Back to Journals » Cancer Management and Research » Volume 11
Survival After Abdominal Q-M Type B versus C2 Radical Hysterectomy for Early-Stage Cervical Cancer
Authors Chen C, Wang W, Liu P, Li P, Wang L ![]() , Jin S
, Jin S ![]() , Bin X, Lang J
, Bin X, Lang J
Received 21 June 2019
Accepted for publication 26 November 2019
Published 31 December 2019 Volume 2019:11 Pages 10909—10919
DOI https://doi.org/10.2147/CMAR.S220212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Chunlin Chen,1,* Wuliang Wang,2,* Ping Liu,1,* Pengfei Li,1,* Lu Wang,1 Shuangling Jin,3 Xiaonong Bin,4 Jinghe Lang1,5
1Department of Obstetrics and Gynecology, Nanfang Hospital, Southern Medical University, Guangzhou 510515, People’s Republic of China; 2Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Zhengzhou University, Zhengzhou 450000, People’s Republic of China; 3Department of Obstetrics and Gynecology, Peace Hospital Affiliated to Changzhi Medical College, Changzhi 046000, People’s Republic of China; 4Department of Epidemiology, College of Public Health, Guangzhou Medical University, Guangzhou 511436, People’s Republic of China; 5Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Peking Union Medical College, Beijing 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunlin Chen; Jinghe Lang
Department of Obstetrics and Gynecology, Nanfang Hospital, Southern Medical University, No. 1838, Guangzhou Avenue, Guangzhou 510515, People’s Republic of China
Tel/Fax +86 206 278 7562
Email [email protected]; [email protected]
Purpose: To evaluate the survival outcomes of abdominal Q-M type B and type C2 radical hysterectomy (RH) for early-stage (IA1 (lymphovascular invasion)-IIA2) cervical cancer.
Patients and methods: Based on this multicenter, retrospective cohort study on the clinical diagnosis and treatment for cervical cancer in China (Four C), the survival outcomes of abdominal type B and type C2 RH for early-stage cervical cancer were compared under real-world and matched cohort study conditions.
Results: In total, 46,313 cases were included in the Four C database, among whom 20,018 underwent abdominal type B or type C2 RH. In the real-world study, no differences were found in the 5-year overall survival (OS) between the type B group (n=15,471) and type C2 group (n=4547), but the 5-year disease-free survival (DFS) was lower in the type C2 group (82.1 vs 84.8%, hazard ratio: 1.144). Based on the inclusion criteria, 9135 cases were included and the type C2 group (n=1818) was found to have a lower 5-year OS and DFS (OS: 89.5 vs 92.0%, hazard ratio: 1.393; DFS: 84.3 vs 87.4%, hazard ratio: 1.342). Subsequently, 1799 cases from each group were matched and the type C2 group had a lower 5-year DFS (84.6 vs 88.4%, hazard ratio: 1.332). Upon further analysis of the subgroups, the type C2 group had a lower 5-year OS and DFS (OS: 90.3 vs 93.8%, hazard ratio: 1.522; DFS: 85.2 vs 89.4%, hazard ratio: 1.439).
Conclusion: Q-M type B RH could be used for the treatment of stage IA1 (lymphovascular invasion)-IIA2 cervical cancer.
Keywords: cervical cancer, early-stage, Q-M type B, survival outcome
Introduction
Globally, cervical cancer is the fourth most common female malignancy, with 90% of cases occurring in developing countries.1 In 2018, there were 569,847 new cases of cervical cancer and 311,365 deaths worldwide.2 Data from the Chinese National Cancer Center shows that there are more than 98,900 new cases and 30,500 deaths from cervical cancer every year in China, and the morbidity and mortality have increased in recent years.3
Surgery is the primary treatment modality for early-stage cervical cancer, and radical hysterectomy is the standard procedure. Guidelines from the National Comprehensive Cancer Network (NCCN) recommend Q-M type C RH for patients diagnosed with IB1-IIA without obvious metastasis.4 However, during Q-M type C RH, the entirety of the parametrium with the pelvic autonomic nerves is removed, leading to a high incidence of morbidity that seriously plagues cervical cancer patients.5–11 The incidence of bladder dysfunction, such as urinary retention, nocturia, urinary incontinence, and urodynamic abnormalities is reported to be 26 to 72%. Approximately 25 to 80% of patients experience anorectal dysfunction. Forms of sexual dysfunction such as decreased sexual desire and orgasm disorders 2 years after surgery occurred at incidences of 51.9 and 84.6%, respectively.
Recently, studies have found that Q-M type B RH can reduce the incidence of the aforementioned surgical complications, due to the relatively narrow scope of surgical resection. Further studies have reported that Q-M type B RH may be comparable to type C RH for selected patients with low-risk, early-stage cervical cancer.12–17 However, some of these studies had small sample sizes or did not consider baseline differences. The use of Q-M type B RH still lacks large samples of supporting data. Moreover, some studies did not consider the effect of pathology risk factors and postoperative adjuvant therapy on the survival outcomes.
Therefore, we performed this study based on a large sample of real-world data with 1:1 case-control matching, which may balance the baseline differences in factors that could influence the prognosis, to retrospectively evaluate the survival outcomes of abdominal Q-M type B and C2 RH.
