Back to Journals » Patient Preference and Adherence » Volume 17
Switching from Monthly to Three-Monthly Long-Acting Injectable Paliperidone: A Survey on Subjective Satisfaction and Safety
Received 16 March 2023
Accepted for publication 5 July 2023
Published 12 July 2023 Volume 2023:17 Pages 1603—1610
DOI https://doi.org/10.2147/PPA.S410028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Joshua Barnett,1 Sofia Pappa1,2
1Department of Mental Health, West London NHS Trust, London, UK; 2Department of Brain Sciences, Imperial College London, London, UK
Correspondence: Joshua Barnett, Department of Mental Health, West London NHS Trust, 43– 47 Avenue Road, London, W38NJ, UK, Tel +44 20 84831792, Email [email protected]
Introduction: Poor adherence to antipsychotic medication is common in the treatment of schizophrenia and other psychotic disorders. Paliperidone palmitate 3-monthly (PP3M) is the first long-acting injectable (LAI) antipsychotic to allow for only four medication administrations per year, and although there is sufficient information available about the clinical effects, there is relatively limited insight into the subjective experience of people with lived experience.
Methods: This descriptive, cross-sectional survey explored patient’s satisfaction and perspectives on the advantages and disadvantages of switching from monthly to 3-monthly paliperidone while also reporting on perceived levels of safety with regard to the reducing dose regimen during the Covid-19 pandemic. Information on discontinuation and hospitalisation rates at one year was also collected from the electronic records.
Results: Of the 46 patients included in the study, the vast majority reported feeling satisfied (89.2%) and safer (93.5%) after switching to the three-monthly formulation. Participants highlighted several advantages of changing to PP3M, most notably convenience (93.5%), improved quality of life (58.7%), decreased stigma (39.1%) and better adherence (28.3%). Furthermore, 93.5% of respondents experienced no disadvantages, while 6.5% described worsening side effects or symptoms. In fact, only one patient discontinued PP3M at one year with the overall number of hospitalisations also reducing in the same period compared to the year before switching.
Discussion: Our findings add to the small, but growing, body of evidence supporting patient satisfaction and acceptance with the use of PP3M and may reinforce the use of less frequent LAIs in clinical practice to enhance individual experience and treatment persistence and decrease levels of stigmatisation.
Keywords: schizophrenia, paliperidone, long-acting injectable, patient satisfaction
Introduction
Poor adherence to antipsychotic medication is a significant problem in the management of schizophrenia.1 It is a strong predictor of relapse and consequently associated with poorer functional outcomes, increased likelihood of suicidal behaviour and premature death and higher rehospitalisation rates and healthcare costs.2 Oral medication requires daily commitment to treatment, which may be hampered by factors such as stigma, cognitive symptoms, lack of social support and impaired insight of the need for continued treatment in this group of patients.3 Long-acting injectable antipsychotics (LAIs) offer a viable alternative which overcomes the need for daily dosing4 while allowing for close monitoring and assertive follow-up.5 They also avoid first-pass metabolism and provide greater bioavailability with more stable plasma levels and reduced plasma peaks.6
Paliperidone palmitate 3-monthly (PP3M) is an approved maintenance treatment available to patients with schizophrenia who have been previously stabilised on paliperidone palmitate 1-monthly (PP1M) for at least four months7 and was the first LAI to require only four administrations per year.8 It is a safe and efficacious formulation9,10 which has been shown to delay time to relapse,11 reduce hospitalisation12,13 and promote functional recovery.14
Though there is sufficient information available about the clinical aspects of PP3M, there is relatively limited insight into patients’ perspectives. One of the few studies evaluating service user experience showed that patients found the reduced dosing of PP3M versus PP1M to be more convenient and less stigmatising,4 although another study showed similar effects in quality of life and health satisfaction.15 Nevertheless, understanding patient’s viewpoints fully is key to the process of shared decision-making16 which has been shown to increase adherence and satisfaction in people with lived experience.17 Furthermore, the safety aspect of reduced face-to-face contact with regard to the Covid-19 pandemic was not reported on but should not be overlooked. Although the peak of the pandemic appears to have passed with the advent of an effective vaccination,18 the virus remains prevalent both in the UK19 and globally.20 Furthermore, people with mental health problems have a lower life expectancy and poorer physical health outcomes than the general population and are at an increased risk of viral infections,21,22 therefore ways to reduce the spread of Covid-19 and other viruses to this vulnerable population remain important. Other situations where access to services may be limited, could also be of relevance such as provision of care within primary services and/or rural areas.
