Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Support Needs of Patients with Chronic Obstructive Pulmonary Disease (COPD) and Asthma Throughout Their Patient Journey: A Qualitative Study
Authors Almonacid C ![]() , Gómez R, Morán I, Muerza I, Pastor M, Garcia-Esparcia P, García E, Soria C
, Gómez R, Morán I, Muerza I, Pastor M, Garcia-Esparcia P, García E, Soria C ![]() , Lázaro E
, Lázaro E ![]() , Querol D
, Querol D
Received 26 March 2025
Accepted for publication 20 July 2025
Published 28 July 2025 Volume 2025:20 Pages 2639—2658
DOI https://doi.org/10.2147/COPD.S526548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Fanny Wai San Ko
Carlos Almonacid,1 Raquel Gómez,2 Ignacio Morán,3 Irantzu Muerza,4 Mariano Pastor,3 Paula Garcia-Esparcia,5 Elena García,5 Cristina Soria,6 Esther Lázaro,6,7 Dolors Querol5
1Departamento de Neumología, Hospital Puerta de Hierro Majadahonda, Madrid, España; 2Asociación Sevilla Respira, Sevilla, España; 3Fundación Española de Asociaciones de Pacientes Alérgicos y con Enfermedades Respiratorias (FENAER), Madrid, España; 4Asociación de Apoyo a Personas Afectadas por el Asma de Bizkaia (ASMABI), Bilbao, España; 5Departamento Médico, Chiesi, España; 6Psicología de la Salud, Suportias, Madrid, España; 7Facultad de Ciencias de la Salud, Universidad Internacional de Valencia, Valencia, España
Correspondence: Esther Lázaro, Health Faculty, Valencian International University, Pintor Sorolla 21, Valencia, 46002, Spain, Email [email protected]
Purpose: Chronic respiratory diseases, such as chronic obstructive pulmonary disease (COPD) and asthma, pose a significant health risk due to the increasingly pronounced rise in its prevalence, associated complications and impact on patients’ quality of life. The aim of this study is to analyse the needs of patients with COPD and asthma throughout their patient journey.
Patients and Methods: To this end, a qualitative and cross-sectional study was conducted based on interviews and focus groups. 28 people took part, including patients, relatives and representatives of patient associations, and they were selected to ensure a diversity of perspectives. The data collected were analyzed by two psychologists with experience in qualitative research, who conducted thematic analysis and made use of data saturation criteria.
Results: The results emphasize that patient needs vary according to the stage of the disease. In the initial stage, patients find it difficult to identify symptoms and risk factors, and demand education on basic concepts and self-care strategies. When diagnosed, they require psycho-emotional support and training on the disease. Insufficient information, particularly concerning the use of inhalers and the different therapies, is a recurrent obstacle in treatment and monitoring. Furthermore, therapeutic nonadherence is affected by factors such as perception of the severity of the disease, related to the treatment and deficiencies in inhaler technique. Additionally, pulmonary rehabilitation and multidisciplinary care are unmet needs that have an impact on patients’ quality of life.
Conclusion: The study highlights the importance of personalizing interventions according to the stage of the patient journey, combining education, disease coping strategies and comprehensive monitoring. Patient groups play a key role as they are a source of emotional support, guidance and self-care. In conclusion, a proposal is made for a patient-centred approach that promotes self-management, equitable access to resources and coordination between healthcare teams to optimise integrated care in respiratory diseases. In this respect, it seems relevant and appropriate to develop training environments for patients diagnosed with asthma/COPD and their carers, where information and training are offered to support good disease management in the different stages of the patient journey.
Keywords: chronic obstructive pulmonary disease, COPD, asthma, patient journey, qualitative study
Introduction
Chronic respiratory diseases pose a significant health risk due to the increase in their prevalence and associated complications.1 In 2017, almost 545 million people worldwide had a chronic respiratory disease, which represents an increase of 39.8% compared with 1990.2 This is the case for chronic obstructive pulmonary disease (COPD), for example, which has become the fourth leading cause of death in the world.3 Furthermore, asthma is a major disease, with an estimated global population of 262 million people.2,4,5 Both COPD and asthma are two highly prevalent respiratory diseases which are characterised by airflow obstruction. Although different etiopathogenic mechanisms and varying levels of response to treatment are observed, in clinical practice, there are clinical presentations that overlap in both diseases.6 Asthma is reversible with optimized treatment, and disease control typically has less impact on one’s social life and overall journey. In contrast, COPD is irreversible, progressively worsening, and has a more significant and lasting impact on daily life. Patients with these respiratory diseases often experience heterogeneous and unpredictable development, which at times may give rise to a worsening of their health, a variety of symptoms such as dyspnoea and associated comorbidities, and the presence of sudden and potentially serious exacerbations.7 The presence of symptoms is associated with worse health status, depression, anxiety and poor sleep quality.8,9
It is important to consider unmet needs or any needs that individuals themselves do not recognise and that may cause a significant emotional impact, feelings of vulnerability and social isolation, which may interfere in their ability to efficiently manage the disease.10 As the disease progresses, physical, emotional, occupational and social complications may become more common and complex, resulting in a decline in these individuals’ health-related quality of life according to the specific symptomatology of each patient.11 Furthermore, as these are chronic diseases, patients must follow treatment advice and specific measures for self-management of symptoms and adherence to treatment.12–15
Throughout the disease process, supporting people diagnosed with COPD or asthma calls for in-depth knowledge about their experiences and needs from a broad perspective. This patient perception may be assessed using qualitative tools based on thematic analysis, by means of which narratives are collected on patients’ quality of life in relation to health.16 Said narratives may be reflected in a patient journey which includes their experiential process throughout the different stages of the disease, covering risk factors, diagnosis, treatment and monitoring.17 Patient journey mapping is an increasingly common approach for evaluating individuals’ experiences within the healthcare system. This study adopts the patient journey framework, a theoretical lens that maps the experiential process of individuals across distinct stages, such as risk factor identification, diagnosis, treatment, and monitoring to comprehensively understand their evolving needs and interactions with the healthcare system.18,19 Patients and their families are the only parties that experience the whole process, connecting each step of the journey. In this respect, understanding the patient pathway may make it easier to implement actions aimed at ensuring that the healthcare system is able to offer better healthcare by redesigning services based on the real needs of patients.20,21
In scientific literature, an increase is observed in studies focused on evaluating patients’ needs through the patient journey in the healthcare field in general18 and in respiratory diseases in particular.17 However, there are no studies that cover the needs of two of the most highly prevalent groups of respiratory diseases, COPD and asthma, or, furthermore, that describe not only the narratives of patients, but also of PAG (Patient Advocacy Group) representatives and relatives. Hence this article is focused on describing the needs of patients with chronic obstructive pulmonary disease and asthma throughout their patient journey.
Materials and Methods
The participants signed the informed consent document and were recruited voluntarily through an association of individuals with COPD or asthma. The guidelines outlined in the Declaration of Helsinki were followed.
In total, 28 people took part in the research, and they were selected to ensure that each subgroup of interest was represented. Data saturation was achieved after the final focus group in November 2023. Saturation was determined when no new themes emerged from the thematic analysis conducted by the two psychologists, ensuring comprehensive coverage of patient, relative, and representative perspectives. Participants were split up into several subgroups, in accordance with a methodological approach of data triangulation.22 All participants were informed of the aims and grounds of the research, and each participant signed the informed consent form. None of the people who were asked to take part refused to do so. The three collection methods were as follows: individual telephone interviews, a patient focus group and another focus group of patient group representatives (see Table 1) In this context, we refer to individuals who hold an official representative role within patient organizations. These participants were not included solely based on their personal experience with the condition, but were invited in their capacity as spokespersons or advocates representing the views and interests of a broader patient community. Research was conducted during the period between December 2021 and November 2023. Only participants and researchers were present in the sessions, and there was no pre-existing relationship between them, except for the PAG. For each method, the researchers had a protocol of semi-structured questions, which were organised so as to collect information on needs and factors concerning quality of life related to health. No identifying data was collected from the participants in the interviews.
