Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Systematic review of catatonia treatment
Authors Pelzer ACM, van der Heijden FMMA, den Boer E
Received 1 August 2017
Accepted for publication 30 October 2017
Published 17 January 2018 Volume 2018:14 Pages 317—326
DOI https://doi.org/10.2147/NDT.S147897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Anne CM Pelzer,1 Frank MMA van der Heijden,2 Erik den Boer3
1Department of Psychiatry, Reinier van Arkel, ‘s-Hertogenbosch, 2Department of Psychiatry, Vincent van Gogh Institute for Psychiatry, Venlo, 3Department of Psychiatry, GGzE, Eindhoven, the Netherlands
Objective: To investigate the evidence-based treatment of catatonia in adults. The secondary aim is to develop a treatment protocol.
Materials and methods: A systematic review of published treatment articles (case series, cohort or randomized controlled studies) which examined the effects of particular interventions for catatonia and/or catatonic symptoms in adult populations and used valid outcome measures was performed. The articles for this review were selected by searching the electronic databases of the Cochrane Library, MEDLINE, EMBASE and PSYCHINFO.
Results: Thirty-one articles met the inclusion criteria. Lorazepam and electroconvulsive therapy (ECT) proved to be the most investigated treatment interventions. The response percentages in Western studies varied between 66% and 100% for studies with lorazepam, while in Asian and Indian studies, they were 0% and 100%. For ECT, the response percentages are 59%–100%. There does not seem to be evidence for the use of antipsychotics in catatonic patients without any underlying psychotic disorder.
Conclusion: Lorazepam and ECT are effective treatments for which clinical evidence is found in the literature. It is not possible to develop a treatment protocol because the evidence for catatonia management on the basis of the articles reviewed is limited. Stringent treatment studies on catatonia are warranted.
Keywords: review, catatonia, therapeutics, electroconvulsive therapy, benzodiazepines, lorazepam, ECT
Introduction
Catatonia is a neuropsychiatric syndrome that was originally described by Karl Kahlbaum in 1874, and hence, Kraepelin considered catatonia as a subtype of dementia praecox.1,2 This conceptualization continued to exist for many years and, consequently, catatonia was classified as a subtype of schizophrenia up to and including Diagnostic and Statistical Manual of Mental Disorders (DSM)-III-R.48 Over time, this classification greatly affected recognition and treatment; however, from the late 70s, it became increasingly evident that catatonia is a condition that is associated with a variety of metabolic, neurologic, psychiatric and toxic conditions.3–5 DSM-IV, therefore, mentioned three entities of catatonia: as a subtype of schizophrenia, as a specification of affective disorders, and due to a medical condition.6 To emphasize the importance of recognizing catatonia, its classification in DSM-5 was altered.7 One of the new features of DSM-5 was the inclusion of catatonia under a separate heading in the chapter on Schizophrenia Spectrum and Other Psychotic Disorders.8 Catatonia appears in three forms in DSM-5: “catatonia associated with another mental disorder”, “catatonic disorder due to another medical condition” and “unspecified catatonia”.9
The pathophysiology and etiology of catatonia remains unclear. One of the hypotheses is that it may be explained by an alteration of the dopaminergic function.10,11 In addition, dysfunction of gamma-aminobutyric acid and glutamate systems may be implicated.12 Benzodiazepines and electroconvulsive therapy (ECT) are the most widely studied treatment methods. However, no uniform treatment method has yet been brought forward. To compare the differences in effects between medication, ECT and placebo, and to develop uniform advice, a Cochrane review was performed based on randomized controlled studies (RCTs). However, the conclusion was that none of the studies could be included in this review.13 A controlled study on the treatment of (chronic) catatonia in people with schizophrenia showed that benzodiazepines have no added value compared to placebo.14 Until now, no broadly accepted treatment guidelines have been described for catatonia. The purpose of this review of the literature is to establish the evidence-based treatment for catatonia in adults. The secondary aim is to develop a treatment protocol based on the available evidence.
Materials and methods
The study design was based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) method.15 We searched the databases of the Cochrane Library, MEDLINE, EMBASE and PSYCHINFO in July 2016 using catatonia (and related terms) AND treatment (and related terms) as keywords. We deliberately chose the general term treatment to obtain the broadest possible spectrum of treatment interventions. The main prerequisites were that the articles had been published in either English or Dutch language and that abstracts were available. Articles were selected for inclusion by two authors independent of each other on the basis of predefined inclusion criteria. Treatment manuscripts (irrespective of design) that investigated the effects of particular interventions on catatonia and/or catatonic symptoms in adult populations were included. Case series were included when at least three cases were described. A report was included if response to treatment was measured using a standardized rating instrument or scale. Consequently, all the included full-text articles were analyzed. The results of the included articles are presented in Tables 1–3.
