Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Surgical Treatment of Clavicular Fractures, Refractures, Delayed and Non-Unions Using a Resorbable, Gentamicin-Eluting Calcium Sulphate/Hydroxyapatite Biocomposite
Authors Peters J ![]() , Singh G, Hakobyan H
, Singh G, Hakobyan H
Received 9 February 2022
Accepted for publication 26 April 2022
Published 9 May 2022 Volume 2022:18 Pages 551—560
DOI https://doi.org/10.2147/TCRM.S361006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Jens Peters, Gurdeep Singh, Hrayr Hakobyan
Department of Trauma Surgery and Orthopaedics, Clinic Sulingen, Sulingen, Lower Saxony, 27232, Germany
Correspondence: Jens Peters, Department of Trauma Surgery and Orthopaedics, Clinic Sulingen, Schmelingstrasse 47, Sulingen, Lower Saxony, 27232, Germany, Tel +49 4271 82 33210, Fax +49 4271 82 33212, Email [email protected]
Objective: This study describes clinical and radiological outcomes following treatment of displaced primary fractures, refractures, delayed unions and non-unions of the clavicle with open reduction and internal fixation (ORIF) with a plate plus filling of the residual bone defect and/or implant augmentation with a gentamicin-loaded bone graft substitute (CERAMENT G, BONESUPPORT).
Patients and Methods: Patients who underwent surgical treatment either for displaced clavicle fractures, refractures, delayed unions or non-unions between June 2018 and May 2021 were enrolled in this retrospective study. Bony consolidation, complication rate, and functional outcomes, including overall health, were assessed.
Results: A total of 26 clavicles in 25 patients with a mean age of 50.7 (16– 85) years, 16 male and 9 female, were enrolled in the study. The mean follow-up was 14.9 (6– 31) months. There were 18 cases of displaced clavicle fractures, four refractures, two delayed unions and two non-unions. The majority of the clavicle lesions were located at the middle third (17/26, 65.4%), seven at the lateral third (26.9%) and two at the medial third (7.7%) of the clavicle. A mean Goldberg score of 7 indicated complete bony union and remodeling of the bone graft substitute in all cases. No complications occurred. The mean University of California at Los Angeles Shoulder Score and the mean Quick Disability of the Arm, Shoulder and Hand Score were 34.6± 0.8 (32– 35) points and 0.6± 1.6 (0– 5.4) points, respectively, and revealed excellent functional results. The mean 12-item Short-Form Survey physical component questionnaire was 57.7± 1.7 (54.1– 58.9) points, and no patient experienced any pain at the last follow-up.
Conclusion: Our initial experience suggests that ORIF using a plate plus bone defect filling and/or implant augmentation with a gentamicin-eluting bone graft substitute may be useful not only for complication management after clavicle fractures but also in the initial treatment of challenging clavicular fractures.
Keywords: clavicle, trauma, non-union, defect augmentation, bone graft substitute
Introduction
The clavicle is the only bony connection between the trunk and the upper extremity.1 Between 2% and 5% of the fractures in adults affect the S-shaped curved bone, which is manifested by incidences between 29 and 64 per 100.000 people per year.2–4 The first widely accepted anatomic classification system by Allman divides the clavicle into a middle, lateral and medial third. Fractures distal to the coracoclavicular (CC) ligament are attributed to the lateral third (type 2), fractures of the proximal end to the medial third (type 3) and fractures that occur in the area between to the middle third (type 1).5 There are more detailed sub-divisions for the various fracture types, eg, by Neer for types 2 and 3 and Jäger&Breitner for type 2 fractures.6,7
About 70% to 80% of the fractures occur in the region of the middle diaphyseal third, of which 19% are comminuted fractures.8,9 Open fractures are rare at the middle third.9 About one out of four of the clavicle fractures occurs at the distal end, whilst medial fractures account for only a low single-digit percentage (2–5%) of all clavicle fractures.3,8–10 Minor or non-displaced fractures, which occur mainly at the medial or distal end of the clavicle, are often treated non-operatively with good functional results.3,9 Displaced fractures, on the other hand, occur more frequently at the clavicle shaft and are more often treated surgically.3,8,9 Widely accepted indications for surgical treatment of clavicle fractures are significant fracture displacement or neurovascular compromise; and for lateral and medial fractures instability of bone fragments, for example, due to impairment of the CC or acromioclavicular (AC) ligaments.3 The surgical procedure for clavicle fractures includes plate fixation after open reduction, but also intramedullary pins, wires or nails, which allow a minimal-invasive approach. However, the optimal procedure remains controversial.11
Complications, mainly non-unions or malunions, occur both after surgical and conservative management of clavicle fractures.12 Surgical intervention on the clavicle shaft used to be associated with complications, particularly high rates of non-union have been described, but more recent literature also refers to certain risk factors predicting non-unions after non-operative treatment.12 The degree of fracture displacement is the single most important risk factor for the development of a non-union after conservative treatment, further risk factors include shaft shortening of more than 2cm.12 Following open reduction and internal fixation (ORIF) of the clavicle midshaft, both non-union rates and deep infection rates are reported with 2.6%, whereas the overall non-union rate following non-operative treatment is 5.9%, and up to 15.1% in case of completely displaced fractures.11,13 For conservatively managed unstable lateral clavicle fractures the risk of non-union is particularly high with 33.3%, compared to 1.6% following surgical treatment.14 Other complications such as infection occur significantly more often after surgical treatment.14 Conservative treatment is also very common at the medial third of the clavicle, associated with non-union rates between 4% and 8%.3 Due to the very small incidence of medial clavicle fractures, there are only limited and very small case series for surgical procedures.3,15
Refractures after non-surgical treatment are mostly associated with secondary trauma or premature return to contact sports and are at high risk to develop non-union.12 They can also occur after (early) implant removal; but are uncommon if implants are removed later than 12 months from bony consolidation.12 The treatment of delayed unions and non-unions can be complicated by infection, and by significant bone loss or bone defects following pseudarthrosis resection and debridement.16,17
Surgical treatment was performed in fractures with a displacement of more than 20mm, an initial shortening of more than 15mm, displaced unstable medial fractures with or without involvement of the sternoclavicular (SC) joint, displaced or unstable lateral fractures with or without involvement of the AC joint, fractures accompanied by injuries to the subclavian artery/vein, fractures with soft tissue compromise, and pathological fractures. We also addressed symptomatic delayed unions or non-unions with ORIF using locking plates and screws. Our novel approach using an antibiotic-eluting bone graft substitute in addition to a plate fixation in fractures, refractures, delayed and non-unions to fill the defects and/or augment the implants can contribute to the prevention of both non-unions and infections.
