")
Back to Journals » Clinical Ophthalmology » Volume 17
Symptomatic Dry Eye Disease and Associated Factors Among Adult Diabetic Patients in Adare General Hospital, Hawassa City, Southern Ethiopia, 2023
Authors Bekele AG, Alimaw YA, Tegegn MT
Received 3 August 2023
Accepted for publication 4 November 2023
Published 13 November 2023 Volume 2023:17 Pages 3429—3442
DOI https://doi.org/10.2147/OPTH.S433679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John B Miller
Asnake Gezahegn Bekele,1 Yezinash Addis Alimaw,2 Melkamu Temeselew Tegegn2
1Department of Ophthalmology, Madda Walabu University Goba Referral Hospital, Goba City, Ethiopia; 2Department of Optometry, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Melkamu Temeselew Tegegn, Department of Optometry, College of Medicine and Health Sciences, University of Gondar, PO Box: 196, Gondar, Ethiopia, Email [email protected]
Introduction: Symptomatic dry eye disease is a multifactorial ocular surface condition caused by disruption of the precorneal tear film and is a common clinical finding in diabetic patients. However, there was no study on the prevalence and associated factors of symptomatic dry eye disease among diabetic patients in Ethiopia or in the study area.
Purpose: This study aimed to investigate the prevalence and associated factors of symptomatic dry eye disease among adult diabetic patients in Adare General Hospital, Hawassa City, Southern Ethiopia, in 2023.
Methods: A hospital-based cross-sectional study design was conducted on 493 adult diabetic patients who were selected using systematic random sampling, from April 23 to June 8, 2023. Data were collected through a face-to-face interview using an ocular surface disease index questionnaire. Binary logistic regression was performed to identify factors potentially associated with symptomatic dry eye disease. Variable with a P value of < 0.05 was considered statistically significant.
Results: A total of 488 subjects participated in this study with a response rate of 99%. The prevalence of symptomatic dry eye disease was 34.8% (95% CI = 30.6– 39.1). College and university educational status (AOR = 5.88, 95% CI = 2.25– 15.38), government employed (AOR = 2.22, 95% CI = 1.05– 4.68), use of visual display unit > 5 hours (AOR = 4.41, 95% CI = 1.51– 12.87), duration of diabetes ≥ 11 years (AOR = 3.57, 95% CI = 1.28– 9.90), poor glycemic control (AOR = 2.13, 95% CI = 1.21– 3.75), allergic conjunctivitis (AOR = 1.99, 95% CI = 1.12– 3.54), and debris in the tear film (AOR = 3.63, 95% CI = 1.53– 8.61) were positively associated with symptomatic dry eye disease.
Conclusion: The study revealed a high prevalence of symptomatic dry eye disease. Higher educational status, government employed, use of visual display unit, longer duration of diabetes, poor glycemic control, allergic conjunctivitis, and tear film debris were significantly associated with symptomatic dry eye disease. Breaks in screen use, good glycemic control, and treatment of ocular morbidities such as allergic conjunctivitis and debris in the tear film were recommended for all diabetic patients.
Keywords: symptomatic dry eye disease, Hawassa City, diabetic patients, Southern Ethiopia
Introduction
Dry eye disease (DED) is a multifactorial ocular surface disease due to tear film instability and hyperosmolarity, ocular surface inflammation, damage, and neurosensory abnormalities.1 DED is classified as aqueous-deficient dry eye, when dryness is caused by decreased tear production, and evaporative dry eye, which results from increased evaporation of the precorneal tear film; however, clinically, mixed forms of dry eye are very common.2
Symptomatic dry eye disease (SDED) is a severe form of dry eye that is characterized by common symptoms such as dryness, ocular pain, burning sensation, ocular fatigue, grittiness, photophobia, soreness, irritation, tearing, and visual disturbances or limitations.3
Diabetes mellitus (DM) is a global health problem that causes ocular surface disorder (dry eye disease).4 DM-associated dry eye disease is caused by altered enzyme metabolism and decreased mucin secretion, dysfunction of the lacrimal gland and tear fluid due to diabetic neuropathy, and dysfunction of the meibomian glands, which leads to tear film instability by reducing the quantity and quality of the lipid layer of the precorneal tear film.5
Evidence has shown that the increasing number of diabetic patients worldwide is one of the contributing factors to increase the prevalence of symptomatic dry eye,6 and the prevalence of dry eye disease in diabetics ranges from 20.6% to 54.3%.7–10 In Ethiopia, the prevalence of symptomatic dry eye was 50.5% on postgraduate students in University of Gondar,11 49.5% on undergraduate students in Hawassa University12 and 43% on Glaucoma patients in Menelik II tertiary hospital.13 Although the prevalence of diabetes mellitus in Ethiopia was 6.5%,14 there was no study that showed the prevalence of symptomatic dry eye among diabetic patients.
Reports showed that older age,5 female sex,6 poor glycemic control,15–21 long duration of diabetes,5,6,15,20–23 peripheral diabetic neuropathy,5,24 use of artificial tears,25 diabetic retinopathy,15,23,24,26,27 and a history of cataract surgery5 were significantly associated with dry eye disease in diabetic patients.
