Back to Journals » Journal of Pain Research » Volume 19
Superolateral Genicular Nerve Block Added to Medial Blocks in Medial Knee Osteoarthritis
Authors Nagai S, Aso K, Sugimura N ![]() , Deguchi S, Ushida T, Ikeuchi M
, Deguchi S, Ushida T, Ikeuchi M
Received 14 October 2025
Accepted for publication 7 May 2026
Published 26 May 2026 Volume 2026:19 574377
DOI https://doi.org/10.2147/JPR.S574377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor King Hei Stanley Lam
Shuhei Nagai,1,2 Koji Aso,1 Natsuki Sugimura,1 Syo Deguchi,1 Takahiro Ushida,2 Masahiko Ikeuchi1
1Department of Orthopaedic Surgery, Kochi Medical School, Kochi University, Nankoku, Japan; 2Department of Pain Medicine, Aichi Medical University, Nagakute, Japan
Correspondence: Shuhei Nagai, Department of Orthopaedic Surgery, Kochi Medical School, Kochi University, 185-1 Oko-cho Kohasu, Nankoku, 783-8505, Japan, Tel +81 888665811, Email [email protected]
Purpose: We aimed to report the observed analgesic outcomes among patients with advanced medial knee OA who received medial genicular nerve blocks with or without an additional superolateral genicular nerve block during a period-based clinical practice setting, and to explore clinical and imaging features associated with an insufficient response after medial-only blocks in a non-randomized observational cohort.
Patients and Methods: In this prospective observational cohort study (October 2024–March 2025), patients with Kellgren–Lawrence grade 3 or 4 medial knee OA and baseline walking pain ≥ 20 mm on a 100-mm Visual Analog Scale (VAS) received genicular nerve blocks as part of their routine clinical care. During two consecutive clinical periods, patients received either medial blocks only (superomedial and inferomedial; “ 2-nerve”) or medial plus superolateral blocks (“ 3-nerve”) (non-randomized allocation by clinical period). Walking VAS and Timed Up and Go (TUG) tests were performed immediately before and after the block (short-term post-block assessment). In the 2-nerve group, patients with < 70% pain reduction (non-responders) were compared with responders using the magnetic resonance imaging OA Knee Score (MOAKS) and quantitative sensory testing (QST).
Results: Walking pain VAS changed from 51.9 to 15.8 mm (2-nerve) and from 61.6 to 10.6 mm (3-nerve); between-group difference in pain reduction was observed, with a larger reduction in the 3-nerve group (p = 0.02). TUG results improved in both groups, without between-group differences. Within the 2-nerve group, lateral femoral BML scores were higher in non-responders than in responders (p = 0.03), whereas MOAKS cartilage, osteophyte, meniscus, and QST parameters did not differ.
Conclusion: Adding a superolateral genicular nerve block was associated with greater short-term walking pain reduction in advanced medial knee OA. Lateral femoral BMLs may help identify patients who may warrant consideration for an individualized approach and may inform diagnostic target selection when medial-only blocks provide insufficient analgesia.
Keywords: bone marrow lesion, MOAKS, magnetic resonance imaging, quantitative sensory testing, ultrasound guidance, diagnostic block
Introduction
Osteoarthritis of the knee (knee OA) affects 20–30% of individuals aged ≥65 years,1,2 and its prevalence is increasing with the progression of population aging.3 The primary symptom of knee OA is pain, which directly impairs activities of daily living (ADLs) when exacerbated. Total knee arthroplasty (TKA) is an effective treatment that markedly improves pain and knee function; however, in older patients with comorbid medical conditions, tolerance to surgical stress is reduced, and the risk of perioperative complications is increased. Therefore, nonoperative treatments are often chosen, even among patients who would otherwise be considered surgical candidates. This trend is expected to become more pronounced in rapidly aging societies, such as that in Japan, highlighting the importance of comprehensive treatment strategies that incorporate surgical interventions as well as minimally invasive and conservative therapies.
Radiofrequency ablation (RFA) of peripheral nerves has become a viable treatment option for patients with severe pain and advanced deformity for whom TKA cannot be performed or is not desired for various reasons. Given its effectiveness and safety, RFA is expected to gain further acceptance; however, to our knowledge, a consensus regarding the target nerves has yet to be established. Even recent meta-analyses assessing the analgesic efficacy of genicular nerve RFA have not resolved the issue of optimal target nerve selection. Specifically, the included studies used heterogeneous ablation protocols, with the number of targeted nerves ranging widely (approximately three to nine), highlighting the ongoing lack of consensus regarding which nerves should be targeted.4,5 Notably, the optimal target selection for medial-type knee OA remains an area of ongoing uncertainty. To date, RFA has been applied to sensory nerves, including the superomedial, inferomedial, and superolateral genicular nerves; the infrapatellar branch of the saphenous nerve; and the medial retinacular nerve.6–9 Recently, following the report by Choi et al, most studies have targeted three nerves: the superomedial, inferomedial, and superolateral genicular nerves10 In Japan, insurance coverage for cooled RFA targeting these three genicular nerves was approved in 2023. Since most cases of knee OA are of the medial type, the necessity of intervention in the lateral nerves remains controversial. Albayrak et al reported no significant differences in outcomes between ablation of the two medial genicular nerves and ablation of three nerves, including the superolateral genicular nerve. From the perspective of invasiveness and potential complications, they suggested that intervention of the superolateral genicular nerve may not always be necessary. However, current evidence has not sufficiently clarified which patient subgroups might benefit from adding the superolateral target, and, to our knowledge, no prior reports have specifically discussed which patient subgroups do not require this additional intervention.11
In medial-type knee OA, disease progression may involve osteoarthritic changes in the lateral compartment, such as cartilage degeneration and bone marrow lesions (BMLs).12 BMLs are strongly associated with weight-bearing pain in knee OA and may represent potent nociceptive sources within the subchondral bone.13,14 Histopathological studies have reported increased expression of nerve growth factor and higher osteoclast density within BML regions, along with increased subchondral nerve fiber density, suggesting amplified nociceptive signaling through nerve sprouting and sensitization.15,16 Consequently, pain in medial-type knee OA is not always confined to the medial compartment and may extend laterally when lateral compartment pathology is present. These findings suggest that lateral compartment pathology, when present, may contribute to pain generation even in medial-type disease and may influence response to medial-only genicular targets. Thus, when lateral compartment BMLs or other lateral-compartment changes are present, adding a superolateral genicular nerve block may be considered as part of an individualized diagnostic approach, although its clinical value requires confirmation in randomized and blinded studies. Therefore, in this non-randomized observational study conducted in routine clinical practice, we aimed to describe the analgesic effect of adding a superolateral genicular nerve block to medial genicular nerve blocks in patients with medial knee OA (Kellgren–Lawrence grade 3 or 4) and to explore clinical and imaging features associated with insufficient response to medial-only blocks.17 This analysis was intended to be hypothesis-generating and to inform future prospective studies evaluating optimal target selection.