Materials and Methods
Establishment of the Four C Database
This multicenter, retrospective, cohort study was approved by the Ethics Committee of Nanfang Hospital, Southern Medical University (ethics approval number NFEC-2017-135, clinical trial registration number CHiCTR1800017778, International Clinical Trails Registry Platform Search Portal, http://apps.who.Int/trialsearch/). In total, 37 hospitals in mainland China participated in the study. Individual written informed consent was waived by the ethics committee, since the information of human’s medical documents was retrospectively gathered and analyzed, and human data was unidentifiable in this study. This study was carried out in accordance with the Declaration of Helsinki and the ethical standards of the institutional and/or national research committee. The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Data Collection and Follow-Up
All hospitalized cervical cancer cases from 2004 to 2016 were identified and exported from the medical records management system of the participating hospitals, based on our previous study.18 In total, 46,313 patients were included to form the Four C database. Three hundred and fifteen relative variables including demographic and clinical details, International Federation of Gynecology and Obstetrics (FIGO) stage, histological type, tumor size, treatment modalities, physical examination, chemistry profiles, surgery related information, histopathology results before and after surgery, adjuvant therapy and complications were retrieved from medical records by well-trained gynecologists. Clinical stage was registered according to the FIGO criteria (revised 2009) before initial treatment.19 Patients whose clinical stage was recorded before 2009 were re-staged by two experienced gynecologists, referring to the original vaginal examination or imaging examination.18 Postoperative adjuvant therapy included either no treatment, chemotherapy alone, radiotherapy alone, concurrent chemo-radiotherapy or sequential chemo-radiotherapy. All patients were followed-up regularly by well-trained gynecologists from all participating units.
Data Double-Input and Management
All of the information was inputted by two gynecologists independently, using EpiData software (Version 3.1, EpiData Association, Odense, Denmark) to check for consistency. All data were summarized and managed by a designated individual.
Inclusion Criteria and Exclusion Criteria
Inclusion Criteria
The inclusion criteria of this study consisted of the following: 18 years old or older; FIGO stage IA1 (lymphovascular invasion, LVSI)-IIA2 cervical cancer; histological type of squamous-cell carcinoma, adenocarcinoma or adenosquamous carcinoma; undergoing surgery as the initial treatment without any preoperative adjuvant treatment; undergoing abdominal Q-M type B or C2 RH plus pelvic lymphadenectomy with or without para-aortic lymphadenectomy; and certain survival outcomes.
Exclusion Criteria
Exclusion criteria consisted of the following: FIGO IIB and above; no surgery performed; undergoing other types of RH other than Q-M type B or C2 RH; no pelvic and para-aortic lymph node resection performed or unknown information regarding lymph node resection; and incidental finding of cervical cancer, pregnancy with cervical cancer, stump cancer or cervical cancer in combination with other malignant tumors.
We selected cases from the Four C database based on the inclusion and exclusion criterion to run further analyses. In the subgroup analysis, we selected patients with one pathologic high-risk factor (positive vaginal margins, lymph node involvement or parametrial involvement) receiving chemo-radiotherapy or patients with any two intermediate-risk factors (tumor size >4 cm, LVSI, deep stromal invasion) receiving radiotherapy as a postoperative standard adjuvant therapy group.20
Definition of Surgery Type
The type of surgery in this study was defined using the classification of Querleu-Morrow.5 Surgery types recorded in the clinical records using the Piver–Rutledge–Smith classification were reclassified according to the new method.21
Case-Control Matching
To eliminate the influence of baseline differences on the data analysis, we used age, FIGO stage, histological subtype, tumor size, lymphovascular status, depth of tumor invasion, lymph node status, vaginal margin and parametrial status as variables for 1:1 ratio case-control matching. In the real-world study (RWS), we included all patients regardless of survival outcome. In the analysis of selected cases by inclusion criteria and subgroup analysis, the cases lost to follow-up were excluded.
Observation Indicators
The primary endpoint was OS and DFS, with a cut-off point for long-term survival outcomes at 5 years after primary surgery. OS was defined as the date of surgery to death from any cause or the last effective follow-up. DFS was defined as the date of surgery to death/relapse or the last effective follow-up.
Statistical Analysis
SPSS version 23.0 (IBM Corporation, Armonk, NY, USA) was used for the statistical analysis. Comparisons were performed via Student’s t test for continuous variables and Pearson’s chi-squared test or Fisher’s exact test for categorical variables. The survival analysis was performed using the Kaplan-Meier method, log rank test and Cox proportional hazards regression model to compare the OS and DFS for 5 years with the hazard ratio (HR) and 95% confidence interval (95% CI). The difference was considered statistically significant when P<0.05. All of the statistical methods and procedures in this study were reviewed by statistical experts.
