Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Syringocystadenoma Papilliferum: A Case Series and Literature Review
Authors Jiang J, Liao Q, Yang J, Zhang H, Huang S, Xian Z, Zhang Z
Received 2 February 2026
Accepted for publication 26 May 2026
Published 8 June 2026 Volume 2026:19 595115
DOI https://doi.org/10.2147/CCID.S595115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anne-Claire Fougerousse
Jingjing Jiang,1,* Qian Liao,1,* Jiao Yang,2 Huan Zhang,3 Shiyan Huang,1 Zilan Xian,1 Zhengzhong Zhang4
1Department of Dermatology, Sichuan Integrative Medicine Hospital, Chengdu, Sichuan Province, People’s Republic of China; 2Department of Dermatology, The First People’s Hospital of Mianyang, Mianyang, Sichuan Province, People’s Republic of China; 3Department of Dermatology, The First People’s Hospital of Yibin, Yibin, Sichuan Province, People’s Republic of China; 4Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhengzhong Zhang, Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, No. 1 Maoyuan South Road, Shunqing District, Nanchong, Sichuan, 637000, People’s Republic of China, Tel +8618080339898, Email [email protected]
Background: Syringocystadenoma papilliferum is an uncommon benign adnexal tumor originating from apocrine or eccrine sweat glands. It frequently occurs on the head and neck and is often associated with nevus sebaceous, posing diagnostic challenges in clinical practice due to its variable clinical presentations.
Purpose: To investigate the clinical and histopathological characteristics and outcomes of five cases with syringocystadenoma papilliferum and to improve the clinical understanding of this disease in combination with the literature.
Patients and Methods: The clinical and histopathological characteristics and outcomes of five Chinese patients with syringocystadenoma papilliferum were retrospectively analyzed.
Results: There were two males and three females with an age at onset ranging from 0 to 69 years. All the skin lesions were located on the head and neck, with 4 cases occurring on the scalp and 1 case occurring on the neck. Clinical manifestations were isolated nodules, plaques, or linear, papillary plaques, with skin-colored to light yellowish, yellowish pink, or red. The skin lesions of all cases showed a slow increase with age. The histopathological findings were as follows: the papillary projections covered by double layers of epithelial cells and stroma rich in plasma cells. The pathologies of the two cases suggested syringocystadenoma papilliferum combined with nevus sebaceous. All cases underwent complete surgical excision treatment. Postoperative follow-up duration ranged from 24 to 48 months, with no recurrence observed in surviving cases.
Conclusion: Syringocystadenoma papilliferum is a rare cutaneous appendageal tumor, which is easily confused with nevus sebaceous and verrucous lesions. It often occurs on the head and neck. In this small case series, two of five cases demonstrated coexisting syringocystadenoma papilliferum with nevus sebaceous, underscoring the recognized association between these entities. For nevus sebaceous lesions that have persisted for a long time or have undergone morphological changes, the possibility of secondary tumors such as syringocystadenoma papilliferum should be considered. Complete surgical resection with histopathological confirmation is recommended as the definitive management strategy, with postoperative follow-up to monitor for potential recurrence or development of secondary tumors, particularly in cases associated with nevus sebaceous.
Keywords: syringocystadenoma papilliferum, nevus sebaceous, tumor, histopathology, treatment
Introduction
Syringocystadenoma papilliferum (SCAP) is an uncommon benign tumor that originates from apocrine or eccrine sweat glands.1,2 SCAP accounts for a small proportion of cutaneous adnexal neoplasms. It most frequently affects the head and neck region, with the scalp being the predominant site. The condition shows no clear sex predilection, and while approximately 50% of lesions are present at birth or develop in early childhood, adult-onset cases are well documented.2 SCAP often occurs concurrently with nevus sebaceous (NS), and NS is the basis for the occurrence of many benign or malignant tumors, such as trichoblastoma and basal cell carcinoma (BCC).3 The skin lesions present in various forms, such as plaque, linear, and solitary nodule.
Due to its variable clinical presentation and relatively low incidence, SCAP is frequently under-recognized in clinical practice. Misdiagnosis is common, with lesions often mistaken for verruca vulgaris, NS without secondary change, lipoma, or pyogenic granuloma. This diagnostic challenge is particularly significant given the potential for SCAP to coexist with NS—a condition that carries its own risk of secondary tumor development. Therefore, increasing awareness of the clinical spectrum and histopathological features of SCAP is essential for accurate diagnosis and appropriate management. A clear diagnosis depends on histopathology.