Materials and Methods
This study was approved by the Ethics Committee of Kochi University School of Medicine (approval number: 2024–104) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants for the collection of personal data, supplementary information, and publication of study results.
This prospective observational cohort study was conducted in routine clinical practice settings. Because exposure was determined by consecutive calendar periods in routine practice, this design can be considered a period-based (quasi-experimental) observational cohort. All genicular nerve blocks in this study were performed as part of routine clinical care—specifically, as diagnostic test blocks routinely conducted prior to RFA. No procedures were performed specifically for research purposes, and no additional interventions were introduced. Group allocation followed the routine care pathway by calendar period rather than randomization; therefore, selection bias and temporal confounding cannot be fully excluded.
Participants
During the study period (October 2024 to March 2025), 30 consecutive patients (12 men and 18 women) with advanced or end-stage medial knee OA who underwent diagnostic genicular nerve blocks as part of routine clinical care were included. Advanced or end-stage medial knee OA was operationally defined as medial-compartment knee osteoarthritis with Kellgren–Lawrence (KL) grade 3 or 4, diagnosed and graded by a board-certified orthopaedic surgeon with expertise in knee disorders. Patients typically proceeded to diagnostic blocks under the following conditions: when conservative measures had been insufficient; they had KL grade 3 or 4 medial knee OA; and at least moderate walking pain (≥20 mm on a 100-mm Visual Analog Scale [VAS]) was reported at consultation. Patients were excluded if they had dementia, lateral or patellofemoral compartment OA, post-traumatic OA, osteonecrosis, inflammatory arthritis/rheumatologic diseases, comorbid psychiatric disorders, lower-limb pain attributable to spinal disease, inability to walk, or allergy to local anesthetics. Patients with radiographically predominant lateral-compartment OA were excluded; however, radiographically medial-type knees were included regardless of mild lateral-compartment MRI findings (eg, BMLs), which were recorded and analyzed. No eligibility criteria were applied beyond those routinely used in clinical decision-making for performing diagnostic genicular nerve blocks prior to RFA.
Effect of Superolateral Genicular Nerve Block
Clinical Care Pathways and Exposure Definition
Care pathways differed by calendar period in routine practice. Between October and December 2024, patients received superomedial and inferomedial genicular nerve blocks only (“2-nerve”). During January–March 2025, patients received superomedial, inferomedial, and superolateral blocks (“3-nerve”). Across the cohort, two patients with dementia and two with lateral-compartment OA were excluded prior to analysis according to routine eligibility considerations. Consequently, the final analysis included 26 patients (33 knees): 13 patients (16 knees) in the 2-nerve period and 13 patients (17 knees) in the 3-nerve period. Because the exposure definition was period-based, unmeasured differences between time periods (eg, referral patterns or clinical practice changes) may have influenced the observed outcomes.
Procedures
Ultrasound-guided genicular nerve blocks were performed as part of routine care following the technique described by Kim et al18 The patients were placed in a supine position with a pillow under the popliteal fossa. A 12-MHz linear probe (KONICA MINOLTA SONIMAGE HS1) was used. The probe was first placed at the junction of the femoral or tibial epicondyles and diaphysis. It was then moved dorsoventrally, and the genicular artery (which accompanies the genicular nerves) was identified using color Doppler. To reduce the risk of vascular puncture, after identifying the genicular artery with color Doppler, the needle was advanced under in-plane ultrasound guidance, and local anesthetic was injected adjacent to the target region while avoiding intravascular injection (with aspiration before injection). Assessments using the pain VAS and the Timed Up and Go (TUG) test were performed immediately before and after the nerve block (2- or 3-nerve), to evaluate the analgesic effect and lower limb function. Because outcomes were assessed immediately after the diagnostic block, this study evaluates short-term post-block responses. All procedures and outcome assessments were performed by the same physician using a standardized, prespecified protocol throughout the study period, to minimize inter-operator and inter-rater variability.
Outcome Measures
The following two outcome measures were included. 1) Pain VAS: A widely used scale for assessing the intensity of pain or discomfort. A 100-mm line was anchored with “no pain” (0) and “worst imaginable pain” (100). The patients were asked to mark a point corresponding to their perceived pain intensity, and the score was recorded in millimeters. 2) TUG test: Measurement of gait ability and lower limb function. Starting from a seated position, patients were instructed to stand up on a command, walk 3 m, turn, return, and sit down. The time required to complete each task was recorded as well.
Clinical Characteristics of Patients with an Insufficient Effect of Medial Genicular Nerve Block
To determine the characteristics of patients with an insufficient analgesic effect from the medial genicular nerve block alone, a further analysis was conducted on 16 knees in the 2-nerve group. Magnetic resonance imaging (MRI) was used to assess the extent of BMLs, osteophytes, cartilage damage, and meniscal extrusion or tears in the lateral femorotibial compartment, using the Osteoarthritis Knee Score (MOAKS). Group allocation was based on previous reports by Broadhurst and Yeom.19,20 Patients whose walking pain VAS decreased by <70% compared with pre-block values were classified as the Non-responder group (NR group: 5 knees), whereas those with ≥70% reduction were classified as the Responder group (R group: 11 knees). Originally proposed for diagnostic block contexts outside the knee, this threshold was adopted as a stricter cutoff to minimize false-positive responder classification when exploring residual pain potentially attributable to lateral-compartment pathology. The MOAKS parameters were compared between the two groups. Quantitative sensory testing (QST) was performed for both groups.
