Back to Journals » Clinical Ophthalmology » Volume 19
Systematic Review of Clinical Practice Guidelines for Post-Cataract Surgery Endophthalmitis Prophylaxis from 2008-2023
Authors Surawatsatien N ![]() , Kasetsuwan P
, Kasetsuwan P ![]() , Pruksacholavit J, Chansangpetch S
, Pruksacholavit J, Chansangpetch S ![]() , Tulvatana W
, Tulvatana W ![]() , Pongsachareonnont PF
, Pongsachareonnont PF ![]() , Susantitaphong P, Reinprayoon U
, Susantitaphong P, Reinprayoon U
Received 7 August 2025
Accepted for publication 14 October 2025
Published 27 October 2025 Volume 2025:19 Pages 3949—3960
DOI https://doi.org/10.2147/OPTH.S559156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Nuntachai Surawatsatien,1,2 Pimpetch Kasetsuwan,2,3 Jipada Pruksacholavit,2,3 Sunee Chansangpetch,2,4 Wasee Tulvatana,2,3 Pear Ferreira Pongsachareonnont,1,5 Paweena Susantitaphong,6,7 Usanee Reinprayoon2,8
1Center of Excellence in Retina, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 3Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 4Center of Excellence in Glaucoma, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Department of Ophthalmology, Faculty of Health Sciences, Queen’s University, Kingston, Ontario, Canada; 6Division of Nephrology, Department of Medicine, Faculty of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn University, Thai Red Cross Society, Bangkok, Thailand; 7Center of Excellence for Metabolic Bone Disease in CKD Patients, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 8Center of Excellence for Cornea and Stem Cell Transplantation, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Usanee Reinprayoon, Center of Excellence for Cornea and Stem Cell Transplantation, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, 1873 Rama IV Road, Pathumwan, Bangkok, Thailand, Email [email protected]
Abstract: Postoperative endophthalmitis remains a significant concern following cataract surgery with a potential for severe vision loss. Although numerous clinical practice guidelines (CPGs) have been published worldwide, they offer differing recommendations for prophylactic measures. This systematic review aimed to synthesize and evaluate existing guidelines for endophthalmitis prophylaxis after cataract surgery. A comprehensive search including citation and gray literature search was conducted. Authors’ contact with peer international ophthalmologists was also employed. Clinical practice guidelines specifically on post-cataract surgery endophthalmitis prophylaxis published between 2008 and 2023 were included in this study. Quality assessment was done using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) tool. Twenty-one guidelines were identified, assessed, and extracted. Intracameral antibiotics, instillation of povidone-iodine into the conjunctival sac, and periorbital skin preparation with povidone-iodine were the most commonly endorsed measures, although recommended concentrations, dosages, and contact times varied. Several guidelines did not address ancillary measures, such as face washing, postoperative eye protection or adjunctive topical antibiotics. While core prophylactic strategies were broadly agreed upon, significant differences persisted likely due to disparate local regulations, idiosyncratic practices, and interpretations of the evidence. Careful selection and employment of any procedure should be tailored according to patient characteristics and circumstances.
Keywords: phacoemulsification, infection, antibiotics, intracameral, prevention
Introduction
Cataract surgery is the most commonly performed surgery by ophthalmologists globally. Prevalence continues to increase due to longer life expectancies.1 Countries with significant elderly populations, such as Japan, China, Singapore, and Thailand, are likely to experience an increasing demand for cataract surgery.2 Cataract surgery plays a crucial role for restoring vision and improving the quality of life for individuals affected by cataracts.3
Postoperative endophthalmitis, though relatively rare, represents a devastating complication following cataract surgery, resulting in significant visual impairment or even blindness. Estimated healthcare costs for postoperative endophthalmitis in the United States was US$6,442.13 with a total cost of US$15,833.53 from a societal perspective.4 Reported incidence rates of endophthalmitis after cataract surgery vary widely across countries and studies, ranging from 0.01% to 0.22% in Asian countries, 0.04%–0.7% in European countries, and 0%–0.29% in the United States.5 There has been an overall decline in incidence during the 21st century.6 This decline can be attributed to an enhanced understanding of risk factors, advancements in preventive measures for infectious control during cataract surgery, such as preoperative antisepsis and antibiotics use before, during, and after surgery, and improvements in surgical techniques.7
Many international academic organizations such as the American Academy of Ophthalmology (AAO)8 and the European Society of Cataract and Refractive Surgeons (ESCRS)9 have established practice guidelines aimed at preventing such complications in cataract surgeries. It is crucial for countries to adopt these guidelines, with a primary focus on reducing endophthalmitis rates while also examining factors such as feasibility, cost-effectiveness, and government funding for preventive measures.
According to the results of the ESCRS guidelines, the prophylactic administration of intracameral cefuroxime at the end of the cataract surgery and the utilization of acrylic intraocular lens (IOL) optic material instead of silicone IOLs significantly reduced the risk of postoperative endophthalmitis.9 Despite originating from a multinational, multicenter investigation involving 16,603 participants, the results of the ESCRS endophthalmitis report were interpreted and published over a decade ago. However, in a world where cataract surgeries are routinely performed, a global consensus on the optimal strategy for post-cataract surgery endophthalmitis prophylaxis remains elusive.10 Even with the established efficacy of prophylactic measures such as intracameral antibiotics and preoperative antisepsis, their implementation remains a subject of ongoing debate and inconsistent adoption, reflecting differences in regional guidelines and resource availability.10 This study aimed to systematically present and synthesize current evidence and recommendations on prophylactic strategies to prevent post-cataract surgery endophthalmitis.