This study aims to report five Chinese cases of SCAP diagnosed and treated, with particular attention to the clinical and histopathological characteristics of the patients, the diagnostic challenges illustrated by cases with histories of misdiagnosis, and the management outcomes following surgical excision. By describing these cases and reviewing the relevant literature, we hope to provide a better perspective for clinical diagnosis and management of SCAP, particularly regarding its relationship with NS and the importance of complete surgical excision.
Cases Presentation
This study reviewed a total of five cases with SCAP diagnosed by histopathology at the Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, China, between 2019 and 2022. Cases were retrieved from the institutional outpatient case management and pathology database. The clinical and histopathological results and outcomes of our series are summarized in Tables 1 and 2. Postoperative follow-up duration ranged from 24 to 48 months. The study was approved by the Medical Ethics Committee of Affiliated Hospital of North Sichuan Medical College (2022ER212-1). Our study was carried out in compliance with the Declaration of Helsinki. Written informed consent was obtained from all patients for the publication of their case details and accompanying images.
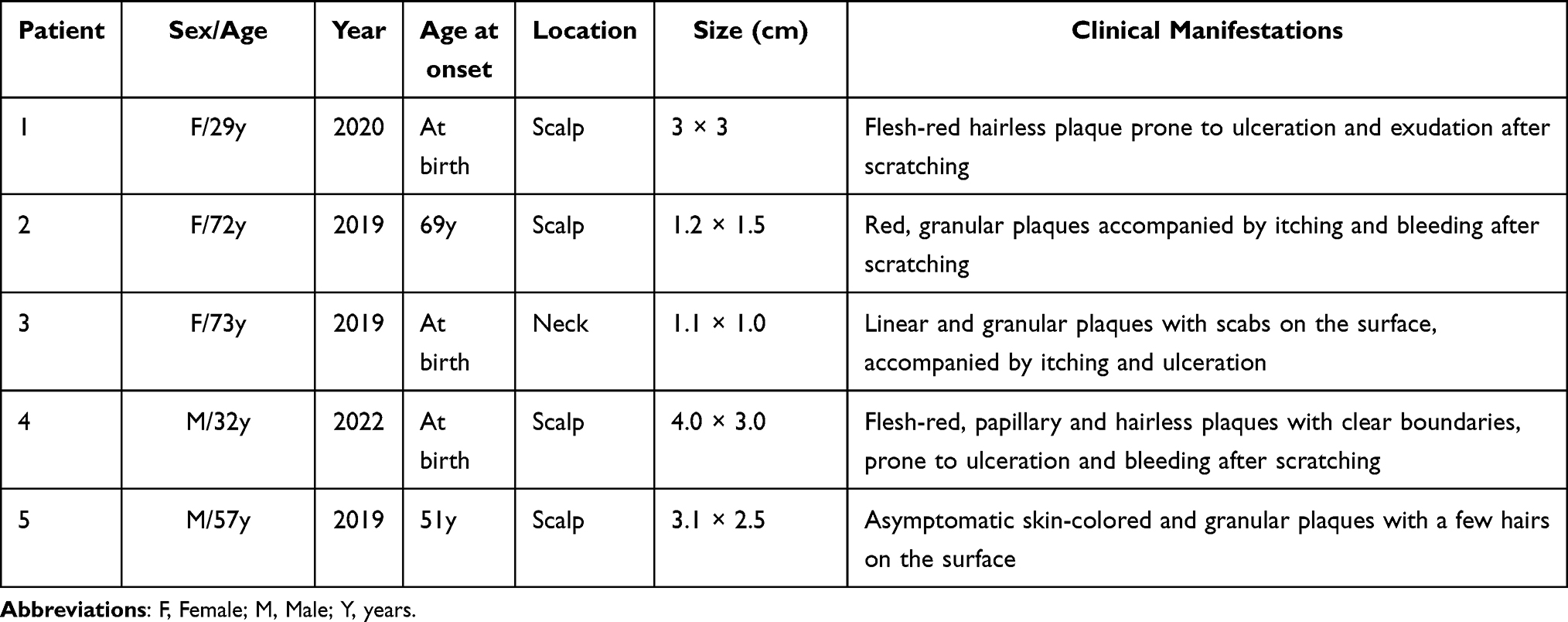 |
Table 1 Clinical Characteristics of Patients with SCAP |
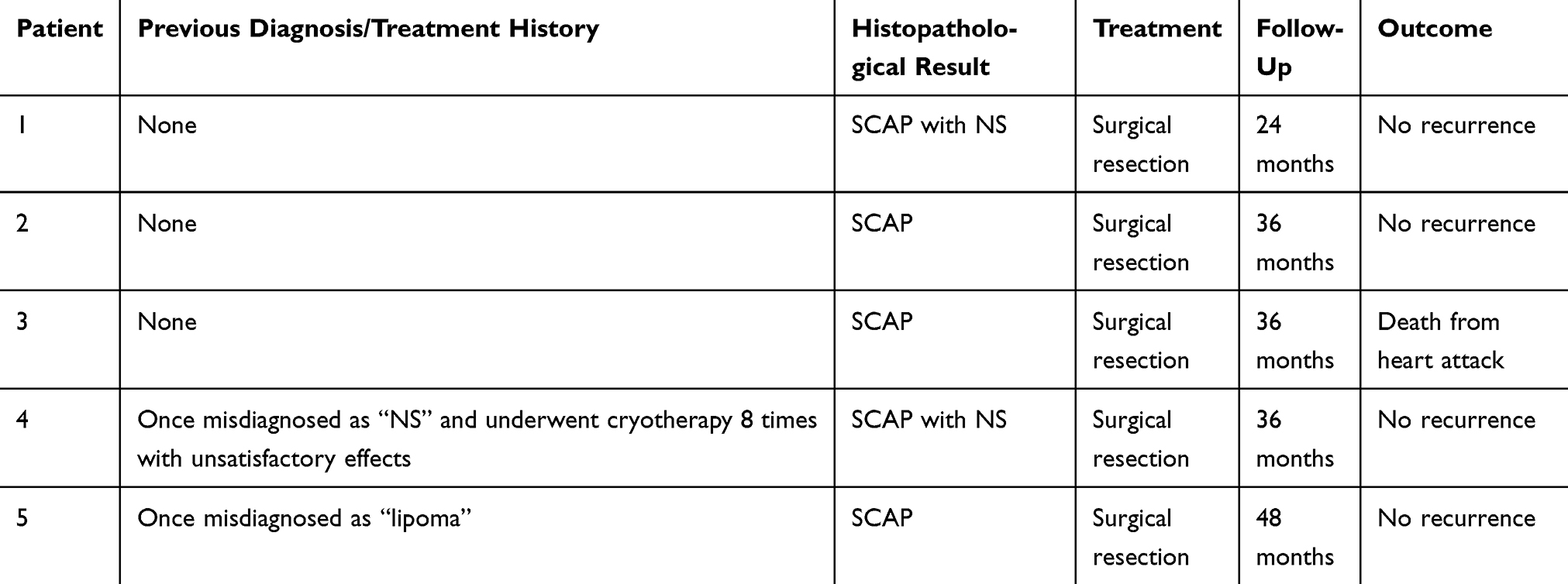 |
Table 2 Histopathological Results, Treatment, and Outcomes of Patients with SCAP |
