the rat formalin test in rats.82,126
Inflammation Induced Facilitated States in Visceral Tissues
Mechanical distention of hollow organs, eg colon/bladder, application of irritants to the peritoneal cavity or the hollow organs, will lead in a pressure dependent fashion to ongoing pain behavior characterized by vocalization, autonomic responses increased abdominal muscle tone and pressing of the abdomen against the floor of the chamber. Such inflammation will lead to a sensitization of the system such that even minor mechanical stimulation will lead to enhanced responses.138,180
Peritoneal Irritants
Behavioral Model
Delivery of irritants such as dilute acetic acid, capsaicin or phenyl benzoquinone into the peritoneal space will result in abdominal constriction in mice and rats,86,107,121 reflecting activation of polymodal nociceptive afferent innervating the peritoneal wall. Distention of hollow organs will yield similar somatomotor response, and the threshold for generating these responses is lowered in the face of colonic inflammation.181
Drug Effect
IP acetaminophen delivered in mice treated with IP acetic acid (ED 50 = 49.5 mg/kg) significantly reduced abdominal constriction in a dose dependent fashion.121 ICV acetaminophen in mice (45–150 µg) suppressed the abdominal constriction response generated by IP acetylcholine.154 IT acetaminophen in mice produced a dose dependent antinociceptive activity in the acetic acid-induced writhing model.121,154 In rabbits, intestinal distension of the distal colon led to a somatic-affective pain response that was reduced in a dose dependent fashion by IT acetaminophen (500–5000 µg).145
Bladder Irritants
Behavioral Model
Acute inflammation of the bladder generated by intra-vesicular installation of an irritant such as cyclophosphamide, or a bacterial infection, leads to an ongoing biting and scratching and a hyperalgesic state with a robust referred somatic pain component.182 This hyperpathic state is mediated by a significant in-migration of inflammatory cells and degranulation of intrinsic mast cells with an associated release of proinflammatory cytokines. Over extended periods, sprouting of bladder afferents is observed and there is a hypertrophy of the urothelium. In the dorsal horns there is an associated activation of astrocyte and microglia,182,238 and PO acetaminophen (45–450 mg/kg). A model of bladder inflammation-induced hyperalgesia displayed no analgesic effect.75
Bone Cancer Pain
Behavioral Model
Bone cancer models typically employ placement of syngeneic cancer cells into the marrow of either the femur or the tibia.183 These osteolytic sarcoma cells initiate remodeling of the bone, a significant sprouting of polymodal nociceptors into the intramedullary environment and an associated reorganization of the spinal dorsal horn that provides the sensory to innervation of the cancerous bone and this leading to a neurochemical profile resembling a robust neuropathic pain state.184
Drug Effect
PO acetaminophen (300 mg/kg) attenuated the tactile allodynia otherwise noted in the mouse bone cancer pain model.78
Nerve Injury Induced Facilitated States
Mononeuropathies
Behavioral Model
These nerve injuries reflect an injury restricted to a nerve trunk or its distribution (eg, L5 ligation (spinal nerve ligation – Chung model), hemiligation of the sciatic nerve (Seltzer model), or loose ligatures placed around the sciatic nerve (chronic compression injury – Bennett model), or ligation of the distal branches of the sciatic (spared nerve injury)). Commonly, rats or mice with these interventions will display a robust tactile and cold allodynia. The underlying mechanism of this hyperpathic state reflects upon the development of neuromas at the site of injury and reactive changes in the dorsal root ganglion of the injured nerve, leading to the development of ongoing afferent traffic from the neuroma and the DRG. These events are accompanied by prominent activation of dorsal horn neurons and glia.137,185
Drug Effect
IP acetaminophen (25–300 mg/kg) dose-dependently, suppressed induced pain in thermal hyperalgesia, mechanical, and cold allodynia in L5 ligated rats.122 Neither IV not IT acetaminophen (2.3–145 mg/kg) significantly reversed the allodynia otherwise observed in the nerve ligated rat.148 Of note, IPLT acetaminophen in the rat Seltzer model ligation neuropathy dose-dependently decreased mechanical allodynia and lowered nociceptive scores associated with hyperalgesia testing155 (see Table 3).
Polyneuropathy
Behavioral Effect
Clinical syndromes such as diabetes and chemotherapeutics can give rise to a distal-symmetric sensory neuropathy with sensory loss, paresthesia and dysesthesia, and is only incompletely reversible.186 Painful diabetic neuropathy is characterized by spontaneous tingling, lancinating, pain that frequently occurs in conjunction with touch-evoked pain and numbness.187 The mechanisms underlying these events are multifocal and include changes in peripheral terminals and DRG morphology and trophic changes in dorsal horn connectivity leading to a facilitated response to otherwise innocuous stimuli.188,189
Drug Effect
PO acetaminophen (151–2265 mg/kg) showed an antinociceptive effect on the vincristine-induced neuropathic pain rat model.80 In addition, oral administration of acetaminophen (5–100 mg/kg) has an antinociceptive effect on the streptozotocin induced diabetic model.103
Preclinical to Clinical Dose Comparisons
The focus in this review has been characterizing the profile of acetaminophen based on published literature. An important point of consideration related to whether these observed effects of acetaminophen dosing are relevant to the human conditions. The issue of dose comparability across species has particular relevance in drug development. In the present case it is evident that dosing in the rodent reveals activity at substantial dose levels. A nominal dose level that is common in those studies where acetaminophen was shown to be efficacious is on the order of 300 mg/kg which would appear substantial. It is beyond the scope of this review, but we would note that there is significant support for the assertion that allometric scaling across species might be more closely approximated through comparisons based on body surface area.190,191 Thus, the typical systemic acetaminophen dose in the rat is on the order of 300 mg/kg. Converting the rat mg/kg dose to a human mg/kg dose on the basis of a body surface area conversion of the rat dose where the rat dose is divided by the body surface area scaling factor (6.2) yields a predicted human dose of 48 mg/kg.192 It is noteworthy that the approved IV dose in humans is 4000 mg/70 kg = 57 mg/kg. Such scaling has been shown to be useful for drawing first order comparisons across species.
Mechanisms of Acetaminophen Action
Metabolism
Acetaminophen (pKa: 9.5) at physiological pH is essentially neutral and is rapidly absorbed after PO delivery. In humans, blood half-life ranges from 1.5–3 h at therapeutic half-lives to 8 h at dose up to 4 g/day.193 Similarly, in the rat half-lives are dose dependent and range from approximately 15 min at low doses and up to 120 min after high (therapeutic) doses (300 mg/kg).194 In all species, elimination largely occurs in the liver, where the majority of the drug undergoes conjugation catalyzed by a variety of transferases and then excretion in urine. The formation of toxic metabolites, such as N-acetyl-p-benzoquinone imine (NAPQI), occurs secondary to this sequence.195 More recently it has been shown that acetaminophen, following deacetylation to its primary amine (4-aminophenol), is conjugated with arachidonic acid through the actions of fatty acid amide hydrolase in the brain and spinal cord to form a variety of biologically active molecules.196 This will be discussed further below.
Mechanisms of Analgesic Action
A number of mechanisms have been hypothesized for the actions of acetaminophen in modulating pain transmission. Broadly speaking, these effects can be considered in terms of an effect of the drug itself or an action mediated by a metabolite. In the human, acetaminophen is known to be metabolized in the liver into p-aminophenol and then converted to N-(4-hydroxyphenyl)-arachidonamide (AM404) via fatty acid amide hydrolase (FAAH) and into N-acetyl-p-benzoquinone imine (NAPQI) via cytochrome P450 (CYP) enzymes.196–198 While this conversion typically occurs in the liver, recent work has shown that acetaminophen can be converted into the AM404 metabolite within the neuraxis.61
Membrane Target
Measurement of acetaminophen levels in the brain revealed significant tissue/blood ratios that were essentially the same across the brain.199 Quantitative autoradiography has failed to demonstrate that acetaminophen binds specifically to any area of the murine brain or spinal cord.200 Competition studies with a variety of targets failed to show interactions with a variety of monoamine receptors or opioid receptors.201
Cyclooxygenase Inhibition
Prostaglandins play an important central and peripheral role in sensitizing systems which are involved in nociceptive transmission.202 The prostanoids are formed by the actions of constitutive (COX1) and inducible forms (COX2) of cyclooxygenase. Common non-steroidal anti-inflammatory drugs (NSAIDs) such as acetylsalicylic acid, or ibuprofen, block activity of these isoforms.203 While a literature has suggested acetaminophen may inhibit cyclooxygenase, minimal evidence supports a direct effect.147,204–206 This assertion is consistent with the side effect profile for acetaminophen, which does not include effects commonly associated with COX1 inhibition known on the gastrointestinal tract, platelet activation, and kidney functions and with COX2 on cardiovascular, gastrointestinal and kidney function.207,208 One explanation for this distinction is that acetaminophen may act as a CNS-COX inhibitor, whereas the other COX inhibitors act both centrally and peripherally. In this regard, acetaminophen acts to interfere with the peroxidase activity of COX2. This interaction is particularly manifest when the cellular environment is low in arachidonic acid and peroxides and may reflect the “central” effects where constitutively expressed COX2 at the spinal level plays a principal role in initiating facilitated states,209,210 and why it appears to display less activity in inflamed tissues (where peroxides and arachidonic acid are highly concentrated). In this regard, acetaminophen inhibits conversion of arachidonic acid to Prostaglandin (PG) E2, PGF2 and thromboxane‐A2 in microglia exposed to lipopolysaccharide211 at 3‐fold lower concentrations in microglia than in peripheral macrophages. A further point is that recent work has suggested that AM404, the downstream metabolite of acetaminophen, can inhibit isolated cyclooxygenase (COX)-1 and COX-2 enzymes and prostaglandin synthesis in macrophage cultures and in brain slices.196,212,213 AM404 is also a potent inhibitor of T cell activation and inhibited TNF gene transcription and protein synthesis, thereby regulating activation of several transcription factors including nuclear factor-kappa B (NF-κB).214
TRP Signaling
The acetaminophen metabolite AM404 can bind to the vanilloid binding site and activate the transient receptor potential vanilloid 1(TRPV1) channel in dorsal root ganglia (DRG) neurons.215,216 Moreover, the antinociceptive effects of acetaminophen are absent in TRPV(1) knockout mice.73 Activation of TRPV1 can lead to inhibition of downstream excitatory T-type calcium channels70. NAPQI, the toxic liver metabolite of acetaminophen, has been shown to activate TRPV1.216 Further, acetaminophen and the metabolite NAPQI sensitizes and activates transient receptor potential ankyrin 1 (TRPA1) slowly but directly by interacting with distinct intracellular cysteine residues.217,218 This TRPA1 activation paradoxically serves to reduce voltage-gated calcium and sodium currents in DRG neurons, while intrathecal acetaminophen and NAPQI produced anti-nociception that was absent in TRPA1 KO mice.141
An important caveat is that the activation of TRP receptors is generally associated with adverse events including activation of pain signaling. It should be noted that NAPQI will result in neurogenic inflammation, which indeed suggest that such metabolites would serve to activate small peptidergic nociceptive afferents.218 If the actions of acetaminophen action are indeed mediated through such signaling, then one would similarly anticipate adverse pain components, which to date have not been noted.
