Back to Journals » Infection and Drug Resistance » Volume 15
Sweet’s Syndrome Accompanied by Coinfection with Multiple Pathogens and Disseminated Mycobacterium phlei Infection Presenting with Osteolytic Destruction During 12 Years of Follow-Up: A Rare Case Report
Authors Tang M, Pan M, Qiu Y, Huang J, Zeng W, Zhang J
Received 26 January 2022
Accepted for publication 29 April 2022
Published 10 May 2022 Volume 2022:15 Pages 2459—2467
DOI https://doi.org/10.2147/IDR.S360063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Mengxin Tang,1,2,* Mianluan Pan,1,* Ye Qiu,1 Jie Huang,3 Wen Zeng,2 Jianquan Zhang1
1Department of Respiratory and Critical Medicine, The Eighth Affiliated Hospital, Sun Yat-Sen University, Shenzhen, Guangdong, 518000, People’s Republic of China; 2Department of Respiratory and Critical Medicine, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China; 3Department of Tuberculosis Ward, Nanning Fourth People’s Hospital, Nanning, Guangxi, 530021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Zeng, Department of Respiratory and Critical Medicine, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China, Tel +8618589883694, Fax +86771-5350031, Email [email protected] Jianquan Zhang, Department of Respiratory and Critical Medicine, The Eighth Affiliated Hospital, Sun Yat-Sen University, Shenzhen, Guangdong, 518000, People’s Republic of China, Tel +8613978123845, Fax +86755-23482484, Email [email protected]
Background: Anti-IFN-γ autoantibodies (AIGAs) are closely related to the disseminated infection of multiple pathogens. Mycobacterium phlei (M. phlei) is a nonpathogenic nontuberculous mycobacteria (NTM), and M. phlei infection of the bone is extremely rare. We report a rare case of high-titer AIGAs presenting with Sweet’s syndrome (SS) accompanied by opportunistic coinfection with multiple pathogens during 12 years of follow-up. The patient in this case also developed disseminated M. phlei infection with osteolytic destruction after treatment for SS.
Case Presentation: A 68-year-old Chinese woman was admitted to our hospital in August 2009 due to fever and cough with expectoration for 3 months. The patient was successively infected with Klebsiella pneumoniae, herpes zoster virus and Candida. Chest computed tomography (CT) showed recurrent consolidations in different lung fields. After 15 months of antimicrobial treatment, the patient experienced partial recovery. In September 2010, the patient was pathologically diagnosed with SS due to the presence of multiple rashes. After prednisone and thalidomide treatment, the rashes subsided, and the pulmonary lesions had completely absorbed. In May 2011, the patient was diagnosed with disseminated tuberculosis and was administered anti-tuberculosis therapy for 3 months without improvement. NTM was subsequently cultured from her sputum and chest wall pus, and she improved after 20 months of anti-NTM therapy. In March 2016, the patient developed osteolytic destruction of the C7-T2 vertebral bodies with a back abscess. NTM was eventually cultured from the dorsal abscess pus and further identified as M. phlei. High-titer AIGAs were detected in the patient’s serum. After another round of aggressive anti-NTM therapy, the patient was finally cured.
Conclusion: Patients with AIGA-associated anti-cytokine autoantibody disease can present with multiple opportunistic infections and SS involving the lung. AIGA-associated immunodeficiency leads to infection with nonpathogenic M. phlei, which is refractory, can cause relapse, and even leads to osteolytic destruction.
Keywords: Mycobacterium phlei, sweet’s syndrome, osteolytic destruction, anti-IFN-γ autoantibodies
Introduction
Anti-IFN-γ autoantibodies (AIGAs) is an anti-cytokine autoantibody disease (ACAD), and the immunodeficiency caused by AIGAs was first defined as adult-onset immunodeficiency (AOID) in 2012.1 In 2019, the International Union of Immunological Societies Expert Committee updated the classification of innate/primary immunodeficiencies. AOID associated with AIGAs belongs to the autoimmune phenotype of primary immunodeficiency.2 AIGAs are closely associated with severe disseminated infections, which can be due to multiple intracellular pathogens, such as nontuberculous mycobacteria (NTM), Salmonella typhi, varicella-zoster virus and Candida, and high titers of AIGAs are strongly associated with the severity, prognosis and recurrence of infections.3–5 In AIGA-associated AOID patients with NTM infection, the occurrence of Sweet’s Syndrome (SS) has attracted increasing attention in the clinic. SS can occur concurrently with NTM infection or before or after NTM infection.6 These phenomena suggest that SS may be a clinical phenotype of AIGA-related ACAD. Mycobacterium phlei (M. phlei) is a nonpathogenic, rapidly growing mycobacterium (RGM) that rarely causes human diseases.7 Herein, we report a rare case with 12 years of follow-up who first presented with SS accompanied by opportunistic infections with multiple pathogens. After hormone treatment for SS, the patient developed disseminated M. phlei infection with osteolytic destruction. The presence of high titers of AIGAs was finally confirmed in the patient’s serum.
