Back to Journals » Clinical Ophthalmology » Volume 18
Surgical Efficiency Comparison Between Two Phacoemulsification Systems
Authors Ibarz-Barberá M, Orts-Vila P, Martínez-Galdón F, Martín-García N ![]() , Tañá-Rivero P
, Tañá-Rivero P
Received 7 December 2023
Accepted for publication 26 February 2024
Published 24 April 2024 Volume 2024:18 Pages 1095—1102
DOI https://doi.org/10.2147/OPTH.S453899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marta Ibarz-Barberá,1 Paz Orts-Vila,2 Fátima Martínez-Galdón,1 Noemí Martín-García,2 Pedro Tañá-Rivero2
1Cataract and Refractive Surgery Department, Madrid, Spain; 2Cataract and Refractive Surgery Department, Alicante, Spain
Correspondence: Marta Ibarz-Barberá, Oftalvist Madrid, Avda Valladolid, 81, Madrid, 28008, Spain, Tel +34 915426010, Email [email protected]
Purpose: To assess the surgical efficiency in cataract surgery comparing two phacoemulsification systems.
Methods: Prospective, consecutive-comparative study in a two-site private practice. Three hundred and one eyes undergoing standard or femtosecond laser-assisted (FLACS) cataract surgery with either the R-Evo Smart (BVI, Waltham, USA) and/or the Centurion Vision System (Alcon, Fort Worth, USA). Preoperative eye characteristics (degree of cataract using the lens opacities classification system LOCS III grading) and intraoperative outcomes (total ultrasound time and total estimated fluid aspirated/drainage bag weighting) were registered in all cases.
Results: One hundred and fifty-five eyes undergone cataract surgery with the R-Evo Smart and 146 eyes with the Centurion Vision System phacoemulsification systems. Mean cataract grade was 3.07 ± 0.78 and 2.96 ± 0.85 for the R-Evo Smart and Centurion Vision System groups, respectively (p = 0.12). Mean total ultrasound time was 18.99 ± 12.85 and 40.24 ± 21.91 seconds for the R-Evo Smart and Centurion Vision System groups, respectively (p < 0.01). Mean total estimated fluid aspirated/drainage bag weighting was 53.00 ± 14.56 g and 54.33 ± 14.88 cc for the R-Evo Smart and Centurion Vision System groups, respectively (p = 0.21). Considering non-FLACS surgery (98 eyes with the R-Evo Smart and 63 eyes with the Centurion Vision System), mean cataract grade was 2.95 ± 0.74 and 2.97 ± 0.91 for the R-Evo Smart and Centurion Vision System groups, respectively (p = 0.44). Mean total ultrasound time was 19.96 ± 11.20 and 42.84 ± 28.35 seconds for the R-Evo Smart and Centurion Vision System groups, respectively (p < 0.01). Mean total estimated fluid aspirated/drainage bag weighting was 55.95 ± 14.76 g and 55.97 ± 13.62 cc for the R-Evo Smart and Centurion Vision System groups, respectively (p = 0.49). No adverse events were found in the two groups of eyes.
Conclusion: The objective measurement of surgical efficiency through total ultrasound time during lens removal and fluid consumption during both lens removal and irrigation/aspiration proved R-Evo Smart to be an efficient phacoemulsification platform, in comparison with the current standard of care Centurion Vision System.
Keywords: cataract, estimated fluid aspirated, phacoemulsification, surgical efficiency, ultrasound time
Introduction
It is well known that cataract is the main cause of reversible blindness in the world, and specifically, it has been reported that about 20 million Americans older than 40 years have cataract in either eye.1 The number of patients affected by this pathology and consequently to be submitted to cataract surgery has been drastically increasing over time. The current gold standard procedure for cataract surgery is phacoemulsification technique due to the small number complications and excellent visual acuity outcomes.2,3 There is a tendency to fewer surgical complication and better predicted refractions and visual outcomes.4 This technique uses a phacoemulsifier irrigator and aspirator, and most of them use peristaltic pump technology.
