")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Suspected Rivaroxaban-Induced Anaphylaxis Secondary to Ingestion of Rivaroxaban and Nimesulide Without Cross-Reactivity to Dabigatran – A Case Report
Authors Gumbis G, Česnavičiūtė I, Didžiokaitė G, Gegeckienė D, Kvedarienė V
Received 17 March 2023
Accepted for publication 30 June 2023
Published 9 October 2023 Volume 2023:16 Pages 1133—1138
DOI https://doi.org/10.2147/JAA.S413057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Gediminas Gumbis,1 Inga Česnavičiūtė,1 Gabija Didžiokaitė,1,2 Daiva Gegeckienė,3 Violeta Kvedarienė4,5
1Faculty of Medicine, Vilnius University, Vilnius, Lithuania; 2Institute of Clinical Medicine, Faculty of Medicine, Vilnius University Clinic of Obstetrics and Gynaecology, Vilnius University, Vilnius, Lithuania; 3Centre of Cardiology, Vilnius University Hospital Santaros Klinikos, Vilnius, Lithuania; 4Institute of Biomedical Sciences, Faculty of Medicine, Vilnius University, Vilnius, Lithuania; 5Centre of Innovative Allergology, Vilnius, Lithuania
Correspondence: Gediminas Gumbis, Faculty of Medicine, Vilnius University, M. K. Čiurlionio g. 21, Vilnius, LT-03101, Lithuania, Tel +37060680714, Email [email protected]
Abstract: Here, we describe a case of anaphylaxis secondary to rivaroxaban in a 61-year-old woman 24 hours after orthopedic surgery. 10– 15 minutes after ingestion of rivaroxaban and nimesulide, the patient’s palms started itching, her face and lips swelled, her face flushed, she developed shortness of breath and subsequently lost consciousness. Serum tryptase levels at the time of the anaphylactic reaction were elevated, with subsequent measurement one month later returning a value within the normal range. Dabigatran and meloxicam were identified as suitable alternative drugs by oral provocation at an allergy clinic. Even though rivaroxaban rarely causes serious allergic reactions, when prescribing it, it is important to analyze patients’ medical history for possible previously experienced drug-induced allergic reactions and to be aware of the risks of possible undesired drug interactions.
Keywords: Xarelto, anticoagulant, DOAC, adverse drug reaction, allergy
Introduction
Anticoagulants, also sometimes referred to as blood thinners, are a class of drugs that prevent blood coagulation. These drugs are used to prevent or reduce the progression of thromboembolic disorders: eg, strokes, deep vein thrombosis (DVT), and pulmonary embolism. There are three main types of anticoagulants: low molecular weight heparins (LMWHs), vitamin K antagonists (eg, warfarin), and direct oral anticoagulants (DOACs). The use of DOACs has rapidly increased in recent years while the use of warfarin decreased due to DOACs exhibiting more predictable pharmacokinetic profiles, less variability in response, decreased coagulation monitoring, and either similar or lower risk of major bleeding events.1–4
Rivaroxaban is one of the most used DOACs approved by the United States Food and Drugs Administration in 2011; for the past few years, it has also been frequently used in Lithuania.5 The drug is the first orally administered inhibitor of factor Xa.5 Rivaroxaban interacts with factor Xa, disrupting the conversion of prothrombin to thrombin.5
Even though adverse reactions caused by rivaroxaban are relatively rare, there are now case reports of various adverse reactions caused by the drug (Table 1). These include eosinophilia, urticaria, angioedema, rashes, anaphylaxis, etc. (Table 1).6–19 Anaphylaxis secondary to rivaroxaban administration, is a rare condition, estimated to occur in about 0.01% of patients.20 There are few previous cases of this condition in the literature.8 Despite the rarity of the condition, it is essential to consider the possibility of rivaroxaban-induced anaphylaxis when prescribing the drug.