Case Presentation
A 68-year-old Chinese female kindergarten teacher with a history of hypothyroidism after hyperthyroidism treatment was admitted to our hospital in September 2010 due to cough, expectoration and fever for 15 months and a rash for 1 month. At the end of May 2009, she first developed cough with expectoration accompanied by fever, and her highest body temperature was 39°C. Chest computed tomography (CT) revealed consolidation in the right lower lobe. The patient showed no obvious improvement after treatment at a local hospital. She was first hospitalized at our hospital in August 2009. Routine blood examination showed a white blood cell (WBC) count of 11 ×109/L, a neutrophil count of 8.6×109/L and a hemoglobin concentration of 62 g/L. The C-reactive protein (CRP) concentration and erythrocyte sedimentation rate (ESR) were 38.7 mg/L and 105 mm/h, respectively. Chest CT revealed pneumonia in the middle and lower lobes of the right lung, and Klebsiella pneumoniae was identified in the sputum. She was treated with antibiotics and was discharged after her symptoms improved. In October 2009, the patient experienced a recurrence of the above symptoms accompanied by herpes zoster on the right chest wall. Chest CT revealed progressive pulmonary lesions with new consolidation in the apicoposterius segment of the upper lobe of the right lung, and Candida albicans was identified in the sputum. Routine blood examination revealed a WBC count of 23.5×109/L, a neutrophil count of 19.8×109/L, and a hemoglobin concentration of 68 g/L. The CRP concentration and ESR were 91.3 mg/L and 69 mm/h, respectively. The patient was treated with clindamycin, cefoperazone sulbactam, fluconazole and ganciclovir as prescribed. Repeated chest CT revealed that the pulmonary lesions and pleural effusion were slightly absorbed, and the patient was discharged and returned to her local hospital for continuous treatment. In September 2010, the patient was admitted to our hospital for the third time due to fever, cough with expectoration and scattered herpes of various sizes on her limbs for one month. She had lost 15 kg since the onset of illness.
The physical examination after admission revealed a body temperature of 38°C; the presence of painful erythematous papules studded with white blisters on her palms, back of the hands, fingers, face and limbs (Figure 1); bilateral axillary and inguinal lymphadenopathy; and moist rales in the bilateral lungs. Routine blood examination revealed that her WBC count, neutrophil count, lymphocyte count and hemoglobin concentration were 24.24×109/L, 20.07×109/L, 2.16×109/L and 85 g/L, respectively. The concentrations of CRP, albumin, globulin, serum immunoglobulin (Ig) G, IgA and IgM were 182 mg/L, 26.2 g/L, 45.9 g/L, 24.53 g/L, 2.64 g/L and 1.38 g/L, respectively. The percentages of total T cells, CD4+ T cells and CD8+ T cells, and CD4/CD8 cells were 50.9%, 29.3%, 17.4% and 1.6, respectively. The levels of creatinine and urea nitrogen were 51 µmol/L and 2.4 mmol/L, respectively. In addition, her transaminase, tumor markers, rheumatoid factor, and anti-Streptococcus hemolysin O were all within normal ranges, and she was negative for plasma human immunodeficiency virus (HIV) antibodies. The results of bone marrow aspiration biopsy suggested iron deficiency anemia. Her lung function test revealed that her forced expiratory volume in the first second (FEV1) was 76.9%, her FEV1/forced vital capacity (FVC) was 78.13%, and her carbon monoxide transfer factor (TLCO) was 46.7%, suggesting mild restrictive ventilatory dysfunction and diffusion disorder. Chest CT showed consolidation and exudation in the apicoposterior segment of the upper lobe and in the posterior basal segment of the lower lobe of the left lung, and a large amount of pleural effusion was noted on the left side. Cytological and biochemical examination of the pleural effusion showed that her total cell count, percent of segmented cells, percent of lymphocytes, adenosine deaminase, and protein concentration were 140×106/L, 70%, 30%, 3.8 U/L, and 37 g/L, respectively. Her Rivalta test was positive, and the effusion was proven to be exudative. Histopathology of the rashes and the lymph node biopsy specimen obtained from the patient confirmed SS (Figure 2). Candida was repeatedly isolated from the sputum, while microbial cultures of the blood and alveolar lavage fluid were negative. In addition, there were no abnormal findings on bronchoscopy. Following treatment with vancomycin, moxifloxacin, cefoperazone, fluconazole and dexamethasone during hospitalization, the patient’s symptoms improved, and the rash subsided. Repeated routine blood tests showed a WBC count of 12.4×109/L, a neutrophil count of 7.92×109/L and a hemoglobin concentration of 108 g/L. Chest CT showed absorption of the pulmonary lesions and pleural effusion. The patient was discharged from the hospital on October 20, 2010. She was continuously treated with oral prednisone and thalidomide outside the hospital, and her condition was stable However, the patient was admitted to the People’s Hospital of Guangxi Zhuang Autonomous Region due to a pulmonary fungal infection and SS and was hospitalized from March 2011 to May 2011. Her specific process of diagnosis and treatment was unknown, and she was discharged after her condition improved.
