Back to Journals » Clinical Ophthalmology » Volume 17
Surgical Augmentation of the Suprachoroidal Space: A Novel Material and Implant
Authors De Francesco T ![]() , Ahmed IIK
, Ahmed IIK ![]()
Received 17 March 2023
Accepted for publication 1 June 2023
Published 21 August 2023 Volume 2023:17 Pages 2483—2492
DOI https://doi.org/10.2147/OPTH.S409958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ticiana De Francesco,1– 3 Iqbal Ike K Ahmed3,4
1Clinica de Olhos De Francesco, Fortaleza, Brazil; 2Hospital de Olhos Leiria de Andrade (HOLA), Fortaleza, Brazil; 3John A. Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 4Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, ON, Canada
Correspondence: Ticiana De Francesco, 499 Barao de Aracati, Fortaleza, Brazil, Tel +55 85 3219-24-25, Email [email protected]
Abstract: Microinvasive glaucoma surgery (MIGS) has emerged as a safer method to lower IOP with minimal impact on patient quality of life compared to traditional glaucoma surgeries. With the advent of MIGS, there has been a renewed interest in exploring the suprachoroidal route. MIGS targeting the suprachoroidal space allow for a safe reduction in IOP while sparing conjunctiva and allowing “blebless” surgery, thus avoiding bleb-related complications. This article aims to review the rationale behind the suprachoroidal MIGS procedures and the literature surrounding the efficacy and safety of a novel suprachoroidal device, the MINIject. The available literature has shown promising IOP lowering results with the MINIject implant with a potentially safer and less invasive approach than traditional glaucoma surgeries.
Keywords: suprachoroidal space, microinvasive glaucoma surgery, glaucoma
Background
Minimally Invasive Glaucoma Surgery
Glaucoma is the leading cause of irreversible blindness worldwide, with over 100 million people expected to suffer from the disease by 2040.1 Lowering intraocular pressure (IOP) is currently the only modifiable risk factor in glaucoma progression and is thus the target of glaucoma treatment.2,3 The advent of microinvasive glaucoma surgery (MIGS) has emerged as a method to lower IOP with a higher safety profile and minimal impact on patient quality of life compared to traditional glaucoma surgeries such as trabeculectomy and tube shunt surgery. These microinvasive procedures have allowed safer interventional therapies at an earlier stage of disease. The variety of MIGS devices available are designed to enhance aqueous humour outflow while typically being conjunctival sparing and minimally traumatic. Currently, this is done by directly accessing Schlemm’s canal.4 Along the spectrum of MIGS devices, a decreased safety profile is usually traded for an increase in efficacy. The European Glaucoma Society defines only the ab interno non-bleb forming procedures as “microinvasive glaucoma surgery.”5 Microshunts and stents that target the subconjunctival space – termed “microinvasive bleb surgery (MIBS)” – are bleb–forming procedures. They have greater potency in lowering IOP but increased relative risks compared with other types of internal MIGS; however, still considerably less invasive than traditional glaucoma surgeries.6 A third option for outflow target is the suprachoroidal space, which is considered a MIGS approach and has been drawing more attention lately. Glaucoma surgeries targeting this space seem particularly promising by using a presumably highly efficient whilst secure outflow route and avoiding subconjunctival filtration blebs.7
The Suprachoroidal Route in Glaucoma Surgery
The physiological outflow of aqueous humour from the anterior chamber (AC) occurs through two pathways: conventional and uveoscleral. The conventional pathway involves aqueous humour flowing through the trabecular meshwork, Schlemm’s canal, and eventually into the distal collector channels and aqueous veins. The uveoscleral pathway consists of the interstitium of the ciliary body, the supraciliary and suprachoroidal spaces, and eventually, the choroidal and scleral vasculature. The prevailing dogma has been that the uveoscleral outflow is responsible for a smaller percentage of the total elimination pathway. More recently, the uveoscleral outflow route has gained more attention as it has been shown that this pathway is much more important than initially thought.8 Thus, increased interest has arisen in developing devices targeting this space.
