Back to Journals » Patient Preference and Adherence » Volume 19
Systematic Review of Experimental Gingivitis Induction Methods: Methodological Variations and Their Impact on Inflammation Progression
Authors Jamjoom AG, Zahid TM ![]()
Received 29 August 2025
Accepted for publication 26 November 2025
Published 2 December 2025 Volume 2025:19 Pages 3835—3848
DOI https://doi.org/10.2147/PPA.S564132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Video abstract presented by Zahid.
Views: 26
Amal Ghazi Jamjoom,* Talal Mansoor Zahid*
Department of Periodontology, Faculty of Dentistry, King Abdulaziz University, Jeddah, 21589, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Amal Ghazi Jamjoom, Department of Periodontology, Faculty of Dentistry, King Abdulaziz University, PO Box 80200, Jeddah, 21589, Saudi Arabia, Email [email protected]
Aim: The purpose of this systematic review was to evaluate methodological variations and outcome patterns in experimental gingivitis studies in human populations. Specifically, differences in induction duration, plaque control strategies, participant characteristics, and their influence on clinical, molecular, and immunologic markers of gingival inflammation were assessed.
Methods: A systematic review of clinical trials and interventional studies involving experimental gingivitis induction via oral hygiene cessation or mechanical plaque accumulation was conducted. Eligible studies involved human participants and reported clinical (gingival index, bleeding on probing, plaque index) or biomarker outcomes. Data sources included peer-reviewed publications obtained through comprehensive database searches. Risk of bias and study quality were assessed. Findings were synthesized narratively due to heterogeneity in design and outcome measures.
Results: The included studies (n = 10) varied in induction duration (9– 28 days) and plaque accumulation method (full-mouth vs stent-based models). Clinical indicators consistently increased during induction phases, though magnitudes varied by methodology and participant profile. Studies identified “fast”, “slow”, and “low” responder phenotypes, underscoring inter-individual variability. Increased pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) and transcriptomic shifts were observed during active inflammation, with reversal during recovery. Methodological inconsistencies and a lack of standardization limited cross-study comparability.
Conclusion: Experimental gingivitis (EG) models reliably induce acute, reversible inflammation. However, methodological heterogeneity and insufficient adjustment for patient-related confounders hinder direct comparisons. Future research should adopt standardized protocols and incorporate stratified analyses to refine causal insights and support clinical translation.
Keywords: gingival index, inflammation, oral hygiene, periodontal diseases, plaque, transcriptome
Introduction
Gingivitis is a reversible inflammatory process of the gingiva, induced by the accumulation of microbial dental plaque at the gingival margin. Clinically, the lesion is symptomatic of redness, swelling, and bleeding on probing with no attachment loss or irreversible tissue damage, separating it from periodontitis and other more severe periodontal infections.1,2 It is widespread among all age groups and populations, as it is estimated that from 50 to 99% of the population has gingivitis at some point in their lives.3 This leads to gingivitis being a significant public health problem and the early, modifiable stage of periodontal disease development.4
To study the changes brought by dental plaque on the gingiva under strictly controlled conditions, Löe et al established the experimental gingivitis (EG) model. This landmark study demonstrated that cessation of oral hygiene in a previously systemically healthy subject would routinely lead to gingival inflammation associated with accumulation of supra-gingival plaque.4,5
It is commonly employed to study the pathogenesis of gingival inflammation, host-microbial interactions, preventive and therapeutic modalities in clinical as well as translational research.6,7 A further application was the formulation of inflammatory response phenotypes (high, low, and slow responders), each bearing different microbial and immunologic profiles.6
However, EG studies vary considerably in design. Protocol differences include induction duration (2–4 weeks), mode of induction (oral hygiene cessation vs mechanical plaque accumulation), and model type (full-mouth, partial-mouth, or stent-based). Such variability affects the timing, severity, and distribution of gingival inflammation, complicating direct comparisons across studies.6,7
The lack of standardized protocols and inconsistent use of clinical indices such as the Gingival Index (GI), Bleeding on Probing (BOP), and Plaque Index (PI) further limit comparability and may contribute to misclassification of outcomes.2,3 There is a need to fill such gaps by systematically testing different kinds of EG models to increase methodological soundness and reproducibility in periodontal research.
An appropriate systematic review is required to compile and evaluate the currently available EG methods, particularly given the growing interest in improving early diagnostic markers and the host-microbial relationship in gingival inflammation.3,6,7 Through systematic evaluation of the effects of these methodological variations on clinical outcomes, this review seeks to offer evidence-based recommendations to researchers regarding selection and optimization of EG protocols.1,4
The main research question addressed by this systematic review is: What is the methodological heterogeneity in EG induction studies, and how does this impact timing and progression of gingival inflammation?
To address this, these were further explored: (1) how induction methods affect inflammation onset; (2) variations in duration and model design; (3) differences in clinical outcomes (GI, PI, BOP); and (4) the extent to which secondary factors such as age, gender, and smoking are considered. The study quality and risk of bias using validated tools (RoB 2, ROBINS-I) were evaluated and provided recommendations for methodological standardization.
Materials and Methods
Protocol and Registration
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) [https://www.crd.york.ac.uk/PROSPERO/view/CRD42021234193] under the registration number CRD42021234193.
Focus Question
This systematic review was guided by a clearly defined research question structured according to the PICOS framework: What are the methodological variations in experimental gingivitis (EG) induction studies, and how do these differences affect the timing and progression of gingival inflammation? The population of interest includes human participants enrolled in EG studies. Interventions focus on various methods of inducing gingival inflammation, such as oral hygiene cessation and mechanical plaque accumulation. Comparisons involve different EG protocols, including variations in model design and duration. The primary outcomes assessed are the timing of inflammation onset and the progression of gingival inflammation, measured through established clinical parameters such as the Gingival Index (GI), Bleeding on Probing (BOP), and Plaque Index (PI).