 |
Figure 1 Painful erythematous papules studded with white blisters on the patient’s left face (A) and right axillary skin (B). |
 |
Figure 2 Histopathology examination of a skin lesion showing dense infiltrates throughout the dermis (hematoxylin-eosin, original magnification ×100; original magnification ×200) (A and B). The infiltrate was predominantly composed of neutrophils (hematoxylin-eosin staining, original magnification x 400) (C). |
On May 21, 2011, the patient was admitted to the Nanning Fourth People’s Hospital due to cough with expectoration, subcutaneous abscesses on her left chest wall and several palpable soybean-sized lymph nodes on her neck bilaterally. She was diagnosed with bilateral pulmonary tuberculosis and a tuberculous abscess of the left chest wall based on chest CT and was administered anti-tuberculosis therapy for 3 months without clinical improvement. Her chest wall abscess continued to ulcerate and discharge pus and did not heal. Routine blood examination revealed a WBC count of 8.14×109/L, a neutrophil count of 6.07×109/L and a hemoglobin concentration of 75.20 g/L. On August 3, 2011, the culture results of the patient’s sputum and chest wall pus were available, and the patient was confirmed to be positive for NTM (unclassified) culture. Based on the results of the antimicrobial susceptibility test (AST) (para-aminosalicylic acid, streptomycin, capreomycin, protionamide, amikacin: R; isoniazide: I; rifampicin, ethambutol, levofloxacin: S), she received combination treatment with isoniazid, rifapentine, ethambutol, and levofloxacin for more than 1 month. Her WBC count, neutrophil count and hemoglobin concentration were 7.58×109/L, 5.42×109/L and 88.7 g/L, respectively. She was discharged after her symptoms improved. She regularly took anti-NTM agents outside the hospital with regular follow-up, and her chest wall lesion had completely healed after 6 months. Repeated routine blood examination showed that her WBC count and hemoglobin concentration were 5.51×109/L and 113 g/L, respectively. The patient was maintained on anti-NTM therapy until December 1, 2012. On March 16, 2013, the patient was admitted to the hospital again due to cough, expectoration and anorexia. Routine blood examination after admission showed a WBC count of 8.98×109/L, a neutrophil count of 6.26×109/L and a hemoglobin concentration of 68.2 g/L. The albumin concentration and ESR were 27.9 g/L and 142 mm/h, respectively. Chest CT revealed exacerbation of her pulmonary lesions, with mottled and linear high-density shadows observed in both lungs. Due to a positive sputum smear for acid-fast bacilli, a recurrence of NTM infection was considered, and clarithromycin was added to the original regimen. The patient’s condition improved again, and she was transferred to the outpatient department for treatment. Repeated laboratory tests on January 24, 2015 revealed that her WBC count, hemoglobin concentration, CD3+ T-cell count, CD4+ T-cell count, CD8+ T-cell count, albumin concentration and A/G were 7.20×109/L, 118 g/L, 1109 cells/μL, 686 cells/μL, 397 cells/μL and 1.17, respectively. Her liver and kidney functions were normal. Chest CT showed absorption of her pulmonary lesions, and she subsequently discontinued anti-NTM treatment.