Outcome Measures
Additional outcome measures included the following. 1) MOAKS: Evaluated BMLs, osteophytes, cartilage damage, and meniscal extrusion/tears in the lateral femorotibial compartment.21 2) QST: Using a tool developed by Izumi et al22 3) Pressure Pain Threshold (PPT): measured on the tibialis anterior muscle using a mini-algometer. 4) TS (Temporal Summation): Ten consecutive pinprick stimulations were applied to the tibialis anterior muscle, and the increase in the VAS score (10th – 1st stimulus) was recorded. 5) Conditioned Pain Modulation (CPM): The change in the PPT of the tibialis anterior muscle was measured with and without a conditioning stimulus applied to the contralateral earlobe using a pain clip.
Sample Size Estimation
The required sample size was estimated a priori for the primary outcome (change in walking pain VAS) using a two-sided significance level of 0.05. Assuming a clinically meaningful mean change of 19.9 mm (the MCID for knee OA) and an SD of within-knee changes of 23.36 mm derived from preliminary data, the minimum required sample sizes were approximately 11, 15, and 18 knees for 80%, 90%, and 95% power, respectively. As this was a non-randomized observational study of consecutive patients in routine practice, the final sample size was determined by the number of eligible knees during the study period. This estimation was based on within-knee pre–post change and was intended to ensure adequate precision for the primary outcome, rather than to power a definitive between-group comparison. Accordingly, the between-group analyses were considered exploratory (hypothesis-generating). This study was not powered for the primary between-group comparison; the sample size was determined by the number of consecutive eligible patients during the study period, and the between-group analyses are exploratory.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, N.Y., USA). Comparisons of baseline characteristics between the 2- and 3-nerve groups were performed using independent t-tests and chi-squared tests. Before between-group comparisons, we assessed distributional assumptions: normality was evaluated using the Shapiro–Wilk test within each group, and homogeneity of variances was assessed using Levene’s test. These assumption checks were performed for the primary between-group comparisons of change scores and for key baseline continuous variables. When these assumptions were satisfied, parametric tests (independent t-tests) were applied; when assumptions were not satisfied, non-parametric alternatives (Mann–Whitney U-tests) were used for between-group comparisons. Comparisons of the VAS and TUG test outcomes between the two groups were performed using independent t-tests and Mann–Whitney U-tests. Given that this was a period-based observational study with a modest sample size, our primary focus for between-group comparisons was on pre–post change scores. Baseline walking pain VAS did not differ significantly between groups, and the between-group analyses were intended to be exploratory (hypothesis-generating) rather than definitive causal estimates. Independent t-tests, chi-square tests, and Fisher’s exact tests were used to compare the NR and R groups. Comparisons of the MOAKS scores between the NR and R groups were performed using the Mann–Whitney U-test. Statistical significance was set at p < 0.05. As some participants contributed data from both knees, a one-knee-per-participant sensitivity analysis was specified to address