Back to Journals » Clinical Ophthalmology » Volume 17
Surgical Outcomes with and without Prism Adaptation of Cases with Acute Acquired Comitant Esotropia Related to Prolonged Digital Device Use
Authors Yagasaki T ![]() , Yokoyama Y
, Yokoyama Y ![]() , Yagasaki A
, Yagasaki A ![]() , Eboshita R, Tagami K, Haga Y, Touya A
, Eboshita R, Tagami K, Haga Y, Touya A
Received 1 January 2023
Accepted for publication 2 March 2023
Published 11 March 2023 Volume 2023:17 Pages 807—816
DOI https://doi.org/10.2147/OPTH.S403300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Teiji Yagasaki,1,2 Yoshimi Yokoyama,2 Ayaka Yagasaki,2,3 Riho Eboshita,1 Keiko Tagami,1 Yayoi Haga,1 Arisu Touya1
1Yagasaki Eye Clinic, Ichinomiya, Aichi, Japan; 2Department of Ophthalmology, Japan Community Healthcare Organization Chukyo Hospital, Nagoya, Aichi, Japan; 3Department of Ophthalmology, Gifu Prefectural General Medical Center, Gifu, Gifu, Japan
Correspondence: Teiji Yagasaki, Yagasaki Eye Clinic, 62-6 Gonaka, Kaimei, Ichinomiya, Aichi, 494-0001, Japan, Tel +81-586-61-8787, Fax +81-586-61-9210, Email [email protected]
Purpose: To analyze surgical results of 32 cases with acute acquired comitant esotropia (AACE) related to prolonged use of digital devices (DDs).
Patients and Methods: Medical records of cases with AACE related to prolonged use of DDs that had undergone surgery were retrospectively revised. Complete medical history and full ophthalmological examinations before and surgery were obtained for all cases. All cases also underwent neurological examinations using brain and orbital imaging. Motor success was considered as alignment within 10 prism diopters (Δ) at both near and distance. Sensory success was defined as stereopsis ≤ 60 arcsec. Nineteen cases (Group S) underwent surgery alone and 13 cases were treated with surgery and prism adaptation (Group S+P). Motor and sensory outcomes were compared between groups.
Results: Mean age at first visit was 22.0 ± 9.0 years and mean daily use of DDs use was 6.3 ± 3.4 hours. Mean angle of preoperative alignment for distance and near were 26.5 ± 13.0Δ and 24.6 ± 16.4Δ, respectively. Surgery was performed at a mean of 23.3 ± 3.5 years old and mean angle of alignment at final examination for distance and near were 5.8 ± 7.7Δ and 3.5 ± 5.7Δ, respectively. Final motor and sensory success rate were 84% and 53%, respectively. No significant differences in motor or sensory outcomes were evident between groups at initial or last visit.
Conclusion: Favorable motor and sensory outcomes were achieved with surgical intervention with and without prism adaptation for AACT related to prolonged use of DDs.
Keywords: acute acquired comitant esotropia, prism adaptation, strabismus surgery, visual function, digital device
Introduction
Acute acquired comitant esotropia (AACE) is a rare type of esotropia, comprising 0.3% of children with strabismus.1 AACE characteristically develops during adolescence and early adulthood with sudden diplopia and comitant deviation.2,3 AACE has been classified into three types according to clinical characteristics and etiology: type 1, caused by interruption of fusion due to monocular obstruction such as occlusion therapy, eye trauma, or a sudden decrease in visual acuity in one eye (Swan type); type 2, caused by physical stress such as fever or psychological stress (Burian-Franceschetti type); and type 3, caused by mild to moderate myopia ≥-5.0D without adequate correction (Bielschowsky type).4–6 Intracranial diseases including intracranial tumors, Chiari malformation, hydrocephalus, and other neurological diseases have been reported as additional etiology of AACE, despite a lack of clear neurological signs other than acute esotropia.6,7 In most of those cases, comitant ocular motility and deviation are observed first and those findings are considered a sign of benign ocular deviation.6,7 However, the comitancy of esotropia is not an absolute guarantee of normal neurological findings, and neuroradiological investigations are recommended to rule out intracranial disease as the cause of acute esotropia.