The aim of this study is to explore the patient subjective satisfaction and perspectives on the advantages and disadvantages of switching from PP1M to PP3M, including their feeling of safety with respect to the Covid-19 pandemic.
Methods
This cross-sectional, observational study was conducted across multiple sites between April-June 2020 in West London NHS trust, a large, urban mental health provider. It was approved as a service evaluation by the department for audit and naturalistic research (project number 1545) and therefore did not require research ethics committee approval. Verbal consent was gained prior to conducting the survey; obtaining written consent was not practical given the Covid-19 restrictions on face-to-face contact that were in place at the time.
The study cohort was formed of patients who were a) receiving PP3M at the time of the survey, b) under the care of secondary mental health services, c) demonstrating adequate mental capacity, and d) providing verbal consent. Initiation of PP3M was subject to independent clinical prescribing decision, and standard of care was unaffected.
A comprehensive list of patients receiving PP3M was obtained by an external pharmacy who coordinate supply and distribution. Two psychiatrists contacted patients on this list and invited them to take part in the survey either in person or over the phone after gaining verbal consent. All other necessary demographical and clinical information was provided by the electronic clinical records system, including the number of hospitalisations one year pre- and post-initiation of PP3M, the level of compliance (ie number of injections at one year) as well as the discontinuation rate at one year and reason if applicable.
Enrolled individuals provided answers to a co-developed four-part questionnaire which focused on their experiences of PP3M compared to PP1M. Using a 5-point Likert scale (1 = strongly agree; 5 = strongly disagree), they were asked how much they agreed or disagreed with the statements made in questions one (I feel satisfied after changing from PP1M to PP3M?) and two (I feel safer having my injection every 3 months instead of every 1 month during the Covid-19 pandemic?). Question three (Have you experienced any advantages from changing PP1M to PP3M?) enquired about possible advantages of changing formulation (no advantages, improved quality of life, decreased stigmatisation, better convenience, improved side effects, better compliance, other) whilst question four (Have you experienced any disadvantages from changing PP1M to PP3M?) looked at disadvantages (no disadvantages, relapse of symptoms, worsening/new side effects, preferred 1-monthly frequency, reduced clinical contact, other); more than one answer could be given to questions three and four. Descriptive analysis was used to summarise the demographic characteristics and questionnaire outcomes. In addition to the total sample (‘all patients’ group), we also reported on the findings of the “Schizophrenia” group separately as PP3M is most commonly used (as per indication and licencing in most places) in the treatment of schizophrenia; this further allows for a comparison with other past or future studies, that solely include patients of schizophrenia which is often the case.
Results
Of the 61 patients who were receiving PP3M at the time, a total of 46 respondents (31 males, 15 females) were included in this study. One declined to participate, while 14 were not contactable despite multiple attempts, making the response rate 97.8% (46/47). The average age of the “all patient” (N = 46) group was 48.5 (48.2 male, 49.0 female), and the range 23–78. The majority of patients (39/46) had a recorded diagnosis of schizophrenia and the remainder schizoaffective Disorder. The mean length of PP1M use (months) prior to switching to PP3M was 47.1 for all patients (52.2 males, 36.5 females). Additional demographical information of the whole study sample characteristics is provided in Table 1.