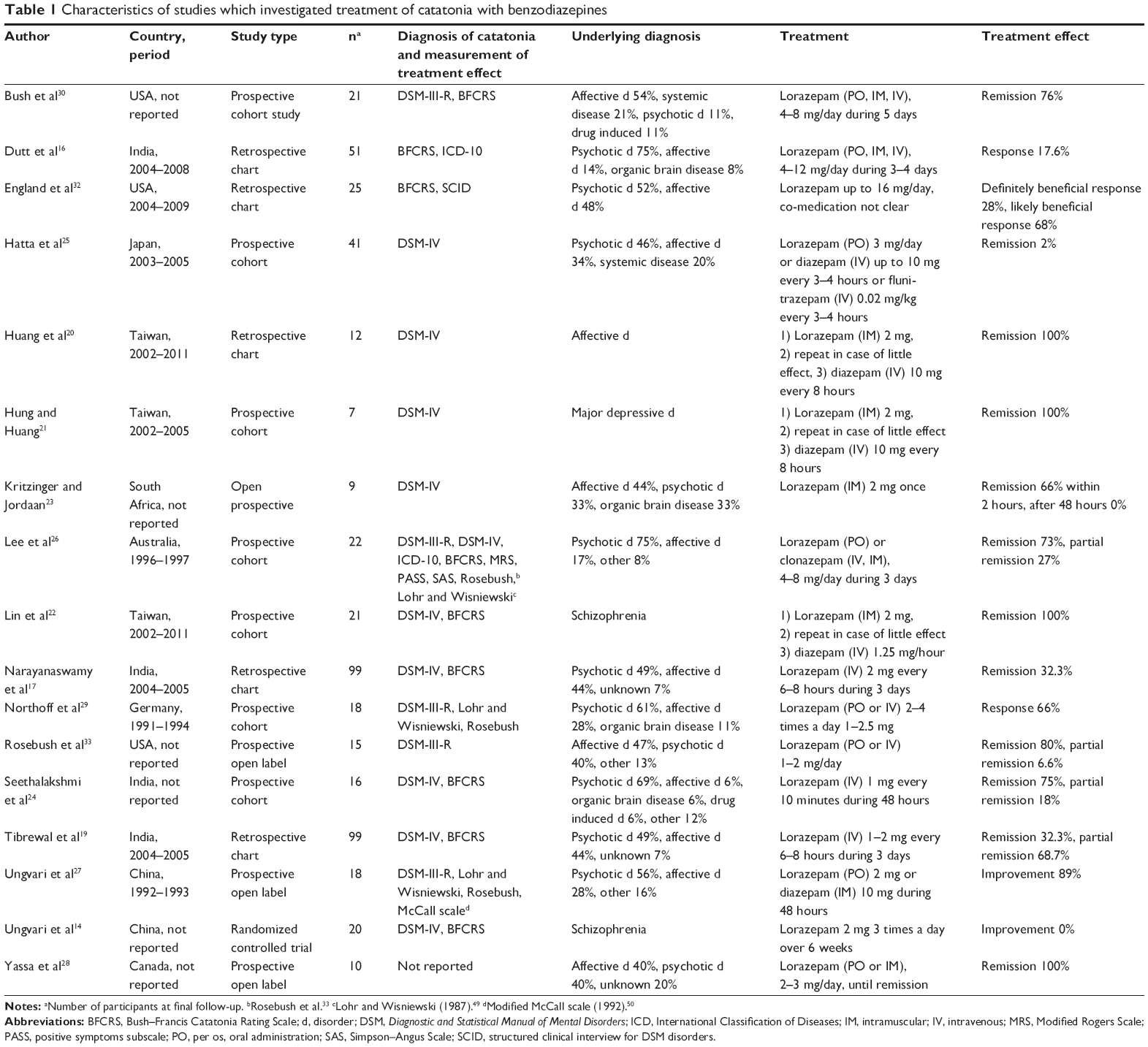 | Table 1 Characteristics of studies which investigated treatment of catatonia with benzodiazepines |
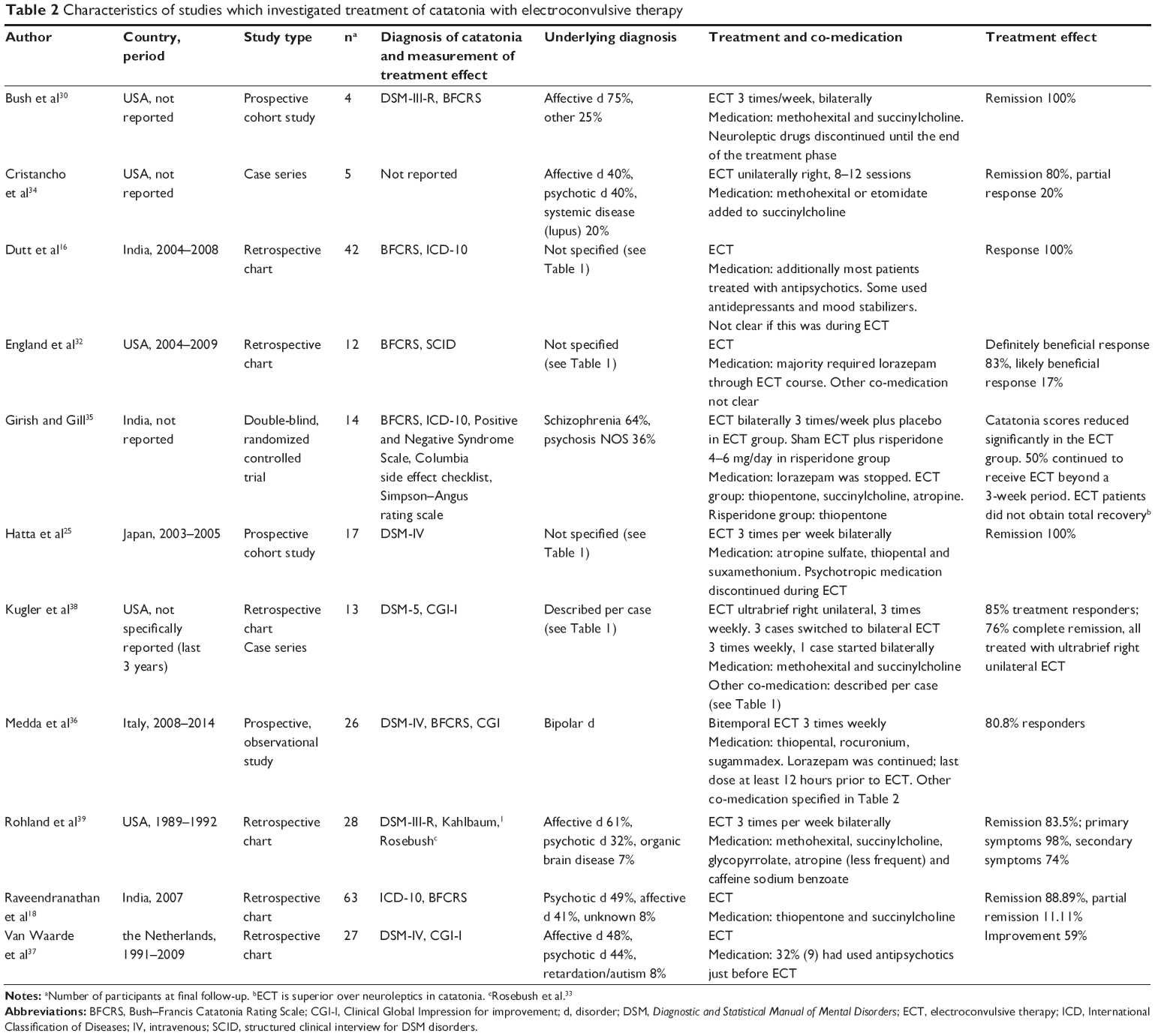 | Table 2 Characteristics of studies which investigated treatment of catatonia with electroconvulsive therapy |
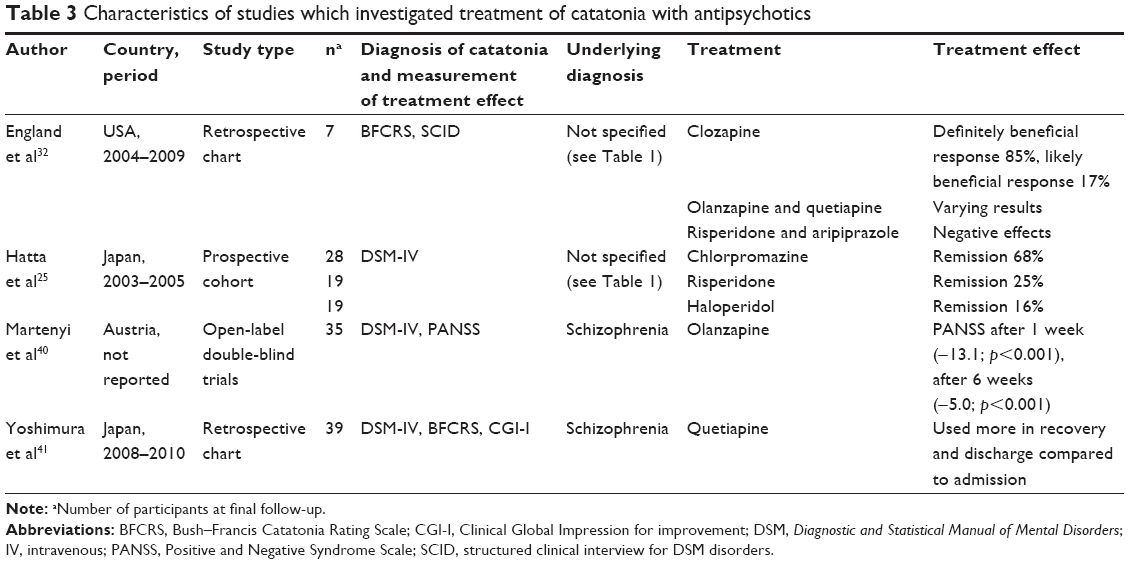 | Table 3 Characteristics of studies which investigated treatment of catatonia with antipsychotics |
Results
Identification
Our search strategy using Ovid database revealed 3,079 potentially relevant manuscripts in the Cochrane Library, MEDLINE, EMBASE and PSYCHINFO. Figure 1 describes the evaluation of these 3,079 publications.
 | Figure 1 Search and selection strategy. Flow diagram for included studies. |
Systematic review results
In total, 31 articles met the inclusion criteria for systematic review. Most of these manuscripts were small scale and four investigations involved cohorts of over 50 people.16–19
Benzodiazepines
Treatment with benzodiazepines is the most extensively studied treatment method and is reported in 17 studies, of which the study characteristics are described in Table 1. Lorazepam is the most widely studied medication, which is administered in doses varying from 2 to 16 mg/day. Three studies investigated a lorazepam/diazepam protocol, with