")
Back to Journals » Clinical Ophthalmology » Volume 18
Surgical Outcome of Inferior Oblique Myectomy versus Recession–Anteriorization in the Treatment of Inferior Oblique Overaction
Authors Vijittrakarnrung T , Lekskul A , Preechaharn P , Aramrungroj S , Wuthisiri W
Received 10 December 2023
Accepted for publication 21 February 2024
Published 13 March 2024 Volume 2024:18 Pages 819—824
DOI https://doi.org/10.2147/OPTH.S454260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thanyathorn Vijittrakarnrung, Apatsa Lekskul, Puncharut Preechaharn, Sukrita Aramrungroj, Wadakarn Wuthisiri
Department of Ophthalmology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Thanyathorn Vijittrakarnrung, Tel +662-201-1533, Email [email protected]
Purpose: This study aimed to compare the surgical outcome of inferior oblique myectomy, IOM versus inferior oblique recession–anteriorization, IORA in the treatment of inferior oblique overaction, IOOA.
Patients and Methods: A retrospective chart review was performed over a 12-year period, from 2009 to 2021. Eighty-nine patients diagnosed with IOOA who underwent IOM or IORA were included. The primary outcome was postoperative residual IOOA (grade 0 to +4) and percentage favorable outcome, defined as IOOA grade ≤ 1+ at 6 months post operation, in each group. The outcomes were compared between the two surgical procedures (IOM and IORA). The secondary outcome was the percentage of postoperative anti-elevation syndrome cases for each surgical procedure.
Results: The median age at the time of surgery was 10.50 years (interquartile range, IQR: 2.83 to 28.33) in the IOM group and 5.08 years (IQR: 2.75 to 29.42) in the IORA group. The favorable outcome at 6 months was 90.91% in the IOM group, which was lower than the 95.74% in the IORA group but the difference was not statistically significant (P-value = 0.390, 95% CI: 0.07– 2.82). The only surgical complication, anti-elevation syndrome, was detected in 3.77% of IOM cases and 5.80% of IORA cases, with an odds ratio of 0.64 on comparing the IOM group to the IORA group (P-value = 0.611, 95% CI: 0.11– 3.62).
Conclusion: These two weakening procedures are effective for treating IOOA. Although IORA seemed slightly superior to IOM in terms of favorable outcomes, the difference was not statistically significant. Moreover, the myectomy procedure was easier, was less time-consuming, had a lower risk of globe perforation and presented fewer complications such as anti-elevation syndrome.
Keywords: inferior oblique overaction, IOOA, inferior oblique myectomy, IOM, inferior oblique recession and anteriorization, IORA
Corrigendum for this paper has been published.
Introduction
Inferior oblique overaction, IOOA is a cause of overelevation in adduction1 which is usually associated with horizontal deviation, as observed in 70% of patients with esotropia, ET and 30% of patients with exotropia, XT.2 Overaction can be categorized by etiology into primary and secondary IOOA. Primary IOOA has no identifiable cause and is commonly found in patients with infantile ET, which is associated with disruption of binocular vision development. Primary IOOA is usually bilateral and manifests as a slight vertical deviation in the primary position, minimal anomalous head posture, AHP and a negative head tilt test. In contrast, secondary IOOA is directly associated with pathology of the ipsilateral 4th cranial nerve or pathology of the superior oblique, SO muscle or tendon itself. Secondary IOOA can be either unilateral or bilateral.3,4 The presentation is similar to that of primary IOOA, with more vertical deviation in the primary position, marked head tilt, and positive Bielschowsky test in unilateral cases.
There are four main surgical weakening procedures of the inferior oblique, IO muscle including IO disinsertion, IOM, IORA and IO denervation and extirpation.5,6 However, because of the high rate of complications and ineffectiveness of surgical results, IO disinsertion,7 IO denervation, and extirpation6,8 are less likely to be the procedures of choice. Therefore, we compared the two remaining procedures: IOM and IORA.