From the perspective of the onset pattern, this group of cases presented two clear paths: congenital onset and acquired. Among them, 3 cases (Cases 1, 3, and 4) were discovered at birth. The skin lesions increased with age, especially significantly enlarged, and underwent morphological changes after puberty. The other two cases (Case 2 and Case 5) were newly developed in adulthood and had relatively short disease courses (3 years and 6 years, respectively), without the prepubertal growth or morphological changes seen in the congenital cases.
All the skin lesions were located on the head and neck. In the early stage, they were mostly skin-colored, flesh-red, or light yellow plaques or nodules. In the later stage, they often developed into typical appearances with granular or papillary surfaces. Four cases (Cases 1, 2, 3, and 4) reported that their skin lesions experienced varying degrees of itching during the course of the disease, and were prone to ulceration, exudation, or bleeding after scratching. These changes could partially heal on their own after the stimulation was stopped. This symptomatic presentation was one of the important reasons that prompted patients to seek medical attention.
Two cases had a history of misdiagnosis. Case 4 was long misdiagnosed as “NS” and received cryotherapy many times with unsatisfactory results (Figure 1). Case 5 was once considered a “lipoma”. All cases in this group showed the typical histological characteristics of SCAP, including cystic invaginations extending into the dermis with multiple papillary projections. The papillary projections were covered by double layers of cuboidal and columnar luminal cells with stroma rich in plasma cells. In case 1 and case 4, sebaceous gland hyperplasia was also noted, confirming that SCAP arose on a background of NS, and both existed (Figure 2).
