")
Back to Journals » International Medical Case Reports Journal » Volume 16
Surgical Treatment of Extracranial Internal Carotid Artery Pseudoaneurysm in an Infant Due to Falling from Height: An Unusual Case
Authors Ucaroglu ER, Tahtabasi M
Received 4 August 2023
Accepted for publication 4 October 2023
Published 10 October 2023 Volume 2023:16 Pages 667—672
DOI https://doi.org/10.2147/IMCRJ.S433360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Erhan Renan Ucaroglu,1 Mehmet Tahtabasi2
1Department of Cardiovascular Surgery, University of Health Sciences- Somalia Turkey Recep Tayyip Erdogan Education and Research Hospital, Mogadishu, Somalia; 2Department of Radiology, University of Health Sciences- Somalia Turkey Recep Tayyip Erdogan Education and Research Hospital, Mogadishu, Somalia
Correspondence: Mehmet Tahtabasi, Somalia Turkey Recep Tayyip Erdogan Education and Research Hospital, Mogadishu, Somalia, Tel +905076159932, Email [email protected]
Abstract: Pseudoaneurysms of the internal carotid artery (ICA) caused by non-penetrating trauma are extremely rare. Patients with ICA pseudoaneurysms may present with cerebral ischemia, cervical masses, neck swelling, hematoma, rupture, pain, or cranial nerve dysfunction. We present a case of a left ICA pseudoaneurysm that developed in a 7-month-old infant because of a fall from height. The patient developed left-sided neck swelling that caused severe airway obstruction and respiratory arrest. The patient was urgently intubated and underwent emergency surgery under general anesthesia to repair the defect in the left ICA. Primary repair was performed to treat the pseudoaneurysms. The pseudoaneurysm sac was not removed because it was complicated and had extended into the respiratory tract. The patient was extubated on the 2nd day and discharged on the 7th day without complications. Follow-up of the patient after two weeks was unremarkable. Extracranial ICA pseudoaneurysms should be identified in patients presenting with blunt trauma. Emergency surgery should be considered for patients with progressive pseudoaneurysms.
Keywords: carotid artery, pseudoaneurysm, trauma, extracranial internal carotid artery pseudoaneurysm, infancy
Background
Extracranial internal carotid artery (ICA) pseudoaneurysms are uncommon lesions that may occur as sequelae of blunt trauma, cancer/radiation necrosis, or mycotic infection.1 The most common location of extracranial ICA pseudoaneurysms is the common carotid artery near bifurcation, followed by ICA.2 Patients with ICA pseudoaneurysms may present with cerebral ischemia, cervical masses, neck swelling, hematoma, rupture, pain, and cranial nerve dysfunction.3 Historically, treatment of pseudoaneurysms has been primarily surgical. However, surgery of pseudoaneurysms located near the skull base is technically challenging and has been associated with high morbidity/mortality rates. More recently, endovascular techniques have become more appealing as multiple studies have provided encouraging results.4,5 In geographical areas where endovascular treatment is not possible, surgical treatment is lifesaving for these patients. Although surgical treatment of ICA aneurysms is challenging because of anatomical complexity, the rate of early mortality and stroke has been reported to be low with surgical treatment, supporting the superiority of invasive intervention.6 Herein, we present a case of left internal carotid artery pseudoaneurysm that developed in a 7-month-old infant due to a fall from height.