Inconsistencies have been observed in previous studies. Some studies have found that IOM and IORA were comparable. In 2020, Elhusseiny et al found that surgical success was achieved in 80% of patients in the recession group and 75% in the myectomy group (P-value = 0.52).9 Insignificant differences were also observed in other studies.10–12 In contrast, some studies have found a statistically significant difference between the two procedures. In 1999, Min et al found that anterior transposition appeared to be more effective in treating IOOA with a success rate of 85%, which is higher than the 25% success rate for myectomy.13 However, in 2020, Farid et al found that IOM had a lower success rate than IORA,14 and in 2019, Nabie et al showed a statistically significant difference between the success rates of IORA and IOM, which were 75% and 96.4%, respectively (P-value = 0.029).15
Comparing IOM with IORA, IOM generally takes fewer operative steps and has lower risk of globe perforation than IORA. In addition, IORA is associated with a risk of postoperative anti-elevation syndrome.16
Based on this controversy, we aimed to determine the success rates of these two procedures in our institute. Moreover, we also studied data regarding complications, especially for anti-elevation syndrome.
Materials and Methods
This study was a retrospective chart review of patients who underwent an IO weakening procedure consisting of either an IOM or an IORA in the department of ophthalmology at Ramathibodi Hospital over a 12-year period (January 2009 to December 2021). Demographic data, including age at surgery, gender, primary or secondary IOOA, laterality, presence of V-pattern, presence of AHP, preoperative and postoperative logarithm of the minimal angle of resolution best-corrected visual acuity, logMAR BCVA, preoperative and postoperative vertical deviation angles, and IOOA grade (grade 0 to +4) were collected. Best-corrected visual acuity, BCVA was converted to the logMAR for statistical analysis. The grades of IOOA are as follows: (0) no IOOA, (+1) minimal upshoot of the adducting eye when taken straight across, (+2) upshoot of the adducting eye is obvious when the abducting eye looks straight across the lateral canthus, (+3) severe upshoot of the adducting eye is seen even with the abducting eye in straight abduction, and (+4) very severe upshoot of the adducting eye is seen as the fixing eye moves straight across into abduction.17 Surgeon preference is key to choosing the procedure (IOM vs IORA). Both unilateral and bilateral cases were included in this study. In cases of bilateral IOOA, the procedure was performed similarly in both eyes. In IORA, the IO was disinserted and anchored to the sclera along the lateral border of the inferior rectus muscle. For IOM, the IO muscle was identified, disinserted and resected at 5 mm. All procedures were performed by two pediatric ophthalmologists (WW and AL) at Ramathibodi Hospital. The primary outcome was the percentage favorable outcome, defined as IOOA grade ≤1+ at 6 months post operation in each group. This was compared for the two surgical procedures (IOM and IORA). The secondary outcome was the percentage of postoperative anti-elevation syndrome cases for each surgical procedure. Data were analyzed using the Mann–Whitney-Wilcoxon test, t-test, chi-square/Fisher’s exact test, multilevel mixed-effect linear regression, and multilevel mixed-effect logistic regression with 95% confidence intervals.
Results
Eighty-nine patients (123 eyes) were enrolled in this study, comprising 55 unilateral cases and 34 bilateral cases. Forty-eight percent of the patients were male. The median age at the time of surgery was 10.50 years (IQR: 2.83 to 28.33) in the IOM group and 5.08 years (IQR: 2.75 to 29.42) in the IORA group (P-value = 0.0591). Of all patients, 41 were classified as having primary IOOA and 48 as having secondary IOOA. Twenty patients (48.78%) in the primary IOOA group underwent IOM, and 21 patients (51.22%) underwent IORA. In the secondary IOOA group, 18 patients (37.50%) were managed with IOM and 30 patients (62.50%) were managed using IORA. This difference was not statistically significant (P-value = 0.284). As mentioned previously, primary IOOA is usually associated with infantile ET, which was found to be 60.98% in this study. All secondary IOOA cases in this study were caused by SO palsy. The majority of patients, 47 out of 48 (97.92%), were diagnosed with congenital SO palsy, while one patient (2.08%) had an acquired disease. The baseline demographic and clinical characteristics of the patients are presented in Table 1. Baseline preoperative vertical deviation, logMAR BCVA, IOOA grading, V-pattern, laterality, and AHP were not statistically different between the two groups.