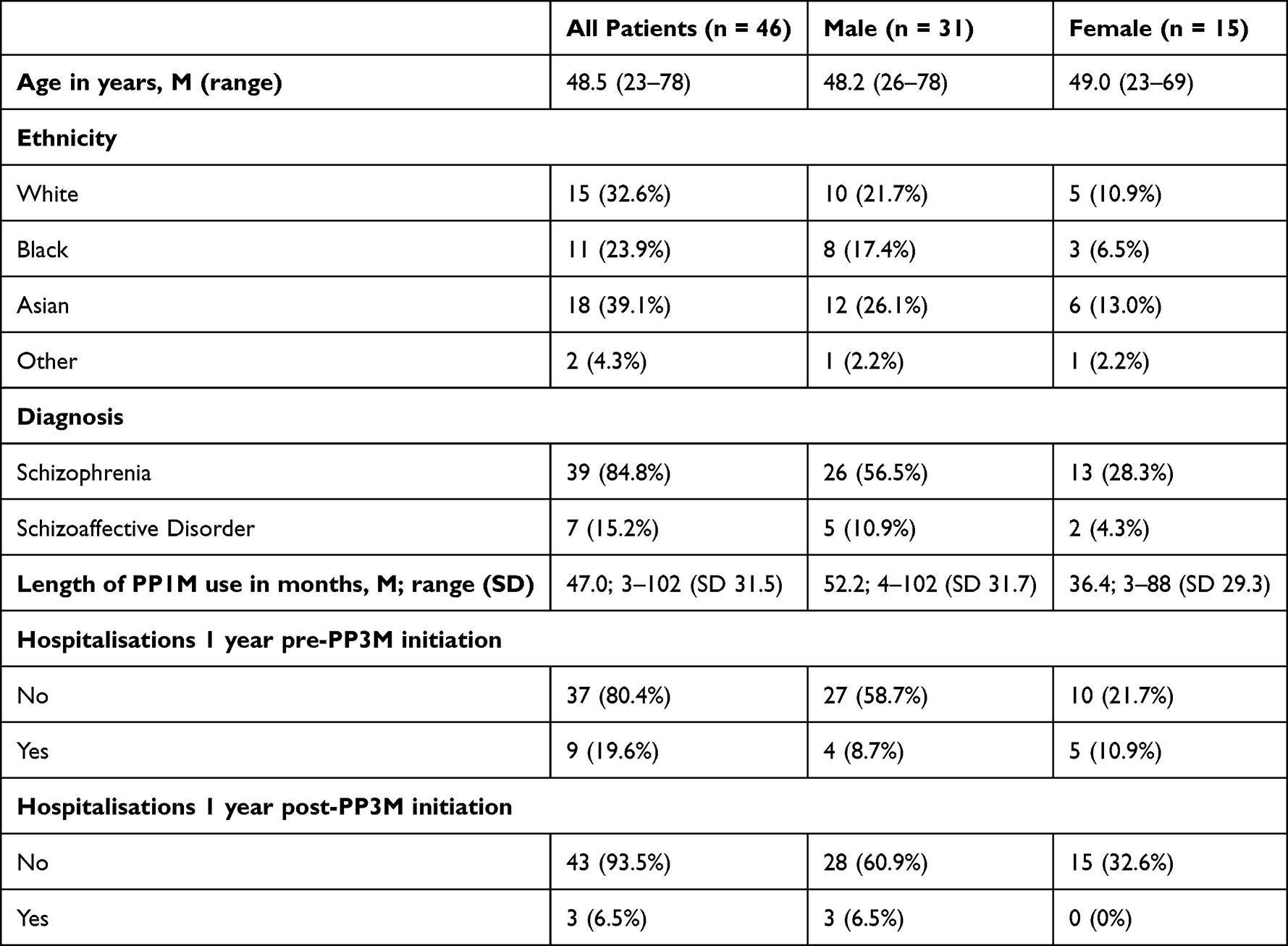 |
Table 1 Demographical Information |
Total hospitalisations one year pre- and post-PP3M initiation were also recorded. The number of patients who did not have any hospitalisations during this period of time increased from 37 (80.1%) before to 43 (93.5%) after switching over to the three-monthly formulation, while the amount of patients hospitalised reduced from 12 to 4 (Table 1). Additionally, 45/46 (97.8%) of participants completed one year of PP3M use with 100% compliance, meaning they received four out of four 3-monthly injections that year. Only one patient (a 47-year-old female with schizophrenia) discontinued following two doses of PP3M before switching back to PP1M due to a worsening of symptoms.
The majority of respondents strongly agreed (69.6%, n = 32/46) or agreed (19.6%, n = 9/46) with the statement that they were satisfied after changing from PP1M to PP3M. About 6.5% (n = 3/46) neither agreed nor disagreed, 4.3% (n = 2/46) disagreed, while no-one strongly disagreed (Figure 1, question 1). Similarly, most patients strongly agreed (56.5%, n = 26/46) or agreed (37%, n = 17/46) that they felt safer with the 3-monthly formulation compared to the 1-monthly during the Covid-19 pandemic. About 6.5% (n = 3/46) neither agreed or disagreed, and none of the respondents disagreed (Figure 1, question 2).
 |
Figure 1 Question 1 (I feel satisfied after changing from PP1M to PP3M) and question 2 (I feel safer having my injection every 3 months instead of every 1 month during the Covid-19 pandemic). |
The most commonly experienced advantage of PP3M over PP1M was convenience (93.5%, n = 43), followed by improved quality of life (58.7%, n = 27/46), decreased stigma (39.1%, n = 18/46), better compliance (28.3%, n = 13/46) and improved side effects (21.7%, n=10/46); 6.5% (n = 3/46) reported not experiencing any advantages (Figure 2, question 3). Furthermore, 93.5% (n = 43/46) described experiencing no disadvantages from the change of formulation. However, 4.3% (n = 2/46) reported worsening/new side effects and 2.2% (n = 1/46) worsening of symptoms (Figure 2, question 4).