Case Presentation
A 7-month-old female infant was brought to the emergency department of our hospital with left-sided neck swelling that caused severe airway obstruction. Her medical history revealed that she fell from a high place about two weeks ago and subsequently developed a slowly growing swelling on the left side of his neck. On physical examination, a pulsatile, palpable mass lesion was detected in the left cervical region. Bedside ultrasonography (US) revealed a saccular aneurysm sac originating from the left ICA. Color Doppler US showed a yin-yang pattern within the aneurysm and jet flow from the ICA to the aneurysm sac (a sign of pseudoaneurysm) (Figure 1). The patient was urgently intubated because of increased respiratory distress and worsening general condition. Computed tomography (CT) was performed after respiratory and hemodynamic stabilization was achieved. CT angiography (CTA) revealed an aneurysmatic filling originating from the left cervical ICA, displacing the artery posteriorly (Figure 2). In addition, CTA revealed narrowing of the lumen and reduced flow in the ICA, distal to the aneurysm (Figure 3). The patient was then transferred to emergency surgery to repair a defect in the left internal carotid artery. Under general anesthesia, an incision was made anterior to the sternocleidomastoid muscle between the mastoid bone and suprasternal notch. The cutaneous, subcutaneous, and platysma layers were passed through, and the carotid artery was accessed. The common carotid artery, ICA, and external carotid artery were wrapped with tape, and the ICA was then dissected from the surrounding tissues towards the distal end and released. When