Results
Study Population
In total, 46,313 cases of cervical cancer patients admitted to 37 hospitals in mainland China between 2004 and 2016 were included in this retrospective cohort study to form the Four C database. We initially selected 20,018 cases that underwent abdominal Q-M type B or C2 RH for a real-world analysis (type B vs type C2: 15,741 vs 4547 cases). Subsequently, 9135 cases were further selected based on the inclusion criteria (type B vs type C2: 7317 vs 1818 cases). In the subgroup analysis, 5137 cases (type B vs type C2: 4143 vs 994 cases) were selected as the postoperative standard adjuvant therapy group (Figure 1).
 |
Figure 1 Study population. |
Survival Analysis in the Initial RWS
In the RWS, we included 20,018 patients who underwent abdominal Q-M type B or type C2 RH for the survival analysis. The OS at 5 years was 90.1% in the Q-M type B RH group and 88.7% in the type C2 group (P=0.087) (Figure 2A). Patients who underwent type C2 RH had a shorter 5-year DFS than those who underwent type B RH (82.1 vs 84.8%, P=0.002; HR, 1.444, 95% CI, 1.027 to 1.275, P=0.014) (Figure 2B).
 |
Figure 2 Kaplan-Meier estimates of overall survival (OS) and disease-free survival (DFS) in the initial RWS. (A) The 5-year OS of the Q-M type B group and the type C2 group were similar (P=0.087). (B) The 5-year DFS of the Q-M type C2 group was shorter than that of the type B group (82.1 vs 84.8%, P=0.002). |
Survival Analysis Based on the Inclusion Criteria
In total, 9135 cases were selected for further analysis based on the inclusion criteria. The baseline characteristics of the patients are summarized in Table 1. The type C2 group had a shorter OS and DFS than the type B group (OS: 89.5 vs 92.0%, P=0.002; HR, 1.392, 95% CI, 1.158 to 1.673, P<0.001; DFS: 84.3 vs 87.4%, P<0.001; HR, 1.342, 95% CI, 1.159 to 1.553, P<0.001) (Figure 3A and B). In the 1:1 matched cohort study, 1799 cases from each group were selected. The OS at 5 years was 91.4% in the type B RH group and 89.5% in the type C2 group (P=0.089) (Figure 3C). Patients who underwent type C2 RH had a shorter DFS than those who underwent type B RH (84.6 vs 88.4%, P=0.003; HR, 1.332, 95% CI, 1.097 to 1.617, P=0.004) (Figure 3D).
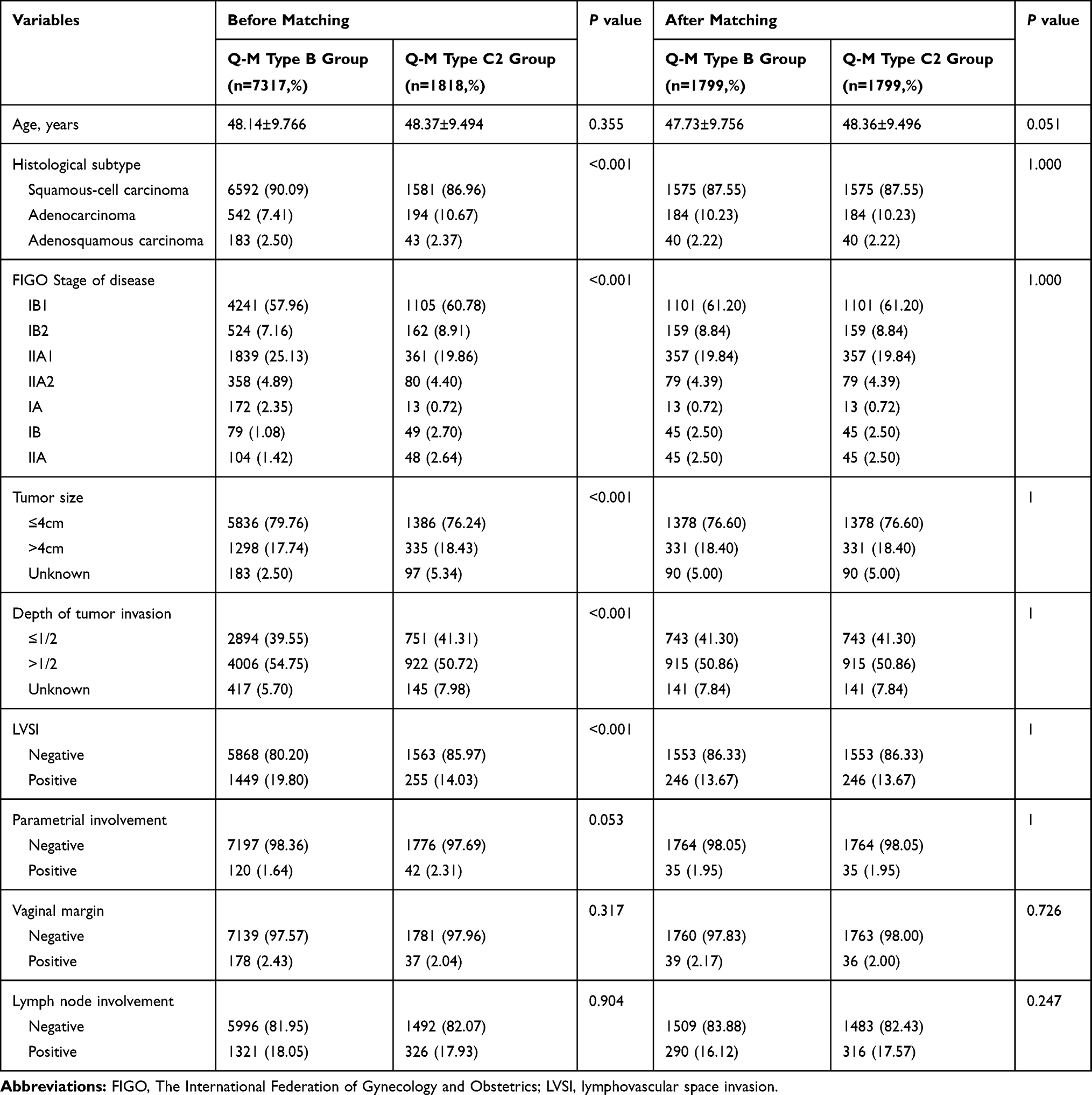 |
Table 1 Characteristics of Inclusive Early-Stage Cervical Cancer Patients, Before and After 1:1 Case-Control Matching |
 |
