Back to Journals » Clinical Epidemiology » Volume 11
Survival, effect measures, and impact numbers after dementia diagnosis: a matched cohort study
Authors Garre-Olmo J ![]() , Ponjoan A
, Ponjoan A ![]() , Inoriza JM
, Inoriza JM ![]() , Blanch J
, Blanch J ![]() , Sánchez-Pérez I
, Sánchez-Pérez I ![]() , Cubí R, de Eugenio R, Turró-Garriga O
, Cubí R, de Eugenio R, Turró-Garriga O ![]() , Vilalta-Franch J
, Vilalta-Franch J
Received 23 April 2019
Accepted for publication 13 June 2019
Published 16 July 2019 Volume 2019:11 Pages 525—542
DOI https://doi.org/10.2147/CLEP.S213228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Josep Garre-Olmo, 1– 3 Anna Ponjoan, 1, 4– 5 José Maria Inoriza, 6,7 Jordi Blanch, 4 Inma Sánchez-Pérez, 6 Rafel Cubí, 4 Rosa de Eugenio, 7 Oriol Turró-Garriga, 1,2 Joan Vilalta-Franch
On behalf of the Registry of Dementia of Girona Study Group (ReDeGi Study Group) 1
1Research Group on Ageing, Disability and Health, Girona Biomedical Research Institute (IDIBGI), Catalonia, Spain; 2Registry of Dementia of Girona, Health Assistance Institute, Catalonia, Spain; 3Department of Medical Sciences, School of Medicine, University of Girona, Catalonia, Spain; 4Vascular Health Research Group (ISV-Girona), Foundation University Institute for Primary Health Care Research Jordi Gol I Gurina, Catalonia, Spain; 5Autonomous University of Barcelona, Catalonia, Spain; 6Research Group on Health Services and Health Outcomes (GRESSIRES), Integrated Health Services Baix Empordà (SSIBE), Catalonia, Spain; 7Hospital de Palamós, Integrated Health Services Baix Empordà (SSIBE), Catalonia, Spain
Background: Knowledge on survival after diagnosis is important for all stakeholders. We aimed to estimate the survival and life expectancy after a dementia diagnosis, and to quantify the impact of dementia subtypes on mortality.
Methods: Retrospective matched cohort study using a linkage between a dementia-specific registry and two primary care electronic medical records databases. Between 1 January 2007 and 31 December 2015 there were 5,156 subjects aged 60 years and over registered by the Registry of Dementia of Girona and matched to 15,468 age-sex and comorbidity individuals without dementia attended by general practitioners in the province of Girona (Catalonia, Spain).
Results: The median survival was 5.2 years (95% CI 5.0 to 5.4), the median life expectancy was 74.7 years (95% CI 71.9 to 76.5), and there were differences by gender. The mortality rate was 127.1 per 1,000 person-years (95% CI 121.6 to 132.7), and the hazard ratio for mortality in persons with dementia ranged between 1.63 (95% CI 1.52 to 1.76) for Alzheimer’s disease and 2.52 (95% CI 1.90 to 3.35) for Parkinson-plus syndromes. There was one death per year attributable to dementia for every 18.6 persons with dementia, and for every 2.4 persons with dementia who die, one death was attributable to dementia.
Conclusion: The prognosis after dementia diagnosis is conditioned by demographic and clinical features. Although survival is larger for women, they also experience a higher number of years of life lost. Parkinson-plus syndromes and dementia due to multiple etiologies are among the most malignant subtypes regarding mortality.
Keywords: epidemiology, diagnosis, dementia, mortality
Corrigendum for this paper has been published
Introduction
The estimated number of people with dementia is expected to triple from 44 million in 2013 to 135 million in 2050.1 Alzheimer’s disease and cerebrovascular disease are the main causes of dementia, but dementia may occur in other less common conditions.2 Compared with persons without dementia, dementia patients have decreased survival rates, and an increased risk of mortality at a given age than those peers without dementia.3 Among mortality risk factors, there has been reported the age of onset, the male gender, the disease severity at time of diagnosis, the dementia subtype, the multimorbidity, and the socio-demographic characteristics.4–6
Despite these general figures related to the malignancy of dementia, there are inconsistencies about the magnitude of the association of risk factors with mortality, and there are variations on the estimates of survival, ranging between 3 years up to 10 years.7 Methodological differences across the studies, such as the inclusion of prevalent or incident cases, the sampling frame, the length of follow-up, and the characteristics of free-dementia comparison group have contributed to inconclusive results.4–6 Moreover, there is an important lack of information on mortality in infrequent dementia subtypes, and due to their low incidence, available data are imprecise and scarce.8–11
A better knowledge on survival time after dementia subtype diagnosis is crucial for patients, families, practitioners and public health planning. Our objectives were: i) to estimate the median survival and life expectancy after a dementia diagnosis compared with age-sex and comorbidity matched individuals without dementia; ii) to provide age-and-gender specific mortality rates; iii) to quantify the effect of dementia on mortality compared with individuals without dementia; iv) to calculate measures of the impact of dementia and diagnostic subtype on the mortality of the patients.
Methods
Study design and data sources
We performed a retrospective age-sex and comorbidity matched cohort study with a 1:3 matching ratio to pair dementia individuals aged 60 years and over with subjects without dementia. We linked a dementia-specific registry and two primary care electronic health records databases using encrypted subjects’ identifiers. The dementia-specific registry used was the Registry of Dementias of Girona (ReDeGi), which registers demographic and clinical data of all the incident cases of dementia diagnosed in the neurology or geriatrics outpatient consultation offices or in the memory clinics of the seven hospitals of the public health care system of the province of Girona (North-East of Catalonia, Spain). The methodological principles of the ReDeGi have been previously described.12 Briefly, a specialist technician of the ReDeGi periodically reviews the medical chart of the notified cases of dementia and registers demographic and clinical information related to the dementia diagnosis workup. Specialist physicians from each hospital in the ReDeGi catchment area examined and diagnosed patients with dementia. All dementia diagnoses were based on an interview with the patient and the caregiver, a general medical examination, haematology and blood chemistry tests, and neuroimaging if required. Dementia diagnoses in the ReDeGi are performed on the basis of the DSM-IV-TR13 criteria, and in a complementary fashion, clinical research criteria are used for dementia subtypes.14–19 Diagnoses were made in the neurology or geriatrics outpatient consultation offices or in the memory clinics of each hospital. Cases were identified and notified to the ReDeGi by the consultants of each HRG hospital who make dementia diagnoses. The adherence to the clinical practice guidelines (CPGs) among the clinical specialists in the catchment area of the ReDeGi during the study period was high. Specifically, the index of adherence to the CPGs was 8.2 out of 9 points, and there were no differences in the adherence index depending on the dementia subtype.20
The primary care electronic health records databases used were the Information System for the Development of Research in Primary Care (SIDIAP) and the Serveis de Salut Integrats Baix Empordà (SSIBE). Both databases include medical information recorded by general practitioners in the catchment area of the ReDeGi. The SIDIAP is representative of the general Catalan population in terms of geography, age and sex distributions, according to the official census data and has been validated for research purposes through a validation comparative procedure.21,22 The SSIBE is an integrated healthcare management organisation responsible for providing public healthcare services, including primary care, specialised care, acute hospitalisation and long-term residential care of the county Baix Empordà, located in the catchment area of the ReDegi. The SSIBE runs an integrated patient database with clinical records and with individual information on the use of resources and activity for the whole population, and has been previously used for research purposes.23,24
Ethical considerations
The study protocol and the use of anonimized data was approved by the Institutional Review Board of the IDIAP Jordi Gol (P16/066), and the SSIBE Research Committee. Written informed consent was obtained for patients registered by the ReDeGi.
