Back to Journals » Infection and Drug Resistance » Volume 19
Susceptibility Patterns and Factors Associated with Multidrug Antibiotic Resistance Among Patients with Productive Cough in Southwestern Uganda
Authors Ezekiel W, Kegoye ES, Ssempijja F ![]() , Maniga JN
, Maniga JN ![]() , Ampeire IP, Abdi AA
, Ampeire IP, Abdi AA ![]()
Received 14 September 2025
Accepted for publication 11 January 2026
Published 22 January 2026 Volume 2026:19 567493
DOI https://doi.org/10.2147/IDR.S567493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Oliver Planz
Winnie Ezekiel,1 Eric Simidi Kegoye,2,3 Fred Ssempijja,4,5 Josephat Nyabayo Maniga,6 Isaac Petit Ampeire,1 Awil Abdulkadir Abdi1
1Department of Internal Medicine, Kampala International University Teaching Hospital, Bushenyi, Uganda; 2Department of Human Anatomy, Kenya Methodist University, Meru, Kenya; 3Department of Human Anatomy, Kampala International University, Bushenyi, Uganda; 4Infection Medicine, Edinburgh Medical School, Deanery of Biomedical Sciences, College of Medicine and Veterinary Medicine, The University of Edinburgh, Edinburgh, UK; 5School of Allied Health, St. Lawrence College, Kingston, Canada; 6Department of Microbiology and Immunology, Kampala International University, Bushenyi, Uganda
Correspondence: Awil Abdulkadir Abdi, Department of Internal Medicine, Kampala International University Teaching Hospital, Bushenyi, Uganda, Email [email protected]
Background: Antibiotic resistance is a growing global public health concern, yet data on bacterial pathogens and susceptibility patterns among patients with productive cough in Uganda are scarce. This study aimed to determine the prevalence, bacterial isolates, susceptibility profiles, and factors associated with antibiotic resistance at Hoima Regional Referral Hospital, Uganda.
Methods: A cross-sectional study was conducted among 216 adult outpatients presenting with productive cough. Sociodemographic, lifestyle, and medical data were obtained using structured questionnaires. Sputum samples were cultured, and antibiotic susceptibility testing was performed using Kirby-Bauer disk diffusion according to Clinical and Laboratory Standards Institute (CLSI) M100 (2022) guidelines. Logistic regression analyses were used to identify factors associated with antibiotic resistance. A p value of < 0.05 was considered statistically significant.
Results: Bacterial pathogens were isolated in 139 (64.4%) patients. The most frequent were Streptococcus pneumoniae 57 (40.8%), Staphylococcus aureus 40 (28.6%), Klebsiella pneumoniae 17 (12.2%), and Streptococcus pyogenes 14 (10.2%). Most bacterial isolates were sensitive to imipenem 105 (75.5%), ceftazidime 92 (66.7%), and cefepime 81 (58.5%), while the lowest was to ampicillin 13 (9.5%) and amoxicillin 13 (9.5%). Antibiotic resistance was associated with smoking (aOR = 2.89, 95% CI: 1.074– 7.784, p = 0.036) and prior use of antibiotic (aOR = 2.65, 95% CI: 1.103– 6.369, p = 0.029).
Conclusion: Among outpatients with a productive cough at Hoima Regional Referral Hospital, Streptococcus pneumoniae, Staphylococcus aureus were the leading Gram-positive isolates, and Klebsiella pneumoniae was the most common Gram-negative. Gram-negative isolates showed more susceptibility to ceftazidime, and overall susceptibility was more for imipenem, whereas ampicillin and amoxicillin demonstrated very low activity. Antibiotic resistance was significantly associated with smoking and prior use of antibiotic. These findings underscore the need for routine sputum culture and sensitivity testing, and strengthened public health measures to reduce smoking and inappropriate use of antibiotic.
Keywords: multidrug resistance, productive cough, Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae, use of antibiotic, smoking, Uganda
Introduction
Antimicrobial resistance (AMR) is a growing global health concern that complicates empirical treatment and contributes to rising morbidity and mortality.1 This can also be attributed further in recent years, due to the widespread and sometimes inappropriate use of broad-spectrum antibiotics during the COVID-19 pandemic.2 In the context of bacterial infection, antibiotic resistance is defined as the ability of bacteria to survive or grow after exposure to antibiotics at levels that could normally inhibit or kill them.3 The WHO’s Global Antibiotic Resistance Surveillance Report 2025 states that > 23 million bacteriologically confirmed cases of bloodstream infections, urinary tract infections, gastrointestinal infections, and urogenital gonorrhoea.4 In 2019, drug-resistant infections were linked to 4.95 million deaths worldwide, with 1.27 million directly attributable to antimicrobial resistance.5 Resistance patterns vary across countries and even within regions of the same country,6,7 making localized data essential for guiding therapy.
The burden of AMR is particularly overwhelming in Sub-Saharan Africa, with western Sub-Saharan Africa reporting an estimated 27.3 deaths per 100,000 attributable to resistance in 2019.5 In Uganda, health facility studies have documented resistance rates as high as 73% in rural populations.8 However, the World Health Organization has reported that Uganda or Africa at large lacks a robust AMR surveillance system and faces challenges of limited diagnostic laboratory capacity.9 This has left clinicians to rely heavily on empirical treatment.
Respiratory tract infections remain among the leading causes of morbidity and mortality in Africa, contributing to 34.6% of deaths from infectious diseases annually.10 Productive cough, one of the most common reasons for seeking medical care, is associated with significant quality of life impairment.11 Left untreated, a productive cough can lead to depression, urinary incontinence, syncope, social embarrassment, sleep disturbance, and depression.12 A study in rural Uganda, chronic cough accounts for the most common chronic respiratory symptoms.13
Despite this high burden, data on bacteriological causes, antibiotic susceptibility patterns, and associated risk factors among patients with productive cough in Uganda remain limited. HRRH serves as the main referral facility for the south-western region, receiving patients from both rural and urban areas where diagnostic capacity is often constrained. Understanding the bacterial profile in this setting is therefore essential for guiding appropriate empirical therapy and strengthening local AMR surveillance. This study was conducted to address this gap.