In March 2016, 1 year after the discontinuation of anti-NTM therapy, the patient was readmitted to the hospital with a back abscess that had continued to ulcerate and discharge pus for 1 month. Physical examination after admission revealed cervical lymph node enlargement, a few moist rales in the left lower lobe and soft tissue swelling in the upper back. On the left side of the spinous processes of the C7-T1 vertebral bodies, a skin ulcer with a diameter of approximately 0.6 cm and a sinus tract with granulation tissue and purulent exudation (leading to the vicinity of the spinous process of the C7-T1 vertebral bodies, which was approximately 3.5 cm deep) were observed. Her WBC count, hemoglobin concentration, CRP concentration, ESR and A/G were 7.43×109/L, 114 g/L, 8.3 mg/L, 38 mm/h and 0.92, respectively. Serum AIGAs were determined by an enzyme-linked immunosorbent assay (ELISA) kit (Cloud-Clone Corp, Wuhan, China), and the AIGA titer was 79276.59 ng/mL (the cutoff value of the AIGA titers was 9583.21 ng/mL).4 Chest CT showed increased pulmonary lesions with multiple patchy exudations, fibrous proliferation and ground glass opacity in both lungs and bronchiectasis in the dorsal segment of the left lower lobe (Figure 3A). Bone CT revealed bony destruction in C7-T2 vertebral bodies with surrounding abscess formation (Figure 3B–D). NTM were cultured from the pus obtained from the patient’s back abscess, and NTM were further identified as M. phlei using the indirect homologous gene method (gene chip). Given that her AST results were the same as before, the patient continued treatment with the original regimen. Furthermore, the patient underwent local sinus tract grabbing. Three months later, the bone destruction had gradually repaired, the surrounding abscess had disappeared, and the skin ulcer and sinus tract had healed. The patient was discharged and remained on treatment with the above regimen, showing gradual improvement. In July 2017, repeated chest CT showed that the pulmonary lesions were absorbed (Figure 3E). Repeated bone CT showed that the bone destruction had further repaired, and the surrounding abscess had disappeared (Figure 3F–H). No lymph node enlargement was found. Routine blood examination revealed a normal WBC count of 5.06×109/L and a normal hemoglobin concentration of 141 g/L. Her CRP concentration and ESR were within the normal range. In April 2018, the patient returned to the hospital for re-examination, and her clinical indicators showed normal results. The patient was cured after 2 years of regular anti-NTM therapy with no recurrence noted at present.
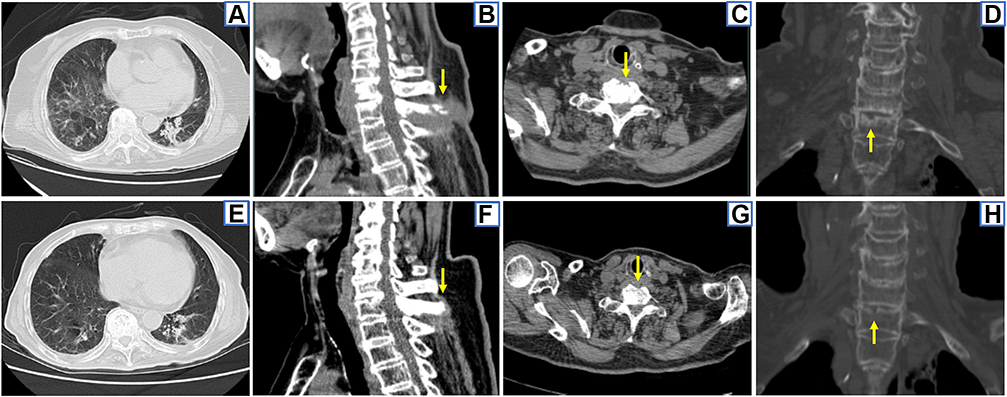 |
Figure 3 CT findings. 2016–3 chest CT showed multiple patchy exudations, fibrous proliferation and ground glass opacity in both lungs, bronchiectasis in the dorsal segment of the left lower lobe and pleural thickening (A). 2016–3 bone CT showed irregular bone destruction of the lower border of the C7 vertebral body, the upper border of the T1 vertebral body and its spinous process, bone defect of the anterior border of the T1 vertebral body, with surrounding abscess and the narrowing of the C7-T1 intervertebral space (arrows) (B–D). 2017–7 chest CT showed absorption of pulmonary lesions after anti-NTM therapy (E). 2017–7 bone CT shows the repair of bone destruction in C7-T1 vertebral bodies and the disappearance of the surrounding abscess after anti-NTM therapy (arrows) (F–H). |
Discussion
SS, which is also known as acute febrile neutrophilic dermatosis, was first reported in 1964 by Robert Douglas Sweet.8 SS can be secondary to malignant tumors or drugs, and there have also been cases of idiopathic SS related to infection. However, the pathogenesis remains unclear.9 Mizoguchi et al10 reported that the frequency of HLA-B54 was significantly higher in Japanese patients with SS (46.4%) than in healthy controls (14.4%), suggesting that the increased frequency of HLA-B54 is involved in its pathogeneses. A painful, red, pseudoblister-like rash is the earliest and most prominent clinical manifestation of SS. However, idiopathic SS, which first presents with pulmonary involvement preceding the appearance of the rash, has also been reported in the literature. The clinical characteristics of idiopathic SS are summarized as follows:11 (1) Patients with idiopathic SS usually present with significant increases in their WBC count, neutrophil count, ESR and CRP concentration, and these patients usually present with unilateral or bilateral pulmonary infiltrative exudation or consolidation with pleural reaction on chest CT as well as lymph node enlargement. (2) Histopathological analysis of the lung tissue specimens obtained from patients with idiopathic SS demonstrated interstitial pneumonia with neutrophil infiltration or accompanied by organizing pneumonia, which was consistent with the histopathological results of the rash. (3) Idiopathic SS is easily misdiagnosed as pneumonia, and it can be cured by hormone therapy rather than antibiotics. The condition is