Figure 3 Kaplan-Meier estimates of OS and DFS based on inclusion criteria in the RWS and matched cohort study. (A, B) The 5-year OS and DFS of the Q-M type C2 group were shorter than those of the type B group in the RWS (OS: 89.5 vs 92.0%, P=0.002; DFS: 84.3 vs 87.4%, P<0.001). (C) The 5-year OS of the Q-M type B group and the type C2 group were similar after matching (P=0.089). (D) The 5-year DFS of the Q-M type C2 group was shorter than that of the type B group after matching (84.6 vs 88.4%, P=0.003). Abbreviations: RH, radical hysterectomy OS, overall survival; DFS, disease-free survival; RWS, real-world study. |
Survival Analysis of the Subgroup in the Matched Cohort Study
A total 5137 of 9135 patients received standardized adjuvant therapy. The baseline analysis is shown in Table 2. In the matched cohort study, 978 cases from each group were selected. Patients who underwent type C2 RH had a shorter OS and DFS than those who underwent type B RH (OS: 90.3 vs 93.8%, P=0.020; HR, 1.523, 95% CI, 1.066 to 2.176, P=0.021; DFS: 85.2 vs 89.4%, P=0.009; HR, 1.438, 95% CI, 1.091 to 1.896, P=0.010) (Figure 4A and B).
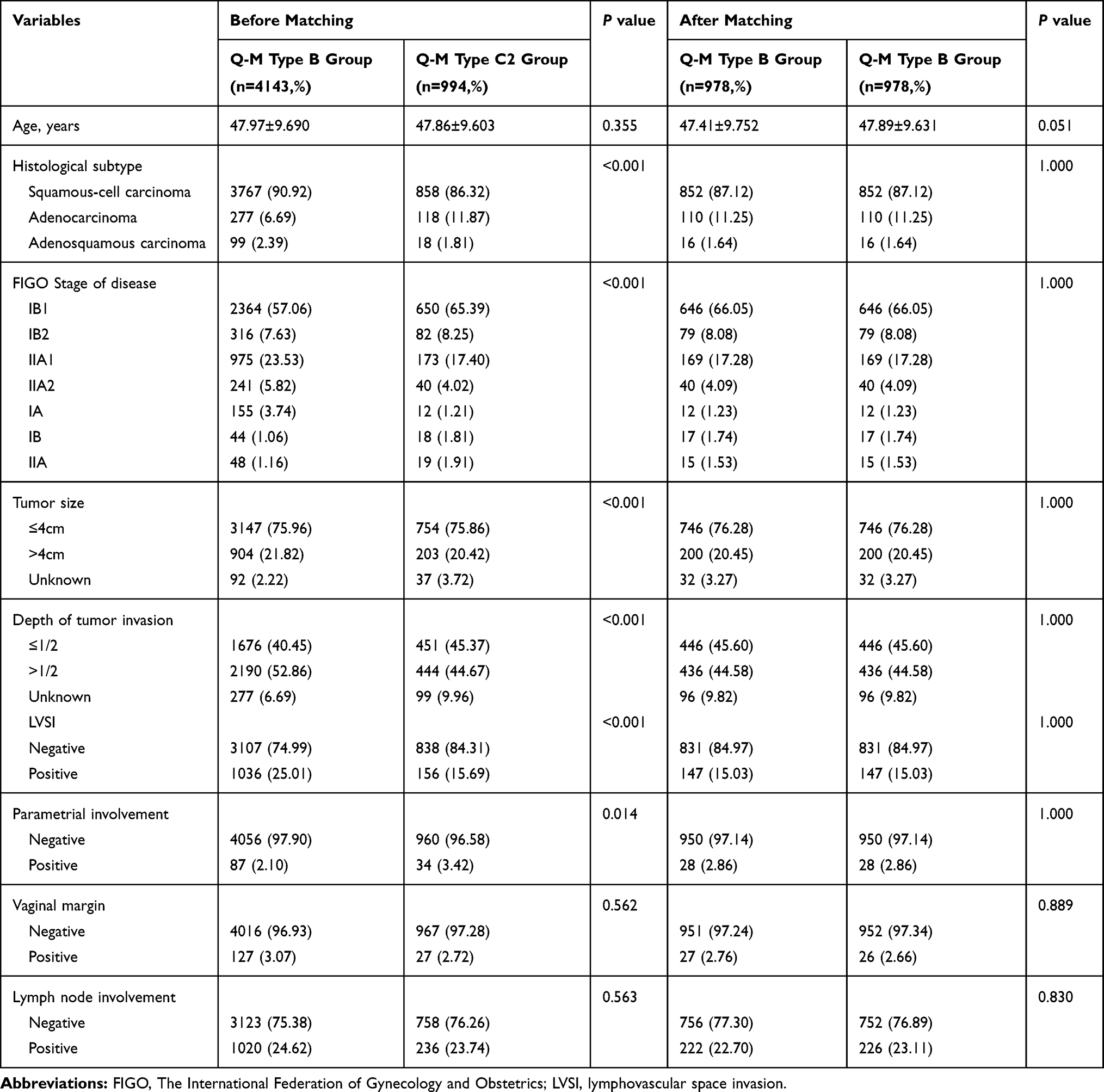 |
Table 2 Characteristics of Inclusive Early-Stage Cervical Cancer Patients Who Underwent Standard Adjuvant Therapy, Before and After 1:1 Case-Control Matching |
 |
Figure 4 Kaplan-Meier estimates of OS and DFS of the standard adjuvant therapy subgroup in the matched cohort study.(A, B) The 5-year OS and DFS of the Q-M type C2 group were shorter than those of the type B group in the RWS (OS: 90.3 vs 93.8%, P=0.020; DFS: 85.2 vs 89.4%, P=0.009). Abbreviations: OS, overall survival; DFS, disease-free survival; RWS, real-world study. |
Discussion
In this multicenter, retrospective, cohort study, patients who underwent Q-M type B RH for early-stage cervical cancer (FIGO IA1 (lymphovascular invasion)-IIA2) had a longer DFS than patients who underwent type C2 RH. In the initial RWS, we selected all the cases of abdominal type B or C2 RH in the database to provide unique insights into treatments and outcomes in routine oncology practice. Type B RH was found to be associated with a lower risk of recurrence/death than type C2 RH in the RWS. To rule out the confounding effects of specific histological subtypes, late stage disease and unknown lymph node resection types, we further refined our inclusion criteria. We found that patients who underwent type B RH had a lower risk of recurrence/death than those who underwent type C2 RH after matching. Considering that some patients may not take adjuvant therapy due to poor compliance or limited objective factors such