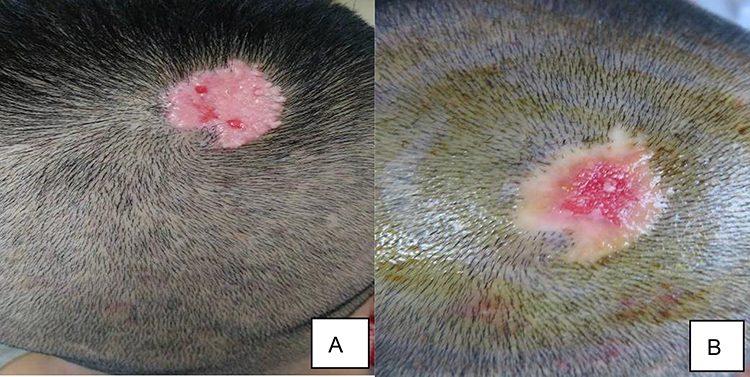 |
Figure 1 The lesion on the scalp of case 4. (A) Flesh-red, papillary, and hairless plaques with clear boundaries prone to ulceration and bleeding after scratching. (B) The lesion after receiving cryotherapy many times. |
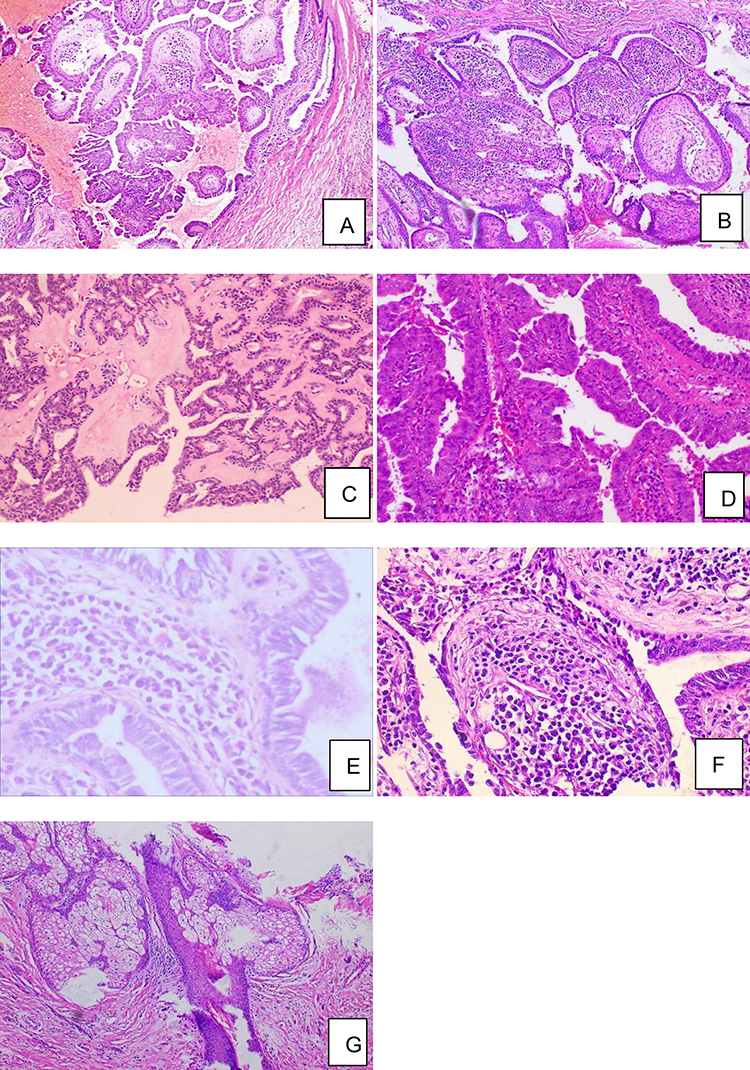 |
Figure 2 Histopathological features. (A–C) Cystic invaginations extending into the dermis, with multiple papillary projections. (D–F) Double layers of cuboidal and columnar luminal cells, with stroma rich in plasma cells. (G) Hyperplasia sebaceous glands. (A) Case 3. (B) Case 4. (C) Case 5. (G) Case 4 (HEx100). (D) Case 1. (E) Case 2. (F) Case 4 (HEx400). |
Discussion
SCAP is a relatively rare benign skin adnexal tumor. Its diagnosis relies on characteristic histopathological manifestations, but clinical identification often faces challenges.4 This series of cases confirms the typical tendency of SCAP to occur in the head and neck.4,5 All the skin lesions in our cases were located on this area, with 80% involving the scalp, which is consistent with the literature reports.5 In addition, there are case reports of the disease occurring in rare areas such as the eyelids, anogenital area, and lower limbs.6–8 Clinically, this group of cases clearly demonstrated two chronological patterns of the onset of SCAP. The majority (3/5) were congenital, with skin lesions presenting at birth or in infancy.2 After a long period, they often significantly increased in size and underwent morphological changes during adolescence. A small number (2/5) were newly developed in adulthood. This bimodal pattern suggests that SCAP may originate from abnormal differentiation of the primitive epithelial germ during the embryonic period or be activated later due to unknown stimuli.