Since the first report pointing out a relationship between AACE and excessive smartphone use by Lee et al in 2016,8 several investigations have proposed associations between AACE and excessive use of digital devices (DDs), such as computers, tablets, and smartphones for near work.9–14 The use of DDs by adolescents and young adults has dramatically increased within the past decade, particularly during lockdowns associated with the coronavirus disease 2019 pandemic.15–17 As a pathological etiology for this new type of AACE, Lee et al and Yilmaz et al speculated that excessive use of DDs would induce strong increases in the tone of both medial rectus muscles following long-acting accommodative efforts and disruption of vergence.8,10 All patients presenting with this condition are instructed to limit or reduce the use of DDs, resulting in improved esodeviation in some patients.8 Nevertheless, if AACE does not improve, surgical treatment is required.
Although surgical options for AACE include unilateral medial rectus recession (UMRR) and bilateral medial rectus recession (BMRR), surgical outcomes for AACE related to prolonged DDs have not been clarified because of unfavorable recurrence or undercorrection with recession procedures using the traditional surgical angle. Regarding better surgical outcomes, Savino et al recommended the preoperative prism adaptation test to determine the surgical dosage according to good postoperative results for six patients comprising one case with Swan type and five cases with Burian-Franceschetti type.18 Zhang et al also reported the results of therapeutic effects in 46 cases of AACE treated using surgery with preoperative prism treatment or surgery alone (Burian-Franceschetti type, n = 21; Bielschowsky type, n = 25).19 They also recommended surgery following preoperative prism treatment based on the findings of improved binocular function and reduced recurrence rate. However, few studies have examined the benefits of prism adaptation test or preoperative prism treatment for AACE related to the excessive use of DDs. We performed surgical alignments with both surgery alone and surgery following prism treatment for AACE related to prolonged use of DDs. This study aimed to compare the therapeutic effects of surgery alone and surgery with prism treatment for AACE related to prolonged use of DDs.
Materials and Methods
Among the 51 cases diagnosed with AACE between 2015 and 2021, cases of the three historical types (Swan type, Franceschetti type, and Bielschowsky type) were excluded after careful confirmation of no history leading to those three types. Cases showing a tendency of the three historical types were excluded from this study. Cases with a history of accommodative esotropia, strabismus surgery, or neurological disorders were excluded. The definition of acute onset could be identified in all cases after interviewing about the sudden onset of diplopia or esotropia because the youngest participant was 5.9 years old. Finally, 32 cases who underwent surgical alignment for AACE related to prolonged use of DDs were retrospectively included in this study. Using DD for ≥4 h per day before or at symptom onset was defined as prolonged or excessive use of DDs according to previous reports.8,10,12,14
At the first visit, all cases underwent ophthalmic and orthoptic examinations. Cycloplegic refraction was performed after administering 1% atropine sulfate eye drops once daily for 3–5 days to completely eliminate accommodative effects, and spherical equivalents (SE) of refractive error were calculated. Patients with overcorrected glasses were excluded from the study. Regarding cases wearing undercorrected glasses, proper glasses based on fully cycloplegic refraction were prescribed. Ocular motility was evaluated clinically using the Hess red-green test under prism neutralization to confirm comitant esodeviation. The deviation was measured using the alternate prism cover test (APCT) in all nine gaze positions with full refractive correction at distance and near. Binocular responses at near and distance were evaluated using Bagolini striated lenses. Near stereoacuity was assessed using the Randot Stereotest (Stereo Optical, Chicago, IL) or Titmus Stereo Test (Stereo Optical). All patients underwent cranial and orbital computed tomography or magnetic resonance imaging to rule out paretic strabismus or other ACCE caused by intracranial diseases.
Based on the angle of esotropia near accommodative fixating targets with the APCT, each case was given an initial prism adaptation using a Fresnel prism (FP) mounted base-out on spectacles, almost equally divided over the left and right eyes. When the measured deviations varied or increased during the APCT, the largest angle was recorded as the angle of esotropia. The prism-adapted angle was defined as the maximum power of the prism to neutralize esodeviation at near and distance after prism adaptation for 30 min. After disappearance of diplopia with prism adaptation, cases were asked if they select to continue prism adaptation until surgical intervention, if necessary. Of all patients, 13 underwent prism adaptation before surgery. All 32 cases were instructed to reduce the use of DDs and were observed for ≥6 months after the initial visit until the degree of esotropia stabilized, according to the policy of re-examination approximately every two months. During this observation period, if the angle of esotropia at near increased (“eat up”) to >5 prism diopters (Δ) as measured by APCT, the power of FP was changed, and this process was repeated until the angle of esotropia remained stable for ≥2 months. Finally, 13 cases who underwent prism adaptation continuously wore FP before surgery.