Cohort construction
Exposed participants were those registered by the ReDeGi between 2007 and 2015, and were categorized according to the following categories: Alzheimer’s disease (AD), vascular dementia (including mixed dementia) (VaD), frontotemporal dementia (FTD), Lewy Body dementia (LBD), Parkinson-Plus Syndromes (PPS), dementia due to multiple aetiologies (DMA), dementia not specified (DNS), and dementia in other diseases (DOD) (see Supplemental file). Non-exposed participants were a random sample of individuals without a dementia diagnosis before or during the entire observational period, and selected from the same primary care electronic health records database. For the exposed participants, the date of the diagnosis of dementia was defined as the index date, and the same date was used as the index date for the non-exposed matched subjects. The matching procedure included age, sex and the Clinical Risk Group (CRG) status category, or the Charlson Comorbidity Index (CCI). The CRG status is a measure of the individual morbidity based on the electronic health records codes and provides a single and mutually exclusive health status category.25 The CCI is a valid and reliable age-weighted measure of the individual comorbidity based on the number and severity of 19 predefined conditions.26,27
Measurements
The age, sex, date of dementia diagnosis, the Clinical Dementia Rating (CDR)28 score, and the dementia subtype diagnostic category were retrieved from the ReDeGi database for participants with dementia. For matched participants, age and sex were retrieved from the primary care electronic health records databases. The CRG score or the CCI score at the time of inclusion, and the vital status at 31st December 2015 (and the date of death for deceased individuals) for all participants were retrieved from the primary care electronic health records databases.
Statistical analysis
The following analyses were performed in order to quantify the impact of dementia on mortality based on left-truncated and right-censored data. We estimated mortality rates using the person-years method.29 Person-years of observation corresponded to the interval between the date of dementia diagnosis for patients, or the date of cohort inclusion for matched individuals, and the date of death or 31 December 2015. All individuals alive on 31 December 2015 or after were censored in the analysis. We calculated 95% confidence intervals (CIs) for mortality rates assuming a Poisson distribution. We computed the mortality rate ratio as the ratio of the death rate for individuals with dementia to the death rate for those without dementia. To compute the median survival years after the diagnosis we used the time on study as the time scale, and to compute the life expectancy we used the subject’s age as time scale.30 We constructed Kaplan-Meier survival curves to estimate the survival distribution, and we used the log-rank test to compare survival years and life expectancy between groups. The number of years of life lost was computed as the difference in life expectancy between participants with and without dementia. In order to control for potential changes in the diagnosis procedures or treatment practices during the study period, we conducted a sensitivity analysis. Specifically, we estimated the median life expectancy for participants included in each calendar year (which had different follow-up periods), and we compared the results for individuals with at least 4 years of follow up with those with a shorter follow-up period. To compare the mortality risk of dementia subtypes we used the Cox proportional hazard model to compute the hazard ratios of death with 95% CI. To measure the effect of dementia in patients’ mortality we calculated the absolute risk increase, the attributable fraction among the exposed, the exposure impact number, the exposed cases impact number, and their associated 95% CI.31,32 All statistical analyses were conducted using STATA 12 SE (STATA Corp. College Station, TX, USA), and we employed an alpha level for statistical significance of 0.05 (two-tailed).
Results
Between 2007 and 2015 the ReDeGi registered 5,323 cases of dementia aged 60 years and over diagnosed in the catchment area. Of these, dementia severity or vital status was missing for 41 and 126 cases respectively, which were excluded. Valid cases included 5,156 individuals with dementia of which 58.3% corresponded to AD, 19.6% were diagnosed as VaD, 5.7% were diagnosed as DNS, 4.7% corresponded to LBD, 3.3% corresponded to PPS, 3.1% were diagnosed as DMA, 2.6% were diagnosed with FTD, and 2.7% corresponded to DOD. The mean age was 80.4 (SD=6.4) years, and 63.7% were female. Dementia severity was mild in 61.7% of the cases, moderate in 29.1%, and severe in 9.2%. There were differences on demographics and severity between dementia subtypes (see Table S1). The matched group included 15,468 individuals without dementia, with a mean age of 80.5 years (SD=6.4) and two thirds were females (63.7%).
The follow-up time ranged between 2 days and 8.9 years, with 16,091 person-years of follow-up for subjects with dementia, and 54,470 person-years of follow-up for subjects without dementia. Among individuals with dementia, 39.7% (95% CI 38.3 to 41.0) died compared to 25.9% (95% CI 25.1 to 26.6) in subjects without dementia. The median survival years for individuals with dementia was 5.2 years (95% CI 5.0 to 5.4), and 8.4 years (95% CI 8.1 to NA) for subjects without dementia (log-rank test =457.4, p<0.001). The median life expectancy for individuals with dementia was 74.7 years (95% CI 71.9 to 76.5), and for individuals without dementia was 83.5 years (95% CI 81.9 to 84.8) (log-rank test =474.2, p<0.001). Table 1 shows median survival years and median life expectancy for individuals with and without dementia stratified by gender and age groups. The sensibility analysis did not report differences in the median life expectancy according the length of the follow up (Table S2). Figure 1 shows the Kaplan-Meier cumulative curves for the survival and life expectancy after the diagnosis of dementia stratified by disease severity.
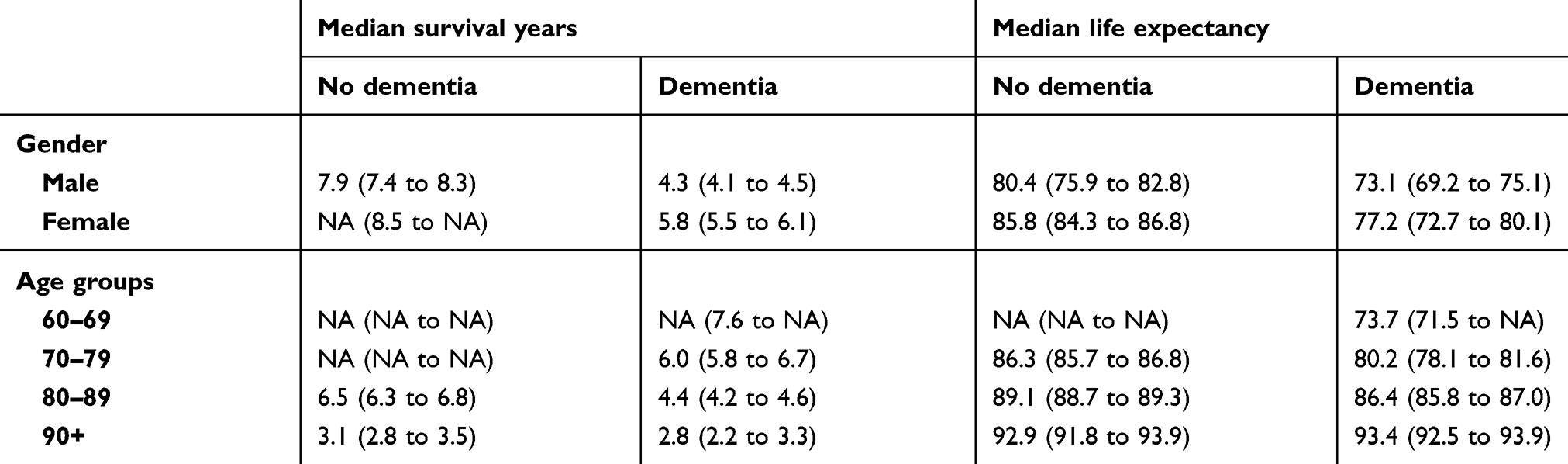 |
Table 1 Median (95% CI) survival time and median life expectancy (in years) for individuals with (n=5,156) and without (n=15,468) dementia stratified by gender and age groups in the province of Girona (Catalonia, Spain), 2007–2015 |
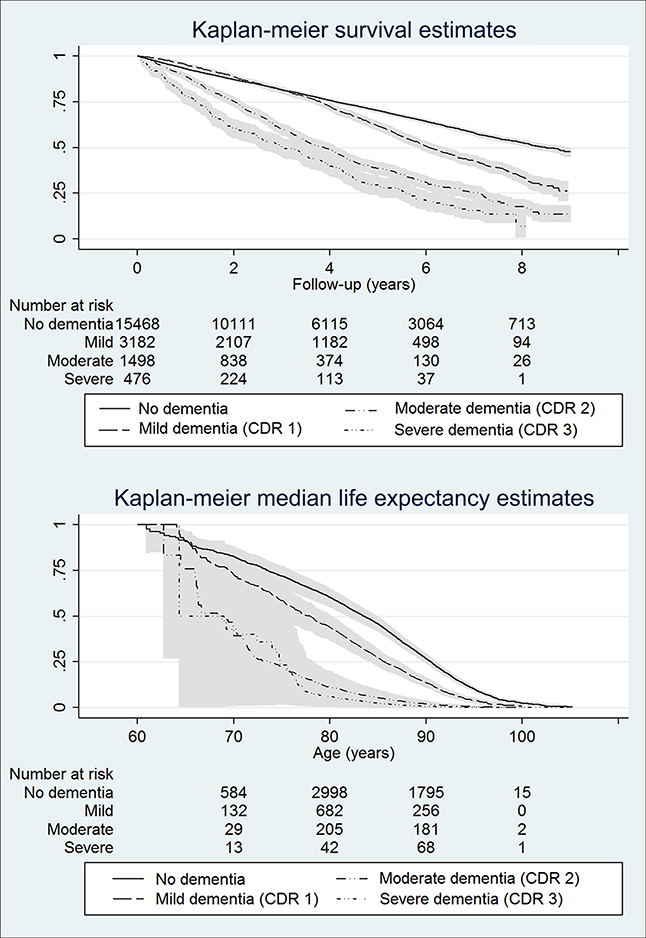 |
Figure 1 Kaplan-Meier survival and life expectancy curves for people without and with dementia stratified by disease severity in the province of Girona (Catalonia, Spain), 2007–2015. Abbreviation: CDR, clinical dementia rating. |
The mortality rate for subjects with dementia was 127.1 per 1,000 person-years (95% CI 121.6 to 132.7), and for subjects without dementia was 73.4 per 1,000 person-years (95% CI 71.2 to 75.7). The absolute risk increase was 53.7 per 1,000 person-years (95% CI 71.2 to75.7), and the mortality rate ratio was 1.73 (95% CI 1.64 to 1.82). The attributable fraction in exposed was 42.2% (95% CI 39.0 to 45.2), the exposure impact number was 18.6 (95% CI 16.8 to 21.0), and the exposed cases impact number was 2.4 (95% CI 2.2 to 2.6). Table 2 shows mortality rates and mortality rate ratios for individuals with and without dementia stratified by gender and age groups, and the impact measures for dementia individuals (Table S3 reports the number of events and person-years stratified by gender and age groups). For individuals aged 90 years and over, dementia did not increase the mortality rate compared to the non-dementia individuals.
