Back to Journals » International Medical Case Reports Journal » Volume 16
Synchronous Volvulus of Ascending and Transverse Colon
Authors Mengistu S ![]() , Asnake M
, Asnake M ![]() , Hassen S, Mekonnen B
, Hassen S, Mekonnen B ![]()
Received 22 March 2023
Accepted for publication 27 June 2023
Published 30 June 2023 Volume 2023:16 Pages 397—400
DOI https://doi.org/10.2147/IMCRJ.S413600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Sisay Mengistu,1 Molla Asnake,2 Suleman Hassen,1 Biruk Mekonnen2
1Department of Surgery, College of Medicine and health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia; 2School of Medicine, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Biruk Mekonnen, School of Medicine, College of Medicine and Health science, Mizan-Tepi University, P.O. Box: 520, Mizan-Aman, Ethiopia, Email [email protected]
Introduction: Colonic volvulus is the torsion of a part of the colon causing large bowel obstruction by strangulation, which may lead to ischemia and then necrosis. Synchronous colonic volvulus is extremely rare; even if there are some case reports on synchronous colonic volvulus, there are no reported cases of synchronous ascending and transverse colon volvulus in the medical literature to our knowledge.
Case Presentation: A 25-year-old girl with a previous history of epilepsy presented with a one-day duration of abdominal cramps with associated symptoms of vomiting of bilious matter, failure to pass faeces, and flatus of the same duration. The patient underwent surgical intervention, and ascending and transverse volvulus were discovered.
Conclusion: In spite of ascending and transverse colon volvulus rarity, we advised including these in the differential diagnosis of patients associated with large bowel obstruction.
Keywords: ascending colon, intestinal volvulus, large bowel obstruction, transverse colon
Introduction
Colonic volvulus is the axial twisting of the colon on its vascular pedicle.1 Colonic volvulus occurs when a segment large bowel becomes torsional, and it often leads to bowel obstruction and strangulation. It is the third leading cause of obstruction, preceded by tumor obstruction and complicated sigmoid diverticulitis worldwide.2,3 The most common sites of volvulus are sigmoid volvulus (52%), cecum volvulus (43%), followed by a transverse colon (3%), and splenic flexure (2%).4,5 A double Synchronous ascending and transverse colon volvulus is an extremely rare situation.6–8 To our knowledge, there is no report available on synchronous ascending and transverse colon volvulus to date. We presented our experience in successfully treating a unique case.
Case Presentation
A 25-year-old girl with a previous history of epilepsy presented to Mizan-Tepi University Teaching Hospital, Mizan-Aman, Ethiopia, an emergency department with a chief complaint of abdominal cramp of one-day duration on July 15, 2022, GC. She also had associated symptoms of vomiting of bilious matter, failure to pass feces and flatulence of the same duration. Otherwise, she has no other complaints. Her vital signs were: a heart rate of 120 beats per minutes, BP of 100/70 mmHg, and a temperature of 37.8 ◦C. On general examination, she had signs of moderate dehydration. Her abdomen was grossly distended, it barely moved with respiration, and there was generalized tenderness with involuntary guarding. Additionally, hypertympanic, hyperactive bowel sounds, and a digital rectal examination revealed an empty rectum.
Her emergent laboratory data were as follows: WBC (9.89 × 1000/μL) with an elevated hemoglobin level (17.1 g/dl) and normal platelet count. Serum electrolytes and renal function tests were in the normal range. Emergency abdominal plain radiography was the next step, which showed distended large bowel segments and distal small bowel with visible fecal matter distal to the descending colon with 2 air-fluid levels (Figure 1).