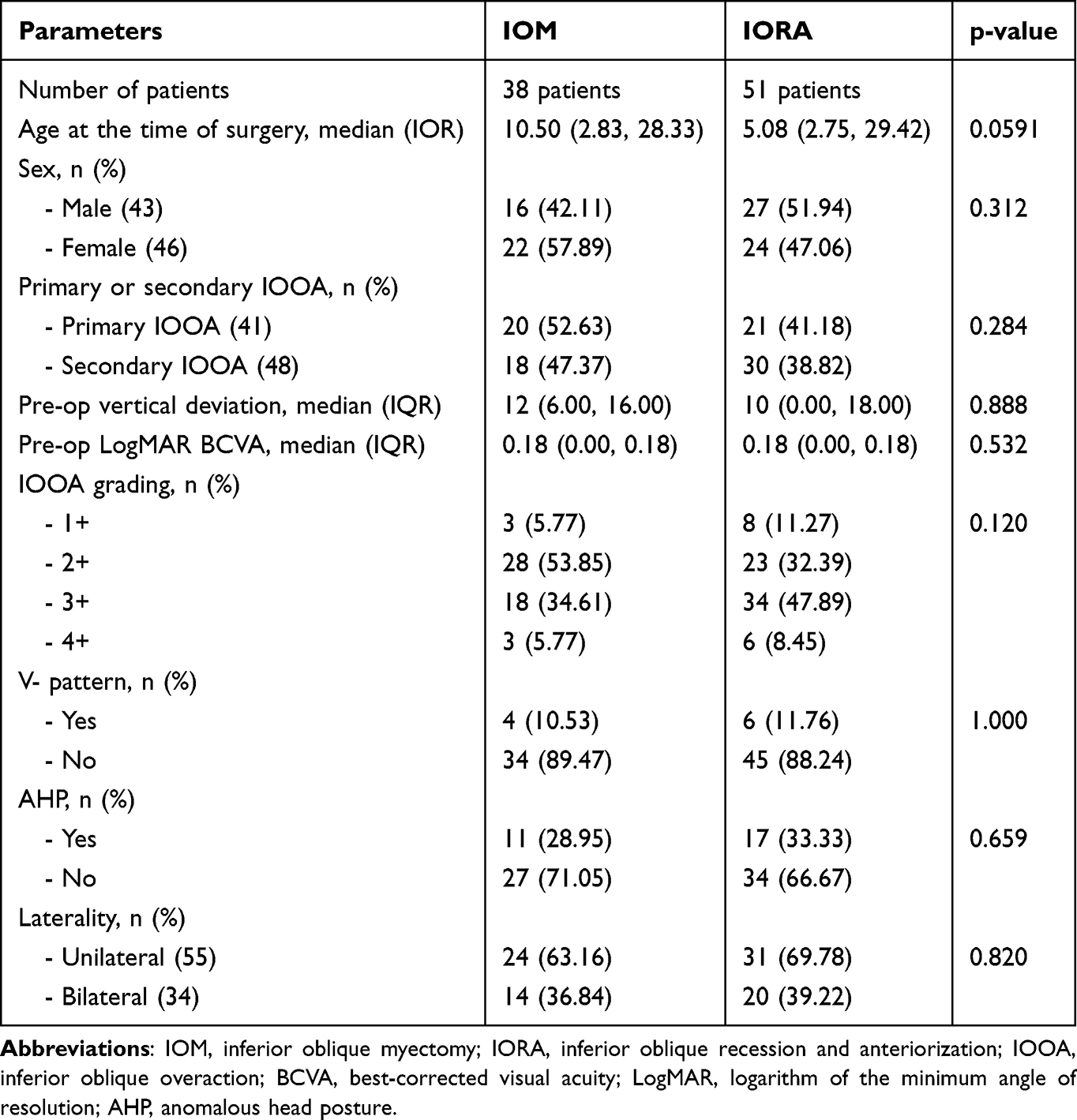 |
Table 1 Baseline Demographic and Clinical Characteristics of the Patients |
Surgical outcomes, in terms of favorable and unfavorable outcomes of both surgical procedures during the follow-up period, are presented in Table 2. Favorable outcomes between the two surgical procedures at each visit were not statistically significant. At 6 months of follow-up, the favorable outcome was 90.91% in the IOM group and 95.74% in the IORA group with an odds ratio of 0.44 (P-value = 0.390; 95% CI: 0.07–2.82). Table 3 shows that the postoperative grading of IOOA was not statistically different between the two procedures and the majority of IOOA grades were grade 0 in both groups. Ten patients had a V pattern at baseline. Of these, four were in the IOM group and six were in the IORA group. All were completely resolved after performing either IOM or IORA at the first visit and 1 month after surgery, and remained stable throughout the follow-up period. The only surgical complication found in this study was anti-elevation syndrome, present in 3.77% of the IOM group and 5.80% of the IORA group with an odds ratio of 0.64 when comparing the IOM group to the IORA group (P-value = 0.611, 95% CI: 0.11–3.62).