Information Sources
A search was done: MEDLINE via PubMed, EMBASE, Scopus, Cochrane Library, and Google Scholar for grey literature. Additionally, the eligible articles’ reference lists were screened manually to ensure completeness.
Search
The search was done for articles published from January 2004 to June 2025. Key-words were selected using MeSH terms and free text, including: “Experimental gingivitis”, “Gingival inflammation”, “Plaque accumulation”, “Oral hygiene cessation”, “Periodontal research”, “Gingival index”, “Bleeding on probing”, “Plaque index”, “Methodological comparison”, “Clinical periodontology”, “Gingival disease models”, “Inflammation progression”, “Oral health research”, “Dental studies”. For transparency, an example of the exact PubMed syntax is provided here:
(“experimental gingivitis” OR “induced gingivitis”) AND (“plaque accumulation” OR “oral hygiene cessation”) AND (humans [MeSH Terms]).
The complete search strategies for all databases are available in the Supplementary Material.
Selection of Studies
Two blinded reviewers independently screened titles/abstracts and full texts against eligibility criteria, resolving disagreements by discussion or third reviewer consultation.
Types of Studies
Included study designs were randomized controlled trials (RCTs), controlled clinical trials (CCTs), and observational studies (cohort and cross-sectional). Studies published between 2004 and 2025 in English were considered. However, landmark studies prior to 2004 that introduced or validated critical methodological approaches were also included for historical and conceptual context.
Types of Participants/Population
Studies involving human participants undergoing experimental gingivitis protocols were included, with no restrictions on age, gender, or smoking status. Studies involving naturally occurring gingivitis or animal models were excluded. Inclusion criteria involved human participants undergoing experimental gingivitis (EG) protocols, explicitly assessed methodological variations, reported at least one clinical outcome related to gingival inflammation, specifically the Gingival Index (GI), Bleeding on Probing (BOP), or Plaque Index (PI), and clearly described the induction protocol and its duration. Studies were excluded if they focused on animal models without direct human relevance, were primarily interventional in nature (ie, aimed at treating gingivitis rather than inducing it), or failed to provide sufficient methodological detail or outcome data necessary for analysis.
Data Extraction
Two reviewers independently extracted data, including study design, setting, population characteristics, gingivitis induction protocols, and clinical outcomes (GI, BOP, PI)—with discrepancies resolved by discussion or a third reviewer. Systemic biomarkers were recorded when available, and each study’s risk of bias was assessed using design-appropriate tools.
Risk of Bias Within Studies
The risk of bias was independently assessed by two reviewers using design-specific, validated tools: RoB 2 (Cochrane Collaboration, London, UK) for RCTs, ROBINS-I (Cochrane, London, UK) for non-randomized interventional studies, and the Newcastle-Ottawa Scale for cohort studies. Disagreements were resolved by discussion or a third reviewer, and results were summarized narratively and in structured tables by study type (see Supplementary Tables 2–4).
Risk of Bias Across Studies
Risk of bias across studies was assessed qualitatively due to heterogeneity and insufficient studies per outcome for quantitative analysis. Funnel plots and Egger’s test were not applied; selective reporting was evaluated by comparing reported outcomes with methods, and any discrepancies were noted in the interpretation.
Statistical Analysis
Quantitative synthesis via meta-analysis was not feasible due to substantial heterogeneity in study designs, outcome measures, and reporting (eg, GI, BOP, PI units, and timing), as well as inconsistent statistical data and varied gingivitis induction protocols. As a result, the findings were synthesized narratively and presented in structured summary tables. Where available, between-group differences and within-subject comparisons were extracted and qualitatively summarized. Attempts to perform subgroup or sensitivity analyses were not conducted due to insufficient standardized data. Instead, methodological variations—such as induction duration, population characteristics, and outcome assessment strategies—were described in detail to inform future protocol standardization efforts in EG research.
Results
Study Selection
A total of 2572 records were identified through database searches: PubMed (1484), Embase (523), Scopus (369), Cochrane Library (76), and Google Scholar (120). After removal of 612 duplicates, 1960 titles and abstracts were screened for eligibility. Of these, 120 full-text articles were retrieved and assessed. Forty studies were excluded during full-text review, and ultimately, only 10 studies met the eligibility criteria out of nearly 2000 screened, underscoring the very limited evidence base available for synthesis (Figure 1).
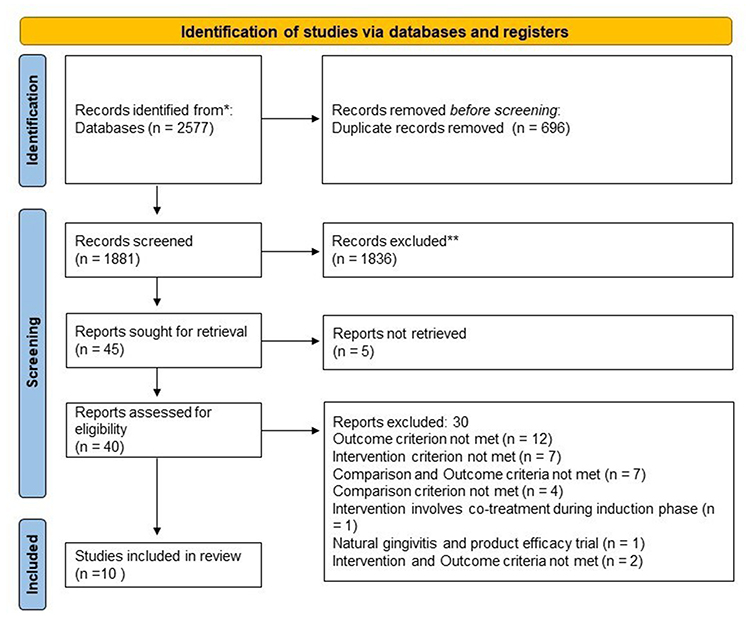 |
Figure 1 PRISMA flow diagram. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. |
Reasons for exclusion included: lack of comparison between EG induction protocols (n = 10), absence of relevant clinical outcomes (n = 19), combined intervention during induction (n = 6), and studies not focused on human populations or using natural gingivitis models (n = 5) (see Supplementary Table 1).