Methods
Study Design and Setting
This was a hospital-based cross-sectional study conducted at Hoima Regional Referral Hospital (HRRH) between April to July 2023. Data were collected from adult patients who were ≥18 years presenting with a productive cough at the outpatient department.
Study Population and Inclusion Criteria
All Adult patients aged ≥18 years with a productive cough who attended the outpatient department during the study period and was willing to participate and signed informed consent.
Exclusion Criteria
Patients already on treatment for tuberculosis and those who were critically ill.
Sample Size Estimation
The aim of the study was to determine the bacterial etiology, susceptibility patterns, and factors associated with antibiotic resistance among adults presenting with a productive cough at HRRH. Leslie Kish’s formula was used to calculate the sample size of the study which states:

where n = sample size, Z = statistic for a level of confidence, P = expected prevalence, d = precision
At 95% confidence (Z = 1.96), using a prevalence of 16.9% for Klebsiella pneumoniae resistance to cefotaxime-clavulanic acid in productive cough from India14 and d = 0.05:
 ,
,  ,
,  216. Therefore, this was the largest among all sample size estimates and was used for the study.
216. Therefore, this was the largest among all sample size estimates and was used for the study.
Sampling Technique and Recruitment
Consecutive sampling was used to recruit adult patients (≥18 years) with productive cough presenting to the outpatient department at HRRH. Recruitment was done daily during the study period, all eligible patients were given an equal opportunity to participate, and duplicate enrollment was avoided by asking the participants if they had participated this study in the last 3 months. A total of 225 patients were initially screened, 1 declined consent and 8 were excluded: 3 were very sick, 5 on tuberculosis treatment.
Data Collection Tools
Data were collected using a structured, interviewer-administered questionnaire developed specifically for this study. There was pilot study questionnaire done for 10 participants at Kampala International University Teaching Hospital not included in the final analysis, and adjustments of language were made to improve clarity and relevance. The tool captured socio-demographic, lifestyle, and medical characteristics. It was used to review for accuracy and completeness daily. Laboratory investigations were conducted on sputum samples for bacterial culture and drug sensitivity.
Data Management and Analysis
All the completed questionnaires and corresponding laboratory results were reviewed daily and were coded and later stored securely. Data were entered into Excel (version 2019), then exported to GraphPad Prism Version 9.5.0 (GraphPad Software, Inc., Boston, MA, USA) and STATA version 14.2 (StataCorp, College Station, TX, USA) for analysis. Descriptive statistics were used to summarize socio-demographic, lifestyle, and medical characteristics of respondents. Findings were presented using tables. Bivariate logistic regression was performed and variables with p < 0.2 at bivariate were included in the multivariate model to identify factors associated with antibiotic resistance. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was set at p < 0.05.
Laboratory Procedures
Sputum Collection and Processing
A wet or productive cough is defined as cough that is accompanied by the expectoration of sputum or phlegm.15,16 Spot sputum samples were collected aseptically before breakfast. For patients who had eaten, mouth rinsing was requested before collection. Participants were instructed to take a deep breath and expectorate sputum while avoiding saliva or nasopharyngeal secretions. Samples appearing salivary were rejected and a repeat specimen was obtained. Each sample was placed in a dry, sterile, leak proof, screw capped translucent container (30 mL capacity) and transported with in 30 min to the microbiology laboratory for analysis. To Ensure reliability and for quality control of the laboratory procedures and results the specimen was collected while ensuring sterile conditions. Also, the sputum containers, reagents for culture, culture media (Blood agar, Chocolate agar, and MacConkey), and drug discs for susceptibility testing were inspected for their expiration dates and the products were used according to the manufacturer’s instructions.17
Cultivation and Identification of Isolates
A satisfactory sputum sample was defined as >25 leukocytes and alveolar macrophages, and <10 squamous epithelial cells per low power field as applied in the hospital’s microbiology laboratory. Direct Gram staining was done on all specimens. No patient was excluded on the basis of sputum quality. Using a sterile wire loop, samples were inoculated onto blood agar, MacConkey agar, and chocolate agar (Oxoid, Hampshire, UK), and streaked across four quadrants for colony isolation. Blood and chocolate agar plates were incubated at 37°C in 5–10% CO2 candle jars for 24 hours. MacConkey agar was incubated aerobically at 37°C for 24 hours. Pure colonies were subcultured in nutrient broth (Oxoid, Hampshire, UK).18 For fastidious organisms, the Clinical and Laboratory Standards Institute (CLSI) recommended media and incubation procedure were followed. Streptococcus pneumoniae and other alpha-haemolytic streptococci were tested on Mueller–Hinton agar supplemented with 5% sheep blood and incubated in 5% CO2. Haemophilus influenzae was tested on Haemophilus Test Medium (HTM). Bacterial identification followed conventional microbiological methods. On blood agar, isolates were examined for colony morphology, hemolysis, and Gram stain. Gram-positive bacteria were identified using catalase, coagulase, optochin susceptibility test (30 μg), bacitracin susceptibility test (30 μg), and bile esculin tests. Gram-negative bacteria were identified using oxidase, indole, urease, citrate utilization, lysine, decarboxylation carbohydrate fragmentation, and gas production.17,19,20
Antimicrobial Susceptibility Testing
Antibiotic susceptibility testing (AST) was performed using the Clinical and Laboratory Standards Institute (CLSI), approved Kirby-Bauer disc diffusion method on Mueller-Hinton agar (Oxoid, Hampshire, UK). The antibiotics tested included gentamicin (10 μg), erythromycin (15 μg), ciprofloxacin (5 μg), doxycycline (30 μg), ampicillin (10 μg), augmentin (20/10 μg), imipenem (10 μg), ceftriaxone (30 μg), chloramphenicol (30 μg), ceftazidime (30 μg), cotrimoxazole (1.25/23.75 μg), cefepime (30 μg), and amoxicillin (10 μg). Daily internal quality control was followed using recommended American Type Culture Collection (ATCC) reference strains, and inhibition zone diameters fell within CLSI ranges. Zone diameters were interpreted as sensitive (S) or resistant (R), with intermediate strains classified as resistant.18,21
Classification of Resistance Patterns
Resistance profiles were classified based on Centre for Disease Control & Prevention (CDC), Atlanta, and European Centre for Disease Control (ECDC) definitions. Bacteria non-susceptible to <3 antibiotic groups were defined as non-multidrug-resistant (NMDR); resistance to ≥3 groups were multidrug-resistant (MDR); resistance to all but 1–2 groups were extensively drug-resistant (XDR); and resistance to all tested groups was pan-drug-resistant (PDR).22,23
Study Variables
- Sociodemographic Factors: Age, Sex, Education level, Occupation
- Lifestyle Factors:
- Smoking and alcohol use were assessed using yes/no questions regarding current status
- Medical Factors:
- Comorbidities: Defined as yes or no form of chronic non-communicable diseases (asthma, diabetes mellitus, hypertension, heart failure, chronic obstructive pulmonary disease), or HIV, confirmed by medication use, self-reported diagnosis, or medical records
- History of hospitalization (Previous 3 months) as yes or no form
- Use of antibiotic: Self-reported use of antibiotic within the last two weeks
Results
Sociodemographic and Life Style Characteristics of the Study Participants
A total of 216 adult participants were enrolled in this study. Majority of patients (115n, 53.2%) were ≥60 years of age and out of whom115 patients (53.2%) were female. Consumption of alcohol was reported by 114 (52.8%) patients, and 29 patients (13.4%) were smokers (Table 1).