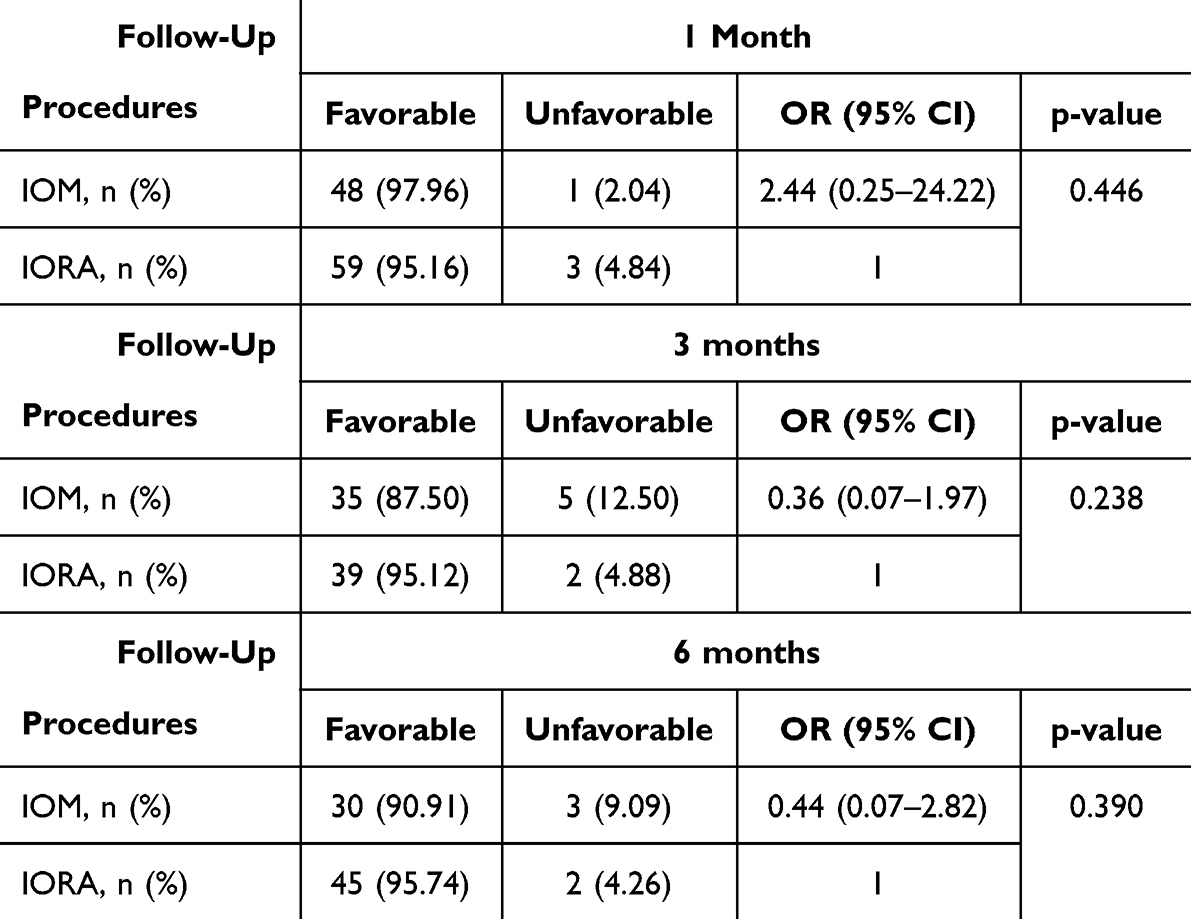 |
Table 2 Comparable of Post-Operative Outcome of IOOA Between IOM and IORA at Each Follow-Up Visit |
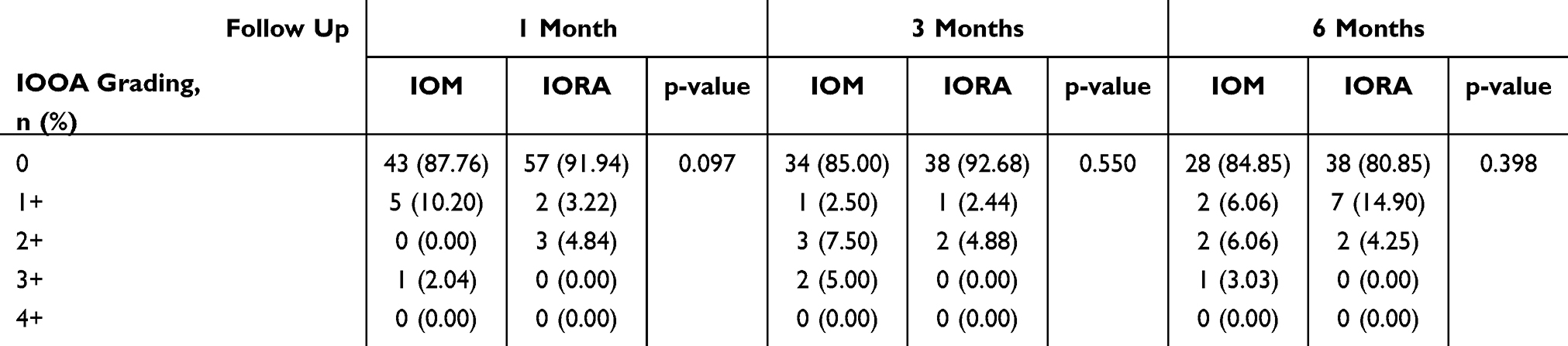 |
Table 3 Comparison of Post-Operative IOOA Grading Between IOM and IORA at 1 Month, 3 Months, and 6 Months Follow-Up |
Discussion
Various IO weakening procedures have been used for treatment of IOOA in both primary and secondary IOOA. These include IOM, IORA, IO disinsertion, and IO denervation and extirpation.5,6 However, because of the simplicity and less time-consuming nature of IOM and the lower recurrence of IOOA in IORA, these two surgical methods have become more popular for treating IOOA than the other methods. Most surgeons prefer one procedure to another, based on their experience. Although many studies have been conducted to compare IOM and IORA, it is still inconclusive which procedure is better.2,15,18 Some studies have suggested IOM over IORA for the treatment of bilateral symmetrical SO palsy with bilateral IOOA because it is simpler and more effective.19,20 Other studies found IORA to be superior in the correction of IOOA and hypertropia in the primary position and other gaze positions.14 The limitation of comparing result outcomes in large populations and the long follow-up period in Asian populations from previous studies instigated our comparison of the outcomes between these two surgical procedures in our institute.
This study compared the surgical outcomes of two different weakening procedures, IOM and IORA, in treating patients with primary and secondary IOOA. The primary outcome was the percentage favorable outcome at each follow-up visit, and the secondary outcome was postoperative complications. Our