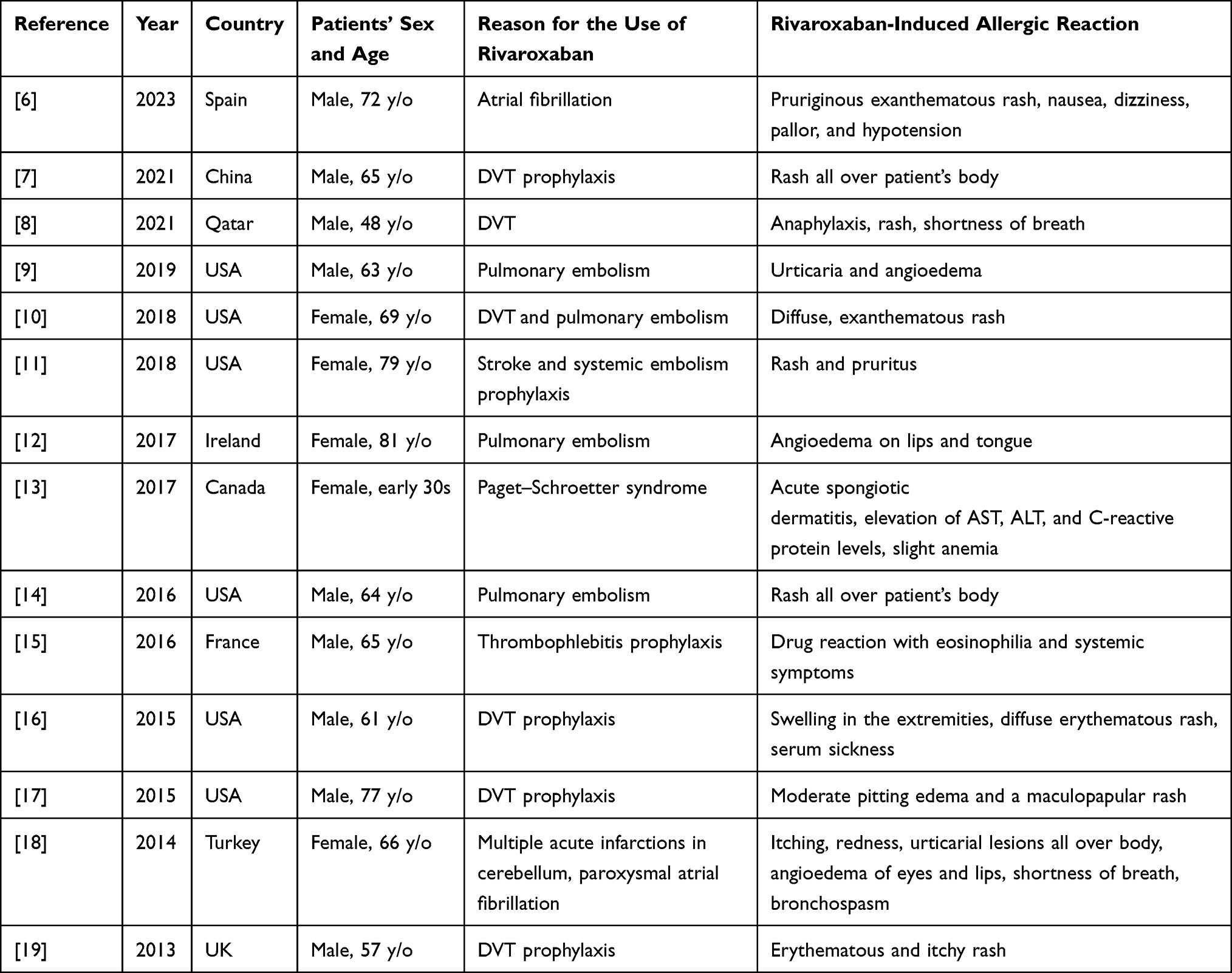 |
Table 1 Summary of Previously Reported Rivaroxaban-Induced Allergic Reactions |
Nimesulide is an NSAID, a cyclooxygenase-2 (COX-2) inhibitor.21 However, its mechanism of action is not yet fully clear as other, not yet identified aspects of its mechanism are suspected to also be involved.22 NSAIDs were identified by previous studies to be the major cause of drug-induced anaphylaxis, however they can also cause delayed-type allergic reactions.20,23 Nimesulide-induced anaphylaxis is also reported in the literature.24
In this article, we present a case of anaphylaxis caused by rivaroxaban in a female patient. Even though we suspect that the cause of the severe allergic reaction in our patient was rivaroxaban, the patient ingested both rivaroxaban and nimesulide prior to the development of anaphylaxis.