variable results.20–22 The manner of administration is mainly oral (PO). If PO administration is not possible because of the patient’s mental health state, parenteral methods (intramuscular [IM] or intravenous [IV]) are used. Four studies primarily opted for such a parenteral method.17,19,23,24 The reason for doing so was not mentioned. In most studies, lorazepam is administered PO as well IM and IV. Some studies chose diazepam, flunitrazepam or clonazepam as IM or IV therapy.25–27 Duration of therapy varies from the administration of just one dose to continued administration for as long as catatonic symptoms persist. Two studies27,28 explicitly describe that the effect of lorazepam wears off after 3–5 hours and that the symptoms subsequently return.
The average percentage, represented in terms of response and remission (Table 1), reported in Western studies varies between 66% and 100%.28,29 Asian studies report percentages between 0% and 100%.14,20 The percentages in India lie between 17% and 100% (full remission plus partial remission).16,19 The lowest percentages are reported in non-Western studies. If patients respond to benzodiazepines, the effect is usually visible within a few days.26,28,30 This effect can be evaluated by using the Bush–Francis Catatonia Rating Scale.26,31 Studies in which the patients displayed long-term symptomatology prior to treatment reported lower response and/or remission percentages.14,16,17,19,25 Overall, benzodiazepines seem to be well tolerated. It was observed that a high dose of lorazepam (16 mg/day) was tolerated without sedation.32 Five of the 17 studies actively reported no adverse effects.14,21,23,27,32 Only Rosebush et al reported one patient in whom marked agitation was seen after lorazepam treatment.33
Electroconvulsive therapy
Eleven studies described the effects of ECT as a treatment method for catatonia. The characteristics of these studies are described in Table 2. In six studies, ECT was administered as a secondary therapy when there was no or insufficient response to benzodiazepines.16,30,32,34–36 ECT was not only initiated after ineffective pharmacotherapy, but also as primary therapy, for example, in life-threatening situations.18,25,37–39 The reported bilateral ECT frequency was three times a week on average.25,30,35,36,38,39 In two studies, ECT was administered unilaterally, the hypothesis being that this would reduce the risk of cognitive side effects.34,38 Because of the small cohort involved in both studies, this hypothesis could not be confirmed. The total number of ECT sessions in the included studies varied from two to 13.