Early untreated DED in diabetics can be complicated by persistent corneal epithelial defects, corneal erosions, and microbial or trophic corneal ulcers, leading to ocular discomfort and visual disturbance or limitation.23 People with dry eye are less efficient in daily life and lose their productivity at work because they suffer from severe eye discomfort and visual disturbances, which affects the patient’s overall quality of life.28,29
Although dry eye disease is one of the most common eye diseases worldwide and is common in diabetic patients in clinical practice in Ethiopia, the actual extent and associated factors of DED in Ethiopia and the study area are not known. Since the Adare General Hospital in Hawassa City is one of the largest diabetic centers in Southern Ethiopia with an integrated eye care service, providing up-to-date information is important for formulating health policies and allocating adequate resources to address this problem in the study area as well in the country (Ethiopia). Therefore, the aim of this study was to determine the prevalence and associated factors of symptomatic dry eye disease among adult diabetic patients in Adare General Hospital, Hawassa City, Southern Ethiopia in 2023.
Methods and Materials
Study Design, Setting, and Period
A hospital-based cross-sectional study design was conducted at Adare General Hospital from April 23 to June 8, 2023. Adare General Hospital is located in Hawassa City, the capital of Sidama Regional State, which is found 275 km away from Addis Ababa. According to the hospital’s planning and information office, Adare General Hospital provides both preventive and curative health care treatments, including eye care, to nearly three million people. With 1 ophthalmologist, 5 optometrists, and 1 ophthalmic nurse, the Department of Ophthalmology at Adare General Hospital provides comprehensive eye care to the surrounding community. Adare General Hospital is also providing care for at least 600 diabetic patients per month over five working days. Clinical care for diabetic patients has been provided by internists, general practitioners, and nurses.
Study Population and Eligible Criteria
All adult patients aged ≥18 years with type I or type II diabetes who were receiving diabetologic care at Adare General Hospital during the survey period. However, adult diabetic patients who were unable to answer the questionnaire because of speech or mental health problem, patients who were admitted to the inpatient unit seriously ill, patients with media opacities such as corneal and vitreous opacities, and patients with a shallow anterior chamber angle, uveitis, and keratitis were excluded.
Sample Size Determination
Sample Size Determination for Objective One
The sample size was determined using a single population proportion formula that  is with the following assumptions (n = Sample size, Z = the value of z statistic at 95% confidence level = 1.96, P = the expected proportion of symptomatic dry eye disease was 49.8%, which was taken from a similar study in Kenya,30 and d – maximum allowable error (5%). The calculated sample size was 384.
is with the following assumptions (n = Sample size, Z = the value of z statistic at 95% confidence level = 1.96, P = the expected proportion of symptomatic dry eye disease was 49.8%, which was taken from a similar study in Kenya,30 and d – maximum allowable error (5%). The calculated sample size was 384.
Sample Size Determination for Objective Two
Female sex was the consistent factor for symptomatic dry eye disease31 used to calculate the sample size for the second objective using the software EPI INFO version 7, considering a confidence level of 95%, power of 80%, a ratio of unexposed to exposed patients of 1.4, an odds ratio of 1.80, and the proportion of case in exposed and unexposed groups were 72.5% and 59.3%, respectively. So that the computer-generated sample size was 448. The sample size determined for the second objective was chosen because it was large and sufficient to meet both objectives. Adding a non-response rate of 10%, the final required sample size was 493.
Sampling Technique and Procedures
Study participants were selected using a systematic random sampling procedure with an interval of 2. To select the first study participant, a single number was drawn by a lottery method, and then continued with every Kth interval. An interval was calculated by dividing the expected number of diabetic patients who visited the diabetes clinic during the data collection period by the calculated sample size (K = N/n, N = 1024, n = 493).
Operational Definitions
Symptomatic dry eye: was defined as those participants who had a score of 13 and above points based on the OSDI questionnaire.32,33
Blood glucose control: was classified as good if the recorded current fasting blood glucose (FBS) level was less than 152 mg/dl and poor if the current FBS level was 152 mg/dl and above.34
Smokers: participants who had smoked at least 100 cigarettes during their lifetime and currently smoked either every day or every other day per week.35
Body Mass Index (BMI) (kg/m2): was classified based on the World Health Organization categorization and calculated as weight in kilograms divided by height in square meters (m2). A BMI of <18.5 was considered underweight, a BMI of 18.5–24.9 kg/m2 was considered normal, a BMI of 25–29.9 kg/m2 was considered overweight, and a BMI of ≥30 kg/m2 was considered obese.36
Visual impairment: was defined as a present visual acuity of less than 6/12 in the better eye based on 11th the International Classification of Diseases definition of visual impairment.37
Duration of diabetes: was categorized as 1–5, 6–10, and ≥11 years.21
Diabetic retinopathy: was diagnosed and classified based on the Early Treatment of Diabetic Retinopathy Study.38
Meibomian gland dysfunction: was diagnosed based on the presence of at least one of the following clinical findings: excessive and abnormal secretion of the meibomian glands, telangiectasia at the posterior lid margin, frothy discharge at the lid margin or in the inner Canthi area, and pouting or obstruction of the meibomian gland orifices.39
Allergic conjunctivitis: was diagnosed based on the following clinical findings: Itching, lacrimation, mucoid discharge, conjunctival hyperemia or papillary reaction, variable chemosis, and eyelid edema.39
Age: was categorized as 18–40, 40–49, 50–59, and ≥60 years.31
Data Collection Tools and Procedure
Data were collected by personal interview, review of medical records, and an eye examination. The personal interview, review of medical records, and measurement of height and weight of study participants were performed by two trained nurses, whereas the eye examination was performed by two experienced optometrists.