Case
A 61-year-old woman was discharged from the hospital the next morning after an orthopedic surgery on her left leg and was recommended to take oral nimesulide and rivaroxaban 10 mg/p. At home, the patient ingested nimesulide and then after half an hour she ingested rivaroxaban; 10–15 minutes after the ingestion of rivaroxaban, the patient developed shortness of breath, her palms started itching, face and lips swelled up, face flushed, and she consequently lost consciousness. During suspected anaphylactic shock, paramedics administered intramuscular adrenaline 1 mg, intramuscular clemastine 1 mg, intravenous dexamethasone 4 mg, and NaCl 0.9% 500mL, as well as oxygen therapy 5 L/min.
At the hospital, a clinical examination was performed, and intravenous fluids (Ringer’s solution 500 mL) and dexamethasone 4 mg were administered. The patient’s blood pressure (BP) was 118/76 mmHg, and pulse rate – 70 times/min. At the time of the anaphylactic reaction serum tryptase level was 30.6 μg/l (normal range 1–15 μg/l).
One month later, the patient was examined in an outpatient allergy clinic. The anamnesis was obtained in compliance with the European Allergy and Clinical Immunology organization (EAACI) drug allergy questionnaire. Previously, the patient had experienced mild allergic reactions in response to rivaroxaban ingestion, such as mild urticaria, mild swelling and itchiness of lips. The latter two have developed after ingestion of rivaroxaban in combination with an antacid drug. She was then treated with clemastine and her symptoms disappeared within a day. No hypersensitivity to non-steroidal anti-inflammatory drugs (NSAIDs) was identified in the medical history. Furthermore, the patient has previously taken nimesulide, with no reported adverse drug reactions (ADRs). Additionally, no food allergy was identified in the medical history.
The serum tryptase level at the time of the allergist’s consultation one month after the anaphylaxis was found to be normal - 5.46 μg/l. The patient did not consent to provocation tests with rivaroxaban and nimesulide to confirm allergy during the allergist’s consultation; therefore, the diagnosis of hypersensitivity to rivaroxaban was based on two previous allergic episodes and elevation of tryptase levels. Two separate provocation tests with alternative drugs meloxicam and dabigatran were performed. These drugs were identified to be safe.
Besides this, the patient has had rhinitis with a persistent runny nose for several years and allergic rhinitis was, thus, suspected. Because of that, for the diagnostic purpose, skin prick tests and molecular allergy diagnostic tests were performed and returned negative. Therefore, diagnosis of allergic rhinitis was ruled out.
Discussion
Anaphylaxis is a suddenly occurring, severe, and potentially fatal systemic allergic reaction.25 Diagnostic criteria for anaphylaxis were previously defined by Cardona et al, 2020; the condition frequently affects respiratory, cardiovascular, and gastrointestinal systems, skin, and mucosal tissue.26 In cases where it is available, the patient’s medical history can also be beneficial in the diagnosis of anaphylaxis.27
Serum tryptase is an important biomarker of anaphylaxis. EAACI as well as Lithuanian allergy organizations recommend tryptase levels in the blood to be tested less than 2 hours after clinical reaction and then again after at least 24 hours.28,29 In the case described here, serum Tryptase levels were tested twice: once immediately after the anaphylaxis and once again one month later at the time of the allergist’s consultation. High serum tryptase level at the time of reaction and normal level after more than 24 hours confirm anaphylaxis as the correct diagnosis.
The patient did not consent to be tested with nimesulide by provocation test, therefore we are unable to confirm with absolute certainty that the anaphylactic episode was not caused by nimesulide. Notably, the patient in this case report had used nimesulide on previous occasions without ADRs. This leads us to suspect that anaphylaxis was caused by rivaroxaban in response to which the patient had previously experienced allergic reactions. Furthermore, we assessed Naranjo Adverse Drug Reaction Probability Scale scores for rivaroxaban and nimesulide with rivaroxaban scoring 5 (reaction classified as “probable”) and nimesulide (reaction classified as “possible”) scoring 4 out of 13 points on the scale (Table 2).30 The difference is due to previous reactions to rivaroxaban in our patient. This difference supports the idea of rivaroxaban being the culprit.