Cannabinoid Signaling
The effects of acetaminophen are reportedly blocked by Cannabinoid (CB) 1 receptor antagonism and by CB1–/– transgenic mice.77,95 This effect is believed to reflect the fact that acetaminophen, by its metabolite AM404, also exerts a possible effect on the endocannabinoid system by acting as a ligand at cannabinoid CB1 receptors, or as an inhibitor of anandamide uptake, an endogenous agonist for CB1 receptors.219,220
Anandamide (AEA) is an endocannabinoid that activates CB1.221,222 AEA is degraded by fatty acid amide hydrolase (FAAH), the enzyme that metabolizes acetaminophen into AM404. Thus, AM404 could act as a competitive inhibitor of FAAH and indirectly activate CB1. Alternatively, AM404 has been shown to inhibit FAAH-like anandamide transporter, a membrane-bound variant of FAAH lacking its hydrolase activity, which is present on neurons and glia and is thought to aid in intracellular transport of AEA.223 By inhibiting FAAH, AM404 could increase levels of AEA available in the synaptic cleft. The insensitivity of CB1 knockout mice and rats pretreated with the CB1 antagonist (AM251) to acetaminophen supports the involvement of CB1 in the mechanism of acetaminophen.95,224 AEA has been reported to activate CB1 receptors on cultured DRG neurons.225,226
As with the hypothesis that acetaminophen alters COX formation while the molecule is not associated with many biological effects associated with COX inhibition, cannabinoids have been shown to have both robust negative and positive reinforcing properties and to produce dependence.227,228 In marked contrast, it is of note that in animals229 and in humans, acetaminophen alone has no established positive or adverse rewarding properties or diversion potential.230
Serotonin Signaling
Several lines of investigation have suggested that acetaminophen may exert its effects through serotonin transmission. As acetaminophen displays little or no affinity for 5-HT receptors, or for neuronal reuptake sites,201 these actions have been argued to reflect an indirect effect notably by a brainstem action altering activity in bulbospinal serotonergic projections. Thus, destruction of bulbospinal 5-HT projections is reported to attenuate the antinociceptive action of acetaminophen.128,133 An important issue is whether the effects of acetaminophen reflect an increase or a decrease in the activation of the bulbospinal projection. It has been reported that acetaminophen increases 5-HT levels in rat brain.128 Such an increase may be interpreted as having increased serotonin to be released. It is equally consistent with the notion that acetaminophen is decreasing terminal release leading to accumulation. In this regard, bulbospinal serotonin projections have been said to facilitate dorsal horn processing leading to hyperalgesia, likely mediated through an excitatory 5-HT receptor such as 5-HT3.231 Others have argued that activation of the descending pathway may lead to a block of dorsal processing by activating a G protein coupled inhibitory 5-HT receptor (eg, 5-HT1 isotypes). Other possibilities are that serotonin, through an excitatory receptor (5-HT2, 3, 7), may activate an inhibitory interneuron such as GABA232 or encephalin,233 as suggested by the report of naloxone sensitivity of acetaminophen antinociception to naloxone, an opioid.234 In the case of acetaminophen, the literature is complex and controversial. Thus, IT 5-HT1B, 5-HT2A/C and 5-HT7 antagonism has been reported to reduce acetaminophen actions.72,151 IT 5-HT3 antagonism has been reported to inhibit the antinociceptive effects of acetaminophen in various pain models87,143,151,173 and specific knock down with 5-HT3 receptor antisense did not alter acetaminophen antinociception.173 In humans, pain reports by median nerve stimulation were significantly reduced by acetaminophen, and this effect was reduced vs control by 5-HT receptor antagonists.235
Concluding Comments
“The current evidence supports the assertion that acetaminophen has a behaviorally relevant, but delimited, analgesic effect in humans and in a variety of preclinical models.” While mechanisms of action remain arguably controversial, the effects of acetaminophen on centrally evoked facilitated states (as after IT sP) and on aversive electrical stimulation strongly support the conclusion that at least a component of the effects of systemic acetaminophen reflect an effect upon CNS nociceptive processing that engage both spinal and supraspinal systems in humans and animals. The long history of acetaminophen in showing a highly desirable side effect profile and the absence of abuse potential is consistent with its wide use as an over-the-counter medication. Though it may possess deleterious effects upon liver function with persistent high-level use, it is surprisingly well tolerated in this regard in humans. A number of proposed mechanisms exist involving serotonin, cannabinoids and TRP signaling, while these mechanisms appear interesting and relevant, they are noteworthy in the absence of effects such as rewarding potential and absent any activating effects that such actions would endow the parent compound. It is the authors' opinion that the mechanisms of this profoundly interesting compound remain to be fully understood.
Significance Statement
Acetaminophen, a drug with a long therapeutic history of utilization, has surprisingly robust effects on a variety of pain states in clinical patients and in preclinical models with a good therapeutic index. In spite of its extensive use, its mechanisms of action are yet poorly understood.
Acknowledgments
This work was supported by a grant from the Japanese Society of Anesthesiology (Grant # 30E118 (HH)) and from the National Institutes of Health (R01NS099338).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr Tony Yaksh reports grants from National Institutes of Health and Japanese Society of Anesthesiology, during the conduct of the study. We have no conflicts of interest.
References
1. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
2. Haykal T, Barbarawi M, Zayed Y, et al. Safety and efficacy of aspirin for primary prevention of cancer: a meta-analysis of randomized controlled trials. J Cancer Res Clin Oncol. 2019;145(7):1795–1809. doi:10.1007/s00432-019-02932-0
3. Honvo G, Leclercq V, Geerinck A, et al. Safety of topical non-steroidal anti-inflammatory drugs in osteoarthritis: outcomes of a systematic review and meta-analysis. Drugs Aging. 2019;36(Suppl 1):45–64. doi:10.1007/s40266-019-00661-0
4. Vranken JH. Elucidation of pathophysiology and treatment of neuropathic pain. Cent Nerv Syst Agents Med Chem. 2012;12(4):304–314. doi:10.2174/187152412803760645
5. Baron R. Neuropathic pain: a clinical perspective. Handb Exp Pharmacol. 2009;194:3–30. doi:10.1007/978-3-540-79090-7_1
6. Prescott LF. Paracetamol: past, present, and future. Am J Ther. 2000;7(2):143–147. doi:10.1097/00045391-200007020-00011
7. Brune K, Renner B, Tiegs G. Acetaminophen/paracetamol: a history of errors, failures and false decisions. Eur J Pain. 2015;19(7):953–965. doi:10.1002/ejp.621
8. Brune K, Hinz B. Paracetamol, ibuprofen, or a combination of both drugs against knee pain: an excellent new randomised clinical trial answers old questions and suggests new therapeutic recommendations. Ann Rheum Dis. 2011;70(9):1521–1522. doi:10.1136/annrheumdis-2011-200242
9. Stephan BC, Parsa FD. Avoiding opioids and their harmful side effects in the postoperative patient: exogenous opioids, endogenous endorphins, wellness, mood, and their relation to postoperative pain. Hawaii J Med Public Health. 2016;75(3):63–67.