The nurses conducted a face-to-face interview using a pretested and structured questionnaire that included information on socio-demographic characteristics such as age, sex, marital status, residence, educational and occupational status, and monthly income; behavioral data such as cigarette smoking, use of visual display devices, sleep duration, and sunlight exposure, ocular history such as use of artificial tears, intravitreal injections, history of cataract surgery, history of eye examination, history of medication use in the form of eye drops and use of eyeglasses, systemic comorbidities such as asthma, sinusitis, antidepressant medications, and the Ocular Surface Disease Index (OSDI) questionnaire. The OSDI questionnaire contained 12 questions assessing dry eye disease symptoms. The response to each question was scored from 0 to 4, in which 0 represents none of the time, 1 some of the time, 2 half of the time, 3 most of the time, 4 all of the time.32,33 The reliability of the items was checked by calculating Cronbach’s alpha value (0.94). Clinical data such as type of diabetes, fasting blood glucose level, duration of DM, type of treatment, and systemic comorbidities such as hypertension, heart disease, dyslipidemia, diabetic neuropathy, vitamin A deficiency, dermatitis, arthritis, thyroid disease, Parkinson’s disease, and use of diuretics were recorded in the medical records of the study participants. Weight was measured with a balance-beam scale and height with a wall-mounted stadiometer, and participants appeared in their underwear and without shoes. After completion of the interview, all study participants underwent a comprehensive eye examination. The presenting visual acuity of the study participants was measured in each eye using a Snellen chart at a distance of 6 meters under good room lighting. A slit-lamp biomicroscope with a 90-diopter Volk lens was used to examine the anterior and posterior portions of the eyes with the pupil dilated with 1% tropicamide eye drops to obtain clinical data such as meibomian gland dysfunction, allergic conjunctivitis, debris in the tear film, diabetic retinopathy, panretinal photocoagulation, and vitrectomy.
Data Quality Control
At Hawassa University Comprehensive Specialized Hospital, 5% of the sample size was used to pretest a structured questionnaire in Amharic, which was used to control for data quality. Two nurses and optometrists who collected the data were trained in it and their work was supervised, which helped to maintain the quality of the data. In addition, the collected data were checked for completeness at the end of the day to ensure data quality.
Data Processing and Analysis
After checking the completeness and consistency of the data, data were entered into the Epidemiological Information (EPI INFO) 7 program and then exported to the Statistical Package for Social Sciences (SPSS) version 25 for analysis. Multicollinearity was checked using the variance inflation factor and tolerance for controlling the effects of confounding variables on final results. Proportions and summary statistics such as mean, median and standard deviation were calculated for the descriptive data. Bivariable binary logistic regression followed by a multivariable binary logistic regression was performed to identify possible factors associated with symptomatic dry eye disease. The strength of the association between dependent and independent variables was expressed by an adjusted odds ratio (AOR) with a 95% confidence interval (CI). The model fitness was ensured by the Hosmer and Lemeshow goodness of fit. A variable with a P value of less than 0.05 was considered statistically significant.
Ethical Consideration
This study adhered to the tenets of the Declaration of Helsinki. Ethical approval was obtained from the Ethical Review Committee of University of Gondar, College of Medicine and Health Sciences, School of Medicine. Besides, a formal permission letter was also obtained from the medical director of Adare General Hospital. After a full explanation of the purpose of the study, written informed consent was obtained from all study participants. All study participants were informed of their right to withdraw from the study at any time during the interview and eye examination. Confidentiality was ensured by avoiding any personal identifiers from the data collection tool. Finally, patients with sight-threatening diabetic eye complications were referred to an eye clinic for further examination and follow-up.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 488 participants were involved in this study, with a response rate of 99.0%. The median age of the participants was 56 years (IQR: 47–65). Of the 488 study participants, 260 (53.3%) were male, 293 (60.0%) were urban dwellers, and 289 (59.2%) had attended primary school or lower educational status (Table 1).
 |
Table 1 Socio-Demographic Characteristics of the Study Participants in Adare General Hospital, Hawassa City, South Ethiopia, 2023 (n = 488) |
Behavioral Factors and Past Ocular History of the Study Participants
Of all study participants, nearly three-quarters (73.8%) used a visual display unit for less than or equal to 2 hours per day, and 353 (72.3%) slept less than 8 hours per day. Nearly half (48.6%) of the participants had no history of eye examination. In addition, only 158 (32.4%) of the participants had a history of wearing spectacles (Table 2).