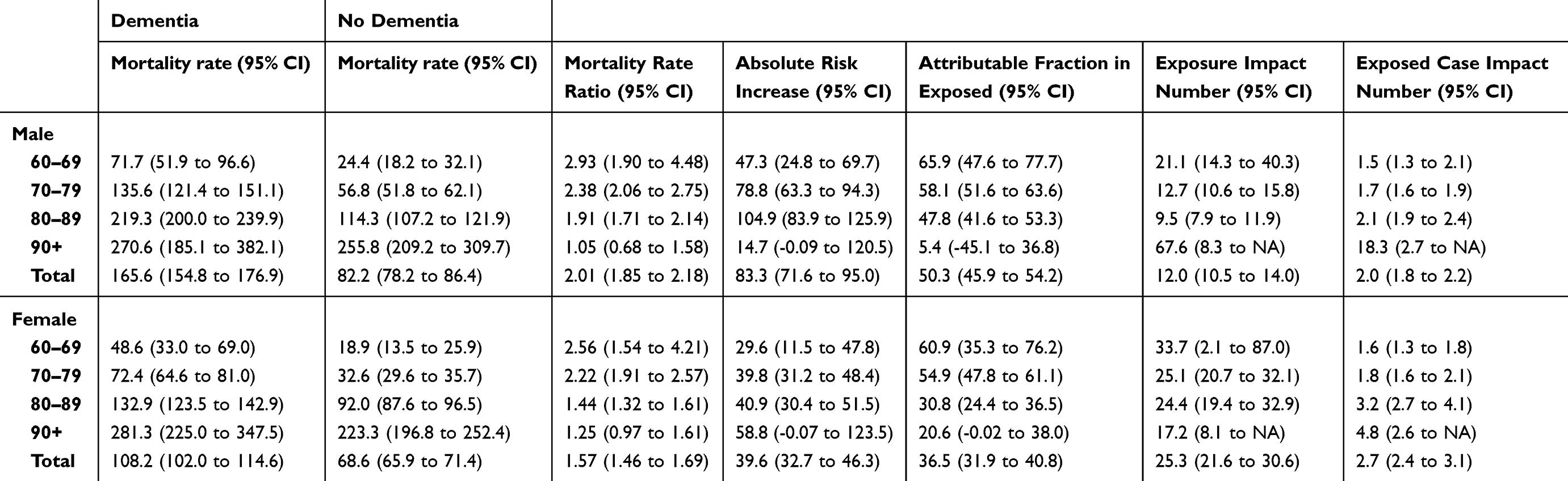 |
Table 2 Mortality rates and 95% confidence intervals (95% CI) per 1000 person-years and impact measures for individuals with (n=5,156) and without (n=15,468) dementia stratified by gender and age groups in the province of Girona (Catalonia, Spain), 2007–2015 |
Tables 3 and 4 report the median survival years and the life expectancy for specific dementia subtypes respectively. AD was the subtype with the best prognosis, both regarding the survival estimates and the life expectancy, while other dementias subtypes, such as PPS, DMA, DNS, and DOD, showed the worst prognosis with a life expectancy below 72 years. Consistently, lower survival time for all dementia diagnostic subtype categories was observed as dementia severity increased. The hazard ratio for death associated with a diagnosis of dementia was 1.79 (95% CI 1.70 to 1.89). There were differences in the hazard ratio for death depending on the subtype of dementia, being AD the diagnostic subtype with the lowest risk (1.63, 95% CI 1.52 to 1.76), and the diagnostic of Parkinson-plus syndromes the one with the highest risk of mortality (2.56, 95% CI 1.90 to 3.35). Figure S1 reports the hazard ratios for mortality stratified by dementia subtype, and the number of years of life lost using the matched non-dementia group as reference for each dementia subtype. Table S4 reports the number of deaths and person-years stratified by gender and dementia diagnostic category, and Table S5 reports the specific mortality rates, the mortality rate ratios, and the impact measures for each dementia subtype stratified by gender.