10. McCrae JC, Morrison EE, MacIntyre IM, Dear JW, Webb DJ. Long-term adverse effects of paracetamol - a review. Br J Clin Pharmacol. 2018;84(10):2218–2230. doi:10.1111/bcp.13656
11. Nagai J, Uesawa Y, Shimamura R, Kagaya H. Characterization of the adverse effects induced by acetaminophen and nonsteroidal anti-inflammatory drugs based on the analysis of the Japanese adverse drug event report database. Clin J Pain. 2017;33(8):667–675. doi:10.1097/AJP.0000000000000457
12. Shankar SR. Intravenous acetaminophen in postoperative patients. JAMA. 2020;324(22):2327. doi:10.1001/jama.2020.21462
13. Dart RC, Green JL. The prescription paradox of acetaminophen safety. Pharmacoepidemiol Drug Saf. 2016;25(5):599–601. doi:10.1002/pds.3930
14. Mazaleuskaya LL, Sangkuhl K, Thorn CF, FitzGerald GA, Altman RB, Klein TE. PharmGKB summary: pathways of acetaminophen metabolism at the therapeutic versus toxic doses. Pharmacogenet Genomics. 2015;25(8):416–426. doi:10.1097/FPC.0000000000000150
15. Krenzelok EP, Royal MA. Confusion: acetaminophen dosing changes based on NO evidence in adults. Drugs R D. 2012;12(2):45–48. doi:10.2165/11633010-000000000-00000
16. Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medication use in the ambulatory adult population of the United States: the slone survey. JAMA. 2002;287(3):337–344. doi:10.1001/jama.287.3.337
17. Toussaint K, Yang XC, Zielinski MA, et al. What do we (not) know about how paracetamol (acetaminophen) works? J Clin Pharm Ther. 2010;35(6):617–638. doi:10.1111/j.1365-2710.2009.01143.x
18. Holmer Pettersson P, Jakobsson J, Owall A. Plasma concentrations following repeated rectal or intravenous administration of paracetamol after heart surgery. Acta Anaesthesiol Scand. 2006;50(6):673–677. doi:10.1111/j.1399-6576.2006.01043.x
19. Holmer Pettersson P, Owall A, Jakobsson J. Early bioavailability of paracetamol after oral or intravenous administration. Acta Anaesthesiol Scand. 2004;48(7):867–870. doi:10.1111/j.0001-5172.2004.00452.x
20. Singla NK, Parulan C, Samson R, et al. Plasma and cerebrospinal fluid pharmacokinetic parameters after single-dose administration of intravenous, oral, or rectal acetaminophen. Pain Pract. 2012;12(7):523–532. doi:10.1111/j.1533-2500.2012.00556.x
21. Filitz J, Ihmsen H, Gunther W, et al. Supra-additive effects of tramadol and acetaminophen in a human pain model. Pain. 2008;136(3):262–270. doi:10.1016/j.pain.2007.06.036
22. Sachs CJ. Oral analgesics for acute nonspecific pain. Am Fam Physician. 2005;71(5):913–918.
23. Jones P, Dalziel SR, Lamdin R, Miles-Chan JL, Frampton C. Oral non-steroidal anti-inflammatory drugs versus other oral analgesic agents for acute soft tissue injury. Cochrane Database Syst Rev. 2015;(7):CD007789. doi:10.1002/14651858.CD007789.pub2
24. Chou D, Abalos E, Gyte GM, Gulmezoglu AM. Paracetamol/acetaminophen (single administration) for perineal pain in the early postpartum period. Cochrane Database Syst Rev. 2013;(1):CD008407. doi:10.1002/14651858.CD008407.pub2
25. McNicol ED, Tzortzopoulou A, Cepeda MS, Francia MB, Farhat T, Schumann R. Single-dose intravenous paracetamol or propacetamol for prevention or treatment of postoperative pain: a systematic review and meta-analysis. Br J Anaesth. 2011;106(6):764–775. doi:10.1093/bja/aer107
26. Stephens G, Derry S, Moore RA. Paracetamol (Acetaminophen) for acute treatment of episodic tension-type headache in adults. Cochrane Database Syst Rev. 2016;6:CD011889. doi:10.1002/14651858.CD011889.pub2
27. Apfel C, Jahr JR, Kelly CL, Ang RY, Oderda GM. Effect of i.v. acetaminophen on total hip or knee replacement surgery: a case-matched evaluation of a national patient database. Am J Health Syst Pharm. 2015;72(22):1961–1968. doi:10.2146/ajhp140179
28. Machado GC, Maher CG, Ferreira PH, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials. BMJ. 2015;350:h1225. doi:10.1136/bmj.h1225
29. Pickering G, Kastler A, Macian N, et al. The brain signature of paracetamol in healthy volunteers: a double-blind randomized trial. Drug Des Devel Ther. 2015;9:3853–3862. doi:10.2147/DDDT.S81004
30. Sinatra RS, Jahr JS, Reynolds LW, Viscusi ER, Groudine SB, Payen-Champenois C. Efficacy and safety of single and repeated administration of 1 gram intravenous acetaminophen injection (paracetamol) for pain management after major orthopedic surgery. Anesthesiology. 2005;102(4):822–831. doi:10.1097/00000542-200504000-00019
31. Yu S, Eftekhary N, Wiznia D, et al. Evolution of an opioid sparse pain management program for total knee arthroplasty with the addition of intravenous acetaminophen. J Arthroplasty. 2019;35(1):89–94. doi:10.1016/j.arth.2019.08.013
32. Li J, Shi SZ, Wang JS, et al. Efficacy of melanoma patients treated with PD-1 inhibitors: protocol for an overview, and a network meta-analysis of randomized controlled trials. Medicine (Baltimore). 2019;98(27):e16342. doi:10.1097/MD.0000000000016342
33. Westrich GH, Birch GA, Muskat AR, et al. Intravenous vs oral acetaminophen as a component of multimodal analgesia after total hip arthroplasty: a randomized, blinded trial. J Arthroplasty. 2019;34(7S):S215–S220. doi:10.1016/j.arth.2019.02.030
34. Van Aken H, Thys L, Veekman L, Buerkle H. Assessing analgesia in single and repeated administrations of propacetamol for postoperative pain: comparison with morphine after dental surgery. Anesth Analg. 2004;98(1):159–165. table of contents. doi:10.1213/01.ANE.0000093312.72011.59
35. Rizkalla N, Zane NR, Prodell JL, et al. Use of intravenous acetaminophen in children for analgesia after spinal fusion surgery: a randomized clinical trial. J Pediatr Pharmacol Ther. 2018;23(5):395–404. doi:10.5863/1551-6776-23.5.395
36. Wininger SJ, Miller H, Minkowitz HS, et al. A randomized, double-blind, placebo-controlled, multicenter, repeat-dose study of two intravenous acetaminophen dosing regimens for the treatment of pain after abdominal laparoscopic surgery. Clin Ther. 2010;32(14):2348–2369. doi:10.1016/j.clinthera.2010.12.011
37. Lee Y, Yu J, Doumouras AG, et al. Intravenous acetaminophen versus placebo in post-bariatric surgery multimodal pain management: a meta-analysis of randomized controlled trials. Obes Surg. 2019;29(4):1420–1428. doi:10.1007/s11695-019-03732-8
38. Faiz HR, Rahimzadeh P, Visnjevac O, Behzadi B, Ghodraty MR, Nader ND. Intravenous acetaminophen is superior to ketamine for postoperative pain after abdominal hysterectomy: results of a prospective, randomized, double-blind, multicenter clinical trial. J Pain Res. 2014;7:65–70. doi:10.2147/JPR.S53234
39. Urman RD, Boing EA, Pham AT, et al. Improved outcomes associated with the use of intravenous acetaminophen for management of acute post-surgical pain in cesarean sections and hysterectomies. J Clin Med Res. 2018;10(6):499–507. doi:10.14740/jocmr3380w
40. Altenau B, Crisp CC, Devaiah CG, Lambers DS. Randomized controlled trial of intravenous acetaminophen for postcesarean delivery pain control. Am J Obstet Gynecol. 2017;217(3):362e1–362 e6. doi:10.1016/j.ajog.2017.04.030
41. Ng QX, Loke W, Yeo WS, Chng KYY, Tan CH. A meta-analysis of the utility of preoperative intravenous paracetamol for post-caesarean analgesia. Medicina (Kaunas). 2019;55(8):424. doi:10.3390/medicina55080424
42. Herring BO, Ader S, Maldonado A, Hawkins C, Kearson M, Camejo M. Impact of intravenous acetaminophen on reducing opioid use after hysterectomy. Pharmacotherapy. 2014;34(Suppl 1):27S–33S. doi:10.1002/phar.1513
43. Jelacic S, Bollag L, Bowdle A, Rivat C, Cain KC, Richebe P. Intravenous acetaminophen as an adjunct analgesic in cardiac surgery reduces opioid consumption but not opioid-related adverse effects: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2016;30(4):997–1004. doi:10.1053/j.jvca.2016.02.010
44. Smith E, Lange J, Moore C, Eid I, Jackson L, Monico J. The role of intravenous acetaminophen in post-operative pain control in head and neck cancer patients. Laryngoscope Investig Otolaryngol. 2019;4(2):250–254. doi:10.1002/lio2.254
45. Mont MA, Lovelace B, Pham AT, et al. Intravenous acetaminophen may be associated with reduced odds of 30-day readmission after total knee arthroplasty. J Knee Surg. 2018. doi:10.1055/s-0038-1646927
46. Woller SA, Eddinger KA, Corr M, Yaksh TL. An overview of pathways encoding nociception. Clin Exp Rheumatol. 2018;36(1):172.
47. Patterson DC, Cagle PJ
48. Wilson SH, Hebbar L. Balancing analgesia and toxicity with postoperative acetaminophen: more studies are still needed. Pain Med. 2019;20(11):2331–2332. doi:10.1093/pm/pnz205
49. Stundner O, Poeran J, Ladenhauf HN, et al. Effectiveness of intravenous acetaminophen for postoperative pain management in hip and knee arthroplasties: a Population-Based Study. Reg Anesth Pain Med. 2019;44(5):565–572. doi:10.1136/rapm-2018-100145
50. Di Munno O, Sarchi C. Effectiveness of tolmetin in rheumatoid arthritis: evaluation by means of a new method. Methods Find Exp Clin Pharmacol. 1982;4(3):203–206.
