Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Surgical Treatment for Cutaneous Mycobacterium abscessus Infection Caused by Injections of Hyaluronic Acid
Received 25 October 2022
Accepted for publication 10 March 2023
Published 20 March 2023 Volume 2023:16 Pages 687—692
DOI https://doi.org/10.2147/CCID.S394594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anne-Claire Fougerousse
Yuanzhi Liu, Yongjun Chen
Department of Medical Cosmetology, Dermatology Hospital of Southern Medical University, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Yongjun Chen, Department of Medical Cosmetology, Dermatology Hospital, Southern Medical University, 2 Lujing Road, Yuexiu District, Guangzhou, 523326, Guangdong, People’s Republic of China, Tel/Fax +86 20-87257353, Email [email protected]
Background: Facial injection has become popular in aesthetic dermatology. Although injections of these tissue fillers are considered a low-risk procedure, they are not without potentially significant drawbacks.
Case Presentation: We would like to report a case about cutaneous Mycobacterium abscessus infection after facial injection of hyaluronic acid in China, which obtained satisfactory clinical efficacy by drainage and surgical excision.
Conclusion: Biological techniques are useful in the diagnosis of cutaneous M. abscessus infection. Surgical excision of skin lesion is effective for cutaneous M. abscessus infection.
Keywords: hyaluronic acid, injection, cutaneous Mycobacterium abscessus, infection, surgical treatment
Background
Facial injection has become popular in aesthetic dermatology. Although injections of these tissue fillers are considered a low-risk procedure, they are not without potentially significant drawbacks. For the past few years, an increase in the incidence of cutaneous non-tuberculous mycobacteria (NTM) infections has been observed.1 Although there is no solid explanation for this phenomenon, it has been at least partially attributed to the increasing development of the cosmetic and aesthetic dermatological industries.2 Skin and soft tissue infections caused by NTM have been increasingly described as a complication associated with cosmetic procedures.3 Cases or outbreaks are therefore reported after mesotherapy,4 hair transplant,2 injection of botulinum toxin A,5,6 illicit intramammary injections of silicone,7 liposuction,8 face lift,9 piercing,10 and tattooing.11 However, few cases of secondary NTM infections after injection of hyaluronic acid filler have been reported. The treatment of NTM infection is also challenging. As NTM is resistant to various antibiotics and differs in antimicrobial sensitivities, surgical treatment is usually required as combination therapy. We would like to report a case about cutaneous Mycobacterium abscessus infection after facial injection of hyaluronic acid in China, which obtained satisfactory clinical efficacy by drainage and surgical excision.
Case Presentation
A 37-year-old woman complained the development of multiple, painful nodules and abscesses on both cheeks about one week after injection of a mixture containing hyaluronic acid (exact product name could not be recalled) for facial depression filling at a private clinic a month ago. The patient has received antimicrobial treatment (oral clarithromycin) for 3 weeks at another hospital, but the symptoms did not improve. The patient denied fever or other systemic symptoms. The patient had no previous filler injection or surgery on her face in the past. Dermatological examination revealed multiple erythematous, non-tender nodules on both cheeks, without palpable lymphadenopathy (Figure 1).
 |
Figure 1 Clinical picture of the patient. |
Results of routine laboratory tests were normal. Smear test of abscess fluid showed gram-positive cocci. Acid fast staining of the puncture fluid was also positive. Mycobacterium abscessus was identified in the bacterial culture of puncture fluid (Figure 2). Moreover, both the polymerase chain reaction (PCR) and mass spectrometry (MS) analysis confirmed Mycobacterium abscessus in the puncture fluid of abscess. Histopathology showed infectious granuloma and infiltration of lymphocytes, plasma cells, multinucleate giant cells, as well as neutrophils in the dermis (Figure 3).