the mastoid bone was approached, the aneurysm sac opened approximately 2 cm below the skull base and began to bleed. Systemic heparinization was performed and vascular clamps were inserted. The defect was small enough to perform primary repair. The defect was closed primarily by using 7/0 Prolene sutures. The aneurysm sac was not removed because it was complicated and had extended into the respiratory tract. After bleeding was controlled, the layers were appropriately closed (Figure 4).
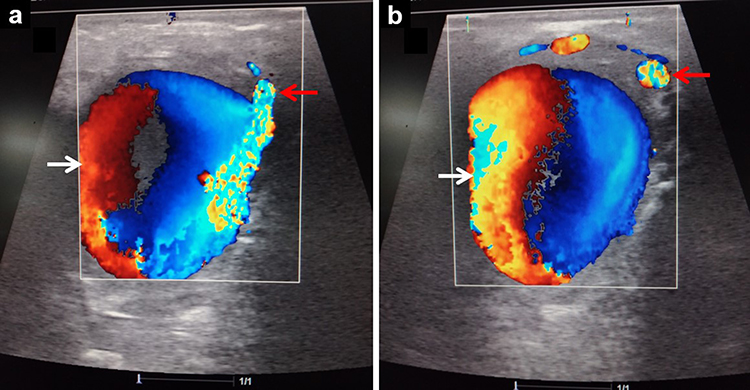 |
Figure 1 Color Doppler ultrasound images (a and b) showing the pseudoaneurysm fed by the internal carotid artery (red arrow) and a yin-yang pattern (white arrow). |
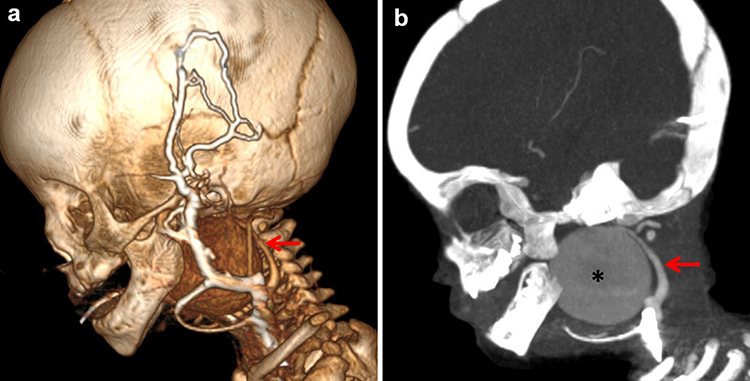 |
Figure 2 Sagittal volume-rendered three-dimensional (a) and maximum intensity projection (b) images demonstrating an aneurysm (asterisk) originating from the internal carotid artery (red arrow). |
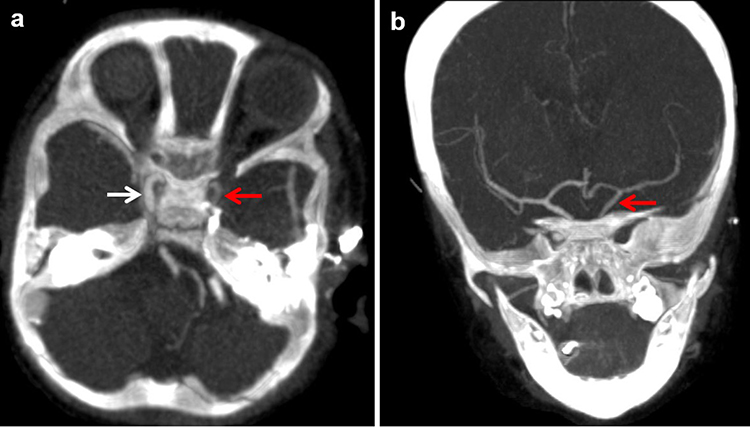 |
Figure 3 Axial (a) and coronal (b) maximum intensity projection images showing poor contrast material filling of the ipsilateral internal carotid artery (red arrow) relative to the contralateral side (white arrow). |
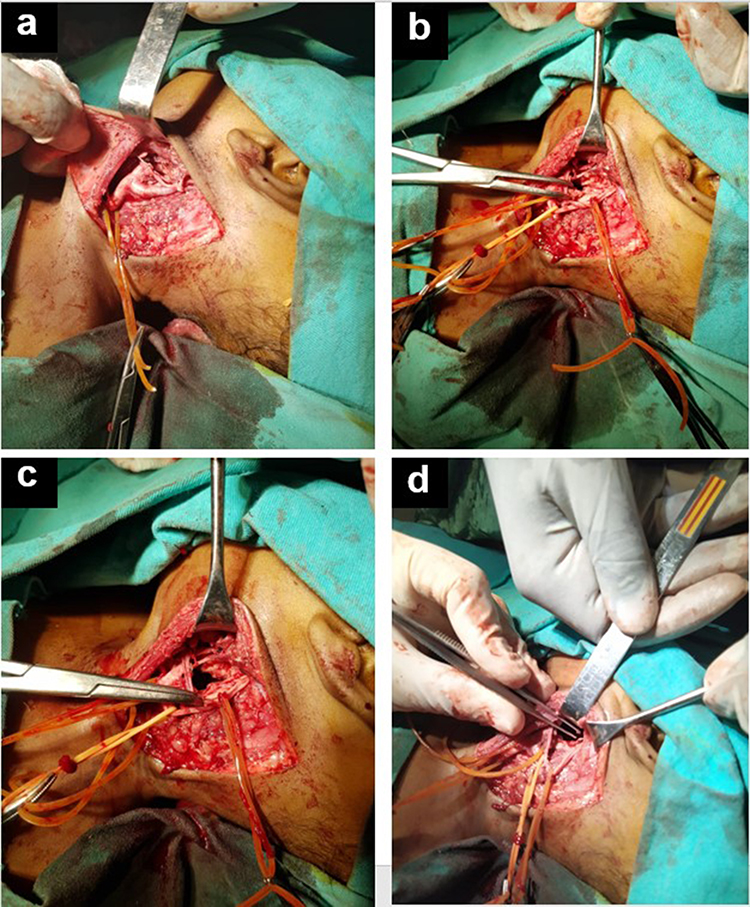 |
Figure 4 Intraoperative images showing dissection of the anatomical layers (a), freeing of the carotid arteries (b), and opening of the aneurysm sac (c and d). |
The patient was admitted to the neonatal intensive care unit. She was extubated on the 2nd day and transferred to the outpatient clinic. The patient was discharged on the 7th day without any postoperative complications. Follow-up of the patient after two weeks was unremarkable.