Phacoemulsification has improved during the last years in order to increase surgical efficacy and reduce complications. One of these relatively new phacoemulsifier irrigator and aspirators is the Centurion Vision System (Alcon, Fort Worth, USA), which uses a small aspiration tubing and a cassette design with low compliance to minimize surge, and Active Fluidics to provide greater intraocular pressure (IOP) stability that minimizes IOP fluctuations happening during occlusion and post-occlusion break events. This device has been proved to be an excellent phacoemulsification system in different clinical studies published in the literature showing improved surgical efficiency.5–9 Recently, the R-Evo Smart (BVI, Waltham, USA), a new phacoemulsification system for cataract surgery, has been developed, it incorporates two regulation systems with the aim of ensuring effectiveness and safety during surgery. The Agile Fluidics system mitigates the surge effect by adjusting the IOP based on the aspiration demand, and the Minimal Stress system makes sure that the elongation length of the phacoemulsification tip in each pulse is consistent with the programmed length, regardless of the hardness of the crystalline nucleus. It uses peristaltic and Venturi pumps, dual-infusion modality and dynamic IOP control.10
The main objective of the study is to compare the surgical efficiency in cataract surgery between two phacoemulsification machines, the R-Evo Smart and the Centurion Vision System, analyzing the total ultrasound time used as well as the total fluid aspirated/drainage bag weighting in each procedure.
Methods
Patients and Surgical Procedure
In this study, we have prospectively examined 301 eyes at two centers, Oftalvist Clinic in Madrid and Alicante, Spain, between May 2023 and October 2023. This study was approved by the Oftalvist Review Board. All patients signed an informed consent before surgery according to the tenets of the Declaration of Helsinki. Patients with cataracts were included in the study. Exclusion criteria considered traumatic, white or Morgagnian cataracts, subluxated crystalline lens, nystagmus, previous vitrectomy, weak zonules or narrow pupils. A full pre-operative assessment was performed in all patients, and specifically cataract degree was classified according to lens opacities classification system (LOCS) III.11 Standard or femtosecond laser-assisted cataract surgery (FLACS) using the Catalys Precision Laser platform (Johnson & Johnson Vision, Santa Ana, USA) with 5-mm capsulotomy was performed through a 2.2-mm, temporally located, clear corneal incision. Two surgeons (MIB and POV) performed the surgeries.
Phacoemulsification Systems and Surgical Parameters
The specifications of the R-Evo Smart and the Centurion Vision Systems are indicated in Table 1. Both machines have been used under the manufacturer´s recommendations in terms of settings for fluidics and energy delivery, particularly for the latter Continuous U/S for Centurion Vision System and Pulsed-Burst U/S for R-Evo Smart. The program used with the R-Evo Smart system was sculpting with continuous ultrasound, chop and segment removal with Multi Burst, epinucleus with pulse mode HD Pulse ON, cortical removal, polish and viscoelastic removal. The program used with the Centurion Vision System was sculpting with torsional/longitudinal continuous, chop and segment removal with torsional continuous, epinucleus with torsional continuous, cortical removal, polish and viscoelastic removal. Details of the surgical settings of both surgical platforms in both centers are shown in Figure 1.
