Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Symptomatic stability with aripiprazole once-monthly: efficacy analyses from acute and long-term studies
Authors Madera JJ, Such P, Zhao C, Baker RA ![]()
Received 19 December 2018
Accepted for publication 9 April 2019
Published 18 June 2019 Volume 2019:15 Pages 1593—1604
DOI https://doi.org/10.2147/NDT.S198786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Jessica J Madera,1 Pedro Such,2 Cathy Zhao,3 Ross A Baker1
1Global Medical Affairs, Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, NJ, USA; 2Medical Affairs Psychiatry, H. Lundbeck A/S, Valby, Denmark; 3Biostatistics, Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, NJ, USA
Objective: To evaluate the effect of aripiprazole once-monthly 400 mg (AOM 400; Abilify Maintena®) on symptom stability in acute treatment and maintenance therapy settings in patients with schizophrenia.
Methods: Results were analyzed from two pivotal maintenance studies (Studies 246 and 247), a long-term (52 weeks), open-label extension of these studies (Study 248), an open-label, mirror-image study in patients switching from oral to long-acting injectable antipsychotic therapy (Study 283), and a study of AOM 400 in the acute setting (Study 291). Symptom stability was assessed using the Positive and Negative Syndrome Scale (PANSS) and the Clinical Global Impression (CGI) scale (CGI-Severity of Illness and CGI-Improvement). Results are reported for the total study population and in subgroups stratified by age.
Results: In Study 246, AOM 400 resulted in significantly greater improvements from baseline vs placebo on all measures of symptom stability, with improvements maintained through 52 weeks. In Study 247, a non-inferiority study, AOM 400 resulted in improvements in PANSS and CGI scores comparable or significantly greater at all timepoints vs oral aripiprazole. In Study 248, AOM 400 resulted in the long-term stability of symptom improvements from the earlier studies. In Study 283, AOM 400 resulted in significant improvements from baseline in PANSS and CGI scores over 24 weeks. In Study 291, AOM 400 resulted in significantly greater improvements from baseline in PANSS and CGI scores vs placebo at all post-baseline timepoints. In post hoc analyses, AOM 400 showed similar efficacy in symptom improvement in adult patients aged ≤35 years and >35 years, with some evidence of a larger treatment effect on PANSS negative symptoms among younger patients in the acute treatment setting.
Conclusion: In acute treatment and maintenance therapy settings, AOM 400 was effective in the rapid stabilization and long-term maintenance of symptoms in patients with schizophrenia.
Keywords: aripiprazole, long-acting injectable, antipsychotics, schizophrenia
Introduction
Schizophrenia is a disabling mental disorder characterized by chronic recurrent psychosis. The majority of patients experience multiple relapses over time involving exacerbations of acute illness.1 Illness exacerbations may have significant negative consequences in terms of social functioning and overall health.1–4 Exacerbations may result in decreased self-esteem and personal autonomy, increased risk of self-harm and harm to others, disruption of vocational and social activities, and increased burden on family and caregivers.2 Relapse is associated with nonadherence to antipsychotic treatment,5 decreased response and increased time to response to treatment,6–8 and failure to recover fully to the same degree as prior to the relapse.1
The goal of treatment in the acute setting is to achieve rapid control of positive symptoms including psychotic thoughts and behaviors. Once an acute episode is stabilized, the goal of maintenance treatment is to keep psychotic symptoms stabilized. Adherence to antipsychotic treatment is crucial to the success of long-term maintenance treatment. Nonadherence is common among patients with schizophrenia and is associated with increased risk of relapse and hospitalization.9 Discontinuation of medication is the most important predictor of risk of relapse in schizophrenia.10–12
Long-acting injectable (LAI) antipsychotics may play an important role in improving adherence to antipsychotic treatment regimen because they remove the need for daily compliance with oral treatment regimens. Additionally, a missed monthly injection visit serves as an alert of potential medication nonadherence.11,13 Aripiprazole once-monthly 400 mg (AOM 400; Abilify Maintena®) is an extended-release injectable solution of aripiprazole. It is the first dopamine D2 receptor partial agonist treatment for schizophrenia available as a LAI.14–17 Although the mechanism of action of aripiprazole remains unknown,17 it has been proposed that its effects are mediated through a combination of partial agonist activity at D2 and 5-HT1A receptors, and antagonist activity at 5-HT2A receptors.14 Other atypical LAI formulations currently available (eg, olanzapine, risperidone, and paliperidone) are antagonists at dopamine D2 and 5-HT2A receptors.18 As a partial agonist, aripiprazole can regulate excess dopamine activity in the mesolimbic pathway to limit positive symptoms, while allowing sufficient dopamine signaling in the mesocortical pathway, which has been linked to reductions of negative and cognitive symptoms.19,20 The unique mechanism of action (partial agonism) of AOM 400 mg, compared with other atypical LAIs, may provide effective treatment of positive and negative symptoms. With a moderate affinity for α-adrenergic or histaminergic receptors, and absence of affinity for cholinergic receptors, aripiprazole has a safety and tolerability profile that compares favorable with other atypical antipsychotics.21 Specifically, AOM 400 is not associated with some of the side effects that may develop with the use of other atypical LAI formulations such as prolactin elevations with risperidone and paliperidone18,22 or postinjection delirium/sedation syndrome with olanzapine.22 In clinical trials, AOM 400 has been shown to be effective both in the treatment of acute psychotic episodes and in the long-term maintenance of stability of symptoms and psychosocial functioning, including reducing the rates of impending relapse and hospitalization.16,23–28 Here we report results of post hoc analyses evaluating the effect of AOM 400 on symptom stability in adult patients with schizophrenia, including analysis of adult patients stratified by age (≤35 years and >35 years), in two pivotal maintenance studies (Studies 246 [NCT00705783]16 and 247 [NCT00706654]23), an open-label extension of these studies (Study 248 [NCT00731549]24), an open-label, mirror-image study (6 months pre- and post-initiation of AOM 400) in patients switching from oral to LAI antipsychotic therapy (Study 283 [NCT01432444]25–27), and a study of AOM 400 in the acute setting (Study 291 [NCT01663532]28).