51. Solomon L, Abrams G. Bumadizone calcium in the treatment of rheumatoid arthritis. S Afr Med J. 1977;52(10):391–393.
52. Pesa J, Meyer R, Quock TP, Rattana SK, Mody SH. Opioid utilization patterns among medicare patients with diabetic peripheral neuropathy. Am Health Drug Benefits. 2013;6(4):188–196.
53. Axelsson B, Borup S. Is there an additive analgesic effect of paracetamol at step 3? A double-blind randomized controlled study. Palliat Med. 2003;17(8):724–725. doi:10.1177/026921630301700816
54. Israel FJ, Parker G, Charles M, Reymond L. Lack of benefit from paracetamol (acetaminophen) for palliative cancer patients requiring high-dose strong opioids: a randomized, double-blind, placebo-controlled, crossover trial. J Pain Symptom Manage. 2010;39(3):548–554. doi:10.1016/j.jpainsymman.2009.07.008
55. Saragiotto BT, Machado GC, Ferreira ML, Pinheiro MB, Abdel Shaheed C, Maher CG. Paracetamol for low back pain. Cochrane Database Syst Rev. 2016;6:CD012230. doi:10.1002/14651858.CD012230
56. Wiffen PJ, Derry S, Moore RA, et al. Oral paracetamol (acetaminophen) for cancer pain. Cochrane Database Syst Rev. 2017;7:CD012637. doi:10.1002/14651858.CD012637.pub2
57. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Clinical guidelines committee of the American college of p. noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
58. Jibril F, Sharaby S, Mohamed A, Wilby KJ. Intravenous versus oral acetaminophen for pain: systematic review of current evidence to support clinical decision-making. Can J Hosp Pharm. 2015;68(3):238–247. doi:10.4212/cjhp.v68i3.1458
59. McNicol ED, Ferguson MC, Haroutounian S, Carr DB, Schumann R. Single dose intravenous paracetamol or intravenous propacetamol for postoperative pain. Cochrane Database Syst Rev. 2016;5:CD007126. doi:10.1002/14651858.CD007126.pub3
60. Mitidieri A, Donati E, Caronzolo N. Injectable supersaturated acetaminophen solution for spinal administration. Available from: https://patents.google.com/patent/DK2874602T3/en.
61. Sharma CV, Long JH, Shah S, et al. First evidence of the conversion of paracetamol to AM404 in human cerebrospinal fluid. J Pain Res. 2017;10:2703–2709. doi:10.2147/JPR.S143500
62. Koppert W, Wehrfritz A, Korber N, et al. The cyclooxygenase isozyme inhibitors parecoxib and paracetamol reduce central hyperalgesia in humans. Pain. 2004;108(1–2):148–153. doi:10.1016/j.pain.2003.12.017
63. Yue Y, Collaku A. Correlation of pain reduction with fMRI BOLD response in osteoarthritis patients treated with paracetamol: Randomized, Double-Blind, Crossover Clinical Efficacy Study. Pain Med. 2018;19(2):355–367. doi:10.1093/pm/pnx157
64. Leopoldino AO, Machado GC, Ferreira PH, et al. Paracetamol versus placebo for knee and hip osteoarthritis. Cochrane Database Syst Rev. 2019;2:CD013273. doi:10.1002/14651858.CD013273
65. Hahn TW, Mogensen T, Lund C, et al. Analgesic effect of i.v. paracetamol: possible ceiling effect of paracetamol in postoperative pain. Acta Anaesthesiol Scand. 2003;47(2):138–145. doi:10.1034/j.1399-6576.2003.00046.x
66. Montserrat-de La Paz S, Garcia-Gimenez MD, Quilez AM, De la Puerta R, Fernandez-Arche A. Ginger rhizome enhances the anti-inflammatory and anti-nociceptive effects of paracetamol in an experimental mouse model of fibromyalgia. Inflammopharmacology. 2018;26(4):1093–1101. doi:10.1007/s10787-018-0450-8
67. Klinger-Gratz PP, Ralvenius WT, Neumann E, et al. Acetaminophen relieves inflammatory pain through CB1 cannabinoid receptors in the rostral ventromedial medulla. J Neurosci. 2018;38(2):322–334. doi:10.1523/JNEUROSCI.1945-17.2017
68. Bhagyashree A, Manikkoth S, Sequeira M, Nayak R, Rao SN. Central dopaminergic system plays a role in the analgesic action of paracetamol: preclinical evidence. Indian J Pharmacol. 2017;49(1):21–25. doi:10.4103/0253-7613.201029
69. Zhu Q, Sun Y, Mao L, et al. Antinociceptive effects of sinomenine in a rat model of postoperative pain. Br J Pharmacol. 2016;173(10):1693–1702. doi:10.1111/bph.13470
70. Kerckhove N, Mallet C, Francois A, et al. Ca(v)3.2 calcium channels: the key protagonist in the supraspinal effect of paracetamol. Pain. 2014;155(4):764–772. doi:10.1016/j.pain.2014.01.015
71. Vijayakaran K, Kesavan M, Kannan K, Sankar P, Tandan SK, Sarkar SN. Arsenic decreases antinociceptive activity of paracetamol: possible involvement of serotonergic and endocannabinoid receptors. Environ Toxicol Pharmacol. 2014;38(2):397–405. doi:10.1016/j.etap.2014.07.001
72. Dogrul A, Seyrek M, Akgul EO, Cayci T, Kahraman S, Bolay H. Systemic paracetamol-induced analgesic and antihyperalgesic effects through activation of descending serotonergic pathways involving spinal 5-HT(7) receptors. Eur J Pharmacol. 2012;677(1–3):93–101. doi:10.1016/j.ejphar.2011.12.016
73. Mallet C, Barriere DA, Ermund A, et al. TRPV1 in brain is involved in acetaminophen-induced antinociception. PLoS One. 2010;5(9):e12748. doi:10.1371/journal.pone.0012748
74. Crawley B, Saito O, Malkmus S, Fitzsimmons B, Hua XY, Yaksh TL. Acetaminophen prevents hyperalgesia in central pain cascade. Neurosci Lett. 2008;442(1):50–53. doi:10.1016/j.neulet.2008.06.062
75. Joshi SK, Mikusa JP, Weaver B, Honore P. Morphine and ABT-594 (a nicotinic acetylcholine agonist) exert centrally mediated antinociception in the rat cyclophosphamide cystitis model of visceral pain. J Pain. 2008;9(2):146–156. doi:10.1016/j.jpain.2007.09.004
76. Ruggieri V, Vitale G, Pini LA, Sandrini M. Differential involvement of opioidergic and serotonergic systems in the antinociceptive activity of N-arachidonoyl-phenolamine (AM404) in the rat: comparison with paracetamol. Naunyn Schmiedebergs Arch Pharmacol. 2008;377(3):219–229. doi:10.1007/s00210-008-0284-9
77. Ottani A, Leone S, Sandrini M, Ferrari A, Bertolini A. The analgesic activity of paracetamol is prevented by the blockade of cannabinoid CB1 receptors. Eur J Pharmacol. 2006;531(1–3):280–281. doi:10.1016/j.ejphar.2005.12.015
78. Saito O, Aoe T, Yamamoto T. Analgesic effects of nonsteroidal antiinflammatory drugs, acetaminophen, and morphine in a mouse model of bone cancer pain. J Anesth. 2005;19(3):218–224. doi:10.1007/s00540-005-0323-3
79. Kwon MS, Shim EJ, Seo YJ, et al. Effect of aspirin and acetaminophen on proinflammatory cytokine-induced pain behavior in mice. Pharmacology. 2005;74(3):152–156. doi:10.1159/000084548
80. Lynch JJ
81. Bujalska M. Effect of nonselective and selective opioid receptors antagonists on antinociceptive action of acetaminophen [part III]. Pol J Pharmacol. 2004;56(5):539–545.
82. Bonnefont J, Alloui A, Chapuy E, Clottes E, Eschalier A. Orally administered paracetamol does not act locally in the rat formalin test: evidence for a supraspinal, serotonin-dependent antinociceptive mechanism. Anesthesiology. 2003;99(4):976–981. doi:10.1097/00000542-200310000-00034
83. Nagakura Y, Okada M, Kohara A, et al. Allodynia and hyperalgesia in adjuvant-induced arthritic rats: time course of progression and efficacy of analgesics. J Pharmacol Exp Ther. 2003;306(2):490–497. doi:10.1124/jpet.103.050781
84. Bujalska M, Gumulka WS. Effect of cyclooxygenase and NO synthase inhibitors on antinociceptive action of acetaminophen. Pol J Pharmacol. 2001;53(4):341–350.
85. Choi SS, Lee JK, Suh HW. Antinociceptive profiles of aspirin and acetaminophen in formalin, substance P and glutamate pain models. Brain Res. 2001;921(1–2):233–239. doi:10.1016/S0006-8993(01)03126-2
86. Al-Swayeh OA, Futter LE, Clifford RH, Moore PK. Nitroparacetamol exhibits anti-inflammatory and anti-nociceptive activity. Br J Pharmacol. 2000;130(7):1453–1456. doi:10.1038/sj.bjp.0703509
87. Pelissier T, Alloui A, Caussade F, et al. Paracetamol exerts a spinal antinociceptive effect involving an indirect interaction with 5-hydroxytryptamine3 receptors: in vivo and in vitro evidence. J Pharmacol Exp Ther. 1996;278(1):8–14.
