Back to Journals » Clinical Ophthalmology » Volume 17
Switching to Conbercept in Diabetic Macular Edema After Unsatisfactory Response to Previous Intravitreal Injection of Ranibizumab
Authors Xing P, Meng B, Hu X, Qu W, Wang S
Received 13 September 2023
Accepted for publication 9 November 2023
Published 17 November 2023 Volume 2023:17 Pages 3491—3497
DOI https://doi.org/10.2147/OPTH.S431145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Peiyu Xing,1,* Bo Meng,2,* Xiaojia Hu,1 Wei Qu,2 Shaowei Wang2
1Department of Ophthalmology, China Medical University the Fourth People’s Hospital of Shenyang, Shenyang, People’s Republic of China; 2Department of Ophthalmology, the 2nd Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaowei Wang, Department of Ophthalmology, the 2nd Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China, Email [email protected]
Objective: To assess the functional and anatomical effects of transitioning to conbercept intravitreal injection (IVC) treatment in patients with diabetic macular edema (DME) who had inadequate responses to prior anti-vascular endothelial growth factor (anti-VEGF) injections.
Methods: We retrospectively included eyes with persistent DME after at least 3 injections of intravitreal ranibizumab (IVR). The analysis included the assessment of best corrected visual acuity (BCVA) and central macular thickness (CMT) during 6 months after the switch.
Results: A total of 30 patients (30 eyes) were included. CMT dropped sharply from 437.8± 40.67μm at baseline to 363.59± 45.09,312.52 ± 39.15, 278.51 ± 37.92, and 292.59 ± 38.09 after 1, 2, 3 and 6 months of IVC, respectively (p < 0.001). BCVA in log MAR units was significantly improved from 0.73± 0.15 at baseline to 0.50± 0.09,0.46± 0.72, 0.40± 0.06 and 0.48± 0.04 after 1, 2, 3 and 6 months, respectively (p < 0.001).
Conclusion: Switching to Conbercept effectively improved visual and anatomical structure in DME patients who had not responded satisfactorily to previous anti-VEGF injections.
Keywords: diabetic macular edema, anti-vascular endothelial growth factor, central macular thickness, best corrected visual acuity, DME, CMT, anti-VEGF, BCVA
Introduction
Diabetic macular edema (DME) is a serious complication of diabetic retinopathy (DR), which leads to visual impairment. Which is characterized by an accumulation of fluid in the macular, the central area of the retina.1 Abnormal blood vessel permeability is responsible for this fluid leakage. In 2010, approximately 20.6 million adults worldwide were estimated to have developed DME, a complication of DR.2 It is expected that this worldwide healthcare challenge will persistently rise at concerning rates, with projections suggesting that the diabetic population will potentially double by 2030.3
The DME is dependent on the critical involvement of vascular endothelial growth factor (VEGF).4 Recently, anti-VEGF agents have become the primary treatment for DME, showing significant improvements in vision and disease control.5
Nevertheless, some patients show no response to intravitreal ranibizumab (IVR) after at least three injections,6–8 and may experience ongoing fluid accumulation and destruction to the retinal neurons, resulting in visual impairment and limited vision recovery.9
Currently, anti-VEGF intravitreal injection (IVC) stands as the first-line therapy for DME. The use of Conbercept has the potential to enhance the treatment of chronic macular edema and offer sustained visual advantages over time. Compared to ranibizumab, Conbercept is a novel anti-VEGF agent, in which core domain is fused by human VEGFR1 immunoglobulin-like domain 2, human VEGFR2 immunoglobulin-like domains 3 and 4, and human immunoglobulin Fc fragment (molecular weight, 142 kd).10 Conbercept demonstrates a higher binding capacity to VEGF compared to natural and monoclonal antibodies, enabling it to efficiently block all variants of VEGF-A, VEGF-B, and placental growth factor.11 Compared with aflibercept, Conbercept has a four-binding site of receptor 2, and it increases the steadiness of the dimer and its affinity to VEGF and VEGF-B.12
After the Phase III clinical trials,13 it was found that using Conbercept regimen led to amelioration in best corrected visual acuity (BCVA) and central macular thickness (CMT) in patients who had DME. As a result, Conbercept is now seen as a feasible choice for addressing DME. However, there are few reports on the effects of an IVC of Conbercept (IVC) on DME patients who had no response of previous IVR.