within-participant non-independence. When bilateral knees were available, the knee with the higher baseline walking VAS was selected for analysis. Given the modest sample size, we did not fit clustered models (eg, mixed-effects models or generalized estimating equations) because such models can be unstable and sensitive to assumptions in small datasets. Instead, we prioritized this one-knee-per-participant sensitivity analysis, and the results were materially unchanged. Because subgroup analyses (NR vs. R) were exploratory and based on a small number of knees, these results should be interpreted cautiously as hypothesis-generating. Additionally, to facilitate the interpretation of the primary between-group comparison, we calculated the mean difference with a 95% confidence interval and a standardized mean difference (Hedges’ g) with a 95% confidence interval for the change in walking pain VAS (pre–post).
Results
Effect of Superolateral Genicular Nerve Block
No significant differences were observed in the baseline patient characteristics between the 2- and 3-nerve groups (Table 1). In the 2-nerve group, walking pain VAS decreased from 51.9 mm (pre-block) to 15.8 mm (post-block) and from 61.6 mm (pre-block) to 10.6 mm (post-block) in the 3-nerve group. A between-group difference in the pre–post change in walking pain VAS was observed (p = 0.02), and the mean reduction was larger in the 3-nerve group. The between-group difference in the change in walking pain VAS (pre–post) corresponded to a mean difference of 14.9 mm (95% CI, 3.0–26.8) and a standardized mean difference (Hedges’ g) of 0.85 (95% CI, 0.12–1.58).
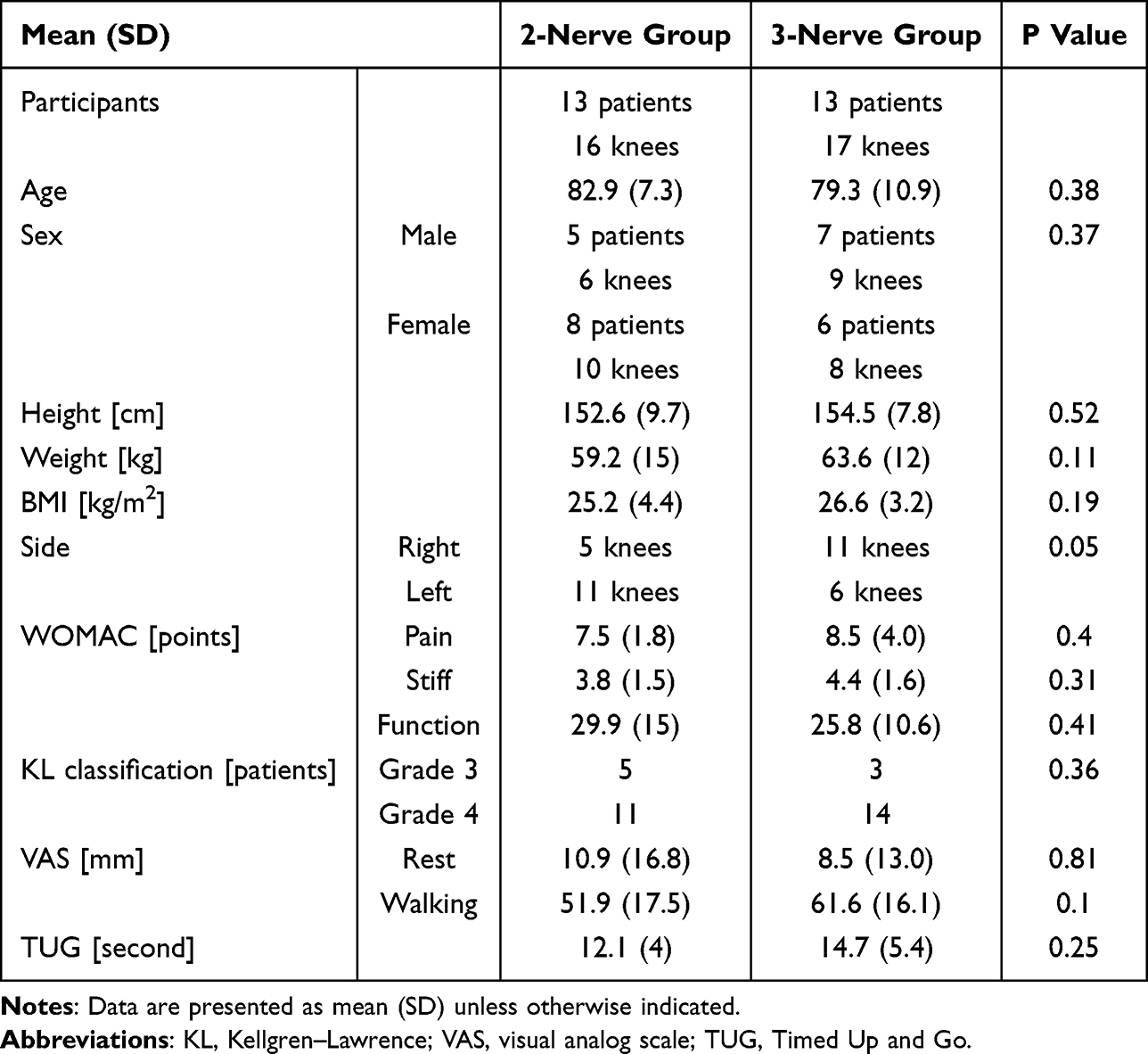 |
Table 1 Baseline Characteristics of the 2-Nerve and 3-Nerve Groups |
Results were materially unchanged in the one-knee-per-participant sensitivity analysis. For the TUG test, TUG time decreased from 12.1 s (pre-block) to 11.0 s (post-block) in the 2-nerve group and from 14.7 s (pre-block) to 12.4 s (post-block) in the 3-nerve group. The between-group difference in the pre–post change in TUG was not significant (p = 0.18) (Figure 1). Results were similarly unchanged in the one-knee-per-participant sensitivity analysis.
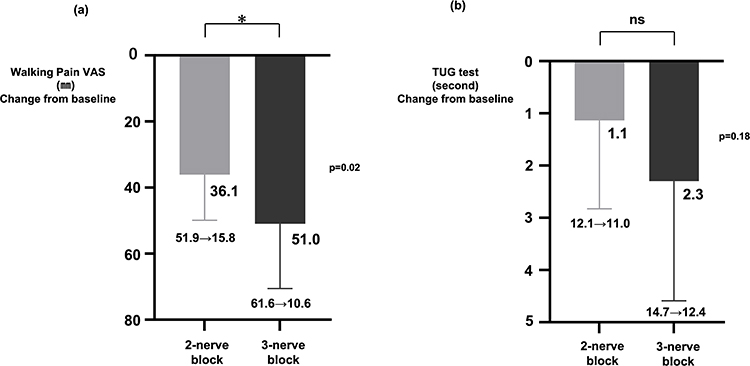 |
Figure 1 Short-term changes in (a) walking pain visual analog scale (VAS) and (b) Timed Up and Go (TUG) test immediately before and after diagnostic genicular nerve blocks. The 2-nerve group received superomedial and inferomedial blocks, and the 3-nerve group received superomedial, inferomedial, and superolateral blocks. Allocation was period-based in routine practice (2-nerve: Oct–Dec 2024; 3-nerve: Jan–Mar 2025). Data are presented as mean ± SD (error bars indicate SD). Between-group comparisons of change scores were performed using the independent t-test or Mann–Whitney U-test. The reduction in walking pain VAS was greater in the 3-nerve group (p = 0.02), whereas the change in TUG did not differ significantly (p = 0.18). Arrow symbols within the numeric labels indicate the change from pre-block to post-block values. *p < 0.05. Abbreviation: ns, not significant. |
Clinical Characteristics of Patients with Insufficient Effect of Medial Genicular Nerve Block
The mean walking pain VAS after medial genicular nerve block was 35.8 mm in the NR group and 6.7 mm in the R group (Table 2). Baseline patient characteristics did not differ significantly between the two groups. Similarly, no significant differences were noted in PPT, TS, or CPM values between the groups.