The aim of this retrospective study was to systematically evaluate the clinical and radiological outcomes following treatment of displaced primary clavicular fractures, refractures, delayed unions and non-unions with ORIF using a plate, and additional bone defect and/or implant augmentation with a gentamicin-eluting bone graft substitute.
Materials and Methods
Patients
Patients who were surgically treated at our level 2 trauma center according to a standardized protocol either for more than 20mm displaced primary fractures, refractures, delayed unions or non-unions of the clavicle between June 2018 and May 2021 were considered for this retrospective study. Patients younger than 18 years at the time of informed consent or with a minimum clinical follow-up shorter than 6 months at our clinic were excluded from the study. Delayed unions were defined as the radiological lack of bridging callus at the fracture site between three and six months from surgical or conservative treatment, and non-union as the lack of periosteal and endosteal ossification at the fracture site at least six months from surgery or conservative treatment.18
Surgical Techniques
Preoperatively, surgical landmarks were identified on radiographs. The clavicle was accessed via an approximately 7cm large intraclavicular incision and dissection of the skin-soft tissue envelope cranially for visualization of the fracture or delayed union/non-union.
Clavicle fractures were treated by ORIF, and filling of the residual bone defect and/or implant augmentation with a gentamicin-loaded bone graft substitute (CERAMENT G, BONESUPPORT AB, Lund, Sweden). CERAMENT G consists of 40 weight percent (wt%) hydroxyapatite and 60wt% calcium sulphate and is delivered pre-formulated with gentamicin sulphate so that 1mL of the injectable paste contains 17.5mg gentamicin sulphate. The hydroxyapatite is highly osteoconductive and promotes bone ingrowth as the material resorbs over time. The gentamicin component prevents the colonization by gentamicin-sensitive microorganisms, as it provides a very high local gentamicin concentration, which stays above the minimal inhibitory concentration (MIC) for most gentamicin-sensible microorganisms for at least 28 days.19,20
Following cleaning and irrigation of the fracture gap, fracture reduction was performed. Fracture reduction was maintained with appropriate fixation forceps. A locking clavicle plate (regularly Winsta-C, Axomed GmbH, Freiburg, Germany), in individual cases LCP superior or superior anterior clavicle plate (DePuy Synthes, West Chester, PA, USA) was fitted and fixed with a minimum of three bicortical screws, which were placed laterally and medially to the fracture. The bone defect, cannulated screws and implant bed were augmented with 5mL CERAMENT G (Figure 1). The gentamicin-loaded hydroxyapatite/calcium sulphate was injected about 5 minutes after the start of mixing, when the paste became more viscous.
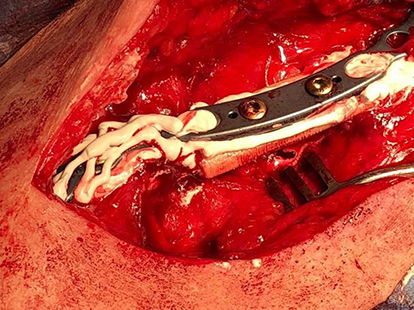 |
Figure 1 Defect and plate augmented with injectable bone graft substitute. |
An additional pseudarthrosis resection was performed and the bone ends were debrided in case of delayed unions or non-unions, followed by fitting of a locking clavicle plate. The resulting bone defect was augmented with 5mL CERAMENT G.
Layered, tension-free wound closure was performed using staple suture technique in all cases, after the bone graft substitute had set at 10 minutes from the start of mixing. Two surgeons performed surgery, one of whom was present at all the surgeries.