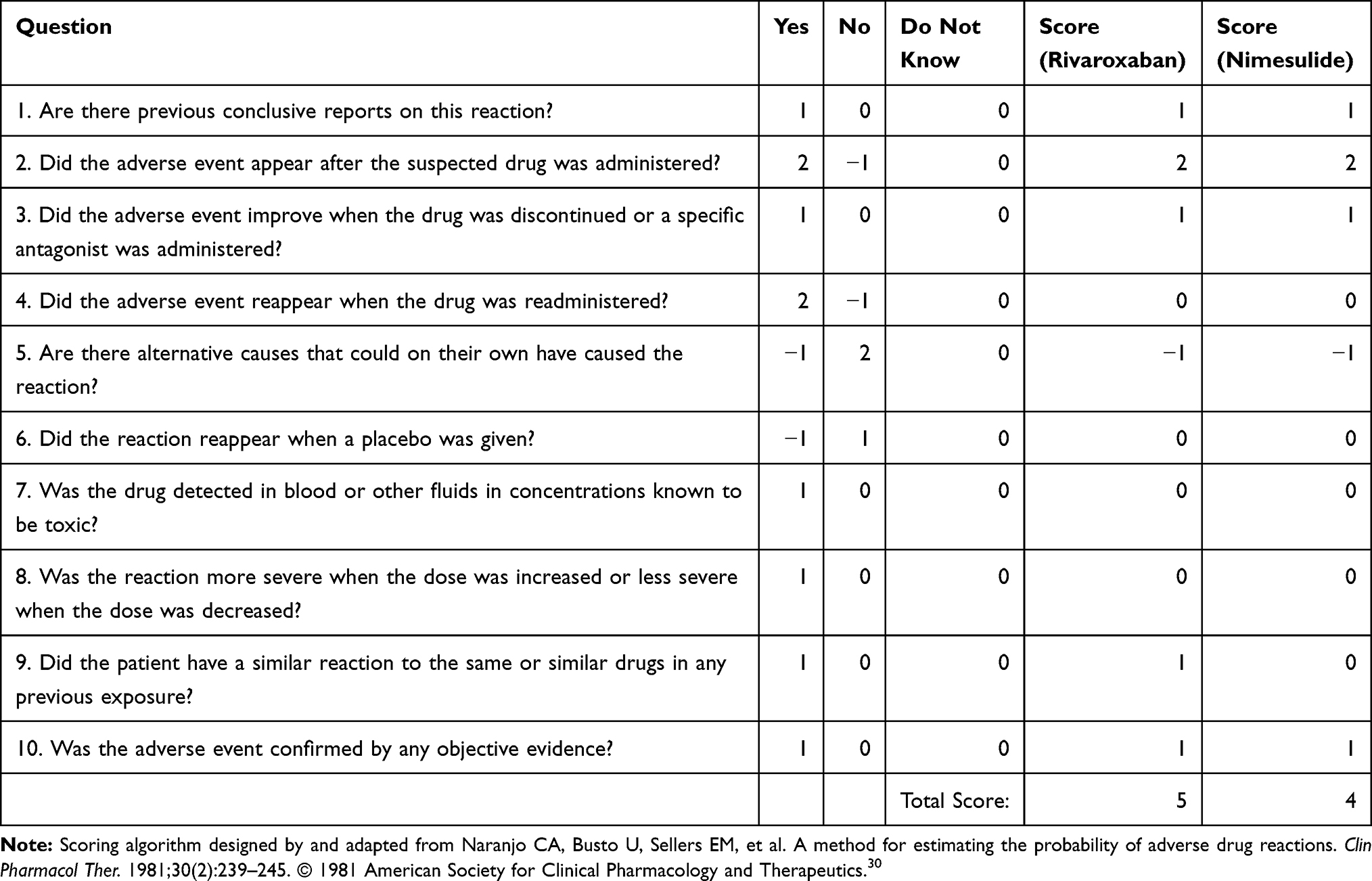 |
Table 2 Naranjo Adverse Drug Reaction Probability Scale Results for Rivaroxaban and Nimesulide. |
Interestingly, possible cross-reactivity was previously noted between rivaroxaban and dabigatran.9 However, mechanisms of this cross-reactivity are not yet fully understood. In contrast to this, dabigatran was identified to be safe for our patient through provocation tests. This raises questions about individual patient responses to these two drugs and points to the possibility to use provocation tests with dabigatran in cases of suspected or confirmed allergy to rivaroxaban.