as medical insurance, physical condition or hospital conditions, we selected patients who received standard postoperative adjuvant therapy in the subgroup analysis. Similar results were revealed that patients who underwent type B RH had higher OS and DFS 5-years after surgery. Through this study, we conclude that Q-M type B RH may be used for the treatment of early-stage cervical cancer.
Over the past 20 years, research on less radical surgery for the treatment of cervical cancer has been conducted. Surgeries with a smaller scope, including cone biopsy, simple hysterectomy, radical trachelectomy and modified RH (mRH), were mainly explored for some low-risk, early-stage cervical cancer patients. van Gent et al reported similar survival outcomes between nerve-sparing RH and conventional RH.22 Q-M type C1 RH is a highly precise surgery that lack popularity in China. Additionally, full evaluation data related to postoperative bladder, anorectal, and sexual dysfunction is not available in the Four C database. Accordingly, we included only Q-M type B and type C2 RH cases in the present study and could not discuss the efficacy of other less radical surgical types. A previous study showed that radical/subradical trachelectomy is a safe and effective fertility-sparing approach for young women with early cervical cancer.23 Post-surgery pregnancy rates could be as high as 78.26% (54/69) and all patients had good pregnancy outcomes. In this study, approximately 13.25% (11/83) of patients received subradical trachelectomy. During this procedure, the ureteral tunnel is not involved and the cardinal and uterosacral ligaments are severed beside the cervix. Our study result that less radical surgery might be better could also provide data supporting less radical fertility-sparing surgery. However, further detailed investigation is needed. Furthermore, several researches has pointed out the possibility of specific biomarkers for early-diagnosis, which might provide evidence for early diagnosis and intervention of early stage cervical cancer to get a better prognosis.24–26 Currently, there is growing interest to use real-world data to address clinical- and policy-relevant questions that cannot be answered with data from clinical trials. Therefore, we utilized a real-world analysis to determine the different survival outcomes between Q-M type B and type C2 RH. In this article, all the data were population-level data obtained from 37 hospitals located in different regions of mainland China.