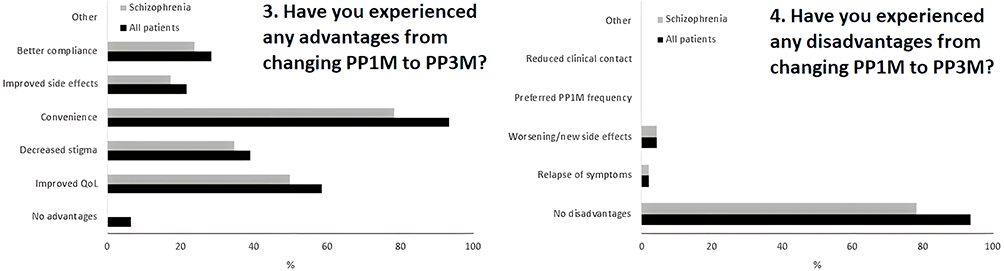 |
Figure 2 Question 3 (Have you experienced any advantages from changing PP1M to PP3M?) and question 4 (Have you experienced any disadvantages from changing PP1M to PP3M?). |
Discussion
The overall experience of patients in this study was that PP3M is preferable and confers multiple advantages versus the 1-monthly preparation. The high patient satisfaction rate (89.2%) is comparable with those reported in the study by Fernandez-Miranda et al (85.6%)23 and Spoelstra et al (69%).5 The positive outcome appears to be multifactorial, mediated by considerable benefits and the absence of serious concerns or risks.
The most commonly cited advantage of switching to a less frequent LAI was convenience (93.5%), which is an often-described benefit for patients4,24,25 that may also lead to a decrease in carer burden.4,26 It is implied that improved convenience is secondary to less frequent dosing which, when compared to PP1M, will inevitably lead to reduced contact with clinicians. Interestingly, no patients reported this as a disadvantage in the survey, despite initial concerns that decreased clinician contact may lead to increased rates of relapse or disengagement.27 Quite the reverse, the “less is more” principle appears to apply in this case as less frequent, ultra-long-acting treatments may be associated with improved social acceptability and hope28 and could contribute to the lessening of stigmatisation described by some respondents (39.1%). Stigmatisation of people with schizophrenia is a challenge frequently reported by service users, as well as physicians, nurses and carers.4 It can lead to low self-esteem29–31 and social withdrawal32 and is also associated with depression, anxiety and both positive and negative symptoms.33,34 Furthermore, over half of all respondents (58.7%) reported an improved quality of life (QoL), which has long been recognised as an important patient outcome.35 It is a multifaceted concept that is affected by both aspects of an illness and its treatment36 and those with schizophrenia consistently report much lower levels compared to both the general population and individuals with physical illness.37,38 While this study did not examine the specific reasons for the perceived improved QoL, it could be posited that less stigma and enhanced convenience, acceptance and tolerability may have all contributed to this. Use of the recently developed paliperidone palmitate 6-monthly could lead to further improvements in the domains of stigmatisation and QoL whilst not compromising on safety or efficacy.39
Over a quarter of patients (28.3%) reported better compliance with PP3M and data from the electronic clinical records system show that 46/47 patients completed one year of PP3M with 100% medication concordance. Previous studies have demonstrated a direct association between improved level of compliance with LAIs (ie no or less missed injections) and rates of hospital admission,40,41 thus it is perhaps unsurprising that the number of patients hospitalised decreased from the periods 1 year pre (9) to 1 year post (3) initiation of PP3M. Interestingly, there was a 100% reduction in the number of hospitalisations in females, while there was only a 25% decrease in males. Typically, psychotic symptoms in females tend to respond better and at lower doses to antipsychotics than men42 which may partly explain this finding, though the sample size is relatively low and the difference could be coincidental. Additionally, the results of this survey show that approximately one-fifth (21.7%) of all patients saw improved tolerability, a finding which replicates the results from previous studies.23 In turn, this reduction in side effect burden may be a factor contributing to the increase in adherence.43,44
This study was carried out during a highly transmissible phase of the Covid-19 pandemic and the majority (93.5%) of patients felt safer with less frequent drug administration. Though Covid-19 is still prevalent, the restrictions that were in place when this survey was deployed are no longer in place. However, the after-effects of the pandemic continue to be felt in the healthcare systems alongside other longstanding challenges such as staff shortages45,46 and accelerated burnout.47 Hence, interventions that reduce clinical contact time and allow for reallocation of resources appear to be of critical importance now more than ever particularly in highly pressured, urban or less accessible, rural parts of the system.