prone to recur and can cause death. The patient in our study presented with fever; markedly increased inflammatory markers of WBC count, neutrophil count and ESR; and repeated consolidation in different lung fields. She was repeatedly diagnosed with bacterial pneumonia and received antimicrobial treatment for 15 months, during which her condition partially improved. Hormone therapy was also irregularly administered during the course of the patient’s disease, and she eventually developed typical rashes. Histopathological examination of the rashes confirmed skin lesions with neutrophilic infiltration in the superficial and middle dermis, and the patient was definitively diagnosed with idiopathic SS involving the lungs, which is a rare clinical type of SS.
Six months later, the patient developed cervical lymphadenopathy, subcutaneous abscesses in the chest wall and increased lung lesions. She was diagnosed with disseminated tuberculosis but did not respond to anti-tuberculosis treatment. NTM was eventually cultured from her sputum and pus of the chest wall abscess. However, due to technical limitations, the specific NTM subspecies could not be identified. Based on the AST results, she was administered anti-NTM therapy and showed significant improvement after treatment. One and a half years later, the patient presented with a worsening cough, expectoration and anemia. In addition, inflammatory markers elevated in her serum and acid-fast bacilli were detected in her sputum. Considering that she could have a recurrence of NTM, clarithromycin was added. She continued to receive anti-NTM therapy for 22 months and then discontinued treatment upon clinical improvement. Unfortunately, one year after the discontinuation of anti-NTM therapy, the patient developed osteolytic destruction of the C7-T2 vertebral bodies with surrounding abscesses and dorsal sinus tract formation. She showed mild systemic symptoms and an inflammatory response but no fever, cough or expectoration. NTM was cultured from the pus of the dorsal abscess and was further identified as Mycobacterium phlei. The AST results were the same as before; thus, she continued therapy with a combination of isoniazid, rifapentine, ethambutol, levofloxacin and clarithromycin and was cured after 2 years. According to previous literature reports, osteolytic destruction caused by NTM infection is not rare. However, due to the insufficient recognition of this condition by clinicians, routine examination of the bones in patients with disseminated NTM infection is often not performed unless severe ostealgia occurs. NTM can affect any bone of the body, manifesting as multiple osteolytic destructions. Radiography and CT showed moth-eaten or irregular bone destruction, bone defects, pathological fractures and periosteal proliferation. Bone ECT showed significantly increased radioactive concentration in multiple bones, while positron emission tomography (PET)/CT showed metabolic activity in multiple bones of the body.12 Furthermore, the most frequently isolated NTM species currently reported in bone and joint NTM infections are slowly growing mycobacterium, which are mainly composed of Mycobacterium avium complex (MAC). In addition, rapidly growing mycobacteria (RGM), such as M. fortuitum and M. abscessus, have also been reported.13,14 M. phlei is an RGM that was previously considered a nonpathogenic NTM and rarely causes diseases in humans.7 Since 1994, six English studies with detailed information on M. phlei infections have been reported, and a total of 6 patients were identified, including 2 patients with postoperative infection and 1 patient with a catheter-related infection. Among the six patients, only one presented with disseminated infection. M. phlei can affect multiple organs, such as the lungs, bones, lymph nodes, peritoneum, synovial fluid, synovium and muscles, and can cause pacemaker infections.7,15 Of the 2 reported patients with M. phlei infections involving the bones, one patient presented with multiple osteolytic destructions due to disseminated infection. This patient had ostealgia, and PET/CT showed bone destruction and metabolic activity in the anterior spinal cord, sacrum, iliac bone, pubic bone, ischium, sternum, scapula, ribs, clavicle and femur. The patient was cured after 26 months of anti-NTM therapy.7 The other patient had a postoperative NTM infection after lumbar fusion, presenting with chronic low back pain and bilateral lower extremity radicular symptoms. The patient’s symptoms completely resolved after anti-NTM therapy combined with the removal of multiple implants, debridement and drainage, and internal fixation.15 However, the patient in our study had no ostealgia; in addition, she also had a paravertebral abscess and sinus tract formation, which was relatively rare in the previously reported cases of NTM infection with bone involvement. After a long course of anti-NTM therapy, the osteolytic destruction in this patient had gradually repaired, and the surrounding abscess gradually disappeared.