It was previously reported that rivaroxaban can cause non-allergic hypersensitivity that resembles anaphylaxis which can be tested for using skin-prick tests.31 In the case described here, diagnosis of anaphylaxis is supported by patient’s medical history and results of serum tryptase testing.
There are two main mechanisms of anaphylaxis: non-immunologic and immunologic, the latter being further divided into IgE-dependent and IgE-independent.32 Khan and Sulaiman, 2021 report that in their presented case, rivaroxaban-induced anaphylaxis is mediated by the IgE-dependent mechanism.8 In the case of the IgE-dependent mechanism, degranulation of basophils or mast cells is induced by IgE-FcεRI receptor interaction and the resulting intracellular signaling cascade. In the present case, we have observed elevated tryptase level at the time of reaction, thus IgE-dependent mechanism with mast cell involvement could be supposed. In Lithuania, sIgE tests for rivaroxaban or nimesulide are not performed; therefore, we are unable to compare our results with previous literature.
According to the World Health Organization’s database of reported potential side effects “VigiAccess”, there are 158,484 potential cases of ADRs registered for rivaroxaban.33 Of these, the category “Immune System Disorders” contains 758 potential cases of ADRs, about 0.48% of all reported ADRs. Among these cases, there are 352 reports of hypersensitivity to rivaroxaban, 60 reports of a rivaroxaban-induced anaphylactic reaction, and 14 reports of rivaroxaban-induced anaphylactic shock.
A large study, ROCKET-AF (Rivaroxaban – Once daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) found that both anaphylaxis and anaphylactic shock occurred in 0.01% of tested patients.20
Furthermore, case reports of rivaroxaban-induced urticaria and angioedema, rivaroxaban-induced rashes as well as rivaroxaban-induced anaphylaxis were published (refer to Table 1 for a comprehensive list of publications to date). Rivaroxaban-induced anaphylactic reactions seem to be rare occurrences, given the number of available case reports as well as reports in the ROCKET-AF study and the “VigiAccess” database.
In the present case, the patient had previously taken rivaroxaban and had already had allergic episodes in response to rivaroxaban whilst in the case reported by Khan and Sulaiman, 2021, the patient had not previously taken rivaroxaban.8 In both cases, the time after ingestion of rivaroxaban and before the onset of the symptoms was very short – 30 and 10–15 minutes, respectively. In both cases, the symptoms included skin itchiness and shortness of breath. Notably, in the previously reported case, the anaphylactic shock did not develop, whereas it did in the present case.
In the case presented here, serum tryptase levels were tested twice, whilst these were not tested in the case reported by Khan and Sulaiman, 2021.8 This is significant, as serum tryptase test levels were elevated in the patient, confirming the diagnosis.
The patient’s IgE levels were tested in the case reported by Khan and Sulaiman, 2021. This test was not performed in the present case; therefore, we are not able to add more evidence towards the understanding of the mechanistic basis of rivaroxaban-induced anaphylaxis.
In the present case, the patient had suffered from a total of three allergic episodes induced by rivaroxaban, with the last one resulting in anaphylaxis and anaphylactic shock. We did not document the drop of BP in the hospital since this was already managed by first aid staff, but we have a clear clinical picture due to results that were acquired through serum tryptase testing.