study demonstrates that both IORA and IOM are effective treatments for IOOA. Both procedures decreased the postoperative IOOA up to 6 months of follow-up. The data presented in Table 2 show that both weakening procedures had impressive results, with nearly 90% of the patients in each group having favorable outcomes at every visit. At 6 months post operation, the recurrence of IOOA in terms of unfavorable outcomes was higher in the IOM group than in the IORA group, but was statistically insignificant (P-value = 0.390). This observation might be explained by the unexpected spontaneous reattachment of the IO muscle in the IOM group, which was cut only 5 mm from its insertion, regardless of IOOA grading (grade +1 to +4). In contrast to the IORA group, the IO muscle was recessed and anteriorized according to the severity of IOOA grading. Intraoperative findings during reoperation in patients who had previously undergone myectomy showed that the cut IO muscle was reattached to the globe. This corresponds to the findings of Min et al and Park.8,13
One complication reported in a previous study by Park7 was IO muscle weakness after the weakening procedure, which was higher in the myectomy group (8%) than in the recession group (4%). Another important complication is adhesion syndrome, which manifests as hypotropia in the primary position, restricted elevation, and a positive traction test in up to 6% of cases of myectomy weakening procedure. However, the only surgical complication found in our study was anti-elevation syndrome which was detected in the IORA group (5.80%), consistent with the previous studies by Kushner,21 Mims,22 Stein,23 and Cho24 that reported anti-elevation syndrome after performing IORA.