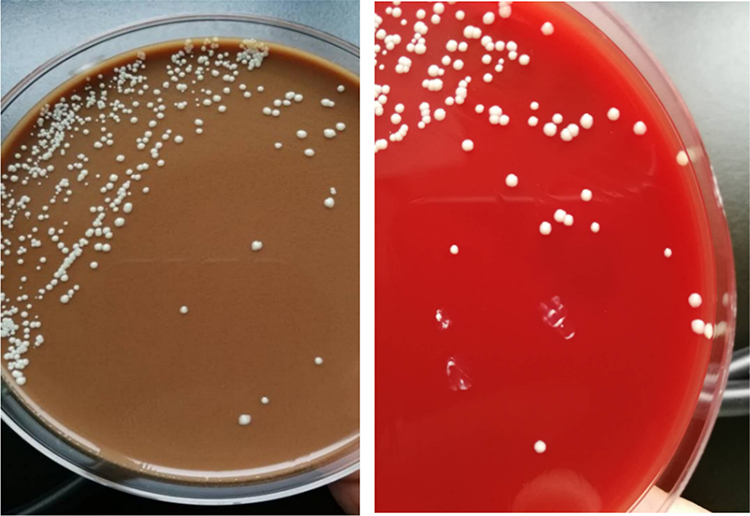 |
Figure 2 Mucoid cream-colored colonies on agar and blood agar from puncture fluid specimens, which were identified as Mycobacterium abscessus by PCR and mass spectrometry analysis. |
 |
Figure 3 Histopathologic results showed infectious granuloma with lymphocytes, plasma cells, multinucleate giant cells infiltrate in the surrounding tissues and heavy lymphocytes, plasma cells, neutrophils infiltrate in deep dermis (H&E stain, Original magnification×10; Original magnification ×40). |
The patient explicitly resisted to take oral medicine because of potential side effects and a long course of treatment. Following needle aspiration of pus, abscesses were washed with 4.4 mL solution containing 7mg diprospan and 600u hyaluronidase. Seven months later, lesions on the left cheek completely disappeared, while lesions on the right cheek showed no significant change. Because of no improvement on the right cheek after an additional drainage and irrigation of the abscess, surgical excision of abscess was performed. The infected skin and subcutaneous tissue were removed during surgery. After operation, mupirocin ointment was applied outside the incision, and dressing was changed every other day until the stitching was removed after 1 week. No recurrence was observed during 18-month follow-up (Figure 4).
 |
Figure 4 Picture of the patient at a 18-month follow-up after treatment. |
Discussion
M. abscessus, together with M. fortuitum and M. chelonae, are the most common rapidly growing non-tuberculous mycobacteria (RGM) pathogens.5 M. abscessus can live and last a long time in various external environments such as soil, decaying vegetation, bioaerosols, and water.11 M. abscessus is capable of surviving longer due to their relative resistance to standard disinfectants such as chlorine, organomercurials, alkaline glutaraldehydes, and 2% formaldehyde.12,13 M. abscessus also forms biofilms so that resistance can easily occur. Therefore, M. abscessus is frequently detected in health-care facilities and can appear after long incubation periods.4,14 The source of the nosocomial infections could be the re-use of needles without proper sterilization and the contaminated gentian violet solution and tap water for medical procedures and instrument cleaning.14 Besides, the use of unapproved medications may be another reason, and there have been reports of abscesses induced by the injection of a variety of contaminated solutions, such as local anesthetic agents and steroids.15 In the present study, the patient underwent the injection of a bottle of dermal fillers contained “hyaluronic acid and epidermal growth factor mixed formulation” (exact name could not be recalled) at a unauthorized private clinic. The lesions occurred 7 days after the injection. The disease history and location of the lesions led us to conclude that the source of the infection in this case may be unapproved cosmetic medications or external environments and medical equipments without proper sterilization.