Study Characteristics
The 10 included studies (see Table 1) were published between 1977 and 2025 and comprised randomized controlled trials (n = 3), controlled clinical trials (n = 4), and prospective cohort or observational studies (n = 3). Sample sizes ranged from 8 to 60 participants, with populations generally comprising healthy adults aged 18–35. The limited number and size of these studies reduce generalizability, but their methodological diversity offers useful contrasts. Gingivitis was generally induced via oral hygiene cessation for periods ranging from 4 to 21 days, though one study employed a stent-based model with dietary modulation.
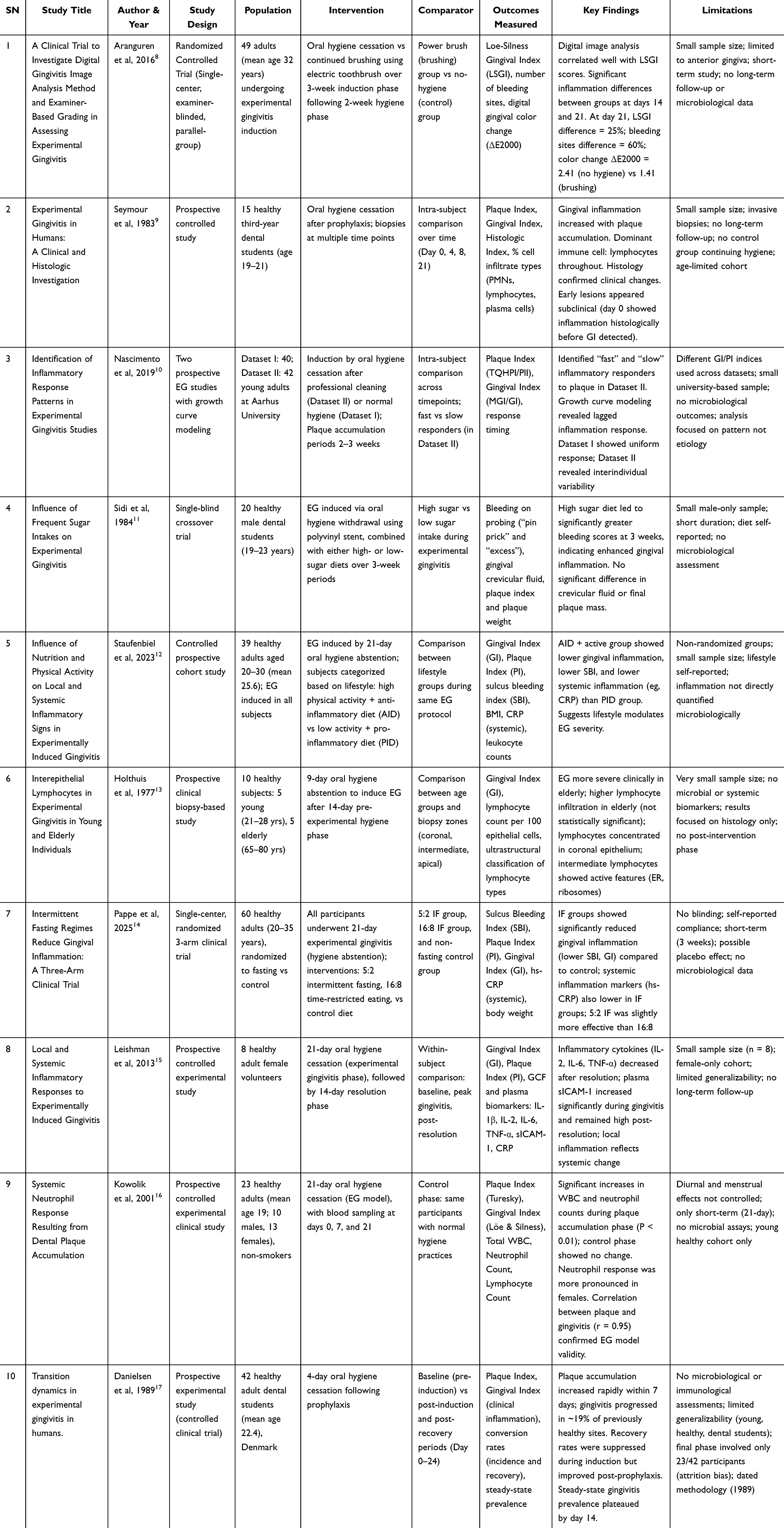 |
Table 1 Summary of Findings from Included Studies on Experimental Gingivitis Models |
To synthesize and highlight the diversity in experimental designs, Table 2 summarizes key methodological differences across the included studies, emphasizing design elements that influence interpretation and comparability.