Materials and Methods
This study collected and reviewed guidelines related to post-cataract surgery endophthalmitis prophylaxis and was constructed using the Patient, Intervention, Comparison, and Outcome (PICO) framework. The population consisted of adult patients who underwent cataract surgery. The intervention focused on perioperative measures aimed at prevention against post-cataract surgery endophthalmitis, with no specific comparators or control groups identified. The outcome was the recommended procedures or practices. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used in reporting study results. The International Prospective Register of Systematic Reviews (PROSPERO) registration number of the study is CRD42025648605.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were established for selecting studies on post-cataract surgery endophthalmitis prophylaxis to be reviewed. Studies meeting the following criteria were considered for inclusion: clinical practice guidelines specifically on post-cataract surgery endophthalmitis prophylaxis published within the study’s timeframe. Exclusion criteria comprised non-guideline literature, clinical practice guidelines with incorrect interventions, and publications not directly relevant to post-cataract surgery endophthalmitis prophylaxis. To guarantee the authority, rigor, and accountability of the recommendations, we further excluded CPGs that lacked endorsement by a national or international ophthalmology organization, as well as manuscripts without a declaration of author affiliation.
Search Strategy and Study Selection
A systematic literature search strategy was conducted across multiple databases, including Medline, Scopus, Embase and Cochrane Library. Keywords such as “cataract”, “cataract surgery”, “endophthalmitis”, “eye or ocular infection”, “prophylaxis”, “prevention”, “preemptive”, “antimicrobial”, “antibiotic”, “antiseptic”, “infectious control”, “recommendation”, “practice”, and “guideline” were utilized and combined using Boolean operators. Example search query are listed in Supplementary Materials. Additionally, citation searches and gray literature including Google Scholar, Guidelines International Network (GIN), the National Institute for Health and Care Excellence (NICE), and personal investigators’ contact with international ophthalmologists were employed to identify additional relevant studies. Electronic searches covered the period from 1st January, 2008 until 29th September, 2023, without language restriction. References were imported in Covidence for further screening. Duplicates were identified and removed both manually and automatically. An initial screening of titles and abstracts was conducted independently by two reviewers with several studies were excluded at this stage due to irrelevancy. Subsequently, full-text reviews were carried out by two independent reviewers to eliminate studies that inadvertently met the exclusion criteria. In case of any discrepancies, a third independent reviewer resolved the disagreement.
Data Extraction
A data extraction form was systematically constructed to cover various aspects of post-cataract surgery endophthalmitis prophylaxis. To avoid bias, misinterpretation and missing outcomes, a careful process on data extraction was done in Covidence Systematic Review Tool by two independent reviewers. The extracted information included research title, date of form completion, year of publication, study location, funding detail (with the name of the funding organization, if disclosed), area of use, study method, perioperative measures such as use of antibiotics before, during, and after surgery (including agent, route, duration, and frequency) as well as other interventions like face washing, lid cleansing, conjunctival sac instillation, eyelash trimming, surgical technique, eye patching, and any additional interventions or recommendations for endophthalmitis prevention following cataract surgery. If the extracted data by two reviewers was inconsistent, a third independent reviewer would make a decision.
Quality Assessment
Two independent assessors evaluated the included CPGs using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument.11 The instrument is comprised of 23 items organized into six domains: scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability, and editorial independence. Each item is rated on a scale from 1 (strongly disagree) to 7 (strongly agree). The scores are then calculated following the AGREE II methodology.11 The inter-rater reliability or discrepancy between assessors was calculated using methods described in previous study by calculating the average standard deviation of each domain.12 Discrepancies are classified as low when assessors’ scores fall within 1.5 standard deviations (SD) of the mean domain score. A medium discrepancy is noted when scores range between 1.5 and 2 SDs from the mean, while a high discrepancy is defined as scores exceeding 2 SDs from the mean domain score. If a high discrepancy is identified or if the assessors’ scores differ by more than 2 points, the domain undergoes re-evaluation. The quality of the guidelines are categorized according to the previous study.12 High-quality CPGs were those that achieved a score of at least 60% in three or more of the six AGREE II domains, including Domain 3 (rigor of development). Moderate-quality CPGs also scored at least 60% in three domains, but excluded Domain 3. Low-quality CPGs were defined as those scoring below 60% in two or more domains and less than 50% in Domain 3, indicating weaker methodological rigor.
Results
Of 710 articles that were identified through online databases, 431 articles were screened by the reviewers. After thoroughly inspecting for each criteria, a consensus was reached on relevant studies resulting in a total of 21 studies eligible for data extraction and inclusion in this systematic review. A schematic presentation of the literature search process is provided in Figure 1. The majority of CPGs were of moderate to high quality. No discrepancies were observed in the quality assessment between two graders. A summary of each study including quality assessment is listed in Table 1.