This research aimed to investigate if patients who had DME but did not show improvement with previous anti-VEGF treatment would experience any further visual and anatomical improvements after changing to Conbercept.
Methods
Between 1st, January 2020 and 31st, December 2022, a retrospective study was conducted in the second affiliated Hospital of Harbin Medical University, involving a sample of 30 patients and 30 eyes diagnosed with DME. The Research Ethics Committee of the Second Affiliated Hospital of Harbin Medical University in Harbin, China, granted approval for this study. All procedures followed the principles of the Declaration of Helsinki. Written informed consent was given by each participant after the discussion of the procedure, follow-up schedules and benefits and risks that may occur.
The diagnosis was made by clinical examination and optical coherence tomography (SD-OCT) in spectral domain. Inclusion criteria were patients diagnosed with DME who had received at least 3 consecutive IVR treatments 6 months prior to switching to Conbercept. Minimum follow-up time was 6 months. Exclusion criteria were patients who underwent phacoemulsification, YAG capsulotomy, or corticosteroid therapy (implant/tenon injection) during treatment that affected possible vision outcomes.
The criteria for eligibility to switch treatments included patients with refractory or persistent DME who met the following requirements CMT measured by SD-OCT was over 300μm, and the reduction in retinal thickness was less than 10% of the baseline thickness; and there was a suboptimal visual improvement (failure to gain at least three lines on the Snellen chart).
0.05mL (0.5 mg) Conbercept (Chengdu Kanghong Biotechnology Co., Ltd.; Chengdu, Sichuan, China), a comprehensive assessment of the eyes was performed on all patients, which included measuring BCVA using Snellen measurement converted to the Logarithm of the Minimum Angle of Resolution (logMAR), using an applanation tonometer to measure intraocular pressure (IOP) examining the anterior segment using a slit lamp, and examining the fundus using indirect ophthalmoscopy. SD-OCT was performed on all patients prior to and at 1, 2, 3, and 6 months following the initial injection.
Statistics
A sample size of 29 patients was determined based on a 2-sided 95% confidence interval (CI) with a width equal to 0.20 when the sample proportion was 0.80. Primary analysis criteria considered patients who discontinued IVC treatment to be improvement of BCVA. We expressed the improvement of BCVA at 6-month as continuous number and provided a 2-sided 95% CI. We used a one-sample Kolmogorov–Smirnov test to examine the normal distribution of the samples. Analysis of variance (one-way analysis of variance) test was employed to compare quantitative that were collected at the different time intervals within the same group. We used SPSS V.19.0 for Windows (SPSS, Chicago, Illinois, USA) to perform data analysis. p value less than 0.05 is considered to be statistically significant.
Results
Table 1 displays the demographic and clinical data for all patients at baseline. This study included 16 females and 14 males, with the mean age of 58.23 ± 8.32 years. There were 25 patients undergoing insulin treatment while the remaining 5 patients were receiving oral anti-diabetic drug treatment. The average number of anti-VEGF injections of the cohort received before switching to Conbercept was 3.86±0.9. The mean HbA1c level was 7.84 ± 0.74. At baseline, the CMT measured 437.8 ± 40.67 μm. The average baseline BCVA was 0.73 ± 0.15.
