Back to Journals » Clinical Ophthalmology » Volume 12
Surgical outcomes associated with a sutureless drainage valve implantation procedure in patients with refractory glaucoma
Authors Pham CN, Radcliffe NM ![]() , Vu DM
, Vu DM
Received 4 September 2018
Accepted for publication 9 November 2018
Published 12 December 2018 Volume 2018:12 Pages 2607—2615
DOI https://doi.org/10.2147/OPTH.S186369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video demonstration of a completely sutureless technique for Ahmed glaucoma valve with pericardial patch graft implantation in the superotemporal quadrant of the eye.
Views: 4879
Caroline N Pham,1 Nathan M Radcliffe,1–3 Daniel M Vu2
1New York University, New York, NY, USA; 2Weill Cornell Medical College, New York, NY, USA; 3New York Eye Surgery Center, New York, NY, USA
Purpose: To evaluate the safety and efficacy profile of a sutureless procedure for drainage valve implantation with combined cataract removal and/or endoscopic cyclophotocoagulation (ECP).
Materials and methods: A retrospective case series study of consecutive surgeries for Ahmed glaucoma valve (AGV; New World Medical) implantation in a 1-year period was analyzed. The surgery was performed using a Tisseel fibrin sealant (Baxter Healthcare Corporation) in place of sutures. Some subsets within the case series also included a cataract extraction with intraocular lens (CEIOL) insertion and/or ECP (Endo Optiks) within the same procedure. Primary outcomes for this study including efficacy (IOP change, reduction in medications) and safety (complications and reoperations) were measured out to 3 years. Comparisons between subsets were made using ANOVA with post hoc Tukey’s pairwise tests.
Results: One hundred twenty-two eyes of 99 patients underwent sutureless AGV implantation surgery. Of the 122, 18 had an AGV implantation only, 46 had an AGV + CEIOL, 35 had an AGV + ECP, and 23 had an AGV + CEIOL + ECP. In total, there was a significant decrease in IOP (P<0.0001) and number of glaucoma medications (P≤0.0054) at each postoperative visit. In a one-way ANOVA, there were no significant differences in mean IOP between the different subsets of surgeries (P>0.05); 10.7% and 14.8% of eyes required a reoperation either for a complication or for uncontrolled glaucoma, respectively.
Conclusion: Sutureless valve implantation is associated with a significant reduction in IOP percentage and medication use after the procedure with a safety profile comparable with other glaucoma surgeries.
Keywords: Ahmed glaucoma valve, glaucoma surgery, tube shunt surgery
Introduction
Tube shunt implantation is an effective surgery for IOP reduction in glaucoma patients who are refractory to medication, laser treatment, or trabeculectomy.1 This option has become increasingly more common in the management of advanced glaucoma patients.2 In patients who have had cataract surgery or a failed trabeculectomy, tube shunts were shown to have a similar likelihood of maintaining a lower IOP and a lower rate of postoperative complications compared with trabeculectomy.3,4 The Tube vs Trabeculectomy (TVT) study demonstrated that overall complication rates were 39% and reoperation rates for those complications were 14% in the tube shunt arm at 3 years.4 Late complications such as tube erosion and obstruction were noted to be 5% and 3%, respectively.4,5
Tissue adhesives such as synthetic cyanoacrylate and biological fibrin sealants have been used in other ophthalmic surgeries such as pterygium and strabismus surgery to reduce operating time and suture-related complications.6 Fibrin sealant produces a more smooth closure than cyanoacrylate with less inflammation and foreign body sensation.6 The fibrin seal is created by a coagulation reaction that occurs between its precursors, fibrinogen, and thrombin.6 Few studies have reported results on using fibrin sealant in securing the tube and/or patch graft underneath the conjunctiva in tube shunt surgery.7–10 These authors have had favorable outcomes with reduced placement of anchoring sutures and a fibrin-assisted conjunctival closure.7–9 Reduced suture placement shortens surgical and healing time as well as decreases inflammation.7 Tube erosion and migration were not observed in these previous studies.7–10
To our knowledge, no study has previously reported on outcomes of a completely sutureless tube shunt surgery and patch graft implantation procedure, whereby the tube tip is placed in the anterior segment. One study analyzed the results of patients undergoing a fully sutureless glaucoma drainage valve procedure with tube tip placement in the pars plana in previously vitrectomized eyes or in eyes undergoing combined pars plana vitrectomy.11 However, their technique did not utilize a patch graft and required that eyes were vitrectomized. In this investigation, we compared outcomes that included IOP reduction (efficacy) and complications (safety) of a novel surgical technique for glaucoma tube shunt surgery via sutureless placement of the patch graft, tube plate, and tube with fibrin sealant closure in patients with and without combined cataract extraction with intraocular lens (CEIOL) insertion and/or endoscopic cyclophotocoagulation (ECP).