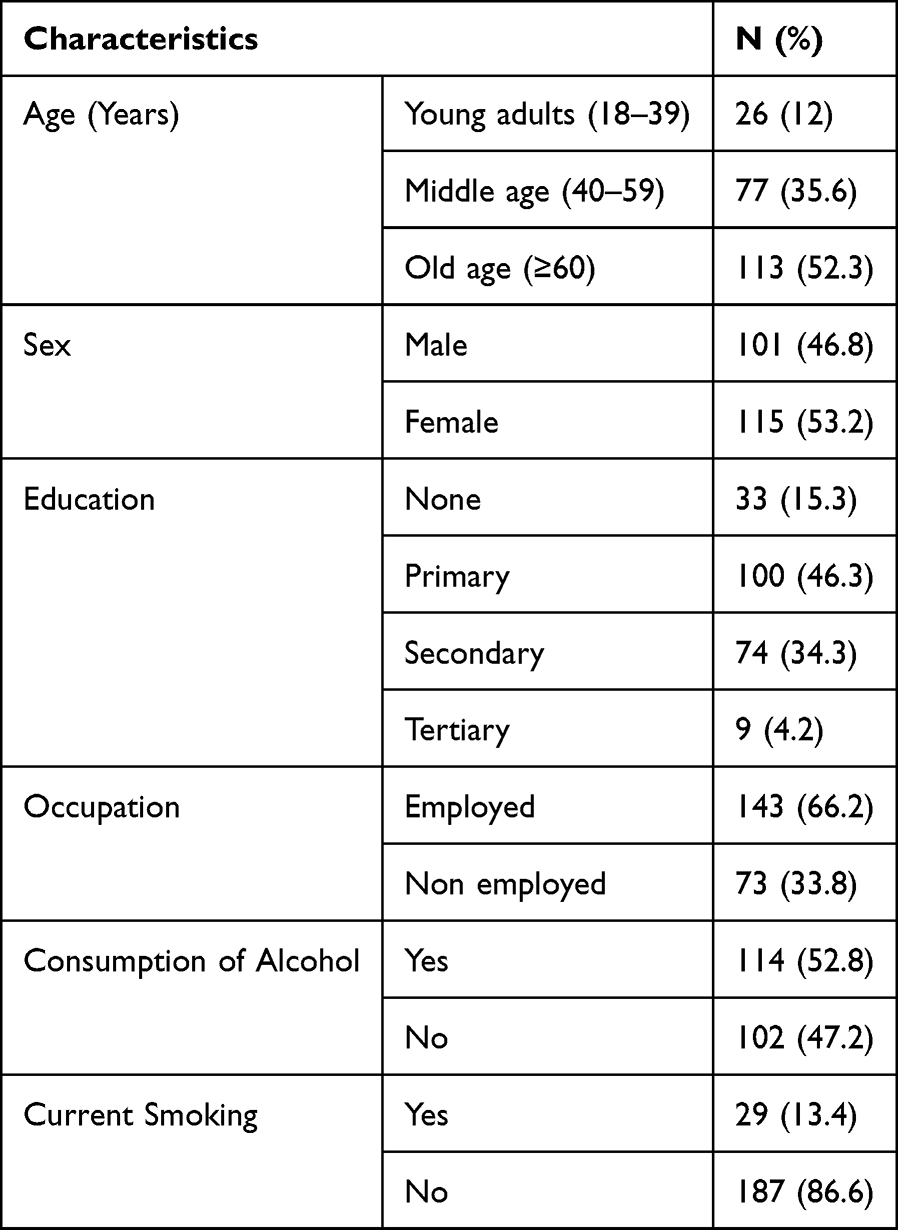 |
Table 1 Sociodemographic and Lifestyle Characteristics of the Study Participants (n=216) |
Medical Factors of the Study Participants
A total of 33 (15.3%) respondents reported a history of hospitalization in the previous three months. More than half of the participants, 127 (58.8%) reported use of antibiotic within the past two weeks. Seventy-nine (36.6%) patients were HIV positive, while 32 (14.8%) patients had diabetes mellitus and 33 (15.3%) patients had hypertension (Table 2).