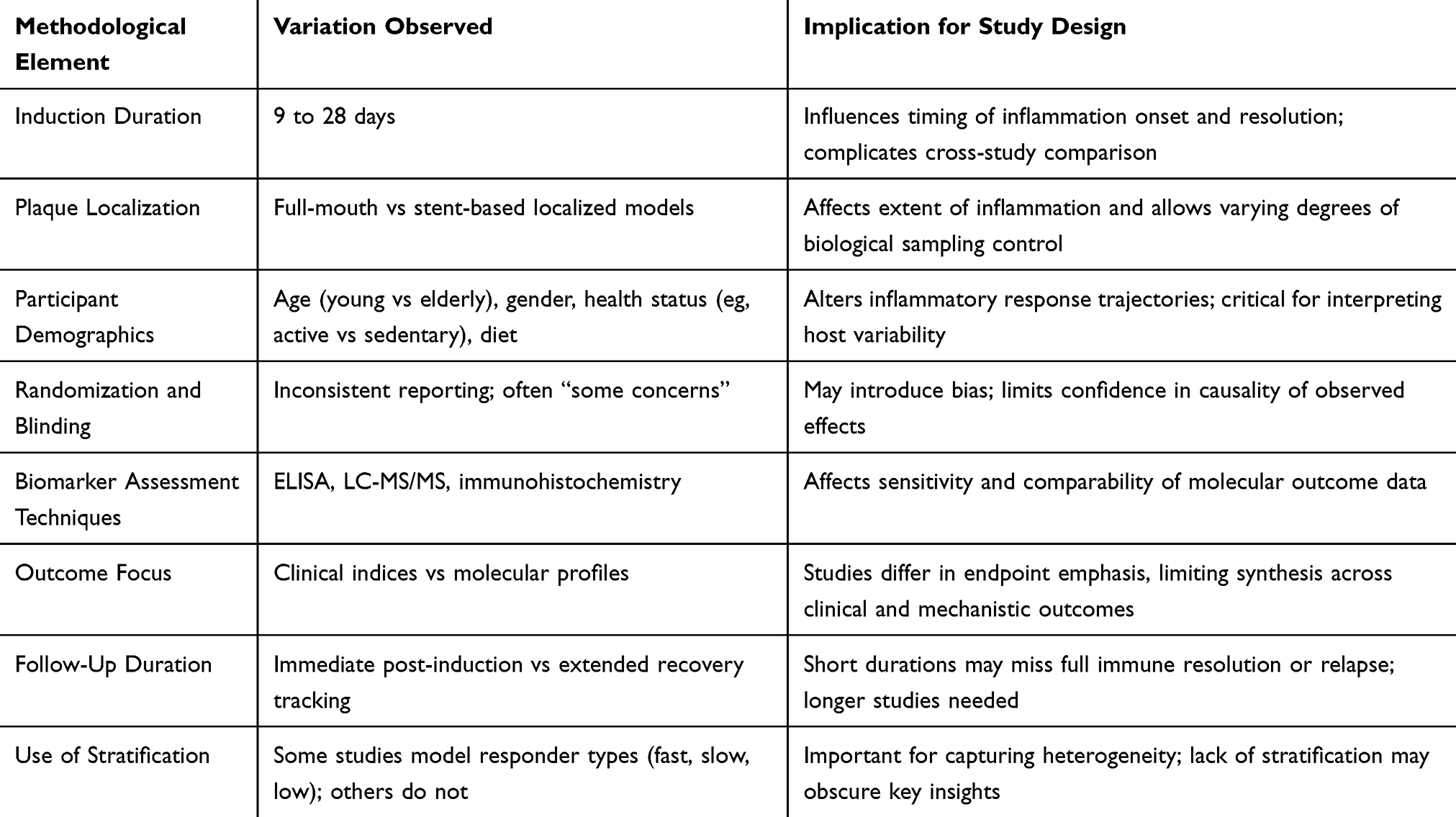 |
Table 2 Key Methodological Differences Among Included Experimental Gingivitis Studies |
Variation in Experimental Gingivitis Models
Induction Methods and Duration
Most studies employed the established Löe et al model, withdrawing oral hygiene to induce gingivitis over durations ranging from 9 to 21 days.5 Some research, such as Danielsen et al,17 enabled an in-depth analysis of the time to onset and resolution of symptoms and signs of inflammation. Pappe et al implemented modifications, with dietary recommendations provided for a 9-day induction.14
Outcome Measures
The most reported parameters were BOP, PI, GI, and GCF cytokine concentrations (eg, IL-6, TNF-α). Some studies extended outcome assessment to systemic markers, including plasma sICAM-1.15
Participant-Level Modifiers
The age, diet, general health, and the manner of fasting practice all had a contribution to the gingival response. Likewise, in fasting individuals, BOP and GCF levels were lower than in non-fasting individuals.14 Another study reported that the consumption of dietary sugar increased BOP with no significant effects on plaque deposition or GCF flow.11
Phenotypic Response Patterns
Inter-individual variation in profiles of inflammatory cytokines and in the rates of transition between health and inflammation was found to be high. Danielsen et al recorded sites in the gingiva showing oscillations from an inflamed to a non-inflamed condition even when the plaque load was kept constant, thus stressing the host-specific responses.17
Results of Individual Studies
The studies analysed presented substantial heterogeneity in terms of the induction of experimental gingivitis (EG) and the clinical parameters assessed. The gingival index (GI), plaque index (PI), and bleeding on probing (BOP) were the most frequently used indices.
For example, Aranguren (2016) reported a 25% lower GI and 60% fewer bleeding sites in the brushing group compared to the no-hygiene group by day 21.8 Similarly, Pappe et al found that intermittent fasting (IF) protocols significantly reduced GI and BOP relative to controls (eg, GI of 0.6 in the 5:2 fasting group vs GI of 1.3 in controls).14
Nascimento et al employed growth curve modeling and identified distinct inflammatory response patterns, categorizing participants as “fast” or “slow” responders.10 Fast responders exhibited GI increases of approximately 1.2 points during the induction phase.10
Sidi and Ashley (1984) found significantly higher BOP scores in participants on a high-sugar diet (p < .05).15 Kowolik et al documented approximately 20% increases in white blood cell and neutrophil counts during plaque accumulation, suggesting a systemic inflammatory response to EG.16
Incomplete reporting of effect sizes, standard deviations, and CIs precluded meta-analysis. Nevertheless, qualitative synthesis revealed that gingival inflammation varies meaningfully with diet, hygiene status, and systemic factors.