Methods
Patients
Detailed methods of the individual studies, including full patient inclusion/exclusion criteria, were previously described in detail.16,23–28 Studies 246 and 247 enrolled adults aged between 18 and 60 years with a diagnosis of schizophrenia (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision [DSM-IV-TR]) for at least 3 years prior to screening who required chronic antipsychotic treatment.16,23 Study 248 enrolled de novo patients or patients who participated in Studies 246 and 247, aged between 18 and 65 years.24
Study 283 enrolled patients aged between 18 and 65 years with a diagnosis of schizophrenia (DSM-IV-TR) for greater than 1 year with 7 months of hospitalization data who had received oral antipsychotic treatment in the 7 months preceding screening and who in the investigator’s opinion required change of treatment for any reason (eg, poor adherence, lack of efficacy, tolerability issues) and might benefit from switching to an LAI antipsychotic. Eligible patients were required to have had at least one inpatient psychiatric hospitalization in the previous 4 years before study screening.25–27
Study 291 enrolled adults with schizophrenia (DSM-IV-TR) aged between 18 and 65 years who were having an acute psychotic episode at screening and baseline, based on the following criteria: a Positive and Negative Syndrome Scale (PANSS) total score of ≥80 and specific psychotic symptoms on the PANSS as measured by a score of >4 on each of 4 specific items: conceptual disorganization, hallucinatory behavior, suspiciousness/persecution, and unusual thought content.28
In accordance with the International Conference on Harmonisation Good Clinical Practice Consolidated Guideline and the Declaration of Helsinki, the protocol and amendments of each study were approved by the governing institutional review board (IRB) or independent ethics committee (IEC) for each respective trial site or country, and all patients provided written informed consent prior to study participation. (See
Study designs
Designs for Studies 246, 247, 248, 283, and 291 are shown in Figure 1 and have been previously reported.16,23–28
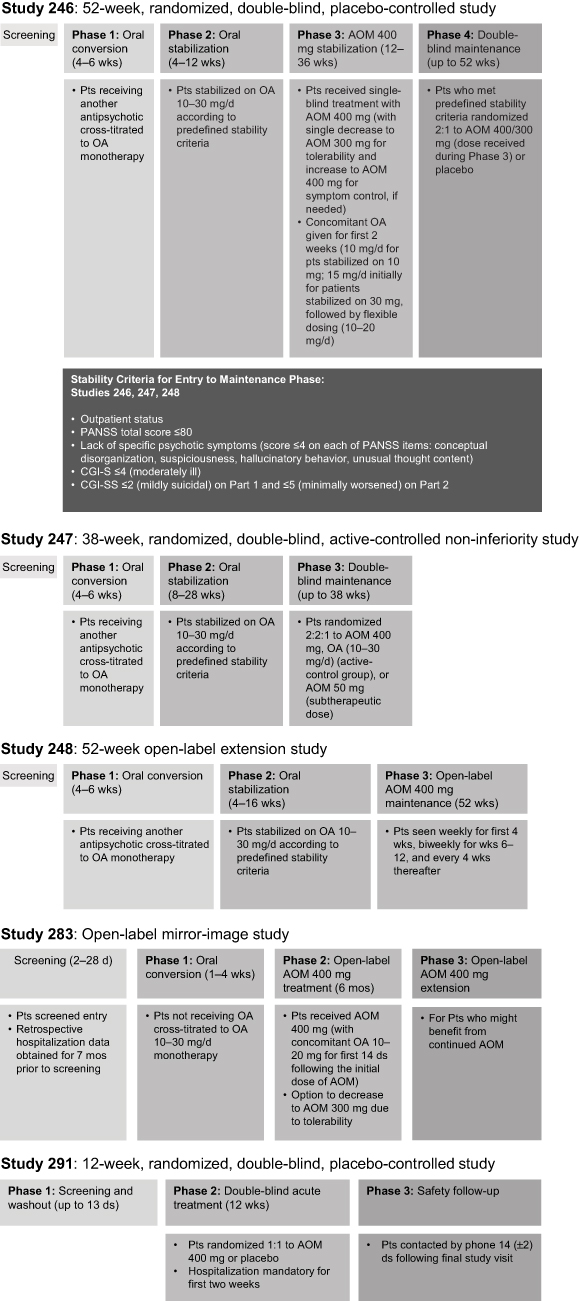 | Figure 1 Study designs (Studies 246,16 247,23 248,24 283,25–27 and 29128).Abbreviations: AOM, aripiprazole once-monthly; CGI-S, Clinical Global Impression Severity; OA, oral aripiprazole; Pts, patients; PANSS, Positive and Negative Syndrome Scale; CGI-SS, Clinical Global Impression-Severity of Suicidality. |
Analyses
Analyses of results from Studies 246, 247, 248, 283, and 291 were conducted to assess symptom stability with AOM 400 in both the acute and maintenance settings. In all studies, symptom stability was assessed using the PANSS, both total and subscale scores, and the Clinical Global Impression (CGI) scale (CGI-Severity [CGI-S] and CGI-Improvement [CGI-I]). PANSS is a clinician-rated instrument for measuring the severity of psychopathology. PANSS consists of three subscales, a positive subscale, a negative subscale, and a general psychopathology subscale, encompassing 30 symptom constructs, rated from 1 (symptom not present) to 7 (symptom extremely severe).29 CGI is a clinician-rated summary evaluation of the impact of a patient’s symptoms on functional ability. It comprises two one-item measures, both based on a 7-point scale, to assess: 1) the severity of psychopathology (CGI-S) and 2) change in severity following initiation of treatment (CGI-I).30
Efficacy analyses for Studies 246 and 247 included assessment of changes from baseline in PANSS total score, positive and negative subscales, and CGI-S using analysis of covariance (ANCOVA), controlling for treatment and baseline value. Last observation carried forward (LOCF) results are reported. The Cochran-Mantel-Haenszel method was used for analysis of CGI-I, based on raw mean score statistics. LOCF results are reported. Efficacy analyses for the oral stabilization phases in Studies 246 and 247 and the AOM 400 stabilization phase in Study 246 included all patients who entered the respective phases and had at least one post-baseline efficacy evaluation. Efficacy analyses for the double-blind, controlled maintenance phase in Studies 246 and 247 included the intent-to-treat (ITT) dataset, composed of all patients randomly assigned to double-blind treatment. Results are reported for the total study population as well as subgroups stratified by age (adult patients aged ≤35 years or >35 years).