Materials and methods
This was a retrospective case series study of consecutive surgeries, completed between June 2014 and June 2015, in which an Ahmed glaucoma valve (AGV; New World Medical, Rancho Cucamonga, CA, USA) was implanted using an entirely sutureless technique. Patients who were refractory to IOP lowering medications were examined and treated by a glaucoma fellowship trained ophthalmologist (NMR) at a private practice in New York City. Surgery was offered to patients in whom the surgeon and patient felt that the risks of IOP lowering surgery were less than the risks of continuing on IOP lowering medications. Informed consent was obtained for each patient prior to proceeding with surgery. All surgical cases that included AGV implantation were considered for inclusion in this study. Some surgeries also included combined CEIOL insertion and/or ECP (Endo Optiks, Little Silver, NJ, USA) if determined to be appropriate by the surgeon. Each patient was followed postoperatively at 1 day, 1 week, 1 month, 3 months, 6 months, and then annually. New York University Langone Medical Center Institutional Review Board exemption for a retrospective study of glaucoma surgical outcomes was obtained, and this study was performed in adherence with the Declaration of Helsinki.
All cases underwent standard patient preparation. Patients underwent monitored anesthesia care and a retrobulbar block in the surgical eye. After the predetermined (usually superotemporal) quadrant was inspected for healthy conjunctiva, a conjunctival limbal-based peritomy was performed ~5 mm posterior to the limbus, with a limited dissection to allow a slightly undersized sub-Tenon’s pocket to capture the plate (Video 1). After priming, the glaucoma implant was placed into the posterior pocket of the peritomy >8 mm posterior to the limbus. The plate was tugged to ensure that it would not come forward. A 5-mm tunnel was constructed, which provided additional resistance to help hold the tube in place. The glaucoma implant tube tip was then placed into the opening with smooth forceps. A pericardial patch graft of appropriate thickness and size was placed over the tube, and Tisseel fibrin sealant (Baxter Healthcare Corporation, Deerfield, IL, USA) was applied over the conjunctival incision and closed using toothed forceps. Subconjunctival steroid and antibiotic were administered in the area surrounding the surgical site.
In patients who had combined CEIOL insertion, standard cataract extraction with temporal clear corneal incision and phacoemulsification was performed prior to conjunctival dissection and insertion of the AGV. After the CEIOL portion of the surgery, viscoelastic was used to inflate the ciliary sulcus if the AGV tube was chosen to be inserted in the sulcus space. If patients had combined ECP, then ECP was performed following AGV insertion with a setting of 0.2–0.3 Watts per application directed at the ciliary processes for 180–360 degrees. In such cases, the use of the endoscope also provided confirmation of correct placement of the AGV tube in the ciliary sulcus.
Data collection including patient demographics, operative complications and findings, and postoperative measurements were recorded by chart review. Prior to surgery, each patient underwent a comprehensive glaucoma evaluation. Baseline IOP measurements by Goldmann applanation tonometry and preoperative number of glaucoma medications were recorded based on the average from each patient’s last three visits prior to AGV implantation surgery. Specific glaucoma diagnosis was determined by clinical assessment and ICD documentation. Each operative note was reviewed and included the location of the tube shunt implant, intraocular location of tube tip placement, as well as any intraoperative complications. All patients were followed up postoperatively to monitor for IOP changes, number of medications, and any adverse events.
Primary outcomes for this study including efficacy (IOP change, number of medications) and safety (complications and reoperations) were measured out to 3 years. Patients who had a reoperation due to complications were excluded from further efficacy and safety analysis after the reoperation. Patients who had a reoperation for uncontrolled glaucoma were excluded from further analysis of IOP change, number of medications, and reoperation rate for uncontrolled glaucoma after the time point of reoperation. However, safety monitoring was continued on those patients for the duration of the study. Any procedures performed after AGV implantation where a patient went back to the operating room or underwent transscleral cyclophotocoagulation in the clinic were considered reoperation. Other interventions in the office such as selective laser trabeculoplasty, wound burping, or anterior chamber reformation were not counted as a reoperation. In a subgroup analysis, patients were divided into groups based on whether an AGV was placed with or without a combined CEIOL insertion and/or ECP. Baseline characteristics and postoperative outcomes were compared using paired t-tests with a 0.05 level of significance. Comparisons between subgroups were made using ANOVA and post hoc Tukey’s pairwise tests. All statistical analyses were conducted with Stata 14 (StataCorp LP, College Station, TX, USA).