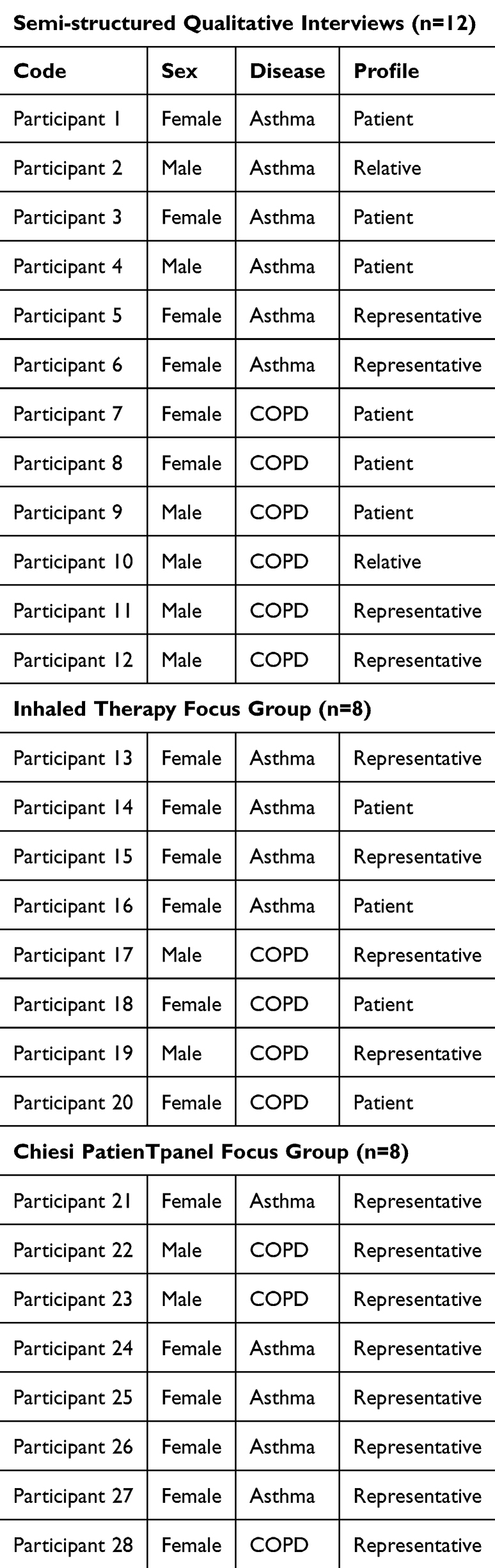 |
Table 1 Description of the Participants in the Study |
Individual interviews with patients, relatives and representatives of groups of patients with COPD and asthma were conducted in December 2021 by telephone. Participants were recruited in collaboration with different national associations (Table 1).
The aforementioned interviews were carried out from a semi-structured qualitative perspective and were conducted by a health psychologist with experience in qualitative research and in respiratory health (CS), with no additional observers present, ensuring a focused and confidential interaction between the researcher and participants. Each interview lasted approximately 60 minutes. As shown in Table 1, a total of 12 patients took part. In the group diagnosed with asthma, 2 men and 4 women participated, with an average age of 56 years and for whom between 3 and 59 years had passed since diagnosis. The COPD group was made up of 4 men and 2 women, with an average age of 60 years and for whom between 5 and 21 years had passed since diagnosis.
Furthermore, the focus group of patients diagnosed with COPD and asthma, held in April 2023, concentrated on establishing a joint reflection to explore the needs and indicators of nonadherence to inhaled therapy from the point of view of patients, as well as possible tools that may improve adherence in this patient group. This specific group focused on analysing the needs related to the treatment phase of the patient journey. Patients were recruited via the groups ASMABI, ASMAMADRID and EPOC España. A total of 4 people diagnosed with asthma and 4 people diagnosed with COPD took part, of whom 6 were female and 2 were male. This took place online using the Microsoft Teams conference call system (Microsoft Corporation, Redmond, USA) and lasted two and a half hours.
Lastly, a focus group was held to identify the needs of patient groups/federations in the various stages of the patient journey in November 2023. It was exclusively made up of patient group representatives, in particular, 5 representatives of asthma patient groups and 3 representatives of COPD patient groups. It took place in person and lasted two and a half hours. Various groups and federations were involved (Table 1).
Focus groups were conducted by a health psychologist and an observer with experience in qualitative health research. In all groups, the inclusion criteria were as follows: patients of legal age; patients diagnosed with asthma or patients diagnosed with COPD; availability to be interviewed by telephone or attend a meeting in person/online; consent to participate and for interviews to be recorded for analysis purposes. Furthermore, in the focus group, all patients had to have been prescribed an inhaled maintenance therapy. The following were considered to be exclusion criteria: patients who did not wish to take part in the study or who were unable to contribute to the collection of necessary information (psychological disorders, non-collaboration, limited understanding of language).
The data were recorded, transcribed and subsequently analysed by two health psychologists with experience in qualitative research, who conducted thematic analysis and made use of data saturation criteria as a key factor for analysis.16 We conducted a thematic analysis using a deductive approach, guided by the Patient Journey Framework developed by Scichilone et al17 which maps the experience of patients with COPD across different disease stages. This framework was selected for its relevance in capturing the evolving needs of patients through diagnosis, treatment, and follow-up.
To ensure methodological rigour and transparency, we followed Braun and Clarke’s six-phase method for thematic analysis16 and adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Table 2). Thematic analysis was deductive and derived from a pre-existing theoretical framework which was used as a guide for the identification and analysis of themes. Data from interviews and both focus groups were transcribed verbatim and analysed together to identify cross-cutting themes while preserving subgroup distinctions (eg, patients, relatives, and representatives).
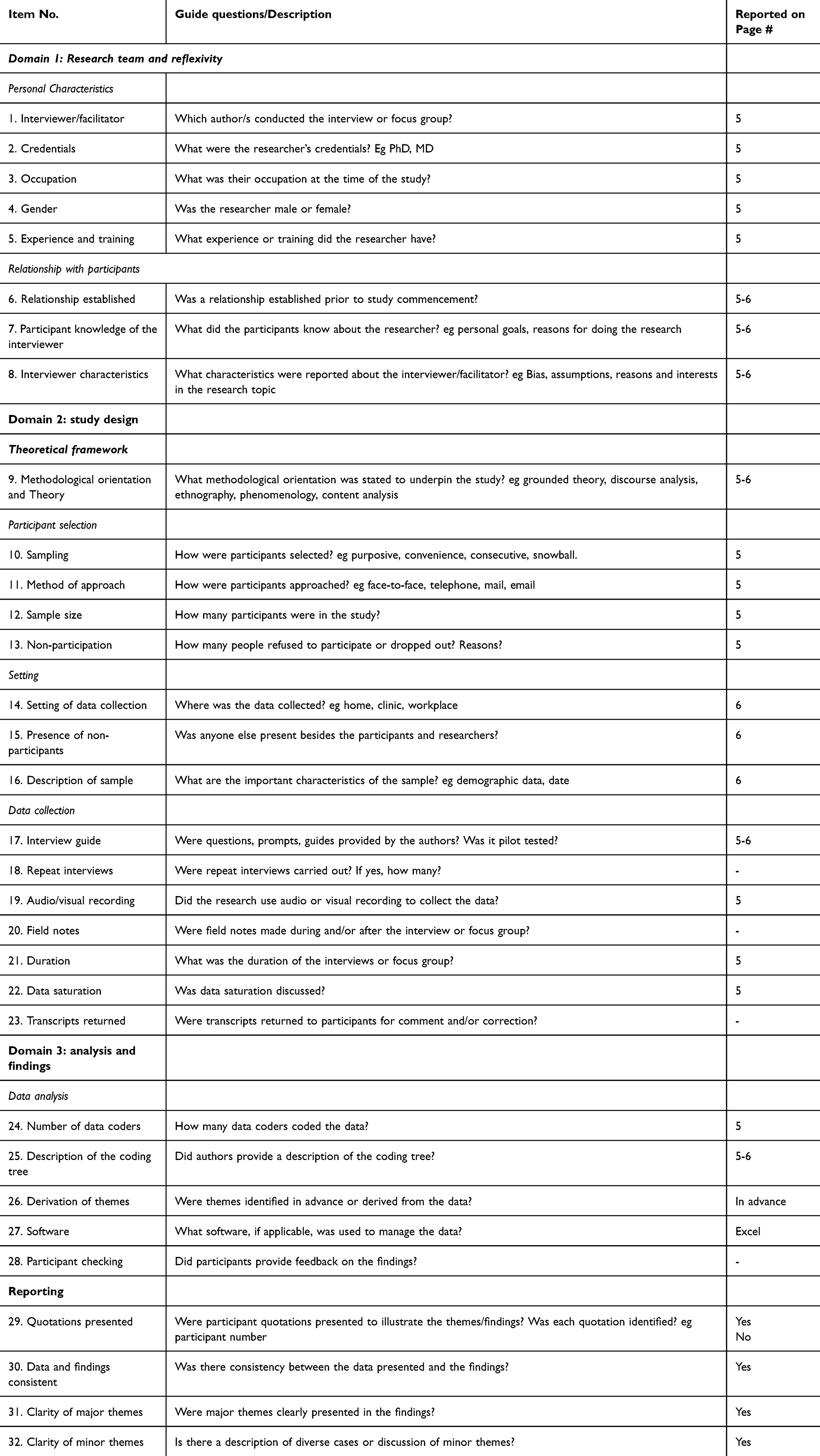 |
Table 2 Consolidated Criteria for Reporting Qualitative Studies (COREQ): 32-Item Checklist |
Two health psychologists (CS and EL), each with extensive experience in qualitative health research, independently coded the transcripts and then jointly refined the coding tree. Discrepancies in coding were resolved through discussion and consensus, with the involvement of a third researcher when needed, to enhance the credibility of findings. Excel was used due to the manageable dataset size.