88. Granados-Soto V, Flores-Murrieta FJ, Lopez-Munoz FJ, Salazar LA, Villarreal JE, Castaneda-Hernandez G. Relationship between paracetamol plasma levels and its analgesic effect in the rat. J Pharm Pharmacol. 1992;44(9):741–744. doi:10.1111/j.2042-7158.1992.tb05511.x
89. Okuyama S, Aihara H. The mode of action of analgesic drugs in adjuvant arthritic rats as an experimental model of chronic inflammatory pain: possible central analgesic action of acidic nonsteroidal antiinflammatory drugs. Jpn J Pharmacol. 1984;35(2):95–103. doi:10.1016/S0021-5198(19)38076-X
90. Dalmann R, Daulhac L, Antri M, Eschalier A, Mallet C. Supra-spinal FAAH is required for the analgesic action of paracetamol in an inflammatory context. Neuropharmacology. 2015;91:63–70. doi:10.1016/j.neuropharm.2014.11.006
91. Viberg H, Eriksson P, Gordh T, Fredriksson A. Paracetamol (acetaminophen) administration during neonatal brain development affects cognitive function and alters its analgesic and anxiolytic response in adult male mice. Toxicol Sci. 2014;138(1):139–147. doi:10.1093/toxsci/kft329
92. Aizawa N, Wyndaele JJ. Effects of phenazopyridine on rat bladder primary afferent activity, and comparison with lidocaine and acetaminophen. Neurourol Urodyn. 2010;29(8):1445–1450. doi:10.1002/nau.20886
93. Soukupova M, Dolezal T, Krsiak M. The synergistic interaction between rilmenidine and paracetamol in the writhing test in mice. Naunyn Schmiedebergs Arch Pharmacol. 2009;379(6):575–580. doi:10.1007/s00210-009-0402-3
94. Qiu HX, Liu J, Kong H, Liu Y, Mei XG. Isobolographic analysis of the antinociceptive interactions between ketoprofen and paracetamol. Eur J Pharmacol. 2007;557(2–3):141–146. doi:10.1016/j.ejphar.2006.11.017
95. Mallet C, Daulhac L, Bonnefont J, et al. Endocannabinoid and serotonergic systems are needed for acetaminophen-induced analgesia. Pain. 2008;139(1):190–200. doi:10.1016/j.pain.2008.03.030
96. Bianchi M, Panerai AE. The dose-related effects of paracetamol on hyperalgesia and nociception in the rat. Br J Pharmacol. 1996;117(1):130–132. doi:10.1111/j.1476-5381.1996.tb15164.x
97. Mburu DN. Evaluation of the anti-inflammatory effects of a low dose of acetaminophen following surgery in dogs. J Vet Pharmacol Ther. 1991;14(1):109–111. doi:10.1111/j.1365-2885.1991.tb00811.x
98. Behrendt WA, Cserepes J. Acute toxicity and analgesic action of a combination of buclizine, codeine and paracetamol (‘Migraleve’) in tablet and suppository form in rats. Pharmatherapeutica. 1985;4(5):322–331.
99. Sewell RD, Gonzalez JP, Pugh J. Comparison of the relative effects of aspirin, mefenamic acid, dihydrocodeine, dextropropoxyphene and paracetamol on visceral pain, respiratory rate and prostaglandin biosynthesis. Arch Int Pharmacodyn Ther. 1984;268(2):325–334.
100. Pircio AW, Buyniski JP, Roebel LE. Pharmacological effects of a combination of butorphanol and acetaminophen. Arch Int Pharmacodyn Ther. 1978;235(1):116–123.
101. Mititelu Tartau L, Popa EG, Lupusoru RV, Lupusoru CE, Stoleriu I, Ochiuz L. Synergic effects of pregabalin-acetaminophen combination in somatic and visceral nociceptive reactivity. Pharmacology. 2014;93(5–6):253–259. doi:10.1159/000362649
102. Vinegar R, Truax JF, Selph JL. Quantitative comparison of the analgesic and anti-inflammatory activities of aspirin, phenacetin and acetaminophen in rodents. Eur J Pharmacol. 1976;37(1):23–30. doi:10.1016/0014-2999(76)90004-2
103. Micov A, Tomic M, Pecikoza U, Ugresic N, Stepanovic-Petrovic R. Levetiracetam synergises with common analgesics in producing antinociception in a mouse model of painful diabetic neuropathy. Pharmacol Res. 2015;97:131–142. doi:10.1016/j.phrs.2015.04.014
104. Shinozaki T, Yamada T, Nonaka T, Yamamoto T. Acetaminophen and non-steroidal anti-inflammatory drugs interact with morphine and tramadol analgesia for the treatment of neuropathic pain in rats. J Anesth. 2015;29(3):386–395. doi:10.1007/s00540-014-1953-0
105. Flower RJ, Vane JR. Inhibition of prostaglandin synthetase in brain explains the anti-pyretic activity of paracetamol (4-acetamidophenol). Nature. 1972;240(5381):410–411. doi:10.1038/240410a0
106. Zapata-Morales JR, Alonso-Castro AJ, Perez-Gutierrez S, et al. Participation of ATP-sensitive K+ channels and mu-opioid receptors in the antinociceptive synergism of the paracetamol-tapentadol co-administration in the formalin-induced pain assay in mice. Drug Dev Res. 2018;79(8):400–405. doi:10.1002/ddr.21476
107. Li Q, Zhuang Q, Gu Y, et al. Enhanced analgesic effects of nefopam in combination with acetaminophen in rodents. Biomed Rep. 2018;8(2):176–183. doi:10.3892/br.2017.1032
108. Fukushima A, Mamada K, Iimura A, Ono H. Supraspinal-selective TRPV1 desensitization induced by intracerebroventricular treatment with resiniferatoxin. Sci Rep. 2017;7(1):12452. doi:10.1038/s41598-017-12717-5
109. Siemian JN, Li J, Zhang Y, Li JX. Interactions between imidazoline I2 receptor ligands and acetaminophen in adult male rats: antinociception and schedule-controlled responding. Psychopharmacology (Berl). 2016;233(5):873–882. doi:10.1007/s00213-015-4166-9
110. Karandikar YS, Belsare P, Panditrao A. Effect of drugs modulating serotonergic system on the analgesic action of paracetamol in mice. Indian J Pharmacol. 2016;48(3):281–285. doi:10.4103/0253-7613.182874
111. Raskovic A, Milanovic I, Pavlovic N, Milijasevic B, Ubavic M, Mikov M. Analgesic effects of rosemary essential oil and its interactions with codeine and paracetamol in mice. Eur Rev Med Pharmacol Sci. 2015;19(1):165–172.
112. Fresno N, Perez-Fernandez R, Goicoechea C, et al. Adamantyl analogues of paracetamol as potent analgesic drugs via inhibition of TRPA1. PLoS One. 2014;9(12):e113841. doi:10.1371/journal.pone.0113841
113. Minville V, Fourcade O, Mazoit JX, Girolami JP, Tack I. Ondansetron does not block paracetamol-induced analgesia in a mouse model of fracture pain. Br J Anaesth. 2011;106(1):112–118. doi:10.1093/bja/aeq277
114. Tomic MA, Vuckovic SM, Stepanovic-Petrovic RM, Ugresic ND, Prostran MS, Boskovic B. Synergistic interactions between paracetamol and oxcarbazepine in somatic and visceral pain models in rodents. Anesth Analg. 2010;110(4):1198–1205. doi:10.1213/ANE.0b013e3181cbd8da
115. Mitchell D, Gelgor L, Weber J, Kamerman PR. Antihypernociceptive synergy between ibuprofen, paracetamol and codeine in rats. Eur J Pharmacol. 2010;642(1–3):86–92. doi:10.1016/j.ejphar.2010.06.004
116. Godfrey L, Yan L, Clarke GD, Ledent C, Kitchen I, Hourani SM. Modulation of paracetamol antinociception by caffeine and by selective adenosine A2 receptor antagonists in mice. Eur J Pharmacol. 2006;531(1–3):80–86. doi:10.1016/j.ejphar.2005.12.004
117. Sandrini M, Pini LA, Vitale G. Differential involvement of central 5-HT1B and 5-HT3 receptor subtypes in the antinociceptive effect of paracetamol. Inflamm Res. 2003;52(8):347–352. doi:10.1007/s00011-003-1185-5
118. Sandrini M, Vitale G, Ottani A, Pini LA. The potentiation of analgesic activity of paracetamol plus morphine involves the serotonergic system in rat brain. Inflamm Res. 1999;48(3):120–127. doi:10.1007/s000110050434
119. Tjolsen A, Lund A, Hole K. The role of descending noradrenergic systems in regulation of nociception: the effects of intrathecally administered alpha-adrenoceptor antagonists and clonidine. Pain. 1990;43(1):113–120. doi:10.1016/0304-3959(90)90056-J
120. Liu J, Reid AR, Sawynok J. Antinociception by systemically-administered acetaminophen (paracetamol) involves spinal serotonin 5-HT7 and adenosine A1 receptors, as well as peripheral adenosine A1 receptors. Neurosci Lett. 2013;536:64–68. doi:10.1016/j.neulet.2012.12.052
121. Miranda HF, Noriega V, Prieto JC. Previous administration of naltrexone did not change synergism between paracetamol and tramadol in mice. Pharmacol Biochem Behav. 2012;102(1):72–76. doi:10.1016/j.pbb.2012.03.008
122. Im KS, Jung HJ, Kim JB, et al. The antinociceptive effect of acetaminophen in a rat model of neuropathic pain. Kaohsiung J Med Sci. 2012;28(5):251–258. doi:10.1016/j.kjms.2011.11.003
123. Sawynok J, Reid AR. Caffeine inhibits antinociception by acetaminophen in the formalin test by inhibiting spinal adenosine A(1) receptors. Eur J Pharmacol. 2012;674(2–3):248–254. doi:10.1016/j.ejphar.2011.10.036
124. Rezende RM, Franca DS, Menezes GB, dos Reis WGP, Bakhle YS, Francischi JN. Different mechanisms underlie the analgesic actions of paracetamol and dipyrone in a rat model of inflammatory pain. Br J Pharmacol. 2008;153(4):760–768. doi:10.1038/sj.bjp.0707630
125. Luccarini P, Childeric A, Gaydier AM, Voisin D, Dallel R. The orofacial formalin test in the mouse: a behavioral model for studying physiology and modulation of trigeminal nociception. J Pain. 2006;7(12):908–914. doi:10.1016/j.jpain.2006.04.010
126. Abbott FV, Hellemans KG. Phenacetin, acetaminophen and dipyrone: analgesic and rewarding effects. Behav Brain Res. 2000;112(1–2):177–186. doi:10.1016/S0166-4328(00)00179-0
127. Srikiatkhachorn A, Tarasub N, Govitrapong P. Acetaminophen-induced antinociception via central 5-HT(2A) receptors. Neurochem Int. 1999;34(6):491–498. doi:10.1016/S0197-0186(99)00023-6
128. Pini LA, Sandrini M, Vitale G. The antinociceptive action of paracetamol is associated with changes in the serotonergic system in the rat brain. Eur J Pharmacol. 1996;308(1):31–40. doi:10.1016/0014-2999(96)00261-0
129. Bjorkman R. Central antinociceptive effects of non-steroidal anti-inflammatory drugs and paracetamol. Experimental studies in the rat. Acta Anaesthesiol Scand Suppl. 1995;103:1–44.