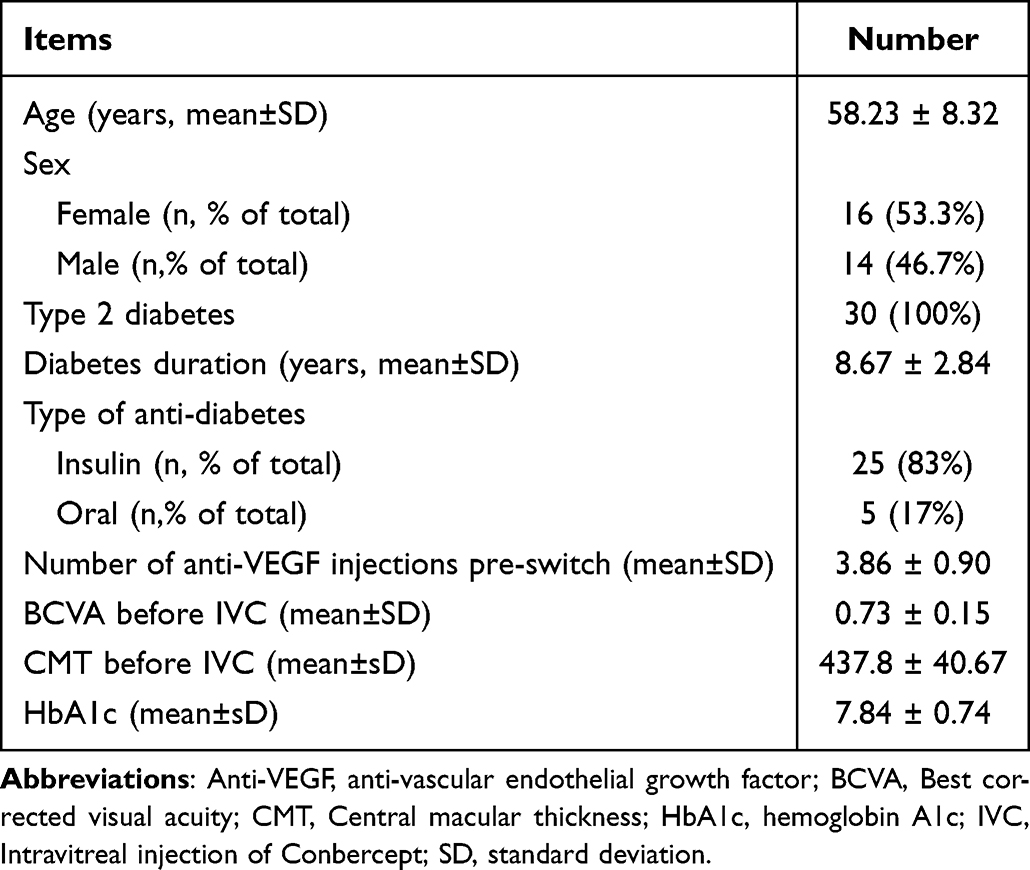 |
Table 1 Demographics and Clinical Characteristics of Patients |
In comparison to the baseline, the BCVA showed improvement at various time points 0.50 ± 0.09 at 1 month (p < 0.001), 0.46 ± 0.72 at 2 months (p < 0.001), 0.40 ± 0.06 at 3 months (p < 0.001), and 0.48 ± 0.04 at 6 months (p < 0.001, Figure 1).
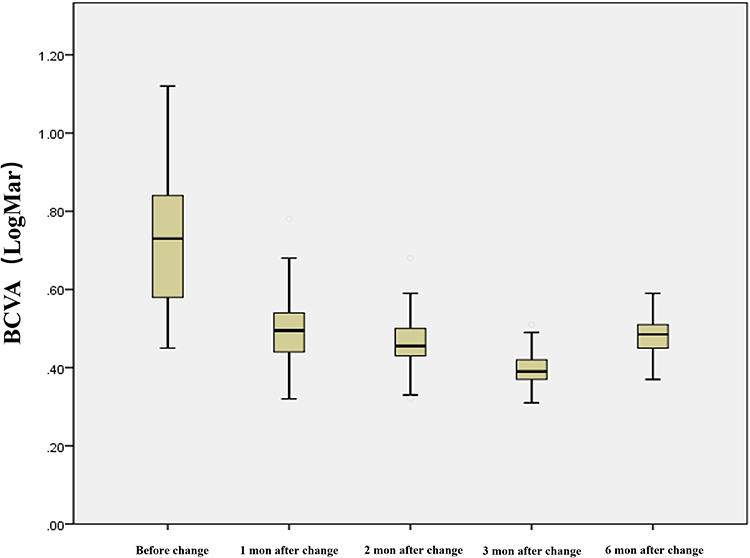 |
Figure 1 BCVA (LogMar) changes. |
Compared with baseline, the CMT decreased significantly to 363.59 ± 45.09 μm at baseline (p < 0.001), further decreasing to 312.52 ± 39.15 μm at 2 months (p < 0.001), 278.51 ± 37.92 μm at 3 months (p < 0.001), and 266.69 ± 38.11 μm at 6 months (p < 0.001, Figure 2).
 |
Figure 2 CMT changes. |
No significant systemic adverse events such as myocardial infarction, transient ischemic attacks and strokes, or eye adverse events, such as endophthalmitis. Retinal detachment and prolonged elevation in intra-ocular pressure were shown during study period.