Triangulation was incorporated through methodological triangulation (interviews and two types of focus groups), data source triangulation (patients, relatives, and patient representatives) and Analyst triangulation with two independent coders. The participation of two researchers reduced any possible bias in the expectations and perception of the researcher.
These strategies helped to mitigate potential researcher bias and enhance the validity of the analysis. Instead of relying solely on dual coding to reduce bias, our process involved reflexive discussions, peer debriefing, and iterative review of themes to ensure a comprehensive interpretation of the data.
Data saturation was determined when no new codes or themes emerged in the final focus group, and the coding framework remained stable This occurred in November 2023. As a basis for analysis, the patient journey established and validated in a previous study17 was used, which had been conducted with 62 COPD patients from 8 different European countries, including representation in Spain (n=9), and with ages ranging between 32 and 70 years (see Figure 1). The 32-item checklist concerning consolidated criteria for reporting qualitative research (COREQ) (Table 3) was used to provide information on important aspects about the research team, study methods, context of the study, findings, analysis and interpretations.
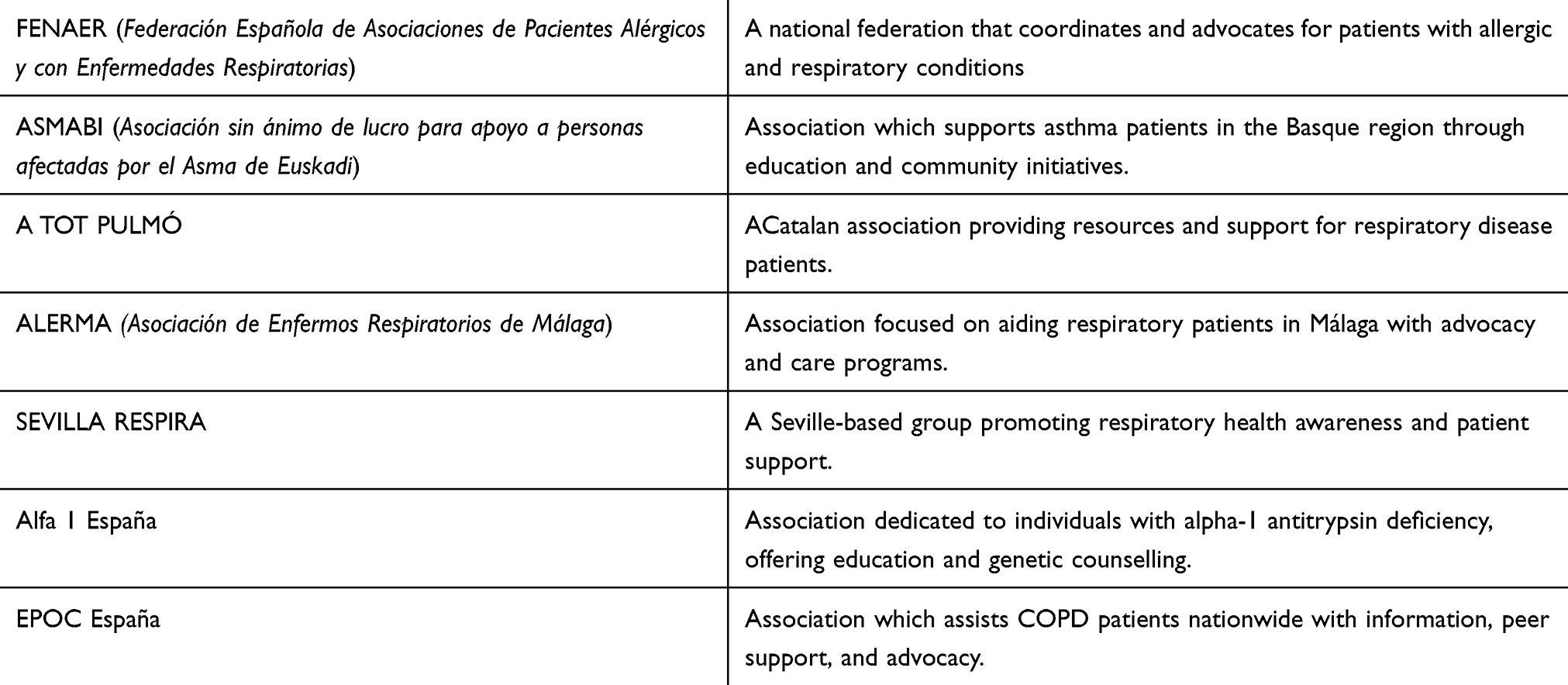 |
Table 3 Associations Participants |
 |
Figure 1 Established stages of the patient journey. |
Results
The thematic analysis, guided by a pre-existing patient journey framework, identified major themes including recognition of risk factors, identification of early symptoms, psycho-emotional and informational needs at diagnosis, challenges in treatment adherence, and the role of pulmonary rehabilitation and patient groups in monitoring, which were consistently reflected across interviews and focus groups.
Risk Factors
Exposure to Risk Factors
It is essential that asthma patients expand their knowledge about factors that trigger exacerbations of the disease (humidity, irritants, smoking, etc). It is also important that they know the possible triggers of an asthma attack and have a personalised action plan in place.
It is essential that patients know about the triggers so that they can get to know their disease, manage it and take measures according to the situation that they are in.
Patient groups believe that social awareness and visibility of asthma must be increased, and information must be given on risk factors, on the chronic nature of the disease, as well as on the importance of managing the respiratory disease.
There is a lack of awareness in society because asthma is trivialised.
In addition, COPD patients stress their need for specific advice on smoking so that they can receive information, ask questions and be given support to stop smoking.
Access to Diagnosis
Initial Symptoms
According to patient groups, during the stage in which the initial symptoms of the disease are experienced, it is important that patients know how to identify the early symptoms associated with the disease such as, for example, dyspnoea, coughing or difficulty breathing. They also highlight the importance of knowing how to distinguish between them, as they can sometimes be confused, as is the case with dyspnoea and difficulty breathing.
In relation to asthma, patient groups state that there is a series of basic concepts that patients must be aware of from the appearance of early symptoms, such as FEV 1 (forced expiratory volume in one second), eosinophils, type 2 inflammation, clinical asthma phenotypes, etc. In COPD, they mention that alpha-1 antitrypsin deficiency is an important concept to be acknowledge at this stage.