Eleven and 19 cases underwent graded UMRR and BMRR for the angle of esotropia measuring <25 Δ and 25Δ-50Δ, respectively. For additional 2 patient measuring 50 Δ or more of the angle of esotropia, a simultaneous three-muscle procedure of BMRR and unilateral lateral rectus resection were performed. The surgical dosage was calculated based on the formula of 3Δ/mm plus 0.5–1.0 mm in cases showing the smaller limbus-insertion distance of medial rectus muscle.20–22 All surgeries were performed under general anesthesia in patients <15 years and local anesthesia for those ≥15 years old by two experimented surgeons (TY and YY). Each case was measured postoperative alignment at 1 day, at 1 week, and every 2 months after surgery. The minimum postoperative follow-up was 6 months, with motor success after surgery considered to be alignment within 10Δ at both near and distance, and sensory success after surgery as near stereoacuity ≤60 arcsec (”).23
This study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the Japan Community Health Care Organization Chukyo Hospital (approval no. 2021030). The study protocols and data collection conformed to all local laws, and informed consent was obtained from all cases or their guardians after all study details were explained.
Statistical analyses were performed using Microsoft Excel for Mac version 16 (Microsoft Corp., Redmond, WA, USA) and StatMate version 5 (ATMS, Chiba, Japan). Numerical data were expressed as mean ± standard deviation (SD) and were compared using the Student’s t-test or Welch test. Categorical data were expressed as numbers and percentages and were compared using the χ2 test, Fisher’s exact test, and McNemar test. Statistical significance was set at p <0.05.
Results
During the entire observation period, no complications to exclude from this study were found in all cases.
All Patients
Of the 32 cases, 22 (69%) were male and 10 (31%) were female. Mean age at onset was 19.7 ± 9.2 (standard deviation) years and mean age at first visit was 22.0 ± 9.0 years. Best-corrected logMAR visual acuity was −0.07 ± 0.10 in the right eye and −0.11 ± 0.22 in the left eye and mean cycloplegic refractive error (spherical equivalents: SE) was −2.97 ± 2.39 D in the right eye and −2.84 ± 2.42 D in the left. Distant and near deviation angles at first visit were 26.5 ± 13.0 Δ and 24.6 ± 16.4 Δ, respectively, with no significant difference apparent between deviation angles (p = 0.180). No cases showed a high AC/A ratio by the heterophoria method. Mean daily time of prolonged near work with DDs was 6.3 ± 3.4 h and nine cases (28%) showed a history of excessive near work (≥8 h a day) with DDs.
Observation time before surgery from the initial visit was 1.3 ± 0.9 years and mean age at surgery was 23.3 ± 3.5 years. The distance and near deviation angles at surgery were 29.5 ± 13.8 Δ and 29.3 ± 16.5 Δ, respectively, and no significant difference was observed between the deviation angles (p = 0.844). However, significant increases in distant and near deviation angles from at the initial visit to at surgery were observed (distant: 3.0 ± 8.1, p = 0.043; near; 4.7 ± 10.3, p = 0.014). Five cases showed an increase of ≥10 Δ in both distant and near deviation angles between the initial visit and surgery. Mean ages at the initial visit and surgery for those 5 cases were 13.0 ± 5.5 years and 14.5 ± 5.1 years, respectively, representing significant differences from the 23.7 ± 8.5 years (p = 0.007) and 24.9 ± 8.6 years (p = 0.005), respectively, for the remaining 27 cases. The mean surgical total dosage was 11.0 ± 4.8 mm.