Discussion
The main cause of DME is the retinal vascular permeability, which leads to fluid accumulation in the retina and causes an increase in its thickness, which is related to disruption of the blood retinal barrier and increased production of VEGF.14
Multiple randomized clinical trials have provided proof for the effectiveness of anti-VEGF medications in treating DME, and improve eyesight and reduce CMT.15,16 In current study, both the BCVA and CMT had been improved among patients with DME who had not responded satisfactorily to previous IVR injections.
In the past three decades, there have been significant developments in diagnosing and treating DME. Ranibizumab, an anti-VEGF treatment, has demonstrated its effectiveness and widespread applicability.17 However, although the results are encouraging some patients do not respond fully or at all to ranibizumab. It poses a challenge to further treatment. A potential solution is to switch to Conbercept, which has been suggested as a useful alternative due to its different pharmacodynamics and reported longer duration of action.18
Elevated levels of platelet-derived growth factor (PDGF) and VEGF in the vitreous humor have been specifically linked to the development of DME, as they play a role in the disruption of the blood-retinal barrier.19 In addition, repeated injections of ranibizumab, which contains murine antibody components, can potentially trigger an immune response, resulting in the formation of neutralizing antibodies and reduced effectiveness of the treatment.20 Switching to Conbercept may help alleviate the tolerance that has developed to previous anti-VEGF medications.
The post-hoc analysis of the DRCR.net protocol I21 supports our study design which favors early switch criteria. According to this study, patients who do not have a satisfactory visual improvement after receiving three rounds of anti-VEGF injections are more likely to be advised to modify their treatment plan and switch to alternate approaches for better functional outcomes. Eyes that showed a suboptimal early response to monthly IVR treatment, demonstrated worse long-term visual outcomes compared to eyes with a noticeable early response,21 at 12 weeks.
While it may be deemed insufficient that patients receive an average of 3–4 ranibizumab injections before switching, there is potential for an ultimate improvement in their conditions if they had continued with ranibizumab treatment. To decrease the likelihood, we selectively included patients in our study who exhibited CMT over 300 μm through SD-OCT, had a decrease in retinal thickness of less than 10% compared to the baseline, or experienced suboptimal visual improvement.
Other studies have shown the conversion of monoclonal antibodies to fusion proteins which support our study. Earlier studies involving 42 eyes showed poor response to monoclonal antibody therapy, so they were treated with fusion proteins instead. In patients with DME who did not respond well to previous anti-VEGF injections, switching to fusion proteins resulted in improved vision and retinal architecture.22
In another study, 40 patients (59 eyes) with DME were switched to fusion protein therapy after not responding to three consecutive injections of monoclonal antibodies. CMT decreased significantly from the baseline measurement of 395.08 ± 129.9 μm to 282.39 ± 95.278, 245.36 ± 79.861, and 201.17 ± 54.042 μm after 1, 3 and 6 months. Additionally, there was a notable improvement in BCVA from 0.95 ± 0.21 to 0.51 ± 0.23 after 6 months.23
The measurement of the half-life of anti-VEGF drugs was conducted in monkey vitreous tissue, and the half-life of ranibizumab in such tissue was estimated to be 3 days,24 while the Conbercept half-life was 4.5 days. Conbercept contains Fc fragments, binds to the endothelium`s Fc receptors for IgG (FcRn receptors) and protects themselves from damage by the endosome, thus lengthening their half-life.25 Ranibizumab has fast systemic clearance in that there is no Fc domains. Reasons for the significant anatomical amelioration with Conbercept might be attributed to its distinct pharmacokinetic and pharmacodynamic characteristics, as Conbercept stays in systemic circulation longer while ranibizumab is rapidly eliminated from the body.26 Conbercept has a higher binding to VEGF-A, resulting in possibly sustained VEGF-A inhibition. Besides, it can bind to two additional growth factors, VEGF-B and pIGF, which are released in angiogenesis.27
Another reason for the additional clinical response of IVC is tachyphylaxis to Conbercept in patients with DME. The peak concentrations are reached in all eye tissues at 6–12 hours after the infusion of Conbercept,28 which patients may eventually yield to, with repeated treatment injections of ranibizumab.29 The multifactoral mechanism includes macrophage up-regulation of VEGF, differing surface receptor expression, variations in pharmacokinetics and development of neutralising antibodies as part of a systemic immune response.29
Despite frequent anti-VEGF therapy, there was no anatomical improvement in these eyes prior to the switch. All eligible patients experienced some improvement in function when switched to Conbercept. The majority of patients experienced improved visual acuity after switching to Conbercept, indicating potential reversibility of functional damage, with all patients being monitored for a minimum of 6 months.