Furthermore, patient groups emphasise that, from the appearance of early symptoms, it is important that patients with respiratory diseases are aware of their rights as patients and that they are given support to manage the various procedures that they will have to go through. For example, they must be aware of the possibility of requesting a second medical opinion or disability assessment.
They also say that now is a good time for patients to start to keep a record of symptoms or to keep a diary of the disease so that they can share it when visiting their doctor, therefore favouring better management of the disease from the beginning.
Patients must work to get to know themselves and get to know their disease.
Being aware of other patients’ experiences also stands out as being necessary at this stage, highlighting the importance of information about the existing patient groups being made available to patients as early as possible.
Search for Information
Both asthma and COPD patients and carers generally use the following sources of information in relation to the disease: health professionals (main source of information, particularly pulmonologists and general practitioners); recognised bodies (FENAER, respiratory patient groups, scientific societies and pharmaceutical laboratory websites); the internet (mainly Google, Wikipedia and YouTube, which is the most common for asking questions and watching videos on respiratory physiotherapy). Patient organisations also make use of websites and social media (Instagram, Facebook, Twitter and YouTube channels or telemedicine apps). One group representative highlights the role of Instagram and TikTok to reach out to a younger audience. Patients and relatives tend to communicate with groups via e-mail and by telephone to ask questions and for advice. Members use WhatsApp groups to offer information about activities and give social support to one another.
I think people trust groups that are focused on the disease more… there is very often different information online.
Patients and relatives tend to go to patient organisations to expand information and training on health and for guidance related to the disease and associated changes, treatment and necessary care. One group representative mentions that patients usually tend to discuss concerns with professionals from patient groups more than with their own referring doctors or health professionals.
Many patients call about problems at work or sick leave. There is a lack of understanding about sick leave for asthma. (group representative)
Patient organisations make it possible to share experiences and knowledge with other patients in order to better deal with and adapt to the disease, therefore creating a support network. Within groups, there tend to be mentoring programmes or expert patients to offer support in early diagnoses and answer any questions that may arise.
It helps to know that there are people who have the same as you, with other characteristics; some are better and react better, while others are worse.
Patients tend to look for groups, especially to find information, support and to feel united, to kind of stick together. (group representative)
The need to carry out training activities aimed at both patients and relatives is also mentioned, bearing in mind the different stages of the disease.
Patients require continuous training on their disease and its progress as, for example, when a mild COPD first appears, the needs and information required are in no way related to a serious COPD. Patients must keep learning according to the stage that they are at.
Carers must be trained for emergency situations…how to administer adrenalin and how to ask for help.
Visiting the Doctor and Specific Tests
For COPD and asthma patients, the professionals considered to be essential in the early stages of the disease are specialists (pulmonologists/allergologists), psychologists and respiratory physiotherapists; in some cases, social workers and nutritionists, as well as nurses, are also mentioned. Most of these profiles are accessed via patient groups. The majority of patients taking part in the study defend the importance of a specialised asthma unit made up of a multidisciplinary team and they also mention the lack of coordination between the different professionals looking after asthma patients.
Anyone who doesn’t have access to an asthma unit has to hire these services privately. (group representative)
In general, participants stated that they had not been given enough information about the disease from their doctor in the first visits, and that they had to turn to other private professionals, patient groups or the internet to get more information and discuss their concerns.
She’s had to learn almost everything about the disease herself. (carer)
When asthma is diagnosed, patients listen to all the information from the pulmonologist, but when they leave the doctor’s office, they realise they haven’t understood anything. (group representative)
The representatives of the PAG consider it is essential that healthcare professionals raise awareness about patients’ associations during their visits. They add that at this stage, it is also crucial to take action so as to avoid underdiagnosis, particularly among primary care professionals.
It is important that doctors ‘prescribe groups’. That professionals say, ‘I can’t help you, but look, go to this place, to a group, to an information platform, to respiratory physiotherapy, to a psychologist …’. There must also be better interaction with primary care, as they’re not aware of respiratory health and it’s underdiagnosed or it’s diagnosed very late. Respiratory health must be spoken about more in general, as patients contact groups when they are already very seriously ill. (group representative)
Diagnosis
When diagnosis is received, both COPD and asthma patients, as well as their relatives, mention the need for receiving psycho-emotional and family support in the early stages of the disease which covers how to deal with the diagnosis, possible emotional disorders, adaptation to the disease, the impact of limitations in everyday life, reorganisation of family roles and loss of autonomy.
When I was diagnosed, my life had to change a lot… you’re really sad…. (asthma patient)
I found the first years really tough because I’ve always been very active…there comes a time when you get worse and worse, and you notice that you can’t do things. (COPD patient)
I feel very insecure, I don’t know how to do anything by myself, I’m really dependent and that dependence is what annoys me a lot of the time. (COPD patient)
When diagnosed, COPD patients consider it essential to have information about the disease (what it means to have COPD, early symptoms, progress, necessary care, the most common comorbidities, available treatment, limitations that may be found, etc.). They also believe it is important to know about patient groups as a meeting point and a source for discussing their concerns.
Knowing exactly what the disease is, its progress, knowing how long you can expect to live with the disease, because I don’t know…, more information about the disease itself.
Maybe they took it for granted that I knew what it was (COPD) and…to be honest, I’d not heard that word until I had this huge relapse.
One day it was given a name…and no more information was given about its diagnosis, like if a cold is detected and you’re given something to take for it.
In this respect, relatives of COPD patients mention that diagnosis must go hand in hand with training so that they can learn about the disease and the care involved, as this will help to favour a better adaptation to the new situation. It will also make it possible for relatives to encourage self-care and the responsibility of the person diagnosed with COPD. The most valued aspects include, on the one hand, receiving appropriate training so that carers can regularly supervise the health status of patients and know how to act in the event of an exacerbation of the disease. On the other hand, access to specific information about physical activity, respiratory physiotherapy and COPD, assistance and procedures (reduced mobility, retirement, disability, etc.) is mentioned, as well as being able to receive advice and psychological support to deal with the new situation.
Relatives or carers ultimately have as many needs as patients do, or even more; it’s hard to imagine a patient without their carer. (group representative)
According to patient groups, there are some aspects that must be considered upon diagnosis, such as: myths about inhalers, the importance of access and information about groups, emotional impact on patients and relatives, education about peak flow (peak expiratory flow meter), the importance of keeping a symptom diary, information about possible side effects and comorbidities, in addition to others.
Treatment and Monitoring
Treatment
As regards treatment, one of the points stressed most by patients is the importance of receiving appropriate training on how to use inhalers correctly. In general, patients say that they have been given very basic training and that they have been assessed by health professionals occasionally. Other patients mention that they themselves have realised that they are not using the inhaler technique correctly or that professionals have discovered this by chance.
It would be great to have training on how to use inhalers because nobody explains to you how you should use them.
They explained it to me once, a nurse showed me how to do it and that was it, nothing more, and that was that.
Furthermore, patients also stress the need to have information available on the disease and the different treatments, as well as to receive advice on how to adapt to new needs that give rise to changes in habits and routines, such as adapting travel or changing diet, etc. They also emphasise that it is essential for them to be given information on healthy habits and care (exercise, breaking bad habits, etc.) and for healthcare teams to appropriately monitor the disease and treatment. One of the major issues of concern for participants is the range of treatments, their complexity and the variety of inhalers.
Sometimes I’m given one inhaler, sometimes another one, an inhaler that’s ok today won’t be alright tomorrow, an inhaler that’s ok tomorrow won’t be alright today.
Relatives also call for training to deal with asthma attacks so as to calm patients down and in order to be a helpful resource as regards treatment, particularly in the event of an asthma attack or exacerbation of the disease. They believe that having more information about the disease and being aware of the care needed by patients is essential.