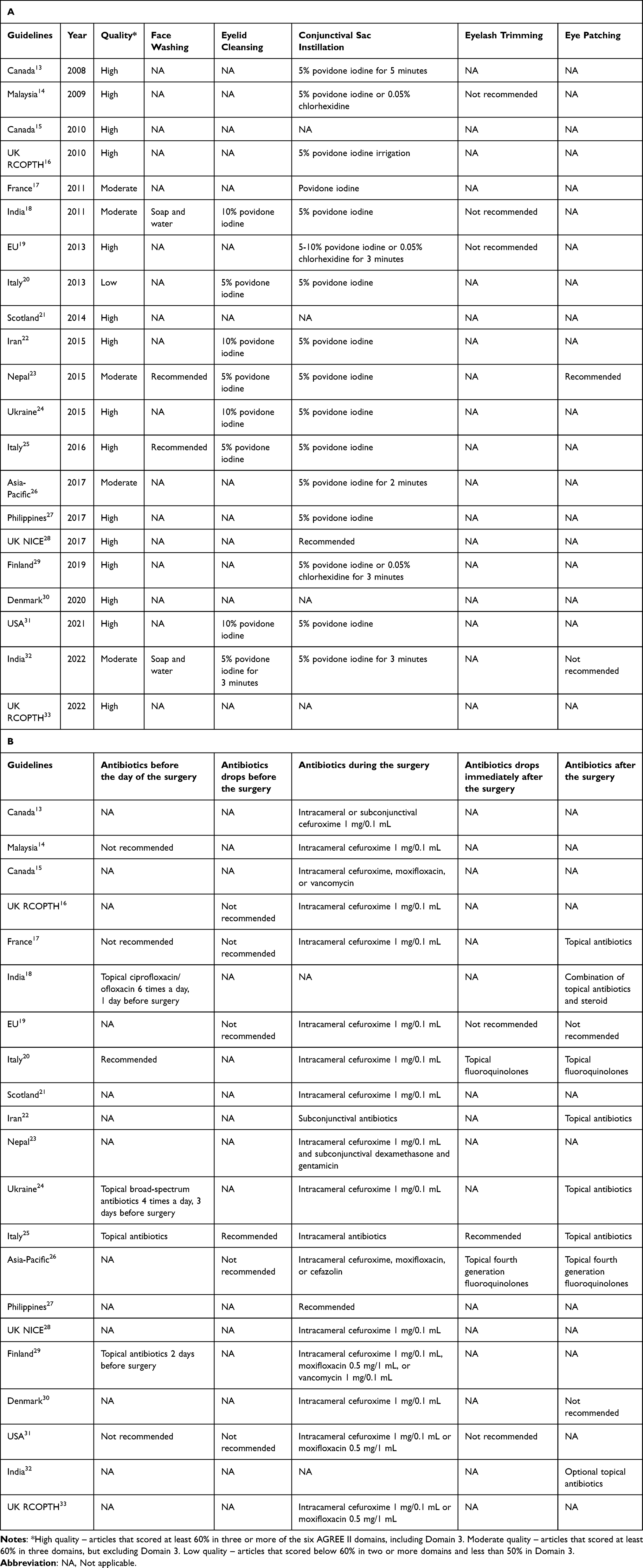 |
Table 1 Summary of the Procedures in the Included Literatures (A) and Summary of the Perioperative Antibiotics in the Included Literatures (B) |
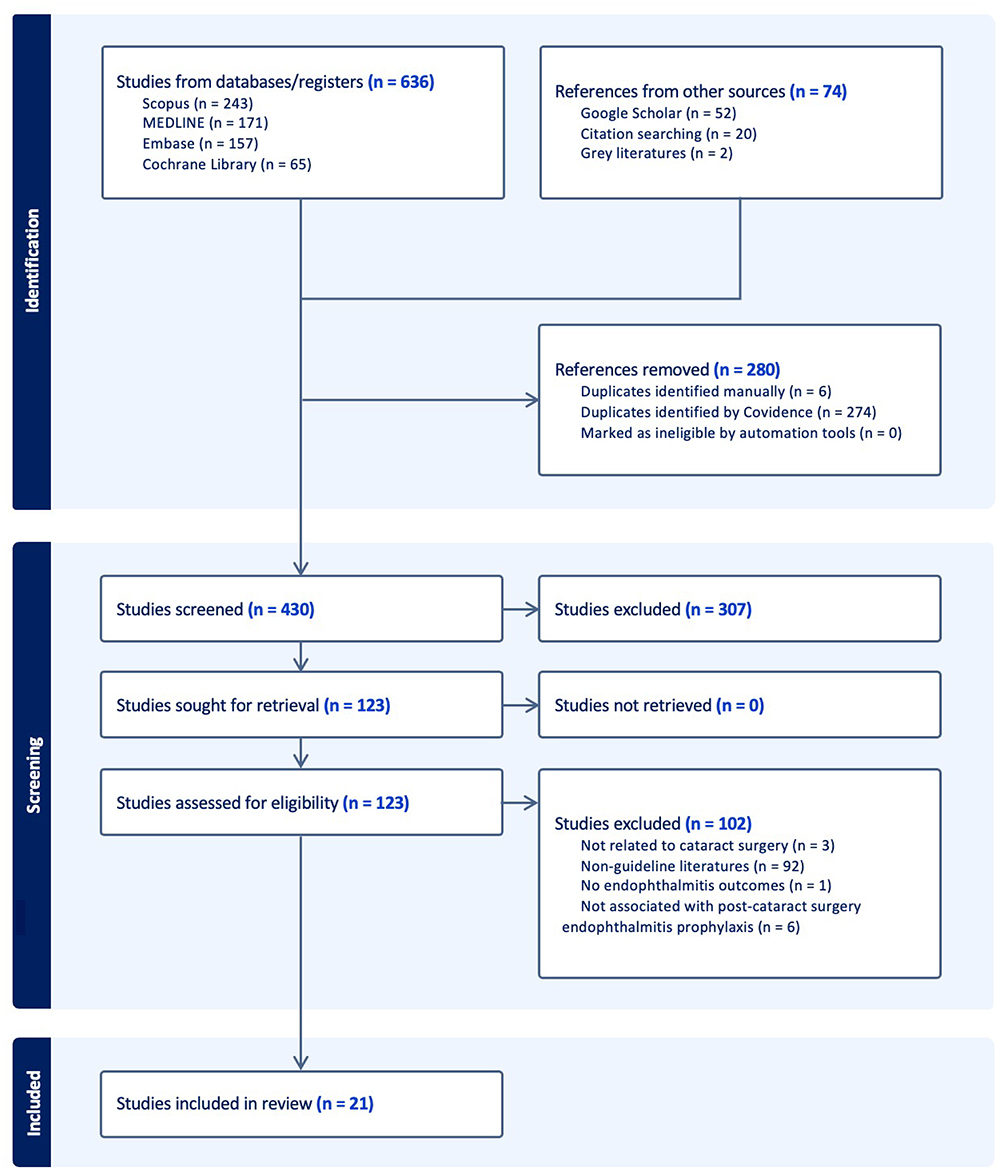 |
Figure 1 A schematic presentation of the literature search process. Bold text indicated total number of studies in each stage. |
Antibiotics Before the Day of the Surgery
Most guidelines (13/21) did not specify whether antibiotics are recommended before the day of the surgery or not. Five guidelines recommended the use of topical antibiotics.18,20,24,25,29 The recommended agent was specified only in one study, which was topical ciprofloxacin or ofloxacin.18 The recommended duration of topical antibiotics was 1–3 days before the surgery.18,24,29 Three guidelines recommended not to use antibiotics before the surgery.14,17,31
Face Washing
Only 4 guidelines made the recommendation on face washing prior to surgery.18,23,25,32 The recommended washing agents were soap and water.18,32 The remaining literature (17/21) did not make a recommendation on this issue.
Eyelid Cleansing
Majority of the guidelines (13/21) did not address this issue. All the remaining articles recommended 5–10% povidone iodine solution for periorbital skin cleansing.18,20,22–25,31,32 Only one article mentioned a 3 minute duration for the cleansing process.32 No guidelines mentioned eyelid scrubbing.
Conjunctival Sac Antiseptic Instillation
Almost all guidelines (17/21) recommended conjunctival sac instillation with 5% povidone iodine solution.13,14,16–20,22–29,31,32 Suggested duration of antiseptic instillation varied between 2 and 5 minutes.13,18,26,29,31 Three articles mentioned 0.05% aqueous chlorhexidine solution for patients with a history of iodine allergy or contact dermatitis.14,19,29
Eyelash Trimming
Three guidelines recommended against eyelash trimming.14,18,19 This topic was not mentioned in the other guidelines.
Antibiotics Drops Before the Surgery
While five guidelines recommended not to use topical antibiotics before the surgery on the operation day, this practice was not discussed in most guidelines (15/21).16,17,19,25,31 Due to the lack of evidence showing antibiotics could prevent postoperative endophthalmitis, only one article suggested this practice based on the opinion of surgeons.25
Intraoperative Antibiotics