Conclusion
Anaphylaxis is a severe, acute, life-threatening condition. Rivaroxaban-induced anaphylaxis is rare; therefore, an understanding of the condition is lacking. Here, we present a case of rivaroxaban-induced anaphylaxis. It is important for physicians to be aware of this possible adverse reaction when prescribing rivaroxaban. When prescribing rivaroxaban, it is important to analyze patients’ medical history and to be aware of the risks of possible undesired drug interactions. It may also be beneficial to use provocation tests with other oral anticoagulants to identify safe alternatives in case of suspected rivaroxaban-induced allergic reactions.
Consent for Publication
Informed consent for publication was obtained from the patient. The patient was informed about the use of de-identified data in scientific research and publications. Institutional approval was not required for this publication.
Disclosure
Prof. Dr. Violeta Kvedarienė reports sponsorship for professional education from Norameda and Berlin Chemie Menarini, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Barnes GD, Lucas E, Alexander GC, Goldberger ZD. National trends in ambulatory oral anticoagulant use. Am J Med. 2015;128(12):1300–1305.e2. doi:10.1016/j.amjmed.2015.05.044
2. Badreldin H, Nichols H, Rimsans J, Carter D. Evaluation of anticoagulation selection for acute venous thromboembolism. J Thromb Thrombolysis. 2017;43(1):74–78. doi:10.1007/s11239-016-1417-5
3. Kjerpeseth LJ, Ellekjær H, Selmer R, Ariansen I, Furu K, Skovlund E. Trends in use of warfarin and direct oral anticoagulants in atrial fibrillation in Norway, 2010 to 2015. Eur J Clin Pharmacol. 2017;73(11):1417–1425. doi:10.1007/s00228-017-2296-1
4. Bezabhe WM, Bereznicki LR, Radford J, et al. Ten-year trends in the use of oral anticoagulants in Australian general practice patients with atrial fibrillation. Front Pharmacol. 2021;12:586370. doi:10.3389/fphar.2021.586370
5. Perzborn E, Roehrig S, Straub A, Kubitza D, Misselwitz F. The discovery and development of rivaroxaban, an oral, direct factor Xa inhibitor. Nat Rev Drug Discov. 2011;10(1):61–75. doi:10.1038/nrd3185
6. Tomás-Pérez M, De Las Vecillas L. Allergy to rivaroxaban cross-reactivity with other direct anticoagulants and the role of the basophil activations test: a case report. J Investig Allergol Clin Immunol. 2023;33(5). doi:10.18176/jiaci.0883
7. Wu Z, Ma Y. Hypersensitivity reaction from Rivaroxaban. Am J Med Sci. 2021;361(5):679–680. doi:10.1016/j.amjms.2020.11.002
8. Khan FY, Sulaiman TO. Anaphylaxis following rivaroxaban ingestion: report of an extremely rare case. Pan Afr Med J. 2021;38. doi:10.11604/pamj.2021.38.333.28401
9. Patil T, Ikekwere C. A case report of rivaroxaban-induced urticaria and angioedema with possible cross-reaction to dabigatran. J Med Cases. 2019;10(12):359–363. doi:10.14740/jmc3399
10. Rudd KM, Panneerselvam N, Patel A. Rash associated with rivaroxaban use. Am J Health Sys Pharm. 2018;75(6):347–349. doi:10.2146/ajhp160985
11. Sasson E, James M, Russell M, Todorov D, Cohen H. Probable rivaroxaban-induced full body rash: a case report. J Pharm Pract. 2018;31(5):503–506. doi:10.1177/0897190017722872
12. Banaga Y, Mohmmed K, Mustafa H, Barrett J. Angioedema 2 months after administration of rivaroxaban (Xarelto). J Clin Case Rep. 2017;7(12). doi:10.4172/2165-7920.10001059
13. Chiasson CO, Canneva A, Roy FO, Doré M. Rivaroxaban-induced hypersensitivity syndrome. CJHP. 2017;70(4). doi:10.4212/cjhp.v70i4.1681