 |
Figure 1 Distended large bowel segments and distal small bowel with visible fecal matter. |
Generalized peritonitis secondary to large bowel obstruction was considered an early diagnosis. Considering history, physical examination, and x-ray findings, after obtaining written consent for a short period of resuscitation, an exploratory laparotomy was performed. Intraoperative findings revealed a synchronous ascending and transverse volvulus. The hepato-colic ligament was absent, and the ascending colon was not fixed with a mobile cecum colon. The patient had a closed loop obstruction with one end at the distal one-third of the transverse colon and the other end at the distal ilium near the ilio-Ceca valve. The ascending colon and the proximal two-thirds of the transverse colon were gangrenous. So the ascending colon was resected along with the transverse colon to perform a standard extended right hemicolectomy and ilio-transverse colon anastomosis. (Figure 2) Additionally, around one litre of hemorrhagic fluid was evacuated from the peritoneal cavity. The postoperative period was uneventful, and the patient was discharged after seven days.
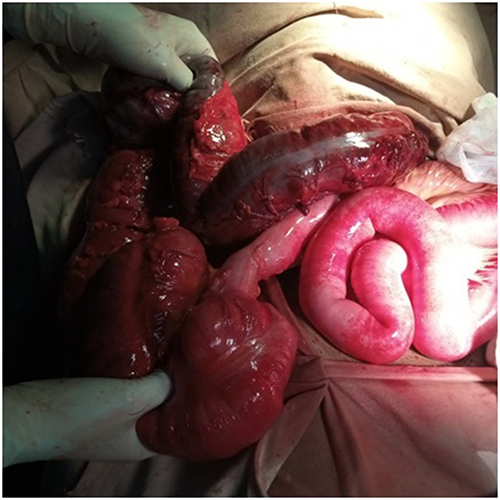 |
Figure 2 Gross operative view of volvulus. |
Discussion
Acute intestinal obstruction accounts for a great proportion of morbidity and mortality in rural Africa. Like in other parts of Africa, intestinal obstruction constitutes a major cause of morbidity and mortality in Ethiopia.7 One study done in Ethiopia revealed the sigmoid volvulus as the main cause (69.0%) of large bowel obstruction, followed by colonic tumor (5.3%). But when we came to the transverse colon and ascending colon volvulus as the cause of LBO, it is rare: transverse colon volvulus was first defined in 1932 by Kallio and is uncommon (1–4% of cases). Therefore, the probability of finding synchronic volvulus ascending and transverse colons is expected to be rare.7,9
A qualitative systematic review done in six cases from Gaston Berger University, Saint-Louis, Senegal, suggested that synchronous volvulus symptoms have no particular pattern other than the symptom of large bowel obstruction.7 Even if imaging remains important, the modalities to be used rest with the surgical teams. In our setup, due to the absence of a CT scan, which has better reliability in diagnosis than plain abdominal radiography is practiced. But in this mentioned study, CT also did not show a typical pattern in 5 of 7 patients, and as a result, the diagnosis of synchronous large bowel volvulus remains difficult preoperatively and is often discovered after surgery.6,9,10 This statement goes along with what is described in this case presentation.
To the best of these authors’ knowledge and as we tried to navigate PubMed, Google Scholar Web of Science, and Scopus, this is the first reported case. The diagnosis of synchronous ascending and transverse colon volvulus was confirmed during the intraoperative period. Since there is no peculiar X-ray lesion on the clinical symptom list for synchronous volvulus other than the finding related to large bowel obstruction.10 As a result, based on patient symptoms and signs, the diagnosis of large bowel obstruction secondary to fecal impaction or intestinal parasitosis was considered. There are a few reported cases of synchronous double volvulus of different segments of the large bowel, but no reported concurrent involvement of the transverse colon and ascending colon, as mentioned above.7
Among the risk factors mentioned for synchronous volvulus, factors that lead to abnormal mobility of the colon are more anatomy-related.10 When we saw this patient, her hepato-colic ligament was absent and the ascending colon was not fixed, which is expected to increase her risk for the volvulus by increasing the risk of bowel twisting.11
The risk factor for synchronous volvulus is mainly associated with different anatomical, physiologic, and congenital factors.10 In our case, the patient’s hepato-colic ligament was absent and the ascending colon was not fixed, which is expected to increase her risk for the volvulus by increasing the risk of bowel twisting.12 This is in line with the qualitative systematic review done at Gaston Berger University, which showed that anatomical abnormalities are associated with abnormal mobility of the colon.7
Conclusion
A rare case report of synchronous volvulus of the ascending and transverse colon in adult is presented. Clinician in the areas should consider this entity when evaluating large bowel obstruction, even if not suspected preoperatively due to non-specified signs and symptoms and X-ray findings. Synchronous volvulus involving the ascending colon and transverse colon has never been reported until the day this case report was written. As a result, to diagnose this type of case, the team managing volvulus cases is advised to be more suspicious. Additionally, underlying risk factors like congenitally unfixed colon (absence of hepato-colic ligament as in our cases) should be assessed thoroughly, unlike in single volvulus.