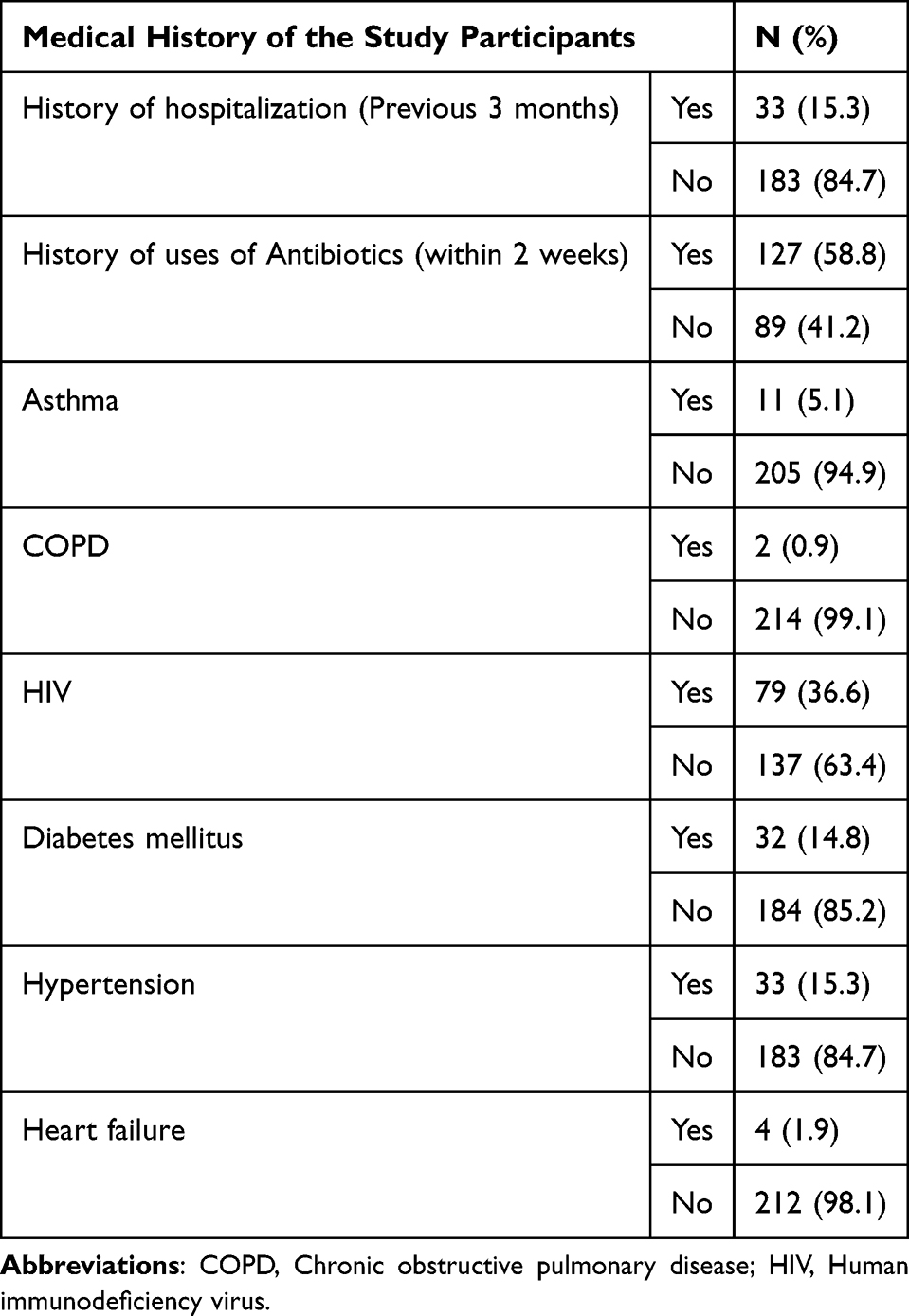 |
Table 2 Medical History of the Study Participants (n=216) |
Distribution of Bacterial Pathogens Isolated from Sputum Samples and Overall Bacterial Growth Status
Out of 216 sputum samples cultured, 139 (64.4%) showed bacterial growth, while 77 (35.6%) showed no growth. A total of 147 bacterial isolates were identified from the 139 positive cultures; eight samples grew more than one organism. The most frequently isolated pathogen was Streptococcus pneumoniae (60; 40.8%), followed by Staphylococcus aureus 42 (28.6%), Klebsiella pneumoniae 18 (12.2%), and Streptococcus pyogenes 15 (10.2%). Less common pathogens included Pseudomonas aeruginosa 5 (3.4%), Streptococcus viridans 3 (2.0%), Moraxella catarrhalis 2 (1.4%), and Haemophilus influenzae 2 (1.4%) (Table 3).
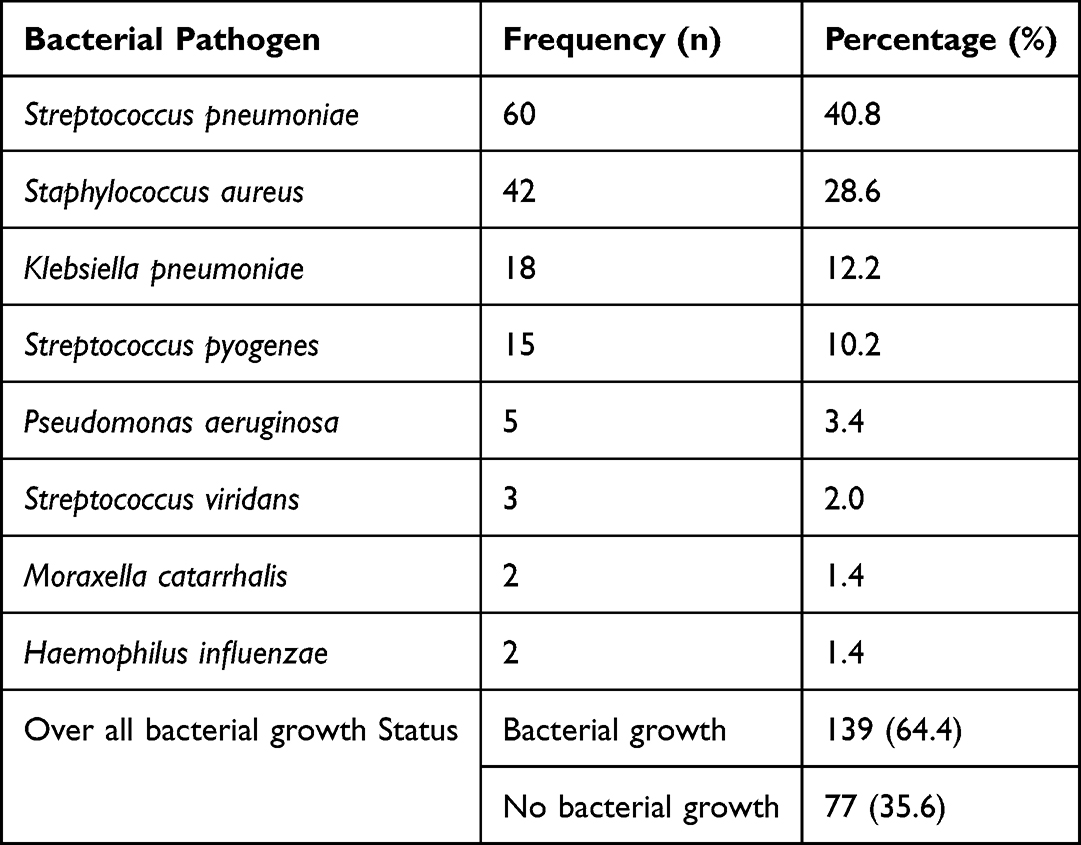 |
Table 3 Distribution of Bacterial Pathogens Isolated From Sputum Samples (n = 147) and Overall Bacterial Growth Status (n = 216) |
Antibiotic Susceptibility Patterns of Bacterial Isolates Recovered from Sputum Samples
A total of 147 bacterial isolates were analyzed for antimicrobial susceptibility. Among Gram-negative isolates, ceftazidime demonstrated the highest activity (76.0%), while imipenem showed the highest overall effectiveness across both Gram-positive and Gram-negative pathogens (75.5%). Cotrimoxazole (56.5%), doxycycline (56.5%), cefepime (58.5%), and ceftriaxone (53.7%) showed moderate activity. In contrast, ampicillin and amoxicillin exhibited the lowest susceptibility rates (each 9.5%) (Table 4).