Common complications of facial injection include infections, bleeding, foreign body reaction, erythema, swelling, itching, bruising, induration, depigmentation, lumpiness, ulceration, and vascular complication,3,16,17 among which RGM infection is rare. Any chronic cutaneous lesion located at any cutaneous site after a medical procedure must evoke the possibility of RGM infection.5 It was reported that the mean time between the first injection and the appearance of the first symptoms was 9.5 weeks (range, 1–29 weeks).18 However, treatment for M. abscessus can be challenging because currently there is no guideline to treat the associated skin and soft tissue infections.19 The consensus is that the choice of therapy for infections with RGM depends on the condition of the patient. Patients who are immunocompromised or with disseminated disease require more aggressive therapy with intravenous antibiotics,7 while for normal patient, optimal treatment is yet to be established, and the use of surgical treatment and/or antibiotic therapy needs to be evaluated on a case-by-case basis.18 Classic antibiotic therapeutic choices for M. abscessus infections are clarithromycin and azithromycin, and other antibiotic susceptibility panels could include amikacin, tigecycline, cefoxitin, ciprofloxacin, doxycycline, imipenem, and sulfonamide. It was reported that RGM frequently exhibits acquired resistance to a single antibiotic.20 Consequently monotherapy was not recommended, and a double or triple antibiotic regimen formulated according to in vitro susceptibility results may be a legitimate choice. The course of antibiotic treatment for localized cutaneous infection is usually 2 through 4 months, and at least 6 months is recommended for the treatment of disseminated disease. It was reported that 10–20% patients experienced a relapse in disease after discontinuing antibiotic therapy at the time of wound healing, therefore therapy should be continued for 4–6 weeks after lesions healing.20 Another study reported that among the 16 patients developed cutaneous infections by RGM, no recurrent abscess occurred in 3 patients (2 of whom had only undergone surgical treatment and 1 of whom who had undergone surgical treatment combined with antibiotic therapy), while in the remaining 13 treated patients, disease initially progressed despite an effective in vitro susceptibility to 2–3 antibiotics.21
In our study, the patient explicitly rejected oral drugs for potential side effects and prolonged course, therefore surgical puncture, drainage, and dissolving of foreign bodies were performed at an early stage. As a result, the lesions on her left cheek were cured with no evidence of recurrence after the first surgical interventions. However, the lesions on the right cheek had no significant change after drainage twice. Therefore, the patient underwent surgical excision and has not relapsed up to now.
This study has some limitations. The patient in this study could not adhere to adequate antibiotic therapy for 4–6 months and stopped taking antibiotics after 3 weeks of oral administration, so antibiotic therapy did not achieve good efficacy. The sample size of this study is too small, and the effect of surgical treatment still needs further research.
Conclusion
The present case indicates that cosmetic dermal filler injections such as hyaluronic acid at unauthorized private clinics can cause M. abscessus infection. Biological techniques are useful in the diagnosis of cutaneous M. abscessus infection. Surgical treatment is an effective option for cutaneous M. abscessus infection when antibiotics do not respond well or patients are unable to insist on oral antibiotics.
Ethics Approval and Consent to Participate
The patient in our case has signed the informed consent. This study was designed in accordance with the Declaration of Helsinki and approved by the ethics committee of Dermatology Hospital, Southern Medical University.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
The authors would like to thank all study participants who were enrolled in this study.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wentworth AB, Drage LA, Wengenack NL, Wilson JW, Lohse CM. Increased incidence of cutaneous nontuberculous mycobacterial infection, 1980 to 2009: a population-based study. Mayo Clin Proc. 2013;88:38–45. doi:10.1016/j.mayocp.2012.06.029