Sixteen of 21 guidelines recommended the use of intracameral cefuroxime 1mg/0.1 mL.13–17,19–21,23,24,26,28–31,33 Two guidelines suggested the use of intracameral antibiotics, but the agent was not specified.25,27 Other intracameral antibiotics mentioned were moxifloxacin, cefazolin, and vancomycin. Additional subconjunctival antibiotics were endorsed by one guideline.22 Two guidelines did not comment on this issue.18,32 Although recommended, four articles suggest the routine use of intraoperative antibiotics should be preserved when the local rate of endophthalmitis is higher than the community or published study rate.15,16,24,32 One guideline also recommended commercially prepared antibiotics to reduce the risk from dilution error.28
Antibiotic Drops Immediately After the Surgery
Sixteen of 21 articles did not specify about this step in the surgery. Three guidelines recommended topical antibiotics at the end of the surgery.20,25,26 Topical fluoroquinolones were mentioned as the antibiotic of choice in 2 articles.20,26 In contrast, two articles recommended against this procedure.19,31
Eye Patching After the Surgery
One guideline recommended eye patching and one recommended against eye patching.23,32 The others 19 articles did not describe this procedure in the guidelines.
Antibiotics Drops After the Surgery
Seven guidelines recommended antibiotics drops for the post-operative period.17,18,20,22,24–26 One proposed the medication to be optional.32 Topical fluoroquinolones were endorsed by 2 articles,20,26 and a combination of topical antibiotics and steroids was endorsed by 1 article.18 Two guidelines were against this practice.19,30 Others (11/21) did not mention this practice.
Discussion
Common sources of infection in cataract surgery include ocular surface flora, periorbital skin infection, contaminated surgical instruments, surgical complications, and delayed wound healing.19 Surgeons and operative teams employ many protocols to ensure safety and to reduce these contaminants before, during, and after the surgery. This review systematically collected, appraised, and extracted data from clinical practice guidelines related to postoperative endophthalmitis prophylaxis from the past 15 years. Amongst 21 guidelines included in this article, two are from international organizations, and 19 are from local ophthalmology societies in Europe, Asia, and North America.