The uveoscleral pathway may contribute roughly 10–60% of total aqueous outflow in human eyes and is relatively pressure-independent.8–11 In fact, in glaucomatous patients, the contribution of the uveoscleral pathway is thought to be higher as there is possibly redirection from the conventional drainage pathway.12 Age has also been demonstrated to play a significant role in uveoscleral drainage, and previous studies demonstrated that young individuals have a higher uveoscleral flow than older ones.8 The ciliary muscle constitutes an important factor determining outflow resistance, and changes in its state of contraction directly influence total uveoscleral flow.13
Anteriorly in the eye, the supraciliary space is located between the ciliary body’s outer surface and the sclera’s inner surface. As this space extends posteriorly and becomes the space between the choroid and the internal surface of the sclera, it is termed the suprachoroidal space. This was considered a potential space that only became visible or accessible in pathologic conditions; however, recent advances in ocular imaging allowed for better visualization of the suprachoroidal space.14 The layers that compose the suprachoroidal space in normal individuals are approximately 35 μm thick and contribute to IOP control by regulating choroidal protein flow through the sclera forming the uveoscleral outflow tract.15 Thus, the supraciliary/suprachoroidal space is a potential target for surgical treatment of glaucoma as it can increase aqueous humour drainage by enhancing the natural uveoscleral outflow pathway.16
Although a few ab interno supraciliary MIGS devices have been commercialized or are in development, targeting the supraciliary space pathway is not a new concept. In the early 1900s, the creation of a cyclodialysis cleft to surgically control intraocular pressure in patients with glaucoma was reported.17 Despite lowering IOP, this procedure was not widely implemented as it was associated with prolonged hypotony and IOP spikes following spontaneous cleft closure.18 With the advent of MIGS, there has been a renewed interest in exploring this route in a safer and more predictable way. The advantage of targeting the uveoscleral pathway through an ab interno approach is sparing conjunctiva and allowing “blebless” surgery, thus avoiding bleb-related complications. IOP elevation in the weeks after implantation should still be observed. This could be related to the closing of the induced cyclodialysis cleft, which usually responds well to IOP-lowering medication.
The CyPass Micro-stent (Alcon, Fort Worth, Texas, USA) was the first ab interno supraciliary device approved by the FDA. A 1-year result of standalone CyPass implantation showed an IOP reduction of 34.7%, with an average reduction of 0.8 medications per subject.19 The 2-year COMPASS results showed sustained IOP reduction with significantly more micro-stent subjects (77%) than controls (60%) achieving a 20% reduction in unmedicated diurnal IOP (p = 0.002). Mean unmedicated IOP reduction from washed-out baseline was 7.4 mmHg for the micro-stent group versus 5.4 mmHg in controls (p < 0.001), with 85% of micro-stent subjects not requiring IOP medications at 24 months. Analysis of the 5-year COMPASS-XT trial showed significantly more patients with endothelial cell loss (ECL) >30% in the cataract surgery combined with Cypass group (27.2%) than the group of cataract surgery standalone (10.0%). These results led to Alcon’s voluntary global market withdrawal of the micro-stent due to safety concerns.20,21
The MINIject
Technical Specifications
MINIject (iSTAR Medical, Wavre, Belgium) is a 5 mm length microinvasive glaucoma drainage implant that targets the supraciliary pathway of aqueous humor drainage. The implant has an oblong cross-sectional shape measuring 1.1 mm x 0.6 mm, with a green-coloured ring positioned at 0.25 mm from the tip of the device to help with implant placement. The device provides a controlled fluid path for the aqueous humor to drain from the AC to the suprachoroidal space (Figure 1). The implant is made of STAR® material, a soft, biocompatible, non-degradable, medical-grade silicone that conforms to the eye anatomy as an organized network of hollow spheres, creating a porous geometry (Figure 2). Each MINIject has approximately 180,000 hollow pores in it. Thus, about two-thirds of the implant is empty space, and the other one-third is silicone. It has been shown that there is very little fibrotic encapsulation surrounding the implant.22 Each pore size is uniformly 27µm. This porous design encourages a natural flow speed, minimizing fibrosis and maintaining implant performance. Over time, the bio-integration of surrounding tissue into the implant’s porous material sustains drainage efficacy, mimicking the natural flow of fluid.22 The device obtained CE marking in November 2021 and an FDA investigational device exemption (IDE) clinical trial, STAR-V, has commenced enrollment.