If I have to give her an adrenalin injection, how can I give her it if she can’t do it herself, where do I give her it, in what circumstances…what do I do afterwards?. (carer)
It’s distressing for relatives to see someone suffocating when they’re having an asthma attack. (group representative)
It was a very serious asthma attack… nobody has explained to me yet how to react in these situations. (carer)
Patients also underline the need to have equal healthcare in which everyone has access to the same therapies, such as respiratory physiotherapy. In this respect, they state that the time between follow-up visits considerably differs between the various autonomous regions, ranging from one week (at times of an asthma attack) to one year. Notable differences are also observed between the various autonomous regions regarding patient experience in terms of information, training and monitoring of inhaled therapy.
To be honest, we’re really abandoned here (…) I get a visit every six months all the same, but there are regions where the doctors are brilliant and there are regions where, unfortunately, we are in the underworld.
According to group representatives, it is essential that patients and families have access to information about updates in treatments and the various therapeutic options, about the benefits of treatment, side effects and also that they are given training on how to use inhalers properly.
Patients are left with the first treatment that they take and, even if it doesn’t work for them, they keep taking it. They don’t question the possibility of changing to another one.
Pulmonary rehabilitation is a fundamental aspect mentioned by group members. They believe that a daily routine of respiratory physiotherapy is necessary. Members stress that exercises and treatment must be personalised, bearing in mind the severity of the disease and their age.
No young person wants to do breathing exercises, but they might be able to do physical activity at a gym to work on this.
Physiotherapists only came when I had COVID, there was nothing when I was admitted for other respiratory problems.
Representatives state that many patients do not know that respiratory physiotherapy is available, while other patients are given exercises that are not suitable for their disease. In addition to this, many professionals are not trained. Participants in the study claim that although there is specialised training for respiratory physiotherapy which is available to everyone, professionals do not show much interest in this area. They all come to the conclusion that there is a great deal of inequality, not only between different autonomous regions, but also between hospitals in the same region and even between doctors at the same hospital. As a solution, various strategies are put forward such as, for example: making practical videos that are regularly updated or designing an online group programme that includes an initial assessment by a respiratory physiotherapist and monitoring of patients in various online sessions.
Adherence to Treatment
Adherence is a key factor in respiratory disease that was stressed by both patients and relatives, as well as by PAG, throughout the various stages of the study.
As regards adherence to treatment, participants insist on the importance of being regularly monitored by a doctor in order to better manage the disease (adjusting treatment, ensuring adherence, etc)., as well as accessing training courses on the use of inhalers.
If we don’t have a good adherence to treatment, we are obviously at a higher risk of having an asthma attack. (group representative)
Table 4 lays out all the indicators of lack of adherence to treatment in the group of asthma patients who have been included in the study, as well as the strategies suggested by the participants themselves to increase adherence. Some indicators of lack of adherence to treatment that were collected are as follows: low perception of the seriousness of the disease (particularly in patients with mild asthma), absence of symptoms, forgetfulness, changes in routines and schedules, inhalers are not suitable for patients or the possible side effects of treatment.
Very often, patients don’t speak with the pulmonologist enough and they don’t have the right device, because they don’t feel comfortable, because they don’t know how to use it properly, because they don’t use it correctly and it doesn’t have any effect on them (…) it is essential that patients find a device that they feel comfortable with and that they use it.
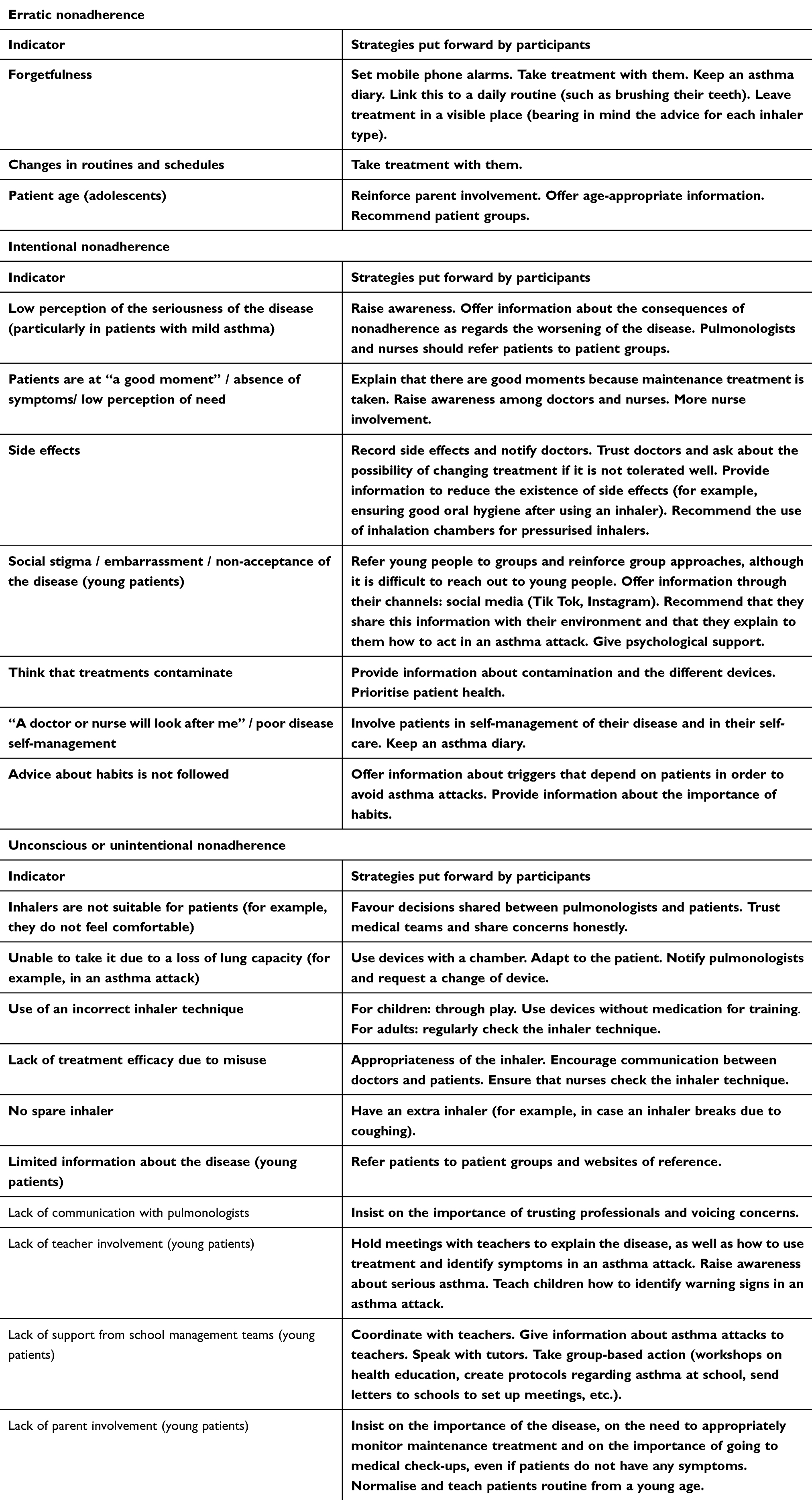 |
Table 4 Indicators of Nonadherence to Treatment in Asthma and Strategies Put Forward by Participants |
As for COPD patients, some indicators of lack of adherence to treatment mentioned were the following: absence of symptoms, lack of knowledge about when to use the device or its inhalation technique, misuse of devices, lack of information about the use of inhalation chambers or the possible side effects of treatments, among others (Table 5).