Table 3 presents a structured summary of these individual study outcomes, including sample sizes, induction protocols, comparator groups, primary outcomes measured, and key findings. This comparative overview facilitates cross-study interpretation and emphasizes the heterogeneity in both clinical and systemic responses to experimentally induced gingivitis.
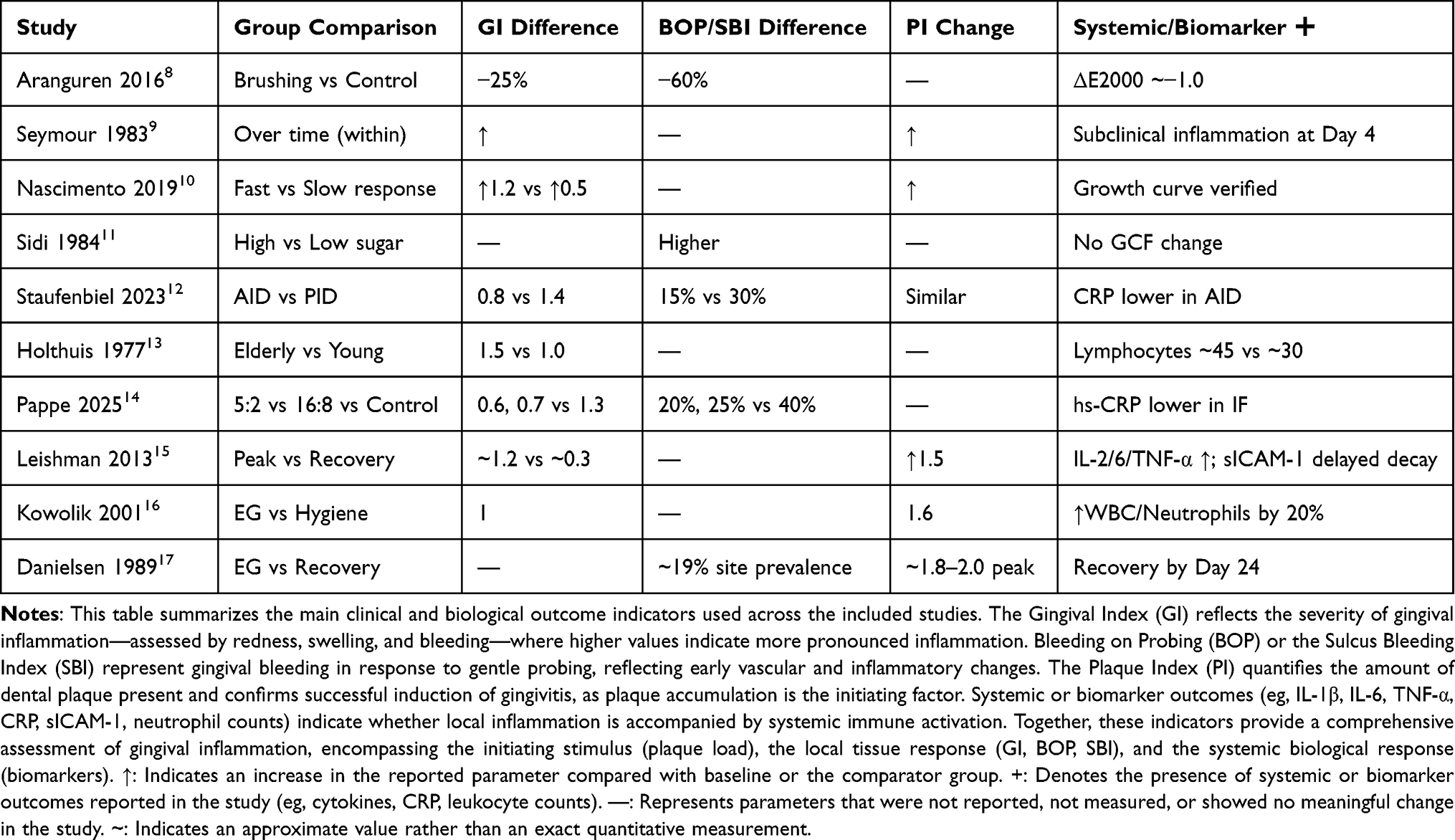 |
Table 3 Summary of Clinical and Biological Outcomes from Included Experimental Gingivitis Studies |
Synthesis of Results
The synthesis of findings across the ten included studies highlights consistent evidence that experimental gingivitis (EG) models reliably induce gingival inflammation through oral hygiene cessation, with or without additional dietary or behavioural interventions. Despite variations in study design, duration, and outcome measures, a core set of indices, including the Gingival Index (GI), Plaque Index (PI), and Bleeding on Probing (BOP), were frequently reported, supporting comparability. Most studies demonstrated statistically significant increases in gingival inflammation during EG induction phases, with improvements following re-initiation of hygiene practices or introduction of modulating interventions (eg, intermittent fasting or anti-inflammatory diets).
Due to heterogeneity in outcome reporting, intervention protocols, and statistical methodologies, a formal meta-analysis was not feasible. Key limitations included inconsistent provision of effect sizes, standard deviations, or confidence intervals, and in some cases, a lack of raw data. However, trends across studies suggest that diet, systemic health markers (eg, CRP, cytokines), and lifestyle factors (eg, physical activity) can influence the magnitude and dynamics of gingival inflammatory responses. Intervention groups employing anti-inflammatory strategies typically showed 20–60% reductions in GI or BOP scores compared to control conditions.
Measures of consistency were evaluated qualitatively. While statistical heterogeneity (eg, I2 statistics) could not be calculated, conceptual consistency was evident: all studies supported the reversibility of plaque-induced gingivitis and the potential modulation of local and systemic inflammation by non-hygienic factors. Future studies with harmonized protocols and complete statistical reporting will be essential to enable quantitative synthesis and more definitive effect estimates.