Results
A total of 122 eyes from 99 participants were included in this study with a mean age of 68.3±10.0 years. Patient demographics and study characteristics are presented in Table 1. Of the 122, 18 had AGV implantation (A group) only, 46 had AGV implantation with CEIOL insertion (CA group), 35 had AGV implantation with ECP (AE group), and 23 had AGV implantation with CEIOL insertion and ECP (ACE group). Mean follow-up time was 25.8±14.7 months from surgery.
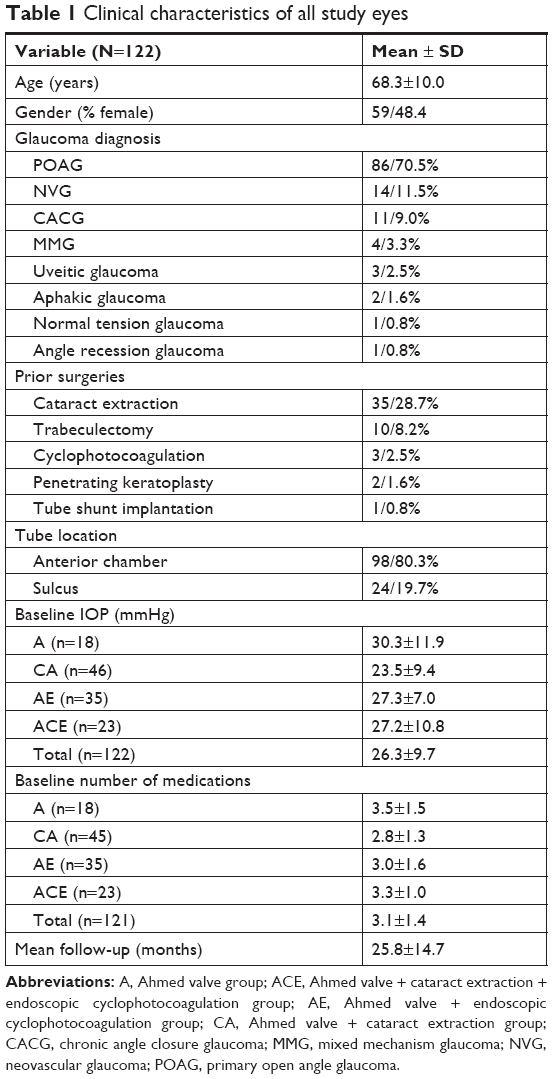 | Table 1 Clinical characteristics of all study eyes |
Overall, the mean baseline IOP for all participants was 26.3±9.7 mmHg and initial number of glaucoma drops was 3.1±1.4. Following implantation of the tube shunt, mean postoperative IOP (mean percent IOP reduction) at 1 day was 13.8±11.7 mmHg (44.6%±46.8%), 12.7±7.3 mmHg (47.1%±33.3%) at 1 week, 16.9±6.1 mmHg (29.4%±29.0%) at 1 month, 16.1±4.8 mmHg (29.4%±25.3%) at 3 months, 16.0±4.6 mmHg (27.7%±25.2%) at 6 months, 15.3±5.3 mmHg (31.5%±33.4%) at 1 year, 15.1±4.0 mmHg (32.6%±25.4%) at 1.5 years, 14.4±3.3 mmHg (35.4%±20.5%) at 2 years, 14.8±4.3 mmHg (32.8%±23.9%) at 2.5 years, and 15.8±5.5 mmHg (28.2%±27.4%) at 3 years. Table 2 summarizes the mean postoperative IOP values for each visit (P<0.0001). A decrease in number of glaucoma medications at each postoperative visit was also statistically significant compared with baseline (P≤0.0054; Table 3). By 2 and 3 years, the mean number of drops was 2.0±1.2 and 2.2±1.3, respectively (P<0.0001 and P=0.0021).