This study included both primary IOOA associated with ET and XT and secondary IOOA found in SO palsy from 2009 to 2021 (12-year period) to compare the percentage favorable outcome of surgery between IOM and IORA procedures in an Asian population. However, these two IO weakening procedures were performed by two pediatric ophthalmologists (WW and AL), and even after more than a decade of data collection only 89 patients were included in our study, which was a limitation in the study. A larger sample size and a longer follow-up period will reflect a more reliable outcome.
Based on our experience, performing myectomy is easier than recession and anteriorization, is less time-consuming, has less risk of globe perforation, and presented less postoperative anti-elevation syndrome, which is commonly found in recession and anteriorization procedures. Anti-elevation syndrome is commonly found during recession and anteriorization because the procedure involves reinsertion of theIO muscle along the temporal aspect of the inferior rectus muscle insertion. This increases the force of infraduction and inhibits the globe from reaching the supraducts.
Conclusions
These two weakening procedures are effective for treating IOOA. Although IORA seemed insignificantly different from IOM, in terms of favorable outcomes of IOOA grading up to 6 months of follow-up, the myectomy procedure was easier, less time-consuming, had less risk of globe perforation, and presented less postoperative anti-elevation syndrome.
This study had some limitations. First, there were biases owing to the retrospective nature of the study. Second, the operation was performed by two pediatric ophthalmologists (WW and AL), which may have affected the results of the operation, including the angle of deviation measurement and IOOA grading. Third, although the data were collected over a 12-year period, only 89 patients were included in the study. The small sample size, short follow-up period, and significant loss to follow-up may have affected the outcomes.
Abbreviations
AHP, Anomalous Head Posture; BCVA, Best Corrected Visual Acuity; ET, Esotropia; IO, Inferior Oblique; IOM, Inferior Oblique Myectomy; IOOA, Inferior Oblique Overaction; IORA, Inferior Oblique Recession and Anteriorization; LogMAR, Logarithm of the Minimum Angle of Resolution; XT, Exotropia; SO, Superior Oblique.
Ethics and Consent to Participate
This study was approved by the Human Research Ethics Committee of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University and adhered to the Declaration of Helsinki. Due to the retrospective nature of the review, the authors confirm that the patient data was anonymized and maintained with confidentiality.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khan AO. 2022–-2023 basic and clinical science course, section 06: pediatric ophthalmology and strabismus; 2022–2023.
2. Aghdam KA, Asadi R, Sanjari MS, Sadeghi A, Razavi M. Comparing two inferior oblique weakening procedures: disinsertion versus myectomy. J Ophthalmic Vis Res. 2021;16(2):212–218.