Surgical and Post-Operative Management
Surgery was performed under general anesthesia and in beach chair position with the upper body elevated by 30 degrees. Following surgical padding, the surgical field was washed and covered with sterile material in a standardized manner. Thirty to 60 minutes preoperatively a single dose of 2g Cefazolin was intravenously administered for peri-operative systemic antibiotic prophylaxis. If microbiological examination was planned, systemic antibiotic administration was delayed until multiple deep samples were taken. Surgical results were documented with X-rays in three planes. Postoperatively, local infiltration analgesia was used, and a sterile wound dressing was applied, as well as elastic wrapping and a fixed shoulder bandage of the affected extremity. The post-operative procedure was also standardized with dressing change on the 2nd postoperative day, and subsequent radiographic documentation of the clavicle in 2 planes. Inpatient stay was on average 5 days. Abduction was limited to 90 degrees for six weeks. Fixed shoulder bandage was applied for a maximum of 10 days postoperatively or until wound consolidation. Intensive physiotherapy, and if necessary lymphatic drainage was prescribed. Load bearing of the upper extremity was not allowed for six weeks. Standardized X-ray examination was performed at 2 and 6 weeks on an outpatient basis. Implant removal was generally recommended and was planned at the earliest for 18 months following surgery.
Data Collection and Outcome Parameters
Patient demographics, comorbidities, medication, aetiology and type of the clavicle lesion, information on surgery including information on implants used, as well as information on adverse events or complications were retrospectively collected from patient files. The University of California at Los Angeles Shoulder Score (UCLA shoulder score, USS), the quick form of the Disability of the Arm, Shoulder and Hand score (QuickDASH score, QDS) and the 12-item Short-Form Survey (SF-12) physical component questionnaire were obtained for patient-reported outcome measures, the latter and the USS using web-based scoring tools available from www.orthotoolkit.com/sf-12/ or https://orthotoolkit.com/UCLA-shoulder/, respectively.21–23 Pain levels were obtained using the visual analogue scale (VAS, range from 0 to 10, 0 indicates no pain, 10 indicates worst pain). Radiographs were retrospectively assessed with regard to proximal and distal bony union, and radiographic appearance of the bone graft substitute. The Goldberg radiographic scoring system, which was developed for the assessment of bone grafting, was used for this purpose.24 The Goldberg radiographic scoring considers the appearance of the graft (resorbed=0 points, mostly resorbed=1 point, largely intact=2 points, reorganizing=3 points) and the distal and proximal bony union separately (non-union=0 points, possible union=1 point, radiographic union=2 points); and the individual scores for the various parameters are summed up. Consequently, in the case of a reorganizing bone graft, and both distal and proximal radiological union, a maximum score of 7 points can be achieved.25 If the bone defects were too small for a separate evaluation of proximal and distal union situation, the union was evaluated for the defect as a whole, and the value obtained was multiplied by two.
Primary outcome measure was the bony consolidation rate of the clavicle lesions using the Goldberg score. Secondary outcome measures were the complication rate of our treatment, with special focus on revision surgeries, wound healing problems, post-operative white wound drainage associated with the degradation of the calcium sulphate component of the CERAMENT, infection including microbiological examination, delayed union or non-union, implant failure or refracture. Further secondary outcome parameters were the shoulder joint function, and the overall health quality at the time of the last follow-up. The functional assessments were carried out by a single surgeon. The radiological assessment was also carried out by a single surgeon, and randomly checked by another surgeon.
Results
We have treated 38 clavicles with the described surgical techniques during the reviewed time period. After applying the inclusion and exclusion criteria and obtaining informed patient consent, a total of 26 clavicles in 25 patients, 16 male and 9 female, were enrolled in the study. The patient cohort was middle aged with a mean age of 50.7 (16–85) years at the time of surgery, and had few comorbidities. Three patients had nicotine abuse as a risk factor. A total of 18 clavicles were treated for a displaced clavicle fracture. One patient was treated for bilaterally fractured clavicles. Four cases were refractures (15.4%) and two cases each were delayed unions (7.7%) and non-unions (7.7%), respectively. The delayed unions occurred after a non-surgical treatment attempt. One of the non-unions had already undergone multiple surgeries and the other developed after conservative treatment. Three of the refractures occurred after surgical treatment and new trauma. The majority of 17/26 (65.4%) clavicle lesions were located at the middle third, seven at the lateral third (26.9%) and two at the medial third (7.7%) of the clavicle. The four refractures, two delayed unions and the two non-unions, which were considered for our case series all occurred after shaft fractures. Hence, nine of the primary fractures were Allman type 1 fractures (50%), seven of type 2 (38.9%), and two at the medial third (11.1%) (Table 1). Three of the seven lateral fractures (42.8%) were of type IIa according to the Jäger&Breitner classification, and two of type IIb (28.6%), respectively; the two remaining lateral fractures were each classified as type I (14.3%) and III (14.3%). The mean follow-up was 14.9 months (6–31 months). With the exception of one LCP superior anterior plate used, all plates were placed superiorly. In 5/26 (19.2%) cases microbiological examinations were performed. Microbiology revealed infection with Cutibacterium acnes (sensitive to gentamicin) in one refracture. In three refractures, and a primary fracture microbiology was negative.