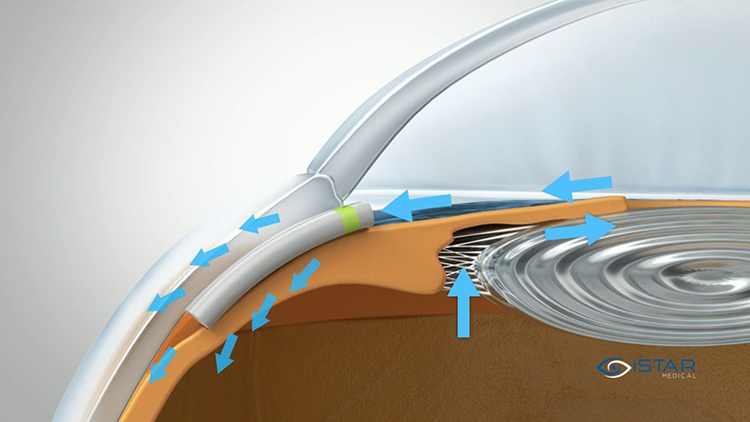 |
Figure 1 Schematic of the device in situ. © iSTAR Medical. |
 |
Figure 2 MINIject device made of STAR material that is composed of an organised network of hollow spheres, creating a porous geometry. © iSTAR Medical. |
Surgical Technique
The MINIject is indicated in adult patients with open-angle glaucoma. Anesthesia can be done according to surgeon preference, but a sub-tenon or retro/peribulbar block is usually recommended to enhance patient comfort. Ensure that the patient’s head position and microscope tilt angle allow sufficient gonioscopic visualization of the iridocorneal angle. The MINIject implant comes preloaded in a transparent sheath which is then to be connected to a handle (Figure 3). Sliding the wheel on the handle allows for precise and intuitive positioning of the MINIject implant via an ab interno procedure. A 2.0 mm temporal clear corneal incision 1.5 mm anterior to the limbus is recommended to allow for an adequate approach angle into the supraciliary space. Intraoperative miotics are recommended. The AC should be filled with cohesive ophthalmic viscosurgical device (OVD, 1.4% or 1.8%, Healon GV® or Healon GV® PRO recommended), and additional OVD should be used as necessary to maintain a deep and stable AC during the implantation process.
 |
Figure 3 The MINIject implant comes preloaded in a transparent sheath which is then connected to a handle. © iSTAR Medical. |
Immediately before entering into the AC with the device, the delivery tool safety lock should be unlocked, and the roller wheel maintained in the forward position until the desired implant location is reached. The distal sheath is inserted into the AC towards the nasal angle. Using a gonioprism to visualize the angle, the flexible sheath is gently advanced between the scleral spur and the ciliary body (Figure 4), then into the supraciliary space by allowing the sheath to glide along the sclera (“hugging the sclera”). The delivery sheath is advanced within the suprachoroidal space until the middle of the green coloured ring on the implant is aligned with the scleral spur (Figure 5). The implant is released by slowly rolling the wheel backwards (towards the surgeon) in several motions until a mechanical stop is reached, as this will retract the sheath and lay the implant in place (Figure 6).
 |
Figure 4 Schematic showing the flexible sheath gently being advanced in between the scleral spur and the ciliary body while visualizing the angle with a gonioprism. © iSTAR Medical. |
 |
Figure 5 Image showing the delivery sheath being advanced within the suprachoroidal space until the middle of the green coloured ring on the implant is aligned with the scleral spur. © iSTAR Medical. |
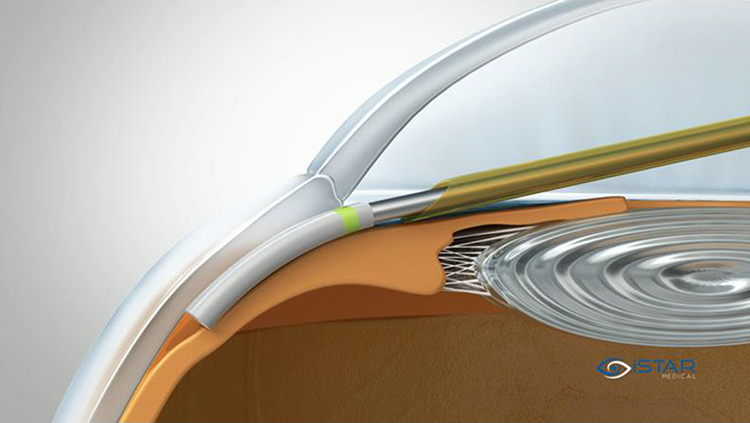 |
Figure 6 Image illustrating the implant being released. © iSTAR Medical. |