Photopulos et al compared Piver type II and type III hysterectomy in terms of recurrence, complications and surgical parameters.12 They found that type II hysterectomy was associated with lower morbidity, fewer complications, lower recurrence rate, shorter surgery time and shorter postoperative hospital stay. However, patients enrolled in this study who underwent type II hysterectomy had less than 3 mm invasion with positive LVSI, 3 mm or less invasion extending to the margin of the cone biopsy specimen, or adenocarcinoma of uncertain invasion, ie, very early stage cervical cancer. Patients who underwent type III hysterectomy were IB or IIA patients with tumor sizes <3.5–4 cm. Differences in disease stages were obvious. Additionally, pathologic risk factors were not included in the baseline analysis and the follow-up period was ambiguous. Similarly, Yang et al analyzed postoperative complications and surgery related parameters of mRH and RH conducted by the same group of surgeons, in which the mRH procedures were referred to the Mayo Clinic due to their surgical expertise.13,14 mRH was feasible for the treatment of exophytic squamous cell cervical carcinoma patients with tumor sizes <2 cm and a depth of invasion <10 mm, diagnosed by conization. Nevertheless, the author did not systematically compare survival outcomes. A Chinese cohort study comprised of 480 stage IB cervical cancer patients who underwent Piver type II or III hysterectomy (240 patients in each group) and either did or did not undergo radiotherapy based on pathology results found no difference in OS or DFS (OS: 100 vs 100%, DFS: 98.33 vs 97.92%), or in the recurrence rate (2.92 vs 2.50%) between the two groups.15 The cervical cancer patients included in this study had squamous cell carcinoma with tumor sizes <2 cm and high-to-moderate differentiation. Further data on whether mRH is suitable for patients with adenocarcinoma or other histology types and cancers with tumor sizes >2 cm is required. Bezerra et al also found that the survival outcomes of patients with I-IIA cervical squamous cell carcinoma or adenocarcinoma in the type II group were similar to those in the type III group.16 However, 9 patients with stage IB2 or IIA included in this study received adjuvant therapy before surgery and the baseline characteristics were not compared. Therefore, whether preoperative adjuvant therapy can affect survival outcomes through currently unclear influences on pathological factors and adjuvant therapy decisions remains inconclusive. Therefore, in our study, patients who received neoadjuvant treatment were excluded. Ditto et al retrospectively analyzed the survival outcomes of patients who underwent Piver type II and type III hysterectomy for IA2, IB1 and IIA1 cervical cancer.17 The results showed that the type II group had a better OS at 5 years after surgery (95.2 vs 86.8%), but similar DFS (91.2 vs 82.9%). Type II hysterectomy is associated with a lower risk of death and recurrence. This finding is quite different from our results, as the difference we found was mainly in DFS. In addition, the patients included in Ditto’s study were non-synchronous, and 28.4% of the patients in the type II group underwent hysterectomy laparoscopically, which may have caused some bias. Several recent contemporary reports have questioned the presumed therapeutic equivalency of abdominal vs minimally invasive approaches.27–29 These reports demonstrated that minimally invasive RH was associated with lower rates of DFS and OS than open abdominal RH. Thus, we included only patients who underwent abdominal surgery in the present study.
Similar results have been reported in previous prospective or randomized controlled trials in which Piver type II hysterectomy showed survival outcomes comparable to those of type III hysterectomy. Prospective randomized trials published by Landoni et al found no differences in the 5-year OS and DFS between type II and type III hysterectomy for IB-IIA cervical cancer patients, while the morbidity from complication in type II surgery was significantly lower, especially urinary damage (13 vs 28%).30 This finding is consistent with previous findings. Panici et al evaluated the oncological outcomes of different surgeries for IA2-IB1 stage cervical cancer patients.31 Surgical decisions were made based on pelvic lymph node status by intraoperative frozen biopsy. Patients with negative lymph nodes diagnosed by frozen biopsy were treated with mRH, while patients with positive lymph nodes underwent RH. In terms of the oncological outcomes, the 5-year OS of 63 patients who underwent mRH surgery vs 20 patients in the RH group was 95 vs 74%, respectively. Panici et al concluded that pretreatment evaluation was feasible to determine if a less radical surgery was applicable. However, pelvic lymph node metastasis has proven to be an important prognostic factor, and this study therefore failed to avoid selection bias. Survival analysis based on these data did not fully reflect the efficacy of different surgeries, but it did indicate the importance of the preoperative imaging assessment of lymph node status in less radical surgical decisions. The midterm results of a randomized controlled trial from China showed no difference in the 2-year DFS between Piver type II and type III groups (100 vs 97.9%).32 Type II hysterectomy could effectively reduce the operation time (163 ± 18.8 min vs 226 ± 16.4 min), intraoperative blood loss (174 ± 27.7 vs 268 ± 37.4 mL) and postoperative urinary retention (5/46 vs 11/47). The postoperative symptom experience scores and postoperative bladder, vaginal or sexual functioning scores of the type II group were significantly lower than those of the type III group. Both groups showed good survival outcomes within 2 years after surgery, but a long-term evaluation is still required. However, this study mainly included laparoscopic surgery and did not consider the effect of postoperative adjuvant therapy. Furthermore, the follow-up was only within 2 years and long-term oncology outcomes still require supportive data. Our research was based on a real-world study. Strict inclusion criteria were defined, and further subgroup analyses were conducted to balance any confounding factors that may have an additional impact on the prognosis; thus, we conducted a substantive analysis of the survival outcome discrepancies between Q-M type B and type C2 RH for the treatment of early-stage cervical cancer.
This study has some limitations. First, in this retrospective study, there is some variability in the definition of the specific surgery type. It remains undeniable that there are differences in the experience of the surgeons, which can affect specific intraoperative decisions. Moreover, the time span of this study is up to 12 years and it is important to consider the learning curve for the two surgical procedures. Second, although we applied 1:1 case-control matching in order to eliminate some known confounding factors, the wide range of cancer characteristics from IA1 to IIA2 and the retrospective nature of this study carries some unknown intervention biases that cannot be adjusted for. The interaction between surgery and adjuvant therapy and the possible reason for the lower survival of patients who underwent more radical surgery warrants further investigation. Additionally, a comparison of the complications and quality of life was absent from this study, but we conducted a detailed analysis of the oncological outcomes.