Many routine practices were not mentioned nor supported by clinical guidelines. Most documented guidelines did not mention the use of topical antibiotics before the day of the surgery. While topical antibiotics have been shown to reduce conjunctival bacterial flora, no evidence has been documented that it can reduce the risk of endophthalmitis.25 In our review, however, three articles suggested using topical antibiotics. There were studies reporting that a 3-day application of topical ofloxacin was more effective in reducing more bacterial load than 1-day or 1-hour applications. These differences were not found with topical moxifloxacin.34
Only 4 guidelines recommended pre-operative face washing but none of the remaining guidelines recommended against it. Although, we have found no study that supports any benefit from face washing, we also recommend this procedure since it is not only basic personal hygiene but is also cost-effective and has a very low risk of complications. We believe that face washing, make-up removal, and removal of artificial eyelashes should be a standard preoperative recommendation to reduce surgical field contamination.
Povidone-iodine skin preparation is used widely in every type of organ surgery. Povidone-iodine solution has a broad spectrum antiseptic property due to the release of free iodine that penetrates the microbial cell wall. Its antimicrobial activity is concentrated and contact-time dependent.35,36 Since the most common organism identified in acute post-cataract surgery endophthalmitis is coagulase-negative Staphylococcus which is a normal flora on human skin,19 it is reasonable to eliminate possible sources of infection as much as possible. Most guidelines recommended 5–10% povidone-iodine solution for periocular skin sterilization. A retrospective study found that 10% povidone-iodine skin preparation was more effective in reducing the incidence of post-extracapsular cataract extraction endophthalmitis than 5% povidone-iodine.35 Only a guideline by All India Ophthalmological Society specifically suggested an exposure time of 3 minutes of 5% povidone-iodine.32 Although there were no other studies that compared the duration of povidone-iodine skin preparation, there was a prospective trial that showed 3 minutes of 5% povidone-iodine applied to periocular skin, conjunctival sac, and cornea significantly reduced bacterial load on both eyelid and ocular surface.36 Another study reported no adverse sequelae in using 10% povidone-iodine for 3 minutes for periocular skin and ocular surface disinfection.37
Topical povidone iodine instilled in conjunctival cul-de-sac before cataract surgery is a standard practice as recommended by almost all guidelines. It is also the only clinical trial proven procedure that effectively reduces ocular surface bacterial load and the incidence of post-cataract surgery endophthalmitis.34,38 Almost all guidelines recommended this procedure as a part of infection prophylaxis. The most frequently suggested concentration is 5%, but there was one article in our review recommending a 5–10% concentration. As previously mentioned, no adverse effect was found with a 3-minute application of 10% povidone-iodine on the ocular surface.37 While no study compared the efficacy between durations of povidone-iodine exposure, one prospective study demonstrated that 30 seconds of contact time was adequate to reduce conjunctival bacterial counts before intravitreal injection.39 Moreover, another study found that conjunctival irrigation with 10 mL of 5% povidone-iodine achieved fewer positive conjunctival cultures compared with topical 5% povidone-iodine.40 Further research is needed to optimize povidone-iodine concentrations and contact durations, given that excessive toxicity to the ocular surface may theoretically heighten the risk of microbial penetration.
Eyelash trimming used to be a widely adopted procedure in many countries but this practice is now uncommon as it has not proven to be an effective method to impact periocular bacterial flora.41 Three guidelines in our review also recommended against this practice. It remains, however, crucial to exclude eyelashes from surgical areas to prevent contamination. Eyelid and eyelash scrubbing is a recommended treatment in patients with blepharitis.42 We propose that this procedure may help reduce the microbial load around the operative field. Further research on this topic would be beneficial.
Preoperative topical antibiotics at the time of surgery are commonly used worldwide to reduce conjunctival bacterial load. Although studies have shown that topical fluoroquinolones were able to reduce conjunctival sac bacterial loads, no studies have demonstrated their efficacy in reducing the postoperative endophthalmitis rate.38 Moreover, the relationship between reduced conjunctival bacterial loads and rates of endophthalmitis has also not been explored. In light of increasing antibiotic resistant bacteria, many guidelines have started to recommend against this practice. To reduce incidence of fluoroquinolone-resistant bacteria, one guideline recommended that topical moxifloxacin should be started 3 days prior to surgery.34
Intracameral cefuroxime is the only antibiotic route in cataract surgery that has been clinically proven to be effective in postoperative endophthalmitis prevention34 from the 2006 ESCRS study of prophylaxis of postoperative endophthalmitis after cataract surgery.43 The ESCRS study is the only multicenter randomized controlled trial that explored the efficacy of antibiotic prophylaxis in cataract surgery. This finding changed the practice of many surgeons worldwide and has led to recommendations from many guidelines included in this article. Unfortunately, there is no commercially intracameral preparation of cefuroxime available in many countries. This leads to surgeons’ concerns over bacterial contamination, dilution errors, and toxic anterior segment syndrome associated with the compound drug and makes this practice not widely used.34 Many recent retrospective studies and meta-analyses have demonstrated that intracameral non-preserved topical fluoroquinolones were equally or more effective than cefuroxime in reducing endophthalmitis prevalence and also equally safe.34,44 Although it is not commercially available in the US, the American Society of Cataract and Refractive Surgery (ASCRS) issued a clinical advisory on intracameral moxifloxacin in 2023. The recommended dosage was 0.5 mg, achievable by using either 0.1 mL of a 0.5% moxifloxacin solution or 0.5 mL of a 0.1% solution.45 Intracameral cefuroxime is also found to be cost-effective in postoperative endophthalmitis prevention.34
Postoperative topical antibiotics are used by nearly all surgeons worldwide. Two guidelines we reviewed recommended against the use of topical antibiotics immediately after the surgery and another two guidelines recommended against the prescription of topical antibiotics after cataract surgery. With the availability of fourth-generation fluoroquinolones, this recommendation might have changed. There are 2 retrospective studies that suggested the incidence of post-cataract surgery endophthalmitis was lower with topical fourth-generation fluoroquinolones prophylaxis compared with the third-generation fluoroquinolones.34 There is currently increasing popularity of the “dropless cataract surgery”. With the combination of intraocular sustained-release dexamethasone and intracameral antibiotics, this method eliminates the need for postoperative topical medication.46 This might lead to a paradigm shift in the use of postoperative topical antibiotics used in cataract surgery.