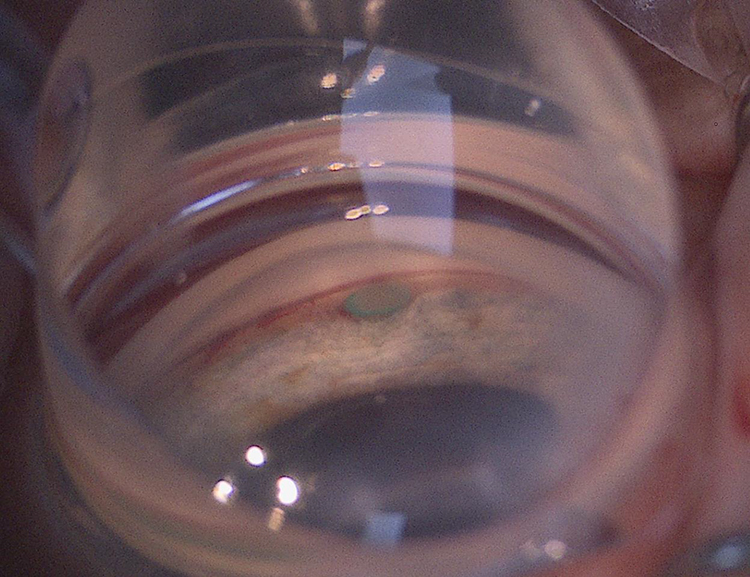 |
Figure 7 Image illustrating the device correctly placed with the green-coloured ring at the level of the scleral spur. Image courtesy of Mr Chrysostomos Dimitriou (United Kingdom). |
The correct implantation of the device should be verified by gonioscopic examination. The mid-portion of the green-coloured ring should be at the level of the scleral spur (Figure 7). At this point, only 0.5mm of the device remains in the AC. Complete removal of OVD should be performed.
Peer-Reviewed Publications to Date
Published data include pre-clinical studies in rabbits and two human trials in predominantly mild-to-moderate glaucoma patients (~90% of patients treated in clinical studies were classified as having mild-to-moderate glaucoma). The STAR-I trial was the first-in-human trial, conducted in Panama and India, and the STAR-II trial that followed was a European trial in Germany, France, and Spain. Summary of MINIject safety and efficacy data are presented in Table 1.
 |
Table 1 Summary of MINIject Safety and Efficacy Data |
STAR- I Trial (6-Month Data)
In 2019, Denis et al23 reported on a prospective, multicenter, interventional, and single-arm study to demonstrate the safety and efficacy of MINIject (STAR-I). This study focused on eyes with open-angle glaucoma uncontrolled by topical hypotensive medications and 25 eyes were treated. It was demonstrated that MINIject was able to significantly lower IOP and eliminate the need for medication in most patients six months after surgery when implanted as a standalone procedure. At the onset of the trial, mean medicated diurnal IOP at baseline was 23.2 (±0.6) mmHg (±standard error), and this decreased at six months to 14.2 (±0.9) mmHg – representing a reduction of 9.0 mmHg or 39.1% (p < 0.0001). In addition, IOP lowering medications decreased from 2.0 (±1.1) (±standard deviation) classes per eye at baseline to 0.3 (±0.7) classes at six months. Of note, 87.5% of patients were medication-free, and 95.8% achieved a minimum 20% IOP reduction from baseline at six-month follow-up. Interestingly, there were no white persons included in this study, and non-white ethnicity is a known risk factor for glaucoma surgery failure.24 There was also a favourable safety profile with no ocular serious adverse events reported, no eye requiring a secondary surgical procedure for complications or failure, and no device-related adverse events. Furthermore, mean endothelial cell density (ECD) was constant comparing baseline (2411 cells/mm2) with 6-month (2401 cells/mm2) results. However, of note, a six-month follow-up is generally considered insufficient to adequately evaluate corneal ECD loss. The authors noted that the IOP reduction in this study was numerically greater or similar to published six and twelve-month outcomes with other bleb-free, ab interno standalone MIGS procedures.