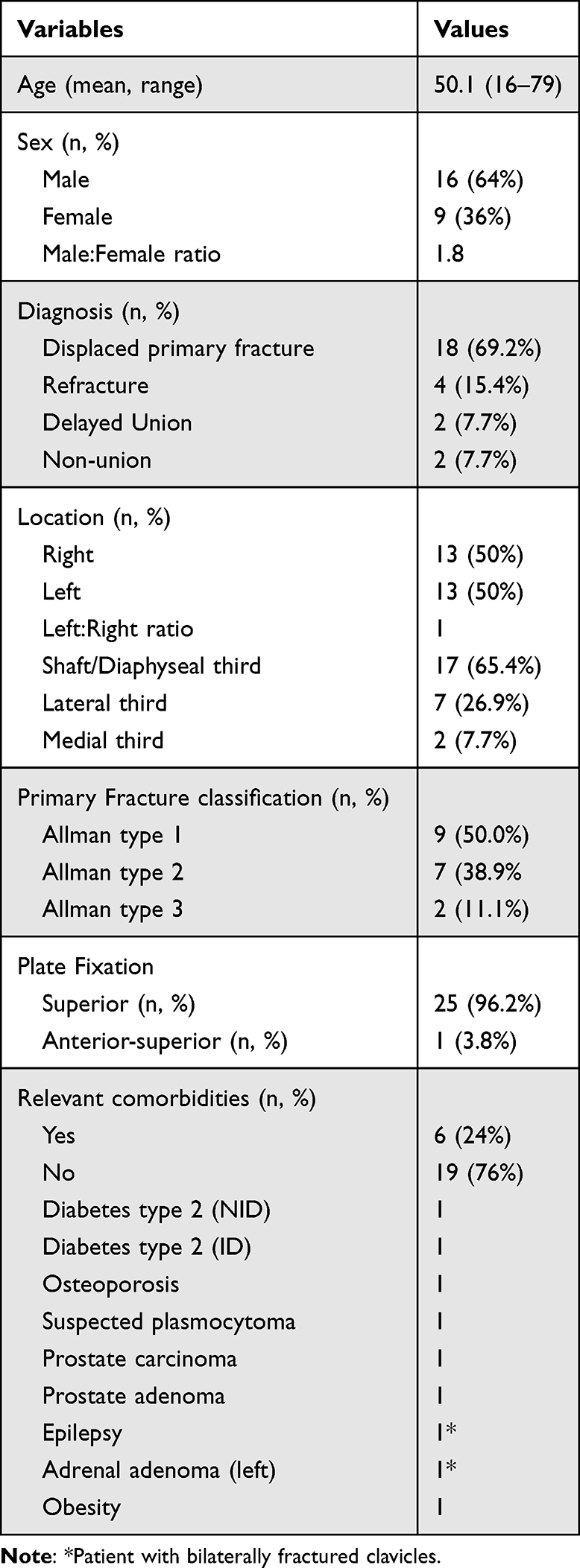 |
Table 1 Demographics and Baseline Characteristics |
Bony union was assessed to be complete in all cases, and the defects into which the bone graft substitute was placed were completely remodeled into bone, resulting in the maximum Goldberg score of seven throughout all cases. Five cases (19.2%) had implant removal between 17.5 and 31 months (mean 20.7 months) from surgery and at least 12 months from complete radiographic consolidation. No complications occurred after the surgeries, neither wound healing disorders nor infections. No cases of delayed bone healing or other complications occurred. Consequently, no revision surgeries became necessary, except for the patient-desired isolated implant removals. In particular, no case of white wound drainage occurred, which is associated with the degradation of the calcium sulphate component of the CERAMENT. With regard to shoulder functionality, the patients had at the time of the last follow-up a mean USS of 34.6±0.8 (32–35) points. The corresponding mean QDS score at that time was 0.6±1.6 (0–5.4) points. Four cases had slightly reduced range of motion. In three cases, both abduction and anteversion were reduced by 10°, and in one case abduction was reduced by 20° and both anteversion and retroversion was reduced by 10°. More detailed information is provided in Table 2. The following Figures 2–4 show the radiographic course of a primary fracture, refracture and delayed union.