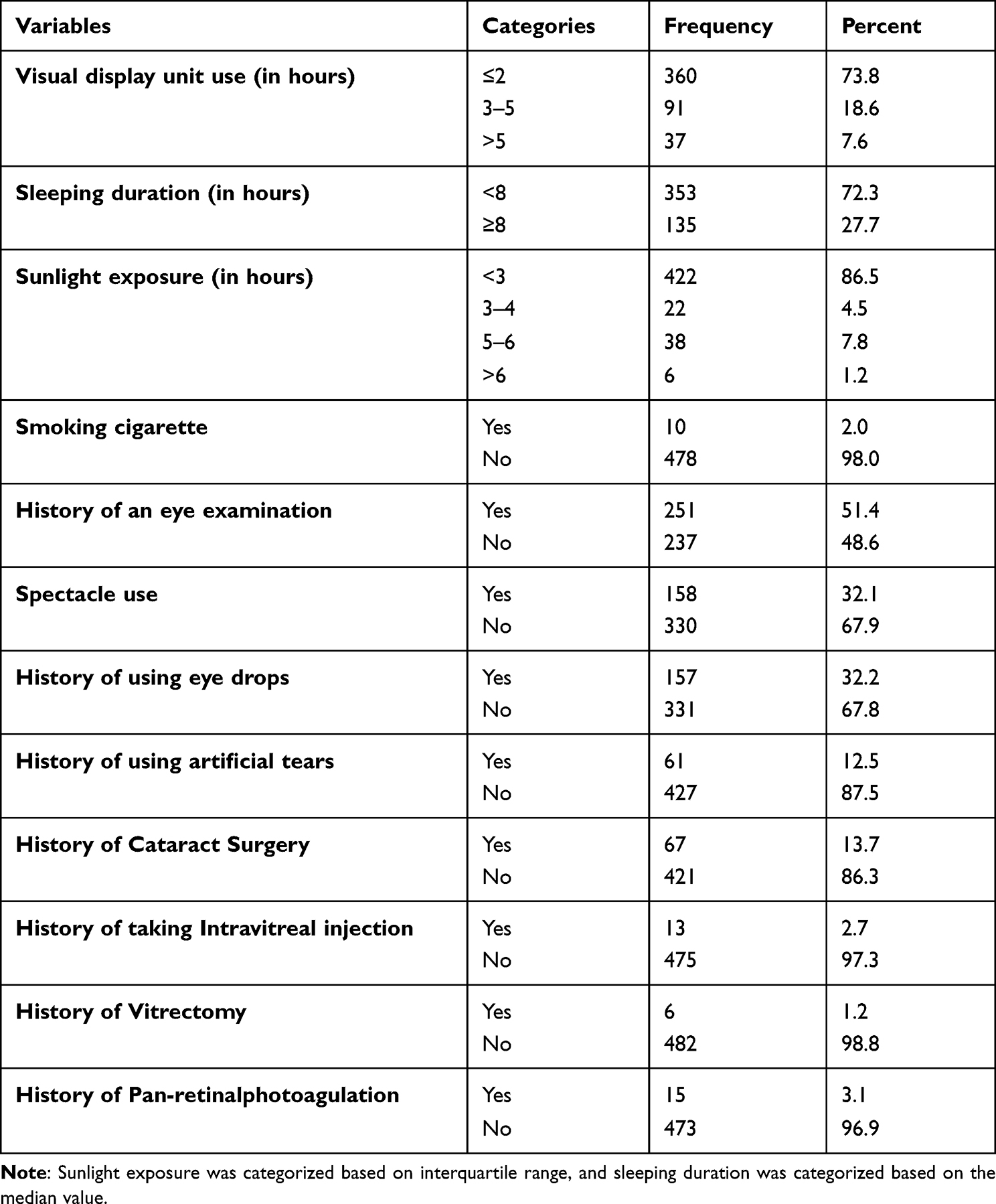 |
Table 2 Behavioral Factors and Past Ocular History of Diabetic Patients in Adare General Hospital, Hawassa City, South Ethiopia, 2023 (n = 488) |
Clinical Characteristics of the Study Participants
Of the total 488 participants, 352 (72.1%) had type II diabetes. The median duration of diabetes was 7 years (IQR: 4–10), and the median value for FBS was 150 mg/dl (IQR: 125–182 mg/dl). Of the 488 participants, 188 (38.5%) and 120 (24.6%) had allergic conjunctivitis and tear film debris, respectively (Table 3).
 |
Table 3 Clinical Data of Diabetic Patients in Adare General Hospital, Hawassa City, South Ethiopia, 2023 (n = 488) |
Systemic Co-Morbidities of the Study Participants
Out of 488 study participants, 146 (29.9%), 55 (11.3%), and 75 (15.4%) had a history of hypertension, dyslipidemia, and diabetic neuropathy, respectively (Table 4).
 |
Table 4 Systemic Comorbidities of Diabetic Patients in Adare General Hospital, Hawassa City, South Ethiopia, 2023 (n = 488) |
Prevalence of Symptomatic Dry Eye Disease
The prevalence of symptomatic dry eye disease in this study was 34.8% (95% CI = 30.6–39.1), of whom 63.5% were found in type 2 diabetic patients.