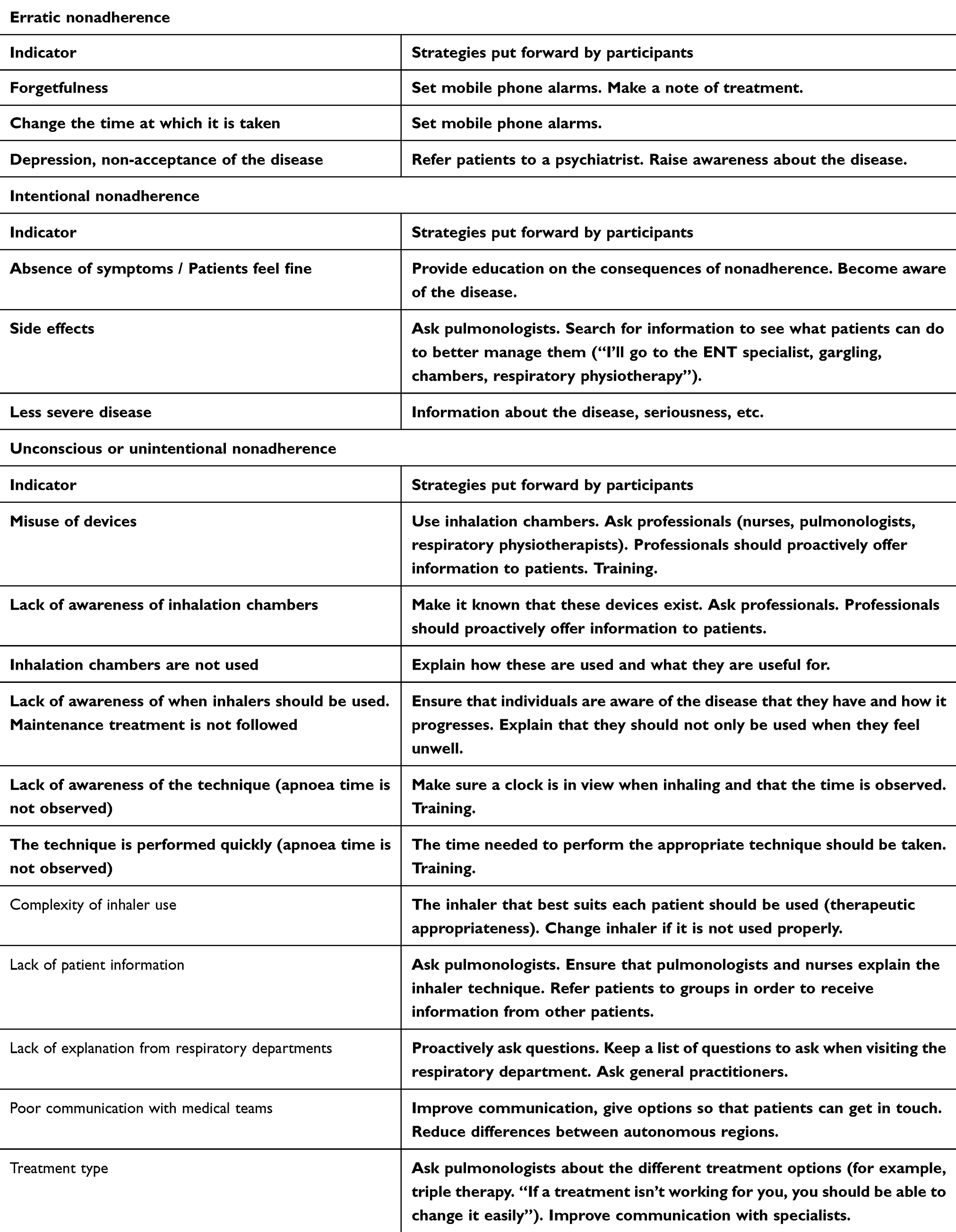 |
Table 5 Indicators of Nonadherence to Treatment in COPD and Strategies Put Forward by Participants |
The participants agree that pulmonologists are the most highly trained professionals when it comes to working on therapeutic adherence, yet general practitioners are the most accessible.
Patients and representatives put forward very different strategies to take action against nonadherence, namely: checking the inhaler technique, reinforcing the self-management of patients for their own disease and treatment, and involving patient groups as much as possible.
Development of Symptoms
Asthma patients emphasize the need to expand information, training, and advice about the disease, treatment, its possible side effects and adjustments that must be made to patients’ everyday lives, throughout the process of symptom development. This is particularly relevant with regard to some specific concerns such as problems sleeping and concentrating, fatigue and physical and socio-occupational limitations. Relatives also call for advice and training, particularly in the event of an asthma attack or exacerbation of the disease, so as to know how to recognise and learn to manage them.
After having a shower, I have to wait fifteen or twenty minutes to catch my breath and be able to shave after. (patient)
You’re scared that something will happen… I don’t want to go on holiday if there’s not a hospital near. (patient)
I used to do spinning and from one day to the next, I couldn’t go up two floors, so what can you do?. (patient)
Similarly, patients value being given advice on how to adapt to new needs that give rise to changes in habits and routines, such as adapting travel, changing diet, healthy habits and care, exercise, breaking bad habits, information for more advanced stages of the disease, as well as for healthcare teams to appropriately monitor the disease.
There is a perception that some professionals underestimate the disease in terms of daily limitations. One group representative describes the relevance of encouraging the figure of an asthma specialist nurse to carry out monitoring and discuss any concerns. Some participants say that they have been given help from medical teams to manage issues at work (sick leave, disability and economic aid).
I had to stop working… I was discharged and it was the doctors who took care of everything.
Other Treatments
Patient group representatives believe that this stage is particularly relevant for COPD patients and that it must not be forgotten about, as some people require advanced treatments such as oxygen therapy or lung transplants.
In the case of COPD, patients and carers generally agree that they have not received enough information about other relevant treatments for the disease, for example, in terms of care, information about healthy lifestyle habits or lung transplants. Representatives agree that there is limited information available in this regard, and they highlight the need for patients to have better information about transplants and other surgical options, as well as oxygen therapy and non-invasive mechanical ventilation. In this sense, information about pulmonary rehabilitation options is highly valued by patients.
Representatives stress the need to talk about palliative care and end-of-life decision making. They believe that this must be considered as another stage that both patients and their environment must be aware of, and they must know that patients themselves have the right to make any decisions they feel are appropriate when the time comes. They underline the need for patients to be given the appropriate support in the last stage of their lives and for their rights to be taken into account.