Discussion
Extracranial carotid artery pseudoaneurysms and aneurysms are extremely rare, altogether accounting for only 0.4–4% of all peripheral artery aneurysms.7 Pseudoaneurysms of the ICA are rare lesions that may occur as a component of deep cervical abscesses, blunt trauma, cancer/radiation necrosis, collagen vascular disease, fibromuscular dysplasia, or as a sequela of mycotic infection.5 The extracranial ICA is at a high risk of injury because it is mobile and vulnerable to stretching.8 Extracranial traumatic vascular injury is seen in approximately 1% to 2% of patients after blunt trauma, and the incidence of ICA pseudoaneurysm following blunt trauma is only 0.08–0.33%.9 The most common cause of injury is blunt trauma from motor vehicle crashes.10 In our case, the extracranial ICA pseudoaneurysm was caused by a fall from height. In the literature search, we could not find any case reports describing an extracranial ICA pseudoaneurysm in an infant. Blunt trauma to the extracranial ICA begins with intimal damage that progresses to dissection, and is likely to lead to a pseudoaneurysm. Pseudoaneurysms are defined as those with > 50% dilatation of the ICA diameter that can grow.11 Our patient developed an extracranial ICA aneurysm following a fall from a progressively enlarged height. Due to this progression, the aneurysm extended and obstructed the airway, resulting in respiratory arrest.
ICA pseudoaneurysms can be diagnosed using color Doppler US, CTA, or magnetic resonance angiography. Currently, the Eastern Association for the Surgery of Trauma’s Blunt Cerebrovascular Injury Practice Management Guidelines recommend CTA as the first-line method for screening for extracranial ICA pseudoaneurysm.12 CTA provides extravascular details that can be used to plan the surgical approach. In our case, we performed CT angiography using the reconstructed 3D images. In addition, the adequacy of the cerebral circulation should be investigated. We used digital compression of the internal carotid artery with neurological monitoring to evaluate cerebral circulation in the patient.
Carotid injuries are difficult to assess and treat because of their complex anatomy, which is confined to a narrow space. Classical surgical repair of ICA aneurysms involves open resection of the entire aneurysm with or without graft.13 Other surgical approaches include resection with direct anastomosis, partial resection with reconstruction, ligation, or bypass. Endovascular approaches are increasingly used more frequently in carotid injuries. Stenting has most commonly been used for high extracranial internal carotid lesions as pseudoaneurysms.14 Compared with surgical treatment of carotid injuries, with an associated mortality rate of up to 22%, carotid stenting appears to be much lower at 0.9%.5,7,14 In a case report by Rojas et al, a 44-year-old woman fell from a height and developed a CCA pseudoaneurysm of the common carotid artery. The patient was treated using endovascular stenting.7 In a study examining pseudoaneurysm in the pediatric population, 6 patients aged 2.5–15 years were presented.15 Two of the children were managed by trapping of the aneurysm and 2 only by proximal parent vessel occlusion. The other 2 children were treated with stent graft deployment across the aneurysm neck to reconstruct the parent vessel. All the patients were doing well during the follow-up period (mean, 14.8 months). This study reveals that the basic treatment is parent occlusion and that endovascular treatment can be performed in selected patients.15 Since our patient was a baby and there was no endovascular method in Somalia, surgery was planned as the first option. In addition, the long-term results of endovascular stenting in infants are not clearly known. Our patient underwent emergency surgery for a pseudoaneurysm extending to the airway. The pseudoaneurysm sac was not removed because it was sufficiently small for the primary repair. The patient did not develop any postoperative complications and was discharged on the 7th day without problem.
Conclusion
Extracranial ICA pseudoaneurysms should be identified in patients presenting with blunt trauma. Emergency surgery should be considered in patients with progressive pseudoaneurysms. There is no doubt about it, it is respiratory failure due to airway compression. Complex anatomical localization of the external ICA makes surgery difficult. If the pseudoaneurysm sac is sufficiently small to enable primary repair, it cannot be removed.
Abbreviations
ICA, Internal carotid artery; US, Ultrasound; CT, Computed tomography; CTA, Computed tomography angiography.