Eye protection after cataract surgery aims not only provides postoperative infection prophylaxis but also protects the eye from trauma, prevents diplopia, and reduces patients’ discomfort.47 Most guidelines did not comment on this issue, but Nepal guidelines recommended eye patching after cataract surgery, while India guidelines recommended against eye patching. There was no trial that supported the efficacy of endophthalmitis prevention by eye protection. One systematic review reported that patients experienced lower or equivalent rates of discomfort when using postoperative bandage contact lenses compared with eye shield, eye patch, and no eye protection.47 When performing bilateral cataract surgery, patients also preferred contact lens bandage or eye patch over no eye protection.47 Another randomized controlled trial found that eye patching is associated with increased corneal edema and slower visual recovery on the first postoperative day compared with an eye shield.48 We propose that decisions regarding postoperative eye protection should consider the vision in the patient’s fellow eye, the patient’s level of cooperation, and the environmental context.
To our knowledge, this is the first systematic review of clinical practice guidelines for post-cataract surgery endophthalmitis prophylaxis. This review includes all guidelines with no language restriction. We found that each country recommended distinct practices, reflecting variations in local regulations, resource availability, and epidemiological considerations. Developing a clinical practice guideline needs to consider all aspects including societal, environmental, and economical aspects of each country. Many differences in recommended protocols such as periorbital skin scrubbing, timing, and routes of antibiotic prophylaxis, creates to a gap of knowledge that could be closed with further research.
There are some limitations of this study. Firstly, despite conducting searches without language restriction and including gray literature sources, our reliance on structured databases and publicly accessible institutional websites may have introduced potential language bias, as some high-quality guidelines published exclusively in non-English local medical literature or not indexed in major databases may have been missed. This challenge is compounded by the fact that many guidelines are not publicly available online, and the authors were unable to establish personal contact with ophthalmologists in every country to obtain them. Consequently, the review may suffer from publication bias toward easily accessible guidelines. Secondly, many guidelines do not offer the evidence behind the recommendations eliminating the ability to perform a meta-analysis. Lastly, the definition on evidence grading and level of recommendation vary amongst each article. The level of recommendation behind each practice was not included in this study.
The substantial variation in prophylactic practices observed across the 21 guidelines reviewed highlights the need for a more universal and evidence-driven consensus. Persistent differences in recommended concentrations, contact times, and ancillary measures create a significant knowledge gap that requires further research. Future studies should prioritize multicenter randomized controlled trials comparing specific protocols to establish optimal, non-region-specific standards. Ultimately, the goal is to synthesize global evidence to create a set of universal prophylaxis recommendations adaptable to local factors like resource availability and antibiotic resistance patterns.
Conclusion
Practice recommendation varies among countries due to idiosyncratic circumstances, socio-economic backgrounds, postoperative endophthalmitis rates, resource availability, and expert opinions. Despite these variations, the most commonly endorsed measures included intracameral antibiotics, instillation of povidone-iodine into the conjunctival sac, and periorbital skin preparation with povidone-iodine. Given the devastating visual consequences of postoperative endophthalmitis and its considerable economic burden on both patients and healthcare systems, establishing efficient and cost-effective prophylactic protocols is critical. However, the absence of a universal consensus continues to limit standardization of care. A coordinated international effort that balances evidence-based medicine with economic feasibility and accessibility could help minimize disparities, reduce preventable blindness, and improve cost-effectiveness of cataract surgery worldwide. Surgeons must also carefully evaluate each patient and surgery and customize a combination of practices to prevent postoperative infection and its consequences.
Acknowledgments
The authors would like to thank the English editing service, Research Affairs, Faculty of Medicine, Chulalongkorn University for the language assessment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Quality Improvement Fund, King Chulalongkorn Memorial Hospital, the Thai Red Cross Society. The sponsor of this study was not involved in the study design, data collection, data analysis, interpretation of results, writing of the manuscript, or the decision to submit this article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harwood RH. Visual problems and falls. Age Ageing. 2001;30(Suppl 4):S13–S18. doi:10.1093/ageing/30.suppl_4.13
2. Organisation for Economic Co-operation and Development, World Health Organization. Measuring progress towards universal health coverage. Health at a Glance. 2022;7(1):66–67.