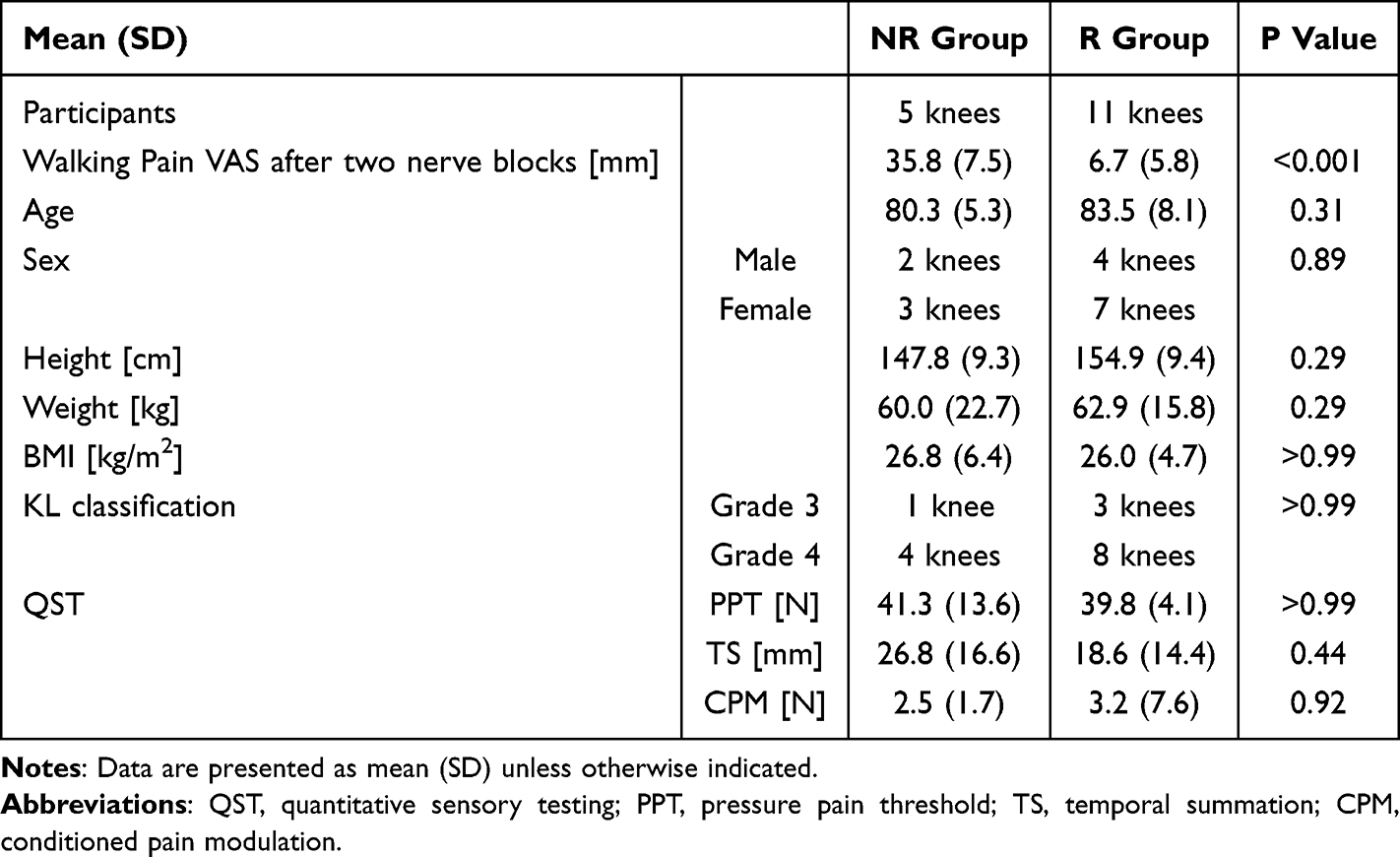 |
Table 2 Characteristics of Responder (R) and Non-Responder (NR) Groups After the 2-Nerve Block |
Regarding MOAKS assessments, no significant differences were observed between groups for osteophytes of the lateral femur (NR: 2.0, R: 2.0; p = 0.91) or lateral tibia (NR: 1.25, R: 1.9; p = 0.40), cartilage damage of the lateral femur (NR: 1.0, R: 1.1; p = 0.85) or lateral tibia (NR: 0.25, R: 0.5; p = 0.88), or meniscal extrusion (NR: 0.25, R: 0.3; p > 0.99) and tears (NR: 1.0, R: 0.6; p = 0.25).
In contrast, BMLs of the lateral femur were significantly more severe in the NR group than in the R group (NR: 2.0, R: 0.5; p = 0.03). Lateral tibial BMLs were higher in the NR group than in the R group (NR: 1.0, R: 0.2); however, this difference was not significant (p = 0.06) (Figure 2). Given the small number of knees in the NR group, these comparisons were considered exploratory.
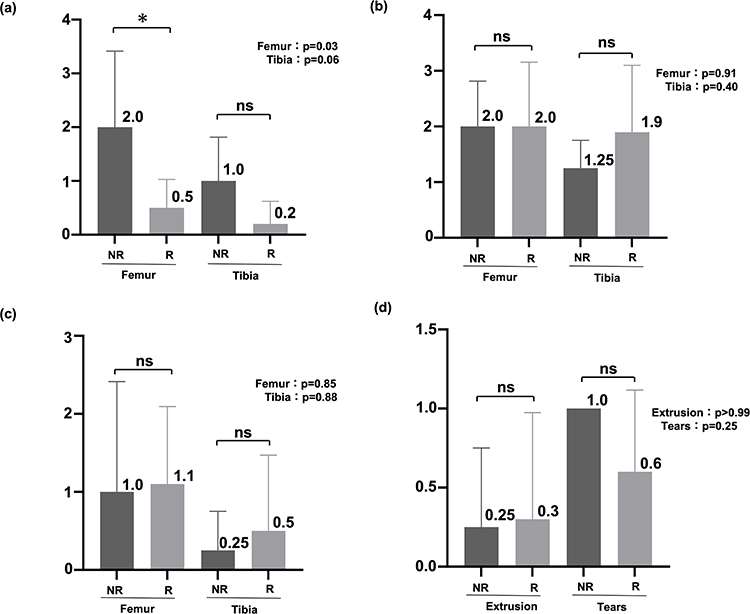 |
Figure 2 MRI Osteoarthritis Knee Score (MOAKS) features in the lateral femorotibial compartment in responder (R) and non-responder (NR) knees after 2-nerve diagnostic genicular nerve blocks: (a) bone marrow lesions (BMLs), (b) osteophytes, (c) articular cartilage, and (d) meniscus. Responders were defined as ≥70% reduction in walking pain VAS; non-responders as <70% reduction (R: n = 11 knees; NR: n = 5 knees). Data are presented as mean ± SD (error bars indicate SD). Between-group comparisons were performed using the Mann–Whitney U-test. *p < 0.05. Lateral femoral BML scores were higher in NR than R knees (p = 0.03), whereas other MOAKS features showed no significant differences. Abbreviation: ns, not significant. |
Discussion
In this study, we propose that the incorporation of a superolateral genicular nerve block to conventional superomedial and inferomedial genicular nerve blocks was associated with additional short-term relief from walking pain in patients with advanced- or end-stage medial knee OA. When BMLs are present in the lateral femoral compartment on MRI, the analgesic effect of medial genicular nerve blocks alone appeared to be insufficient, suggesting that targeting the superolateral genicular nerve might offer greater benefit. Because this was a period-based, non-randomized observational study with immediate post-block assessment, these findings should be interpreted as exploratory associations rather than confirmatory evidence of treatment effect. Importantly, these results reflect only immediate responses to diagnostic lidocaine blocks, and there is a substantial gap between short-term block response and the clinical goal of durable pain relief after RFA; therefore, extrapolation of the present findings to sustained RFA efficacy should be avoided and requires direct confirmation in studies evaluating RFA outcomes with longer follow-up.