 | Table 2 Mean IOP at each postoperative follow-up visit compared with baseline |
 | Table 3 Number of glaucoma medications at postoperative follow-up visits compared with baseline |
A subgroup analysis comparing each surgery type was included in order to determine if there were any differences in mean IOP or number of glaucoma medications. In the subgroup analysis, there were no significant differences for mean IOP at baseline and postoperatively among the surgical groups regardless of whether an AGV implantation was combined with another procedure (CEIOL insertion and/or ECP) using one-way ANOVA analysis (P>0.05, Table 2). Table 3 shows that the comparison between number of glaucoma medications in each subgroup was not significantly different at each visit (P>0.1) except at 1 month, 3 months, 6 months, 2.5 years, and 3 years (P<0.05). In post hoc Tukey’s pairwise analysis, there was a statistical difference in the number of glaucoma medications between the CA and ACE subgroups at 1 month (0.7±1.1 vs 1.7±1.6, P=0.045), between the CA and A subgroups at 3 months (1.3±1.1 vs 2.5±1.2, P=0.019), and between the CA and AE subgroups at 6 months (1.4±1.1 vs 2.5±1.8, P=0.029). At 3 years, there was a significant difference between number of medications between the CA and AE subgroups (1.5±1.2 vs 2.9±1.3, P=0.023), as well as CA and ACE subgroups (1.5±1.2 vs 3.3±0.5, P=0.049). There was no statistical difference in the post hoc Tukey’s test at 2.5 years because the sample size was not large enough to detect a difference between four subgroups.
Eighteen of 122 eyes (14.8%) required reoperation due to uncontrolled glaucoma in the first 3 years (Table 4). Of the 18, 11 eyes underwent micropulse transscleral cyclophotocoagulation (Iridex Corp, Mountain View, CA, USA). The other seven eyes had a reoperation that involved an intraocular surgery: one had an AGV revision with bleb needling and ECP at 2.5 months, one had an AGV revision with bleb needling and a second AGV implantation at 2 months, one had a second AGV implantation only at 17 months, one had a combined tube trimming with Trab360 ab interno trabeculotomy (Sight Sciences, Menlo Park, CA, USA) at 1 month, one required a Baerveldt tube shunt (BVT; Abbott Medical Optics, Inc, Santa Ana, CA, USA) at 30 months, and the last required a Xen gel stent (Allergan, Inc, Dublin, Ireland) at 32 months.
 | Table 4 Interventions or reoperations following initial surgery for uncontrolled glaucoma |
In our study, 52 of 122 eyes (42.6%) developed at least one complication in the first 3 years after surgery. The most common complications were posterior capsular opacification (26.1%; adjusted for eyes in CA and ACE subgroups only), followed by hyphema (18.0%) and shallow anterior chamber (8.2%, Table 5). Most complications were mild and resolved with observation, medical management, or with office-based procedures. There were five (4.1%) cases of recurrent iritis, three (2.5%) cases of iris obstruction, and one (0.8%) case of dysesthesia, which were not associated with tube or plate migration on examination. There were five (4.1%) cases of corneal edema that persisted beyond 3 months postoperatively in patients without a prior history of endothelial disease, but four of those cases resolved over time. One of the cases of corneal edema was in a patient with concomitant tube erosion and shallow anterior chamber, but the corneal edema and shallow anterior chamber resolved after reoperation for tube erosion at 4 months without the need for corneal surgery.