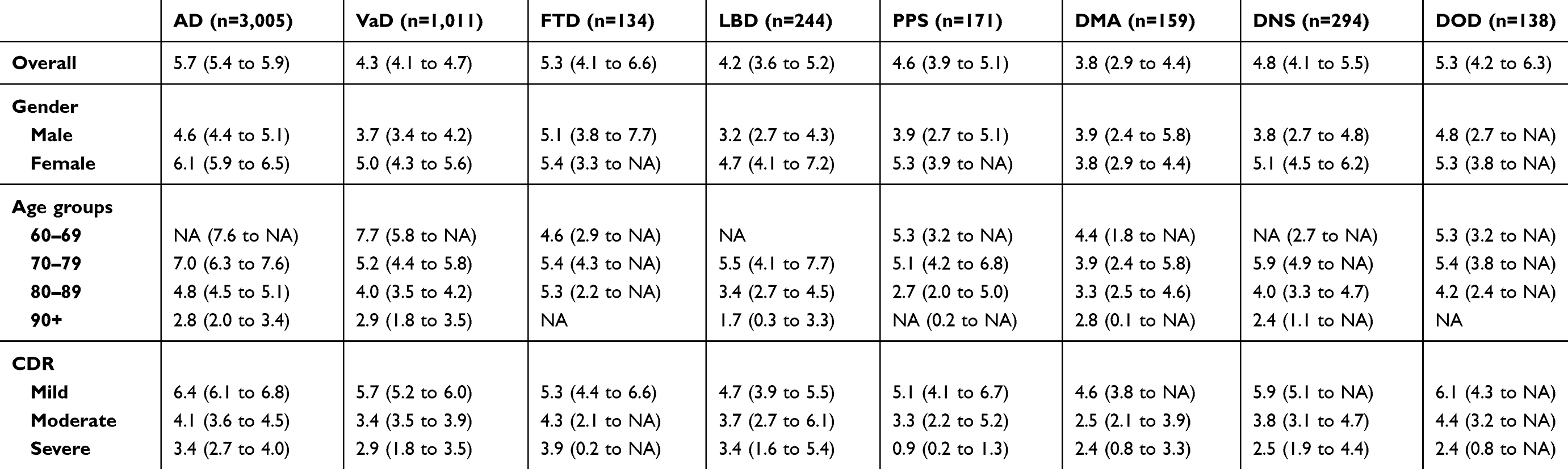 |
Table 3 Median (95% CI) survival time after diagnosis for dementia subtypes by gender, age and disease severity groups in the province of Girona (Catalonia, Spain), 2007–2015 |
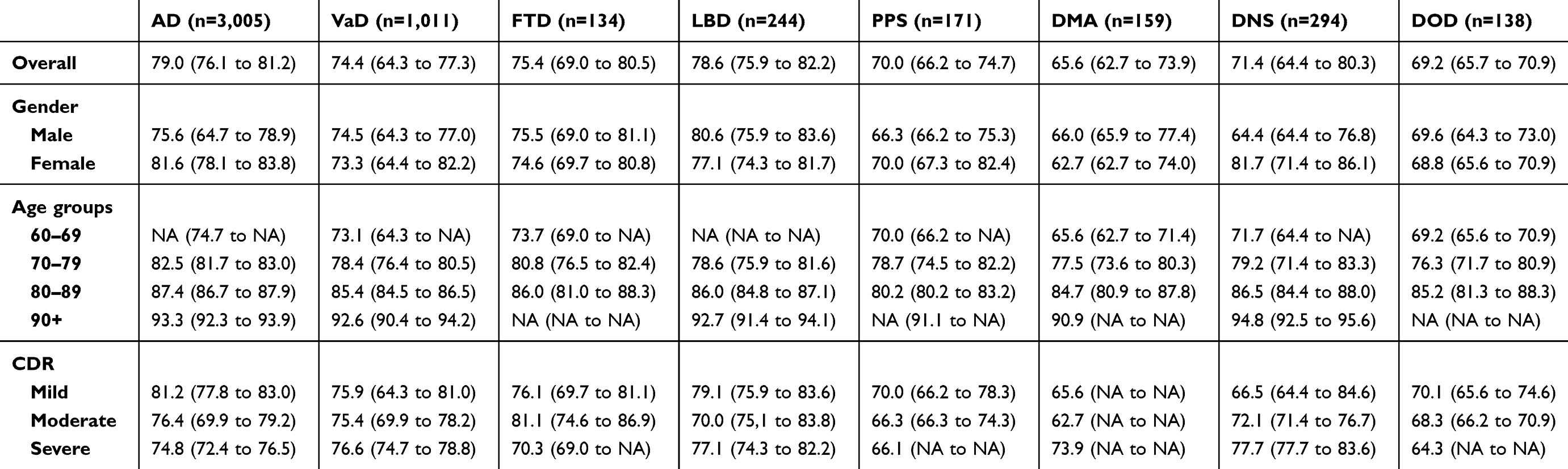 |
Table 4 Median (95% CI) life expectancy (in years) for dementia subtypes by gender, age and disease severity groups in the province of Girona (Catalonia. Spain), 2007–2015 |
Discussion
Main findings
Our study showed a reduction in life expectancy due to dementia of 8.8 years and a difference between women and men of 1.5 years in estimated survival after the diagnosis of dementia. However, compared to men, women experienced a reduction of 1.3 years in their life expectancy. We found that people with dementia had 1.73 times as many deaths per year of follow-up compared with matched persons without dementia. Among dementia individuals, 42.2% of deaths were due to dementia. For every 18.6 people with dementia, there was on average one death per year attributable to dementia, and for every 2.4 persons with dementia who died, on average one death was attributable to dementia. The prognosis after diagnosis was conditioned to age, gender, disease severity, and dementia subtype, being the PPS and DMA the most malignant subtypes in terms of risk of death and life. Dementia diagnosis after 90 years did not reduce life expectancy. This study provides age- and gender-specific estimates of prognosis after dementia diagnosis, and highlights important differences according to disease severity and dementia subtype. Mortality rates and effect measures are important for public health planning and policy makers when estimating the cost of dementia in healthcare and social systems. We also report impact numbers, which are measures intuitively easy to understand, and can be useful when communicating the impact of dementia and several dementia diagnostic subtypes on the mortality to patients and caregivers, clinicians and healthcare providers, as well as to the general population.
Comparison with other studies
The comparison between studies on mortality and dementia should be made cautiously, as differences in methodology including study design, age of participants, and length of follow-up, among other, may be responsible for the observed differences. According to a previous systematic review, forty-two articles comprising data for more than 11,000 dementia patients reported duration from diagnosis to death ranging from 1.1 to 8.5 years on the average. However, the authors could not conduct a meta-analysis due to the large heterogeneity of the published data.4 Another systematic review reported a median survival time from the age of diagnosis ranging between 3.2 to 6.6 years for dementia or AD cohorts as a whole.5 Our estimates of survival are in agreement with prior population-based and primary-care based research reporting a decrease of survival with age at diagnosis.33,34 In addition, our mortality rate estimates fit with those obtained in a population-based study in the same geographical area, with a mortality rate between 73 and 129 per 1,000 person-years among persons aged 75 years and over.35 Likewise, the Swedish Dementia Registry estimated a mortality rate of 134 and 101 per 1,000 person-years for men and women, respectively, which also fits with our estimates.36
Regarding the estimation of other dementia-related mortality metrics, our matched design overcomes previous limitations due to the characteristics of the comparison group. Previous studies using random or only age-and sex matched samples often had a dementia-free group significantly younger and/or healthier than the dementia group, and consequently, it is difficult to disentangle if the differences in survival and life expectancy are attributable to the age, to the medical comorbidity or to dementia.4 Likewise, in the estimation of the life expectancy and the years of life lost, a common practice has been to compare the data with those from life tables for general population adjusted for gender and age.36–38 This method has the inconvenient that it may underestimate the number of years lost, because life tables include all the population, even individuals with dementia. This bias may be high for the oldest groups, for whom the prevalence of dementia is high.4
Strengths and limitations
We used an age-gender and comorbidity matched design with an open cohort of 20,624 persons and a follow-up up to 9 years. Persons with dementia were drawn from a dementia-specific registry which reduced the risk of an information bias. In the ReDeGi catchment area, suspected cases of dementia are referred by primary care physicians to memory clinics or secondary care services, most commonly located in public hospitals. The ReDeGi captures an estimated 75% of all new dementia cases in its area under surveillance, and a recent study has shown a high adherence to the clinical practice guidelines among the physicians in the catchment, indicating a high diagnostic validity.20,39 Medical comorbidity was recorded from primary care electronic health records databases, and the random sample of persons without dementia came from the same primary care area than participants with dementia, allowing us to compare survival patterns among people within the same healthcare system. The date of dementia diagnosis was used to estimate the expected survival, which has an interest from a clinical perspective, and provides important information for both patients and their families, and health professionals.40 We used age as time scale to estimate the life expectancy. This alternative approach to the standard approach for survival analysis makes an optimal use of the data by means of extending the follow-up time for each individual, providing the median age at death, which was computed as a function of time since the birth date of each individual.30 The conducted sensibility analysis strengths our life expectancy estimates, and does not suggest that our results could be confused due to possible changes in diagnostic procedures or treatment practices during the study period or due to differences in the follow-up length.