A notable clinical detail is that 80% of the cases in this group presented symptoms such as itching and easy ulceration, bleeding, or exudation after scratching. Although the symptoms are not specific, it is a key reason that prompts patients to seek medical attention. It may be related to the congestion of blood vessels in the dermal papillae and the infiltration of inflammatory cells, especially plasma cells. Additionally, reactive cervical lymphadenopathy may be present in some cases involving inflamed or ulcerated lesions, likely reflecting regional immune response rather than metastatic spread. This clinical finding should not be misinterpreted as evidence of malignancy.9 Besides, it suggests that symptomatic manifestations are important clues for the clinical identification of SCAP. In differential diagnosis, this symptom can easily mislead clinicians to consider pyogenic granuloma or infectious skin lesions. A more typical diagnostic trap is reflected in the misdiagnosed cases of this group. Case 4 was long mistaken for simple NS due to the large range of skin lesions and the insignificant papillary changes on the surface. Case 5 was considered a lipoma as it presented as an asymptomatic skin-colored mass. These examples reveal the diversity of the clinical manifestations of SCAP. For long-term, atypical papules, plaques, or nodules on the head and neck, SCAP should be included in the differential diagnosis, and the final diagnosis must rely on histopathology.
Regarding molecular features, activating mutations of SCAP associated with the RAS/MAPK signaling pathway have been detected, including HRAS, KRAS, and BRAF mutations in sporadic cases.10 Studies targeting SCAP in specific anatomical sites have revealed heterogeneity, with BRAF V600E mutations predominating in anogenital lesions.5 While these molecular insights are informative, they were not directly assessed in our cases and remain an area for future investigation.
Based on the literature, SCAP is not an isolated pathological entity. Its clinical and pathological manifestations are deeply embedded in a broader disease spectrum, which has significant diagnostic and management significance. Firstly, its association with NS is the most classic. Among the five cases presented, two were pathologically confirmed to have concurrent SCAP and NS. SCAP is one of the most common benign tumors associated with NS, which may be due to the presence of ectopic apocrine glands that are located in the deepest part of the NS, which can contribute to either apocrine cysts or SCAP.3,11 Clinicians should be highly vigilant about the possibility of concurrent SCAP or other tumors, such as BCC, for skin lesions diagnosed with NS, especially when new symptoms such as itching and pain, morphological changes such as nodulation and papillomatous hyperplasia, or darkening of color occur after puberty. The experience of case 4 in this study is highly instructive. The patient had received cryotherapy due to skin lesions diagnosed as NS, but the effect was unsatisfactory. Eventually, surgical resection was performed, and the pathology confirmed SCAP with NS. This case indicates that for NS with suspected or concurrent tumors, simple destructive treatments such as laser or cryotherapy are often incomplete and prone to recurrence, and may even delay diagnosis. Complete surgical resection and pathological examination are the gold standards for treating such skin lesions, which can not only cure SCAP but also allow comprehensive assessment of the background of NS.