The percentages, represented in terms of response and remission (Table 2), ranged from 59% to 100%.16,37 Most articles were based on chart reviews and case studies and, consequently, lacked any form of randomization, control group, uniform treatment and crucial information on medication or co-medication. Of the 11 studies which investiged ECT, six studies actively reported about side effects. Cristancho et al34 describe that all patients tolerated ECT well without major adverse effects or cognitive impairment. However, in other studies, patients treated with ECT were observed to have cognitive/memory impairment or complained of headache during treatment.32,35,36 The risk of cognitive adverse effects may be related to higher ECT frequency and must be balanced against the risk of morbidity and mortality due to catatonia.37
Antipsychotics
Four studies (Table 3) examined the role of antipsychotics in treating catatonia. It should be noted that the examined cohorts largely consisted of patients with an underlying psychotic disorder. England et al concluded that clozapine has a beneficial effect on catatonic symptoms.32 On the other hand, classic antipsychotics may result in clinical deterioration and appear to be associated with the development of lethal catatonia or malignant neuroleptic syndrome. Hatta et al observed that patients responded better to an antipsychotic drug with low affinity for dopamine receptors (clozapine) than to an antipsychotic drug with high affinity (haloperidol).25 The main disadvantage of this study is that the effect cannot be attributed to any of the used antipsychotics due to the use of co-medication.
Treatment with olanzapine demonstrated mixed results.32 It was concluded that treatment with olanzapine decreased symptoms measured by the Positive and Negative Syndrome Scale score. However, another study did not include the use of an instrument for measuring catatonia, so no specific effect could be attributed to this treatment.40 Yoshimura et al observed that quetiapine was more significantly used around the time of recovery and discharge, compared to other antipsychotics.41 However, after 30 months, in most patients, this antipsychotic drug had been replaced with another due to lack of effect. Here too, the effect of co-medication is not entirely clear. Adverse effects such as worsening of catatonic symptoms, increasing confusion, agitation and restlessness in patients treated with typical antipsychotics have been mentioned.32 Others reported that tremor and rigidity occurred in most of the cases.25 Yoshimura et al observed that three patients on first-generation antipsychotics and risperidone developed a neuroleptic malignant syndrome.41
Other treatment methods
The use of carbamazepine in the acute phase of catatonia was examined in an open prospective study involving nine patients.23 Carbamazepine was administered when patients did not sufficiently respond to lorazepam. This study revealed that lorazepam initially produces good results, but its effect wears off after a few hours. Eventually, all patients were given carbamazepine, whereupon four patients recovered and one patient showed partial recovery. It should be noted that this study involved a small study group without adequate information about co-medication.
Packing therapy involves wrapping the catatonic patient in cold wet towels in order to reinforce, inter alia, sensory integration. The researchers concluded that it could be used as a co-intervention, but not as primary treatment.42
McDaniel et al described the effect of topiramate on catatonic symptoms in four cases unresponsive to benzodiazepines and antipsychotics.43 After treatment with topiramate, the patients showed recovery or improvement, but it is not clear whether this improvement was the result of the use of topiramate.
The effect of amineptine in patients with schizophrenia and chronic catatonia was examined in an RCT conducted by Ungvari. The author concluded that amineptine has no effect on catatonic symptomatology.44
Therapeutic efficiacy of the N-methyl-D-aspartate (NMDA) antagonist amantadine has been reported by Northoff et al45 and Freitas de Lucena et al.46 Northoff et al reported three cases with acute akinetic catatonia, in which IV infusion of 500 mg amantadine (if necessary, repeated after 24 hours) led to resolution of catatonic symptoms. Considerable reduction of scores in various motor scales was seen with most pronounced effects 4–6 hours after administration. Patients were not taking antipsychotic or any other psychotropic drugs. It should be mentioned that amantadine might exacerbate psychotic symptoms. Therefore, Northoff et al excluded cases of paranoid schizophrenia. Freitas de Lucena et al evaluated the use of amantadine for 4 weeks in five cases of acute catatonia in schizophrenia of schizoaffective disorder. Doses were increased up to 600 mg/day over a period of 4 weeks. Patients were medication free for at least 72 hours. Antipsychotic medication was reintroduced in the third week. In all five patients, amantadine led to considerable reduction in catatonic symptoms. The best response was observed between 10 and 21 days.