Strengths and Limitations
To our knowledge, the present study is the first to evaluate the subjective feeling of safety from switching to PP3M with regard to the Covid-19 pandemic. Only attitudes of patients were recorded, whereas surveying carers as well as clinicians may have provided further insights. The cross-sectional design of the study provides only a snapshot of patients’ perspectives and change in opinion overtime cannot be measured. The questionnaire was also only administered to patients receiving PP3M at the time and who may have had a different experience to those who discontinued therapy, although discontinuation reported by our and other studies has been particularly low.48,49 Additionally, the characteristics and viewpoints of the 15 patients (14 not contactable and 1 declined to participate) who were receiving PP3M but not involved in the study may have impacted on the overall findings. Furthermore, the age and gender distribution of the study sample, albeit quite representative of the patient population on LAIs, may reduce generalisability. For example, while there may appear to be a disproportionate gender distribution (31 males, 15 females), this is not surprising given the higher risk of schizophrenia in men, together with earlier age of onset and a worse prognosis.50 In addition, the study subjects represent a diverse ethnic background. However, other potential confounding factors such as duration of illness, level of functioning and accommodation have not been accounted for.
The co-developed survey included four straightforward questions that allowed us to easily deliver it to a population who could have some difficulties in maintaining attention and concentration due to the psychiatric disorder.51 However, a significant drawback of this study is that widely employed validated scales were not used for evaluating satisfaction, stigmatisation or QoL which may reduce comparability with future research. Finally, responses may have been subject to social desirability bias.
Conclusion
The study findings showed that the overall experience of switching from PP1M to PP3M was very positive, often leading to improved treatment persistence and quality of life as well as decreased stigma. The importance of better tolerability and enhanced safety with less frequent medication administration under pandemic conditions was also highlighted alongside the ability to enhance capacity where demand is high or provide easier access to such treatments in less developed or rural areas. The results are in line with a small, but growing, body of evidence supporting patient satisfaction and acceptance with the use of PP3M and longer-acting treatments in general.
Ethics Statement
This non-interventional study was approved as a service evaluation by the West London NHS Trust department for audit and naturalistic research (project number 1545) and therefore did not require additional research ethics committee approval. Verbal consent was gained prior to conducting the survey; obtaining written consent was not practical given the Covid-19 restrictions on face-to-face contact that were in place at the time.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship or publication of this article.
Disclosure
Dr Sofia Pappa reports grants, personal fees from Recordati, personal fees from Janssen, Sunovion and Rovi, outside the submitted work. Joshua Barnett has nothing to declare.
References
1. Olivares JM, Alptekin K, Azorin K, et al. Psychiatrists’ awareness of adherence to antipsychotic medication in patients with schizophrenia: results from a survey conducted across Europe, the Middle East, and Africa. Patient Prefer Adherence. 2013;7:121–132. doi:10.2147/PPA.S37534
2. Subotnik KL, Nuechterlein KH, Ventura J, et al. Risperidone nonadherence and return of positive symptoms in the early course of schizophrenia. Am J Psychiatry. 2011;168(3):286–292. doi:10.1176/appi.ajp.2010.09010087
3. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):822–829. doi:10.1001/jamapsychiatry.2015.0270
4. Pungor K, Sanchez P, Pappa S, et al. The Patient, Investigator, Nurse, Carer Questionnaire (PINC-Q): a cross-sectional, retrospective, non-interventional study exploring the impact of less frequent medication administration with paliperidone palmitate 3-monthly as maintenance treatment for schizophrenia. BMC Psychiatry. 2021;21:300. doi:10.1186/s12888-021-03305-z
5. Spoelstra SK, Bruins J, Bais L, et al. One-month versus three-month formulation of paliperidone palmitate treatment in psychotic disorders: patients’, relatives’, and mental health professionals’ perspectives. Patient Prefer Adherence. 2022;16:615–624. doi:10.2147/PPA.S349460
6. Ereshefsky L, Mascarenas C. Comparison of the effects of different routes of antipsychotic administration on pharmacokinetics and pharmacodynamics. J Clin Psychiatry. 2003;64(Suppl 16):18–23.