All cases were followed up after surgery between 6.0 months and 8.3 years (mean: 2.5 ± 2.0 years). Significant differences in deviation angles between distant and near were observed at 1 week after surgery (3.0 ± 4.6 Δ and 1.5 ± 3.6 Δ, p = 0.001) and at the final visit (5.8 ± 7.7 Δ and 3.5 ± 5.7 Δ, p = 0.012), respectively. Although the increase in near deviation angles between 1 week after surgery and the final visit was not significant (1.5 ± 3.6 Δ and 3.5 ± 5.7 Δ, p = 0.078), the distant increase was significant (3.0 ± 4.6 Δ and 5.8 ± 7.7 Δ, p = 0.032). However, the motor success rate remained as high from 94% (30 cases) at 1 week after surgery to 78% (25 cases) at the final visit with no significant difference (p = 0.150). Of 6 cases of motor unsuccess, 5 cases received additional surgery to achieve motor success again. Usage time for DDS in all four cases that did not maintain motor success was longer than that before surgery (6.0 ± 2.0 h vs 9.5 ± 1.5 h, p = 0.006).
Distant and near binocular responses at the initial visit were positive only in 4 cases (13%) and 7 cases (22%), respectively. However, distant and near binocular positive responses increases to 22 cases (69%) and 29 cases (91%), respectively, at 1 week after surgery (p < 0.001 each). Subsequently, distant and near positive responses highly remained in 21 cases (66%) and 27 cases (84%), respectively, at the final visit (p < 0.001 each).
Although near stereoacuity at the initial visit was positive in only 4 cases, we observed 27 cases (84%) at 1 week after surgery and 30 cases (94%) at the final visit who showed positive responses (p < 0.001 each). Moreover, the fine stereopsis (≤60”) success rates at 1 week after surgery and at the final visit were found in 47% (15 cases) and 53% (17 cases), respectively.
Comparisons in Baseline Characteristics and Parameters Between Cases with and without Prism Adaptation
Among the 32 cases, 13 (41%) underwent surgery and prism adaptation (S+P group). The remaining 19 cases (59%) underwent surgery alone (S group). The baseline characteristics of the two groups at the initial visit are listed in Table 1. Both groups were generally well balanced for age of onset, sex, best-corrected logMAR visual acuity, cycloplegic refractive error, and deviation angle, but not for initial age (S+P group: 25.8 ± 9.9 years; S group: 19.4 ± 7.4 years; p = 0.044). In the S+P group, six cases underwent UMRR and seven underwent BMRR. In the S group, five cases underwent UMRR, 12 patients underwent BMRR, and two cases underwent a simultaneous three-muscle procedure of BMR and unilateral lateral rectus resection.
 |
Table 1 Comparison of Patients with and without Prism Treatment |
Clinical evaluation outcomes are listed in Table 1. Although age at surgery was slightly lower in the S group (20.7 ± 7.5 years) than for participants in the S+P group (27.1 ± 9.8 years, p = 0.044), no significant differences in distant or near deviation angles at surgery, 1 week after surgery and the final visit were identified between groups.
Table 2 shows sensory and motor success rates in both groups. No significant differences in binocular response at near and at distant were seen between groups at the initial visit, 1 week after surgery, and the final visit. Although near stereoacuity was significantly better in the S+P group than in the S group at surgery (p = 0.036), near stereoacuity at initial visit, 1 week after surgery and the final visit were also generally well balanced between groups (Figure 1). No significant difference in final sensory success rates in the S+P group and in the S group were found (p = 0.803). Moreover, final motor success rates showed no significant difference between in both groups (p = 0.401).