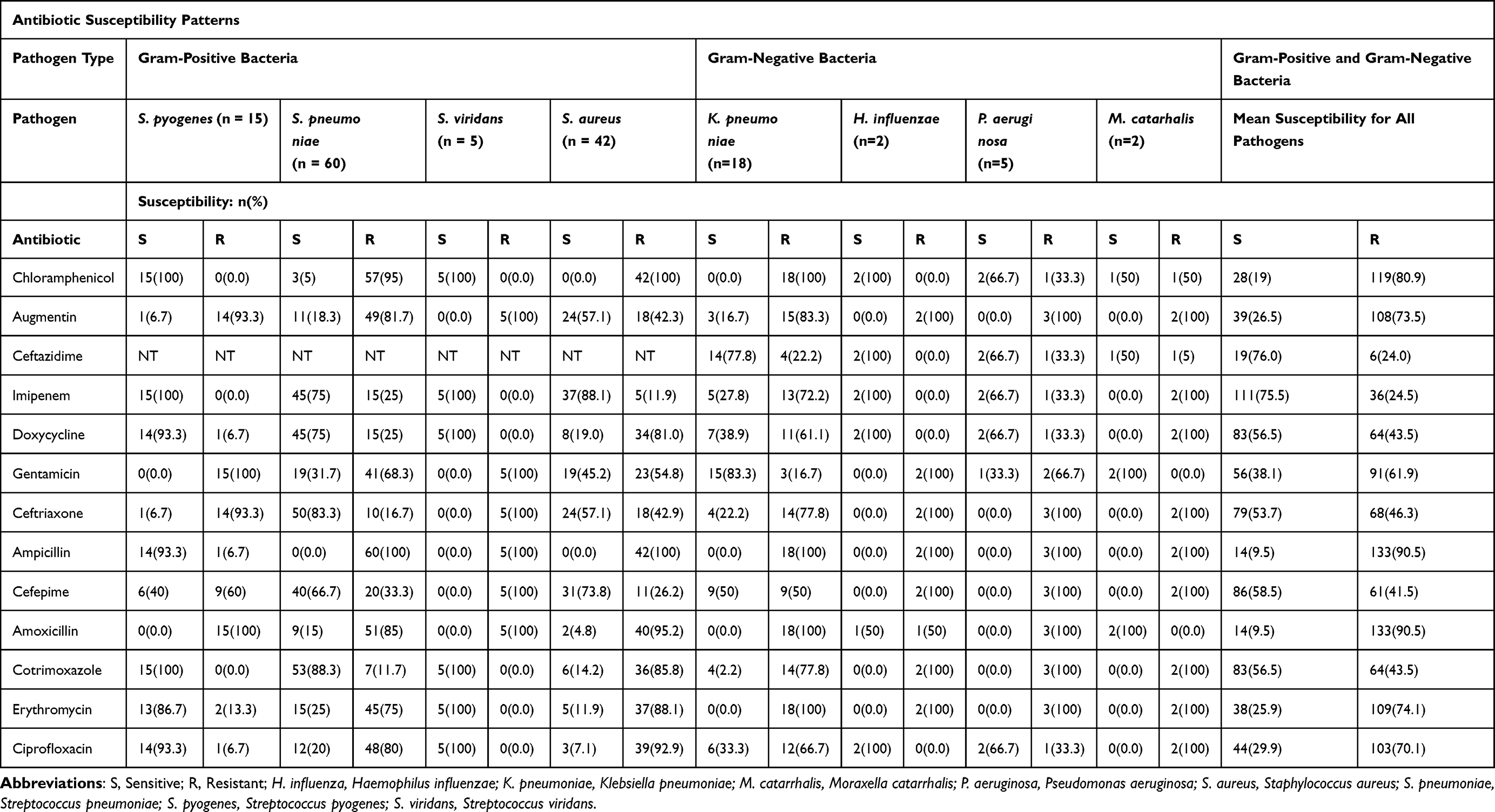 |
Table 4 Antibiotic Susceptibility Patterns of Bacterial Isolates Recovered from Sputum Samples. (N= 147) |
Distribution of Antibiotic Resistance Patterns Among Bacterial Isolates (n = 147)
Among the 147 bacterial isolates obtained from sputum samples, 65.3% were non-multidrug resistant (NMDR), while 34.7% demonstrated multidrug resistance (mDR).
Factors Associated with Multidrug Resistance (mDR) Among Bacterial Isolates from Sputum Samples (n = 147): Bivariate and Multivariate Analysis
In our study, factors that were significant at the multivariate level and considered independently associated with mDR resistance were use of antibiotic within the past two weeks (aOR = 2.65; p = 0.029) and smoking (aOR = 2.89; p = 0.036) (Table 5).