For Study 248, mean changes from baseline for PANSS total score, positive and negative subscales, CGI-S, and CGI-I were summarized using descriptive statistics. LOCF results are reported. Efficacy analyses for the oral stabilization phase included all patients who received at least one dose of oral aripiprazole (OA) and completed at least one post-baseline efficacy evaluation. Efficacy analyses for the open-label maintenance phase included all patients who received at least one dose of AOM 400 and completed at least one post-baseline efficacy evaluation. Descriptive statistics were also used to summarize rates of sustained remission at Week 52. LOCF results are reported. Sustained remission was defined as scores of ≤3, sustained for ≥6 months, on eight prespecified items across the three subscales of the PANSS – positive symptoms (delusions, hallucinatory behavior, conceptual disorganization), negative symptoms (blunted affect, social withdrawal, lack of spontaneity), and general psychopathology symptoms (usual thought content, mannerisms/posturing).31 This analysis included all patients who received at least one dose of AOM 400 and who had at least one post-baseline efficacy evaluation during the open-label maintenance phase. Results are reported for the total study population as well as subgroups stratified by age (adult patients aged ≤35 years or >35 years).
For Study 283, mean changes from baseline in PANSS total score, positive and negative subscales, CGI-S, and CGI-I were summarized using descriptive statistics and/or the paired t-test. LOCF results are reported. Efficacy analyses for the open-label AOM 400 treatment phase included the ITT dataset, containing all patients who entered the open-label AOM 400 treatment phase. Results are reported for the total study population as well as subgroups stratified by age (adult patients aged ≤35 years or >35 years).
For Study 291, comparison of changes from baseline in PANSS total score, positive and negative subscales, and CGI-S were performed using the Mixed Model Repeated Measure (MMRM) method using the observed case (OC) dataset, with fixed effects of treatment, region (pooled site), week, treatment-by-week interaction, and baseline-by-week interaction as covariates. An unstructured covariance structure for observations within a subject was used. CGI-I score was analyzed using the Cochran-Mantel-Haenszel row mean score test. LOCF results are reported. Post hoc exploratory analyses were conducted to evaluate the change in PANSS and CGI scores by age (adult patients aged ≤35 years or >35 years). These analyses included patients in the efficacy sample defined as modified ITT population who received at least one dose of AOM 400 or placebo and had at least one post-baseline efficacy assessment. Within-group difference in the least squared mean (LSM) change from baseline for AOM 400 vs placebo was calculated in the efficacy sample to determine treatment effect using MMRM method (including treatment group, pooled centers, week, and treatment-by-week interaction as factors, and baseline-by-week interaction as covariate) and ANCOVA (including treatment group and pooled centers as factors, and baseline value as covariate) of OC data. LSM treatment effects for adult patients aged ≤35 years or >35 years are reported by treatment week for PANSS total and positive and negative subscales and CGI-S.
Results
Patient characteristics and disposition
Baseline demographics and patient disposition for Studies 246, 247, 248, 283, and 291 have been reported previously.16,23–28 In the original studies in which patients were randomized, baseline demographics and disease characteristics were similar between treatment groups.
Efficacy
Study 246
In Study 246, aripiprazole resulted in improvements in PANSS total score, positive and negative subscale scores, and CGI-S score relative to baseline during both oral and AOM 400 stabilization phases (Figures 2 and 3). Mean (SD) PANSS total score decreased from 65.06 (14.69) at baseline to 58.79 (12.05) at Week 12 of the OA stabilization phase and from 58.79 (12.05) at baseline to 54.47 (11.86) at Week 36 of the AOM 400 stabilization phase. Mean (SD) CGI-S scores decreased from 3.40 (0.82) at baseline to 3.13 (0.79) at Week 12 of the OA stabilization phase and from 3.13 (0.79) at baseline to 2.88 (0.82) at Week 36 of the AOM 400 stabilization phase.