3. Cicinelli MV, Buchan JC, Nicholson M, et al. Cataracts. Lancet. 2023;401(10374):377–389. doi:10.1016/S0140-6736(22)01839-6
4. Leung EH, Gibbons A, Stout JT, et al. Intracameral moxifloxacin for endophthalmitis prophylaxis after cataract surgery: cost-effectiveness analysis. J Cataract Refract Surg. 2018;44(8):971–978. doi:10.1016/j.jcrs.2018.05.022
5. Kessel L, Flesner P, Andresen J, et al. Antibiotic prevention of postcataract endophthalmitis: a systematic review and meta-analysis. Acta Ophthalmol. 2015;93(4):303–317. doi:10.1111/aos.12684
6. Jabbarvand M, Hashemian H, Khodaparast M, et al. Endophthalmitis occurring after cataract surgery: outcomes of more than 480 000 cataract surgeries, epidemiologic features, and risk factors. Ophthalmology. 2016;123(2):295–301. doi:10.1016/j.ophtha.2015.08.023
7. Taban M, Behrens A, Newcomb RL, et al. Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol. 2005;123(5):613–620. doi:10.1001/archopht.123.5.613
8. Miller KM, Oetting TA, Tweeten JP. American academy of ophthalmology preferred practice pattern cataract/anterior segment panel. cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):1–26.
9. Endophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978–988. doi:10.1016/j.jcrs.2007.02.032
10. Garg P, Khor WB, Roy A. APAX consortium. A survey of Asian Eye Institutions on perioperative antibiotic prophylaxis in cataract surgery. Int Ophthalmol. 2023;43(11):4151–4162. doi:10.1007/s10792-023-02816-w
11. Brouwers MC, Kho ME, Browman GP. on behalf of the AGREE next steps consortium. AGREE II: advancing guideline development, reporting and evaluation in healthcare. Can Med Assoc J. 2010;182:E839–842. doi:10.1503/cmaj.090449
12. Johnston A, Kelly SE, Hsieh SC, et al. Systematic reviews of clinical practice guidelines: a methodological guide. J Clin Epidemiol. 2019;108:64–76. doi:10.1016/j.jclinepi.2018.11.030
13. Canadian Ophthalmological Society Cataract Surgery Clinical Practice Guideline Expert Committee. Canadian Ophthalmological Society evidence-based clinical practice guidelines for cataract surgery in the adult eye. Can J Ophthalmol. 2008;43(Suppl 1):S7–S57. doi:10.3129/i08-133
14. Ismail M, Livingstone BI, Muhammad HM, et al. Clinical Practice Guidelines Management of Post-Operative Infectious Endophthalmitis. Putrajaya: CPG Secretariat, Ministry of Health Malaysia; 2009.
15. Ndegwa S, Cimon K, Severn M. Intracameral antibiotics for the prevention of endophthalmitis post-cataract surgery: review of clinical and cost-effectiveness and guideline. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2010 (Rapid Response Report: Peer-Reviewed Summary with Critical Appraisal). Available from: http://www.cadth.ca/index.php/en/hta/reports-publications/search/publication/2683.
16. Smith R, Bishai K, Coronini-Cronberg S, et al. eds.. Commissioning Guide: Adult Cataract Surgery. London: Clinical Council for Eye Health Commissioning, The Royal College of Ophthalmologists; 2010.
17. Cochereau I, Korobelnik JF, Robert PY, Hajjar J. French agency for the safety of health products. antibioprophylaxie en chirurgie ophtalmologique. À propos des recommandations de l’AFSSAPS. J Fr Ophtalmol. 2011;34(6):428–430. doi:10.1016/j.jfo.2011.05.002
18. Deshpande M, editor. Guidelines for the Management of Cataract in India. New Delhi: Sightsavers; 2011.
19. Barry P, Cordovés L, Gardner S. ESCRS Guidelines for Prevention and Treatment of Endophthalmitis Following Cataract Surgery: Data, Dilemmas and Conclusions. Dublin: The European Society for Cataract & Refractive Surgeons; 2013.
20. Prevenzione dell’endoftalmite postoperatoria [homepage on the Internet]. Rome: Società Oftalmologica Italina; 2013. Available from: https://www.sedesoi.com/.
21. Antibiotic prophylaxis in surgery (SIGN publication No.104) [homepage on the Internet]. Edinburgh: Scottish Intercollegiate Guidelines Network (SIGN); 2008. Available from: http://www.sign.ac.uk.
22. Rajavi Z, Javadi MA, Daftarian N, et al. Customized clinical practice guidelines for management of adult cataract in Iran. J Ophthalmic Vis Res. 2015;10(4):445–460. doi:10.4103/2008-322X.176913
23. Cataract surgery protocol [homepage on the internet]. nepal: international agency for prevention of blindness and apex body for eye health, Nepal Ophthalmic Society; 2015. Available from: https://nos.com.np/s/protocol/.
24. Adapted evidence-based guidelines: cataract [homepage on the Internet]. Ukraine: State Expert Center,Ministry of Health; 2015. Available from https://www.dec.gov.ua/.
25. Linee Guida Clinico Organizzative Sulla Chirurgia Della Cataratta [homepage on the Internet. Rome: Società Oftalmologica Italina; 2016. Available from: https://www.sedesoi.com/.
26. Principles of preferred practice in cataract surgery [homepage on the Internet. Singapore: Asia-Pacific Association of Cataract & Refractive Surgeons Secretariat; 2017. Available from: https://apacrs.org/.