This was not a population-based study, and several limitations must be taken into account. First, the ReDeGi registers data from individuals attended in the healthcare system, and caution is needed to extrapolate our results to the general population. It could not be ruled out that the specific healthcare system can have an impact on the survival and life expectance. In this sense, our results are less comparable to other populations with differences in the organization of their healthcare systems regarding their accesibility and treatments availability. Despite this, the estimates of the magnitude of the associations are, nevertheless, generalizable. Second, we cannot exclude that some non-exposed persons may have had an undiagnosed dementia, because current literature suggests that dementia tends to be under diagnosed in primary care electronic medical records.41,42 In this case, results would be biased against dementia consequences on survival and life expectancy. Third, we classified the dementia subtypes according to the clinical diagnosis and without neuropathological confirmation, syndromic overlaps or multiple underlying pathologies cannot be ruled out.43 Fourth, we did not account for socioeconomic o education level. Socioeconomic inequalities in mortality are well-known,44 and although the precise nature of the relationship between socioeconomic status and dementia remains unclear,38 it is plausible to consider that unfavourable social determinants would be associated with an increased risk of dementia-related death independently of common risk behaviours and comorbidities.45 Fifth, due to the low incidence of different subtypes of dementia, we clustered several diagnostic categories into broader groups based on common underlying etiologic mechanisms, such as FTD and PPS groups, or based on their low frequency, such as the DOD groups. This approach may have confounded some mortality estimates, because there is evidence that some dementia phenotypes of the same general category have different survival times. For instance, heterogeneous estimates of mortality have been reported for FTD and PPS phenotypes.8,11 Furthermore, the low number of cases of these subtypes of dementia limits the precision of the mortality estimates. Sixth, we did not have information about the cause of death, nor either if dementia was the underlying cause of death. However, the use of death certificates to understand the contribution of dementia to the mortality has been questioned due to an underreport of dementia as the primary cause of death.46 Seventh, we controlled for the effect of medical comorbidity at the moment of diagnosis by using a comorbidity index instead matching on specific comorbidities. Moreover, we did not investigate competing risks of death such as the cardiovascular risk factors across the follow-up. It has been proposed the concept of “mixed mortality” to more accurately reflect the contribution of multiple processes to dying, understanding that dementia contributes to death insidiously over the course of years through a cascade of events.47 Further studies including pooled data coming from different populations, healthcare systems and countries are needed in order to better understand how co-occurring chronic conditions and dementia may influence mutually, increasing the risk of mortality.48
Conclusion
In this matched cohort study, dementia was related with an increased risk of mortality. However, the malignancy of dementia on patients’ survival showed a descending pattern with increasing age at diagnosis. Our results provide reliable up-to-date information about the effect of dementia on survival and life expectancy after the diagnosis. Our study adds to evidence that age at diagnosis, dementia subtype and disease severity are important key factors to take into account from a clinical perspective regarding the dementia-related risk of mortality.
Data availability statement
Data available on request due to privacy/ethical restrictions.
Acknowledgments
This study was supported by research grant PI05/01980 from the Spain’s Ministry of Science and Innovation through the Carlos III Health Institute. The funder had no role in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; or the preparation, review, or approval of the manuscript.The ReDeGi Group consists of the following investigators: Department of Neurology, University Hospital Josep Trueta –Santa Caterina Hospital: Berta Alemany, Cristina Coll, Anna Cots, Marta Hernàndez, Jordi Gich, Secundino Lòpez-Pousa, Manuela Lozano, AlbertMolins, Immaculada Pericot-Nierga, Lluís Ramiò-Torrentà, René Robles, Judit Salavedra, Joaquín Serena, Yolanda Silva, Berta Solano, Mikel Terceño, Antoni Turon Estrada, Joan Vilalta-Franch; Dementia Unit, Palamòs Hospital: Elisabet Alsina,Olga Belchí, Rosa de Eugenio, Erélido Hernàndez, Margarita Flaqué; Neurology Department, Figueres Hospital: Olga Carmona, Marta Cullell, Teresa Osuna, Ma del Mar Fernàndez, Cecile Van Eendenburg; Neurology and Geriatrics Departments, Olot Hospital: Josep Bisbe, Marta Linares, Fabian Marquez Daniel, Natalia Vallmajò; Neurology and Geriatrics Departments, Blanes Hospital: Héctor Perkal, Marta Viñas; Neurology Department; Campdevànol Hospital: Isabel Casas, Josefa Turbau, Josep Ma Cuy, Anna Manzano; Pharmacy Unit, Healh Region of Girona: Anna Maria Roig, Joan Coromina, Mònica Palacios Soto.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin Prince A, Wimo A, Guerchet M, et al.World Alzheimer report 2015 the global impact of dementia an analysis of prevalence, incidence, cost and trends. 2015. Available from: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf. Accessed January 8, 2019.
2. Ferrari C, Nacmias B, Sorbi S. The diagnosis of dementias: a practical tool not to miss rare causes. Neurol Sci. 2018;39(4):615–627. doi:10.1007/s10072-018-3288-3
3. Prince M, Ali G-C, Guerchet M, Prina AM, Albanese E, Wu Y-T. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimers Res Ther. 2016;8(1):23. doi:10.1186/s13195-016-0188-8
4. Brodaty H, Seeher K, Gibson L. Dementia time to death: a systematic literature review on survival time and years of life lost in people with dementia. Int Psychogeriatrics C Int Psychogeriatr Assoc. 2012;24(7):1034–1045. doi:10.1017/S1041610211002924
5. Todd S, Barr S, Roberts M, Passmore AP. Survival in dementia and predictors of mortality: a review. Int J Geriatr Psychiatry. 2013;28(11):1109–1124.
6. Guehne U, Riedel-Heller S, Angermeyer MC. Mortality in dementia. Neuroepidemiology. 2005;25(3):153–162. doi:10.1159/000086680
7. Kua EH, Ho E, Tan HH, Tsoi C, Thng C, Mahendran R. The natural history of dementia. Psychogeriatrics. 2014;14(3):196–201. doi:10.1111/psyg.2014.14.issue-3
8. Kansal K, Mareddy M, Sloane KL, et al. Survival in frontotemporal dementia phenotypes: a meta-analysis. Dement Geriatr Cogn Disord. 2016;41:109–122. doi:10.1159/000443205
9. Nunnemann S, Last D, Schuster T, Förstl H, Kurz A, Diehl-Schmid J. Survival in a German population with frontotemporal lobar degeneration. Neuroepidemiology. 2011;37(3–4):160–165. doi:10.1159/000331485
10. Chiu WZ, Kaat LD, Seelaar H, et al. Survival in progressive supranuclear palsy and frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2010;81(4):441–445. doi:10.1136/jnnp.2009.195719
11. Glasmacher SA, Leigh PN, Saha RA. Predictors of survival in progressive supranuclear palsy and multiple system atrophy: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2017;88(5):402–411. doi:10.1136/jnnp-2016-314956
12. Garre-Olmo J, Flaqué M, Gich J, et al. A clinical registry of dementia based on the principle of epidemiological surveillance. BMC Neurol. 2009;9:5.
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (
14. McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB consortium. Neurology. 2005;65(12):1863–1872. doi:10.1212/01.wnl.0000187889.17253.b1
15. The Lund and Manchester Groups. Clinical and neuropathological criteria for frontotemporal dementia. J Neurol Neurosurg Psychiatry. 1994;57(4):416–418. doi:10.1136/jnnp.57.4.416
16. Litvan I, Agid Y, Calne D, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP International Workshop. Neurology. 1996;47(1):1–9. doi:10.1212/WNL.47.1.1
17. Riley DE, Lang AE. Corticobasal degeneration: clinical diagnostic criteria. Adv Neurol. 2000;82:29–34.
18. [17] Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. Neurology. 1996;46(5):1470. doi:10.1212/WNL.46.5.1470
19. Neary D, Snowden JS, Gustafson L, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51(6):1546–1554. doi:10.1212/WNL.51.6.1546
20. Turró-Garriga O, Calvó-Perxas L, Vilalta-Franch J, et al. Adherence to clinical practice guidelines during dementia work-up in a real-world setting: a study from the registry of dementias of Girona. Callahan B, ed. J Alzheimer’s Dis. 2017;53(3):997–1007. doi:10.3233/JAD-170284
21. García-Gil MDM, Hermosilla E, Prieto-Alhambra D, et al. Construction and validation of a scoring system for the selection of high-quality data in a Spanish population primary care database (SIDIAP). Inform Prim Care. 2011;19(3):135–145.
22. Bolíbar B, Fina Avilés F, Morros R, et al. [SIDIAP database: electronic clinical records in primary care as a source of information for epidemiologic research]. Med Clin (Barc). 2012;138(14):617–621. doi:10.1016/j.medcli.2012.01.020
23. Inoriza JM, Coderch J, Carreras M, et al. [Measurement of morbidity attended in an integrated health care organization]. Gac Sanit. 2009;23(1):29–37. doi:10.1016/j.gaceta.2008.02.003
24. Carreras M, Ibern P, Inoriza JM. Ageing and healthcare expenditures: exploring the role of individual health status. Health Econ. 2018;27(5):865–876. doi:10.1002/hec.3635
25. Hughes JS, Averill RF, Eisenhandler J, et al. Clinical Risk Groups (CRGs). Med Care. 2004;42(1):81–90. doi:10.1097/01.mlr.0000102367.93252.70
26. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
27. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
28. Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–2414. doi:10.1212/wnl.43.3_part_1.532
29. Breslow NDN. Statistical Methods in Cander Research, Vol II: The Design and Analysis of Cohort Studies. Vol. 150. London: Oxford University Press; 1994.