This report focuses on a patient with 12 years of follow-up who first presented with SS, followed by opportunistic infections with Klebsiella pneumoniae, herpes zoster virus and Candida. Six months later, the patient developed a disseminated M. phlei infection. However, during the treatment for NTM infection, repeated T-lymphocyte subpopulation analysis showed that the CD3+ T-cell counts, CD4+ T-cell counts and CD8+ T-cell counts in this patient were normal, and the plasma HIV antibody test was negative. However, the patient experienced clinical relapse with osteolysis as the prominent manifestation, which is a rare clinical feature. These clinical features often suggest the possibility of a severe underlying immunodeficiency in this patient. It has been confirmed in the literature that AOID associated with AIGAs is strongly associated with infection, recurrence and the prognosis of multiple intracellular pathogens including NTM.3,4,16
Since AIGAs were first reported to be associated with disseminated NTM infection in HIV-negative individuals in 2004,17 AIGAs have been regarded as an important susceptibility factor for HIV-negative individuals infected with NTM,18 and high titers of AIGAs are highly related to NTM severity, prognosis and recurrence.16 Subsequent studies have found that AIGAs are closely related to severe disseminated opportunistic infections caused by multiple intracellular pathogens.19 In addition, disseminated NTM infection (dNTMI) of bone leading to multiple osteolytic destructions frequently occurs in patients with positive AIGAs.12 SS is associated with various diseases, among which NTM infection-related SS is the most common. Chaowattanapanit et al9 reported that NTM infection accounted for 70.9% of all SS occurrences in Thailand, especially in northeastern Thailand. NTM infection complicated with SS mostly occurs in AIGA-positive patients, and SS predominantly occurs simultaneously with NTM infection. SS can also occur before or after an NTM infection.6 A recent study found that AIGAs directly contribute to the occurrence of SS and can indirectly mediate the occurrence of SS through dNTMI. Meanwhile, the combined effect of both AOID and dNTMI further promotes the prevalence of SS.20 Therefore, SS is considered to be a clinical phenotype of AOID due to AIGAs. In this case, SS occurred prior to disseminated M. phlei infection, and the patient did not reappear with the typical rashes of SS during her clinical course of multiple recurrences of NTM infection. Therefore, we consider that the occurrence of SS in this case may not be related to NTM infection; the SS in this patient may be a clinical phenotype of ACAD due to high-titer AIGAs. According to previous literature reports, the most common subspecies of disseminated NTM disease in AOID patients is MAC.18 The most common NTM subspecies of SS-associated NTM infections is RGM, especially M. abscessus.9 M. phlei is an RGM, and disseminated M. phlei infection complicated with SS in AIGA-positive patients is very rare. Our study is the first to report a patient with this condition.
From the 12-year consultation process of the patient, we can summarize the following experience. Idiopathic SS with pulmonary involvement as the first manifestation requires clinical attention and awareness. The pathogenesis of SS is unknown. We cannot exclude the notion that SS is a clinical phenotype of high-titer AIGA-related ACAD and that the multiple infections of the patient are also related to AIGA-related ACAD. SS, herpes zoster virus, Candida, NTM, osteolysis and recurrent infections have been demonstrated to be associated with increased AIGAs;3,5,12 thus, routine testing for AIGAs is clinically recommended for patients with these conditions. For the treatment of rare subspecies of RGM, such as an M. phlei infection, a combination regimen of multiple antibiotics dominated by macrolides (based on AST) is preferred according to the guidelines.21 If the patient is confirmed to have high titers of AIGAs in the serum, the duration of anti-NTM treatment should be longer than 2 years. It is better to dynamically monitor the titers of AIGAs and inflammatory indicators to determine the clinical prognosis as early as possible. For AIGA-positive patients showing persistent or recurrent infections despite aggressive anti-NTM therapy, immunotherapy for AIGAs should be considered. Several studies have reported that immunosuppressive agents such as anti-CD20 monoclonal antibodies and cyclophosphamide can effectively reduce AIGA titers and have achieved favorable clinical outcomes in patients with refractory NTM infections.22,23 However, the detection of AIGAs in the patient serum was not considered until March 2016, when the patient was finally confirmed to have high titers of AIGAs. Furthermore, the patient showed a good response to anti-NTM therapy in 2016, so she did not receive immunotherapy for AIGAs throughout the clinical course.