Ethics Approval
Ethical approval for this study was obtained from College of Medicine and Health Science, Mizan-Tepi University, and Reference No. HSE/00429/2012.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Acknowledgments
The authors would like to thank Mizan-Tepi University for technical support and ethical approval for this case study. We also would like thank MTU department of surgery for their help in supplementing patient documents.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Samlali A, Boussaidane S, Hamri A, Narjis Y, Benelkhaiat Benomar R. Synchronous volvulus of the transverse and sigmoid colon: a rare case of large bowel obstruction. PAMJ. 2021;38(231):1.
2. Ballantyne GH, Brandner MD, Beart RW Jr, Ilstrup DM. Volvulus of the colon. Incidence and mortality. Ann Surg. 1985;202(1):83–92. doi:10.1097/00000658-198507000-00014
3. Friedman JD, Odland MD, Bubrick MP. Experience with colonic volvulus. Dis Colon Rectum. 1989;32(5):409–416. doi:10.1007/BF02563694
4. Perrot L, Fohlen A, Alves A, Lubrano J. Management of the colonic volvulus in 2016. J Visc Surg. 2016;153(3):183–192. PMID: 27132752. doi:10.1016/j.jviscsurg.2016.03.006
5. Udezue NO. Sigmoid volvulus in Kaduna, Nigeria. Dis Colon Rectum. 1990;33(8):647–649. doi:10.1007/BF02150738
6. Islam S, Hosein D, Harnarayan P, Naraynsingh V. Synchronic volvulus of splenic flexure and caecum: a very rare cause of large bowel obstruction. BMJ Case Rep. 2016;2016:bcr2015213029. doi:10.1136/bcr-2015-213029
7. Ndong A, Diao ML, Tendeng JN, Diallo AC, Ma Nyemb PM, Konaté I. Synchronous sigmoid and transverse volvulus: a case report and qualitative systematic review. Int J Surg Case Rep. 2020;75:297–301. doi:10.1016/j.ijscr.2020.09.027
8. Katsanos K, Ignatiadou E, Markouizos G, Doukas M, Siafakas M, Fatouros M. Non-toxic megacolon due to transverse and sigmoid colon volvulus in a patient with ulcerative colitis. J Crohns Colitis. 2009;3(1):38–41.
9. Hellinger MD, Steinhagen RM. Colonic volvulus. In: Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, editors. The ASCRS Textbook of Colon and Rectal Surgery.
10. McBrearty A, Harris A, Gidwani A. Transverse-sigmoid colon knot: a rare cause of bowel obstruction. Ulster Med J. 2011;80(2):107–108.
11. Hoseini A, Eshragi Samani R, Parsamoin H, Jafari H. Synchronic volvulus of sigmoid and transverse colon: a rare case of large bowel obstruction, Ann. Colorectal Res. 2014;2(1):1–2.
12. Lianos G, Ignatiadou E, Lianou E, Anastasiadi Z, Fatouros M. Simultaneous volvulus of the transverse and sigmoid colon: case report. J Italian Surg Assoc. 2012;33(10):324–326.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.