Conclusions
In conclusion, we found that Q-M type B RH was associated with higher 5-year DFS than Q-M type C2 RH among women with early-stage cervical cancer in a real-world study and in a 1:1 case-control matching comparison. In patients who received standard adjuvant therapy, Q-M type B RH was associated with a higher 5-year OS and DFS. Q-M type B RH could be used for the treatment of early-stage (IA1 (lymphovascular invasion)-IIA2) cervical cancer.
Ethics Approval
This study was approved by the Ethics Committee of Nanfang Hospital, Southern Medical University (ethics approval number NFEC-2017-135).
Acknowledgements
We thank Min Hao (The Second Hospital of ShanXi Medical University), Shan Kang (The Fourth Hospital of Hebei Medical University), Bin Ling (China-Japan Friendship Hospital), Lixin Sun and Hongwei Zhao (Shanxi Cancer Hospital), Jihong Liu and Lizhi Liang (Sun Yat-sen University Cancer Center), Lihong Lin and Yu Guo (Anyang Tumor Hospital), Li Wang (The Affiliated Tumor Hospital of Zhengzhou University), Weidong Zhao (Anhui Provincial Cancer Hospital), Yan Ni (The Yuncheng Central Hospital of Shanxi province), Wentong Liang and Donglin Li (Guizhou Provincial People’s Hospital), Jianxin Guo (Daping Hospital, The Third Military Medical University), Shaoguang Wang (The Affiliated Yantai Yuhuangding Hospital of Qingdao University), Xuemei Zhan and Mingwei Li (Jiangmen Central Hospital), Weifeng Zhang (Ningbo Women & Children’s Hospital), Peiyan Du (The Affiliated Cancer Hospital and Institute of Guangzhou Medical University), Ziyu Fang (Liuzhou Workers’ Hospital), Rui Yang (Shenzhen Hospital of Peking University), Long Chen (Qingdao Municipal Hospital), Encheng Dai and Ruilei Liu (Linyi People’s Hospital), Yuanli He and Mubiao Liu (Zhujiang Hospital, Southern Medical University), Jilong Yao and Zhihua Liu (Shenzhen Maternity & Child Health Hospital), Xueqin Wang (The Fifth Affiliated Hospital of Southern Medical University), Anwei Lu (Maternal and Child Health Hospital of Guiyang Province), Yan Xu (Guangzhou Pan Yu Central Hospital), Ben Ma (Guangzhou First People’s Hospital), Zhonghai Wang (Shenzhen Nanshan People’s Hospital), Lin Zhu (The Second Hospital of Shandong University), Hongxin Pan (The Third Affiliated Hospital of Shenzhen University), Qianyong Zhu (No.153. Center Hospital of Liberation Army/Hospital No.988 of the Chinese People’s Liberation Army Joint Support Force), Dingyuan Zeng and Zhong Lin (Maternal and Child Health Care Hospital of Liuzhou), Xiaohong Wang (Laiwu People’s Hospital/Jinan City People’s Hospital) and Bin Zhu (The Affiliated Yiwu Women and Children Hospital of Hangzhou Medical College) for their contribution to the data collection.
Disclosure
Dr Chunlin Chen reports grants from the National Science and Technology Program during the Twelfth Five-year Plan Period (2014BAI05B03), grants from the Natural Science Foundation of Guangdong Province (2015A030311024) and grants from the Guangzhou Municipal Science and Technology Project (158100075). The authors report no other conflicts of interest in this work.