7. Lamb YN, Keatin GM. Paliperidone palmitate intramuscular 3-monthly formulation: a review in schizophrenia. Drugs. 2016;76:1559–1566. doi:10.1007/s40265-016-0645-5
8. Magnusson MO, Samtani MN, Plan EL, et al. Dosing and switching strategies for paliperidone palmitate 3-month formulation in patients with schizophrenia based on population pharmacokinetic modeling and simulation, and clinical trial data. CNS Drugs. 2017;31:273–288. doi:10.1007/s40263-017-0416-1
9. Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):830–839. doi:10.1001/jamapsychiatry.2015.0241
10. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. 2016;19(7):pyw018. doi:10.1093/ijnp/pyw018
11. Weiden PJ, Kim E, Bermak J, et al. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. 2017;78:e813–e820. doi:10.4088/JCP.16m11308
12. García-Carmona JA, Barnett J, Campos-Navarro MP, et al. Comparative effectiveness of long-acting injectable antipsychotics in a large naturalistic cohort across two European centers: findings from the long-acting injectable antipsychotics collaborative (LAICO) study. Neurosci Appl. 2022;1:100111. doi:10.1016/j.nsa.2022.100111
13. Tiihonen J, Mittendorfer-Rutz E, Majak M, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29,823 patients with schizophrenia. JAMA Psychiatry. 2017;74:686–693. doi:10.1001/jamapsychiatry.2017.1322
14. Mathews M, Gopal S, Nuamah I, et al. Clinical relevance of paliperidone palmitate 3-monthly in treating schizophrenia. Neuropsychiatr Dis Treat. 2019;15:1365–1379. doi:10.2147/NDT.S197225
15. Di Lorenzo R, Iorio A, Pinelli M, et al. Effectiveness and quality of life with paliperidone palmitate 3-monthly in comparison with other long-acting drugs. Neuropsychiatr Dis Treat. 2022;18:829–846. doi:10.2147/NDT.S356341
16. Pappa S, Barnett J, Gomme S, et al. Shared and supported decision making in medication in a mental health setting: how far have we come? Community Ment Health J. 2021;57:1566–1578. doi:10.1007/s10597-021-00780-2
17. Finnerty MT, Layman DM, Chen Q, et al. Use of a web-based shared decision-making program: impact on ongoing treatment engagement and antipsychotic adherence. Psychiatr Serv. 2018;69(12):1215–1221. doi:10.1176/appi.ps.201800130
18. Bernal JL, Andrews N, Gower C, et al. Effectiveness of Covid-19 vaccines against the B.1.617.2 (Delta) variant. N Engl J Med. 2021;385:585–594. doi:10.1056/NEJMoa2108891
19. Office of National Statistics UK. Coronavirus (COVID-19) latest insights. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19/latestinsights.