STAR-II Trial (6-Month Data)
In 2020, Garcia-Feijoo et al25 reported on a prospective, multicenter, interventional, and single-arm study to investigate the safety and efficacy profile of MINIject in European centres (STAR-II). This study focused on eyes with primary open-angle glaucoma uncontrolled by topical glaucoma medications and enrolled 31 eyes. The primary endpoint for this study was a responder analysis of success >60% at 6 months. Success was defined as diurnal IOP between 5 and 21 mmHg with at least 20% reduction in diurnal IOP, regardless of medication use. At the six-month follow-up, the primary endpoint was met in 75.9% (22/29) patients. Mean IOP decreased from a medicated baseline of 24.6 (±3.8) mmHg to 14.7 (±6.0) mmHg representing a 9.9 mmHg or 40.2% reduction (p < 0.0001). Moreover, IOP-lowering medications decreased from 2.9 (±1.2) classes per eye at baseline to 1.0 (±1.3) classes or a 63.4% reduction in medications at six months. Furthermore, there was no demonstrable significant mean decrease in corneal central ECD from 2235±419 cells/mm2 to 2120±467 cells/mm2. These results were comparable to the STAR-I trial, although, in this study, additional incisional glaucoma surgery was required in 9.7% of patients. Finally, two cases were aborted intraoperatively due to difficulties in delivering the MINIject via a dual-operator delivery tool. Feedback from this trial led to the development of a single-operator delivery tool to be used in future studies. Some mechanical improvements included modifying the tip shape, improving handle ergonomics, enhancing the packaging of the sheath to decrease implant movement during transportation, and increasing operator control during implant release. The implant itself remains the same.
STAR-I Trial (2-Year Data)
In 2020, Denis et al26 published a two-year follow-up in 21 patients from the initial cohort of 25 treated patients in the STAR-I trial. At the beginning of the trial, mean medicated baseline IOP was 23.2 (±2.9) mmHg which decreased to 13.8 (±3.5) mmHg after two years, representing a −40.7% reduction in IOP. Also, IOP lowering medications decreased from 2.0 (±1.1) classes per eye at baseline to 1.0 (±1.3) classes at two years post-implantation. Overall, all patients achieved a 20% IOP reduction, with 48% of patients remaining medication-free at two years. Of note, no serious ocular adverse events or secondary surgeries required for glaucoma management or device-related complications were reported. The ocular adverse events occurring in less than one-third of patients were mostly transient inflammation and IOP elevation. Mean ECD mildly decreased by 5% for matched eyes (2411 cells/mm2 to 2341 cells/mm2), with no patient having greater than 30% central ECD loss. The authors noted that the minimal ECD loss after 2 years might be due to MINIject’s soft and conforming material, and its design which reduces the amount of material in the AC. Finally, quality of life questionnaires showed a reduction or absence in all ocular symptoms representing a significant improvement in patient’s quality of life. The authors once again noted that the IOP and medication reduction in this study were comparable to other standalone MIGS devices targeting Schlemm’s canal or the supraciliary space.
Pre-Clinical Studies
The formation of low-permeability fibrous tissue around glaucoma implants represents a major challenge in delivering long-term IOP reduction. In 2020, Grierson et al22 performed an in vivo study in rabbit eyes to assess the ocular biocompatibility and tissue integration of MINIject. Overall, no biocompatibility issues were identified through the six post-operative months in two rabbit studies. Histological analysis through the six post-operative months showcased that the implant was well tolerated, despite the rabbit model being renowned for its aggressive inflammatory response.22 Minimal fibroplasia and encapsulation were observed, with the implant becoming rapidly colonized by macrophages only via cell migration. No evidence of fibrosis or dense connective tissue, which would limit aqueous humor passage, or device degradation were observed. Clinical evaluation between the sham and test groups was similar, suggesting any reactions were due to the ab-externo surgical technique necessary in this rabbit model, rather than the MINIject implant. Time-point analysis demonstrated that the pore colonization, once established by 1 month, was stable throughout the study. Taken together, the minimal fibrous encapsulation and stable cellular pore colonization point toward the implant’s longevity in delivering long-term IOP lowering.
Ongoing Trials and Interim Results
STAR-I Trial (3 Year Data)
In 2021, a three-year follow-up from the initial cohort of the STAR-I trial was presented at the 2021 World Glaucoma Congress.27 Preliminary results showcased a sustained IOP reduction of 36% from 22.6 (±2.1) mmHg at baseline to 14.4 (±3) mmHg at three-years post-implantation. In addition, there was a reduction in the number of IOP lowering medications from 1.5 classes per eye at baseline to 0.9 classes at the three-year interval. In terms of success rates, 86% of patients achieved an IOP reduction ≥20% from baseline and 86% achieved IOP ≤18mmHg at three years. Mean corneal ECD loss at the three-year interval was 4.5%, with no patient reporting a greater than 30% corneal ECD loss to date. Of note, this dataset was extracted from a single-centre, and, given the global disruption of the COVID-19 pandemic, data collection and analyses from other centres were impeded. Only 14 eyes of the 25 initial eyes were captured in this data analysis. Further data collection and analysis from other sites are expected at the four-year interval.