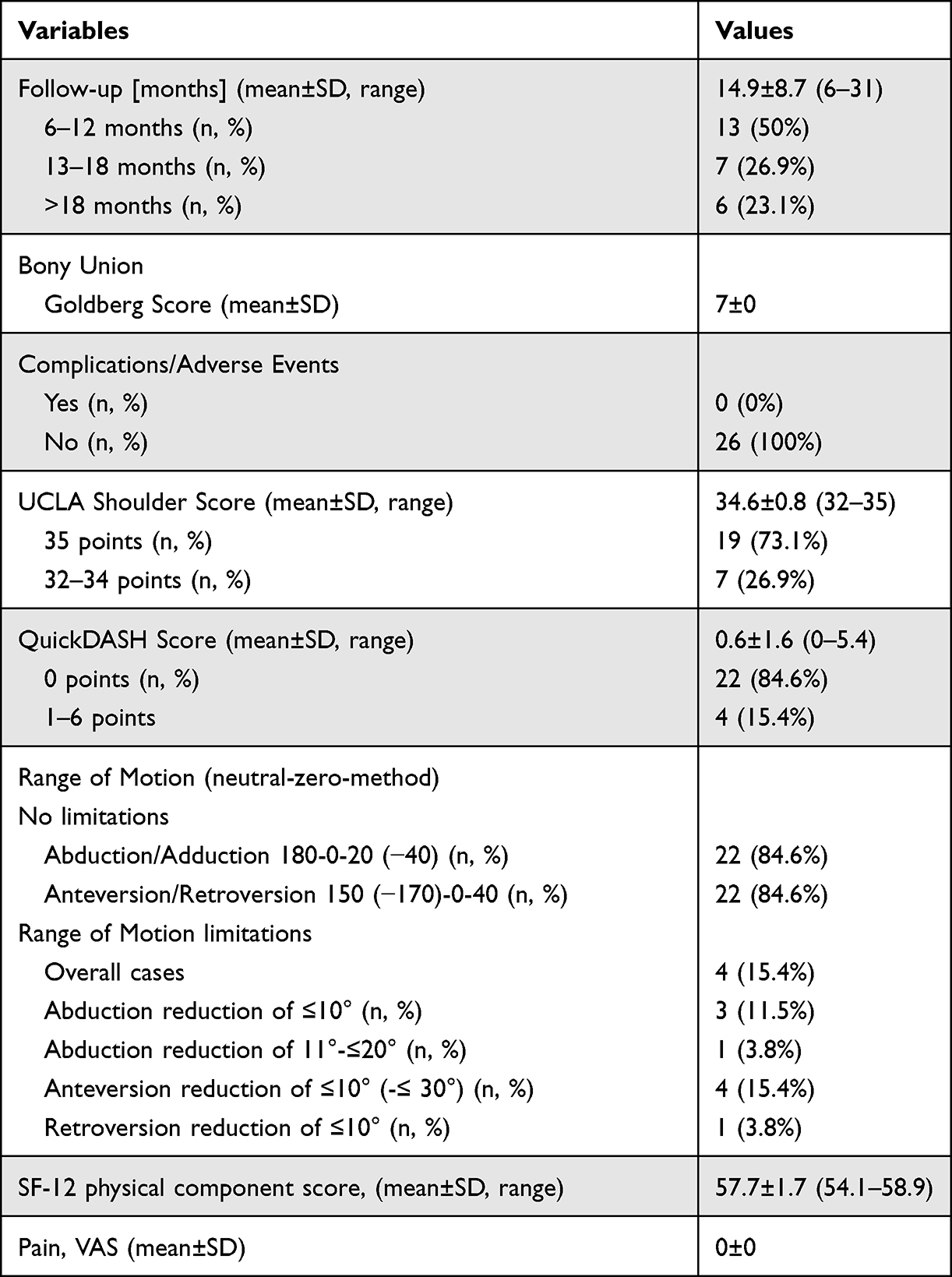 |
Table 2 Radiographic, Clinical and Functional Outcomes |
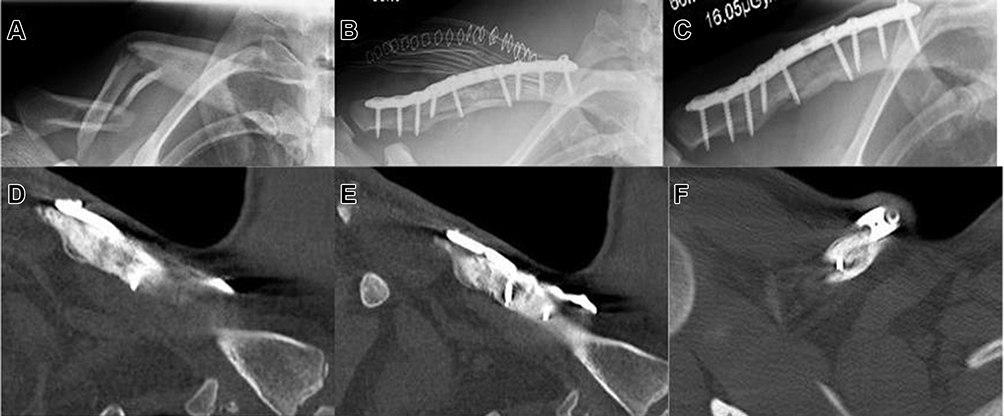 |
Figure 2 Displaced Allman type 1 fracture with free fragment; (A) preoperative axial radiograph; (B) postoperative axial radiograph after ORIF with a plate and screws and augmentation of both the bone defect and the plate with gentamicin-loaded bone graft substitute; (C) axial radiograph at 6 months showing bony consolidation; (D and E) coronal computed tomography (CT) scan at six months, various layers; and (F) transversal CT scan at 6 months confirming excellent bony consolidation. |
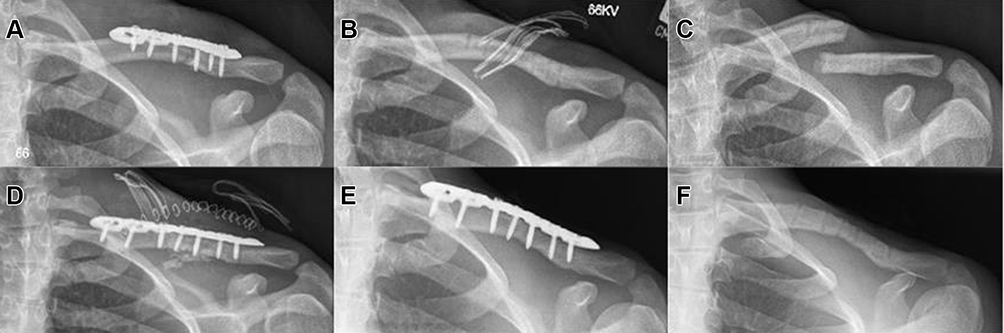 |
Figure 3 Refracture; (A) axial radiograph following initial surgical treatment of an Allman type 1 fracture without defect augmentation; (B) axial radiograph following implant removal; (C) axial radiograph of the refracture following implant removal; (D) post-operative axial radiograph after ORIF and defect/implant augmentation, (E) axial radiograph at 12 months revealing excellent radiographic union; and (F) axial radiograph upon implant removal at 18 months. |
 |
Figure 4 Delayed union after non-surgical treatment of an Allman type 1 fracture; (A) axial radiograph of a little displaced shaft fracture; (B) axial radiograph at 2 months revealing delayed union; (C) anterior-posterior (AP) radiograph confirming delayed union; (D) axial radiograph following surgical intervention with resection of the delayed union and debridement, ORIF and filling of the residual bone defect with CERAMENT G; (E) axial radiograph and (F)AP radiograph at 12 months showing excellent bony union. |
Discussion
Our study has the distinct feature that both primary fractures and their frequent complications, ie, delayed unions, non-unions and refractures were included, since we follow a similar surgical protocol for these cases. In the case of delayed unions and non-unions, pseudarthrosis resection and surgical debridement were performed. Apart from that, our surgical procedure does not differ for the various indications. We additionally fill the defects and/or augment the implants with a gentamicin-eluting bone graft substitute in the surgical treatment of clavicle fractures to prevent both non-unions and infections. The resorbable gentamicin-eluting bone graft substitute used is established in both the preventive use for acute fractures and the treatment of bone defects due to bone infections or (infected) non-unions.26–28 It allows for an extremely high local gentamicin concentration and is shown to remodel into bone.19,20
In our case series, we did not observe any notable differences regarding bone healing or complications for the various indications. Bony consolidation was complete in all cases at the time of the last follow-up, and the bone graft substitute had completely remodeled into bone. This was indicated by the maximum Goldberg score of 7 throughout all cases. No complications, such as wound healing problems, infection, delayed union or non-union, implant failure or refracture occurred. None of the patients had pain (VAS=0 throughout all cases) at the time of the last follow-up that would have required removal of the implant. No revision surgeries were necessary. Five patients (19.2%) had recommended implant removal more than 18 months from surgery. Furthermore, no post-operative white wound drainage was observed, which is a known common phenomenon associated with the degradation of the calcium sulphate component of the CERAMENT, usually resolving without complication. White drainage is often connected to a thin soft tissue envelope, especially at the tibia shaft.27,29 Concerning the thin soft tissue coverage at the clavicle, the absence of drainage was encouraging. Functionality impairment was limited to minor joint range of motion reductions of 10° in both abduction and anteversion in three cases, and of 20° in abduction, 10° anteversion and 10° retroversion in one case, when compared to literature values.30 The latter was manifested in a case that was treated for a shaft non-union, the other three cases following treatment of displaced and unstable lateral clavicle fractures.