130. Bjorkman R, Hallman KM, Hedner J, Hedner T, Henning M. Acetaminophen blocks spinal hyperalgesia induced by NMDA and substance P. Pain. 1994;57(3):259–264. doi:10.1016/0304-3959(94)90001-9
131. Kanui TI, Karim F, Towett PK. The formalin test in the naked mole-rat (heterocephalus glaber): analgesic effects of morphine, nefopam and paracetamol. Brain Res. 1993;600(1):123–126. doi:10.1016/0006-8993(93)90409-g
132. Malmberg AB, Yaksh TL. Antinociceptive actions of spinal nonsteroidal anti-inflammatory agents on the formalin test in the rat. J Pharmacol Exp Ther. 1992;263(1):136–146.
133. Tjolsen A, Lund A, Hole K. Antinociceptive effect of paracetamol in rats is partly dependent on spinal serotonergic systems. Eur J Pharmacol. 1991;193(2):193–201. doi:10.1016/0014-2999(91)90036-P
134. Carlsson KH, Jurna I. Central analgesic effect of paracetamol manifested by depression of nociceptive activity in thalamic neurones of the rat. Neurosci Lett. 1987;77(3):339–343. doi:10.1016/0304-3940(87)90524-6
135. Ferreira SH, Lorenzetti BB, Correa FM. Central and peripheral antialgesic action of aspirin-like drugs. Eur J Pharmacol. 1978;53(1):39–48. doi:10.1016/0014-2999(78)90265-0
136. Hunskaar S, Fasmer OB, Hole K. Acetylsalicylic acid, paracetamol and morphine inhibit behavioral responses to intrathecally administered substance P or capsaicin. Life Sci. 1985;37(19):1835–1841. doi:10.1016/0024-3205(85)90227-9
137. Hama AT, Sagen J. Cannabinoid receptor-mediated antinociception with Acetaminophen drug combinations in rats with neuropathic spinal cord injury pain. Neuropharmacology. 2010;58(4–5):758–766. doi:10.1016/j.neuropharm.2009.12.010
138. Munro G, Christensen JK, Erichsen HK, et al. NS383 selectively inhibits acid-sensing ion channels containing 1a and 3 subunits to reverse inflammatory and neuropathic hyperalgesia in rats. CNS Neurosci Ther. 2016;22(2):135–145. doi:10.1111/cns.12487
139. Sandrini M, Vitale G, Ruggieri V, Pini LA. Effect of acute and repeated administration of paracetamol on opioidergic and serotonergic systems in rats. Inflamm Res. 2007;56(4):139–142. doi:10.1007/s00011-006-6113-z
140. Roca-Vinardell A, Ortega-Alvaro A, Gibert-Rahola J, Mico JA. The role of 5-HT1A/B autoreceptors in the antinociceptive effect of systemic administration of acetaminophen. Anesthesiology. 2003;98(3):741–747. doi:10.1097/00000542-200303000-00025
141. Andersson DA, Gentry C, Alenmyr L, et al. TRPA1 mediates spinal antinociception induced by acetaminophen and the cannabinoid delta(9)-tetrahydrocannabiorcol. Nat Commun. 2011;2(1):551. doi:10.1038/ncomms1559
142. Cui JG, Zhang X, Zhao YH, Chen C, Bazan N. Allodynia and hyperalgesia suppression by a novel analgesic in experimental neuropathic pain. Biochem Biophys Res Commun. 2006;350(2):358–363. doi:10.1016/j.bbrc.2006.09.055
143. Alloui A, Chassaing C, Schmidt J, et al. Paracetamol exerts a spinal, tropisetron-reversible, antinociceptive effect in an inflammatory pain model in rats. Eur J Pharmacol. 2002;443(1–3):71–77. doi:10.1016/S0014-2999(02)01578-9
144. Raffa RB, Stone DJ
145. Jensen FM, Dahl JB, Frigast C. Direct spinal effect of intrathecal acetaminophen on visceral noxious stimulation in rabbits. Acta Anaesthesiol Scand. 1992;36(8):837–841. doi:10.1111/j.1399-6576.1992.tb03574.x
146. Seo YJ, Kwon MS, Choi HW, et al. The differential effects of acetaminophen on lipopolysaccharide induced hyperalgesia in various mouse pain models. Pharmacol Biochem Behav. 2008;91(1):121–127. doi:10.1016/j.pbb.2008.06.020
147. Matsunaga A, Kawamoto M, Shiraishi S, et al. Intrathecally administered COX-2 but not COX-1 or COX-3 inhibitors attenuate streptozotocin-induced mechanical hyperalgesia in rats. Eur J Pharmacol. 2007;554(1):12–17. doi:10.1016/j.ejphar.2006.09.072
148. Curros-Criado MM, Herrero JF. Antinociceptive effects of NCX-701 (nitro-paracetamol) in neuropathic rats: enhancement of antinociception by co-administration with gabapentin. Br J Pharmacol. 2009;158(2):601–609. doi:10.1111/j.1476-5381.2009.00343.x
149. Bonnefont J, Chapuy E, Clottes E, Alloui A, Eschalier A. Spinal 5-HT1A receptors differentially influence nociceptive processing according to the nature of the noxious stimulus in rats: effect of WAY-100635 on the antinociceptive activities of paracetamol, venlafaxine and 5-HT. Pain. 2005;114(3):482–490. doi:10.1016/j.pain.2005.01.019
150. Romero-Sandoval EA, Mazario J, Howat D, Herrero JF. NCX-701 (nitroparacetamol) is an effective antinociceptive agent in rat withdrawal reflexes and wind-up. Br J Pharmacol. 2002;135(6):1556–1562. doi:10.1038/sj.bjp.0704589
151. Courade JP, Chassaing C, Bardin L, Alloui A, Eschalier A. 5-HT receptor subtypes involved in the spinal antinociceptive effect of Acetaminophen in rats. Eur J Pharmacol. 2001;432(1):1–7. doi:10.1016/S0014-2999(01)01464-9
152. Shibasaki J, Konishi R, Kitasaki T, Koizumi T. Relationship between blood levels and analgesic effects of acetaminophen in mice. Chem Pharm Bull (Tokyo). 1979;27(1):129–138. doi:10.1248/cpb.27.129
153. Pelissier T, Alloui A, Paeile C, Eschalier A. Evidence of a central antinociceptive effect of paracetamol involving spinal 5HT3 receptors. Neuroreport. 1995;6(11):1546–1548. doi:10.1097/00001756-199507310-00020
154. Raffa RB, Stone DJ
155. Dani M, Guindon J, Lambert C, Beaulieu P. The local antinociceptive effects of paracetamol in neuropathic pain are mediated by cannabinoid receptors. Eur J Pharmacol. 2007;573(1–3):214–215. doi:10.1016/j.ejphar.2007.07.012
156. Deciga-Campos M, Ortiz-Andrade R. Enhancement of antihyperalgesia by the coadministration of N-palmitoylethanolamide and acetaminophen in diabetic rats. Drug Dev Res. 2015;76(5):228–234. doi:10.1002/ddr.21259
157. Gonzalez-Trujano ME, Uribe-Figueroa G, Hidalgo-Figueroa S, Martinez AL, Deciga-Campos M, Navarrete-Vazquez G. Synthesis and antinociceptive evaluation of bioisosteres and hybrids of naproxen, ibuprofen and paracetamol. Biomed Pharmacother. 2018;101:553–562. doi:10.1016/j.biopha.2018.02.122
158. Lopez-Canul M, Comai S, Dominguez-Lopez S, Granados-Soto V, Gobbi G. Antinociceptive properties of selective MT(2) melatonin receptor partial agonists. Eur J Pharmacol. 2015;764:424–432. doi:10.1016/j.ejphar.2015.07.010
159. Girard P, Niedergang B, Pansart Y, Coppe MC, Verleye M. Systematic evaluation of the nefopam-paracetamol combination in rodent models of antinociception. Clin Exp Pharmacol Physiol. 2011;38(3):170–178. doi:10.1111/j.1440-1681.2011.05477.x
160. Wong CL, Wai MK, Roberts MB. The effect of aspirin and paracetamol on the increased naloxone potency induced by morphine pretreatment. Eur J Pharmacol. 1980;67(2–3):241–246. doi:10.1016/0014-2999(80)90504-x
161. Girard P, Pansart Y, Coppe MC, Niedergang B, Gillardin JM. Modulation of paracetamol and nefopam antinociception by serotonin 5-HT(3) receptor antagonists in mice. Pharmacology. 2009;83(4):243–246. doi:10.1159/000207448