Risk of Bias Within Studies
A rigorous assessment of risk of bias was performed across all included studies using tools appropriate to their methodological design. This section details both the narrative and structured evaluations of bias. Randomized controlled trials (RCTs) were assessed using the Cochrane Risk of Bias 2.0 (RoB 2) tool, non-randomized interventional studies using the ROBINS-I framework, and observational cohort studies using the Newcastle-Ottawa Scale (NOS). Risk of bias was considered at both the study level and, when applicable, the outcome level. The results are presented in a combination of narrative synthesis and structured summary tables for clarity.
To ensure transparency in the review process, Supplementary Table 1 presents a list of full-text studies excluded during eligibility screening, along with specific reasons for exclusion. Most commonly, studies failed to meet the comparison or outcome criteria—focusing solely on biochemical markers or involving co-interventions during the induction phase, which conflicted with this review’s objective of evaluating methodological variation in EG induction protocols.
For randomized controlled trials, Supplementary Table 2 and Figure 2 provide a domain-level RoB 2 assessment. Three RCTs8,11,14 were categorized as having “some concerns” overall. This was primarily due to limitations in allocation concealment, inability to blind participants (a typical challenge in EG studies), and absence of pre-registered analysis plans. However, outcome measurement was typically robust due to the use of objective clinical indices such as Gingival Index (GI) and Bleeding on Probing (BOP), and examiner blinding was commonly reported.
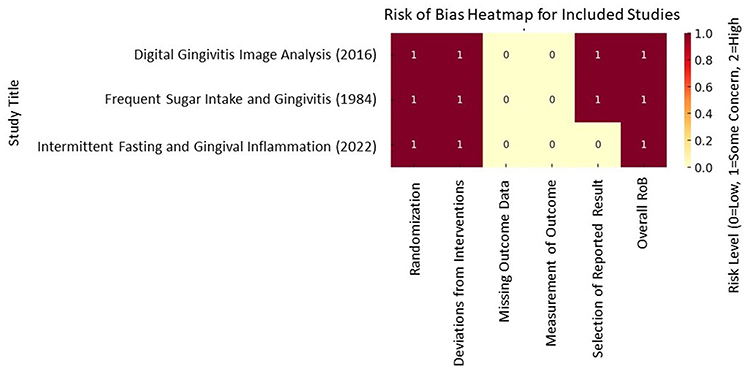 |
Figure 2 Risk of Bias Heatmap for 3 randomized controlled trial among the included studies. |
Non-randomized studies, detailed in Supplementary Table 3, showed a broader range of risk. Seymour et al9 had a moderate risk, whereas Leishman et al,15 Kowolik et al,16 and Danielsen et al17 were judged to be at serious risk, largely due to potential confounding, incomplete follow-up, or selective outcome emphasis. In contrast, Supplementary Table 4 summarizes NOS evaluations for three cohort studies.10,12 All were judged to be of “Good” quality by AHRQ criteria, although limited representativeness and absence of blinded outcome assessment slightly constrained their reliability. Collectively, these evaluations highlight the need for greater methodological rigor and standardization in EG induction protocols.
Risk of Bias Across Studies
The cumulative assessment of risk of bias across the included literature suggests that the overall quality of evidence is moderate, with consistent methodological limitations that may affect the interpretation and generalizability of findings. The most frequent sources of bias across studies were small sample sizes, lack of participant blinding, and inadequate reporting of randomization procedures or allocation concealment. Although several studies used examiner blinding and objective indices (eg, GI, PI, BOP), the inability to blind participants in oral hygiene cessation models introduces potential performance bias. Additionally, no study included a prospectively registered protocol, increasing the likelihood of selective reporting. Publication bias was not formally assessed due to a lack of effect size data, but small studies with positive results may indicate selective reporting. Across-study variability in outcome definitions and induction protocols limited cross-study synthesis. Still, directional consistency (eg, plaque → increased GI/BOP) lends support to findings.
Discussion
Experimental gingivitis (EG) models consistently show that cessation of oral hygiene rapidly induces gingival inflammation, with resolution upon resuming regular oral care. This reproducibility underscores EG’s role as a robust model for studying reversible periodontal inflammation. However, the translation of these controlled findings into daily life depends heavily on patient adherence to oral hygiene practices. In real-world settings, lapses in compliance are frequent, and the biological response patterns identified in EG studies— “fast”, “slow”, or “low” responders—highlight how variability in patient behaviour and biological predisposition interact.
Importantly, EG studies emphasize that simple behavioural interventions, such as consistent toothbrushing and dietary control, have profound effects on disease onset and resolution. Findings that intermittent fasting or reduced sugar intake modulate gingival inflammation suggest that adherence to preventive lifestyles directly influences oral outcomes. From a clinical perspective, the EG model illustrates the tangible consequences of poor adherence: within 14–21 days of hygiene neglect, inflammation reliably develops, while reintroduction of hygiene demonstrates the benefits of even modest improvements. This rapid feedback loop can be leveraged in patient education and in tailoring preventive strategies to responder phenotypes.
The classical 21-day model introduced by Löe et al remains the gold standard, confirming that plaque accumulation alone is sufficient to trigger reversible gingivitis. Decades of follow-up studies have reproduced this paradigm and tested variables such as age, lifestyle, and diet, further verifying its validity.7 For example, Holm-Pedersen et al showed greater inflammation in older individuals, while high sugar intake aggravated gingivitis severity.18
At the systemic level, the rise in inflammatory biomarkers such as IL-6 and CRP during EG induction illustrates that adherence lapses may have implications beyond oral health. This highlights the importance of supporting patient compliance not only for local gingival outcomes but also for broader systemic well-being.