 |
Table 1 Specification for the Two Phacoemulsification Systems |
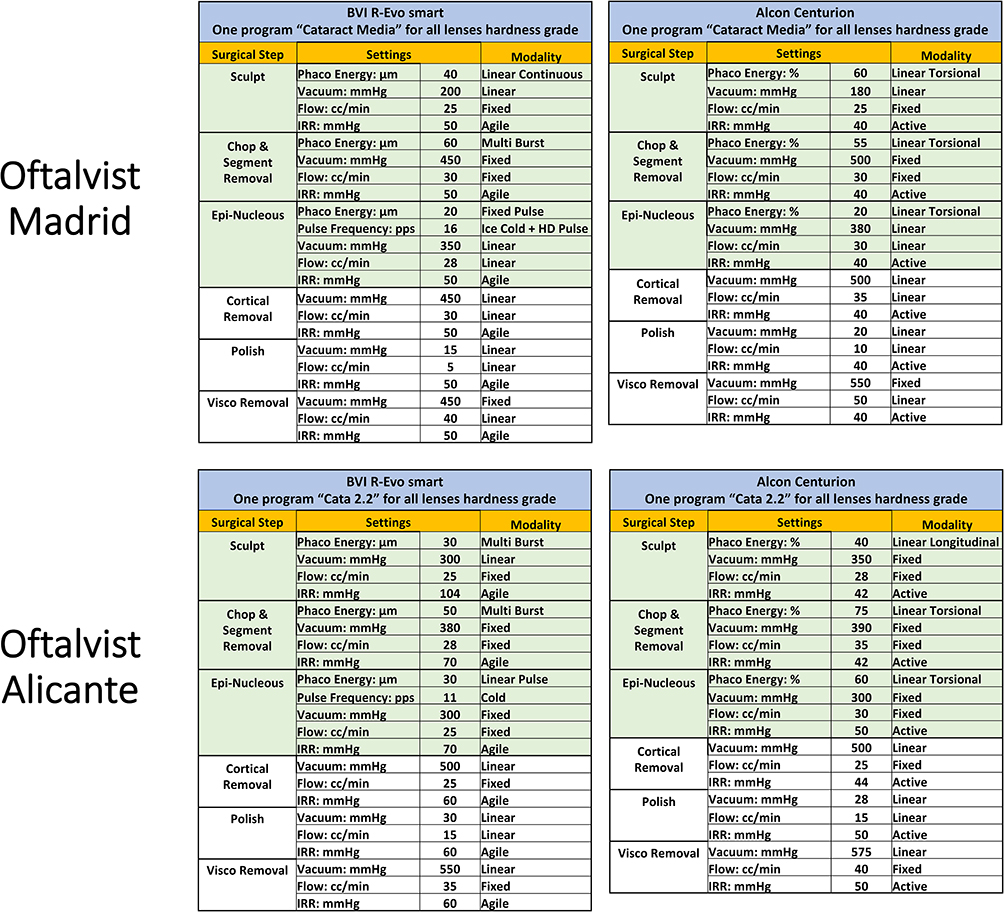 |
Figure 1 Details of the surgical settings of both surgical platforms in the two clinical centers. |
Measurements and Analysis
Measurement of ultrasound time was recorded from both systems. In relation to the total estimated fluid aspiration, it was recorded directly for the Centurion Vision System. For the R-Evo Smart system the drainage bag weighting was used. The weight (measured with a precision balance) of the bag plus the weight of the liquid used for priming was subtracted from the total weight. Figure 2 visualizes where the drainage bag has been cut after each case (A) and the act of weighing the drainage bag on the high precision digital scale (B). The R-Evo Smart drainage bag has a one-way valve that prevents aspirated fluid to drop off, therefore ensuring the consistency of the measurement.
 |
Figure 2 Picture where the drainage bag has been cut after each case (A) and the act of weighing the drainage bag on the high precision digital scale (B). |
Analysis of the outcomes was carried out using Excel (2019, version 16.43, Microsoft Corporation, Redmond, USA) with all measurements given as the mean ± standard deviation (SD) and ranges. A sub-analysis of the non-FLACS eyes was done.