Discussion
There are currently no broadly accepted guidelines for the treatment of catatonia. The articles included in our review all have a level of evidence not exceeding 1b (individual RCT), of which most do not exceed 2b (individual cohort study).47 In addition, the diversity of methods and outcome measures used makes unambiguous interpretation of these studies impossible, and therefore, it was not feasible to develop an evidence-based treatment protocol. However, the investigated articles clearly show similarities in terms of design and results, which may prove useful in clinical practice and are a starting point for further research.
The response rate to benzodiazepines in Western studies lies between 66% and 100%.26–28,30,33 Non-Western studies reported the lowest response rates. A possible explanation for this is that these studies involved chronic, untreated catatonia.14,16,17 In addition, response seems to depend on dosage and frequency of administration. Studies which involved doses of 2–2.5 mg and more frequent administration (several times a day) showed higher response and remission.20–22,26,28–30 No evident side effects have been described for these dosages. The maximum daily dose used was 12–16 mg.16,32 As benzodiazepines can easily be administered in various settings, they are the therapy of first choice. Lorazepam is the most widely studied compound within this treatment framework. Some studies also examined the effect of diazepam,20–22 but there are no studies that explicitly measured the differences in effects between different types of benzodiazepines. The studies also varied in terms of manner of administration (PO, IM or IV). There are no indications that there is any preference based on efficacy in this respect. How long therapy should be continued was not really examined. There are, though, indications that prolonged treatment is required to obtain a lasting effect.23,27,28 When treatment with lorazepam proves beneficial, this effect is noticeable within several hours to a few days.19–22,24,27,28,30,33 No maximum term for treatment with lorazepam was mentioned, but if it does not entirely produce the desired effect within 4–5 days, it is recommended to consider ECT.16,30 ECT appeared to be a very effective treatment for patients who do not respond to benzodiazepines.16,18,25,30,32,34,36
In severe catatonia involving potentially life-threatening situations such as severe dehydration, autonomic dysregulation, thrombosis or decubitus, ECT may be a good alternative to pharmacotherapy. If treatment with lorazepam is nonetheless the preferred option, it is recommended to provide this therapy in this category of patients at a psychiatric department of a general hospital where the patient’s condition can be better monitored and appropriate measures can be taken (infusion, heparin). Chronic catatonic symptoms constitute another possible reason for opting for ECT in an earlier phase. Various studies described chronic catatonia as a significant patient characteristic of nonresponders to lorazepam.14,17,19 A possible explanation for this is that acute and chronic catatonia have different neurobiologic bases.14 There is no specific cut-off value between acute and chronic catatonia, but generally chronic catatonic symptoms are described as lasting for at least tens of days.17,19
ECT is a very effective therapy for catatonia, also when benzodiazepine (lorazepam) trials have failed.16,18,25,30,35,36 The response percentages vary between 59% and 100%.18,25,30,34,39 The reason why this therapy is a secondary treatment option (in most cases) is that ECT cannot be administered in all settings and because of the potential side effects.
The role of antipsychotics in treating catatonia is not entirely clear. They do seem to be an appropriate therapy when a psychotic disorder is considered to be the underlying cause of catatonia. In these cases, the results of the articles suggest to select an atypical instead of a typical antipsychotic to avoid the risk of deterioration of catatonic symptoms and induction of extrapyramidal movement disorders.
There is insuffient evidence to confirm the therapeutic effects of carbamazepine, topiramate and amineptine. Studies about NMDA antagonists do stress the importance of the potential involvement of glutamatergic dysfunction. However, double-blind control trials are needed to elaborate further on this hypothesis.
Conclusion
In summary, the results clearly showed that benzodiazepines and ECT are the only treatments for which there is clinical evidence. Identifying and treating the underlying disorder is essential in the treatment of catatonia. Moreover, the role of antipsychotics is not yet entirely clear. However, there does not seem to be evidence for the use of antipsychotics as therapy for catatonic patients without any underlying psychotic disorder. Typical antipsychotics can worsen the clinical picture. On the basis of the investigated articles, we were not able to develop a treatment protocol because the evidence for catatonia management is limited. Therefore, an urgent need is warranted for more stringent intervention studies in people with catatonia.
Acknowledgments
The authors thank Gertie van Bergen and Christien Geelen for their secretarial support and Sanne Rasing for her support in designing the review.
Disclosure
In the past, Frank MMA van der Heijden has received some personal fees from Lundbeck, Takeda, Servier and Janssen-Cilag (participation in advisory board and speaker fees). The authors report no other conflicts of interest in this work.