3. Mostafa AM, Kassem RR. Comparative study of unilateral versus bilateral inferior oblique recession/anteriorization in unilateral inferior oblique overaction. Eur J Ophthalmol. 2018;28(3):272–278. doi:10.5301/ejo.5001062
4. Ozsoy E, Gunduz A, Ozturk E. Inferior oblique muscle overaction: clinical features and surgical management. J Ophthalmol. 2019;2019:9713189. doi:10.1155/2019/9713189
5. Stager D Jr, Dao LM, Felius J. Uses of the inferior oblique muscle in strabismus surgery. Middle East Afr J Ophthalmol. 2015;22(3):292–297. doi:10.4103/0974-9233.159723
6. Del monte MA, Parks MM. Denervation and extirpation of the inferior oblique. An improved weakening procedure for marked overaction. Ophthalmology. 1983;90(10):1178–1185. doi:10.1016/S0161-6420(83)34409-2
7. Parks MM. The weakening surgical procedures for eliminating overaction of the inferior oblique muscle. Am J Ophthalmol. 1972;73(1):107–122. doi:10.1016/0002-9394(72)90313-3
8. Parks MM. Inferior oblique weakening procedures. Int Ophthalmol Clin. 1985;25(4):107–117. doi:10.1097/00004397-198502540-00010
9. Elhusseiny AM, Gore C, Ali A Sadiq M, et al. Self-grading effect of inferior oblique myectomy and recession. J AAPOS. 2020;24(4):218.e1–218.e6. doi:10.1016/j.jaapos.2020.04.014
10. Ghazawy S, Reddy AR, Kipioti A, et al. Myectomy versus anterior transposition for inferior oblique overaction. J AAPOS. 2007;11(6):601–605. doi:10.1016/j.jaapos.2007.06.011
11. Yoo JH, Kim S-H, Seo JW, et al. Self-grading effect of inferior oblique recession. J Pediatr Ophthalmol Strabismus. 2013;50(2):102–105. doi:10.3928/01913913-20121127-03
12. Ozsoy E, Gunduz A, Ozturk E, Cankaya C. Surgical management of primary inferior oblique muscle overaction: a subgroup-specific surgical approach. Beyoglu Eye J. 2020;5(1):38–42.
13. Min B-M, Park J-H, Kim S-Y, et al. Comparison of inferior oblique muscle weakening by anterior transposition or myectomy: a prospective study of 20 cases. Br J Ophthalmol. 1999;83(2):206–208. doi:10.1136/bjo.83.2.206
14. Farid MF, Anany M, Abdelshafy M. Surgical outcomes of three different weakening procedures of inferior oblique muscle in the treatment of unilateral superior oblique palsy. BMC Ophthalmol. 2020;20(1):298. doi:10.1186/s12886-020-01568-w
15. Nabie R, Raoufi S, Hassanpour E, et al. Comparing graded anterior transposition with myectomy in primary inferior oblique overaction – a clinical trial. J Curr Ophthalmol. 2019;31(4):422–425. doi:10.1016/j.joco.2019.04.002
16. Niyaz L, Yücel OE, Gul A. Infrequent complications of inferior oblique recession surgery. Semin Ophthalmol. 2017;32(5):593–596. doi:10.3109/08820538.2015.1132332
17. Wright KW, Thompson L. Color Atlas of Strabismus Surgery.
18. Sieck EG, Madabhushi A, Patnaik JL, et al. Comparison of different surgical approaches to inferior oblique overaction. J Binocul Vis Ocul Motil. 2020;70(3):89–93. doi:10.1080/2576117X.2020.1776566
19. Huang Y-T, Chen JJ-Y, Wu M-Y, et al. The effects of modified graded recession, anteriorization and myectomy of inferior oblique muscles on superior oblique muscle palsy. J Clin Med. 2021;10(19):4433. doi:10.3390/jcm10194433
20. Bahl RS, Marcotty A, Rychwalski PJ, et al. Comparison of inferior oblique myectomy to recession for the treatment of superior oblique palsy: table 1. Br J Ophthalmol. 2013;97(2):184–188. doi:10.1136/bjophthalmol-2012-301485
21. Kushner BJ. Restriction of elevation in abduction after inferior oblique anteriorization. J AAPOS. 1997;1(1):55–62. doi:10.1016/S1091-8531(97)90024-0
22. Mims JL 3rd, Wood RC. Antielevation syndrome after bilateral anterior transposition of the inferior oblique muscles: incidence and prevention. J AAPOS. 1999;3(6):333–336. doi:10.1016/S1091-8531(99)70040-6
23. Stein LA, Ellis FJ. Apparent contralateral inferior oblique muscle overaction after unilateral inferior oblique muscle weakening procedures. J AAPOS. 1997;1(1):2–7. doi:10.1016/S1091-8531(97)90016-1
24. Cho YA, Kim JH, Kim S. Antielevation syndrome after unilateral anteriorization of the inferior oblique muscle. Korean J Ophthalmol. 2006;20(2):118–123. doi:10.3341/kjo.2006.20.2.118
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.