Factors Associated with Symptomatic Dry Eye Disease
Using bivariable binary logistic regression analysis, educational status, occupational status, monthly income, visual display unit (VDU) use, duration of sleep, history of eye examination, spectacle use, history of using eye drops, history of using artificial tears, arthritis, type of DM, duration of DM, glycemic control, treatment mode, dyslipidemia, heart disease, hypertension, diabetic neuropathy, history of cataract surgery, meibomian gland dysfunction, allergic conjunctivitis, debris in the tear film, diabetic retinopathy, and BMI were independently associated with symptomatic dry eye disease. However, in multivariable binary logistic regression analysis, educational status, occupational status, use of visual display unit, duration of DM, glycemic control, debris in the tear film, and allergic conjunctivitis were significantly associated with symptomatic dry eye disease.
Participants with an educational status of College and University were 5.88 times (AOR = 5.88, 95% CI = 2.25–15.38) more likely to have symptomatic dry eye disease than those with an educational status of primary school or lower. Participants who were government employed were 2.22 times (AOR = 2.22, 95% CI = 1.05–4.68) more likely to have symptomatic dry eye disease than those who were employed in the private business.
The odds of symptomatic dry eye disease were 4.41 times higher (AOR = 4.41, 95% CI = 1.51–12.87) in participants who used a VDU > 5 hours than in participants who used a VDU ≤ 2 hours. The odds of developing symptomatic dry eye disease were 3.57 times (AOR = 3.57, 95% CI = 1.28–9.90) higher in participants with diabetes duration since diagnosis ≥11 years than in participants with diabetes duration ≤5 years.
Participants with poor glycemic control were 2.13 times (AOR = 2.13,95% CI = 1.21–3.75) more likely to have symptomatic dry eye disease than participants with good glycemic control. Participants with allergic conjunctivitis were 1.99 times (AOR = 1.99,95% CI = 1.12–3.54) more prone to symptomatic dry eye disease than participants without allergic conjunctivitis. Individuals with debris in the tear film were 3.63 times (AOR = 3.63, 95% CI = 1.53–8.61) more likely to have symptomatic dry eye disease than those without debris in the tear film (Table 5).
 |
Table 5 Factors Associated with Symptomatic Dry Eye Disease Among Adult Diabetic Patients in Adare General Hospital, Hawassa City, South Ethiopia, 2023 (n = 488) |
Discussion
In this study, the prevalence of symptomatic dry eye disease (SDED) was 34.8% (95% CI = 30.6–39.1). This result is consistent with the studies conducted in Berhampur 37.2%,24 and India 32.8%.40
On the other hand, the result of this study was higher than that of the study conducted in Iran 17.7%.41 The difference might be due to differences in inclusion and exclusion of the study population. For example, in a study conducted in Iran, only type 2 diabetes was included and the use of medication or history of any other ocular or systemic disease that may affect tear production was excluded.
In contrast, the outcome of this study was lower than previous studies conducted in the United Kingdom 44%,42 Albania 52.9%,17 Iran 54.3%,23 Saudi Arabia 51.7%,25 Erbil, Iraq 41.5%,43 Hoskote, Bangalore 55.7%,26 India 68%,44 Ghana 72.3%,45 and Nairobi, Kenya 49.8%.30 The discrepancy could be due to differences in the socio-demographic characteristics of the study participants, the study setting, and the measurement tool (diagnosis) for the outcome variable. For example, in the studies conducted in Iran, Hoskote, Bangalore, Ghana, and Kenya, tear break-up time, Schirmer test, and ocular surface disease index questionnaire were used to diagnose dry eye, whereas in this study, only OSDI questionnaire was used to diagnose dry eye.