Results
The study comprised 155 eyes that underwent cataract surgery using the R-Evo Smart and 146 eyes that underwent cataract surgery with the Centurion Vision System. Within each study group, a sub-group of patients underwent standard phacoemulsification procedure only and the second sub-group underwent to FLACS procedure followed by phacoemulsification. No adverse events were found in the two groups of eyes during the procedures. Table 2 shows the surgical outcomes obtained. For the whole sample, our results revealed that there was no statistically significant difference between cataract degree between both groups of eyes (p > 0.12): mean cataract grade according to LOCS III classification was 3.07 ± 0.78 and 2.96 ± 0.85 for the R-Evo Smart and Centurion Vision System eye groups, respectively. In terms of surgical outcomes, our values revealed that the mean total ultrasound time was 18.99 ± 12.85 and 40.24 ± 21.91 seconds for the R-Evo Smart and Centurion Vision System eye groups, respectively. The differences between both groups of eyes were statistically significant: p <0.01. The mean total estimated fluid aspirated/drainage bag weighting was 53.00 ± 14.56 g and 54.33 ± 14.88 cc for the R-Evo Smart and Centurion Vision System eye groups, respectively. In this parameter, we did not find statistically significant differences: p = 0.21. Regarding the possible correlation between cataract grade, ultrasound time and amount of aspirated fluid, Figure 3 shows