STAR-II Trial (2 Year Data)
Preliminary two-year follow-up data from the STAR-II trial of the initial 29 eyes were presented at the 2021 American Academy of Ophthalmology.28 Results of 27 eyes demonstrated an IOP reduction of 36.3% from 24.6 (±3.7) mmHg at baseline to 15.5 (±6.6) mmHg at the final follow-up visit at two years. Likewise, there was a reduction in the number of IOP lowering medications from 2.9 per eye at baseline to 1.4 at the two-year interval. Success, defined as IOP≤ 21mmHg and >5mmHg with ≥20% reduction from baseline, was achieved in 78% of patients. Finally, utilizing ultrasound biomicroscopy, no implant migration was observed at the twelve-month follow-up.
Pooled Data for Mean Corneal ECD
The corneal endothelial maintains stromal hydration via active pump functions and its barrier, thereby ensuring corneal clarity.29 Loss of corneal endothelial cells is irreversible and results in corneal edema and bullous keratopathy, which in turn reduces corneal transparency and decreases visual acuity. Increasing evidence demonstrates that corneal endothelial loss is associated with glaucoma either through elevated IOP and direct mechanical compression, cellular toxicity associated with long-term exposure to preservatives in IOP-lowering medications, and intraocular surgery.30–32 Of note, recent studies have shown patients with POAG and normal-tension glaucoma have lower corneal endothelial cell densities compared to healthy controls, further highlighting the importance of minimizing any further loss due to intra-ocular surgeries.30,32
Pooled data across the STAR-I, II and III trials of 41 eyes at the two-year interval demonstrated a mean central ECD loss of 6% from baseline. For standalone glaucoma procedures, like Preserflo (Santen Inc., FL, USA) and trabeculectomy, the mean ECD loss ranges from 5.2% to 6.9% at one year.33 At the two-year interval, there were no MINIject patients with a mean ECD loss of greater than 30%.28 In contrast, when comparing ECD loss in the COMPASS (CyPass), HORIZON (Hydrus), and iStent pivotal trials at two years, the percentage of patients with mean ECD loss >30% ranged from 7.2% to 13.6%, depending on whether cataract surgery was performed alone or combined with MIGS.34–36 The COMPASS-XT trial found a correlation between device placement in the AC and ECL. The greater the length of the device in the AC, the greater ECL was noticed. When the CyPass device was placed in its ideal position (no retention rings visible), the ECL rate was similar to controls. The Cypass stiffness could also have contributed to ECL, assuming that the device would be located closer to the peripheral cornea due to the more vertical orientation in the angle.21 One of the advantages of the MINIject is the soft material that easily conforms to the eye anatomy and follows the curvature of the inner sclera. Also, the device is only 0.5 mm in the AC, with the green-coloured ring positioned at the level of the scleral spur. Issues regarding ECL are likely not a supraciliary space issue in general, but rather device design and positioning related.
Conclusion
With the advent of MIGS, the suprachoroidal space has regained increased interest as a route for glaucoma surgery. Targeting the uveoscleral pathway with the MINIject implant through an ab interno approach provides an opportunity for lowering IOP by using a presumably efficient and secure outflow route with a more predictable and safer result. Long-term studies with a bigger sample size are still warranted to evaluate the safety and durability of the effect and compare short- and long-term outcomes of this procedure.
Avoiding subconjunctival filtration blebs is one of the main advantages of these procedures, thus reducing patient recovery time and eliminating bleb-related complications. Clinical studies have shown promising IOP lowering results with the MINIject implant, predominantly in patients with mild to moderate glaucoma with a potentially safer and less invasive approach than traditional glaucoma surgeries. With these encouraging results, this area of glaucoma treatment warrants further research towards more long-term data, as well as results in patients with severe glaucoma, to further characterize the efficacy and safety profile of this device.
Acknowledgement
The authors acknowledge Mr Chrysostomos Dimitriou (Colchester Eye Centre, Essex, UK) for supplying the case image for Figure 7, and thank Katherin Awad BSc MBA for editorial support.
Funding
There were no fees or grants received for this study.