Data Sharing Statement
All data relevant to this study have been included in this published article. Further datasets analyzed in the current study are available from the corresponding author upon reasonable request.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent form is available for review by the editor of the journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that they received no funding for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Maras D, Lioupis C, Magoufis G, Tsamopoulos N, Moulakakis K, Andrikopoulos V. Covered stent-graft treatment of traumatic internal carotid artery pseudoaneurysms: a review. Cardiovasc Intervent Radiol. 2006;29(6):958–968. doi:10.1007/s00270-005-0367-7
2. Liapis C, Gugulakis A, Misiakos E, Verikokos C, Dousaitou B, Sechas M. Surgical treatment of extracranial carotid aneurysms. Int Angiol. 1994;13(4):290–295.
3. Radak Đ, Davidović L, Vukobratov V, et al. Carotid artery aneurysms: Serbian multicentric study. Ann Vasc Surg. 2007;21(1):23–29. doi:10.1016/j.avsg.2006.10.004
4. Kaya V, Tahtabasi M, Yıldırım İO. Risk factors for the rupture of anterior communicating artery aneurysms: coexistence of fetal-type posterior cerebral artery and A1 segment hypoplasia/agenesis. J Clin Neurosci. 2023;110:74–79. doi:10.1016/j.jocn.2023.02.008
5. Yi AC, Palmer E, Luh G, Jacobson JP, Smith DC. Endovascular treatment of carotid and vertebral pseudoaneurysms with covered stents. Am J Neuroradiol. 2008;29(5):983–987. doi:10.3174/ajnr.A0946
6. Li Z, Chang G, Yao C, et al. Endovascular stenting of extracranial carotid artery aneurysm: a systematic review. Eur J Vasc Endovasc Surg. 2011;42(4):419–426. doi:10.1016/j.ejvs.2011.05.008
7. Rojas D, Stefanov S, Riera Del Moral L, Álvarez J, Riera de Cubas L. Endovascular treatment of posttraumatic pseudoaneurysm of the common carotid artery. Case Rep Vasc Med. 2015;2015:1–4. doi:10.1155/2015/427040
8. Foreman PM, Harrigan MR. Blunt traumatic extracranial cerebrovascular injury and ischemic stroke. Cerebrovasc Dis Extra. 2017;7(1):72–83. doi:10.1159/000455391
9. Harrigan MR. Ischemic Stroke due to Blunt Traumatic Cerebrovascular Injury. Stroke. 2020;51(1):353–360. doi:10.1161/STROKEAHA.119.026810
10. Esnault P, Cardinale M, Boret H, et al. Blunt cerebrovascular injuries in severe traumatic brain injury: incidence, risk factors, and evolution. J Neurosurg. 2017;127(1):16–22. doi:10.3171/2016.4.JNS152600
11. Biasi L, Azzarone M, De Troia A, Salcuni P, Tecchio T. Extracranial Internal Carotid Artery Aneurysms: case report of a saccular wide-necked aneurysm and review of the literature. Acta bio-medica. 2018;79(3):217–222.
12. Bromberg WJ, Collier BC, Diebel LN, et al. Blunt cerebrovascular injury practice management guidelines: the eastern association for the surgery of trauma. J Trauma Inj Infect Crit Care. 2010;68(2):471–477. doi:10.1097/TA.0b013e3181cb43da
13. Welleweerd JC, Moll FL, de Borst GJ. Technical options for the treatment of extracranial carotid aneurysms. Expert Rev Cardiovasc Ther. 2012;10(7):925–931. doi:10.1586/erc.12.61
14. Berne JD, Reuland KR, Villarreal DH, McGovern TM, Rowe SA, Norwood SH. Internal carotid artery stenting for blunt carotid artery injuries with an associated pseudoaneurysm. J Trauma Inj Infect Crit Care. 2008;64(2):398–405. doi:10.1097/TA.0b013e31815eb788
15. Balasundaram P, Sebastian LJD, Jain N, Prabhakar A, Garg A, Gaikwad S. Management of arterial pseudoaneurysms of the neck in a pediatric population: an endovascular case series and review of literature. World Neurosurg. 2019;125:e273–e281. doi:10.1016/j.wneu.2019.01.061
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.