that the higher the cataract grade, the higher the US time for both phacoemulsification systems (Centurion R2=0.08, R-EVO R2=0.2). Fluid consumption tends to increase slightly with both devices with harder cataracts (Centurion R2=0.01, R-EVO R2=0.01).
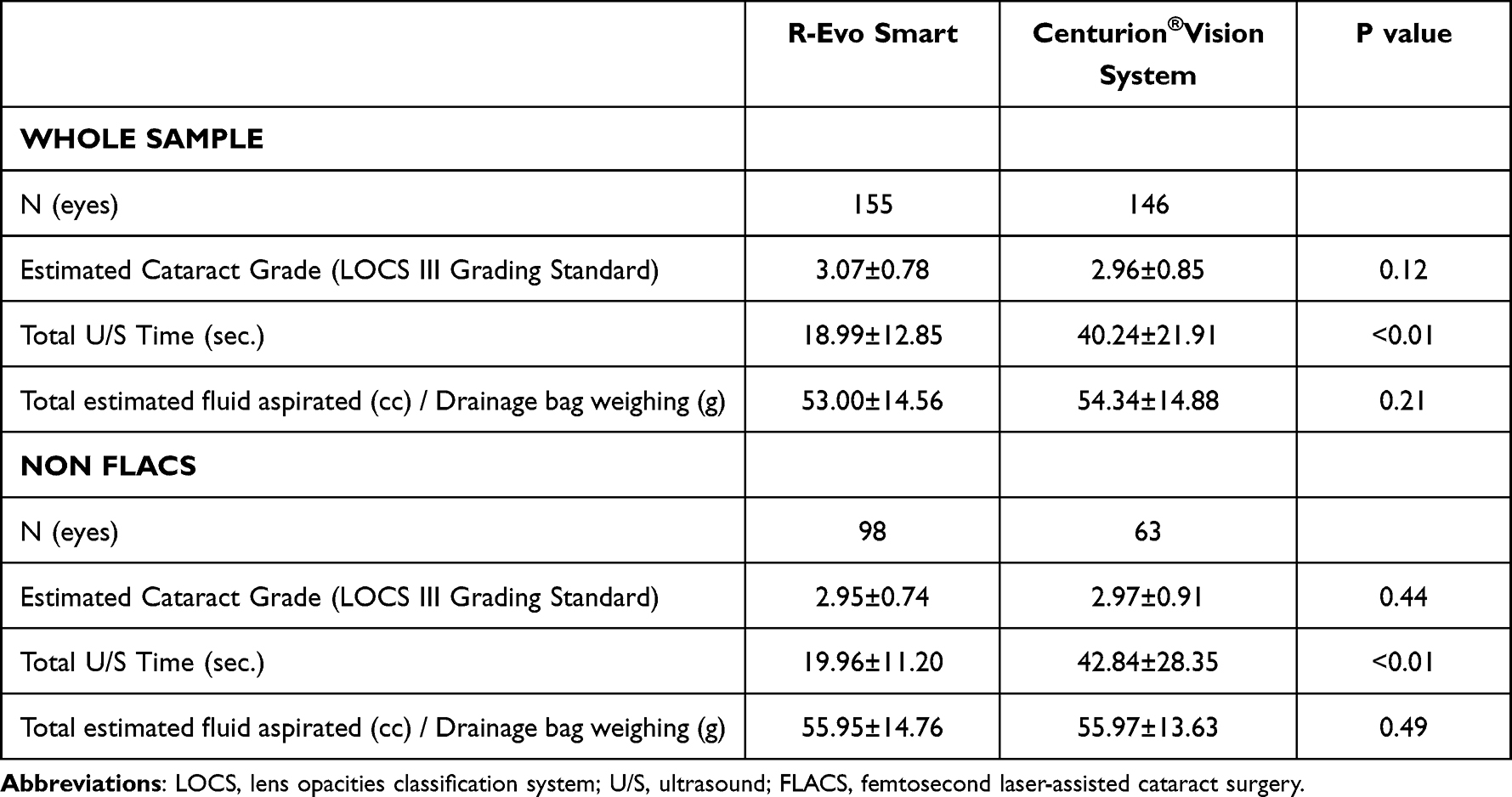 |
Table 2 Surgical Outcomes Obtained Using the Two Phacoemulsification Systems |
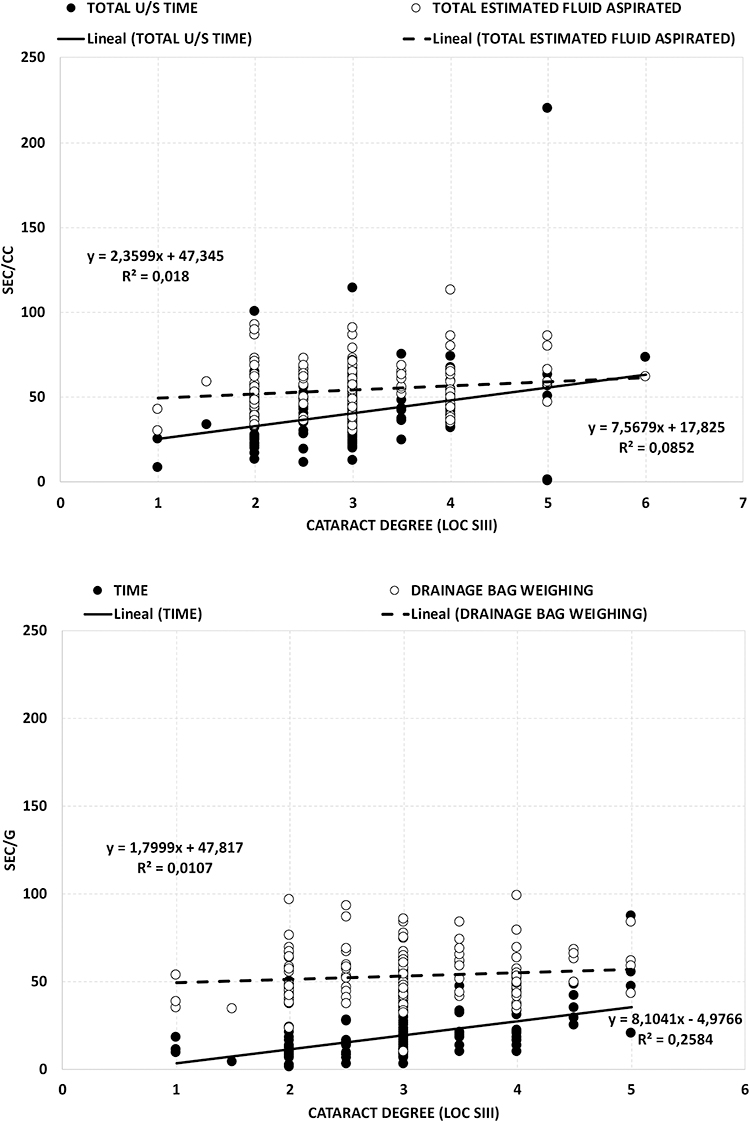 |
Figure 3 Total US/time and Total estimated fluid aspirated versus cataract degree (LOCS III scale) for the Centurion Vision System (top) and Time and Drainage bag weighing versus cataract degree (LOCS III scale) for the R-Evo Smart (bottom). Both graphs show the linear regression adjustments for the different parameters measured (equation and R2 values are also shown). |
For the non-FLACS eyes (98 versus 63 eyes for the R-Evo Smart and Centurion Vision System eye groups, respectively), our results showed no statistically significant differences between the degree of cataract: 2.95 ± 0.74 for the R-Evo Smart and 2.97 ± 0.91 for the Centurion Vision System (p = 0.44). The total ultrasound time was statistically significant between systems: 19.96 ± 11.20 and 42.84 ± 28.35 seconds for the R-Evo Smart and Centurion Vision System eye groups, respectively (p < 0.01). The mean total estimated fluid aspirated/drainage bag weighting was 55.95 ± 14.56 g and 55.97 ± 13.63 cc for the R-Evo Smart and Centurion Vision System eye groups, respectively (p = 0.49).