Discussion
This study is focused on describing the needs of patients with chronic obstructive pulmonary disease (COPD) and asthma throughout their patient journey along the different stages, such as identification of risk factors, diagnosis, as well as treatment and monitoring.17
Variability of Patient Needs Across the Disease Journey
The needs of these patients vary considerably throughout the course of the disease. In this respect, identification of risk factors, identification of early symptoms associated with the disease and having the resources and knowledge to take appropriate action are considered to be essential by the participants of this study. This is an important point to bear in mind as in other studies,23 a significant discrepancy has been observed between patients’ perceptions about the symptoms that they experience and disease management. Although some patients feel that their disease is under control, many experience frequent symptoms that have a significant effect on their quality of life. Thus, there is a need to implement initiatives to raise patients’ expectations.23
Psychological Impact and Support Needs at Diagnosis
The diagnosis stage is particularly significant for participants of the study as it is a time at which patients and relatives have a greater need for psycho-emotional and instrumental support, as well as training on the disease. COPD or asthma patients may experience a higher level of psychological distress than the general population, which includes anxiety and depression. This is a relevant point due to the impact on mental health and because, furthermore, patients with anxiety or depression are more likely to suffer a higher number of acute exacerbations, incidents of rehospitalisation and they are at a greater risk of mortality.24
Role of Patient Advocacy Groups in Supporting Self-Management
According to participants, one of the main sources of information for patients is PAG (Patient Advocacy Group). These offer emotional support, as well as peer-based support and advice to improve physical, emotional and mental health, while encouraging a change of behaviour and self-care.25,26 Health professionals are also key in the early stages of the disease and diagnosis as they serve as a reliable source of information about the disease. Furthermore, the participants in the study highlight the importance of health professionals prescribing support resources, such as patient groups. Self-care strategies and expert patients encourage the active participation of patients in care and treatment plans, as well as the use of support strategies among peers.27 Patients and relatives do not consider the information received in the various stages of the disease to be enough. The lack of sufficient information reported by participants may be related to difficulties in doctor-patient communication, the passive role patients adopt, and systemic pressures, such as healthcare system overload. Ineffective communication and time constraints in overcrowded healthcare settings can hinder the flow of clear and practical information. Furthermore, patients with COPD and asthma may assume a passive role due to emotional distress or limited health literacy, which reduces their participation in seeking clarification during consultations. It therefore seems relevant and appropriate to develop training environments for patients diagnosed with asthma/COPD and their carers, where information and training are offered to support good disease management in the different stages of the patient journey. In scientific literature, it has been observed that combining the education of patients/relatives and professionals with an active role of pharmaceutical personnel in patient monitoring promotes a better quality of life and patient satisfaction.28
Challenges in Treatment Adherence and Inhaler Training
Receiving appropriate training on how to use inhalers correctly is one of the key points mentioned by the participants of this study, in terms of the issues related to treatment. Bearing in mind that, according to several studies, the rates of inhaler misuse in asthma and COPD patients are high,29 the time invested by health professionals to improve the inhaler technique in asthma and COPD patients is vital to improving health outcomes.30
Another one of the key issues in all stages of the patient journey is therapeutic adherence, which is stressed by both patients and relatives, as well as by group representatives. Lack of adherence to inhaled therapy is associated with a poorer management of symptomatology, a higher cost of medical attention, as well as a decrease in the quality of medical attention related to health. Being able to recognise the factors of lack of adherence to inhaler use has clear benefits when it comes to developing effective educational strategies. In this respect, it has become necessary to conduct future research that goes into more depth and that sheds light on the various types of nonadherence factors.13
Inequities in Access to Therapies and Social Determinants
As can be observed, treatment is a key factor in the patient journey. In this respect, patients underline the importance of being able to have equal healthcare in which everyone has access to the same therapies, such as respiratory physiotherapy. Moreover, COPD and asthma place a substantial economic burden on patients and their families, often involving expenses for treatments, private care, and lost income due to work limitations. Social determinants of health come into play here, such as income, education, occupation and access to medical attention, which have a significant effect on healthcare and on health. However, said determinants have not been studied in as much detail as required in the field of chronic respiratory diseases, particularly in pulmonary rehabilitation.31 Even though pulmonary rehabilitation is one of the most profitable treatments for COPD, its use may be limited due to a lack of awareness or difficulties in access. Various authors back approaches based on community exercise programmes that are supervised by certified personal trainers or on telemedicine and remote patient monitoring strategies.32,33
Symptom Development and Lifestyle Interventions
As regards the development of symptoms, the participants of this study stand by the need to expand on the training and advice received about their disease throughout the process. People with COPD or asthma experience limitations that have an impact on their health-related quality of life and they often tend to focus more on these difficulties than on the symptomatology as such. It is therefore important that health professionals bear in mind the impact of the disease on individuals when prescribing treatment.34 Patients tend to experience significant variability in their respiratory symptoms either daily or weekly, particularly in the morning as they are more severe, as well as interference in daily life activities. This symptomatic variability is key because it may give rise to unsuitable self-prescription of medicine.35,36
Furthermore, lifestyle changes are beneficial to the prevention and comprehensive treatment of COPD and asthma. Interventions aimed at promoting healthy lifestyle habits, such as vaccination and prevention of infections, reduction in smoking, physical inactivity, obesity or malnutrition may increase the expectancy and quality of life of this patient group.37
Proposed Strategies for Integrated Care and Future Research
In accordance with the sections stipulated throughout the journey of patients with COPD and asthma, it is relevant that interventions are adapted to patient needs, combining strategies to favour disease management, raising patient awareness and encouraging self-care.38 Interventions must be based on a personalised action plan which is focused on monitoring the development of symptoms or exacerbations, on knowledge of psychological coping and stress management strategies, as well as enhancing responsibility in therapeutic adherence and healthy lifestyle choices.38
The main strengths of this study include taking a patient-centred perspective, which gives rise to a more in-depth understanding of the impact of lifestyles and needs expressed by patients throughout the patient journey. The sample size of the study is also extensive, considering the qualitative methodology and the use of thematic analysis. Furthermore, the use of a rigorous qualitative analysis approach based on a data triangulation methodology makes it possible to collect accurate information directly from patients, relatives and group representatives. All participants in this study stated that they had been medically diagnosed with COPD and asthma, and information was therefore collected on the needs of two of the most prevalent respiratory diseases.
As regards limitations of the study, it may be stressed that the exclusive inclusion of qualitative data may be complemented with data obtained by means of quantitative methodology, with the use of instruments validated for the study population. The qualitative approach offers a large amount of narrative information, although care must be taken when generalising results and this must be limited to the field in which these have been collected, as well as to the age groups of the participants. In addition, the sample was not selected at random, therefore the possibility of bias related to social desirability must be considered. Other limitation of this study is that focus group participants were required to have been prescribed inhaled maintenance therapy, which may restrict the generalizability of the findings to all individuals with asthma or COPD. The results must be interpreted taking into account the heterogeneity of the sample, which included not only patients but also family members and representatives of patient groups. This diversity could have introduced variations in the findings, as patients’ perspectives and experiences may differ from those of those indirectly involved in care.
The timeframe for data collection (2022–2023) likely overlaps with COVID-19. Although the recruitment process and study procedures were not affected by the COVID-19 context, it is possible that participants’ experiences and perceptions were shaped to some extent by the broader social and healthcare environment during 2021 and 2023. We acknowledge this as a contextual factor that may have influenced how some participants cope with the topics discussed.
Furthermore, future research could consider COPD and asthma patients separately to analyze their specific needs in more detail. While we sought diversity in the patient sample, it is recommended to explore participants’ needs according to disease stage or time since diagnosis. People with more recent diagnoses or more advanced COPD may experience different needs and challenges.
Compared to published literature, this article provides a comprehensive view of the patient’s experience throughout their patient journey, identifying specific needs at each stage of the disease, from diagnosis to treatment and follow-up. In addition, it considers the perspective of family members and patient associations, something not addressed in the other studies, and emphasizes the importance of multidisciplinary strategies and the role of patient groups as a source of emotional support and education.39–41
The needs of COPD and asthma patients vary considerably throughout the course of the disease. Patients do not consider the information received in the various stages of the disease to be enough. It therefore seems relevant and appropriate to develop training environments for patients diagnosed with COPD/asthma and their carers, where information and training are offered to support good disease management in the different stages of the patient journey.
Conclusions
1. Patients with COPD and asthma require psycho-emotional support and specific education throughout their entire patient journey.
2. Training in inhaler techniques and regular monitoring by multidisciplinary teams are essential to increase therapeutic adherence and optimize clinical outcomes, as many patients reported inadequate initial instruction and persistent misuse.
3. The integration of patient groups and personalized pulmonary rehabilitation programs can improve quality of life and clinical management across all disease stages.
4. Pulmonary rehabilitation and respiratory physiotherapy programs should be made more accessible and tailored to the age and severity of patients, given the strong demand and perceived inequality in access across regions.
5. Primary care, should actively refer patients to patient associations early in the diagnostic process, as these groups play a critical role in emotional support, disease education, and treatment adherence.
Data Sharing Statement
There is no data set associated with the paper.
Ethics Statement
Ethics approval was not required for this study according to Spanish Law. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, ensuring respect for participants’ dignity, rights, and well-being. In addition, we complied with applicable data protection regulations, including Regulation (EU) 2016/679 (GDPR) and Spanish Law Ley Orgánica 3/2018, and ensured the confidentiality and voluntary nature of participation. The participants signed the informed consent document and were recruited voluntarily through an association of individuals with COPD or asthma. No identifying data was collected from the participants in the interviews.
Funding
Chiesi España sponsored this project without participating in study design, data analysis, or preparation of the manuscript.
Disclosure
Elena García and Dolors Querol are employees of Chiesi España. The authors report there are no competing interests to declare.