Disclosure
Dr Ticiana De Francesco is a consultant for Abbvie; Glaukos; Carl Zeiss, Elios Vision, Glaukos, Iantrek, NovaEye, Myra Vision. Dr Iqbal Ike K Ahmed is a consultant for iSTAR Medical, grants and/or personal fees from Aequus, Ace Vision, Aerie Pharmaceuticals, Akorn, Alcon, Allergan, Aquea Health, Inc, ArcScan, Avellino Lab USA, Inc, Avisi, Bausch Health, Beaver Visitec, Beyeonics, Bionode, Carl Zeiss Meditec, Centricity Vision, Inc, CorNeat Vision, Custom Surgical, Elios Vision, ElutiMed, Equinox, eyeFlow, Inc, EyeMed, EyeQ Technologies, Exhaura Limited, Genentech, Glaukos, Gore, Heine, Heru, Iantrek, InjectSense, Iridex, iCare, iStar, grants, Ivantis, Johnson & Johnson Vision, Labtician Thea, LayerBio, Leica Microsystems, Life Long Vision, Long Bridge Medical, Inc, MicroOptx, MST Surgical, Myra Vision, New World Medical, NovaEye, Ocular Instruments, Ocular Therapeutix, Oculo, Oculus Surgical, Omega Ophthalmics, PolyActiva, PulseMedica, Radiance Therapeutics, Inc, Radius XR, Rheon Medical SA, Ripple Therapeutics, Sanoculis, Santen, Shifamed, LLC, Sight Sciences, Smartlens, Inc, Stroma, Thea Pharma, TFS Health Science, ViaLase, Visus Therapeutics, Vizzario, VSY Biotechnology, and Zilia, Inc, outside the submitted work.
References
1. Jonas JB, Aung T, Bourne RR, Bron AM, Ritch R, Panda-Jonas S. Glaucoma. Lancet. 2017;390(10108):2183–2193. PMID: 28577860. doi:10.1016/S0140-6736(17)31469-1
2. Heijl A. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268. doi:10.1001/archopht.120.10.1268
3. Agis Investigators. The advanced glaucoma intervention study (AGIS): 7. the relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/S0002-9394(00)00538-9
4. Saheb H, Ahmed IIK. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–104. doi:10.1097/ICU.0b013e32834ff1e7
5. European Glaucoma Society. Terminology and Guidelines for Glaucoma.
6. De Francesco T, Ahmed IIK. An overview on options in glaucoma surgery. Glaucoma Now; 2021.
7. Moisseiev E, Loewenstein A, Yiu G. The suprachoroidal space: from potential space to a space with potential. Clin Ophthalmol. 2016;10:173–178. PMID: 26869750; PMCID: PMC4734808. doi:10.2147/OPTH.S89784
8. Toris CB, Yablonski ME, Wang Y-L, Camras CB. Aqueous humor dynamics in the aging human eye. Am J Ophthalmol. 1999;127(4):407–412. doi:10.1016/S0002-9394(98)00436-X
9. Weinreb RN. Uveoscleral outflow: the other outflow pathway. J Glaucoma. 2000;9(5):343–345. doi:10.1097/00061198-200010000-00001
10. Bill A, Phillips CI. Uveoscleral drainage of aqueous humour in human eyes. Exp Eye Res. 1971;12(3):275–281. doi:10.1016/0014-4835(71)90149-7
11. Weinreb RN, Toris CB, Gabelt BT, Lindsey JD, Kaufman PL. Effects of prostaglandins on the aqueous humor outflow pathways. Surv Ophthalmol. 2002;47:S53–S64. doi:10.1016/S0039-6257(02)00306-5
12. Shaarawy T, Gigon A. The suprachoroidal route in glaucoma surgery. J Curr Glaucoma Pract. 2016;10(1):13–20. doi:10.5005/jp-journals-10008-1197
13. Bill A. Effects of atropine and pilocarpine on aqueous humour dynamics in cynomolgus monkeys (Macaca irus). Exp Eye Res. 1967;6(2):120–125. PMID: 4960736. doi:10.1016/s0014-4835(67)80062-9
14. Emami-Naeini P, Yiu G. Medical and surgical applications for the suprachoroidal space. Int Ophthalmol Clin. 2019;59(1):195. doi:10.1097/IIO.0000000000000251
15. Bryce C, Hwan Jung J, Prausnitz MR. The suprachoroidal space as a route of administration to the posterior segment of the eye. Adv Drug Deliv Rev. 2018;126:58–66. doi:10.1016/j.addr.2018.03.001
16. Figus M, Posarelli C, Passani A, et al. The supraciliary space as a suitable pathway for glaucoma surgery: ho-hum or home run? Surv Ophthalmol. 2017;62(6):828–837. doi:10.1016/j.survophthal.2017.05.002