Discussion
The basic principle of any cataract removal procedure is to achieve maximum efficacy without compromising safety. High vacuum, a longer effective phacoemulsification time, and higher cataract density have been shown to be independent predictors of endothelial cell loss.12–14 Developments in this area aim to reduce ultrasound energy, reducing the quantity of fluid aspirated and lowering effective phacoemulsification time while aiming at increasing the stability of the anterior chamber. In this study, we focused on the ultrasound time and effective fluid use to compare the efficacy of two different phacoemulsification systems.
The study comprised 155 eyes that underwent cataract surgery using the R-Evo Smart and 146 eyes that underwent cataract surgery with the Centurion Vision System with comparable nucleus hardness in both groups. The whole sample was divided into two subgroups for analysis depending on the use of FLACS (FLACS vs non-FLACS). The mean total ultrasound time (18.99 ± 12.85 seconds versus 40.24 ± 21.91 seconds) was lower for R-Evo Smart, while no differences in the mean total estimated fluid aspirated (53.00 ± 14.56 g versus 54.33 ± 14.88 cc, R-Evo Smart vs Centurion Vision System), were found. Subgroup analysis (FLACS vs non-FLACS) showed similar results between both groups, a statistically significant lower effective phacoemulsification time and similar fluid consumption with R-Evo Smart.
The latest phacoemulsification systems incorporate several improvements in their designs that aim to reduce effective phacoemulsification time, chatter (the phenomenon of lens material bouncing of the phaco tip),6 and subsequent cumulative dissipated energy (torsional amplitude × torsional time × a coefficient of 0.46) delivered into the eye. Centurion Vision System was released in 2013 including a newly designed phacoemulsification tip designed for torsional ultrasound (Ozil) with a 50% enhancement in sideways tip displacement (data on file, Alcon Laboratories, 2015) that minimizes stromal changes by reducing the amount of energy delivered to the incision site while reducing chatter.15,16 R-Evo Smart incorporates a new design called “Minimal Stress™ ultrasound delivery Technology” that maintains the consistency between the programmed length of the phaco tip stroke and the actual tip elongation independently from the nucleus hardness, reducing the amount of wasted energy compared to traditional ultrasound systems.10 According to the study published by Cimino et al,17 the most important factors that result in tissue fragmentation are stroke amplitude, suction and acceleration of the tip, while Chen et al6 showed that higher frequency produces better tissue fragmentation with a lower effective phacoemulsification time and lower delivery of cavitation bubbles. R-Evo Smart maintains the consistency of the stroke length and reduces surge through synergic work of a small-bore rigid aspiration tubing (1.3 mm) combined with a narrower design of a flared tip. According to the results of the current study, the innovative ultrasound delivery technology (Minimal Stress) in association with advanced design of energy emission forms (Multi Burst, HD Pulse) and in conjunction with the safety supported by Agile fluidics may help reduce the total ultrasound time compared to the current standard of practice.