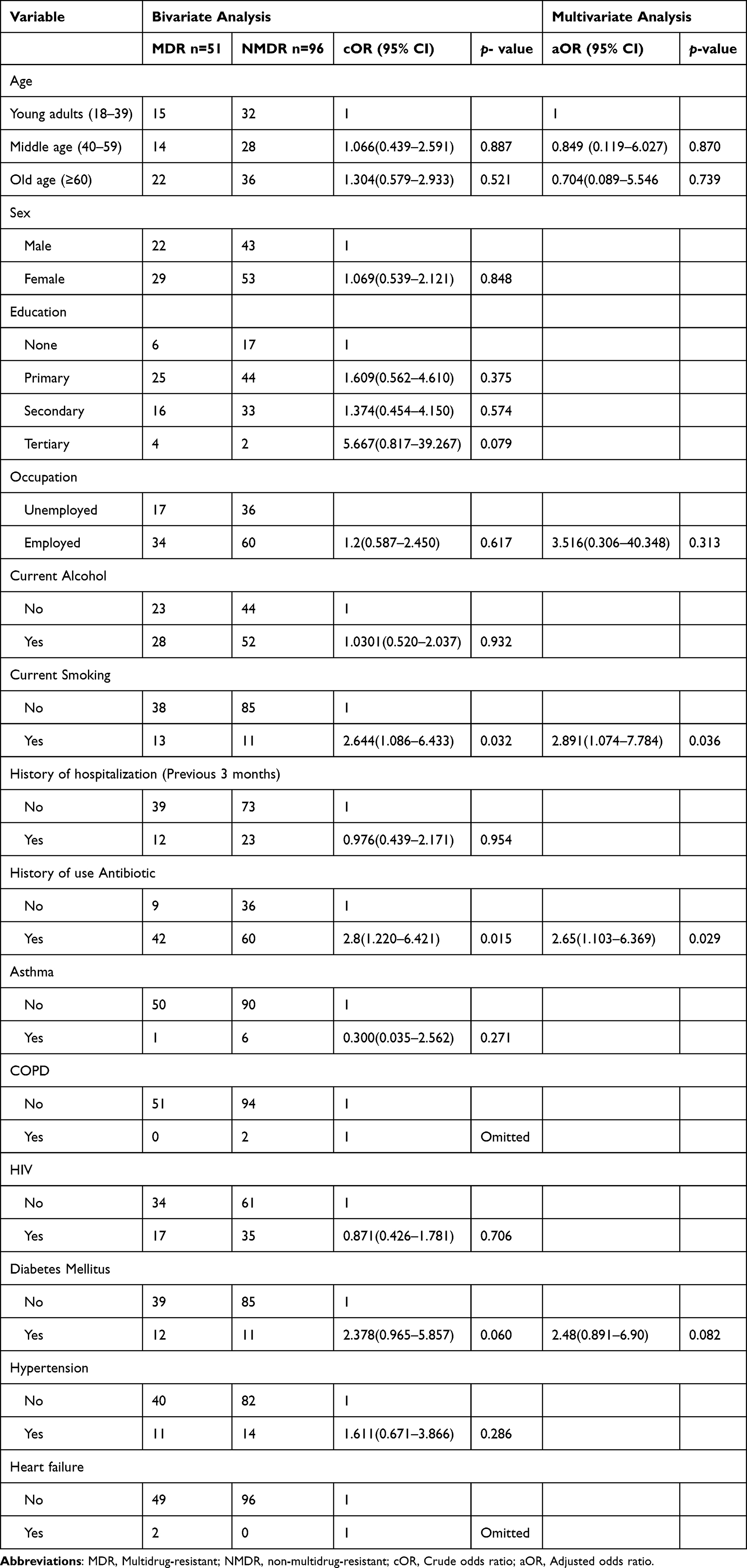 |
Table 5 Factors Associated with Multidrug Resistance Among Bacterial Isolates (n = 147) |
Discussion
This study conducted in southwestern rural Uganda investigated bacterial pathogens in patients presenting with productive cough, characterize their antibiotic susceptibility profiles, and examined risk factors for resistance. We observed bacterial growth in 64.4% of sputum samples and presence of multiple pathogens in a few samples. Majority of the isolates were Gram-positive organisms like S. pneumoniae (40.8%) followed by S. aureus (28.6%) and S. pyogenes (10.2%), while K. pneumoniae (12.2%) was the leading Gram-negative isolate. Multidrug resistance (mDR) was independently associated with smoking and recent antibiotic exposure, highlighting concerns for antibiotic stewardship and respiratory infection management.
In this study, Gram-positive bacteria were predominant where this distribution contrasts with findings from Tanzania, where Gram-negative organisms dominated, and K. pneumoniae was the most common pathogen.24 Our study included only outpatients, whereas the kishibmo et al study involved hospitalized patients with pneumonia and multiple comorbidities, which explains the higher isolation rates of opportunistic pathogens. Similar differences have been reported in Asian countries, where P. aeruginosa and K. pneumoniae predominate.10,14,25 Differences in age distribution, healthcare-seeking behavior, and specimen types, including the use of sputum, bronchial washings, and endotracheal secretions, likely contribute to these regional variations in bacterial distribution.