30. Lamarca R, Alonso J, Gómez G, Muñoz A. Left-truncated data with age as time scale: an alternative for survival analysis in the elderly population. J Gerontol A Biol Sci Med Sci. 1998;53(5):M337–43. doi:10.1093/gerona/53A.5.M337
31. Heller RF, Dobson AJ, Attia J, Page J. Impact numbers: measures of risk factor impact on the whole population from case-control and cohort studies. J Epidemiol Community Heal. 2002;56:606–610. doi:10.1136/jech.56.8.606
32. Hildebrandt M, Bender R, Gehrmann U, Blettner M. Calculating confidence intervals for impact numbers. BMC Med Res Methodol. 2006;6:32. doi:10.1186/1471-2288-6-32
33. Rait G, Walters K, Bottomley C, Petersen I, Iliffe S, Nazareth I. Survival of people with clinical diagnosis of dementia in primary care: cohort study. BMJ. 2010;341:c3584–c3584.
34. Xie J, Brayne C, Matthews FE; Medical Research Council Cognitive Function and Ageing Study collaborators. Survival times in people with dementia: analysis from population based cohort study with 14 year follow-up. BMJ. 2008;336(7638):258–262. doi:10.1136/bmj.39433.616678.25
35. Llinàs-Regla J, López-Pousa S, Vilalta-Franch J, Garre-Olmo J, Román GC. Mortality after a diagnosis of dementia in a population aged 75 and over in Spain. Neuroepidemiology. 2008;31(2):80–88. doi:10.1159/000144088
36. Garcia-Ptacek S, Farahmand B, Kåreholt I, Religa D, Cuadrado ML, Eriksdotter M. Mortality risk after dementia diagnosis by dementia type and underlying factors: a cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis. 2014;41(2):467–477. doi:10.3233/JAD-131856
37. Luck T, Roehr S, Jessen F, et al. Mortality in Individuals with Subjective Cognitive Decline: results of the Leipzig Longitudinal Study of the Aged (LEILA75+). J Alzheimer’s Dis. 2015;48:33–42. doi:10.3233/JAD-150090
38. van de Vorst IE, Vaartjes I, Geerlings MI, Bots ML, Koek HL. Prognosis of patients with dementia: results from a prospective nationwide registry linkage study in the Netherlands. BMJ Open. 2015;5(10):e008897. doi:10.1136/bmjopen-2015-008897