The mean total fluid aspirated or effective fluid use (as described by other authors18), plays an important role in endothelial safety during cataract surgery, since a higher fluid consumption increases the loss of endothelial cells.19 According to our results, both phacoemulsification systems have comparable fluid consumption. Centurion uses an active fluid dynamic management system that applies pressure directly to the irrigation bag, constantly adjusting fluctuations that result in a more stable anterior chamber, minimizing abrupt swings in aspiration flow rate, pressure, and rate of vacuum (data on file, Alcon Laboratories, 2015).6 R-Evo Smart incorporates a system that regulates intraocular pressure to avoid fluctuations called “Agile Fluidics™ that consists of a set of controlled irrigation that enables a dynamic intraocular pressure management, as well as a compatible rigid irrigation solution container, plus the “Easysys Fluidic System”. It works through a proprietary algorithm that reacts to the vacuum measured by the system sensor with more pressure feeding into the irrigation bottle. The compensation is linear and instantaneous both with increasing and decreasing vacuum levels. The system increases up to only 20 mmHg, for vacuums up to 400 mmHg.
We need to consider some limitations of our study. The main variable used for comparison between R-Evo Smart and Centurion was the total ultrasound time (or effective phacoemulsification time), widely used in numerous studies for comparison of outcomes between phacoemulsification devices.20–22 The cumulative dissipated energy is another parameter used for comparative studies, but exclusively among different Alcon´s devices, since it is a proprietary measurement of that company. Second, the measurement of the total fluid aspirated is given automatically by Centurion, but not by R-Evo Smart that required a precision balance and a mathematical calculation to subtract the bag’s weight from the total weight after each surgery. And finally, it would also be of interest to consider the frequency of the ultrasound that each system uses for comparison, since a higher frequency phacoemulsification was associated with a lower effective phacoemulsification time and effective fluid use as well as better endothelial preservation according to Dewan et al.18 Future studies considering these points and quantitative assessment of corneal endothelium would be desirable to confirm the outcomes reported.
Conclusions
In summary, the current clinical study demonstrates that both phacoemulsification systems are safe and efficient for different degrees of cataracts with no surgical complications. Patients with cataracts may benefit from the use of these two systems when submitted to cataract surgery. Specifically, our study indicates that the R-Evo Smart is an efficient phacoemulsification platform when measuring surgical efficiency through total ultrasound time and fluid consumption, in comparison with the current standard of care Centurion Vision System.
Data Sharing Statement
The data are not available for sharing.
Funding
This study was funded by Beaver-Visitec International, Inc. (BVI), Waltham, USA.
Disclosure
Dr. Ibarz-Barberá reports has received grants from BVI, Cutting Edge and Hoya Surgical Optics. Dr. Paz Orts-Vila has received grants for Alcon Laboratories, AST Products, BVI, Carl Zeiss Meditec, Hoya Surgical Optics, HumanOptics, Johnson&Johnson and Ocumension. Dr Tañá-Rivero has received grants for Alcon Laboratories, AST Products, BVI, Carl Zeiss Meditec, Hoya Surgical Optics, HumanOptics, Johnson&Johnson, Staar Surgical and Vialase Inc. The authors report no other conflicts of interest in this work.
References
1. Congdon N, Vingerling JR, Klein BE, et al.; Eye Diseases Prevalence Research Group. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol. 2004;122(4):487–494.