 | Figure 2 PANSS total score and positive and negative subscale scores over the course of Studies (A) 246,16 (B) 247,23 (C) 248,24 (D) 283,25–27 and (E) 291.28Notes: (A) Kane JM, Sanchez R, Perry PP, et al. Aripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled study. The Journal of Clinical Psychiatry. 73:617–624, 2012. Copyright 2012, Physicians Postgraduate Press. Reprinted by permission.16 (B) Data from Fleischhacker et al.23(C) Reproduced from Peters-Strickland T, Baker RA, McQuade RD, et al. Aripiprazole once-monthly 400 mg for long-term maintenance treatment of schizophrenia: a 52-week open-label study. NPJ Schizophr. 2015;1:15039. Creative Commons license and disclaimer available from: |
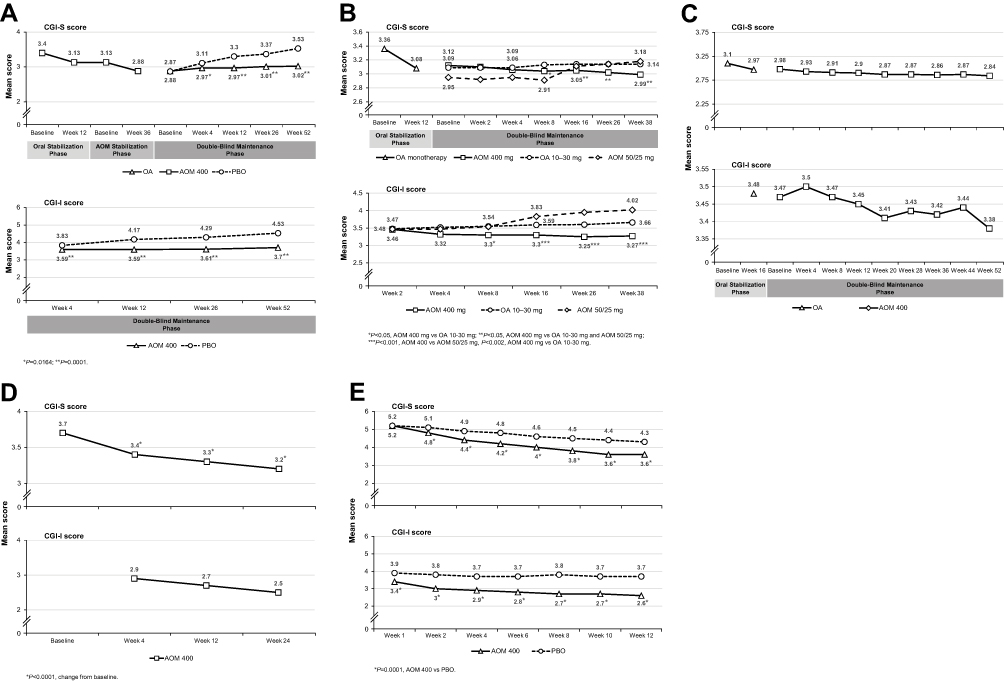 | Figure 3 CGI-S and CGI-I scores over the course of Studies (A) 246,16 (B) 247,23 (C) 248,24 (D) 283,25–27 and (E) 291.28
Notes: (A) Kane JM, Sanchez R, Perry PP, et al. Aripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled study. The Journal of Clinical Psychiatry. 73:617–624, 2012. Copyright 2012, Physicians Postgraduate Press. Reprinted by permission.16 (B) Copyright © 2014. Reproduced from Fleischhacker WW, Sanchez R, Perry PP, et al. Aripiprazole once-monthly for treatment of schizophrenia: double-blind, randomised, non-inferiority study. Br J Psychiatry. 2014;205:135–144.23 (C) Reproduced from Peters-Strickland T, Baker RA, McQuade RD, et al.Aripiprazole once-monthly 400 mg for long-term maintenance treatment of schizophrenia: a 52-week open-label study. NPJ Schizophr. 2015;1:15039. Creative Commons license and disclaimer available from: |
In the double-blind maintenance phase, significant differences between the AOM 400 and placebo treatment groups in change from baseline LS mean scores were achieved by Week 2 for PANSS total score and positive subscale score and by Week 4 for PANSS negative subscale score and CGI-S score (Figures 2 and 3). These differences were maintained throughout the 52-week double-blind treatment phase. Significant differences in mean (SD) changes from baseline in CGI-I score were seen at Week 4 and were maintained throughout double-blind treatment. At Week 52, the LS mean (SE) change from baseline in PANSS total score for the AOM 400 group was 1.43 (0.756) vs 11.55 (1.066) for the placebo group (Difference [95% CI]: –10.11 [–12.68, –7.54]; P<0.0001). The LS mean (SE) change from baseline in PANSS positive score at Week 52 for the AOM 400 group was 0.44 (0.265) vs 4.25 (0.374) for the placebo group (Difference [95% CI]: –3.82 [–4.72, –2.91]; P<0.0001). The LS mean (SE) change from baseline in PANSS negative score at Week 52 for the AOM 400 group was 0.19 (0.201) vs 1.55 (0.284) for the placebo group (Difference [95% CI]: –1.36 [–2.04, –0.67]; P=0.0001). At Week 52, the LS mean (SE) change from baseline in CGI-S score was 0.14 (0.051) for the AOM 400 group vs 0.66 (0.073) for the placebo group (Difference [95% CI] –0.52 [–0.70–0.35]; P<0.0001).
AOM 400 resulted in similar efficacy in adult patients aged ≤35 years and >35 years. At Week 52 of the double-blind maintenance phase, adjusted mean changes from baseline in PANSS total score, PANSS positive and negative subscale scores, and CGI-S and CGI-I scores were significantly greater vs placebo for both age cohorts. Significant improvements vs placebo in PANSS total score and PANSS positive subscale score occurred early in treatment (by Week 2–4) for both age cohorts. There was a difference between age cohorts in how early changes from baseline reached significance vs placebo for both PANSS negative subscale score and CGI-S score. Significance was achieved earlier (Week 4–6) for patients aged >35 years vs adult patients aged ≤35 years (Week 26 for PANSS negative subscale and Week 14 and 18 for CGI-S).
Study 247
In Study 247, similar to Study 246, OA resulted in decreases (improvements) relative to baseline in PANSS total score, positive and negative subscale scores, and CGI-S score during the oral stabilization phase (Figures 2 and 3). Mean (SD) PANSS total score decreased from 62.64 (13.74) at baseline to 57.05 (12.75) at Week 28 of the OA stabilization phase.
During the double-blind maintenance phase, AOM 400 resulted in further small improvements from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score at every timepoint (Figures 2 and 3). Changes from baseline in LS mean PANSS total score, positive and negative subscale scores, and CGI-S score for the AOM 400 group were either comparable or significantly greater at all timepoints vs the OA 10–30 mg group. Compared with the subtherapeutic dose of AOM (50/25 mg), AOM 400 resulted in significantly greater improvements in PANSS total score by Week 4 and every timepoint thereafter. AOM 400 resulted in numerically greater LS mean changes from baseline in PANSS negative subscale scores vs AOM 50/25 mg at all timepoints and significantly greater LS mean changes from baseline vs AOM 50/25 mg in PANSS positive subscale score from Week 12 through 38 and in CGI-S score from Week 10 through Week 38. Mean CGI-I score for the AOM 400 group was significantly lower vs the OA 10–30 mg group from Week 10 through 38 and vs the AOM 50/25 mg group from Week 8 through Week 38.