Conventionally, the standard targets for RFA in medial knee OA are the superomedial, inferomedial, and superolateral genicular nerves.10 However, Albayrak et al reported no significant improvement with additional superolateral genicular nerve intervention, casting doubts regarding its necessity.11 However, the present study, after analyzing both clinical symptoms and MRI findings, suggests that patients with specific imaging characteristics, particularly lateral femoral BMLs, may represent a subgroup more likely to benefit from a superolateral genicular nerve block. This could represent a novel and clinically relevant finding, although further validation is required. Importantly, the BML-related subgroup observations in this study are hypothesis-generating and should not be interpreted as establishing a definitive predictive biomarker.
From a methodological standpoint, future research could also benefit from data-driven approaches to refine patient stratification. Recent advances in data-driven methods, including machine learning and multimodal data integration, offer the potential to improve patient stratification and outcome prediction by jointly leveraging clinical variables with imaging and sensory measures. While examples from other clinical domains demonstrate the potential of multimodal integration approaches, OA-specific validation is required. Furthermore, given the small sample size and the observational design of the present study, applying complex predictive modeling would carry a high risk of overfitting and is not appropriate at this stage. Future studies with larger cohorts could evaluate whether integrating MRI features (eg, BML-related patterns) with QST and clinical characteristics improves the prediction of short-term diagnostic block response and, importantly, whether such signals extend to longer-term outcomes. 23,24
The insufficient analgesic effect of medial genicular nerve blocks in patients with lateral femoral BMLs can be explained by considering the following two factors: the role of BMLs as potent nociceptive sources and the anatomical distribution of their innervating nerves. BMLs are associated with weight-bearing pain in knee OA.13,14 Histopathological analyses demonstrated increased expression of nerve growth factor and higher osteoclast density within BML regions, which may amplify nociceptive signaling through nerve sprouting and sensitization in the bone marrow and subchondral bone.15 Furthermore, PGP9.5 immunostaining revealed increased nerve fiber density in subchondral bone affected by BMLs.16 These findings collectively support the concept that BMLs represent a critical source of pain in knee OA. Anatomically, the genicular nerves include cutaneous branches as well as fibers innervating the subchondral bone and periosteum.25,26 Pain originating from lateral femoral BMLs is thought to be transmitted, partly, via the superolateral genicular nerve.27,28 Accordingly, in patients with lateral femoral BMLs, blocking only the superomedial and inferomedial branches may leave nociceptive input from the lateral compartment intact, resulting in insufficient analgesia. In contrast, the addition of a superolateral block can suppress subchondral and periosteal pain pathways associated with BMLs, thereby providing additional pain relief. In this study, no significant differences were observed in QST parameters between groups, suggesting that pain sensitivity and central sensitization were unlikely to account for the differential analgesic effect. Rather, these findings support the interpretation that targeting peripheral pain generators, such as lateral femoral BMLs, provides a plausible mechanistic explanation for the additive benefit of the 3-nerve block approach. Nevertheless, mechanistic plausibility does not eliminate the possibility of bias from non-randomized allocation, and causal interpretation should be avoided. Moreover, mechanistic plausibility does not justify assuming that short-lived anesthetic responses will translate into durable benefit after nerve ablation, and this clinical leap should be explicitly recognized.
Furthermore, 76% (25/33 knees) of the patients in this study were classified as KL grade 4, with a mean age of 81.1 years, indicating a cohort of older patients with end-stage disease. Unlike previous studies, this study indicates the potential value of intervention even in more advanced and severe cases, although the findings should be regarded as exploratory and preliminary.
While both groups demonstrated improvement in TUG test performance, no significant difference was observed between the groups. This suggests that while nerve blocks provide immediate analgesic effects, functional outcomes such as gait ability and lower limb performance depend on multiple factors, including muscle strength, balance, and range of motion. Therefore, a single nerve block is unlikely to be sufficient for meaningful functional recovery and should be considered part of a multimodal approach.
Although prior studies have reported comparable outcomes between fluoroscopy- and ultrasound-guided genicular interventions,18 we used ultrasound to guide needle placement and potentially reduce procedure-related complications and because musculoskeletal ultrasound can support the overall treatment strategy in knee osteoarthritis pain care. Ultrasound enables real-time assessment of relevant findings such as effusion and synovitis and, with Doppler, facilitates identification of neurovascular structures to enhance safety and individualize targeting.29,30 Thus, ultrasound may function as an extension of clinical evaluation that informs treatment planning and shared decision-making, rather than serving solely as an injection-guidance tool.
The OARSI-OMERACT criteria (≥50% pain reduction and ≥20 mm decrease) are widely used to define knee OA responders.31 However, this study adopted the definition proposed by Yeom et al and Broadhurst et al, requiring a ≥70% reduction in walking pain VAS to classify patients as responders19,20 This approach was chosen to reduce the risk of underestimating residual pain related to lateral pathology. By applying stricter responder criteria, false positives were minimized, thereby increasing the internal validity of this analysis.