2. Lundström M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European registry of quality outcomes for cataract and refractive surgery database. J Cataract Refract Surg. 2012;38(6):1086–1093. doi:10.1016/j.jcrs.2012.03.006
3. Tsinopoulos IT, Lamprogiannis LP, Tsaousis KT, et al. Surgical outcomes in phacoemulsification after application of a risk stratification system. Clin Ophthalmol. 2013;7:895–899. doi:10.2147/OPTH.S42726
4. Lundström M, Dickman M, Henry Y, et al. Changing practice patterns in European cataract surgery as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery 2008 to 2017. J Cataract Refract Surg. 2021;47(3):373–378. doi:10.1097/j.jcrs.0000000000000457
5. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14:96. doi:10.1186/1471-2415-14-96
6. Chen M, Anderson E, Hill G, Chen JJ, Patrianakos T. Comparison of cumulative dissipated energy between the Infiniti and centurion phacoemulsification systems. Clin Ophthalmol. 2015;9:1367–1372. doi:10.2147/OPTH.S88225
7. Davison JA. Two-speed phacoemulsification for soft cataracts using optimized parameters and procedure step toolbar with the CENTURION vision system and balanced tip. Clin Ophthalmol. 2015;9:1563–1572. doi:10.2147/OPTH.S90245
8. Solomon KD, Lorente R, Fanney D, Cionni RJ. Clinical study using a new phacoemulsification system with surgical intraocular pressure control. J Cataract Refract Surg. 2016;42(4):542–549. doi:10.1016/j.jcrs.2016.01.037
9. Oh LJ, Nguyen CL, Wong E, Wang SSY, Francis IC. Prospective study of Centurion® versus Infiniti®phacoemulsification systems: surgical and visual outcomes. Int J Ophthalmol. 2017;10(11):1698–1702. doi:10.18240/ijo.2017.11.10
10. Rossi T, Saffioti S, Angelini G, et al. Testing a novel device for accurate ultrasound delivery during crystalline lens phacoemulsification surgery. Transl Vis Sci Technol. 2020;9(3):7. doi:10.1167/tvst.9.3.7
11. Chylack LT, Wolfe JK, Singer DM, et al.; For the Longitudinal Study of Cataract Study Group. The lens opacities classification system III. Arch Ophthalmol. 111;1993:831–836. doi:10.1001/archopht.1993.01090060119035
12. El-Din YM S, Gamal El-Din S, Amad RA, Rahman Mowafy DA. Time parameters in continuous versus pulsed ultrasound phacoemulsification: a comparative study. Med J Cairo Univ. 2009;77:89–93.
13. Soliman Mahdy MAE, Eid MZ, Mohammed MA-B, Hafez A, Bhatia J. Relationship between endothelial cell loss and microcoaxial phacoemulsification parameters in noncomplicated cataract surgery. Clin Ophthalmol. 2012;6:503–510. doi:10.2147/OPTH.S29865
14. Conrad-Hengerer I, Al Juburi M, Schultz T, Hengerer FH, Dick HB. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser–assisted cataract surgery: three-month follow-up. J Cataract Refract Surg. 2013;39:1307–1313. doi:10.1016/j.jcrs.2013.05.033
15. Tjia KF. Novel balanced phaco tip for microcoaxial torsional phaco.
16. Liu Y, Zeng M, Liu X, et al. Torsional mode versus conventional ultrasound mode phacoemulsification. J Cataract Refract Surg. 2007;33(2):287–292. doi:10.1016/j.jcrs.2006.10.044
17. Cimino WW, Bond LJ. Physics of ultrasonic surgery using tissue fragmentation: part I. Ultrasound Med Biol. 1996;22:89–100. doi:10.1016/0301-5629(95)02021-7
18. Dewan T, Malik PK, Kumari R. Comparison of effective phacoemulsification time and corneal endothelial cell loss using 2 ultrasound frequencies. J Cataract Refract Surg. 2019;45(9):1285–1293. doi:10.1016/j.jcrs.2019.04.015
19. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors for corneal endothelial injury during phacoemulsification. J Cataract Refract Surg. 1996;22:1079–1084. doi:10.1016/S0886-3350(96)80121-0
20. Fahmy HL, Saad Eldien HM. New technique for nuclear fragmentation in phacoemulsification. Global Adv Res J Med Med Sci. 2014;3:291–297.
21. Richard J, Hoffart L, Chavane F, Ridings B, Conrath J. Corneal endothelial cell loss after cataract extraction by using ultrasound phacoemulsification versus a fluid-based system. Cornea. 2008;27:17–21. doi:10.1097/ICO.0b013e3181583115
22. Vargas LG, Holzer MP, Solomon KD, Sandoval HP, Auffarth GU, Apple DJ. Endothelial cell integrity after phacoemulsification with 2 different handpieces. J Cataract Refract Surg. 2004;30:478–482. doi:10.1016/S0886-3350(03)00620-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.