39. Calvó-Perxas L, Aguirregomozcorta M, Casas I, et al. Rate of dementia diagnoses according to the degree of aging of the population. Int Psychogeriatrics. 2015;27(3):419–427. doi:10.1017/S1041610214002130
40. Bunn F, Burn A-M, Goodman C, et al. Comorbidity and dementia: a scoping review of the literature. BMC Med. 2014;12:192. doi:10.1186/s12916-014-0141-2
41. Perera G, Pedersen L, Ansel D, et al. Dementia prevalence and incidence in a federation of European Electronic Health Record databases—the European Medical Informatics Framework resource. Alzheimer’s Dement. 2017;2:130–139.
42. Jaakkimainen RL, Bronskill SE, Tierney MC, et al. Identification of physician-diagnosed Alzheimer’s disease and related dementias in population-based administrative data: a validation study using family physicians’ electronic medical records. J Alzheimer’s Dis. 2016;54(1):337–349. doi:10.3233/JAD-160105
43. Brunnström H, Englund E. Clinicopathological concordance in dementia diagnostics. Am J Geriatr Psychiatry. 2009;17(8):664–670. doi:10.1097/JGP.0b013e3181a6516e
44. McFadden E, Luben R, Wareham N, Bingham S, Khaw K-T. Occupational social class, educational level, smoking and body mass index, and cause-specific mortality in men and women: a prospective study in the European Prospective Investigation of Cancer and Nutrition in Norfolk (EPIC-Norfolk) cohort. Eur J Epidemiol. 2008;23(8):511–522. doi:10.1007/s10654-008-9267-x
45. Russ TC, Stamatakis E, Hamer M, Starr JM, Kivimäki M, Batty GD. Socioeconomic status as a risk factor for dementia death: individual participant meta-analysis of 86 508 men and women from the UK. Br J Psychiatry. 2013;203(1):10–17. doi:10.1192/bjp.bp.112.119479
46. Romero JP, Benito-León J, Mitchell AJ, Trincado R, Bermejo-Pareja F. Under reporting of dementia deaths on death certificates using data from a population-based study (NEDICES). J Alzheimers Dis. 2014;39(4):741–748. doi:10.3233/JAD-131622
47. James BD, Leurgans SE, Hebert LE, Scherr PA, Yaffe K, Bennett DA. Contribution of Alzheimer disease to mortality in the United States. Neurology. 2014;82(12):1045–1050. doi:10.1212/WNL.0000000000000513