Participants with an educational status of secondary school, college, and university were 2.69 and 5.88 times more likely to have symptomatic dry eye disease, respectively, than those with an educational status of primary school or lower. This result was confirmed by a study conducted in France.46 This could be because as education levels increase, so does the likelihood of coming into contact with visual display devices such as computers, smartphones, and tablets. So, spending more time with screens while blinking less leads to dry eye disease.47
Participants who worked 3–5 and >5 hours at a VDU had a 3.03- and 4.41-fold higher risk of symptomatic dry eye disease, respectively, than participants who worked ≤2 hours per day at a VDU. Studies conducted on Japanese at VDU users,47 Turkey lecturer,48 and Chinese medical students49 reached similar conclusions. The possible reason for this association could be that individuals working at a VDU for a long period of time are exposed to a low blink rate and evaporation of the precorneal tear film contributes to the development of SDED.47
Participants with allergic conjunctivitis were 1.99 times more prone to symptomatic dry eye disease than participants without allergic conjunctivitis. A study conducted in Ethiopia among postgraduate students11 reached a similar conclusion. Allergic conjunctivitis is an inflammatory disorder of the conjunctiva that decreases goblet cell density, alters the lipid layer of the pre-corneal tear film, and increases meibomian gland duct distortion. Those conditions can increase the probability of developing dry eye disease.50,51 Besides, individuals who have used medications such as antihistamines for the treatment of allergic conjunctivitis were more likely to develop dry eye disease than their counterparts.52
The odds of symptomatic dry eye disease for those participants with a duration of diabetes since diagnosis of 6–10 years and ≥11 years were 2.33 and 3.57 times higher than those participants with a duration of diabetes ≤5 years, respectively. This result was in line with the studies conducted in China,5,6 Albania,17 Iran,23 India,18–21,40 Pakistan,22 and Egypt.15 The impact of diabetes on the ocular surface is directly proportional to the duration of DM; that means as the duration of diabetes increases, diabetes could damage the accessory lacrimal gland, which leads to a reduction of basic tear secretion and instability of tear film, which facilitate the occurrence of dry eye disease in diabetic patients.53
Participants who had poor glycemic control were 2.13 times more likely to have symptomatic dry eye disease than participants with good glycemic control. This finding was consistent with the studies conducted in China,16 Albania,17 India,18–21 and Egypt.15 Uncontrolled high blood glucose damages the microvasculature of the lacrimal gland, causes autonomic neuropathy that affects the tear gland, and also disrupts the normal chemical composition and quality of the tear film by increasing the concentration of glucose in the tear film.17,53
Individuals with debris in the tear film were 3.63 times more likely to have symptomatic dry eye disease than those without debris in the tear film, which was similar finding in a study conducted in Egypt.15 The possible explanation for this association is that debris can cause blurring of vision and a foreign body sensation in the eye since the debris is the collection or accumulation of the lipid and mucin of the tear film that is found on the cornea and moves with each blink.
Participants who were government employed were 2.22 times more likely to have symptomatic dry eye disease than those who were employed in the private business. This is due to the fact that employed individuals spent more time on visual display units with a reduced blinking rate.
Limitations of the Study
Because the study design was cross-sectional, it does not show the actual cause and effect relationship. The result of this study might be underestimated because the data were collected using only the OSDI questionnaire instead of using a combination of OSDI tools with other objective tests such as the tear break-up time, Schirmer test, and tear osmolarity test. Current fasting blood sugar was used to assess glycemic control because of the lack of facilities to assess glycated hemoglobin in the study area. Moreover, this study did not assess the impact of total cholesterol, HDL-C, LDL-C, and creatinine levels on the existence of dry eye disease because of the lack of these data in the medical records of the study participants during the data collection period.
Conclusion
The study revealed a high prevalence of symptomatic dry eye disease. Higher educational status, government employed, use of visual display unit, longer duration of diabetes, poor glycemic control, allergic conjunctivitis, and tear film debris were significantly associated with symptomatic dry eye disease. Breaks in screen use, good glycemic control, and treatment of ocular morbidities such as allergic conjunctivitis and debris in the tear film were recommended for all diabetic patients. Moreover, further longitudinal studies using objective tests of dry eye are needed to identify the exact predictors of symptomatic dry eye among diabetic patients.
Data Sharing Statement
All the necessary data are included in the manuscript, and if needed, the supporting data are available by request to the corresponding author.
Acknowledgments
The authors would like to acknowledge the University of Gondar for financial support to conduct the fieldwork of this research. The authors would also like to acknowledge study participants for providing their valuable time and genuine response.
Funding
There is no funding provided for this research for publication.
Disclosure
The authors declare that there are no conflicts of interest in this research work.
References
1. Novack GD, Asbell P, Barabino S, et al. TFOS DEWS II clinical trial design report. Ocul Surf. 2017;15(3):629–649. doi:10.1016/j.jtos.2017.05.009
2. Messmer EM. The pathophysiology, diagnosis, and treatment of dry eye disease. Dtsch Arztebl Int. 2015;112(5):71–81. doi:10.3238/arztebl.2015.0071
3. Alharbi A, Alanazi N, Alhamad J, et al. Prevalence of symptomatic dry eye and its risk factors among coastal population in eastern province of Saudi Arabia. J Clin Exp Ophthalmol. 2018;9:34.