At Week 38, the LS mean (SE) change from baseline in PANSS total score for the AOM 400 group was –1.66 (0.718) vs 0.58 (0.714) for the OA 10–30 mg group (Difference [95% CI]: –2.24 [–4.23, –0.25]; P=0.0272) and 3.08 (1.017) for the AOM 25/50 mg group (Difference [95% CI]: –4.74 [–7.19, –2.30]; P=0.0002). The LS mean (SE) change from baseline in PANSS positive score at Week 38 for the AOM 400 group was –0.12 (0.249) vs 0.52 (0.247) for the OA 10–30 mg group (Difference [95% CI]: –0.64 [–1.33, 0.05]; P=0.0675) and 1.46 (0.352) for the AOM 25/50 mg group (Difference [95% CI]: –1.58 [–2.43, –0.73]; P=0.0003). The LS mean (SE) change from baseline in PANSS positive score at Week 38 for the AOM 400 group was –0.74 (0.220) vs –0.15 (0.219) for the OA 10–30 mg group (Difference [95% CI]: –0.59 [–1.20, 0.02]; P=NS) and –0.19 (0.312) for the AOM 25/50 mg group (Difference [95% CI]: –0.56 [–1.31, 0.19]; P=NS). At Week 38, the LS mean (SE) change from baseline in CGI-S score was –0.13 (0.049) for the AOM 400 group vs 0.05 (0.049) for the OA 10–30 mg group (Difference [95% CI] –0.17 [–0.31, –0.04]; P=0.0123) and 0.23 (0.070) for the AOM 25/50 mg group (Difference [95% CI]: –0.36 [–0.52, –0.19]; P<0.0001).
AOM 400 showed similar efficacy in adult patients aged ≤35 years and >35 years, resulting in numerically and, in some instances, statistically greater improvements from baseline across both age cohorts vs OA 10–30 mg and AOM 50/25 mg in PANSS total score, PANSS positive and negative subscale scores, and CGI-S and CGI-I scores. At Week 38, among patients aged >35 years, mean changes from baseline in PANSS total score and PANSS positive subscale score for AOM 400 were significantly greater vs both comparison groups. At Week 38, AOM 400 resulted in a significantly greater mean (SD) improvement from baseline in CGI-S score vs OA 10–30 mg (–0.16 [0.097] vs 0.11 [0.089]; P=0.04) among adult patients aged ≤35 years and a significantly greater mean (SD) improvement from baseline in CGI-S score vs AOM 50/25 mg (–0.12 [0.057] vs 0.27 [0.084]; P<0.0001) among patients aged >35 years. Significantly greater improvements in CGI-I at Week 38 occurred for AOM 400 vs both comparison groups across both age cohorts.
Study 248
In Study 248, during the oral stabilization phase, OA resulted in improvements from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score (Figures 2 and 3). Mean (SD) PANSS total score decreased from 57.21 (15.29) to 54.19 (12.79) (mean [SD] change from baseline –3.02 [8.14]). These improvements were maintained and extended during the 52-week, open-label maintenance phase of the study. For the total efficacy sample, AOM 400 resulted in further small decreases from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score at all timepoints during the study. Mean (SD) PANSS total score decreased from 54.26 (12.86) at baseline to 52.53 (13.99) at Week 52 (mean [SD] change from baseline –1.74 [9.53]). Mean (SD) PANSS positive subscale score decreased from 11.77 (3.72) at baseline to 11.29 (4.04) at Week 52 (mean [SD] change from baseline –0.49 [3.22]). Mean (SD) PANSS negative subscale score decreased from 15.79 (4.81) at baseline to 15.39 (4.88) at Week 52 (mean [SD] change from baseline –0.40 [3.03]). Mean (SD) CGI-S score decreased from 2.98 (0.85) at baseline to 2.84 (0.96) at Week 52 (mean [SD] change from baseline –0.13 [0.66]). Mean (SD) CGI-I score decreased from 3.47 (0.82) at baseline to 3.38 (1.07) at Week 52.
Improvements from baseline in mean PANSS total score, positive and negative subscale scores, and CGI-S score were seen for each of the study source groups, Study 246 patients, Study 247 patients, and de novo patients. Each of these groups had small decreases from baseline in scores at Week 52 for each measure, with the exception of de novo patients, who had a small increase from baseline in mean PANSS negative subscale score at Week 52.
Of the 937 patients who received AOM 400 for ≥6 months, 484/937 (51.7%) met sustained remission criteria, 236/414 (57%) from Study 246, 217/416 (52.2%) from Study 247, and 31/107 (29%) of de novo patients. There was an increase in the percentage of patients who met remission criteria from baseline through Week 52 for the total sample and by enrollment source. Both positive and negative PANSS subscale scores showed small but continued improvements in these stabilized patients (mean [SD] change from baseline to Week 52: –0.5 [3.4] and –0.5 [3.2] for positive and negative subscale scores, respectively).
AOM 400 was effective in improvement in PANSS total score, PANSS positive and negative subscale scores, and CGI-S score for both age cohorts, with numerically greater improvements seen in the adult patient group aged ≤35 years vs >35 years across all endpoints. At Week 54, AOM 400 resulted in numerically greater mean (SD) changes from baseline among adult patients aged ≤35 years vs >35 years in PANSS total score (–2.61 [10.70] vs –1.30 [9.95]), PANSS positive subscale score (–0.72 [3.50] vs –0.38 [3.32]), PANSS negative subscale score (–0.77 [3.23] vs –0.30 [3.18]), and CGI-S score (–0.23 [0.74] vs –0.09 [0.68]).