The coexistence of SCAP with other appendage tumors further supports the possibility of a shared potential for origin. For instance, a case of SCAP coexisting with the rarer tubular apocrine adenoma (TAA) in NS has also been reported.11 Similar reports are rare worldwide, and this combination suggests that they may derive from apocrine glands in the deeper portion of the NS.11 More importantly, the symbiotic environment of these benign tumors may harbor potential for additional neoplasms. There are some reports in the literature on the concurrent occurrence of SCAP and basal cell carcinoma (BCC).3,12 Given that the PTCH gene has been detected in NS, SCAP, and BCC, it has been hypothesized—though not definitively established—that SCAP may represent a transitional stage in the progression from NS to BCC in rare instances.13 Therefore, clinicians and pathologists should recognize that dealing with an SCAP lesion, especially one related to NS, involves examining a tumor field that may contain multiple benign and, rarely, malignant components. This emphasizes the importance of complete resection and comprehensive pathological assessment. However, there are still limitations in current cognition. Most of the evidence comes from small-sample studies or case reports. Whether SCAP in different anatomical sites represents distinct molecular subtypes and the key events underlying malignant transformation still need to be verified by large-scale systematic research.
Histopathological examination is the gold standard for diagnosis. It presents invaginations from the epidermis into the dermis, double-layered cuboidal to columnar luminal cells with multiple papillary structures, and plasma cell-rich inflammatory infiltration.2,4,14 The pathological manifestations in our cases all presented typical SCAP features. In terms of non-invasive detection technology, the features of dermoscopy and reflectance confocal microscopy (RCM) have gradually been studied. On dermoscopy, pinkish-white exophytic papillary structures and a polymorphic vascular pattern are presented.2,15–17 On RCM, dark linear clefts and grayish epithelial islands within or around dark clefts have been observed.15,18 While the reports about dermoscopic and RCM findings of SCAP are limited, confirmation with larger samples is needed.
All patients in this group were cured through complete surgical resection, and there was no recurrence during the follow-up period except for case 3 who died of heart disease. This is consistent with the nature of benign tumors in SCAP and once again confirms the effectiveness of surgical resection. For small skin lesions, primary closure is sufficient. For larger skin lesions, as shown in Case 4, plastic surgical techniques such as fractional excision, flap repair, or skin grafting need to be considered.
This study has certain limitations. Firstly, as a single-center retrospective study, the number of cases is limited, and there may be selection bias. Secondly, the follow-up time varies among different cases. While several case series of SCAP have been published previously, the present series contributes to the literature by documenting the clinical experience from a Chinese population and providing detailed documentation of instructive cases with histories of misdiagnosis and inappropriate treatment (Cases 4 and 5). These cases offer practical clinical lessons regarding the importance of maintaining a high index of suspicion for SCAP in atypical or treatment-resistant lesions on the head and neck. In addition, this series provides valuable references for clinical practice through detailed clinicopathological descriptions. The molecular genetic characteristics of SCAP, whether SCAP related to NS has different molecular markers, and the potential role of non-surgical therapies in inoperable patients might be future research directions.
Conclusion
In this series of five cases, all patients were successfully treated with complete surgical resection, with no recurrence observed in surviving patients during follow-up. SCAP is a benign appendage tumor with diverse clinical manifestations, often associated with NS. For plaques and nodules that have long existed in the head and neck area, especially those with morphological changes or symptoms such as ulceration and bleeding, SCAP should be included in the differential diagnosis to avoid misdiagnosis. When SCAP occurs in the background of NS, its clinical significance is important, and the tumor transformation potential of NS should be monitored vigilantly. Complete surgical resection is the gold standard for treatment, ensuring a low recurrence rate and obtaining tissue for a clear diagnosis. Larger multi-center studies are needed to further characterize the clinical spectrum of this rare tumor.
Ethics and Consent Statement
Written informed consent was obtained from all the patients for the publication of the case details and accompanying images.