14. Vernon HM, Nielsen AK, O’Bryan EC. Hypersensitivity reaction after administration of rivaroxaban (Xarelto). Am J Emerg Med. 2016;34(7):1325.e1–1325.e2. doi:10.1016/j.ajem.2015.12.021
15. Radu C, Barnig C, de Blay F. Rivaroxaban-induced drug reaction with eosinophilia and systemic symptoms. J Investig Allergol Clin Immunol. 2016;26(2):124–126. doi:10.18176/jiaci.0027
16. Snyder DJ, Matusik FB. Rivaroxaban-induced serum sickness after total knee arthroplasty. Am J Health Sys Pharm. 2015;72(18):1567–1571. doi:10.2146/ajhp140549
17. Barrett P, Vuppalanchi R, Masuoka H, Chalasani N. Severe drug-induced skin and liver injury from rivaroxaban. Dig Dis Sci. 2015;60(6):1856–1858. doi:10.1007/s10620-014-3504-9
18. Altin C, Ozturkeri OAY, Gezmis E, Askin U. Angioedema due to the new oral anticoagulant rivaroxaban. Ann Card Anaesth. 2014;2(17):173–174. doi:10.4103/0971-9784.129888
19. Yates J, Choudhry M, Keys G. A case report describing a suspected rivaroxaban hypersensitivity reaction in a surgical patient: suspected rivaroxaban hypersensitivity in a surgical patient. J Clin Pharm Ther. 2013;38(2):159–161. doi:10.1111/jcpt.12013
20. Hofmeier KS, Bircher AJ. Hypersensitivity reactions to modern antiplatelet and anticoagulant drugs. Allergo J Int. 2015;24(2):58–66. doi:10.1007/s40629-015-0048-2
21. Warner TD, Giuliano F, Vojnovic I, Bukasa A, Mitchell JA, Vane JR. Nonsteroid drug selectivities for cyclo-oxygenase-1 rather than cyclo-oxygenase-2 are associated with human gastrointestinal toxicity: a full in vitro analysis. Proc Natl Acad Sci USA. 1999;96(13):7563–7568. doi:10.1073/pnas.96.13.7563
22. Caiazzo E, Ialenti A, Cicala C. The relatively selective cyclooxygenase-2 inhibitor nimesulide: what’s going on? Eur J Pharmacol. 2019;848:105–111. doi:10.1016/j.ejphar.2019.01.044
23. Aun MV, Blanca M, Garro LS, et al. Nonsteroidal anti-inflammatory drugs are major causes of drug-induced anaphylaxis. J Allergy Clin Immunol. 2014;2(4):414–420. doi:10.1016/j.jaip.2014.03.014
24. Dubini M, Marraccini P, Gagliardi C, Marelli S, Rivolta F. Anaphylaxis to nimesulide. Ann Allergy Asthma Immunol. 2021;127(1):144–145. doi:10.1016/j.anai.2021.04.007
25. Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117(2):391–397. doi:10.1016/j.jaci.2005.12.1303
26. Cardona V, Ansotegui IJ, Ebisawa M, et al. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organ J. 2020;13(10):100472. doi:10.1016/j.waojou.2020.100472
27. Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: cardiac arrest in special circumstances. Resuscitation. 2021;161:152–219. doi:10.1016/j.resuscitation.2021.02.011
28. Černiauskienė M, Bagdonaitė L, Karčiauskaitė D, Kvedarienė V. Prevalence and variability of allergen-specific immunoglobulin E in patients with elevated tryptase levels. Med Sci Monit. 2022;28. doi:10.12659/MSM.937990
29. Muraro A, Worm M, Alviani C, et al. EAACI guidelines: anaphylaxis (2021 update). Allergy. 2022;77(2):357–377. doi:10.1111/all.15032
30. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
31. Hakkenbrak NAG, Truijers M. Life-threatening non-allergic drug hypersensitivity reaction as a very rare side effect of rivaroxaban administration in the Netherlands. Vasc Endovascular Surg. 2021;55(7):749–751. doi:10.1177/15385744211004763
32. Montañez MI, Mayorga C, Bogas G, et al. Epidemiology, mechanisms, and diagnosis of drug-induced anaphylaxis. Front Immunol. 2017;8:614. doi:10.3389/fimmu.2017.00614
33. World Health Organisation. VigiAccess database. Available from: https://www.vigiaccess.org/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.