 |
Table 2 Sensory and Motor Outcomes of Patients with and without Prism Treatment |
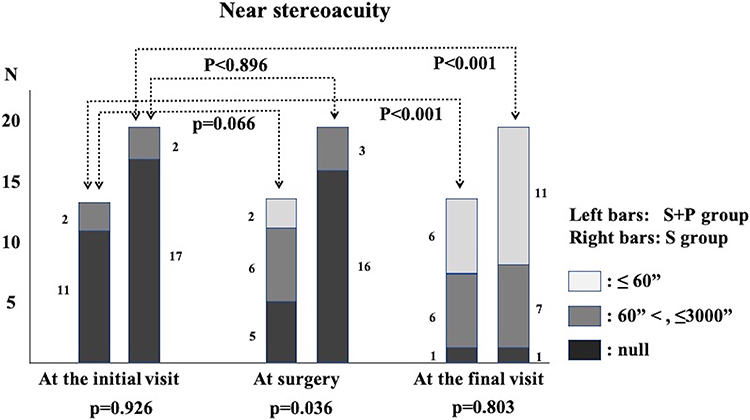 |
Figure 1 Comparisons in near stereoacuity between group treated with surgery alone and group treated with surgery and prism adaptation. Abbreviations: S+P, cases treated with surgery and prism adaptation; S, cases treated with surgery alone; “, arc seconds. Notes: Although outcomes in near stereoacuity of both groups at the last visit were significantly better than those at the initial visit, no significant differences in near stereoacuity were evident between the groups at either the initial or last visit. |
Comparisons of Motor and Sensory Status Between Initial Visit, Surgery, and Final Visit
The distant and near deviation angles in the S+P group between at the initial visit and at surgery showed no significant difference (the distant: p = 0.952 and the near: p = 0.5350). However, distant and near deviation angles in the S group were significantly increased from 27.8 ± 13.5Δ and 25.5 ± 17.1Δ at the initial visit to 33.5 ± 13.5Δ and 32.8 ± 17.5Δ at surgery (distant: p = 0.011 and near: p = 0.012).
In the S+P group, although distant and near binocular responses at the initial visit were positive in only 3 (20%) and 4 (31%) cases, respectively, positive distant and near binocular responses at surgery increased in frequency to 5 (33%) and 10 (77%) cases (p = 0.480 and p = 0.031, respectively). However, in the S group, no significant differences in distant or near binocular responses were found between the initial visit and surgery (at distance: one case (5%) and one case (5%); p = 0.480; near: three cases (16%); and one case (5%), p = 0.617).
In both groups, although a significant improvement in near stereoacuity was seen at the final visit (p < 0.001 each), no significant differences in near stereoacuity were identified between at the initial visit and at surgery (S+P group, p = 0.066; S group, p = 0.896) (Figure 1).
Discussions
Several studies have reported the surgical outcomes of AACE. Lyon et al reported good surgical outcomes for only five cases of classical types of AACE in patients aged 3–24 years24 and Lee et al also reported surgical outcomes in three cases of 12 AACE related to excessive smartphone use.8 However, those articles reported surgical outcomes from few cases of AACE. Therefore, whether surgical interventions for AACE offer favorable postoperative motor and sensory outcomes has not been established.
Cai et al reported favorable surgical outcomes in 44 cases of AACE, including 14 cases associated with presumed prolonged use of DDs.20 In that series, postoperative angles of deviation at distance and near were 0.8 ±1.6Δ and 0.7 ±1.8Δ, respectively, and 30 cases (68%) showed good stereoacuity (≤60)”, similar to our results (p = 0.182). Kim and Noh also reported a favorable surgical motor success (alignment ≤8Δ) rate of 79% and a sensory success (stereoacuity ≤60”) rate of 50% at the final follow-up in 24 cases of AACE,21 in which 18 cases underwent UMR and lateral rectus resection, and six cases underwent BMR. In our study, the overall motor success rate was 81% and good stereoacuity (≤60)” rate was 53% at the final visit. Moreover, measurable near stereoacuity was obtained in 30 cases (94%) with surgical intervention, regardless of preoperative prism adaptation.
Although Bielschowsky speculated that as one cause of AACE, despite uncorrected myopia, excessive near work might lead to ill‐balanced forces of the eyes for convergence and divergence, and that esotropia may occur due to increased tonus of the medial rectus muscles,5 the exact mechanism of AACE associated with prolonged use of DDs has not been fully established. Campos reported that reduced divergent fusion amplitude was detected in Burian-Franceschetti-type AACE, while Bielschowsky-type AACE showed a convergence spasm.25 Ali et al recently suggested that cases with esophoria have enhanced divergence amplitudes to suppress manifest esotropia and that diplopia and manifest esotropia could occur in cases of failing the divergence amplitude to overcome esophoria in adulthood as the underlying mechanism of AACE.26 The recession procedure of the medial rectus muscle may relieve convergence spasm or reduce the accommodation amplitude, resulting in increased divergence amplitudes.25–27 In the present study, we excluded cases wearing improper or undercorrected glasses to differentiate Bielschowsky-type AACE from this study type of AACE and we selected recession of the medial rectus muscle as the basic procedure for AACE associated with prolonged usage of DDs. Based on the favorable surgical results of 94% motor success rate at 1 week after surgery and 78% motor success rate at the final visit, the mechanism underlying AACE associated with prolonged usage of DDs was thought to be as speculated above, and the mechanism of AACE associated with prolonged usage of DDs may be similar to that of Bielschowsky-type AACE. If this mechanism is appropriate, the prolonged use of DDs may trigger the development of AACE, and one of the major causes of this study type of AACE may be poor ability to normalize or minimize enhanced divergence amplitudes. The further investigations will be necessary to get to the bottom of those questions.