The mean QDS was 0.6 points in our study, and the mean USS 34.6 points, which indicated excellent results. The scale scores for the QDS range between 0 (no disability) and 100 (most severe disability) points, the scores for the USS range between 0 and 35 points, with more than 27 points indicating good/excellent results.31,32 The mean value of the SF-12 physical score in our study was 57.7 points, which was notably higher than the average value of a 50-year-old normative sample in Germany.33
Defects following primary fractures at the clavicle are normally small. Osseous consolidation can often be seen within six months from surgery in case of a complication-free course.34–36 On the other hand, there are significant complication rates reported for both non-surgical and surgical treatment of clavicle fractures. Leroux et al published a population-based study from Canada in which 24.6% of the patients had at least one reoperation within 2 years from ORIF in midshaft fractures. The most common reason was isolated plate removal, which caused reoperation in 18.6% of the patients, followed by deep infection, non-union, and malunion, which applied for 2.6%, 2.6%, and 1.1%.13 Following conservative treatment, non-unions are the most common complication. In addition to the location and type of fracture, the surgical outcomes depend largely on the surgical technique. Complications associated with plate fixation of clavicle fractures include both implant failure or prominence, (deep) infections, non-unions and refracture.37 Wijdicks et al reviewed the literature for complications upon plate fixation of clavicle fractures and found non-union rates and malunion rates below 10% in 10/11 studies, and both wound and deep infection rates below 10% in 9/11 studies, with wound infections being reported in the majority of cases.38 Rollo et al retrospectively analyzed 71 non-union cases, in which the primary fractures were treated conservatively in 13 cases; with ORIF and plate fixation in 12 cases; with closed reduction and K-wire fixation in 24 cases; and ORIF with K-wire in 22 cases. The authors identified 22 infected non-unions, which all occurred in patients, which had been treated surgically; and identified both the infection and biomechanics as reason for the initial treatment failure.16 Refractures are uncommon if implants are removed later than 12 months after bony consolidation.12 They have a significantly elevated risk to develop non-union compared to primary fractures.12,39
While there are several reports on treatment of clavicular non-unions with autograft or allograft, we could not identify any specific studies with bone graft substitutes. Martetschläger et al reviewed the literature on treatment of clavicular non-unions and identified studies reporting favorable outcomes for non-union treatment with bone grafting, but also studies reporting good results if the defect was left empty.39 They recommended bone grafting in case of bone loss or bone defects resulting from resection of atrophic non-union. Schnetzke et al retrospectively analyzed both their results with and without bone grafting. The radiological and functional outcomes of 58 patients who were treated for non-union or delayed union by plate fixation were evaluated. Following removal of the bone sclerosis the defect was either filled with autologous bone graft or left empty. The authors found that bone grafting significantly accelerated bone healing and led to significantly enhanced bony consolidation and reduced pain according to the VAS. Additionally, the risk of revision surgery was significantly reduced, Constant Score revealed significantly and DASH score considerably better functional outcomes in the bone graft group. Health status was assessed with the Short-Form 36 (SF-36) score and was good in both groups, with significant better results for the bone graft group for the physical functioning scale. The authors concluded that treatment of clavicular non-unions should generally preferably be supported by bone grafting.40
Our study had several limitations, including its retrospective and non-controlled design, the overall small sample size; and especially the small samples sizes for refractures, delayed unions, and non-unions, which did not allow for separate subgroup analyses.