Study 283
In Study 283, AOM 400 resulted in significant decreases from baseline in mean PANSS total score, positive and negative subscale scores, and CGI-S score as early as Week 4 for all measures (Figures 2 and 3). These changes from baseline were maintained through Week 24 of the study. Mean (SD) PANSS total score changed from 75.0 (18.3) at baseline to 66.4 (17.2) at Week 24 (mean [SD] change from baseline: –8.4 [17.7]; P<0.0001). Mean (SD) PANSS positive subscale score changed from 18.3 (5.3) at baseline to 15.3 (5.1) at Week 24 (mean [SD] change from baseline: –3.0 [5.4]; P<0.0001). Mean (SD) PANSS negative subscale score changed from 20.0 (6.1) at baseline to 18.2 (5.5) at Week 24 (mean [SD] change from baseline: –1.6 [5.8]; P<0.0001). Mean (SD) CGI-S score changed from 3.7 (0.8) at baseline to 3.2 (1.0) at Week 24 (mean [SD] change from baseline: –0.5 (1.0)]; P<0.0001). Mean (SD) CGI-I score decreased from 2.9 (0.9) at Week 4 to 2.5 (1.0) at Week 24.
For the overall efficacy sample and among patients who received treatment for at least 3 months, AOM 400 resulted in significant improvements (decreases) from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score across both age cohorts (adult patients aged ≤35 years and >35 years), with numerically larger treatment effects seen among patients aged >35 years across all measures. Improvements from baseline across all measures occurred early in treatment (Week 4) for both age cohorts and were maintained throughout the study.
Study 291
In Study 291, AOM 400 resulted in significantly greater decreases in mean change from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score vs placebo at all post-baseline timepoints (Figures 2 and 3). LS mean (SE) change from baseline in PANSS total score at Week 10 (the primary efficacy endpoint) was –26.8 (1.6) for AOM 400 vs –11.7 (1.6) for placebo (Difference [95% CI]: –15.1 [–19.4,–10.8]; P<0.0001). Week 12 LS mean (SE) change from baseline in PANSS positive subscale score was –9.9 (0.6) for AOM 400 vs –4.8 (0.6) for placebo (Difference [95% CI]: –5.1 [–6.7,–3.6]; P<0.0001). Week 12 LS mean (SE) change from baseline in PANSS negative subscale score was –4.7 (0.4) for AOM 400 vs –2.2 (0.5) for placebo (Difference [95% CI]: –2.5 [–3.7,–1.3]; P<0.0001). Week 12 LS mean (SE) change from baseline in CGI-S score was –1.4 (0.1) for AOM 400 vs –0.6 (0.1) for placebo (Difference [95% CI]: –0.8 [–1.0,–0.5]; P<0.0001). Week 12 mean (SD) CGI-I score was 2.6 (1.2) for AOM 400 vs 3.7 (1.3) for placebo (P<0.0001).
AOM 400 showed similar efficacy in improvement in PANSS total score, PANSS positive subscale score, and CGI-S score in adult patients aged ≤35 years and >35 years. AOM 400 resulted in significant improvements vs placebo in changes from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score early in treatment (Week 1 for PANSS total score, PANSS positive and negative subscale scores, and CGI-S score for adult patients aged ≤35 years; Week 2 for PANSS total score, PANSS positive subscale score, and Week 1 for PANSS negative subscale score and CGI-S score in patients aged >35 years) and maintained these differences throughout the study. A numerically larger treatment effect was observed for AOM 400 on the PANSS negative subscale score among adult patients aged ≤35 years vs those aged >35 years.
Safety
Safety results, including rates of treatment-emergent adverse events, from Studies 246, 247, 248, 283, and 291, have been detailed previously.16,23–28 Briefly, in Study 246, the most common treatment-emergent AEs (occurring in ≥5% of the patients treated with AOM 400 and greater than placebo) during the double-blind stage were insomnia (10%), headache (5.9%), and tremor (5.9%).16 In Study 247, insomnia, akathisia, headache, and weight increase/decrease were reported by 9–12% of the patients treated with AOM 400 during the randomized phase.23 In both of these registration trials, most treatment-emergent AEs were mild to moderate in severity and rates of discontinuation due to AEs were low.16,23 Additionally, AOM 400 demonstrated a low risk of inducing prolactin elevations, weight gain, metabolic disturbances, or sedation, and did not show any clinically relevant changes in objective measures of extrapyramidal symptoms.16,23 In the long-term open-label extension study (Study 248), the safety and tolerability profile of AOM 400 was similar to that observed in the lead-in studies, with no new safety signals arising during long-term treatment.24
Discussion
Findings from the analyses presented here support and expand previously reported efficacy findings from studies of AOM 400 in the acute treatment and maintenance therapy settings, specifically including analyses of adult patients 35 years of age and younger. Our analyses focused on symptom stability as measured by PANSS total score, PANSS positive and negative subscale scores, and CSI-S and CGI-I scores, as well as a composite of selected PANSS positive and negative symptom scores used to define sustained remission. Both PANSS and CGI scores played an important role in defining the occurrence or risk of relapse/exacerbation for the primary endpoints for both pivotal trials of AOM 400 as maintenance treatment (Studies 246 and 247). In the 52-week, placebo-controlled trial (Study 246), time to impending relapse/exacerbation of psychotic symptoms for AOM 400 was significantly delayed vs placebo, resulting in early termination of the study.16 In the 38-week, active-controlled trial (Study 247), Kaplan–Meier estimated the rate of impending relapse (up to Week 26) was significantly lower for AOM 400 vs AOM 50 mg and non-inferior to aripiprazole oral daily treatment.23 Efficacy results from Study 248, the 52-week, open-label extension of Studies 246 and 247, demonstrated further long-term symptom stability with 95% of the patients who were stable at baseline remaining stable through Week 52.24
Our analyses of Studies 246 and 247 demonstrated that symptom improvements achieved during stabilization phases in both studies were robustly maintained throughout the course of each study (52 weeks for Study 246 and 38 weeks for Study 247), reflecting long-term stability of symptom improvements. Our efficacy analysis stratified by age (adult patients aged ≤35 years and >35 years) showed that symptom improvements were consistent across age groups. Results from Study 248 extend our understanding of the long-term effect of AOM 400 in maintaining symptom stability. For the total efficacy sample, as well as across the three source groups for the study (patients from Studies 246 and 247 and de novo patients), AOM 400 not only maintained the improvements achieved during OA stabilization, but resulted in further small improvements from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score over the course of the 52-week study, regardless of patient age. Numerically greater improvements were seen in adults aged ≤35 years vs >35 years, suggesting a somewhat larger treatment effect for AOM 400 among younger patients. Further study in a randomized, controlled setting with larger sample sizes is required to confirm possible age-related differences in effect. Using stringent remission criteria based on a composite of PANSS negative and positive symptom scores, more than half of patients who remained in the study for ≥6 months achieved sustained remission.