162. O’Neil MJ. The Merck Index: An Encyclopedia of Chemicals, Drugs, and Biologicals. Royal Society of Chemistry; 2013.
163. Samuel H, He Y, Jain P. Handbook of Aqueous Solubility Data Second Edition. CRC Press; 2010:492.
164. Kalatzis E. Reactions of acetaminophen in pharmaceutical dosage forms: its proposed acetylation by acetylsalicylic acid. J Pharm Sci. 1970;59(2):193–196. doi:10.1002/jps.2600590211
165. Gilpin RK, Zhou W. Studies of the thermal degradation of acetaminophen using a conventional HPLC approach and electrospray ionization-mass spectrometry. J Chromatogr Sci. 2004;42(1):15–20. doi:10.1093/chromsci/42.1.15
166. Fairbrother JE. Analytical Profiles of Drug Substances. Vol. 3. Acetominophen. Academic Press; 1974:1–110.
167. Kelava T, Cavar I, Culo F. Influence of small doses of various drug vehicles on acetaminophen-induced liver injury. Can J Physiol Pharmacol. 2010;88(10):960–967. doi:10.1139/y10-065
168. D’Amour F, Smith D. A method for determining loss of pain sensation. J Pharmacol Exp Ther. 1941;72:74–79.
169. Woolfe G, MacDonald A. The evaluation of the analgesic action of pethidine hydrochloride (demerol). J Pharmacol Exp Ther. 1944;80:300–307.
170. Dirig DM, Salami A, Rathbun ML, Ozaki GT, Yaksh TL. Characterization of variables defining hindpaw withdrawal latency evoked by radiant thermal stimuli. J Neurosci Methods. 1997;76(2):183–191. doi:10.1016/s0165-0270(97)00097-6
171. Barrot M. Tests and models of nociception and pain in rodents. Neuroscience. 2012;211:39–50. doi:10.1016/j.neuroscience.2011.12.041
172. Randall LO, Selitto JJ. A method for measurement of analgesic activity on inflamed tissue. Arch Int Pharmacodyn Ther. 1957;111(4):409–419.
173. Libert F, Bonnefont J, Bourinet E, et al. Acetaminophen: a central analgesic drug that involves a spinal tropisetron-sensitive, non-5-HT(3) receptor-mediated effect. Mol Pharmacol. 2004;66(3):728–734. doi:10.1124/mol.66.3
174. Carlsson KH, Monzel W, Jurna I. Depression by morphine and the non-opioid analgesic agents, metamizol (dipyrone), lysine acetylsalicylate, and paracetamol, of activity in rat thalamus neurones evoked by electrical stimulation of nociceptive afferents. Pain. 1988;32(3):313–326. doi:10.1016/0304-3959(88)90043-7
175. Davidson N, Southwick CA. The effect of topically applied amino acids on primary afferent terminal excitability in the rat cuneate nucleus. J Physiol. 1970;210(2):172P–173P.
176. Hokfelt T, Kellerth JO, Nilsson G, Pernow B. Experimental immunohistochemical studies on the localization and distribution of substance P in cat primary sensory neurons. Brain Res. 1975;100(2):235–252. doi:10.1016/0006-8993(75)90481-3
177. Woller SA, Eddinger KA, Corr M, Yaksh TL. An overview of pathways encoding nociception. Clin Exp Rheumatol. 2017;107(5):40–46.
178. Brennan TJ, Vandermeulen EP, Gebhart GF. Characterization of a rat model of incisional pain. Pain. 1996;64(3):493–501. doi:10.1016/0304-3959(95)01441-1
179. Yaksh TL, Ozaki G, McCumber D, et al. An automated flinch detecting system for use in the formalin nociceptive bioassay. J Appl Physiol. 2001;90(6):2386–2402. doi:10.1152/jappl.2001.90.6.2386
180. Regmi B, Shah MK. Possible implications of animal models for the assessment of visceral pain. Animal Model Exp Med. 2020;3(3):215–228. doi:10.1002/ame2.12130
181. Greenwood-van Meerveld B, Prusator DK, Johnson AC. Animal models of gastrointestinal and liver diseases. Animal models of visceral pain: pathophysiology, translational relevance, and challenges. Am J Physiol Gastrointest Liver Physiol. 2015;308(11):G885–903. doi:10.1152/ajpgi.00463.2014
182. Birder L, Andersson KE. Animal modelling of interstitial cystitis/bladder pain syndrome. Int Neurourol J. 2018;22(Suppl 1):S3–9. doi:10.5213/inj.1835062.531
183. Simmons JK, Hildreth BE
184. Jimenez-Andrade JM, Mantyh WG, Bloom AP, Ferng AS, Geffre CP, Mantyh PW. Bone cancer pain. Ann N Y Acad Sci. 2010;1198(1):173–181. doi:10.1111/j.1749-6632.2009.05429.x
185. Sorkin LS, Yaksh TL. Behavioral models of pain states evoked by physical injury to the peripheral nerve. Neurotherapeutics. 2009;6(4):609–619. doi:10.1016/j.nurt.2009.07.007
186. Grothey A. Clinical management of oxaliplatin-associated neurotoxicity. Clin Colorectal Cancer. 2005;5(Suppl 1):S38–46. doi:10.3816/CCC.2005.s.006
187. Lee-Kubli CA, Calcutt NA. Painful neuropathy: mechanisms. Handb Clin Neurol. 2014;126:533–557. doi:10.1016/B978-0-444-53480-4.00034-5
188. Lee-Kubli C, Marshall AG, Malik RA, Calcutt NA. The H-reflex as a biomarker for spinal disinhibition in painful diabetic neuropathy. Curr Diab Rep. 2018;18(1):1. doi:10.1007/s11892-018-0969-5
189. Apostolidis L, Schwarz D, Xia A, et al. Dorsal root ganglia hypertrophy as in vivo correlate of oxaliplatin-induced polyneuropathy. PLoS One. 2017;12(8):e0183845. doi:10.1371/journal.pone.0183845
190. Chaturvedi PR, Decker CJ, Odinecs A. Prediction of pharmacokinetic properties using experimental approaches during early drug discovery. Curr Opin Chem Biol. 2001;5(4):452–463. doi:10.1016/s1367-5931(00)00228-3
191. Rhomberg L, Lewandowski T. Methods for identifying a default cross-species scaling factor. Hum Ecol Risk Assess. 2006;12(6):1094–1127. doi:10.1080/10807030600977269
192. Nair AB, Jacob S. A simple practice guide for dose conversion between animals and human. J Basic Clin Pharm. 2016;7(2):27–31. doi:10.4103/0976-0105.177703
193. Cummings AJ, King ML, Martin BK. A kinetic study of drug elimination: the excretion of paracetamol and its metabolites in man. Br J Pharmacol Chemother. 1967;29(2):150–157. doi:10.1111/j.1476-5381.1967.tb01948.x
194. Galinsky RE, Levy G. Dose- and time-dependent elimination of acetaminophen in rats: pharmacokinetic implications of cosubstrate depletion. J Pharmacol Exp Ther. 1981;219(1):14–20.