References
1. Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. 2019;393(10167):169–182. doi:10.1016/S0140-6736(18)32470-X
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
4. Koh WJ, Abu-Rustum NR, Bean S, et al. Cervical cancer, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(1):64–84. doi:10.6004/jnccn.2019.0001
5. Querleu D, Morrow CP. Classification of radical hysterectomy. Lancet Oncol. 2008;9(3):297–303. doi:10.1016/S1470-2045(08)70074-3
6. Wit EM, Horenblas S. Urological complications after treatment of cervical cancer. Nat Rev Urol. 2014;11(2):110–117. doi:10.1038/nrurol.2013.323
7. Benedetti-Panici P, Zullo MA, Plotti F, Manci N, Muzii L, Angioli R. Long-term bladder function in patients with locally advanced cervical carcinoma treated with neoadjuvant chemotherapy and type 3–4 radical hysterectomy. Cancer. 2004;100(10):2110–2117. doi:10.1002/cncr.20235
8. Plotti F, Angioli R, Zullo MA, et al. Update on urodynamic bladder dysfunctions after radical hysterectomy for cervical cancer. Crit Rev Oncol Hematol. 2011;80(2):323–329. doi:10.1016/j.critrevonc.2010.12.004
9. Jensen PT, Groenvold M, Klee MC, Thranov I, Petersen MA, Machin D. Early-stage cervical carcinoma, radical hysterectomy, and sexual function. A longitudinal study. Cancer. 2004;100(1):97–106. doi:10.1002/cncr.11877
10. Wang X, Chen C, Liu P, et al. The morbidity of sexual dysfunction of 125 Chinese women following different types of radical hysterectomy for gynaecological malignancies. Arch Gynecol Obstet. 2018;297(2):459–466. doi:10.1007/s00404-017-4625-0
11. Sood AK, Nygaard I, Shahin MS, Sorosky JI, Lutgendorf SK, Rao SS. Anorectal dysfunction after surgical treatment for cervical cancer. J Am Coll Surg. 2002;195(4):513–519. doi:10.1016/S1072-7515(02)01311-X
12. Photopulos GJ, Zwaag RV. Class II radical hysterectomy shows less morbidity and good treatment efficacy compared to class III. Gynecol Oncol. 1991;40(1):21–24. doi:10.1016/0090-8258(91)90078-J
13. Yang YC, Chang CL. Modified radical hysterectomy for early Ib cervical cancer. Gynecol Oncol. 1999;74(2):241–244. doi:10.1006/gyno.1999.5434
14. Magrina JF, Goodrich MA, Weaver AL, Podratz KC. Modified radical hysterectomy: morbidity and mortality. Gynecol Oncol. 1995;59(2):277–282. doi:10.1006/gyno.1995.0022
15. Cai HB, Chen HZ, Zhou YF, Lie DM, Hou HY. Class II radical hysterectomy in low-risk IB squamous cell carcinoma of cervix. Int J Gynecol Cancer. 2009;19(1):46–49. doi:10.1111/IGC.0b013e318197f847
16. Bezerra AL, Martins MR, Bezerra SM, Figueiroa JN, Batista TP. Class II radical hysterectomy for stage I–IIA cervix cancer: prognostic factors associated to recurrence and survival in a northeast Brazil experience. J Surg Oncol. 2011;104(3):255–259. doi:10.1002/jso.21939
17. Ditto A, Martinelli F, Ramondino S, et al. Class II versus Class III radical hysterectomy in early cervical cancer: an observational study in a tertiary center. Eur J Surg Oncol. 2014;40(7):883–890. doi:10.1016/j.ejso.2014.02.229
18. Zhang W, Chen C, Liu P, et al. Impact of pelvic MRI in routine clinical practice on staging of IB1-IIA2 cervical cancer. Cancer Manag Res. 2019;11:3603–3609. doi:10.2147/CMAR.S197496
19. Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105(2):103–104. doi:10.1016/j.ijgo.2009.02.012
20. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynecol Obstet. 2018;143(Suppl 2):22–36. doi:10.1002/ijgo.12611
21. Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for women with cervical cancer. Obstet Gynecol. 1974;44:265–272.
22. van Gent MDJM, Rademaker M, van der Veer JCB, et al. Long-term oncological outcome after conventional radical hysterectomy versus 2 nerve-sparing modalities for early stage cervical cancer. Int J Gynecol Cancer. 2017;27(8):1729–1736. doi:10.1097/IGC.0000000000001067
23. Wang A, Cui G, Jin C, et al. Multicenter research on tumor and pregnancy outcomes in patients with early-stage cervical cancer after fertility-sparing surgery. J Int Med Res. 2019;47(7):2881–2889. doi:10.1177/0300060519845974
24. Valenti G, Vitale SG, Tropea A, Biondi A, Laganà AS. Tumor markers of uterine cervical cancer: a new scenario to guide surgical practice? Updates Surg. 2017;69(4):441–449. doi:10.1007/s13304-017-0491-3
25. Nicol AF, de Andrade CV, Gomes SC
26. Vitale SG, Valenti G, Rapisarda AMC, et al. P16INK4a as a progression/regression tumour marker in LSIL cervix lesions: our clinical experience. Eur J Gynaecol Oncol. 2016;37(5):685–688.
27. Ramirez PT, Frumovitz M, Pareja R, et al. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N Engl J Med. 2018;379(20):1895–1904. doi:10.1056/NEJMoa1806395
28. Melamed A, Margul DJ, Chen L, et al. Survival after minimally invasive radical hysterectomy for early-stage cervical cancer. N Engl J Med. 2018;379(20):1905–1914. doi:10.1056/NEJMoa1804923
29. Kim SI, Cho JH, Seol A, et al. Comparison of survival outcomes between minimally invasive surgery and conventional open surgery for radical hysterectomy as primary treatment in patients with stage IB1-IIA2 cervical cancer. Gynecol Oncol. 2019;153(1):3–12. doi:10.1016/j.ygyno.2019.01.008
30. Landoni F, Maneo A, Cormio G, et al. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: a prospective randomized study. Gynecol Oncol. 2001;80(1):3–12. doi:10.1006/gyno.2000.6010
31. Panici PB, Angioli R, Palaia I, et al. Tailoring the parametrectomy in stages IA2-IB1 cervical carcinoma: is it feasible and safe? Gynecol Oncol. 2005;96(3):792–798. doi:10.1016/j.ygyno.2004.11.018
32. Sun H, Cao D, Shen K, et al. Piver Type II vs. Type III hysterectomy in the treatment of early-stage cervical cancer: midterm follow-up results of a randomized controlled trial. Front Oncol. 2018;8:568. doi:10.3389/fonc.2018.00568
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.