References
Kahlbaum K. Die Katatonie oder das Spannungsirresein. [Catatonia]. Berlin: August Hirschwald; 1874. German. | ||
Kraepelin E. Dementia Preacox and Paraphrenia (RM Barclay, Vert.). Huntington, NY: R.E. Krieger; 1919. | ||
Van der Heijden FM, Tuinier S, Arts NJ, Hoogendoorn ML, Kahn RS, Verhoeven WM. Catatonia: disappeared or under-diagnosed? Psychopathology. 2005;38(1):3–8. | ||
Fink M, Taylor MA. Catatonia: A Clinician’s Guide to Diagnosis and Treatment. Cambridge: Cambridge University Press; 2003. | ||
Caroff S, Mann S, Francis A, Fricchione G. Catatonia: From Psychopathology to Neurobiology. Washington, DC: American Psychiatric Publishing; 2004. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. 4th ed. Washington, DC: American Psychiatric Publishing; 1994. | ||
Tandon R, Heckers S, Bustillo J, et al. 2013. Catatonia in DSM-5. Schizophr Res. 2013;150(1):26–30. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Publishing; 2013. | ||
Ungvari GS. Catatonia in DSM-5: controversies regarding its psychopathology, clinical presentation and treatment response. Neuropsychopharmacol Hung. 2014;16(4):189–194. | ||
Northoff G, Demisch L, Wenke J, Pflug B. Plasma homovanillic acid concentrations in catatonia. Biol Psychiatry. 1996;39(6):436–443. | ||
Yamamura S, Ohoyama K, Hamaguchi T, et al. Effects of quetiapine on monoamine, GABA, and glutamate release in rat prefrontal cortex. Psychopharmacology (Berl). 2009;206(2):243–258. | ||
Unal A, Bulbul F, Alpak G, Virit O, Copoglu US, Savas HA. Effective treatment of catatonia by combination of benzodiazepine and electroconvulsive therapy. J ECT. 2013;29(3):206–209. | ||
Gibson R, Walcott G. Benzodiazepines for catatonia in people with schizophrenia and other serious mental illnesses. Cochrane Database Syst Rev. 2008;4:CD006570. | ||
Ungvari GS, Chiu HF, Chow LY, Lau BS, Tang WK. Lorazepam for chronic catatonia: a randomized, double-blind, placebo-controlled cross-over study. Psychopharmacology (Berl). 1999;142(4):393–398. | ||
Liberati ADGA, Tetzlaff J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. | ||
Dutt A, Grover S, Chakrabarti S, Avasthi A, Kumar S. Phenomenology and treatment of Catatonia: a descriptive study from north India. Indian J Psychiatry. 2011;53(1):36–40. | ||
Narayanaswamy JC, Tibrewal P, Zutshi A, Srinivasaraju R, Math SB. Clinical predictors of response to treatment in catatonia. Gen Hosp Psychiatry. 2012;34(3):312–316. | ||
Raveendranathan D, Narayanaswamy JC, Reddi SV. Response rate of catatonia to electroconvulsive therapy and its clinical correlates. Eur Arch Psychiatry Clin Neurosci. 2012;262(5):425–430. | ||
Tibrewal P, Narayanaswamy J, Zutshi A, Srinivasaraju R, Bada Math S. Response rate of lorazepam in catatonia: a developing country’s perspective. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(8):1520–1522. | ||
Huang YC, Lin CC, Hung YY, Huang TL. Rapid relief of catatonia in mood disorder by lorazepam and diazepam. Biomed J. 2013;36(1):35–39. | ||
Hung YY, Huang TL. Lorazepam and diazepam rapidly relieve catatonic features in major depression. Clin Neuropharmacol. 2006;29(3):144–147. | ||
Lin CC, Huang TL. Lorazepam-diazepam protocol for catatonia in schizophrenia: a 21-case analysis. Compr Psychiatry. 2013;54(8):1210–1214. | ||
Kritzinger PR, Jordaan GP. Catatonia: an open prospective series with carbamazepine. Int J Neuropsychopharmacol. 2001;4(3):251–257. | ||
Seethalakshmi R, Dhavale S, Suggu K, Dewan M. Catatonic syndrome: importance of detection and treatment with lorazepam. Ann Clin Psychiatry. 2008;20(1):5–8. | ||
Hatta K, Miyakawa K, Ota T, Usui C, Nakamura H, Arai H. Maximal response to electroconvulsive therapy for the treatment of catatonic symptoms. J ECT. 2007;23(4):233–235. | ||
Lee JW, Schwartz DL, Hallmayer J. Catatonia in a psychiatric intensive care facility: incidence response to benzodiazepines. Ann Clin Psychiatry. 2000;12(2):89–96. | ||