195. McGill MR, Jaeschke H. Metabolism and disposition of acetaminophen: recent advances in relation to hepatotoxicity and diagnosis. Pharm Res. 2013;30(9):2174–2187. doi:10.1007/s11095-013-1007-6
196. Hogestatt ED, Jonsson BA, Ermund A, et al. Conversion of acetaminophen to the bioactive N-acylphenolamine AM404 via fatty acid amide hydrolase-dependent arachidonic acid conjugation in the nervous system. J Biol Chem. 2005;280(36):31405–31412. doi:10.1074/jbc.M501489200
197. Woolbright BL, Jaeschke H. Role of the inflammasome in Acetaminophen-induced liver injury and acute liver failure. J Hepatol. 2017;66(4):836–848. doi:10.1016/j.jhep.2016.11.017
198. Athersuch TJ, Antoine DJ, Boobis AR, et al. Paracetamol metabolism, hepatotoxicity, biomarkers and therapeutic interventions: a perspective. Toxicol Res (Camb). 2018;7(3):347–357. doi:10.1039/c7tx00340d
199. Courad JP, Besse D, Delchambre C, et al. Acetaminophen distribution in the rat central nervous system. Life Sci. 2001;69(12):1455–1464. doi:10.1016/s0024-3205(01)01228-0
200. Godfrey L, Morselli A, Bennion P, Clarke GD, Hourani SM, Kitchen I. An investigation of binding sites for paracetamol in the mouse brain and spinal cord. Eur J Pharmacol. 2005;508(1–3):99–106. doi:10.1016/j.ejphar.2004.11.061
201. Raffa RB, Codd EE. Lack of binding of acetaminophen to 5-HT receptor or uptake sites (or eleven other binding/uptake assays). Life Sci. 1996;59(2):PL37–40. doi:10.1016/0024-3205(96)00273-1
202. Svensson CI, Yaksh TL. The spinal phospholipase-cyclooxygenase-prostanoid cascade in nociceptive processing. Annu Rev Pharmacol Toxicol. 2002;42:553–583. doi:10.1146/annurev.pharmtox.42.092401.143905
203. Patrignani P, Patrono C. Cyclooxygenase inhibitors: from pharmacology to clinical read-outs. Biochim Biophys Acta. 2015;1851(4):422–432. doi:10.1016/j.bbalip.2014.09.016
204. Lucas R, Warner TD, Vojnovic I, Mitchell JA. Cellular mechanisms of acetaminophen: role of cyclo-oxygenase. FASEB J. 2005;19(6):635–637. doi:10.1096/fj.04-2437fje
205. Ayoub SS, Colville-Nash PR, Willoughby DA, Botting RM. The involvement of a cyclooxygenase 1 gene-derived protein in the antinociceptive action of paracetamol in mice. Eur J Pharmacol. 2006;538(1–3):57–65. doi:10.1016/j.ejphar.2006.03.061
206. Smith HS. Potential analgesic mechanisms of acetaminophen. Pain Physician. 2009;12(1):269–280. doi:10.36076/ppj.2009/12/269
207. Rao P, Knaus EE. Evolution of nonsteroidal anti-inflammatory drugs (NSAIDs): cyclooxygenase (COX) inhibition and beyond. J Pharm Pharm Sci. 2008;11(2):81s–110s. doi:10.18433/J3T886
208. Nandakishore R, Yalavarthi PR, Kiran YR, Rajapranathi M. Selective cyclooxygenase inhibitors: current status. Curr Drug Discov Technol. 2014;11(2):127–132. doi:10.2174/1570163811666140127123717
209. Yaksh TL, Dirig DM, Malmberg AB. Mechanism of action of nonsteroidal anti-inflammatory drugs. Cancer Invest. 1998;16(7):509–527. doi:10.3109/07357909809011705
210. Yaksh TL, Dirig DM, Conway CM, Svensson C, Luo ZD, Isakson PC. The acute antihyperalgesic action of nonsteroidal, anti-inflammatory drugs and release of spinal prostaglandin E2 is mediated by the inhibition of constitutive spinal cyclooxygenase-2 (COX-2) but not COX-1. J Neurosci. 2001;21(16):5847–5853. doi:10.1523/JNEUROSCI.21-16-05847.2001
211. Greco A, Ajmone-Cat MA, Nicolini A, Sciulli MG, Minghetti L. Paracetamol effectively reduces prostaglandin E2 synthesis in brain macrophages by inhibiting enzymatic activity of cyclooxygenase but not phospholipase and prostaglandin E synthase. J Neurosci Res. 2003;71(6):844–852. doi:10.1002/jnr.10543
212. Turman MV, Kingsley PJ, Marnett LJ. Characterization of an AM404 analogue, N-(3-hydroxyphenyl)arachidonoylamide, as a substrate and inactivator of prostaglandin endoperoxide synthase. Biochemistry. 2009;48(51):12233–12241. doi:10.1021/bi901181z
213. Saliba SW, Marcotegui AR, Fortwangler E, et al. AM404, paracetamol metabolite, prevents prostaglandin synthesis in activated microglia by inhibiting COX activity. J Neuroinflammation. 2017;14(1):246. doi:10.1186/s12974-017-1014-3
214. Caballero FJ, Navarrete CM, Hess S, et al. The acetaminophen-derived bioactive N-acylphenolamine AM404 inhibits NFAT by targeting nuclear regulatory events. Biochem Pharmacol. 2007;73(7):1013–1023. doi:10.1016/j.bcp.2006.12.001
215. Zygmunt PM, Chuang -H-H, Movahed P, et al. The anandamide transport inhibitor AM404 activates vanilloid receptors. Eur J Pharmacol. 2000;396(1):39–42. doi:10.1016/S0014-2999(00)00207-7
216. Stueber T, Meyer S, Jangra A, Hage A, Eberhardt M, Leffler A. Activation of the capsaicin-receptor TRPV1 by the acetaminophen metabolite N-arachidonoylaminophenol results in cytotoxicity. Life Sci. 2018;194:67–74. doi:10.1016/j.lfs.2017.12.024
217. Wang Y, Lin W, Wu N, et al. An insight into paracetamol and its metabolites using molecular docking and molecular dynamics simulation. J Mol Model. 2018;24(9):243. doi:10.1007/s00894-018-3790-9
218. Nassini R, Materazzi S, Andre E, et al. Acetaminophen, via its reactive metabolite N-acetyl-p-benzo-quinoneimine and transient receptor potential ankyrin-1 stimulation, causes neurogenic inflammation in the airways and other tissues in rodents. FASEB J. 2010;24(12):4904–4916. doi:10.1096/fj.10-162438
219. De Petrocellis L, Bisogno T, Davis JB, Pertwee RG, Di Marzo V. Overlap between the ligand recognition properties of the anandamide transporter and the VR1 vanilloid receptor: inhibitors of anandamide uptake with negligible capsaicin-like activity. FEBS Lett. 2000;483(1):52–56. doi:10.1016/S0014-5793(00)02082-2
220. Beltramo M, Stella N, Calignano A, Lin SY, Makriyannis A, Piomelli D. Functional role of high-affinity anandamide transport, as revealed by selective inhibition. Science. 1997;277(5329):1094–1097. doi:10.1126/science.277.5329.1094
221. Howlett AC, Abood ME. CB1 and CB2 receptor pharmacology. Adv Pharmacol. 2017;80:169–206. doi:10.1016/bs.apha.2017.03.007
222. Busquets-Garcia A, Bains J, Marsicano G. CB1 receptor signaling in the brain: extracting specificity from ubiquity. Neuropsychopharmacology. 2018;43(1):4–20. doi:10.1038/npp.2017.206
223. Fu J, Bottegoni G, Sasso O, et al. A catalytically silent FAAH-1 variant drives anandamide transport in neurons. Nat Neurosci. 2011;15(1):64. doi:10.1038/nn.2986
224. Barriere DA, Mallet C, Blomgren A, et al. Fatty acid amide hydrolase-dependent generation of antinociceptive drug metabolites acting on TRPV1 in the brain. PLoS One. 2013;8(8):e70690. doi:10.1371/journal.pone.0070690
225. Evans RM, Scott RH, Ross RA. Chronic exposure of sensory neurones to increased levels of nerve growth factor modulates CB1/TRPV1 receptor crosstalk. Br J Pharmacol. 2007;152(3):404–413. doi:10.1038/sj.bjp.0707411
226. Weinhold P, Gratzke C, Streng T, Stief C, Andersson KE, Hedlund P. TRPA1 receptor induced relaxation of the human urethra involves TRPV1 and cannabinoid receptor mediated signals, and cyclooxygenase activation. J Urol. 2010;183(5):2070–2076. doi:10.1016/j.juro.2009.12.093
227. Tanda G. Preclinical studies on the reinforcing effects of cannabinoids. A tribute to the scientific research of Dr. Steve Goldberg. Psychopharmacology (Berl). 2016;233(10):1845–1866. doi:10.1007/s00213-016-4244-7
228. Tanda G, Goldberg SR. Cannabinoids: reward, dependence, and underlying neurochemical mechanisms–a review of recent preclinical data. Psychopharmacology (Berl). 2003;169(2):115–134. doi:10.1007/s00213-003-1485-z
229. Nazarian A, Are D, Tenayuca JM. Acetaminophen modulation of hydrocodone reward in rats. Pharmacol Biochem Behav. 2011;99(3):307–310. doi:10.1016/j.pbb.2011.05.003
230. Jouanjus E, Guernec G, Lapeyre-Mestre M; French Addictovigilance N. Medical prescriptions falsified by the patients: a 12-year national monitoring to assess prescription drug diversion. Fundam Clin Pharmacol. 2018;32(3):306–322. doi:10.1111/fcp.12356
231. Suzuki R, Rahman W, Hunt SP, Dickenson AH. Descending facilitatory control of mechanically evoked responses is enhanced in deep dorsal horn neurones following peripheral nerve injury. Brain Res. 2004;1019(1–2):68–76. doi:10.1016/j.brainres.2004.05.108
232. Dupuis A, Wattiez AS, Pinguet J, et al. Increasing spinal 5-HT2A receptor responsiveness mediates anti-allodynic effect and potentiates fluoxetine efficacy in neuropathic rats. Evidence for GABA release. Pharmacol Res. 2017;118:93–103. doi:10.1016/j.phrs.2016.09.021
233. Miller KE, Salvatierra AT. Apposition of enkephalin- and neurotensin-immunoreactive neurons by serotonin-immunoreactive varicosities in the rat spinal cord. Neuroscience. 1998;85(3):837–846. doi:10.1016/S0306-4522(97)00522-8
234. Pini LA, Vitale G, Ottani A, Sandrini M. Naloxone-reversible antinociception by paracetamol in the rat. J Pharmacol Exp Ther. 1997;280(2):934–940.
235. Pickering G, Loriot MA, Libert F, Eschalier A, Beaune P, Dubray C. Analgesic effect of acetaminophen in humans: first evidence of a central serotonergic mechanism. Clin Pharmacol Ther. 2006;79(4):371–378. doi:10.1016/j.clpt.2005.12.307
236. Durso GR, Luttrell A, Way BM. Way BM over-the-counter relief from pains and pleasures alike: acetaminophen blunts evaluation sensitivity to both negative and positive stimuli. Psychol Sci. 2015;26(6):750–758. doi:10.1177/0956797615570366
237. Dewall CN, Macdonald G, Webster GD, et al. Acetaminophen reduces social pain: behavioral and neural evidence. Psychol Sci. 2010;21(7):931–937. doi:10.1177/0956797610374741
238. Grundy L, Caldwell A, Brierley SM. Mechanisms underlying overactive bladder and interstitial cystitis/painful bladder syndrome. Front Neurosci. 2018;12:931. doi:10.3389/fnins.2018.00931
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.