20. World Health Organisation. WHO Coronavirus (Covid-19) dashboard. Available from: https://covid19.who.int/.
21. Cullen W, Gulati G, Kelly BD. Mental health in the COVID-19 pandemic. QJM. 2020;113(5):311–312. doi:10.1093/qjmed/hcaa110
22. Rodgers M, Dalton J, Harden M, et al. Integrated care to address the physical health needs of people with severe mental illness: a mapping review of the recent evidence on barriers, facilitators and evaluations. Int J Integr Care. 2018;18(1):9. doi:10.5334/ijic.2605
23. Fernández-Miranda JJ, Díaz-Fernández S, De Berardis D, López-Muñoz F. Paliperidone Palmitate Every Three Months (PP3M) 2-year treatment compliance, effectiveness and satisfaction compared with Paliperidone Palmitate-Monthly (PP1M) in people with severe schizophrenia. J Clin Med. 2021;10(7):1408. doi:10.3390/jcm10071408
24. Blackwood C, Sanga P, Nuamah I, et al. Patients’ preference for long-acting injectable versus oral antipsychotics in schizophrenia: results from the patient-reported medication preference questionnaire. Patient Prefer Adherence. 2020;14:1093–1102. doi:10.2147/PPA.S251812
25. Lai JK, Margolese HC. A qualitative study of patient experience when switching from paliperidone palmitate once monthly (PP1M) to paliperidone palmitate three monthly (PP3M) long-acting injectable antipsychotic. Schizophr Res. 2019;204:443–444. doi:10.1016/j.schres.2018.09.012
26. Garcia-Portilla MP, Llorca PM, Maina G, et al. Symptomatic and functional outcomes after treatment with paliperidone palmitate 3-month formulation for 52 weeks in patients with clinically stable schizophrenia. Ther Adv Psychopharmacol. 2020;10:2045125320926347. doi:10.1177/2045125320926347
27. Buckley PF, Schooler NR, Goff DC, et al. Comparison of injectable and oral antipsychotics in relapse rates in a pragmatic 30-month schizophrenia relapse prevention study. Psychiatr Serv. 2016;67(12):1370–1372. doi:10.1176/appi.ps.201500466
28. Pietrini F, Albert U, Ballerini A, et al. The modern perspective for long-acting injectables antipsychotics in the patient-centered care of schizophrenia. Neuropsychiatr Dis Treat. 2018;15:1045–1060. doi:10.2147/NDT.S199048
29. Vauth R, Kleim B, Wirtz M, Corrigan PW. Self-efficacy and empowerment as outcomes of self-stigmatizing and coping in schizophrenia. Psychiatry Res. 2007;150:71–80. doi:10.1016/j.psychres.2006.07.005
30. Wahl OF. Mental health consumers’ experience of stigma. Schizophr Bull. 1999;25:467–478. doi:10.1093/oxfordjournals.schbul.a033394
31. Wright ER, Gronfein WP, Owens TJ. Deinstitutionalization, social rejection, and the self-esteem of former mental patients. J Health Soc Behav. 2000;41:68–90. doi:10.2307/2676361
32. Sibitz I, Unger A, Woppmann A, Zidek T, Amering M. Stigma resistance in patients with schizophrenia. Schizophr Bull. 2011;37(2):316–323. doi:10.1093/schbul/sbp048
33. Lysaker PH, Vohs JL, Tsai J. Negative symptoms and concordant impairments in attention in schizophrenia: associations with social functioning, hope, self-esteem and internalized stigma. Schizophr Res. 2009;110(1–3):165–172. doi:10.1016/j.schres.2009.01.015
34. Yanos PT, Roe D, Markus K, Lysaker PH. Pathways between internalized stigma and outcomes related to recovery in schizophrenia spectrum disorders. Psychiatr Serv. 2015;59:1437–1442. doi:10.1176/ps.2008.59.12.1437
35. Eack SM, Newhill CE. Psychiatric symptoms and quality of life in schizophrenia: a meta-analysis. Schizophr Bull. 2007;33(5):1225–1237. doi:10.1093/schbul/sbl071
36. Awad AG, Voruganti LN. Measuring quality of life in patients with schizophrenia. PharmacoEconomics. 2012;30:183–195. doi:10.2165/11594470-000000000-00000
37. Bobes J, Garcia-Portilla MP, Bascaran MT, Saiz PA, Bouzoño M. Quality of life in schizophrenic patients. Dialogues Clin Neurosci. 2007;9(2):215–226. doi:10.31887/DCNS.2007.9.2/jbobes
38. Narvaez JM, Twamley EW, McKibbin CL, Heaton RK, Patterson TL. Subjective and objective quality of life in schizophrenia. Schizophr Res. 2008;98(1–3):201–208. doi:10.1016/j.schres.2007.09.001
39. Najarian D, Sanga P, Wang S, et al. A randomized, double-blind, multicenter, noninferiority study comparing paliperidone palmitate 6-month versus the 3-month long-acting injectable in patients with schizophrenia. Int J Neuropsychopharmacol. 2022;25(3):238–251. doi:10.1093/ijnp/pyab071