There were some limitations in our case study. First, as a retrospective case study, the medical records and imaging data of the patient were incomplete or not sufficiently detailed. Furthermore, due to the long disease course and repeated visits to multiple hospitals, the specific dosage of some therapeutic drugs was unclear. Second, clinicians do not have a deep understanding of SS with pulmonary involvement as the first manifestation and often consider that it is caused by infection, resulting in a delayed diagnosis. Third, AOID due to AIGAs has gained attention only in recent years; thus, the titers of AIGAs in the patient serum were not detected during the early phase of the clinical course due to the insufficient recognition of the syndrome by clinicians at that time.
Conclusions
Patients with AIGA-associated anti-cytokine autoantibody disease can experience coinfection with multiple opportunistic pathogens, such as Klebsiella pneumoniae, herpes zoster virus, Candida and NTM. Patients with this syndrome can also develop SS, with SS involving the lung being a rare type. AIGA-associated immunodeficiency leads to infection with nonpathogenic M. phlei, which is refractory, can cause relapse and can even lead to osteolytic destruction.
Abbreviations
AIGAs, anti-IFN-γ autoantibodies; ACAD, anti-cytokine autoantibody disease; AOID, adult-onset immunodeficiency; AST, antimicrobial susceptibility testing; NTM, nontuberculous mycobacteria; SS, sweet’s syndrome; M. phlei, Mycobacterium phlei; RGM, rapidly growing mycobacterium; CT, computed tomography; WBC, white blood cell; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HIV, human immunodeficiency virus; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; TLCO, carbon monoxide transfer factor; MAC, Mycobacterium avium complex; PET, positron emission tomography; dNTMI, disseminated NTM infection.
Data Sharing Statement
All the data are fully available without restriction.
Ethics Approval and Informed Consent
This study was approved by the Faculty of Medicine at The First Affiliated Hospital of Guangxi Medical University to publish the case details [2021 (KY-E-004)]. All patients or the patients’ parents provided written informed consent for publication of this case report and any accompanying images. The study was carried out in accordance with the principles of the Declaration of Helsinki. The first author vouches for the completeness and accuracy of the data and for the adherence of the study to the protocol.
Consent for Publication
Signed consent was obtained for the publication of the case details from the participant.
Acknowledgments
We have not received substantial contributions from nonauthors.
Author Contributions
All authors contributed to the study conception and design, execution, acquisition of data (imaging features), analysis, and interpretation; drafted and revised the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Natural Science Foundation of China (NSFC 82060364 and 81760010), the Science and Technology Department of Guangxi Zhuang Autonomous Foundation of Guangxi Key Research and Development Program (No. GuikeAB20238025), and Guangxi Natural Science Foundation (NO. 2021GXNSFBA220064).
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Browne SK, Burbelo PD, Chetchotisakd P, et al. Adult-onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367(8):725–734. doi:10.1056/NEJMoa1111160
2. Tangye SG, Al-Herz W, Bousfiha A, et al. Human inborn errors of immunity: 2019 update on the classification from the international union of immunological societies expert committee. J Clin Immunol. 2020;40(1):24–64. doi:10.1007/s10875-019-00737-x
3. Browne SK. Anticytokine autoantibody-associated immunodeficiency. Annu Rev Immunol. 2014;32:635–657. doi:10.1146/annurev-immunol-032713-120222
4. Zeng W, Qiu Y, Tang S, Zhang J, Pan M, Zhong X. Characterization of anti–interferon-γ antibodies in HIV-negative patients infected with disseminated talaromyces marneffei and Cryptococcosis. Open Forum Infect Dis. 2019;6(10):ofz208. doi:10.1093/ofid/ofz208
5. Hong GH, Ortega-Villa AM, Hunsberger S, et al. Natural history and evolution of anti-interferon-gamma autoantibody-associated immunodeficiency syndrome in Thailand and the United States. Clin Infect Dis. 2020;71(1):53–62. doi:10.1093/cid/ciz786