There were several limitations in this study, including its retrospective non-randomized design, the limited number of eyes included, no control group the relatively short duration of follow-up, and the added challenge posed by the multifactorial nature of DME. Moreover, due to the retrospective study design, having considered only the CMT and BCVA in current study and left out other parts of the macula (8 ETDRS sub-fields) it is difficult to judge the effectiveness of the study. Furthermore, we also have not reported on the fluid collection and the effect of IVC on it, thus our findings should be noted with cautions. Further prospective, well-designed study is needed.
Conclusion
Conbercept therapy demonstrated a notable improvement in both the anatomy and functionality of persistent DME cases which did not respond adequately or completely to ranibizumab.
Data Sharing Statement
The data used to support the findings of this study are included in the article.
Acknowledgments
We thank Home for Researchers editorial team (www.home-for-researchers.com) for improving the English language in this manuscript.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; participated in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ciulla TA, Zinman B. Diabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapies. Diabetes Care. 2003;26(9):
2. Yau JW, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
3. Wild RG, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. doi:10.2337/diacare.27.5.1047
4. Antonetti DA, Barber AJ, Hollinger LA, Wolpert EB, Gardner TW. Vascular endothelial growth factor induces rapid phosphorylation of tight junction proteins occludin and zonula occluden 1. A potential mechanism for vascular permeability in diabetic retinopathy and tumors. J Biol Chem. 1999;274(33):23463–23467. doi:10.1074/jbc.274.33.23463
5. Glassman AR, Wells JA 3rd, Josic K, et al. Five-Year Outcomes after Initial Aflibercept, Bevacizumab, or Ranibizumab Treatment for Diabetic Macular Edema (Protocol T Extension Study). Ophthalmology. 2020;127(9):1201–1210. doi:10.1016/j.ophtha.2020.03.021
6. McCloskey CF, Mongan AM, Chetty S, McAteer DMJ, Quinn SM. Aflibercept in Diabetic Macular Oedema Previously Refractory to Standard Intravitreal Therapy: an Irish Retrospective Study. Ophthalmol Ther. 2018;7(1):173–183. doi:10.1007/s40123-018-0123-0
7. Klein KA, Cleary TS, Reichel E. Effect of intravitreal aflibercept on recalcitrant diabetic macular edema. Int J Retina Vitreous. 2017;3:16. doi:10.1186/s40942-017-0064-0
8. Calugaru D, Calugaru M. Conversion to Aflibercept After Prior Anti-VEGF Therapy for Persistent Diabetic Macular Edema. Am J Ophthalmol. 2016;168:290–291. doi:10.1016/j.ajo.2016.05.015
9. Nguyen QD, Tatlipinar S, Shah SM, et al. Vascular endothelial growth factor is a critical stimulus for diabetic macular edema. Am J Ophthalmol. 2006;142(6):961–969. doi:10.1016/j.ajo.2006.06.068
10. Zhang M, Yu D, Yang C, et al. The pharmacology study of a new recombinant human VEGF receptor-fc fusion protein on experimental choroidal neovascularization. Pharm Res. 2009;26(1):204–210. doi:10.1007/s11095-008-9718-9
11. Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15(2):171–185. doi:10.1007/s10456-011-9249-6
12. Zhang M, Zhang J, Yan M, et al. A Phase 1 Study of KH902, a Vascular Endothelial Growth Factor Receptor Decoy, for Exudative Age-Related Macular Degeneration. Ophthalmology. 2011;118(4):672–678. doi:10.1016/j.ophtha.2010.08.008
13. Liu K, Wang H, He W, et al. Intravitreal conbercept for diabetic macular oedema: 2-year results from a randomised controlled trial and open-label extension study. Br J Ophthalmol. 2022;106(10):1436–1443. doi:10.1136/bjophthalmol-2020-318690
14. Campos Polo R, Rubio Sanchez C, Garcia Guisado DM, Diaz Luque MJ. Aflibercept for clinically significant diabetic macular edema: 12-month results in daily clinical practice. Clin Ophthalmol. 2018;12:99–104. doi:10.2147/OPTH.S154421
15. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for Diabetic Macular Edema. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
16. Rajendram R, Fraser-Bell S, Kaines A, et al. A 2-year prospective randomized controlled trial of intravitreal bevacizumab or laser therapy (BOLT) in the management of diabetic macular edema: 24-month data: report 3. Arch Ophthalmol. 2012;130(8):972–979. doi:10.1001/archophthalmol.2012.393
17. Akbas YB, Alagoz C, Cakmak S, Demir G, Alagoz N, Artunay HO. Three year outcomes of intravitreal ranibizumab and aflibercept treatment of patients with diabetic macular edema: a comparative study. Therapeutic Adv Ophthalmol. 2023;15. doi:10.1177/25158414231195174
18. Ren F, Zhang X, Gong H, et al. Two different initial treatment regimens of Conbercept in diabetic macular edema: 12-month results from a multicenter randomized controlled study. Photodiagnosis Photodyn Ther. 2023:44. doi:10.1016/j.pdpdt.2023.103745
19. Lee S-J, Kim M, Kim Y. Comparison of aqueous concentrations of angiogenic and inflammatory cytokines based on optical coherence tomography patterns of diabetic macular edema. Indian J Ophthalmol. 2015;63(4). doi:10.4103/0301-4738.158069
20. Zou C, Han C, Zhao M, et al. Change of ranibizumab-induced human vitreous protein profile in patients with proliferative diabetic retinopathy based on proteomics analysis. Clin Proteomics. 2018;15(1). doi:10.1186/s12014-018-9187-z
21. Gonzalez VH, Campbell J, Holekamp NM, et al. Early and Long-Term Responses to Anti-Vascular Endothelial Growth Factor Therapy in Diabetic Macular Edema: analysis of Protocol I Data. Am J Ophthalmol. 2016;172:72–79. doi:10.1016/j.ajo.2016.09.012
22. Ibrahim WS, Eldaly ZH, Saleh MG, Rateb MF, Aldoghaimy AH. Switching to Aflibercept in Diabetic Macular Edema after Unsatisfactory Response to Other Anti-vascular Endothelial Growth Factor Drugs. Korean J Ophthalmol. 2019;33(2):122–130. doi:10.3341/kjo.2018.0037
23. Nawar AE, Wasfy T, Shafik HM. Switching to ziv-aflibercept in resistant diabetic macular edema non responsive to ranibizumab injection. BMC Ophthalmol. 2022;22(1):287. doi:10.1186/s12886-022-02503-x
24. Gaudreault J, Fei D, Rusit J, Suboc P, Shiu V. Preclinical pharmacokinetics of Ranibizumab (rhuFabV2) after a single intravitreal administration. Invest Ophthalmol Vis Sci. 2005;46(2):726–733. doi:10.1167/iovs.04-0601
25. Ternant PG. Pharmacokinetics and concentration-effect relationships of therapeutic monoclonal antibodies and fusion proteins. Expert Opin Biol Ther. 2005;5(Suppl 1):S37–47. doi:10.1517/14712598.5.1.s37
26. Liu L. Pharmacokinetics of monoclonal antibodies and Fc-fusion proteins. Protein Cell. 2017;9(1):15–32. doi:10.1007/s13238-017-0408-4
27. Li H, Lei N, Zhang M, Li Y, Xiao H, Hao X. Pharmacokinetics of a long-lasting anti-VEGF fusion protein in rabbit. Exp Eye Res. 2012;97(1):154–159. doi:10.1016/j.exer.2011.09.002
28. Du PH, Wu Q, Zhu M, et al. Observation of total VEGF level in hyperglycemic mouse eyes after intravitreal injection of the novel anti-VEGF drug conbercept. Mol Vis. 2015;21:185–193.
29. Eghoj MS, Sorensen TL. Tachyphylaxis during treatment of exudative age-related macular degeneration with ranibizumab. Br J Ophthalmol. 2012;96(1):21–23. doi:10.1136/bjo.2011.203893
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Intravitreal Brolucizumab for Diabetic Macular Edema After Vitrectomy: A Before-and-After Study at a Specialized Center in Japan
Saito K, Akiyama H
Clinical Ophthalmology 2025, 19:1957-1964
Published Date: 23 June 2025
Serum Apolipoprotein B and B/A1 Ratio as Early Negative Biomarkers for OCT- and OCTA-Detected Retinal Changes in Diabetic Macular Edema
Soedarman S, Julia M, Gondhowiardjo TD, Kurnia KH, Prasetya ADB, Triyoga IF, Sasongko MB
Clinical Ophthalmology 2025, 19:2165-2178
Published Date: 9 July 2025