The ability to reproduce gingival inflammation in several studies illustrates the model’s stability as a consistent means of investigating acute, reversible mucosal inflammation. Its reproducible course of development and regression ensures that it is used in testing interventions as well as studies of disease pathogenesis in a controlled environment.5,11 Yet, individual differences in response trajectory profiles, eg, “fast”, “slow”, “low” responders, hint at differences in immune and microbial regulation that dictate between-individual and between-site variation in timing and strength of inflammation.6,10,17 This heterogeneity stresses the importance of an individualized approach to analysis, whether in clinical practice or research. At the molecular level, high levels of pro-inflammatory cytokines, IL-1β, IL-6, and TNF-α during induction and systemic responses such as the rise in neutrophil number and soluble ICAM-1, are indicative of a more general immunologic activation besides local tissue changes.12,15,19 Such alterations of biomarkers provide functional information and potential surrogate endpoints for future clinical studies.
In this respect, it can be assumed that the 21-day model of oral hygiene discontinuation, introduced by Löe (1965) and coworkers, is the gold standard, and it still serves as a foundation work for experimental gingivitis investigation by showing that plaque formation is the only cause of reversible inflammatory changes of the gingivae. Decades of research have continued to confirm the validity of the model, which is regarded as a control for the induction of inflammation.5 Follow-up studies have developed and verified the basic paradigm, and tested variables that might affect the outcome of inflammatory processes.
For example, Holm-Pedersen et al showed that gingival inflammation is different in magnitude between young and old subjects, highlighting the role of age in modulation of host response. Consistently, papers examining nutritional influences have supported the role of sugar in aggravating plaque-induced inflammation, further suggesting a relationship between diet and gingival health.12,18 At the molecular level, the work by Eberhard et al and Leishman et al demonstrated that overall inflammatory markers (hsCRP, IL-6, and TNF-α) are elevated after the induction of localized gingivitis, illustrating the systemic values associated with oral inflammation.15,19 These cytokines drive leukocyte recruitment, vascular permeability, and tissue remodelling, key events in early gingival inflammation. Additionally, systemic responses—such as elevations in neutrophil counts and soluble intercellular adhesion molecule-1 (sICAM-1)—indicate that even localized gingival inflammation can trigger broader immunological signaling.12,15,19 The concurrent rise in sICAM-1 suggests endothelial activation, possibly linking gingival inflammation to vascular inflammatory processes relevant in systemic diseases. Such biomarker dynamics not only provide insight into the underlying mechanisms of inflammation but also offer measurable, temporally sensitive surrogate endpoints for intervention trials.
This review included only 10 studies out of over 1900 screened titles, reflecting a limited evidence base that constrains the generalizability of findings. Nevertheless, the included studies encompassed a variety of experimental gingivitis (EG) models, notably both whole-mouth and stent-type designs, which enhances applicability across clinical contexts. The use of both clinical parameters (eg, gingival index, bleeding on probing) and molecular data (eg, cytokines, transcriptomic profiles) allowed for a multidimensional assessment of inflammation. Additionally, the identification of host-response phenotypes (eg, “fast” vs “slow” responders) added interpretive depth regarding interindividual variation in inflammatory dynamics.
Despite these strengths, several limitations should be noted. The lack of standardized protocols across studies—especially for induction duration and recovery—reduces comparability. Most studies were short-term in design and lacked longitudinal follow-up, preventing insights into the sustained or systemic consequences of EG.
Furthermore, publication and language bias may have skewed the results, as non-English and unpublished (grey) literature were excluded. This may have led to an overrepresentation of studies reporting positive effects.
Methodologically, the included studies often suffered from inconsistent reporting of critical features, including randomization methods, blinding procedures, and participant selection criteria—introducing risk of bias and limiting reproducibility. There was also substantial heterogeneity in protocols, including the duration of induction (9 to 28 days), the mode of plaque accumulation (full-mouth vs stent-type), and participant characteristics (eg, age, dietary habits, physical activity levels).
Finally, biomarker-related limitations were notable There was significant variability in the sampling methods (eg, saliva vs GCF) and analytical platforms (eg, ELISA vs LC-MS/MS), which complicates synthesis across studies. While molecular results were informative, the interpretation remained largely descriptive. Future reviews should aim for mechanistic integration, linking molecular profiles with clinical outcomes and inflammatory trajectories.
The significance of experimental gingivitis models for practice and policy is substantial. The ubiquitous finding of variability in individuals’ inflammatory response as fast, slow, or low responders is a promising potential for personalized oral care. These findings may be translated by clinicians to categorize patients into different risk groups and tailor oral hygiene programs and preventive measures accordingly.6,10,20 Furthermore, EG models provide a consistent and monitored model for the assessment of the development and resolution of inflammation that provides valid surrogate endpoints for clinical trials investigating periodontal treatments or systemic anti-inflammatory agents.15,19 The ability to identify local oral inflammation and systemic biomarker associations provides additional evidence for the application of the models in the context of an integrative-based healthcare approach.
Achieving progress in this field will require future research to emphasize the development and adoption of standardized experimental protocols. In particular, standardization of cessation of oral hygiene time, techniques to localize plaque (full-mouth, stent-based), and definitions of the recovery healing phase are necessary to enhance reproducibility and comparability between studies.8,14 Furthermore, the composition of the participating cohort should be broadened to include individuals from underrepresented groups, such as older people, etc., in order to enhance generalizability and to show subgroup-specific risk patterns.12,18 Further, the incorporation of high-resolution molecular tools that construct maps with transcriptomics, proteomics, and metabolomics, as well as longitudinal study designs, would help provide a more complete model of the initiation and resolution of inflammation.21,22 These advances will provide for a better understanding of the biological pathways in gingival inflammation and the related systemic ramifications.
Conclusions
This review confirms that experimental gingivitis models reliably reproduce reversible inflammation within short periods of oral hygiene discontinuation. Methodological heterogeneity—differences in induction time, plaque control, and participant characteristics—creates variability in outcomes, but the universal lesson is clear: adherence to oral hygiene practices is decisive in determining gingival health.