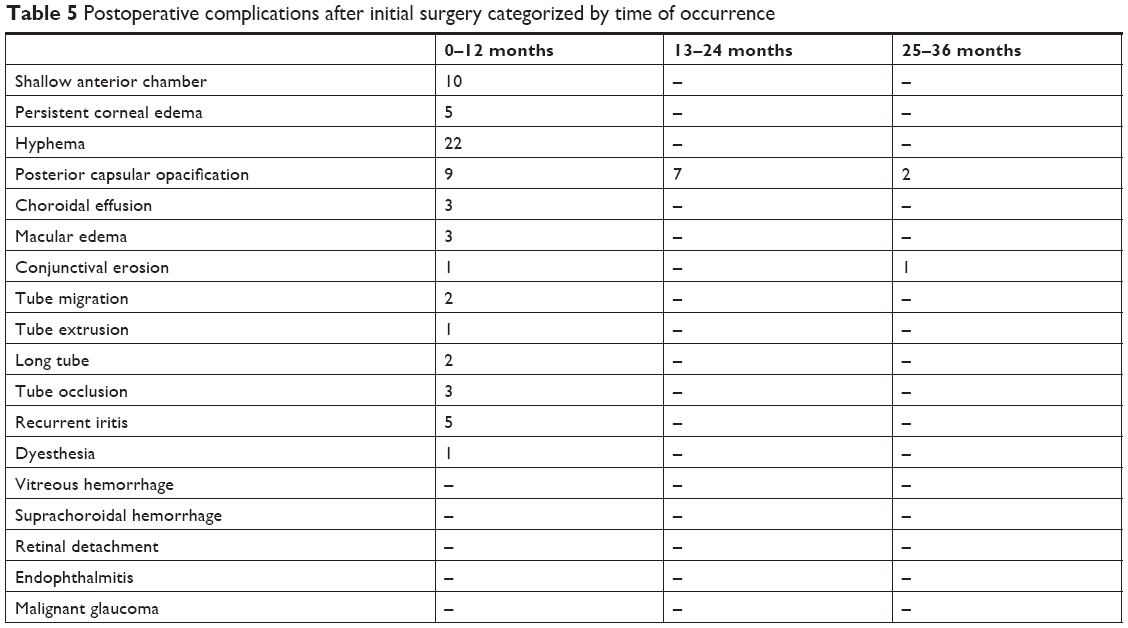 | Table 5 Postoperative complications after initial surgery categorized by time of occurrence |
Thirteen eyes (10.7%) returned to the operating room within the first 3 years due to a complication (Table 6). Most reoperations for complications occurred within the first year. Two out of the 13 patients had a reoperation for conjunctival erosion: one was within the first year and the other was within 3 years. Two patients had a revision due to anterior migration of the tube (one at 5 months and the other at 11 months). One other patient developed a tube extrusion, requiring reoperation at 9 months. Two patients had a combination case of prophylactic tube trimming with another procedure due to the appearance of a long tube in the anterior segment. Of those two, one patient was already planned for a pars plana vitrectomy due to severe proliferative diabetic retinopathy, and it was decided at that time that a combined tube trimming would be performed at 9 months, while the other had a combined tube trimming with Trab360 trabeculotomy at 1 month, as mentioned above. Another patient had a history of penetrating keratoplasty and corneal edema prior to initial AGV implantation with ECP, and later required a Descemet’s stripping endothelial keratoplasty at 2 months out. There were no cases of diplopia or reoperation for strabismus.
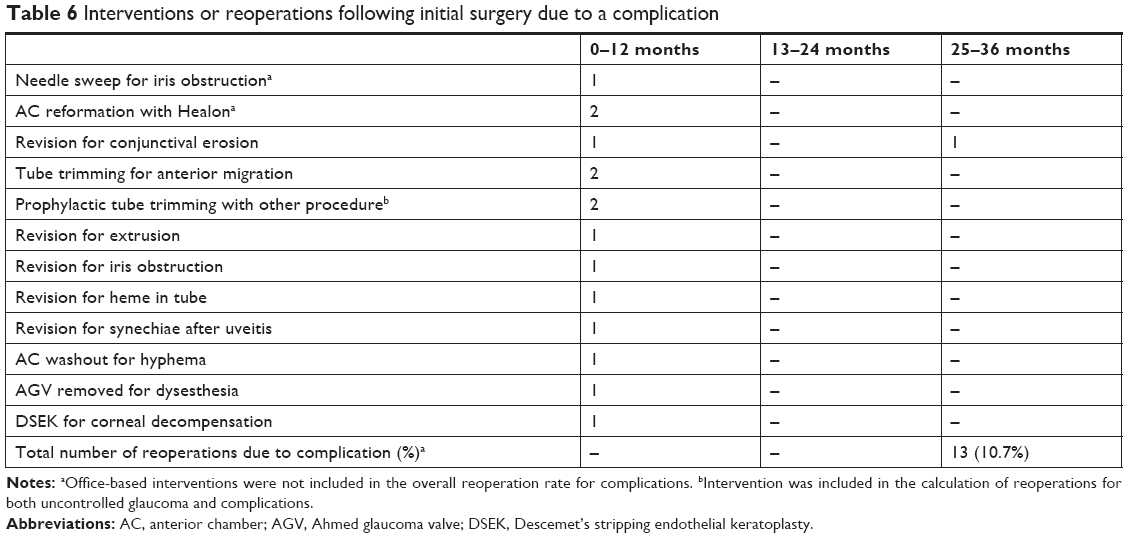 | Table 6 Interventions or reoperations following initial surgery due to a complication |
Discussion
Sutureless placement of an AGV with fibrin sealant closure is associated with comparable outcomes vs the traditional technique for tube shunt placement. In this novel technique, the valve plate, tube, and patch graft are surgically secured into the eye through a careful, modified wound construction and sealant-based conjunctival wound closure without the use of anchoring or closing sutures. In this study population, there was a significant decrease in IOP and glaucoma medications used in the overall study at each postoperative visit compared with baseline. This group had a high mean baseline IOP that was refractory to glaucoma medications prior to surgery (Table 1). Furthermore, the subgroup analysis showed that sutureless placement of the tube shunt with or without combination CEIOL insertion and/or ECP had no significant differences in IOP at each visit. However, patients who had tube shunt surgery with CEIOL insertion tended to require less medications than another subgroup at half of the measured time points (Table 3). Performance of a sutureless technique reduces the overall number of steps in tube shunt implantation and is a safe procedure with complication rates similar to previous multicenter studies that have investigated the long-term outcomes of tube shunt implantation.4,12,13