17. Heine L. Die Cyclodialyse, eine neuen Glaukomoperation. Med Wochenschr. 1905;31:824–826.
18. Goldmann H. Uber die wirkungsweise der cyclodialyse. Ophthalmologica. 1951;121:94–100. doi:10.1159/000300942
19. García-Feijoo J, Rau M, Grisanti S, et al. Supraciliary micro-stent implantation for open-angle glaucoma failing topical therapy: 1-year results of a multicenter study. Am J Ophthalmol. 2015;159(6):1075–1081.e1. PMID: 25747677. doi:10.1016/j.ajo.2015.02.018
20. Vold S, Ahmed II, Craven ER, et al; CyPass Study Group. Two-year COMPASS Trial results: supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology. 2016;123(10):2103–2112. PMID: 27506486. doi:10.1016/j.ophtha.2016.06.032
21. Lass JH, Benetz BA, He J, et al. Corneal endothelial cell loss and morphometric changes 5 years after phacoemulsification with or without CyPass micro-stent. Am J Ophthalmol. 2019;208:211–218. PMID: 31377278. doi:10.1016/j.ajo.2019.07.016
22. Grierson I, Minckler D, Rippy MK, et al. A novel suprachoroidal microinvasive glaucoma implant: in vivo biocompatibility and biointegration. BMC Biomed Eng. 2020;2(1):10. doi:10.1186/s42490-020-00045-1
23. Denis P, Hirneiß C, Reddy KP, et al. A first-in-human study of the efficacy and safety of MINIject in patients with medically uncontrolled open-angle glaucoma (STAR-I). Ophthalmol Glaucoma. 2019;2(5):290–297. doi:10.1016/j.ogla.2019.06.001
24. Martin MJ, Summer A, Gold EB, et al. Race and primary open-angle glaucoma. Am J Ophthalmol. 1985;99(4):383–387. doi:10.1016/0002-9394(85)90001-7
25. García Feijoó J, Denis P, Hirneiß C, et al. A European study of the performance and safety of MINIject in patients with medically uncontrolled open-angle glaucoma (STAR-II). J Glaucoma. 2020;29(10):864–871. doi:10.1097/IJG.0000000000001632
26. Denis P, Hirneiß C, Durr GM, et al. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br J Ophthalmol. 2022;106(1):65–70. doi:10.1136/bjophthalmol-2020-316888
27. Ahmed I Three-year results of a supraciliary drainage device in patients with open angle glaucoma.
28. Singh I, Denis P, Hirneiß C, et al. A European study of the efficacy and safety of a supraciliary glaucoma drainage device in patients with open angle glaucoma (STAR-II).
29. Zi-Yan Y, Wu L, Qu B, et al. Changes in corneal endothelial cell density in patients with primary open-angle glaucoma. World J Clin Cases. 2019;7(15):1978–1985. doi:10.12998/wjcc.v7.i15.1978
30. Kim KN, Lee SB, Lee YH, et al. Changes in corneal endothelial cell density and the cumulative risk of corneal decompensation after Ahmed glaucoma valve implantation. Br J Ophthalmol. 2016;100(7):933–938. doi:10.1136/bjophthalmol-2015-306894
31. Cho SW, Kim JM, Choi CY, et al. Changes in corneal endothelial cell density in patients with normal-tension glaucoma. Jpn J Ophthalmol. 2009;53(6):569–573. doi:10.1007/s10384-009-0740-1
32. Setälä K. Corneal endothelial cell density after an attack of acute glaucoma. Acta Ophthalmol. 2009;57(6):1004–1013. doi:10.1111/j.1755-3768.1979.tb00531.x
33. Summary of safety and effectiveness data compass data. The FDA; 2016. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150037B.pdf.
34. Summary of safety and effectiveness data Hydrus data. The FDA; 2018. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf17/P170034B.pdf.
35. Summary of safety and effectiveness data iSTENT data. The FDA; 2018. Available from: http://www.accessdata.fda.gov/cdrh_docs/pdf17/P170043B.pdf.
36. Oddone F, Roberti G, Posarelli C, et al. Endothelial cell density after XEN implant surgery: short-term data from the Italian XEN glaucoma treatment registry (XEN-GTR). J Glaucoma. 2021;30:559–565. doi:10.1097/IJG.0000000000001840
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Combined MIGS: Comparing Additive Effects of Phacoemulsification, Endocyclophotocoagulation, and Kahook Dual Blade
Oberfeld B, Golsoorat Pahlaviani F, Hall N, Falah-Trzcinski H, Trzcinski J, Chang T, Solá-Del Valle D
Clinical Ophthalmology 2023, 17:1647-1659
Published Date: 8 June 2023