Conclusion
The literature reports relevant complication rates not only in the treatment of delayed unions, non-unions, and refractures, but also after conservative and surgical treatment of specific fractures such as significantly displaced fractures, fractures with significant shaft shortening, and displaced and unstable Neer type II fractures. Our initial experience suggests that plate ORIF with bone defect and/or implant augmentation with a gentamicin-eluting bone graft substitute (CERAMENT G, BONESUPPORT) may be useful not only for complication management after clavicle fractures but also in the initial treatment of challenging primary clavicular fractures, in order to reduce the risk of complications at this stage.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the medical association of Lower Saxony. All patients gave written informed consent before their enrollment in the study.
Disclosure
JP reports that he is a consultant for ARTIQO GmbH, BONESUPPORT AB, and MicroPort Scientific GmbH. GH and HH report no conflicts of interest in this work.
References
1. Matthes G, Müller-Mai CM. Clavicula. In: Müller-Mai C, Ekkernkamp A, editors. Frakturen: Klassifikationen Und Behandlungsoptionen[Fractures: Classifications and treatment options]. Heidelberg: Springer; 2010:417–426.
2. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994;300:127–132. doi:10.1097/00003086-199403000-00016
3. van der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. J Shoulder Elbow Surg. 2012;21(3):423–429. doi:10.1016/j.jse.2011.08.053
4. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am. 2009;91(2):447–460. doi:10.2106/JBJS.H.00034
5. Allman FL
6. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968;58:43–50. doi:10.1097/00003086-196805000-00007
7. Jäger M, Breitner S. Therapiebezogene Klassifikation der lateralen Claviculafraktur [Therapy related classification of lateral clavicular fracture]. Unfallheilkunde. 1984;87(11):467–473.
8. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002;11(5):452–456. doi:10.1067/mse.2002.126613
9. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br. 1998;80(3):476–484. doi:10.1302/0301-620X.80B3.0800476
10. Bakir MS, Merschin D, Unterkofler J, et al. Injuries of the medial clavicle: a cohort analysis in a level-I-trauma-center. concomitant injuries. management. classification. Chirurgia. 2017;112(5):594. doi:10.21614/chirurgia.112.5.586
11. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD; Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the evidence-based orthopaedic trauma working group. J Orthop Trauma. 2005;19(7):504–507. doi:10.1097/01.bot.0000172287.44278.ef
12. Jeray KJ, Hill AD. Complications of clavicle fractures—Diagnosis and management. In: Disorders of the Shoulder: Trauma. Vol. 3. Wolters Kluwer Health Adis (ESP); 2013:135–150.
13. Leroux T, Wasserstein D, Henry P, et al. Rate of and risk factors for reoperations after open reduction and internal fixation of midshaft clavicle fractures: a population-based study in Ontario, Canada. J Bone Joint Surg Am. 2014;96(13):1119–1125. doi:10.2106/JBJS.M.00607
14. Oh JH, Kim SH, Lee JH, Shin SH, Gong HS. Treatment of distal clavicle fracture: a systematic review of treatment modalities in 425 fractures. Arch Orthop Trauma Surg. 2011;131(4):525–533. doi:10.1007/s00402-010-1196-y
15. Wurm M, Siebenlist S, Zyskowski M, et al. Excellent clinical and radiological outcome following locking compression plate fixation of displaced medial clavicle fractures. BMC Musculoskelet Disord. 2021;22(1):905. doi:10.1186/s12891-021-04775-8
16. Rollo G, Pichierri P, Marsilio A, Filipponi M, Bisaccia M, Meccariello L. The challenge of nonunion after osteosynthesis of the clavicle: is it a biomechanical or infection problem? Clin Cases Miner Bone Metab. 2017;14(3):372–378. doi:10.11138/ccmbm/2017.14.3.372
17. Martetschläger F, Gaskill TR, Millett PJ. Management of clavicle nonunion and malunion. J Shoulder Elbow Surg. 2013;22(6):862–868. doi:10.1016/j.jse.2013.01.022
18. Stufkens SA, Kloen P. Treatment of midshaft clavicular delayed and non-unions with anteroinferior locking compression plating. Arch Orthop Trauma Surg. 2010;130(2):159–164. doi:10.1007/s00402-009-0864-2
19. Stravinskas M, Horstmann P, Ferguson J, et al. Pharmacokinetics of gentamicin eluted from a regenerating bone graft substitute: in vitro and clinical release studies. Bone Joint Res. 2016;5(9):427–435. doi:10.1302/2046-3758.59.BJR-2016-0108.R1