Study 283, a mirror-image, community-based, naturalistic study conducted in patients who switched from oral antipsychotic treatment to AOM 400, provided a real-world perspective on maintenance of symptom stability. AOM 400 resulted in significant decreases from baseline in PANSS total score, positive and negative subscale scores, and CGI-S score early (Week 4 for all measures) and maintained these changes through Week 24. Efficacy analysis stratified by age (adult patients aged ≤35 years and >35 years) showed that symptom improvements were consistent across a range of ages. Symptom improvements and stability seen during the trial translated into significantly reduced rates of hospitalization when compared with retrospective hospitalization data.25,26
Our analysis of Study 291 provides a perspective on symptom control in the acute setting, among patients who were experiencing an acute psychotic episode. AOM 400 was significantly more effective vs placebo in improving PANSS total score, positive and negative subscale scores, and CGI-S score from baseline, with significant differences achieved at every post-baseline timepoint. The present results are confirmed by an analysis showing a significant benefit of AOM 400 across the range of PANSS Marder factors.32 Our analysis of efficacy results in Study 291 stratified by patient age (adults aged ≤35 years or >35 years) provides some insights on the effect of age on the pattern of symptom improvement after initiation of AOM 400. Comparable effects were seen with adult patients aged ≤35 years and those aged >35 years in terms of mean change from baseline in PANSS total score and positive subscale score. However, numerically larger treatment effects were observed on the PANSS negative subscale in adult patients aged ≤35 years vs those aged >35 years, raising the question of whether patients earlier in the course of illness may be more sensitive to improvements in negative symptoms. Further study is necessary for larger sample sizes adequately powered to detect age-related differences in symptoms in patients with schizophrenia. The present results do, however, underscore the importance of protecting patients from deterioration of clinical symptoms, especially where younger patients may have more to lose in terms of functioning. Negative symptoms are often associated with long-term functional deficits,33 including the potential to negatively affect self-esteem.34
Safety and tolerability results from analyses reported here were consistent with the established AOM 400 safety/tolerability profile.
The results presented here provide an overview of the efficacy of AOM 400 with respect to symptom stability in the acute treatment and maintenance therapy settings across five separate studies. While our analyses provide a valuable view of the efficacy of AOM 400 across diverse patient populations and treatment settings, this report is limited in interpretations that can be made across studies due to differences in the design and objectives of the studies included. Additionally, differences in the patient populations studied compared to real-life clinical populations may limit the generalizability of our findings. The population in the pivotal relapse-prevention trials (Studies 246 and 247) were limited to patients with chronic schizophrenia of relatively mild severity who had been stabilized with on AOM 400 or OA, respectively; patients with psychiatric comorbidities were excluded.16,23 The long-term extension study (Study 248) of AOM 400 maintenance treatment,24 as well as the mirror-image, naturalistic study (Study 283),25–27 was of open-label design and lacked a parallel control group. Limitations of the study of AOM 400 in the acute treatment of schizophrenia (Study 291) included the exclusion of patients with comorbid DSM-IV-TR Axis I diagnoses or substance abuse and the intense weekly follow-up.28 In general, patients in a clinical trial who have regular symptom assessment are likely to be more adherent than patients in real-world clinical practice. Lastly, results of the effect of AOM 400 on symptomatic stability in subgroups stratified by age (≤35 years or >35 years) were from post hoc analyses; age stratification was not planned a priori.
Conclusion
Results from analyses of data from studies in both the acute treatment and maintenance settings demonstrate the efficacy of AOM 400 in rapid stabilization of symptoms and long-term maintenance of symptom stability. The efficacy of AOM 400 is generally consistent across patient age groups, with a somewhat greater treatment effect in negative symptoms for younger adult patients (≤35 years) in the acute treatment setting. Safety/tolerability data are consistent with previous reports.
Acknowledgments
Editorial support for this manuscript was provided by BioScience Communications (New York City, NY, USA), with funding from Otsuka Pharmaceutical Development & Commercialization, Inc.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. RAB was responsible for the clinical management of studies 246, 247, 248, 283, and 291; CZ was responsible for this manuscript’s data analysis; JJM, PS, and RAB were responsible for this manuscript’s data interpretation.
Disclosure
JJM, CZ, and RAB are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. PS is an employee of H. Lundbeck A/S. The authors report no other conflicts of interest in this work.