48. Snowden MB, Steinman LE, Bryant LL, et al. Dementia and co-occurring chronic conditions: a systematic literature review to identify what is known and where are the gaps in the evidence? Int J Geriatr Psychiatry. 2017;32(4):357–371. doi:10.1002/gps.4652
Supplementary materials
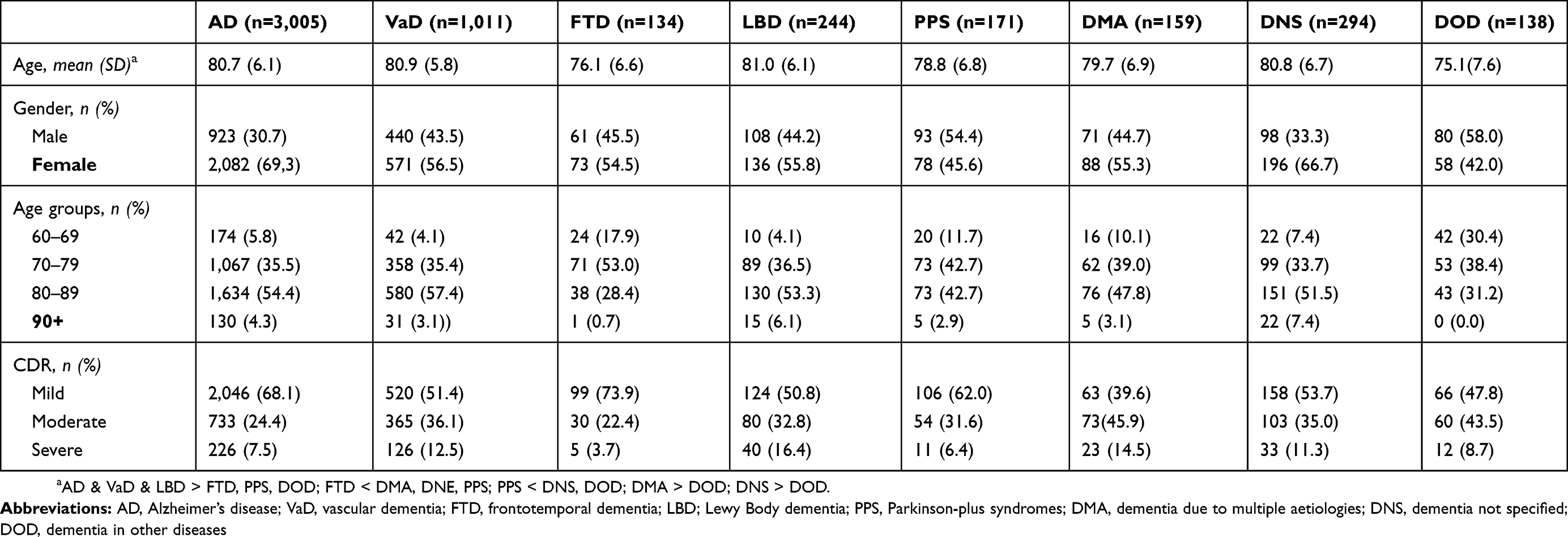 |
Table S1 Demographic and clinical severity for dementia subtypes (n=5,156) in the province of Girona (Catalonia, Spain), 2007–2015 |
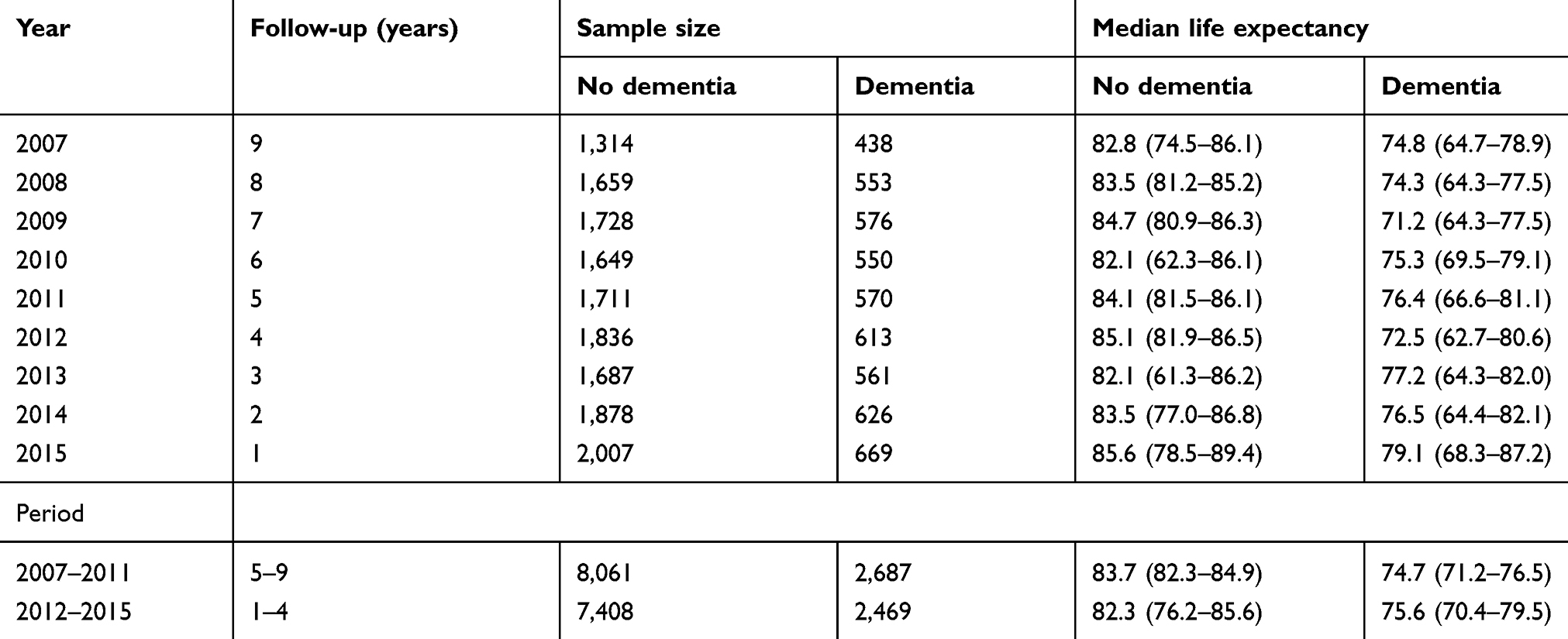 |
Table S2 Median (95% CI) life expectancy (in years) for individuals with and without dementia stratified by year, gender and age groups in the province of Girona (Catalonia, Spain), 2007–2015 |
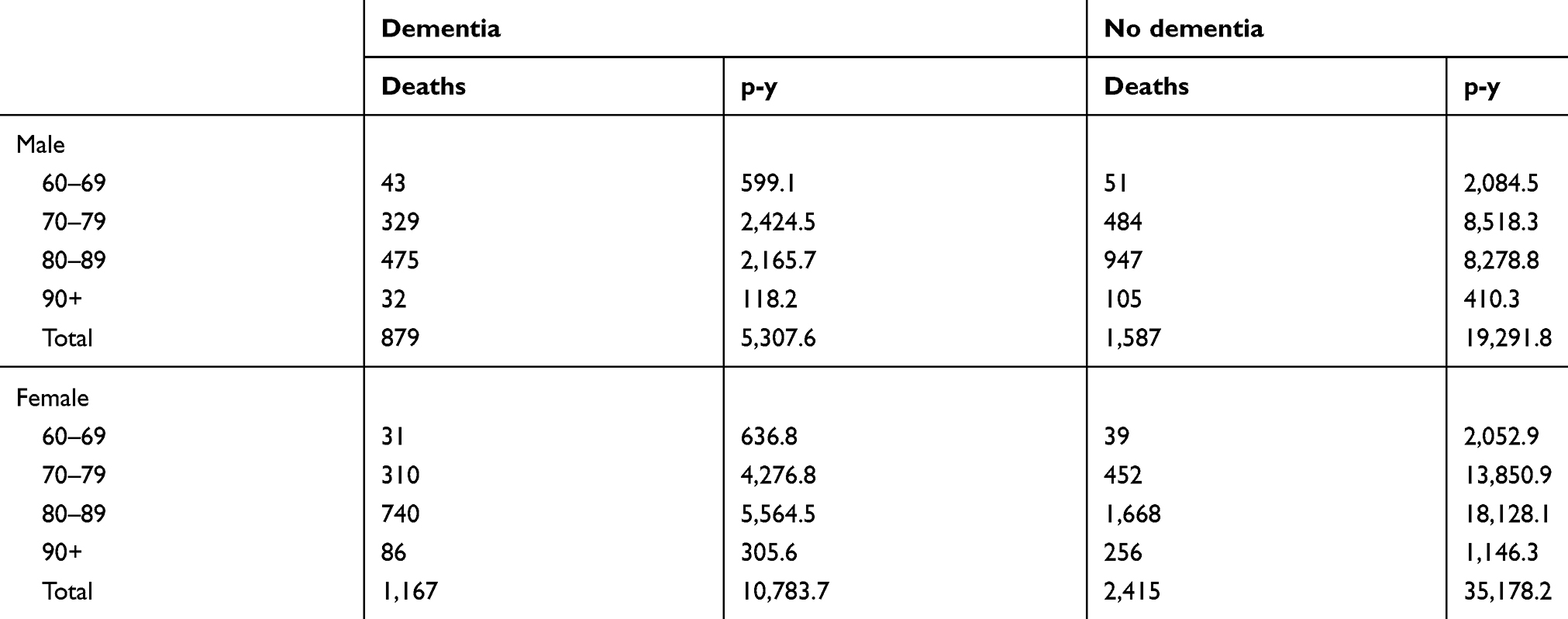 |
Table S3 Number of events and person-years (p-y) for individuals with (n=5,156) and without (n=15,468) dementia stratified by gender and age groups in the province of Girona (Catalonia, Spain), 2007–2015 |
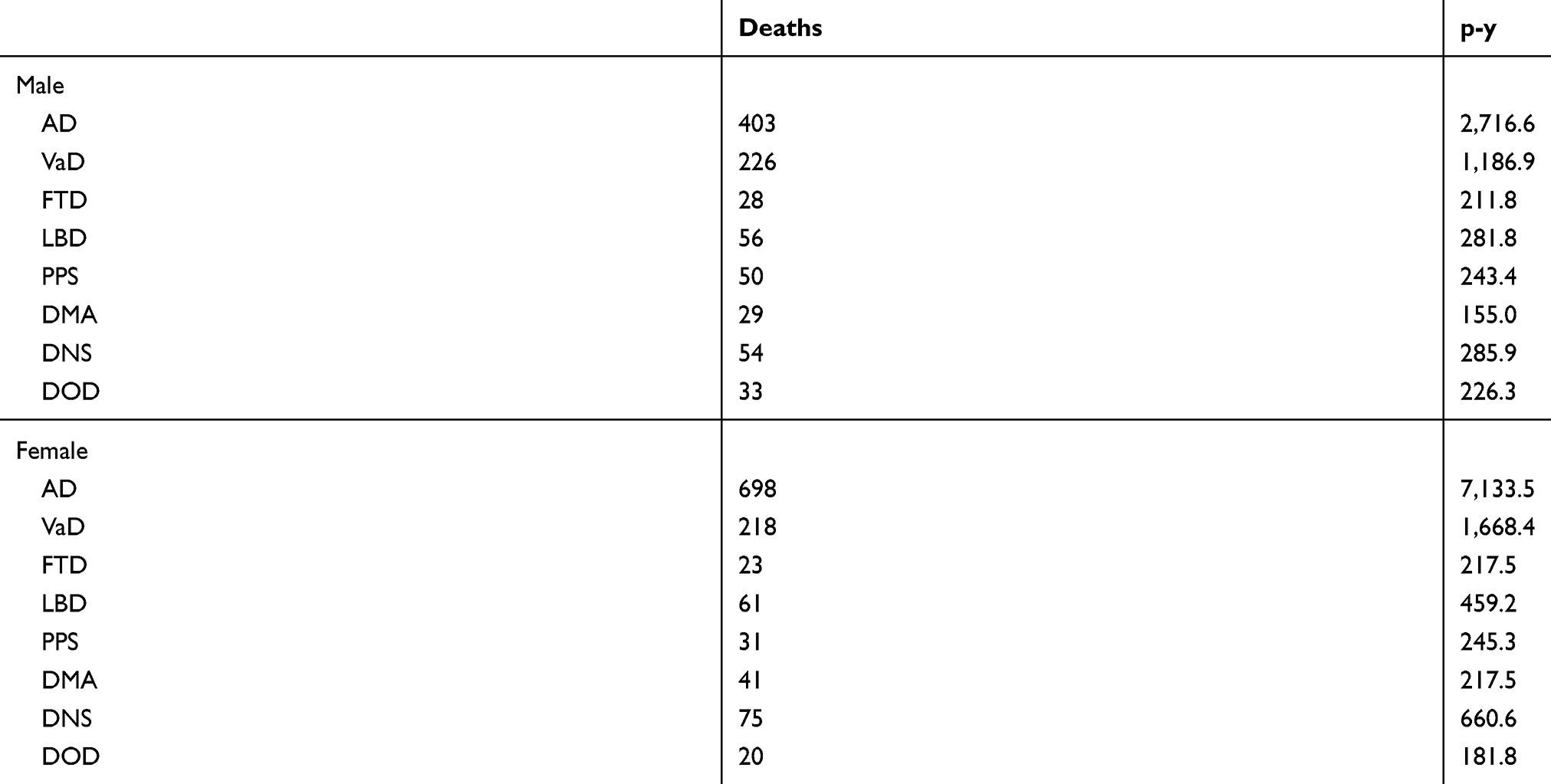 |
Table S4 Number of events and person-years for individuals with (n=5,156) and without (n=15,468) dementia stratified by gender and age groups in the province of Girona (Catalonia, Spain), 2007–2015 |
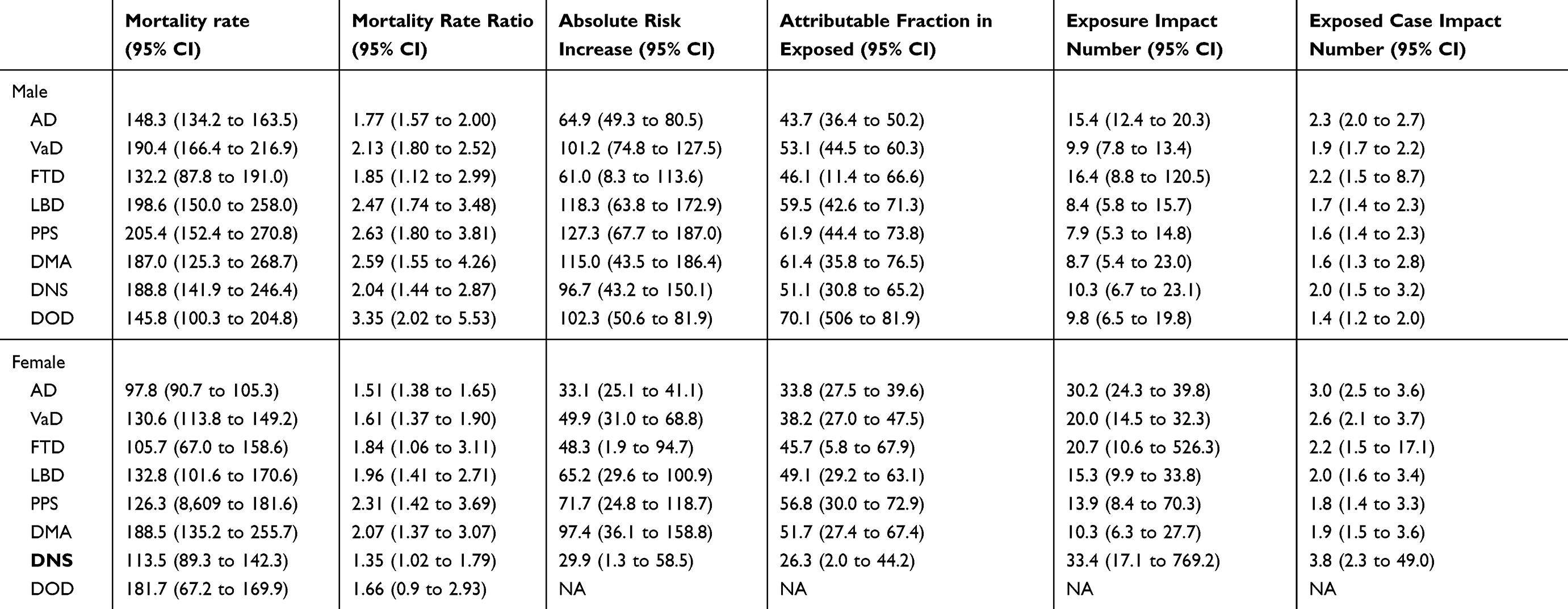 |
Table S5 Mortality rates and 95% confidence intervals (95% CI) per 1,000 person-years and impact measures for dementia subtypes (n=5,156) stratified by gender and dementia subtype in the province of Girona (Catalonia, Spain), 2007–2015 |
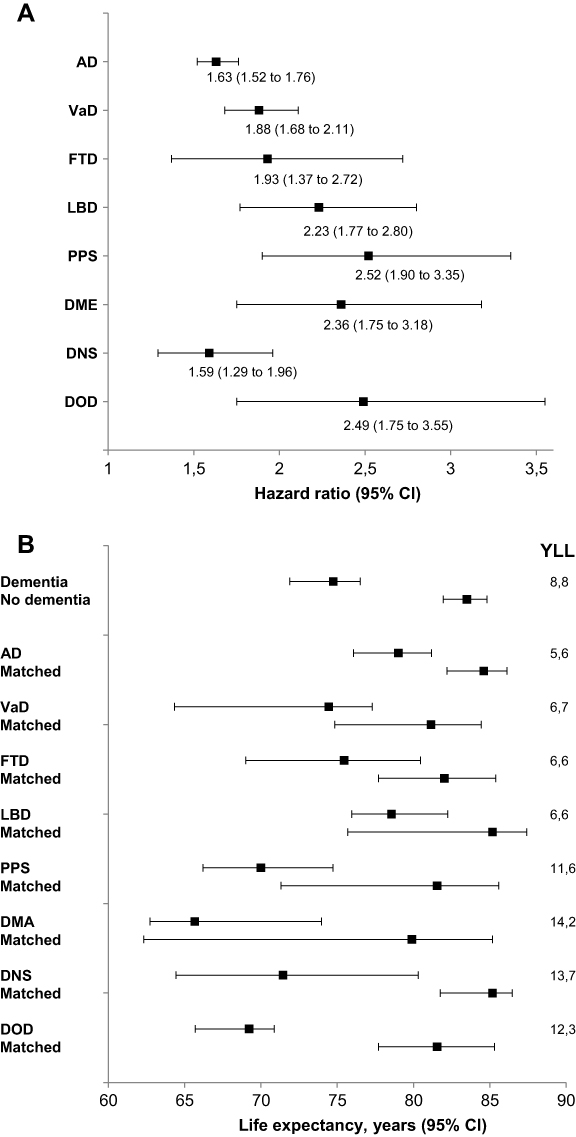 |
Figure S1 Hazard ratios for death, median life expectancy and years of life lost for people after dementia subtype diagnosis in relation to people without dementia in the province of Girona (Catalonia, Spain), 2007–2015. Abbreviations: AD, Alzheimer’s disease; VaD, vascular dementia; FTD, frontotemporal dementia; LBD; Lewy body dementia; PPS, Parkinson-plus syndromes; DMA, dementia due to multiple aetiologies; DNS, dementia not specified; DOD, dementia in other diseases; YLL, years of life lost. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.