Cumulatively through 3 years, reoperation was needed in 10.7% of eyes due to complications and in 14.8% of eyes due to uncontrolled glaucoma. In the Ahmed Baerveldt Comparison (ABC) study, the reoperation rate at 3 years was 11.0% for complications and 14.5% for worsening glaucoma in patients who had an AGV surgery.12 In the Ahmed vs Baerveldt (AVB) study, 11.3% of patients required an additional glaucoma surgery after initial AGV surgery.13 In our series, 11 of the 18 patients who had reoperations for uncontrolled glaucoma received micropulse transscleral cyclophotocoagulation, which is considered less invasive than intraocular surgery. Also, our cumulative complication rates at 3 years was 42.6% of total eyes, which is similar to other studies.12,13 The ABC study states that 44.7% of patients who had AGV surgery developed a late complication between 3 months and 3 years, while the AVB study reports a complication rate of 51.6% within 3 years. In our study, most complications resolved with observation, medical management, or office-based procedures.
The use of fibrin sealants in surgical conjunctival closure has been performed successfully in other procedures like pterygium surgery for over a decade.14,15 Kahook and Noecker found that IOP reduction and number of drops were similar postoperatively in patients who had suture-based closure vs Tisseel sealant closure of a BVT implant with a sutured-in plate and patch graft.7 They also reported that surgical times and level of conjunctival inflammation were statistically lower in the fibrin-sealed group. Although that was not a measured outcome in our study, we observed that surgery time, healing time, postoperative patient discomfort, and inflammation were decreased in completely sutureless AGV implantation. Additionally, sutures can be a site of irritation for the patient and are possible sites for infection and tube erosion.7,16,17 Fibrosis from sutures may additionally lead to inflammation and scarring in the subconjunctival space. In one study involving AGV surgeries with reduced anchoring sutures and fibrin-sealed wound closure, there were no cases of tube erosion or conjunctival exposure at 2 years.8 In our study, there were two cases (1.6%) of conjunctival erosion at 3 years. There were five cases (4.7%) of erosion in the TVT study and two cases (1.5%) of erosion in the ABC study at 3 years, as well as four cases (3.2%) of erosion in the AVB study at 1 year. In order to ensure that the conjunctiva is sealed at the end of our cases, subconjunctival steroid and antibiotic are injected near the region of the tube shunt with an appreciable bleb rise without leak from the closed wound.