6. Jutivorakool K, Sittiwattanawong P, Kantikosum K, et al. Skin manifestations in patients with adult-onset immunodeficiency due to anti-interferon-gamma autoantibody: a relationship with systemic infections. Acta Derm Venereol. 2018;98(8):742–747. doi:10.2340/00015555-2959
7. Tanaka S, Hoshino Y, Sakagami T, Fukano H, Matsui Y, Hiranuma O. Pathogenicity of Mycolicibacterium phlei, a non-pathogenic nontuberculous Mycobacterium in an immunocompetent host carrying anti-interferon gamma autoantibodies: a case report. BMC Infect Dis. 2019;19(1):454. doi:10.1186/s12879-019-4050-z
8. Sweet RD. An acute febrile neutrophilic dermatosis. Br J Dermatol. 1964;76:349–356. doi:10.1111/j.1365-2133.1964.tb14541.x
9. Chaowattanapanit S, Choonhakarn C, Chetchotisakd P, Sawanyawisuth K, Julanon N. Clinical features and outcomes of sweet’s syndrome associated with non-tuberculous Mycobacterial infection and other associated diseases. J Dermatol. 2016;43(5):532–536. doi:10.1111/1346-8138.13167
10. Mizoguchi M, Matsuki K, Mochizuki M, et al. Human leukocyte antigen in sweet’s syndrome and its relationship to behçet’s disease. Arch Dermatol. 1988;124(7):1069–1073. doi:10.1001/archderm.1988.01670070057019
11. Yang M, Zhang J, He Z, et al. Lung involvement of 3 cases of idiopathic sweet syndrome and literature review. Zhonghua Jie He He Hu Xi Za Zhi. 2015;38(8):589–594.
12. Tang M, Huang J, Zeng W, et al. Retrospective analysis of 10 cases of disseminated nontuberculous Mycobacterial disease with osteolytic lesions. Infect Drug Resist. 2021;14:4667–4679. doi:10.2147/IDR.S337956
13. Kim CJ, Kim UJ, Kim HB, et al. Vertebral osteomyelitis caused by non-tuberculous mycobacteria: predisposing conditions and clinical characteristics of six cases and a review of 63 cases in the literature. Infect Dis. 2016;48(7):509–516. doi:10.3109/23744235.2016.1158418
14. Kim JH, Jung IY, Song JE, et al. Profiles of extrapulmonary nontuberculous Mycobacteria infections and predictors for species: a multicenter retrospective study. Pathogens. 2020;9(11):949. doi:10.3390/pathogens9110949
15. McGee AW Jr, Dean CS, Ignatiuk A, Savelli C, Kleck CJ. Mycobacterium phlei vertebral osteomyelitis. J Am Acad Orthop Surg Glob Res Rev. 2019;3(12):
16. Chi CY, Lin CH, Ho MW, et al. Clinical manifestations, course, and outcome of patients with neutralizing anti-interferon-gamma autoantibodies and disseminated nontuberculous mycobacterial infections. Medicine. 2016;95(25):e3927. doi:10.1097/MD.0000000000003927
17. Döffinger R, Helbert MR, Barcenas-Morales G, et al. Autoantibodies to interferon-gamma in a patient with selective susceptibility to mycobacterial infection and organ-specific autoimmunity. Clin Infect Dis. 2004;38(1):e10–e14. doi:10.1086/380453
18. Valour F, Perpoint T, Senechal A, et al. Interferon-gamma autoantibodies as predisposing factor for nontuberculous mycobacterial infection. Emerg Infect Dis. 2016;22(6):1124–1126. doi:10.3201/eid2206.151860
19. Chawansuntati K, Rattanathammethee K, Minireview: WJ. Insights into anti-interferon-gamma autoantibodies. Exp Biol Med. 2021;246(7):790–795. doi:10.1177/1535370220981579
20. Kiratikanon S, Phinyo P, Rujiwetpongstorn R, et al. Adult-onset immunodeficiency due to anti-interferon-gamma autoantibody-associated sweet syndrome: a distinctive entity. J Dermatol. 2022;49(1):133–141. doi:10.1111/1346-8138.16202
21. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous Mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416. doi:10.1164/rccm.200604-571ST
22. Laisuan W, Pisitkun P, Ngamjanyaporn P, Suangtamai T, Rotjanapan P. Prospective pilot study of cyclophosphamide as an adjunct treatment in patients with adult-onset immunodeficiency associated with anti-interferon-γ autoantibodies. Open Forum Infect Dis. 2020;7(2):ofaa035. doi:10.1093/ofid/ofaa035
23. Koizumi Y, Sakagami T, Nishiyama N, et al. Rituximab restores IFN-γ-STAT1 function and ameliorates disseminated Mycobacterium avium infection in a patient with anti-interferon-γ autoantibody. J Clin Immunol. 2017;37(7):644–649. doi:10.1007/s10875-017-0425-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.