27. Committee on Standards, Philippine Academy of Ophthalomology. Clinical practice guidelines: management of cataract among adults. Philipp J Ophthalmol. 2017;1(Suppl):S9–S28.
28. National Institute for Health and Care Excellence. Cataract in Adults: Management (NICE Guideline NG77). London: National Institute for Health and Care Excellence (NICE); 2017.
29. Kaihi (aikuiset). homepage on the Internet]. Helsinki: Finnish Medical Society Duodecim; 2019. Available from: https://www.kaypahoito.fi/hoi50035.
30. National clinical guideline for treatment of age-related cataract [homepage on the Internet. Copenhagen: Danish Health Authority, Ministry of Health; 2020. Available from: https://www.sst.dk/.
31. American Academy of Ophthalmology Preferred Practice Pattern Cataract/Anterior Segment Panel. Cataract in the adult eye preferred practice pattern. Ophthalmology. 2022;129(1):1–126.
32. Verma L, Agarwal A, Dave VP, et al. All India Ophthalmological Society (AIOS) task force guidelines to prevent intraocular infections and cluster outbreaks after cataract surgery. Indian J Ophthalmol. 2022;70(2):362–368. doi:10.4103/ijo.IJO_94_22
33. Intraoperative antimicrobial prophylaxis in elective cataract surgery patients with penicillin allergy [homepage on the Internet]. London: The Royal College of Ophthalmologists; 2022. Available from: https://www.rcophth.ac.uk/.
34. Vazirani J, Basu S. Role of topical, subconjunctival, intracameral, and irrigative antibiotics in cataract surgery. Curr Opin Ophthalmol. 2013;24(1):60–65. doi:10.1097/ICU.0b013e32835a93be
35. Wu PC, Li M, Chang SJ, et al. Risk of endophthalmitis after cataract surgery using different protocols for povidone-iodine preoperative disinfection. J Ocul Pharmacol Ther. 2006;22(1):54–61. doi:10.1089/jop.2006.22.54
36. Zia IC, Mackie G, Gallacher G, et al. The efficacy of 5% povidone-iodine for 3 minutes prior to cataract surgery. Eur J Ophthalmol. 2009;19(4):560–564. doi:10.1177/112067210901900407
37. Nguyen CL, Oh LJ, Wong E, et al. Povidone-iodine 3-minute exposure time is viable in preparation for cataract surgery. Eur J Ophthalmol. 2017;27(5):573–576. doi:10.5301/ejo.5000964
38. Soleimani M, Haydar AA, Cheraqpour K, et al. In praise of povidone-iodine application in ophthalmology. Surv Ophthalmol. 2024;69(2):211–223. doi:10.1016/j.survophthal.2023.11.002
39. Friedman DA, Mason JO, Emond T, et al. Povidone-iodine contact time and lid speculum use during intravitreal injection. Retina. 2013;33(5):975–981. doi:10.1097/IAE.0b013e3182877585
40. De Kaspar HM, Chang RT, Singh K, et al. Prospective randomized comparison of 2 different methods of 5% povidone-iodine applications for anterior segment intraocular surgery. Arch Ophthalmol. 2005;123(2):161–165. doi:10.1001/archopht.123.2.161
41. Perry LD, Skaggs C. Preoperative topical antibiotics and lash trimming in cataract surgery. Ophthalmic Surg. 1977;8(5):44–48.
42. Rocha KM, Farid M, Raju L. the ASCRS cornea clinical committee. eyelid margin disease (blepharitis and meibomian gland dysfunction): clinical review of evidence-based and emerging treatments. J Cataract Refract Surg. 2024;50(8):876–882. doi:10.1097/j.jcrs.0000000000001414
43. Barry P, Seal DV, Gettinby G. the ESCRS Endophthalmitis Study Group. ESCRS study of prophylaxis of postoperative endophthalmitis after cataract surgery: preliminary report of principal results from a European multicenter study. J Cataract Refract Surg. 2006;32(3):407–410. doi:10.1016/j.jcrs.2006.02.021
44. Bowen RC, Zhou AX, Bondalapati S, et al. Comparative analysis of the safety and efficacy of intracameral cefuroxime, moxifloxacin and vancomycin at the end of cataract surgery: a meta-analysis. Br J Ophthalmol. 2018;102(9):1268–1276. doi:10.1136/bjophthalmol-2017-311051
45. Myer WG, Chang DF, Shorstein NH, Mah FS, Mamalis N, Miller KM. the ASCRS cataract clinical committee. ASCRS clinical advisory on intracameral moxifloxacin injection for infection prophylaxis. J Cataract Refract Surg. 2023;49(10):1068–1070. doi:10.1097/j.jcrs.0000000000001237
46. Assil KK, Greenwood MD, Gibson A, et al. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction. Curr Opin Ophthalmol. 2021;32(Suppl 1):S1–S12. doi:10.1097/ICU.0000000000000708
47. Dhoot AS, Popovic MM, Lee S, et al. Eye protection following cataract surgery: a systematic review. Can J Ophthalmol. 2023;58(3):179–186. doi:10.1016/j.jcjo.2021.11.001
48. Gazit I, Dubinsky-Pertzov B, Or L, et al. Eye patching after cataract surgery is associated with an increased risk of short-term corneal oedema. Acta Ophthalmol. 2021;99(1):e81–e85. doi:10.1111/aos.14510
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.