The predominance of S. pneumoniae in this study aligns with findings from several studies, where this organism remains the most common cause of respiratory infections.26,27 S. pneumoniae is a major contributor to morbidity in elderly or immunocompromised individuals, particularly those with chronic conditions or alcohol use, both of which were prevalent among our participants. The organism often colonizes the nasopharynx asymptomatically but becomes pathogenic in individuals with weakened immunity, increasing the risk of infection and antibiotic resistance,28–30 it possesses a polysaccharide capsule and other immune-modulating toxins that promote evasion of phagocytosis, host cell lysis and inflammation contributing to respiratory disease severity.31 Staphylococcus aureus produces metallophores, such as staphyloferrins and staphylopine, which enable acquisition of iron and zinc in nutrient from the host, supporting persistence and virulence during infection.32 Klebsiella pneumoniae is increasingly becoming an important respiratory pathogen contributing to severe disease. Its polysaccharide capsule provides protection against host immune clearance, while siderophore systems such as enterobactin, salmochelin, and aerobactin enable iron acquisition from host enhancing survival and pathogenicity.33
All bacterial isolates were susceptible to at least one antibiotic, but overall resistance was high, across all isolates, imipenem and ceftazidime demonstrated the highest efficacy, followed by cefepime, cotrimoxazole, doxycycline, and ceftriaxone. In contrast, penicillin derivatives and chloramphenicol exhibited very limited activity. These findings mirror resistance trends reported in Nigeria and Pakistan, where Ceftazidime and Imipenem remained effective while Ampicillin and Augmentin showed high resistance.25,26 However, studies conducted in Tanzania and India reported different susceptibility patterns compared to our findings but similarly observed high resistance to penicillin derivatives,14,24 highlighting regional differences in antibiotic use and resistance selection pressures. High resistance to penicillin derivatives observed reflects their widespread, often empirical use for respiratory infections. Among Gram-negative isolates, their resistance may be attributed to the characteristics of multidrug resistance mechanisms including metallo beta lactamase (MBL), AmpC beta lactamase (AmpC) and extended spectrum beta lactamase (ESBL).34,35 In our setting, empirical prescribing without microbiological confirmation remain common in both rural and urban areas and frequent self-medication may contribute for resistance. Also, weak antimicrobial stewardship and inconsistent access to diagnostic facilities further support the persistence of resistant strains in outpatient populations.
Cigarette smokers were nearly three times more likely to harbor mDR bacterial isolates. Smoking impairs mucociliary clearance by damaging respiratory tract cilia, increasing susceptibility to recurrent infections and subsequent antibiotic exposure, both of which contribute to antibiotic resistance.18,36
Similarly, prior use of antibiotic was linked to mDR isolates, almost three times more likely to have resistant bacteria. Inappropriate or repeated antibiotic prescriptions and misuse exert selective pressure on bacteria, driving the emergence of resistance.37
Strength and Limitations of the Study
To the best of our knowledge, this is among the few studies conducted to evaluate both gram-positive and gram-negative bacterial isolates and their antibiotic resistance patterns among outpatients with productive cough in Uganda. This was a single-center, hospital-based cross-sectional study, findings may not be generalizable to the wider community. Molecular studies to detect atypical bacterial pathogens were not performed.
Conclusion
This study found that S. pneumoniae, S. aureus, and K. pneumoniae were the most common bacterial isolates in adults with productive cough, Gram-negative isolates showed the highest susceptibility to ceftazidime, and overall susceptibility was greatest for imipenem, whereas ampicillin and amoxicillin demonstrated very low activity but marked resistance to penicillin-class antibiotics and chloramphenicol. Multidrug resistance was linked to smoking and prior use of antibiotic. Routine sputum culture, pneumococcal vaccination, and alongside public health strategies to reduce cigarette smoking and inappropriate use of antibiotic are recommended. Future studies incorporating molecular resistance profiling and community-based surveillance would further guide antibiotic stewardship efforts.
Data Sharing Statement
Data can be obtained by contacting [email protected] (corresponding author).
Ethics Statement
The study was reviewed and approved by the Kampala International University Research and Ethics Committee (KIU-IREC) (Ref: KIU-2022-203), the Directorate of Postgraduate Studies, and the Faculty of Clinical Medicine and Dentistry. Administrative clearance was obtained from the Director of Hoima Regional Referral Hospital. The research was conducted in accordance with the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants with details in both English and the local language. Participation was voluntary, and confidentiality was assured.
Acknowledgment
The research co-authors acknowledge all the participants of the study.
Funding
This study did not receive any specific grant from funding agencies.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Yau JW, Thor SM, Tsai D, Speare T, Rissel C. Antimicrobial stewardship in rural and remote primary health care: a narrative review. Antimicrob Resist Infect Control. 2021;10(1):105. doi:10.1186/s13756-021-00964-1
2. Chaaban T, Ezzeddine Z. Antibiotic misuse during the COVID-19 pandemic in lebanon: a cross-sectional study. COVID. 2024;4:921–12.
3. Wagenlehner FME, Dittmar F. Re: global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Eur Urol. 2022;82(6):658. doi:10.1016/j.eururo.2022.08.023
4. World Health Organisation. Global antibiotic resistance surveillance report 2025. 2025.
5. Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
6. Akova M. Epidemiology of antimicrobial resistance in bloodstream infections. Virulence. 2016;7(3):252–266. doi:10.1080/21505594.2016.1159366
7. Tang KWK, Millar BC, Moore JE. Antimicrobial Resistance (AMR). Br J Biomed Sci. 2023;80. doi:10.3389/bjbs.2023.11387
8. Ackers-Johnson G, Kibombo D, Kusiima B, et al. Antibiotic resistance profiles and population structure of disease-associated Staphylococcus aureus infecting patients in fort portal regional referral hospital, Western Uganda. Microbiology. 2021;167(5). doi:10.1099/mic.0.001000
9. Obakiro SB, Kiyimba K, Paasi G, et al. Prevalence of antibiotic-resistant bacteria among patients in two tertiary hospitals in Eastern Uganda. J Glob Antimicrob Resist. 2021;25:82–86. doi:10.1016/j.jgar.2021.02.021
10. Khan S, Priti S, Ankit S. Bacteria etiological agents causing lower respiratory tract infections and their resistance patterns. Iran Biomed J. 2015;19(4):240–246. doi:10.7508/ibj.2015.04.008
11. Arinze JT, de Roos EW, Karimi L, Verhamme KMC, Stricker BH, Brusselle GG. Prevalence and incidence of, and risk factors for chronic cough in the adult population: the Rotterdam Study. ERJ Open Res. 2020;6(2):00300–2019. doi:10.1183/23120541.00300-2019
12. Bergmann M, Haasenritter J, Beidatsch D, et al. Prevalence, aetiologies and prognosis of the symptom cough in primary care: a systematic review and meta-analysis. BMC Fam Pract. 2021;22(1):151. doi:10.1186/s12875-021-01501-0
13. North CM, Kakuhikire B, Vořechovská D, et al. Prevalence and correlates of chronic obstructive pulmonary disease and chronic respiratory symptoms in rural southwestern Uganda: a cross-sectional, population-based study. J Glob Health. 2019;9(1):010434. doi:10.7189/jogh.09.010434
14. Vijay S. Prevalence of Lrti in patients presenting with productive cough and their antibiotic resistance pattern. J Clin Diagn Res. 2016;10(1):DC09–DC12.