This study had some limitations. First, the sample size was relatively small, limiting the generalizability of the results. The small sample size may have limited statistical power for some comparisons, particularly functional outcomes, certain imaging features, and exploratory subgroup analyses. Therefore, we interpreted these findings cautiously and focused on describing observed differences rather than drawing definitive conclusions. To enhance transparency, we reported effect estimates with 95% confidence intervals for key outcomes (including mean differences and standardized effect sizes); however, because of the observational design and the wide confidence intervals, the effect size estimates should be interpreted cautiously. Second, the group allocation was non-randomized and determined by consecutive clinical periods, which may introduce selection bias and temporal confounding; therefore, causal inference regarding the added block is limited. Although baseline characteristics were similar between groups, this period-based allocation cannot exclude unmeasured differences in patient case-mix or clinical practice over time. Consequently, the between-group VAS difference should be interpreted as an observed association rather than a definitive treatment effect. Although the allocation was period-based, the risk of performance and measurement bias related to operator or assessor differences was mitigated because the same physician conducted all interventions and outcome assessments using an unchanged, standardized protocol throughout the study. Third, the study was conducted in a non-blinded setting, which may have introduced expectation-related reporting and performance bias. Because patients were aware of which block they received, both subjective outcome reporting (eg, VAS) and procedural conduct could have been influenced by expectations, potentially influencing the magnitude of the observed analgesic response. Fourth, subjective outcome measures (eg, VAS) were used without objective assessments (eg, activity monitoring and muscle strength testing). Fifth, the technical accuracy of the nerve block procedures and anatomical variations among patients were not assessed. Sixth, unlike prior studies that compared RFA targeting two versus three genicular nerves, we were unable to perform a direct comparison of 2- versus 3-target RFA because reimbursement requirements in Japan necessitate the ablation of all three standard targets. Consequently, while the present findings may offer insights into target selection, their direct application to RFA protocols remains speculative. Finally, the follow-up period was restricted to immediate post-block assessments, allowing evaluation only of short-term analgesic effects. Accordingly, the findings of this study reflect short-term responses to diagnostic lidocaine blocks rather than definitive evidence of sustained clinical benefit or RFA efficacy, precluding conclusions regarding the durability of pain relief or long-term clinical outcomes and representing the major limitation of this study. Moreover, because only diagnostic blocks were evaluated, any implications for definitive RFA outcomes should be regarded as indirect and require confirmation in future studies directly assessing RFA with appropriate blinding and randomization when feasible. Because some participants provided data from both knees, observations were not entirely independent. To mitigate the potential impact of within-participant clustering, we performed a sensitivity analysis restricted to one knee per participant; when bilateral data were available, the knee with the higher baseline walking VAS was selected. The results of this one-knee-per-participant analysis remained materially unchanged compared with the main analysis, supporting the robustness of our primary findings. Despite these limitations, the current findings provide preliminary evidence suggesting that lateral femoral BMLs may serve as an imaging marker to help identify patients who could be more likely to benefit from additional superolateral genicular nerve intervention. These observations are hypothesis-generating and underscore the need for further large-scale, randomized studies with extended follow-up periods.
Conclusion
In patients with advanced or end-stage medial knee OA, adding a superolateral genicular nerve block to conventional medial blocks was associated with additional short-term pain relief in an immediate post-block assessment. This approach may be particularly useful in patients with lateral femoral BMLs, which may serve as a practical imaging feature to support an individualized diagnostic strategy, such as considering an additional superolateral diagnostic block when medial-only targets provide insufficient analgesia, and to inform diagnostic target selection. From a clinical practice perspective, reviewing lateral-compartment MRI features (particularly lateral femoral BMLs) may help guide diagnostic target selection and support a more individualized, stepwise approach to genicular interventions. However, given that this was a period-based, non-randomized, non-blinded observational study evaluating only short-term responses to diagnostic lidocaine blocks, these findings should be viewed as preliminary and hypothesis-generating rather than confirmatory; they should not be extrapolated to suggest sustained clinical benefit or RFA outcomes. Future studies with larger cohorts and longer follow-up, ideally including randomized and blinded designs with direct evaluation of RFA outcomes, are needed to confirm the clinical value of this strategy and to determine whether it predicts durable pain relief and functional improvement. Because allocation was determined by calendar period in routine practice, the possibility of temporal confounding cannot be fully excluded.
Abbreviations
OA, osteoarthritis; MRI, magnetic resonance imaging; VAS, visual analog scale; MOAKS, MRI osteoarthritis knee score; NR, non-responder; CPM, conditioned pain modulation; PPT, pressure pain threshold; RFA, radiofrequency ablation; BML, bone marrow lesion; TUG, timed up and go; TS, temporal summation; QST, quantitative sensory testing; MCID, minimal clinically important difference; ADL, activities of daily living; TKA, total knee arthroplasty.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Kochi University School of Medicine (approval number: 2024–104) and conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants for the collection of personal data, supplementary information, and publication of study results. Because this was a non-interventional observational study analyzing outcomes of routine care, clinical trial registration was not applicable.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Acknowledgments
We would like to express our sincere gratitude to Koji Aso for his dedicated support in patient recruitment and careful revision of the manuscript. We also thank Natsuki Sugimura and Syo Deguchi for their assistance with patient recruitment. We are grateful to Takahiro Ushida and Masahiko Ikeuchi for their contributions to the study design and critical manuscript review and for providing the necessary environment to conduct this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Mannoni A, Briganti MP, Di Bari M, et al. Epidemiological profile of symptomatic osteoarthritis in older adults: a population based study in Dicomano, Italy. Ann Rheum Dis. 2003;62(6):576–12. doi:10.1136/ard.62.6.576
2. Andrianakos AA, Kontelis LK, Karamitsos DG, et al. Prevalence of symptomatic knee, hand, and Hip osteoarthritis in Greece. The ESORDIG study. J Rheumatol. 2006;33(12):2507–2513.