40. Barnett J, Mason K, Pappa S. The relationship between level of compliance with aripiprazole long-acting injectable and risk of hospitalisation. Eur Neuropsychopharmacol. 2021;53(supp. 1):S354–S355. doi:10.1016/j.euroneuro.2021.10.453
41. Pappa S, Mason K. Partial compliance with long-acting paliperidone palmitate and impact on hospitalization: a 6-year mirror-image study. Ther Adv Psychopharmacol. 2020;10:204512532092478. doi:10.1177/2045125320924789
42. Seeman M. The pharmacodynamics of antipsychotic drugs in women and men. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.650904
43. Pappa S, Barnett J, Mason K. A 10-year observational study of the use, acceptability and effectiveness of long-acting paliperidone palmitate: implications for clinical decision making. CNS Drugs. 2023;37:107–116. doi:10.1007/s40263-022-00976-4
44. Pappa S, Mason K, Howard E. Long-term effects of paliperidone palmitate on hospital stay and treatment continuation. Int Clin Psychopharmacol. 2019;34(6):305–311. doi:10.1097/yic.0000000000000285
45. Dalingwater L. NHS staffing shortages and the Brexit effect. Observatoire de la société britannique. 2019;24:67–86. doi:10.4000/osb.3216
46. Iacobucci G. Covid-19: NHS trusts declare “critical incidents” because of staff shortages. BMJ. 2022;376:o3. doi:10.1136/bmj.o3
47. Pappa S, Barnett J, Berges I, Sakkas N. Tired, worried and burned out, but still resilient: a cross-sectional study of mental health workers in the UK during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(9):4457. doi:10.3390/ijerph18094457
48. Wallman P, Clark I, Taylor D. Effect of 3-monthly paliperidone palmitate on hospitalisation in a naturalistic schizophrenia cohort – a five-year mirror image study. J Psychiatr Res. 2022;148:131–136. doi:10.1016/j.jpsychires.2022.01.044
49. Wallman P, Clark I, Taylor D. Discontinuation and relapse with paliperidone palmitate three-monthly for maintenance of schizophrenia: two year follow-up of use in clinical practice. J Psychopharmacol. 2021;35(9):1091–1098. doi:10.1177/02698811211009794
50. Leung A, Chue P. Sex differences in schizophrenia, a review of the literature. Acta Psychiatr Scand Suppl. 2000;401:3–38. doi:10.1111/j.0065-1591.2000.0ap25.x
51. Schaefer J, Giangrande E, Weinberger DR, Dickinson D. The global cognitive impairment in schizophrenia: consistent over decades and around the world. Schizophr Res. 2013;150(1):42–50. doi:10.1016/j.schres.2013.07.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Personal and Social Functioning and Health-Related Quality of Life in Patients with Schizophrenia Treated with the Long-Acting Injectable Antipsychotic Risperidone ISM
Litman R, Naber D, Anta L, Martínez J, Filts Y, Correll CU
Neuropsychiatric Disease and Treatment 2023, 19:219-232
Published Date: 25 January 2023
The Effect of Longer Dosing Intervals for Long-Acting Injectable Antipsychotics on Outcomes in Schizophrenia
Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, Wang S, Richarz U, Gopal S, Kane JM
Neuropsychiatric Disease and Treatment 2023, 19:531-545
Published Date: 7 March 2023
Paliperidone Palmitate versus Risperidone Long-Acting Injectable in Patients with Schizophrenia: A Meta-Analysis of Efficacy and Safety
Zhao M, Qin B, Mao Y, Zhang Y, Zhao R, Wang A, Wang H, Zhao J, Wang C
Neuropsychiatric Disease and Treatment 2023, 19:749-757
Published Date: 5 April 2023
Efficacy and Safety of Paliperidone Palmitate 6-Month versus Paliperidone Palmitate 3-Month Long-Acting Injectable in European Patients with Schizophrenia: A Post Hoc Analysis of a Global Phase-3 Double-Blind Randomized Non-Inferiority Study
Giron‐Hernandez C, Han JH, Alberio R, Singh A, García-Portilla MP, Pompili M, Knight RK, Richarz U, Gopal S, Antunes J
Neuropsychiatric Disease and Treatment 2023, 19:895-906
Published Date: 13 April 2023
Aripiprazole Plasma Concentrations Delivered from Two 2-Month Long-Acting Injectable Formulations: An Indirect Comparison
Harlin M, Chepke C, Larsen F, Bell Lynum KS, Chumki SR, Fitzgerald H, Such P, Madera-McDonough J, Yildirim M, Panni M, Saklad SR
Neuropsychiatric Disease and Treatment 2023, 19:1409-1416
Published Date: 8 June 2023