To achieve better motor and sensory outcomes in surgical interventions for AACE associated with presumed intensive near work with DDs, some studies have recommended prism adaptation test or correction therapy before surgery. In 2020, Yilmaz et al reported good surgical results for 27 cases of AACE only associated with presumed intensive near work with DDs.10 They performed surgery based on the maximum amount of prism to neutralize deviation at near and distance after approximately 30 min of prism adaptation and recommended surgical dosage based on the prism-adapted angle as a safer approach than arbitrary augmentation for patients with AACE. However, they did not compare the surgical results between patients with and without prismatic correction for AACE associated with prolonged near work with DDs. In 2020, Zhang et al reported comparative results for the therapeutic effects of surgery following prism treatment versus surgery alone in cases of AACE.19 Among the 46 cases, 26 underwent additional prism treatment before surgery (S+P group), and the remaining 20 cases were treated with surgery alone (S group), as in our report. Although no significant differences in motor success (≤10Δ) rate were observed between approaches at 12 months post-treatment (96% vs 90%, p > 0.05), the number of cases showing central near stereoacuity (≤60) “was significantly higher in the S+P group (85%) than in the S group (55%) at 12 months post-treatment. In our results, no significant differences in near stereoacuity were found between the S+P and S groups at the final visit (46% vs. 58%, respectively; p = 0.803), reflecting a lack of therapeutic effects of surgery following prism treatment on the outcomes of near stereoacuity. One reason for such sensory outcomes may be differences in the type of AACE. Zhang et al reported 21 cases of Burian-Franceschetti type and 25 cases of Bielschowsky type,19 and found that 19% of the S+P group and 15% of the S group were preoperatively positive for central near stereopsis. However, in our report, none of the cases in either group showed near stereopsis ≤60” at the initial visit. The destruction of sensory functions in cases of AACE related to prolonged near work with DDs could be worse than in cases of historical types.
In this study, no significant differences in sensory or motor outcomes for AACE related to prolonged near work with DDs were observed between groups undergoing surgical intervention with or without prism treatment. However, although cases undergoing surgical intervention with prism treatment showed no significant differences in the angle of esotropia between the initial visit and surgery, distant and near deviation angles in cases treated with surgery alone increased significantly from 27.8 ± 13.5Δ at the initial visit to 33.5 ± 13.5Δ at surgery and from 25.5 ± 17.1Δ to 32.8 ± 17.5Δ, respectively (p = 0.011 and p = 0.012, respectively). In cases treated with surgery alone, binocular responses and near stereoacuity were so poor that the increase in deviation angles could not be reduced or minimized. In general, AACE occurs after complete development of binocular function, and some potential for good sensory recovery may persist after the occurrence of esodeviation. Alignment control with prism treatment may thus facilitate the recovery of binocularities to reduce or minimize increases in deviation angles, even in AACE related to prolonged near-work with DDs. For those speculations, further investigations will be necessary for better surgical outcomes of AACE and the etiology of AACE related to prolonged near-work with DDs.