Acknowledgments
We would like to thank the patients and physicians for participating in our research.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sho Y, Sakai T, Yamate T, et al. Unusual congenital syringocystadenoma papilliferum on the scalp presenting as only erosion at birth. Eur J Dermatol. 2020;30(2):198–7. doi:10.1684/ejd.2020.3730
2. Taneja G, Dhanta A, Anthony ML, Hazarika N. Dermoscopic clues to syringocystadenoma papilliferum. J Cutan Aesthet Surg. 2022;15(2):199–201. doi:10.4103/JCAS.JCAS_103_21
3. Idriss MH, Elston DM. Secondary neoplasms associated with nevus sebaceus of Jadassohn: a study of 707 cases. J Am Acad Dermatol. 2014;70(2):332–337. doi:10.1016/j.jaad.2013.10.004
4. Mammino JJ, Vidmar DA. Syringocystadenoma Papilfiferum. Int J Dermatol. 1991;30(11):763–766. doi:10.1111/j.1365-4362.1991.tb04780.x
5. Konstantinova AM, Kyrpychova L, Nemcova J, et al. Syringocystadenoma papilliferum of the anogenital area and buttocks: a report of 16 cases, including human papillomavirus analysis and HRAS and BRAF V600 mutation studies. Am J Dermatopathol. 2019;41(4):281–285. doi:10.1097/DAD.0000000000001285
6. Loza-Escutia O, Godínez-Chaparro JA, Guevara-Castillo RM, de Jesús Quintal-Ramírez M, Quispe Susara EN. Syringocystadenoma papilliferum of eyelid, an unusual presentation: a case series. Dermatol Prac Conceptual. 2023;13(4):e2023239. doi:10.5826/dpc.1304a239
7. Steshenko O, Chandrasekaran N, Lawton F. Syringocysadenoma papilliferum of the vulva: a rarity in gynaecology. BMJ Case Rep. 2014;2014:bcr2014203902. doi:10.1136/bcr-2014-203902
8. Yoshii N, Kanekura T, Setoyama M, Kanzaki T. Syringocystadenoma papilliferum: report of the first case on the lower leg. J Dermatol. 2004;31(11):939–942. doi:10.1111/j.1346-8138.2004.tb00632.x
9. Nikolaev NN, Yankov YG. Lymph nodes of the head and neck: in normal and pathological conditions. Varna Med Forum. 2023;12(1):69–74. doi:10.14748/vmf.v12i1.9034
10. Shen A-S, Peterhof E, Kind P, et al. Activating mutations in the RAS/mitogen-activated protein kinase signaling pathway in sporadic trichoblastoma and syringocystadenoma papilliferum. Hum Pathol. 2015;46(2):272–276. doi:10.1016/j.humpath.2014.11.002
11. Kim MS, Lee JH, Lee W-M, Son S-J. A case of tubular apocrine adenoma with syringocystadenoma papilliferum that developed in a nevus sebaceus. Ann Dermatol. 2010;22(3):319–322. doi:10.5021/ad.2010.22.3.319
12. Jiang J, Chen Y, He Q, et al. Syringocystadenoma papilliferum and basal cell carcinoma arising in nevus sebaceous. Clin Cosmet Invest Dermatol. 2022;15:2021–2026. doi:10.2147/CCID.S378746
13. Askar S, Kilinc N, Aytekin S. Syringocystadenoma papilliferum mimicking basal cell carcinoma on the lower eyelid: a case report. Acta chirurgiae plasticae. 2002;44(4):117–119.
14. Bruno CB, Cordeiro FN, Soares Fdo E, Takano GHS, Mendes LST. Aspectos dermatoscópicos do siringocistoadenoma papilífero associado a nevo sebáceo. An Bras Dermatol. 2011;86(6):1213–1216. doi:10.1590/S0365-05962011000600027
15. Karaarslan I, Acar A, Yaman B, Ozdemir F. Reflectance confocal microscopic findings of a tiny syringocystadenoma papilliferum. JAAD Case Rep. 2019;5(4):323–325. doi:10.1016/j.jdcr.2019.02.023
16. Lombardi M, Piana S, Longo C, et al. Dermoscopy of syringocystadenoma papilliferum. Australas J Dermatol. 2018;59(1):e59–e61. doi:10.1111/ajd.12654
17. Dash S, Nayak AK, Sethy M, Palit A, Behera B. Dermoscopic findings of de novo syringocystadenoma papilliferum. Indian J Dermatol Venereol Leprol. 2021;87:278–280. doi:10.25259/IJDVL_575_20
18. Vigil SR, Yi AN, Elwood H, Durkin J, Smidt AC. Pediatric syringocystadenoma papilliferum arising de novo on the leg: characteristics observed with reflectance confocal microscopy. Pediatr Dermatol. 2025;42(4):882–884. doi:10.1111/pde.15869
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Leiomyoma with Bizarre Nuclei: A Current Update
Guo E, Li C, Hu Y, Zhao K, Zheng Q, Wang L
International Journal of Women's Health 2022, 14:1641-1656
Published Date: 25 November 2022
The Current Status and Future Directions on Nanoparticles for Tumor Molecular Imaging
Yin C, Hu P, Qin L, Wang Z, Zhao H
International Journal of Nanomedicine 2024, 19:9549-9574
Published Date: 14 September 2024