3. Leveille SG. Musculoskeletal aging. Curr Opin Rheumatol. 2004;16(2):114–118. doi:10.1097/00002281-200403000-00007
4. Quazi M, Madrid R, Thiyagarajan S, et al. Genicular nerve radiofrequency ablation for the treatment of chronic knee pain: systematic review with Bayesian network meta-analysis. Pain Med. 2025:pnaf181. doi:10.1093/pm/pnaf181
5. McCormick ZL, Cohen SP, Walega DR, et al. Technical considerations for genicular nerve radiofrequency ablation: optimizing outcomes. Reg Anesth Pain Med. 2021;46(6):518–523. doi:10.1136/rapm-2020-102117
6. Ikeuchi M, Ushida T, Izumi M, Tani T. Percutaneous radiofrequency treatment for refractory anteromedial pain of osteoarthritic knees. Pain Med. 2011;12(4):546–551. doi:10.1111/j.1526-4637.2011.01086.x
7. Konya ZY, Akin Takmaz S, Başar H, Baltaci B, Babaoğlu G. Results of genicular nerve ablation by radiofrequency in osteoarthritis-related chronic refractory knee pain. Turk J Med Sci. 2020;50(1):86–95. doi:10.3906/sag-1906-91
8. Fonkoue L, Stoenoiu MS, Behets CW, et al. Validation of a new protocol for ultrasound-guided genicular nerve radiofrequency ablation with accurate anatomical targets: cadaveric study. Reg Anesth Pain Med. 2021;46(3):210–216. doi:10.1136/rapm-2020-101936
9. Wong PK, Kokabi N, Guo Y, et al. Safety and efficacy comparison of three- vs four-needle technique in the management of moderate to severe osteoarthritis of the knee using cooled radiofrequency ablation. Skelet Radiol. 2021;50(4):739–750. doi:10.1007/s00256-020-03619-1
10. Choi W-J, Hwang S-J, Song J-G, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011;152(3):481–487. doi:10.1016/j.pain.2010.09.029
11. Albayrak O, Toprak CS, Gunduz OH, Sencan S. Is conventional radiofrequency ablation of the superolateral branch, one of the three genicular nerves targeted as standard, necessary or not? A non-inferiority randomized controlled trial. Korean J Pain. 2024;37(3):264–274. doi:10.3344/kjp.24098
12. Ding C, Wang Y. Association between medial meniscal extrusion and knee structural progression in adults with symptomatic knee osteoarthritis: a prospective cohort study. Skeletal Radiol. 2025;54(2):219–228. doi:10.1007/s00256-024-04731-2
13. Aso K, Shahtaheri SM, McWilliams DF, Walsh DA. Association of subchondral bone marrow lesion localization with weight-bearing pain in people with knee osteoarthritis: data from the osteoarthritis initiative. Arthritis Res Ther. 2021;23(1):35. doi:10.1186/s13075-021-02422-0
14. Zhang Y, Nevitt M, Niu J, et al. Fluctuation of knee pain and changes in bone marrow lesions, effusions, and synovitis on magnetic resonance imaging. Arthritis Rheum. 2011;63(3):691–699. doi:10.1002/art.30148
15. Aso K, Sugimura N, Wada H, Deguchi S, Ikeuchi M. Increased nerve growth factor expression and osteoclast density are associated with subchondral bone marrow lesions in osteoarthritic knees. Osteoarthr Cartil Open. 2024;6(3):100504. doi:10.1016/j.ocarto.2024.100504
16. Koushesh S, Shahtaheri SM, McWilliams DF, et al. The osteoarthritis bone score (OABS): a new histological scoring system for the characterisation of bone marrow lesions in osteoarthritis. Osteoarthr Cartil. 2022;30(5):746–755. doi:10.1016/j.joca.2022.01.008
17. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
18. Kim DH, Lee MS, Lee S, Yoon SH, Shin JW, Choi SS. A prospective randomized comparison of the efficacy of ultrasound- vs fluoroscopy-guided genicular nerve block for chronic knee osteoarthritis. Pain Physician. 2019;22(2):139–146.
19. Broadhurst NA, Bond MJ. Pain provocation tests for the assessment of sacroiliac joint dysfunction. J Spinal Disord. 1998;11(4):341–345. doi:10.1097/00002517-199808000-00013
20. Yeom JS, Lee JW, Park KW, et al. Value of diagnostic lumbar selective nerve root block: a prospective controlled study. AJNR Am J Neuroradiol. 2008;29(5):1017–1023. doi:10.3174/ajnr.A0955
21. Hunter DJ, Guermazi A, Lo GH, et al. Evolution of semi-quantitative whole joint assessment of knee OA: MOAKS (MRI Osteoarthritis Knee Score). Osteoarthr Cartil. 2011;19(8):990–1002. doi:10.1016/j.joca.2011.05.004
22. Izumi M, Hayashi Y, Saito R, et al. Detection of altered pain facilitatory and inhibitory mechanisms in patients with knee osteoarthritis by using a simple bedside tool kit (QuantiPain). PAIN Rep. 2022;7(3):e998. doi:10.1097/PR9.0000000000000998
23. Lyu X, Liu J, Gou Y, et al. Development and validation of a machine learning-based model of ischemic stroke risk in the Chinese elderly hypertensive population. View. 2024;5(6):20240059. doi:10.1002/VIW.20240059
24. Yuan Y, Zhang X, Wang Y, et al. Multimodal data integration using deep learning predicts overall survival of patients with glioma. View. 2024;5(5):20240001. doi:10.1002/VIW.20240001
25. Morgan M, Nazemian V, Harrington K, Ivanusic JJ. Mini review: the role of sensory innervation to subchondral bone in osteoarthritis pain. Front Endocrinol. 2022;13:1047943. doi:10.3389/fendo.2022.1047943
26. Devor M. Pain in osteoarthritis: driven by intrinsic rather than extrinsic joint afferents and why this should impact treatment. Interv Pain Med. 2023;3(1):100381. doi:10.1016/j.inpm.2023.100381
27. Kim JH, Shustorovich A, Arel AT, Downie SA, Cohen SP, Kim SY. Genicular nerve anatomy and its implication for new procedural approaches for knee joint denervation: a cadaveric study. Pain Med. 2022;23(1):144–151. doi:10.1093/pm/pnab238
28. Fonkoué L, Behets C, Kouassi JK, et al. Distribution of sensory nerves supplying the knee joint capsule and implications for genicular blockade and radiofrequency ablation: an anatomical study. Surg Radiol Anat. 2019;41(12):1461–1471. doi:10.1007/s00276-019-02291-y
29. Rossi-Semerano L, Breton S, Semerano L, et al. Application of the OMERACT synovitis ultrasound scoring system in juvenile idiopathic arthritis: a multicenter reliability exercise. Rheumatology. 2021;60(8):3579–3587. doi:10.1093/rheumatology/keaa804
30. Bains SS, Swartz GN, Katanbaf R, et al. Platelet-rich plasma injections are inferior to corticosteroid injections for short-term pain relief: a prospective, double-blinded, randomized controlled trial. J Arthroplasty. 2025;40(7 Suppl 1):S59–S64. doi:10.1016/j.arth.2025.03.013
31. Pham T, Van Der Heijde D, Lassere M, et al. Outcome variables for osteoarthritis clinical trials: the OMERACT-OARSI set of responder criteria. J Rheumatol. 2003;30(7):1648–1654.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.