To our knowledge, all previous studies that have investigated reduced suture placement and/or fibrin sealant closure have had no cases of tube or plate mobilization.7–10 One study investigated outcomes for cyanoacrylate-sealed AGVs without any sutures or patch graft and with tube insertion into the pars plana in previously vitrectomized patients or in patients with combined pars plana vitrectomy.11 Although there were only 17 eyes in that study, there were no reported cases of plate migration. In a case series that identified three patients with AGVs implanted under traditional suturing technique, the authors noted dynamic movement of the tube associated with eye movements, initially observed between 6 months and 7 years after surgery.18 They hypothesized that dynamic movement of the plate could potentially occur due to separation of the plate from the sclera because of suture loosening or from fibrosis after other surgeries. In our study, there were two cases of tube trimming for anterior migration (1.6%) and one case of tube extrusion that required revision (0.8%) in the first 3 years. In two other cases, prophylactic tube trimming was performed in combination with another procedure due to the appearance of a long tube in the anterior segment (1.6%), though plate migration was not observed. Of these five patients, there was no apparent association with having undergone a combination procedure as two cases were from the A subgroup, two cases were from the CA subgroup, and one case was from the ACE subgroup. None of these patients had a history of uveitis or prolonged postoperative inflammation. While tube migration was not mentioned as a complication in the ABC study, the authors reported reoperations in their AGV arm involving tube repositioning (n=1, 0.9%), tube extension (n=2, 1.8%), and explantation for extrusion (n=1, 0.9%) at 3 years.11 We believe that, in our technique, the placement of the AGV plate posterior to the equator allows for the orbit’s normal anatomy to prevent the anterior migration of the plate. Additionally, because the tube shunt is not sewn in, we believe that the plate will rest in a position with least force against the extraocular muscles and thus should have less effect on diplopia. No cases in this study had any reported diplopia. In the ABC study, 6.3% and 11.9% of patients with AGVs developed diplopia at 1 year and 3 years, respectively.12,19
Although this study was designed to evaluate the safety and efficacy of sutureless AGV implantation, a subgroup analysis of different combinations of AGV surgery with CEIOL insertion and/or ECP was undertaken to identify whether significant differences in IOP and number of medications existed inside the overall group. Although postoperative IOP was not significantly different, the CA subgroup tended to require less medications than the other three subgroups at various time points, including the ACE subgroup at 1 month and 3 years. Although it was not statistically different, baseline IOP and number of medications were slightly lower in patients who underwent AGV + CEIOL surgery, which may account for differences in treatment response in the postoperative subgroup analysis. Retrospective studies have found that AGV + CEIOL surgery reduces IOP and number of medications after surgery.20,21 To our knowledge, there have been no comparative studies between AGV surgery alone vs combined AGV + CEIOL insertion. A recent prospective study has compared BVT surgery alone with BVT + CEIOL insertion and found that patients who underwent BVT + CEIOL insertion tended to have higher postoperative IOP.22 No prior studies in the literature have investigated outcomes of combined AGV + ECP or combined AGV + CEIOL + ECP surgery. Further larger studies involving combined procedures with AGV implantation vs AGV implantation alone will be needed to compare their IOP lowering effect.
The present study is not without limitations. The retrospective nature of this study implies that the associations found herein do not mean causation. While the authors suspect that patient comfort and wound healing were better, this would require a prospective study with specific endpoints and a control to measure this outcome. Also, given the retrospective nature, data were collected by chart review for each patient visit, and therefore reported information did not follow a standardized study intake. Future studies may benefit from more quantitative analyses to investigate whether there is any tube shunt migration using anterior segment optical coherence tomography of the tube position or angle. This study population included consecutive surgical patients from a busy urban private practice who were referred to a glaucoma specialist because medical therapy already failed. Therefore, this study may have generalizability to advanced glaucoma patients in a community or urban setting. All glaucoma tube shunts in this study were AGVs, and therefore, our observations may not apply to other glaucoma drainage devices due to their different designs. AGVs, unlike BVTs, do not have wings that are placed under the extraocular muscles, which may mean lower risk of migration in BVTs. Since this was a case series study, a case–control comparison could not be made directly between sutureless and traditional suturing methods. However, the IOP reduction, number of medications, and complications were similar among this population vs other multicenter studies that have previously investigated efficacy and safety of tube shunt implantation.
Conclusion
In this study, an entirely sutureless glaucoma tube shunt implantation technique with fibrin sealant closure had statistically significant reduction in IOP and glaucoma medications out to 3 years. Postoperative complications and number of reoperations due to uncontrolled IOP or complications including erosion and tube positioning were similar to those reported in previous multicenter studies that investigated glaucoma drainage devices. There is the need for further investigations into the long-term complications of sutureless glaucoma tube shunt surgery since complications such as erosion and migration can be late-onset. Also, in this study, we report a subgroup analysis on outcomes for sutureless tube shunt surgery combined with either CEIOL insertion and/or ECP, in which there were no statistical differences in IOP reduction between groups. Thus, sutureless glaucoma tube shunt surgeries could represent a potential evolution in the refinement of this surgical method.
Disclosure
The authors report the following financial relationships: NMR is a consultant for New World Medical, Iridex Corporation, Allergan, Inc., Endo Optiks, Inc., and Sight Sciences. None of these organizations had any role in the design or conduct of this study. The other authors report no conflicts of interest in this work.