Ungvari GS, Leung CM, Wong MK, Lau J. Benzodiazepines in the treatment of catatonic syndrome. Acta Psychiatr Scand. 1994;89(4):285–288. | ||
Yassa R, Iskandar H, Lalinec M, Cleto L. Lorazepam as an adjunct in the treatment of catatonic states: an open clinical trial. J Clin Psychopharmacol. 1990;10(1):66–68. | ||
Northoff G, Wenke J, Demisch L, Eckert J, Gille B, Pflug B. Catatonia: short-term response to lorazepam and dopaminergic metabolism. Psychopharmacology (Berl). 1995;122(2):182–186. | ||
Bush G, Fink M, Petrides G, Dowling F, Francis A. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137–143. | ||
Bush G, Fink M, Petrides G, Dowling F, Francis A. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129–136. | ||
England ML, Ongür D, Konopaske GT, Karmacharya R. Catatonia in psychotic patients: clinical features and treatment responses. J Neuropsychiatry Clin Neurosci. 2011;23(2):223–226. | ||
Rosebush PI, Hildebrand AM, Furlong BG, Mazurek MF. Catatonic syndrome in a general psychiatric inpatient population: frequency, clinical presentation, and response to lorazepam. J Clin Psychiatry. 1990;51(9):357–362. | ||
Cristancho P, Jewkes D, Mon T, Conway C. Successful use of right unilateral ECT forcatatonia: a case series. J ECT. 2014;30(1):69–72. | ||
Girish K, Gill N. Electroconvulsive therapy in lorazepam non-responsive catatonia. Indian J Psychiatry. 2003;45(1):21–25. | ||
Medda P, Toni C, Luchini F, Giorgi Mariani M, Mauri M, Perugi G. Catatonia in 26 patients with bipolar disorder: clinical features and response to electroconvulsive therapy. Bipolar Disord. 2015;17(8):892–901. | ||
Van Waarde JA, Tuerlings JH, Verwey B, van der Mast RC. Electroconvulsive therapy for catatonia: treatment characteristics and outcomes in 27 patients. J ECT. 2010;26(4):248–252. | ||
Kugler J, Hauptman A, Collier S, et al. Treatment of catatonia with ultrabrief right unilateral electroconvulsive therapy: a case series. J ECT. 2015;31(3):192–196. | ||
Rohland BM, Carroll BT, Jacoby RG. ECT in the treatment of the catatonic syndrome. J Affect Disord. 1993;29(4):255–261. | ||
Martenyi F, Metcalfe S, Schausberger B, Dossenbach MR. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62 (Suppl 2):25–27. | ||
Yoshimura B, Hirota T, Takaki M, Kishi Y. Is quetiapine suitable for treatment of acute schizophrenia with catatonic stupor? A case series of 39 patients. Neuropsychiatr Dis Treat. 2013;9:1565–1571. | ||
Cohen D, Nicoulaud L, Maturana A, et al. Investigating the use of packing therapy in adolescents with catatonia: a retrospective study. Clin Neuropsychiatry. 2009;6(1):29–34. | ||
McDaniel WW, Spiegel DR, Sahota AK. Topiramate effect in catatonia: a case series. J Neuropsychiatry Clin Neurosci. 2006;18(2):234–238. | ||
Ungvari GS. Amineptine treatment of persistent catatonic symptoms in schizophrenia: a controlled study. Neuropsychopharmacol Hung. 2010;12(4):463–467. | ||
Northoff G, Eckert J, Fritze J. Glutamatergic dysfunction in catatonia? Successful treatment of three acute akinetic catatonic patients with the NMDA antagonist amantadine. J Neurol Neurosurg Psychiatry. 1997;62(4):404–406. | ||
de Lucena DF, Pinto JP, Hallak JE, Crippa JA, Gama CS. Short-term treatment of catatonia with amantadine in schizophrenia and schizoaffective disorder. J Clin Psychopharmacol. 2012;32(4):569–572. | ||
CEBM. Oxford Centre for Evidence-based Medicine – Levels of Evidence; 2009. Available from: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/. Accessed July 3, 2017. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-III-R. 3th ed. Washington, DC: American Psychiatric Publishing; 1988. | ||
Lohr JB, Wisniewski AA. Movement disorders: a neuro-psychiatric approach. New York: Guilford; 1987. | ||
McCall WV, Shelp FE, Donald WM. Controlled investigation of the amobarbital interview for catatonic mutism. Am J Psychiatry. 1992; 149:202–206. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.