References
1. Jabbarian LJ, Zwakman M, van der Heide A, et al. Advance care planning for patients with chronic respiratory diseases: a systematic review of preferences and practices. Thorax. 2018;73(3):222–230. doi:10.1136/thoraxjnl-2016-209806
2. Soriano JB, Kendrick PJ, Paulson KR, GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. Pauwels RA, Buist AS, Calverley PMA, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(5):1256–1276. doi:10.1164/ajrccm.163.5.2101039
4. Dharmage SC, Perret JL, Custovic A. Epidemiology of asthma in children and adults. Front Pediatr. 2019;7:246. doi:10.3389/fped.2019.00246
5. Song P, Adeloye D, Salim H, et al. Global, regional, and national prevalence of asthma in 2019: a systematic analysis and modelling study. J Glob Health. 2022;12:04052. doi:10.7189/jogh.12.04052
6. Cosío BG, Fiorentino F, Scrimini S. EPOC y asma. Archivos de Bronconeumología. 2010;46:2–7. doi:10.1016/S0300-2896(10)70060-0
7. Bousquet J, Kaltaev N. Global Surveillance, Prevention and Control of Chronic Respiratory Diseases: a Comprehensive Approach. World Health Organization; 2007. Available from: https://iris.who.int/handle/10665/43776.
8. Jones PW, Watz H, Wouters EF, Cazzola M. COPD: the patient perspective. COPD. 2016;11:13–20. doi:10.2147/COPD.S85977
9. Miravitlles M, Worth H, Soler Cataluña JJ, et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study. Respir Res. 2014;15(1):122. doi:10.1186/s12931-014-0122-1
10. Clari M, Ivziku D, Casciaro R, Matarese M. The unmet needs of people with chronic obstructive pulmonary disease: a systematic review of qualitative findings. COPD. 2018;15(1):79–88. doi:10.1080/15412555.2017.1417373
11. Cappa V, Marcon A, Di Gennaro G, et al. Health-related quality of life varies in different respiratory disorders: a multi-case control population based study. BMC Pulm Med. 2019;19(1):32. doi:10.1186/s12890-019-0796-8
12. Kharaba Z, Feghali E, El Husseini F, et al. An assessment of quality of life in patients with asthma through physical, emotional, social, and occupational aspects. a cross-sectional study. Front Public Health. 2022;10:883784. doi:10.3389/fpubh.2022.883784
13. Plaza V, López-Viña A, Entrenas LM, et al. Differences in adherence and non-adherence behaviour patterns to inhaler devices between COPD and asthma patients. COPD. 2016;13(5):547–554. doi:10.3109/15412555.2015.1118449
14. Rand CS, Wise RA. Measuring adherence to asthma medication regimens. Am J Respir Crit Care Med. 1994;149(2Pt 2):S69–76;discussionS77–78. doi:10.1164/ajrccm/149.2_Pt_2.S69
15. Singh M, Kansra S. Adherence issues in asthma. Indian Pediatr. 2006;43(12):1050–1055.
16. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
17. Scichilone N, Whittamore A, White C, Nudo E, Savella M, Lombardini M. The patient journey in chronic obstructive pulmonary disease (COPD): a human factors qualitative international study to understand the needs of people living with COPD. BMC Pulm Med. 2023;23(1):506. doi:10.1186/s12890-023-02796-8
18. Davies EL, Bulto LN, Walsh A, et al. Reporting and conducting patient journey mapping research in healthcare: a scoping review. J Adv Nurs. 2023;79(1):83–100. doi:10.1111/jan.15479
19. Sijm-Eeken M, Zheng J, Peute L. Towards a Lean Process for Patient Journey Mapping – a Case Study in a Large Academic Setting. In: Digital Personalized Health and Medicine. IOS Press; 2020:1071–1075. doi:10.3233/SHTI200326
20. Di BT, Ml D, Tj O, Km M. Patient journeys: the process of clinical redesign. Med j Austr. 2008;188(S6). doi:10.5694/j.1326-5377.2008.tb01668.x
21. Gualandi R, Masella C, Viglione D, Tartaglini D. Exploring the hospital patient journey: what does the patient experience? PLOS ONE. 2019;14(12):e0224899. doi:10.1371/journal.pone.0224899
22. Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–547. doi:10.1188/14.ONF.545-547
23. Fletcher M, Hiles D. Continuing discrepancy between patient perception of asthma control and real-world symptoms: a quantitative online survey of 1,083 adults with asthma from the UK. Prim Care Respir J. 2013;22(4):431–438. doi:10.4104/pcrj.2013.00091
24. Rahi MS, Thilagar B, Balaji S, et al. The impact of anxiety and depression in chronic obstructive pulmonary disease. Adv Respir Med. 2023;91(2):123–134. doi:10.3390/arm91020011
25. Chen Z, Fan VS, Belza B, Pike K, Nguyen HQ. Association between social support and self-care behaviors in adults with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2017;14(9):1419–1427. doi:10.1513/AnnalsATS.201701-026OC
26. Doull M, O’Connor AM, Welch V, Tugwell P, Wells GA. Peer support strategies for improving the health and well‐being of individuals with chronic diseases. Cochrane Database Syst Rev. 2017;2017(6):CD005352. doi:10.1002/14651858.CD005352.pub2
27. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. doi:10.1016/s0738-3991(02)00032-0
28. Lemmens KMM, Nieboer AP, Huijsman R. A systematic review of integrated use of disease-management interventions in asthma and COPD. Respir Med. 2009;103(5):670–691. doi:10.1016/j.rmed.2008.11.017
29. Çakmaklı S, Özdemir A, Fırat H, Aypak C. An evaluation of the use of inhalers in asthma and chronic obstructive pulmonary disease. J Taibah Univ Med Sci. 2023;18(4):860–867. doi:10.1016/j.jtumed.2023.01.001
30. Kocks JWH, Chrystyn H, van der Palen J, et al. Systematic review of association between critical errors in inhalation and health outcomes in asthma and COPD. Npj Prim Care Resp Med. 2018;28(1):1–6. doi:10.1038/s41533-018-0110-x
31. Ly L, Pascoe A, Philip J, Hudson P, Smallwood N. Social determinants of advanced chronic respiratory interventions: a scoping review. Eur Respir Rev. 2023;32(169):230068. doi:10.1183/16000617.0068-2023
32. Arnold MT, Dolezal BA, Cooper CB. Pulmonary rehabilitation for chronic obstructive pulmonary disease: highly effective but often overlooked. Tuberc Respir Dis. 2020;83(4):257–267. doi:10.4046/trd.2020.0064
33. Troosters T, Casaburi R, Gosselink R, Decramer M. Pulmonary rehabilitation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172(1):19–38. doi:10.1164/rccm.200408-1109SO
34. Svedsater H, Roberts J, Patel C, Macey J, Hilton E, Bradshaw L. Life impact and treatment preferences of individuals with asthma and chronic obstructive pulmonary disease: results from qualitative interviews and focus groups. Adv Ther. 2017;34(6):1466–1481. doi:10.1007/s12325-017-0557-0
35. Espinosa de Los Monteros MJ, Peña C, Soto Hurtado EJ, Jareño J, Miravitlles M. Variability of respiratory symptoms in severe COPD. Archivos de Bronconeumología. 2012;48(1):3–7. doi:10.1016/j.arbr.2011.07.006
36. Peña VS, Miravitlles M, Gabriel R, et al. Geographic variations in prevalence and underdiagnosis of COPD: results of the IBERPOC multicentre epidemiological study. Chest. 2000;118(4):981–989. doi:10.1378/chest.118.4.981
37. Ambrosino N, Bertella E. Lifestyle interventions in prevention and comprehensive management of COPD. Breathe. 2018;14(3):186–194. doi:10.1183/20734735.018618
38. Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI. Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PLOS ONE. 2019;14(8):e0220116. doi:10.1371/journal.pone.0220116
39. Volpato E, Pennisi V, Pennisi A, et al. Delving into uncontrolled or severe asthma: perspectives from patients and healthcare professionals in a cross-sectional study. J Asthma Allergy. 2024;17:1207–1226. doi:10.2147/JAA.S483020
40. Volpato E, Centanni S, Banfi P, et al. Narrative analysis of the impact of COVID-19 on patients with chronic obstructive pulmonary disease, their caregivers, and healthcare professionals in Italy. Int J Chron Obstruct Pulmon Dis. 2021;16:2181–2201. doi:10.2147/COPD.S312372
41. Gatti V, Banfi P, Centanni S, et al. Enlightening chronic obstructive pulmonary disease through patients’ and caregivers’ narratives. Int J Chron Obstruct Pulmon Dis. 2018;13:3095–3105. doi:10.2147/COPD.S172214
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.