4. International Diabetes Federation. IDF Diabetes Atlas.
5. Pan L-Y, Kuo Y-K, Chen T-H, Sun -C-C. Dry eye disease in patients with type II diabetes mellitus: a retrospective, population-based cohort study in Taiwan. Front Med. 2022;9:980714. doi:10.3389/fmed.2022.980714
6. Du X, Yang Z, Guo Y, et al. Analysis of risk factors for dry eye disease and effect of diquafosol sodium ophthalmic solution on the tear film after vitrectomy in patients with type 2 diabetes mellitus: a preliminary study. Int Ophthalmol. 2023;43(6):1849–18591. doi:10.1007/s10792-022-02584-z
7. Kaiserman I, Kaiserman N, Nakar S, Vinker S. Dry eye in diabetic patients. Am J Ophthalmol. 2005;139(3):498–503. doi:10.1016/j.ajo.2004.10.022
8. Yoon K-C, Im S-K, Seo M-S. Changes of tear film and ocular surface in diabetes mellitus. Korean J Ophthalmol. 2004;18(2):168–174. doi:10.3341/kjo.2004.18.2.168
9. Yu L, Chen X, Qin G, et al. Tear film function in type 2 diabetic patients with retinopathy. Ophthalmologica. 2008;222(4):284–291. doi:10.1159/000140256
10. Zeng X, Lv Y, Gu Z, et al. The effects of diabetic duration on lacrimal functional unit in patients with type II diabetes. J Ophthalmol. 2019;2019:1–11. doi:10.1155/2019/8127515
11. Zeleke TC, Adimassu NF, Alemayehu AM, et al. Symptomatic dry eye disease and associated factors among postgraduate students in Ethiopia. PLoS One. 2022;7(8):1–9.
12. Mohammed S, Kefyalew B, Kebede BN, Lorato MM. Prevalence and associated factors of symptomatic dry eye among undergraduate students in Hawassa University College of Medicine and Health Sciences, Hawassa, Ethiopia. BMJ Open Ophthalmol. 2022;7(1):1–5. doi:10.1136/bmjophth-2022-001149
13. Sahlu M, Giorgis AT. Dry eye disease among Glaucoma patients on topical hypotensive medications, in a tertiary hospital, Ethiopia. BMC Ophthalmol. 2021;21(1):155. doi:10.1186/s12886-021-01917-3
14. Bishua KG, Jenkinsb C, Yebyod HG, et al. Diabetes in Ethiopia: a systematic review of prevalence, risk factors, complications, and cost. Obesity Medicine. 2019;15:100132. doi:10.1016/j.obmed.2019.100132
15. Kamel SS, Mohammed TH, El Zankalony YA, Saad AH. Prevalence of dry eye in diabetics. J Egypt Ophthalmol Soc. 2017;110(3):77. doi:10.4103/ejos.ejos_19_17
16. Zhang X, Zhao L, Deng S, et al. Dry Eye Syndrome in Patients with Diabetes Mellitus: prevalence, Etiology, and Clinical Characteristics. J Ophthalmol. 2016;2016:1–7. doi:10.1155/2016/8201053
17. Burda N, Mema V, Md EM, et al. Prevalence of dry eye syndrome at patients with diabetus melitus tip 2, one year retrospective study. J Acute Dis. 2012;1(2):110–114. doi:10.1016/S2221-6189(13)60026-8
18. Divya K, Dhivya N, Ganesh MR, Sundar D. Dry eye disease and tear dysfunction in patients with type 2 diabetes: a hospital-based study from South India. Sudanese J Ophthalmol. 2019;11(1):14. doi:10.4103/sjopthal.sjopthal_4_19
19. Dutta SK, Paul G, Paul G. Correlation of dry eye and diabetes mellitus. Indian J Clin Exp Ophthalmol. 2021;7(1):25–30. doi:10.18231/j.ijceo.2021.007
20. Khetwani D, Karambelkar V, Gadre GA. Ocular surface disorders in type 2 diabetes mellitus. Int J Contemp Med Res. 2019;6:9–12.
21. Waris S, Balaji RN, Huda R. To study prevalence of dry eyes in diabetic patients. Indian J Clin Exp Ophthalmol. 2019;5(1):40–43. doi:10.18231/2395-1451.2019.0010
22. Faheem M, Abid S, Naqvi H, et al. Frequency of Dry Eyes with and without Posterior Blepharitis in Diabetes Patients. Pakistan Armed Forces Medical Journal. 2022;72(5):1783–1786. doi:10.51253/pafmj.v72i5.7576
23. Manaviat MR, Rashidi M, Afkhami-Ardekani M, Shoja MR. Prevalence of dry eye syndrome and diabetic retinopathy in type 2 diabetic patients. BMC Ophthalmol. 2008;8(1):1–5. doi:10.1186/1471-2415-8-10
24. Panigrahi S, Pati S, Mahapatra B, et al. Dry eye disease in type 2 diabetes mellitus: association with diabetic retinopathy and neuropathy. Eur J Mol Clin Med. 2022;9(3):56.
25. Almohammed BA, Alnafeesah AA, Aldharman SS, et al. Prevalence and Severity of Dry Eye Disease Symptoms Among Diabetics: a Nationwide Survey. Cureus. 2022;14(11). doi:10.7759/cureus.30981
26. Acharlu P, Nadig R, Vijayalekshmi S, Srivastava VK. Dry eye in diabetics: clinical study in rural population. MIJOPH. 2020;14(3):46–49. doi:10.26611/10091431
27. Shaikh R, Ameen J. Prevalence of dry eye disease in type 2 diabetic patients and its co-relation with the duration, glycemic control and retinopathy. Al Ameen J Med Sci. 2015;8:225–229.