By framing EG findings in the context of patient behavior, the review underscores the critical role of adherence to preventive care. The recognition of responder phenotypes provides an additional dimension for personalized oral health strategies, supporting tailored education and adherence interventions. Future studies should not only refine methodological consistency but also explore how adherence behaviors and patient preferences intersect with biological variability to inform effective, individualized preventive approaches.
In conclusion, EG models continue to provide key insights into inflammation dynamics, but their most significant contribution lies in revealing how patient adherence to oral hygiene profoundly influences gingival and systemic health. This emphasizes the urgent need to prioritize adherence-driven strategies in both clinical care and broader public health initiatives.
Abbreviations
EG, Experimental gingivitis; GI, Gingival Index; PI, Plaque Index; BOP, Bleeding on Probing; RCT, Randomized controlled trials; GCF, Gingival crevicular fluid; IF, Intermittent fasting.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Murakami S, Mealey BL, Mariotti A, Chapple ILC. Dental plaque-induced gingival conditions. J Periodontol. 2018;89 Suppl 1:S17–s27. doi:10.1002/JPER.17-0095
2. Preethanath R, Ibraheem W, Anil A. Pathogenesis of gingivitis. In: Oral Diseases. IntechOpen; 2020.
3. Trombelli L, Farina R, Silva CO, Tatakis DN. Plaque-induced gingivitis: case definition and diagnostic considerations. J Clin Periodontol. 2018;45 Suppl 20:S44–s67. doi:10.1111/jcpe.12939
4. Chapple ILC, Mealey BL, Van Dyke TE, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: consensus report of workgroup 1 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89 Suppl 1:S74–s84. doi:10.1002/JPER.17-0719
5. Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36(3):177–187. doi:10.1902/jop.1965.36.3.177
6. Bamashmous S, Kotsakis GA, Kerns KA, et al. Human variation in gingival inflammation. Proc Natl Acad Sci U S A. 2021;118(27). doi:10.1073/pnas.2012578118
7. Hsu YT, Lee HL, Wen B, Daubert D, Darveau R. Gingival crevicular fluid during experimental gingivitis: a review of immune and tissue regulation. J Periodontol. 2025;96(10):1099–1112. doi:10.1002/JPER.24-0715
8. Aranguren L. A Clinical Trial to Investigate Digital Gingivitis Image Analysis Method and Examiner-Based Grading in Assessing Experimental Gingivitis. University of Connecticut Graduate School; 2016.
9. Seymour GJ, Powell RN, Cole KL, et al. Experimental gingivitis in humans. J Periodontal Res. 1983;18(4):375–385. doi:10.1111/j.1600-0765.1983.tb00373.x
10. Nascimento GG, Danielsen B, Baelum V, Lopez R. Identification of inflammatory response patterns in experimental gingivitis studies. Eur J Oral Sci. 2019;127(1):33–39. doi:10.1111/eos.12588
11. Sidi AD, Ashley FP. Influence of frequent sugar intakes on experimental gingivitis. J Periodontol. 1984;55(7):419–423. doi:10.1902/jop.1984.55.7.419
12. Staufenbiel I, Adam K, Hahn A, et al. Influence of nutrition and physical activity on local and systemic inflammatory signs in experimentally induced gingivitis. Nutrients. 2023;15(15):3344. doi:10.3390/nu15153344
13. Holthuis AF, Holm-Pedersen P, Folke LEA. Interepithelial lymphocytes in experimental gingivitis in young and elderly individuals. J Periodontal Res. 1977;12(3):166–178. doi:10.1111/j.1600-0765.1977.tb00120.x
14. Pappe CL, Maetschker J, Dujardin S, et al. Intermittent fasting regimes reduce gingival inflammation: a three-arm clinical trial. J Clin Periodontol. 2025;52(5):681–694. doi:10.1111/jcpe.14151
15. Leishman SJ, Seymour GJ, Ford PJ. Local and systemic inflammatory responses to experimentally induced gingivitis. Dis Markers. 2013;35(5):543–549. doi:10.1155/2013/948569
16. Kowolik MJ, Dowsett SA, Rodriguez J, De La Rosa RM, Eckert GJ. Systemic neutrophil response resulting from dental plaque accumulation. J Periodontol. 2001;72(2):146–151. doi:10.1902/jop.2001.72.2.146
17. Danielsen B, Manji F, Nagelkerke N, Fejerskov O, Baelum V. Transition dynamics in experimental gingivitis in humans. J Periodontal Res. 1989;24(4):254–260. doi:10.1111/j.1600-0765.1989.tb01790.x
18. Holm-Pedersen P, Agerbaek N, Theilade E. Experimental gingivitis in young and elderly individuals. J Clin Periodontol. 1975;2(1):14–24. doi:10.1111/j.1600-051X.1975.tb01722.x
19. Eberhard J, Grote K, Luchtefeld M, et al. Experimental gingivitis induces systemic inflammatory markers in young healthy individuals: a single-subject interventional study. PLoS One. 2013;8(2):e55265. doi:10.1371/journal.pone.0055265
20. Zemouri C, Jakubovics NS, Crielaard W, et al. Resistance and resilience to experimental gingivitis: a systematic scoping review. BMC Oral Health. 2019;19(1):212. doi:10.1186/s12903-019-0889-z
21. Jönsson D, Ramberg P, Demmer RT, Kebschull M, Dahlén G, Papapanou PN. Gingival tissue transcriptomes in experimental gingivitis. J Clin Periodontol. 2011;38(7):599–611. doi:10.1111/j.1600-051X.2011.01719.x
22. Offenbacher S, Barros S, Mendoza L, et al. Changes in gingival crevicular fluid inflammatory mediator levels during the induction and resolution of experimental gingivitis in humans. J Clin Periodontol. 2010;37(4):324–333. doi:10.1111/j.1600-051X.2010.01543.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.