15. Martin MJ, Harrison TW. Causes of chronic productive cough: an approach to management. Respir Med. 2015;109(9):1105–1113. doi:10.1016/j.rmed.2015.05.020
16. Satia I, Mayhew AJ, Sohel N, et al. Impact of productive and dry chronic cough on mortality in the Canadian longitudinal study on aging (CLSA). J Thorac Dis. 2022;14(12):5087–5096. doi:10.21037/jtd-22-1306
17. Helmy AK, Sidkey NM, El-Badawy RE, Hegazi AG. Emergence of microbial infections in some hospitals of Cairo, Egypt: studying their corresponding antimicrobial resistance profiles. BMC Infect Dis. 2023;23(1):424. doi:10.1186/s12879-023-08397-4
18. Reta O, Daka D. Nasopharyngeal carriage rate of streptococcus pneumoniae, related risk factors, and antibiotic susceptibility among inmates in hawassa central prison institute: Hawassa, Sidama national region, Ethiopia. Heal Serv Res Manag Epidemiol. 2023;10:23333928231186690.
19. Gebre AB, Begashaw TA, Ormago MD. Bacterial profile and drug susceptibility among adult patients with community acquired lower respiratory tract infection at tertiary hospital. Southern Ethiopia. 2021;21:1–10.
20. Murdoch DR, Morpeth SC, Hammitt LL, et al. Microscopic analysis and quality assessment of induced sputum from children with pneumonia in the PERCH study. Clin Infect Dis. 2017;64(Suppl 3):S271–9. doi:10.1093/cid/cix083
21. Arun N, Saurabh K, Muni S, Kumari N, Dev A. A comparative study of bacterial infections between COVID-19 and non-COVID-19 patients with respect to different isolates and their antibiotic sensitivity pattern. Cureus. 2023;15(6).
22. Durdu B, Meric Koc M, Hakyemez IN, et al. Risk factors affecting patterns of antibiotic resistance and treatment efficacy in extreme drug resistance in intensive care unit-acquired klebsiella pneumoniae infections: a 5-year analysis. Med Sci Monit. 2019;25:174–183. doi:10.12659/MSM.911338
23. Basak S, Singh P, Rajurkar M. Multidrug resistant and extensively drug resistant bacteria: a study. J Pathog. 2016;2016:1–5. doi:10.1155/2016/4065603
24. Kishimbo P, Sogone NM, Kalokola F, Mshana SE. Prevalence of gram negative bacteria causing community acquired pneumonia among adults in Mwanza City, Tanzania. Pneumonia. 2020;12(1):7. doi:10.1186/s41479-020-00069-0
25. Ullah K, Baloch M, Saleem F, Khan AA, Saeed H, Islam M. Antibiotic susceptibility patterns of bacterial isolates of patients with upper respiratory tract infections. Brazilian J Pharm Sci. 2022;58:1–14.
26. Iroezindu MO, Chima EI, Isiguzo GC, et al. Sputum bacteriology and antibiotic sensitivity patterns of community-acquired pneumonia in hospitalized adult patients in Nigeria: a 5-year multicentre retrospective study. Scand J Infect Dis. 2014;46(12):875–887. doi:10.3109/00365548.2014.954263
27. Shanmugam S, Thekkinkattil M, Kanayalal M, M C, Mohnot C, M K. Surveillance data on micro-organisms in respiratory tract infections at a tertiary care teaching hospital in South India. Int J Res Med Sci. 2015;3(9):2366–2375. doi:10.18203/2320-6012.ijrms20150633
28. Chebib N, Cuvelier C, Malézieux-Picard A, et al. Pneumonia prevention in the elderly patients: the other sides. Aging Clin Exp Res. 2021;33(4):1091–1100. doi:10.1007/s40520-019-01437-7
29. van Aalst M, Lötsch F, Spijker R, et al. Incidence of invasive pneumococcal disease in immunocompromised patients: a systematic review and meta-analysis. Travel Med Infect Dis. 2018;24(April):89–100. doi:10.1016/j.tmaid.2018.05.016
30. Smith EL, Wheeler I, Adler H, et al. Upper airways colonisation of Streptococcus pneumoniae in adults aged 60 years and older: a systematic review of prevalence and individual participant data meta-analysis of risk factors. J Infect. 2020;81(4):540–548. doi:10.1016/j.jinf.2020.06.028
31. Brooks LRK, Mias GI. Streptococcus pneumoniae’s virulence and host immunity: aging, diagnostics, and prevention. Front Immunol. 2018;9(June):1366. doi:10.3389/fimmu.2018.01366
32. Ghssein G, Ezzeddine Z. The key element role of metallophores in the pathogenicity and virulence of staphylococcus aureus: a review. Biology. 2022;11(10):1525. doi:10.3390/biology11101525
33. Abbas R, Chakkour M, Zein H, Dine E, Obaseki EF, Obeid ST. General overview of klebsiella pneumonia: epidemiology and the role of siderophores in its pathogenicity. Biology. 2024;13(2):78. doi:10.3390/biology13020078
34. Geleta D, Abebe G, Alemu B, Workneh N, Beyene G. Mechanisms of bacterial drug resistance with special emphasis on phenotypic and molecular characterization of extended spectrum beta-lactamase. New Microbiol. 2024;47(1):1–14.
35. Castanheira M, Simner PJ, Bradford PA. Extended-spectrum β-lactamases: an update on their characteristics, epidemiology and detection. JAC-Antimicrobial Resist. 2021;3(3). doi:10.1093/jacamr/dlab092
36. Matapa K, Dix-Peek T, Cockeran R, Anderson R, Steel H, Feldman C. Cigarette smoke exposure induces expression of the pneumococcal erm(B) macrolide resistance gene. Tob Induc Dis. 2019;17(November). doi:10.18332/tid/113528
37. Baraz A, Chowers M, Nevo D, Obolski U. The time-varying association between previous antibiotic use and antibiotic resistance. Clin Microbiol Infect. 2023;29(3):390.e1–390.e4. doi:10.1016/j.cmi.2022.10.021
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.