This study had some limitations. First, the sample size of our study was small. Second, the confirmation of the daily time of prolonged near work with DDs and the type of equipment DDs used in this study were based on self-reports of all cases, as in previous reports.8–14,26 The self-report method may be less accurate with statistical processing. Recently, Iimori et al reported the clinical findings of acute acquired comitant esotropia in young 42 patients and found a positive history of excessive near work in their cases.28 However, they did not define the daily time of excessive near work, and their qualitative judgment of excessive near work was based only on self-reports. For retrospective clinical investigations, this disadvantage of clinical findings based on self-reports is considered to be within the allowable error ranges. Third, the best timing for surgery for this type of AACE has yet to be established. Our results showed no differences in the angle of esotropia among patients undergoing surgery and prism treatment for 2.7 years between the initial visit and at surgery. Surgical intervention may be recommended soon after the application of prism treatment. However, the age at the initial visit and at surgery in patients undergoing surgery and prism treatment were significantly greater than those in patients treated with surgery alone. Moreover, some younger patients showed an increase of 10Δ or more in the angle of esotropia near and distant during the observation period. Given these findings, the safest age for prompt surgery to control the increase in esotropia angle remains unclear. Further investigations are necessary to clarify these limitations. We believe that an observation period to confirm stable deviation angles is necessary for optimal motor and sensory outcomes after surgery in cases of AACE related to prolonged near work with DDs.
Conclusions
No significant differences in binocular response at near and at distant were seen between groups at the initial visit, 1 week after surgery, and the final visit. Although near stereoacuity was significantly better in the S+P group than in the S group at surgery, near stereoacuity at initial visit, 1 week after surgery and the final visit were also generally well balanced between 2 groups. Final motor success rates also showed no significant difference. Therefore, favorable motor and sensory outcomes were achieved with surgical intervention for AACE related to prolonged use of DDs, regardless of preoperative prism adaptation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author [TY], upon reasonable request.
Acknowledgments
We would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any grants or funding.
Disclosure
The authors declare that they have no conflicts of interest in this study.
References
1. Mohney BG. Common forms of childhood strabismus in an incidence cohort. Am J Ophthalmol. 2007;144:465–467. PMID: 17765436. doi:10.1016/j.ajo.2007.06.011
2. von Noorden GK, Campos EC. Esodeviations. In: Binocular Vision and Ocular Motility: Theory and Management of Strabismus.
3. Clark AC, Nelson LB, Simon JW, Wagner R, Rubin SE. Acute acquired comitant esotropia. Br J Ophthalmol. 1989;73:636–638. PMID: 2765443. doi:10.1136/bjo.73.8.636
4. Burian HM, Miller JE. Comitant convergent strabismus with acute onset. Am J Ophthalmol. 1958;45:55–64. PMID: 13520873. doi:10.1016/0002-9394(58)90223-x
5. Bielschowsky A. Das Einwartfschien der Myopia. Dtsch Ophthalmol Gesell. 1922;43:245–248.
6. Hoyt CS, Good WV. Acute onset concomitant esotropia: when is it a sign of serious neurologic disease? Br J Ophthalmol. 1995;79:498–501. PMID: 7612566. doi:10.1136/bjo.79.5.498
7. Buch H, Vinding T. Acute acquired comitant esotropia of childhood: a classification based on 48 children. Acta Ophthalmol. 2015;93:568–574. PMID: 25989866. doi:10.1111/aos.12730
8. Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive smartphone use. BMC Ophthalmol. 2016;16:37. PMID: 27061181. doi:10.1186/s12886-016-0213-5
9. Mehta A, Greensher JE, Dahl GJ, Miller KE. Acute onset esotropia from excessive smartphone use in a teenager. J Pediatr Ophthalmol Strabismus. 2018;55:e42–e44. PMID: 30571837. doi:10.3928/01913913-20181017-01
10. Yilmaz PT, Fatihoglu ÖU, Sener E. Acquired comitant esotropia in children and young adults: clinical characteristics, surgical outcomes, and association with presumed intensive near work with digital displays. J Pediatr Ophthalmol Strabismus. 2020;57:251–256. PMID: 32687210. doi:10.3928/01913913-20200422-02
11. Vagge A, Giannaccare G, Scarinci F, et al. Acute acquired concomitant esotropia from excessive application of near vision during the COVID-19 lockdown. J Pediatr Ophthalmol Strabismus. 2020;57:e88–e91. PMID: 33090234. doi:10.3928/01913913-20200828-01
12. Wu Y, Dai S, Liang F, Sun B. Excessive smartphone use may cause acute acquired comitant esotropia. J Ophthalmol Vision Res. 2020;2:1–6.
13. Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: digital eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69:140–144. PMID: 33323599. doi:10.4103/ijo.IJO_2535_20
14. Mohan A, Sen P, Mujumdar D, Shah D, Jain E. Series of cases of acute acquired comitant esotropia in children associated with excessive online classes on smartphone during COVID-19 pandemic; digital eye strain among kids (DESK) study-3. Strabismus. 2021;29:163–167. PMID: 34223812. doi:10.1080/09273972.2021.1948072
15. Pietrobelli A, Fearnbach N, Ferruzzi A, et al. Effects of COVID‐19 lockdown on lifestyle behaviors in children with obesity: longitudinal study update. Obes Sci Pract. 2021:1–4. PMID: 32352652. doi:10.1002/osp4.581
16. Wong CW, Tsai A, Jonas JB, et al. Digital screen time during the COVID-19 pandemic: risk for a further myopia boom? Am J Ophthalmol. 2020;223:333–337. PMID: 32738229. doi:10.1016/j.ajo.2020.07.034
17. Bahkir FA, Grandee SS. Impact of the COVID-19 lockdown on digital device-related ocular health. Indian J Ophthalmol. 2020;68:2378–2383. PMID: 33120622. doi:10.4103/ijo.IJO_2306_20
18. Savino G, Colucci D, Rebecchi MT, Dickmann A. Acute onset concomitant esotropia: sensorial evaluation, prism adaptation test, and surgery planning. J Pediatr Ophthalmol Strabismus. 2005;42:342–348. PMID: 16382558. doi:10.3928/01913913-20051101-02
19. Zhang P, Zhang Y, Gao L, Yang J. Comparison of the therapeutic effects of surgery following prism adaptation test versus surgery alone in acute acquired comitant esotropia. BMC Ophthalmol. 2020;20:303. PMID: 32703185. doi:10.1186/s12886-020-01574-y
20. Cai C, Dai H, Shen Y. Clinical characteristics and surgical outcomes of acute acquired comitant esotropia. BMC Ophthalmol. 2019;19:173. PMID: 31391009. doi:10.1186/s12886-019-1182-2
21. Kim DH, Noh HJ. Surgical outcomes of acute acquired comitant esotropia of adulthood. BMC Ophthalmol. 2021;21:45. PMID: 33461540. doi:10.1186/s12886-020-01793-3
22. Yoshida T, Yagasaki T, Sato M, Awaya S. Effects of medial rectus muscle insertion on grading recession in esotropia surgery. J Eye. 1995;12:1332–1334. Japanese.
23. Birch EE, Jingyun W. Stereoacuity outcomes after treatment of infantile and accommodative esotropia. Optom Vis Sci. 2009;86:647–652. PMID: 19390468. doi:10.1097/OPX.0b013e3181a6168d
24. Lyons CJ, Tiffin PAC, Oystreck D. Acute acquired comitant esotropia: a prospective study. Eye. 1999;13:617–620. PMID: 10696312. doi:10.1038/eye.1999.169
25. Campos EC. Why do the eyes cross? A review and discussion of the nature and origin of essential infantile esotropia, microstrabismus, accommodative esotropia, and acute comitant esotropia. J AAPOS. 2008;12:326–331. PMID: 18550403. doi:10.1016/j.jaapos.2008.03.013
26. Ali MH, Berry S, Qureshi A, Rattanalert N, Demer JL. Decompensated esophoria as a benign cause of acquired esotropia. Am J Ophthalmol. 2018;194:95–100. PMID: 30053478. doi:10.1016/j.ajo.2018.07.007
27. Hussaindeen JR, Mani R, Agarkar S, Ramani KK, Surendran TS. Acute adult onset comitant esotropia associated with accommodative spasm. Optom Vis Sci. 2014;91:46–51. PMID: 24584303. doi:10.1097/OPX.0000000000000182
28. Iimori H, Suzuki H, Komori M, Hikoya A, Hotta Y, Sato S. Clinical findings of acute acquired comitant esotropia in young patients. Jpn J Ophthalmol. 2022;66:87–93. PMID: 34655005. doi:10.1007/s10384-021-00879-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.