References
1. Lieberman JA, Perkins D, Belger A, et al. The early stages of schizophrenia: speculations on pathogenesis, pathophysiology, and therapeutic approaches. Biol Psychiatry. 2001;50:884–897. doi:10.1016/S0006-3223(01)01303-8
2. Kane JM. Treatment strategies to prevent relapse and encourage remission. J Clin Psychiatry. 2007;68(Suppl 14):27–30.
3. Wyatt RJ. Neuroleptics and the natural course of schizophrenia. Schizophr Bull. 1991;17:325–351. doi:10.1093/schbul/17.2.325
4. Emsley R, Chiliza B, Asmal L. The evidence for illness progression after relapse in schizophrenia. Schizophr Res. 2013;148:117–121. doi:10.1016/j.schres.2013.05.016
5. Ayuso-Gutierrez JL, del Rio Vega JM. Factors influencing relapse in the long-term course of schizophrenia. Schizophr Res. 1997;28:199–206. doi:10.1016/S0920-9964(97)00131-X
6. Emsley R, Nuamah I, Hough D, Gopal S. Treatment response after relapse in a placebo-controlled maintenance trial in schizophrenia. Schizophr Res. 2012;138:29–34. doi:10.1016/j.schres.2012.02.030
7. Lieberman JA, Alvir JM, Koreen A, et al. Psychobiologic correlates of treatment response in schizophrenia. Neuropsychopharmacology. 1996;14(3 Suppl):13S–21S. doi:10.1016/0893-133X(95)00200-W
8. Lindenmayer JP, Liu-Seifert H, Kulkarni PM, et al. Medication nonadherence and treatment outcome in patients with schizophrenia or schizoaffective disorder with suboptimal prior response. J Clin Psychiatry. 2009;70:990–996. doi: 10.4088/JCP.08m04221.
9. Valenstein M, Ganoczy D, McCarthy JF, Myra Kim H, Lee TA, Blow FC. Antipsychotic adherence over time among patients receiving treatment for schizophrenia: a retrospective review. J Clin Psychiatry. 2006;67:1542–1550. doi:10.4088/JCP.v67n1008
10. Kane JM. Review of treatments that can ameliorate nonadherence in patients with schizophrenia. J Clin Psychiatry. 2006;67(Suppl 5):9–14.
11. Nasrallah HA. The case for long-acting antipsychotic agents in the post-CATIE era. Acta Psychiatr Scand. 2007;115:260–267. doi:10.1111/j.1600-0447.2006.00982.x
12. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry. 1999;56:241–247.
13. Kane JM, Leucht S, Carpenter D, Docherty JP. Expert consensus panel for optimizing pharmacologic treatment of psychotic D. The expert consensus guideline series. Optimizing pharmacologic treatment of psychotic disorders. Introduction: methods, commentary, and summary. J Clin Psychiatry. 2003;64(Suppl 12):5–19.
14. Burris KD, Molski TF, Xu C, et al. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther. 2002;302:381–389.
15. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology. 2003;28:1400–1411. doi:10.1038/sj.npp.1300203
16. Kane JM, Sanchez R, Perry PP, et al. Aripiprazole intramuscular depot as maintenance treatment in patients with schizophrenia: a 52-week, multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2012;73:617–624. doi:10.4088/JCP.11m07530
17.
18. Orsolini L, Tomasetti C, Valchera A, et al. An update of safety of clinically used atypical antipsychotics. Expert Opin Drug Saf. 2016;15:1329–1347. doi:10.1080/14740338.2016.1201475
19. Stahl SM. Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications.
20. Lieberman JA. Dopamine partial agonists: a new class of antipsychotic. CNS Drugs. 2004;18:251–267. doi:10.2165/00023210-200418040-00005
21. Bishara D. Once-monthly paliperidone injection for the treatment of schizophrenia. Neuropsychiatr Dis Treat. 2010;6:561–572. doi:10.2147/NDT.S8505
22. De Berardis D, Fornaro M, Serroni N, et al. Treatment of antipsychotic-induced hyperprolactinemia: an update on the role of the dopaminergic receptors D2 partial agonist aripiprazole. Recent Pat Endocr Metab Immune Drug Discov. 2014;8:30–37. doi:10.2174/1872214807666131229125700
23. Fleischhacker WW, Sanchez R, Perry PP, et al. Aripiprazole once-monthly for treatment of schizophrenia: double-blind, randomised, non-inferiority study. Br J Psychiatry. 2014;205:135–144. doi:10.1192/bjp.bp.113.134213
24. Peters-Strickland T, Baker RA, McQuade RD, et al. Aripiprazole once-monthly 400 mg for long-term maintenance treatment of schizophrenia: a 52-week open-label study. NPJ Schizophr. 2015;1:15039. doi:10.1038/npjschz.2015.39
25. Kane JM, Sanchez R, Zhao J, et al. Hospitalisation rates in patients switched from oral anti-psychotics to aripiprazole once-monthly for the management of schizophrenia. J Med Econ. 2013;16:917–925. doi:10.3111/13696998.2013.804411
26. Kane JM, Zhao C, Johnson BR, et al. Hospitalization rates in patients switched from oral anti-psychotics to aripiprazole once-monthly: final efficacy analysis. J Med Econ. 2015;18:145–154. doi:10.3111/13696998.2014.979936
27. Peters-Strickland T, Zhao C, Perry PP, et al. Effects of aripiprazole once-monthly on symptoms of schizophrenia in patients switched from oral antipsychotics. CNS Spectr. 2016;21:460–465. doi:10.1017/S1092852916000365
28. Kane JM, Peters-Strickland T, Baker RA, et al. Aripiprazole once-monthly in the acute treatment of schizophrenia: findings from a 12-week, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2014;75:1254–1260. doi:10.4088/JCP.14m09168
29. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13:261–276. doi:10.1093/schbul/13.2.261
30. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4:28–37.
31. Andreasen NC, Carpenter WT
32. Ismail Z, Peters-Strickland T, Miguelez M, et al. Aripiprazole once-monthly in the treatment of acute psychotic episodes in schizophrenia: post hoc analysis of positive and negative syndrome scale marder factor scores. J Clin Psychopharmacol. 2017;37:347–350. doi:10.1097/JCP.0000000000000710
33. Arango C, Buchanan RW, Kirkpatrick B, Carpenter WT. The deficit syndrome in schizophrenia: implications for the treatment of negative symptoms. Eur Psychiatry. 2004;19:21–26. doi:10.1016/j.eurpsy.2003.10.004
34. Hofer A, Kemmler G, Eder U, Edlinger M, Hummer M, Fleischhacker WW. Quality of life in schizophrenia: the impact of psychopathology, attitude toward medication, and side effects. J Clin Psychiatry. 2004;65:932–939. doi:10.4088/JCP.v65n0709
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.