28. Uchino M, Schaumberg DA. Dry eye disease: impact on quality of life and vision. Curr Ophthalmol Rep. 2013;1(2):51–57. doi:10.1007/s40135-013-0009-1
29. Yamada M, Mizuno Y, Shigeyasu C. Impact of dry eye on work productivity. Clinicoecon Outcomes Res. 2012;307–312. doi:10.2147/CEOR.S36352
30. Ogundo C, Illako D, Maina J. Prevalence of dry eye syndrome in diabetic patients attending Kenyatta National Hospital, Kenya. J Ophthalmol Eastern Central Southern Africa. 2015;19(2):73.
31. Kang J-H, Shin S-Y. What is the meaning of hs-CRP and HbA1c in patients with dry eye syndrome in diabetes? J Korea Soc Computer Information. 2020;25(3):185–190.
32. Schiffman RM, Christianson MD, Jacobsen G, et al. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
33. Lu F, Tao A, Hu Y, et al. Evaluation of reliability and validity of three common dry eye questionnaires in Chinese. J Ophthalmol. 2018;2018:1–6. doi:10.1155/2018/2401213
34. Care D. Standards of medical care in diabetes-2020. Diabetes Care. 2020;43:S1–S224.
35. Dhungana RR, Karki KB, Bista B, et al. Prevalence, pattern and determinants of chronic disease multimorbidity in Nepal: secondary analysis of a national survey. BMJ Open. 2021;11(7):e047665. doi:10.1136/bmjopen-2020-047665
36. World Health Organization. Obesity: Preventing and Managing the Global Epidemic; 2000.
37. GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2):548.
38. Solomon SD, Goldberg MF. ETDRS Grading of Diabetic Retinopathy: still the Gold Standard? Ophthalmic Res. 2019;62(4):190–195. doi:10.1159/000501372
39. Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach.
40. Guglani S, Gajjar P, Patoria V. Evaluation of prevalence of dry eyes in diabetic patients. J Adv Med Dental Sci Res. 2021;9(6):32–35.
41. Najafi L, Malek M, Valojerdi AE, et al. Dry eye disease in type 2 diabetes mellitus; comparison of the tear osmolarity test with other common diagnostic tests: a diagnostic accuracy study using STARD standard. J Diabetes Metab Disord. 2015;14:1–8. doi:10.1186/s40200-015-0157-y
42. Yazdani-ibn-Taz MK, Han MM, Jonuscheit S, et al. Patient-reported severity of dry eye and quality of life in diabetes. Clin Ophthalmol. 2019;13:217. doi:10.2147/OPTH.S184173
43. Hameed ZG, Abdulgani AI, Abdullah AA. Prevalence of dry eye among 195 patients with diabetes mellitus patients. Zanco J Med Sci. 2016;20(2):1368–1375. doi:10.15218/zjms.2016.0033
44. Patil S, Bishnoi S, Joshi A. Study of dry eye parameters in diabetics in a tertiary care hospital. Med J Patil Univ. 2021;14(2):155–159.
45. Abu EK, Ofori AO, Boadi-Kusi SB, et al. Dry eye disease and meibomian gland dysfunction among a clinical sample of type 2 diabetes patients in Ghana. Afr Health Sci. 2022;22(1):293–302. doi:10.4314/ahs.v22i1.36
46. Malet F, Le Goff M, Colin J, et al. Dry eye disease in French elderly subjects: the Alienor Study. Acta Ophthalmol. 2014;92(6). doi:10.1111/aos.12174
47. Uchino M, Schaumberg DA, Dogru M, et al. Prevalence of dry eye disease among Japanese visual display terminal users. Ophthalmology. 2008;115(11):1982–1988. doi:10.1016/j.ophtha.2008.06.022
48. Vayısoğlu SK, Öncü E, Dursun Ö, Dinç E. Investigation of dry eye symptoms in lecturers by ocular surface disease index. Turk J Ophthalmol. 2019;49(3):142–148. doi:10.4274/tjo.galenos.2018.67915
49. Yu-Ping H, Wen-Fang Z, Peng L, et al. Prevalence of symptomatic dry eye disease among Chinese college students with associated risk factors. Int Eye Sci. 2016;1019–1025.
50. Suzuki S, Goto E, Dogru M, et al. Tear film lipid layer alterations in allergic conjunctivitis. Cornea. 2006;25(3):277–280. doi:10.1097/01.ico.0000178277.29010.bc
51. Arita R, Itoh K, Maeda S, et al. Meibomian gland duct distortion in patients with perennial allergic conjunctivitis. Cornea. 2010;29(8):858–860. doi:10.1097/ICO.0b013e3181ca3668
52. Zhang S, Hong J. Risk factors for dry eye in Mainland China: a multi-center cross-sectional hospital-based study. Ophthalmic Epidemiol. 2019;26(6):393–399. doi:10.1080/09286586.2019.1632905
53. Erdur SK, Aydin R, Ozsutcu M, et al. The relationship between metabolic syndrome, its components, and dry eye: a cross-sectional study. Curr Eye Res. 2017;42(8):1115–1117. doi:10.1080/02713683.2017.1280511
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.