2. Eustace K, Jolliffe V, Sahota A, Gholam K. Cutaneous Mycobacterium abscessus infection following hair transplant. Clin Exp Dermatol. 2016;41:768–770. doi:10.1111/ced.12900
3. Medeiros CC, Cherubini K, Salum FG, de Figueiredo MA. Complications after polymethylmethacrylate (PMMA) injections in the face: a literature review. Gerodontology. 2014;31:245–250. doi:10.1111/ger.12044
4. Garcia-Navarro X, Barnadas MA, Dalmau J, Coll P, Gurgui M, Alomar A. Mycobacterium abscessus infection secondary to mesotherapy. Clin Exp Dermatol. 2008;33:658–659. doi:10.1111/j.1365-2230.2008.02869.x
5. Fang RY, Sun QN. Mycobacterium abscessus infections following injection of botulinum toxin. J Cosmet Dermatol. 2020;19:817–819. doi:10.1111/jocd.13094
6. Saeb-Lima M, Solis-Arreola GV, Fernandez-Flores A. Mycobacterial infection after cosmetic procedure with botulinum toxin a. J Clin Diagn Res. 2015;9:WD01–2. doi:10.7860/JCDR/2015/11741.5756
7. Fox LP, Geyer AS, Husain S, Della-Latta P, Grossman ME. Mycobacterium abscessus cellulitis and multifocal abscesses of the breasts in a transsexual from illicit intramammary injections of silicone. J Am Acad Dermatol. 2004;50:450–454. doi:10.1016/j.jaad.2003.09.008
8. Meyers H, Brown-Elliott BA, Moore D, et al. An outbreak of Mycobacterium chelonae infection following liposuction. Clin Infect Dis. 2002;34:1500–1507. doi:10.1086/340399
9. Wallace RJ. The clinical presentation, diagnosis, and therapy of cutaneous and pulmonary infections due to the rapidly growing mycobacteria, M. fortuitum and M. chelonae. Clin Chest Med. 1989;10:419–429. doi:10.1016/S0272-5231(21)00644-4
10. Trupiano JK, Sebek BA, Goldfarb J, Levy LR, Hall GS, Procop GW. Mastitis due to Mycobacterium abscessus after body piercing. Clin Infect Dis. 2001;33:131–134. doi:10.1086/320885
11. Wongkitisophon P, Rattanakaemakorn P, Tanrattanakorn S, Vachiramon V. Cutaneous Mycobacterium abscessus infection associated with mesotherapy injection. Case Rep Dermatol. 2011;3:37–41. doi:10.1159/000324766
12. Selvaraju SB, Khan IU, Yadav JS. Biocidal activity of formaldehyde and nonformaldehyde biocides toward Mycobacterium immunogenum and Pseudomonas fluorescens in pure and mixed suspensions in synthetic metalworking fluid and saline. Appl Environ Microbiol. 2005;71:542–546. doi:10.1128/AEM.71.1.542-546.2005
13. Carson LA, Petersen NJ, Favero MS, Aguero SM. Growth characteristics of atypical mycobacteria in water and their comparative resistance to disinfectants. Appl Environ Microbiol. 1978;36:839–846. doi:10.1128/aem.36.6.839-846.1978
14. Rotunda AM, Kolodney MS. Mesotherapy and phosphatidylcholine injections: historical clarification and review. Dermatol Surg. 2006;32:465–480. doi:10.1111/j.1524-4725.2006.32100.x
15. Tiwari TS, Ray B, Jost KC, et al. Forty years of disinfectant failure: outbreak of postinjection Mycobacterium abscessus infection caused by contamination of benzalkonium chloride. Clin Infect Dis. 2003;36:954–962. doi:10.1086/368192
16. Balighi K, Kamyab K, Azizpour A. Granuloma annulare after Botulinum toxin A injection: a rare association. J Cosmet Dermatol. 2020;19:2549–2551. doi:10.1111/jocd.13310
17. Griffin I, Schmitz A, Oliver C, et al. Outbreak of tattoo-associated nontuberculous mycobacterial skin infections. Clin Infect Dis. 2019;69:949–955. doi:10.1093/cid/ciy979
18. Regnier S, Cambau E, Meningaud JP, et al. Clinical management of rapidly growing mycobacterial cutaneous infections in patients after mesotherapy. Clin Infect Dis. 2009;49:1358–1364. doi:10.1086/606050
19. Lee WJ, Kang SM, Sung H, et al. Non-tuberculous mycobacterial infections of the skin: a retrospective study of 29 cases. J Dermatol. 2010;37:965–972. doi:10.1111/j.1346-8138.2010.00960.x
20. Jogi R, Tyring SK. Therapy of nontuberculous mycobacterial infections. Dermatol Ther. 2004;17:491–498. doi:10.1111/j.1396-0296.2004.04051.x
21. Uslan DZ, Kowalski TJ, Wengenack NL, Virk A, Wilson JW. Skin and soft tissue infections due to rapidly growing mycobacteria: comparison of clinical features, treatment, and susceptibility. Arch Dermatol. 2006;142:1287–1292. doi:10.1001/archderm.142.10.1287
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.