20. Ferguson J, Athanasou N, Diefenbeck M, McNally M. Radiographic and histological analysis of a synthetic bone graft substitute eluting gentamicin in the treatment of chronic osteomyelitis. J Bone Jt Infect. 2019;4(2):76–84. doi:10.7150/jbji.31592
21. Amstutz HC, Sew Hoy AL, Clarke IC. UCLA anatomic total shoulder arthroplasty. Clin Orthop Relat Res. 1981;155:7–20. doi:10.1097/00003086-198103000-00002
22. Beaton DE, Wright JG, Katz JN; Upper Extremity Collaborative Group. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005;87(5):1038–1046. doi:10.2106/JBJS.D.02060
23. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
24. Goldberg VM, Powell A, Shaffer JW, Zika J, Bos GD, Heiple KG. Bone grafting: role of histocompatibility in transplantation. J Orthop Res. 1985;3(4):389–404. doi:10.1002/jor.1100030401
25. Choi Y, Yang YH, Kwon YH. Reliability of Goldberg scoring system in the radiographic evaluation of bony union after bone grafting. Clin Orthop Surg. 2021;13(4):549. doi:10.4055/cios19152
26. Aljawadi A, Islam A, Jahangir N, et al. One-stage combined “fix and flap” approach for complex open Gustilo-Anderson IIIB lower limbs fractures: a prospective review of 102 cases. Arch Orthop Trauma Surg. 2021:1–10. doi:10.1007/s00402-020-03392-9
27. McNally MA, Ferguson JY, Lau AC, et al. Single-stage treatment of chronic osteomyelitis with a new absorbable, gentamicin-loaded, calcium sulphate/hydroxyapatite biocomposite: a prospective series of 100 cases. Bone Joint J. 2016;98-B(9):1289–1296. doi:10.1302/0301-620X.98B9.38057
28. Freischmidt H, Armbruster J, Reiter G, Grützner PA, Helbig L, Guehring T. Individualized techniques of implant coating with an antibiotic-loaded, hydroxyapatite/calcium sulphate bone graft substitute. Ther Clin Risk Manag. 2020;16:689–694. doi:10.2147/TCRM.S242088
29. Pesch S, Hanschen M, Greve F, et al. Treatment of fracture-related infection of the lower extremity with antibiotic-eluting ceramic bone substitutes: case series of 35 patients and literature review. Infection. 2020;48(3):333–344. doi:10.1007/s15010-020-01418-3
30. Buckup K, Buckup J, Pässler HH. Klinische Tests an Knochen, Gelenken Und Muskeln: Untersuchungen-Zeichen-Phänomene [Clinical Tests on Bones, Joints and Muscles: Examinations-Signs-Phenomena]. Springer; 2012.
31. Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord. 2006;7(1):44. doi:10.1186/1471-2474-7-44
32. Nutton RW, McBirnie JM, Phillips C. Treatment of chronic rotator-cuff impingement by arthroscopic subacromial decompression. J Bone Joint Surg Br. 1997;79(1):73–76. doi:10.1302/0301-620X.79B1.0790073
33. Strada L, Schmidt CS, Rosenkranz M, et al. Factors associated with health-related quality of life in a large national sample of patients receiving opioid substitution treatment in Germany: a cross-sectional study. Subst Abuse Treat Prev Policy. 2019;14(1):1–14. doi:10.1186/s13011-018-0187-9
34. Beirer M, Siebenlist S, Crönlein M, et al. Clinical and radiological outcome following treatment of displaced lateral clavicle fractures using a locking compression plate with lateral extension: a prospective study. BMC Musculoskelet Disord. 2014;15(1):1–9. doi:10.1186/1471-2474-15-380
35. Pecci M, Kreher JB. Clavicle fractures. Am Fam Physician. 2008;77(1):65–70.
36. Ferran NA, Hodgson P, Vannet N, Williams R, Evans RO. Locked intramedullary fixation vs plating for displaced and shortened mid-shaft clavicle fractures: a randomized clinical trial. J Shoulder Elbow Surg. 2010;19(6):783–789. doi:10.1016/j.jse.2010.05.002
37. Böstman O, Manninen M, Pihlajamäki H. Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma. 1997;43(5):778–783. doi:10.1097/00005373-199711000-00008
38. Wijdicks FJ, Van der Meijden OA, Millett PJ, Verleisdonk EJ, Houwert RM. Systematic review of the complications of plate fixation of clavicle fractures. Arch Orthop Trauma Surg. 2012;132(5):617–625. doi:10.1007/s00402-011-1456-5
39. Martetschläger F, Gaskill TR, Millett PJ. Management of clavicle nonunion and malunion. J Shoulder Elbow Surg. 2013;22(6):862-8.
40. Schnetzke M, Morbitzer C, Aytac S, et al. Additional bone graft accelerates healing of clavicle non-unions and improves long-term results after 8.9 years: a retrospective study. J Orthop Surg Res. 2015;10(1):1–9. doi:10.1186/s13018-014-0143-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.