References
Minckler DS, Francis BA, Hodapp EA, et al. Aqueous shunts in glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2008;115(6):1089–1098. | ||
Arora KS, Robin AL, Corcoran KJ, Corcoran SL, Ramulu PY. Use of various glaucoma surgeries and procedures in medicare beneficiaries from 1994 to 2012. Ophthalmology. 2015;122(8):1615–1624. | ||
Gedde SJ. Results from the tube versus trabeculectomy study. Middle East Afr J Ophthalmol. 2009;16(3):107–111. | ||
Gedde SJ, Schiffman JC, Feuer WJ, et al. Three-year follow-up of the tube versus trabeculectomy study. Am J Ophthalmol. 2009;148(5):670–684. | ||
Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814. | ||
Panda A, Kumar S, Kumar A, Bansal R, Bhartiya S. Fibrin glue in ophthalmology. Indian J Ophthalmol. 2009;57(5):371–379. | ||
Kahook MY, Noecker RJ. Fibrin glue-assisted glaucoma drainage device surgery. Br J Ophthalmol. 2006;90(12):1486–1489. | ||
Quaranta L, Riva I, Floriani IC. Outcomes of using a sutureless bovine pericardial patch graft for Ahmed glaucoma valve implantation. Eur J Ophthalmol. 2013;23(5):738–742. | ||
Zeppa L, Romano MR, Capasso L, Tortori A, Majorana MA, Costagliola C. Sutureless human sclera donor patch graft for Ahmed glaucoma valve. Eur J Ophthalmol. 2010;20(3):546–551. | ||
Choudhari NS, Neog A, Sharma A, Iyer GK, Srinivasan B. Our experience of fibrin sealant-assisted implantation of Ahmed glaucoma valve. Indian J Ophthalmol. 2013;61(1):23–27. | ||
García-Delpech S, Sanz-Marco E, Martinez-Castillo S, et al. Ahmed valve, suture-less implantation: a new approach to an easier technique. J Glaucoma. 2013;22(9):750–756. | ||
Barton K, Feuer WJ, Budenz DL, et al. Three-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2014;121(8):1547–1557. | ||
Christakis PG, Tsai JC, Kalenak JW, et al. The Ahmed versus Baerveldt study: three-year treatment outcomes. Ophthalmology. 2013;120(11):2232–2240. | ||
Uy HS, Reyes JM, Flores JD, Lim-Bon-Siong R. Comparison of fibrin glue and sutures for attaching conjunctival autografts after pterygium excision. Ophthalmology. 2005;112(4):667–671. | ||
Karalezli A, Kucukerdonmez C, Akova YA, Altan-Yaycioglu R, Borazan M. Fibrin glue versus sutures for conjunctival autografting in pterygium surgery: a prospective comparative study. Br J Ophthalmol. 2008;92(9):1206–1210. | ||
Bayraktar Z, Kapran Z, Bayraktar S, Acar N, Unver YB, Gök K. Delayed-onset streptococcus pyogenes endophthalmitis following Ahmed glaucoma valve implantation. Jpn J Ophthalmol. 2005;49(4):315–317. | ||
Huddleston SM, Feldman RM, Budenz DL, et al. Aqueous shunt exposure: a retrospective review of repair outcome. J Glaucoma. 2013;22(6):433–438. | ||
Law SK, Coleman AL, Caprioli J. Dynamic tube movement of Ahmed glaucoma valve. J Glaucoma. 2009;18(8):628–631. | ||
Budenz DL, Barton K, Feuer WJ, et al. Treatment outcomes in the Ahmed Baerveldt Comparison Study after 1 year of follow-up. Ophthalmology. 2011;118(3):443–452. | ||
Rai AS, Shoham-Hazon N, Christakis PG, Rai AS, Ahmed IIK. Comparison of the Ahmed and Baerveldt glaucoma shunts with combined cataract extraction. Can J Ophthalmol. 2018;53(2):124–130. | ||
Kwon J, Sung KR. Factors associated with outcomes of combined phacoemulsification and ahmed glaucoma valve implantation. Korean J Ophthalmol. 2018;32(3):211–220. | ||
El Wardani M, Bergin C, Bradly K, Sharkawi E. Baerveldt shunt surgery versus combined Baerveldt shunt and phacoemulsification: a prospective comparative study. Br J Ophthalmol. 2018;102(9):1248–1253. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.