")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 16
Superior Mesenteric Artery Syndrome as a Rare Cause of Postoperative Intractable Vomiting: A Case Report
Authors Edem S , Goswami AG, Karki B, Acharya P, Chauhan U, Kumar N , Basu S
Received 23 April 2023
Accepted for publication 24 June 2023
Published 29 June 2023 Volume 2023:16 Pages 101—105
DOI https://doi.org/10.2147/CEG.S416391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Wing-Kin Syn
Sanketh Edem,1 Aakansha Giri Goswami,1 Bibek Karki,1 Preeti Acharya,1 Udit Chauhan,2 Navin Kumar,1 Somprakas Basu1
1Departments of General Surgery, All India Institute of Medical Sciences, Rishikesh, India; 2Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, India
Correspondence: Somprakas Basu, General Surgery, All India Institute of Medical Sciences, Virbhadra Road, Rishikesh, 249203, India, Email [email protected]
Background: Superior mesenteric artery syndrome is a very rare cause of proximal intestinal obstruction. The objective of this clinical case report is to highlight that this unusual condition can occur in the early postoperative period and medical management may completely cure the condition.
Clinical Case: A middle-aged female who was being treated for pulmonary tuberculosis underwent exploratory laparotomy with limited ileal resection and a loop ileostomy for multiple ileal perforations. Postoperatively, she was restarted on anti-tubercular drugs (ATD) but developed a drug reaction, recurrent bilious vomiting, and jaundice and ATD had to be stopped. But her vomiting did not abate and she progressively developed septicemia. An abdominal CT scan diagnosed Wilkie’s syndrome, and she was managed non-operatively by decubitus, parenteral nutrition, and nasojejunal tube feeding supplemented with prokinetics and antibiotics. But her sepsis did not resolve. Intraoperative histopathology suggested Candida infection, and she recovered only after systemic antifungal therapy.
Discussion: Debilitation conditions like tuberculosis cause weight loss and loss of intra-abdominal fat pad, which is known to precipitate SMA syndrome. However, its presentation in the early post-operative period is rare. Symptoms may vary from non-specific abdominal fullness and weight loss to features of acute bowel obstruction. CECT of whole abdomen can help in confirming the diagnosis. SMA syndrome is often not considered in differential diagnosis and can delay treatment. Medical management is the mainstay treatment option, although surgery is reserved for cases, which fail medical treatment.
Conclusion: High suspicion is needed to diagnose SMA syndrome in the postoperative period, which precipitates with intractable bilious vomiting. Medical management may be curative. The precipitating factor for SMA syndrome should also be addressed to improve the overall patient outcome.
Keywords: superior mesenteric artery syndrome, postoperative nausea and vomiting, fungal infection, medical therapy, Wilkie’s syndrome
Introduction
First described by Wilkie in 1927, superior mesenteric artery (SMA) syndrome, also known as Wilkie’s syndrome is an unusual cause of duodenal obstruction.1 It is characterized by compression of the distal duodenum due to the narrowing of the space between the superior mesenteric artery and the aorta and is commonly attributed to the loss of the intervening retroperitoneal fat pad due to rapid weight loss. Predisposing factors causing loss of weight and fat pad include debilitating illnesses like malignancy, malabsorption syndromes, AIDS, trauma, and burns.2 In the congenital variety, short ligament of Treitz causes high insertion of duodenojejunal angle, compressing the third part of duodenum. The reported incidence in the literature ranges from 0.1% to 0.3%3 and females between 10 and 40 years are most commonly affected.4 Symptoms vary from abdominal pain, post-prandial vomiting, bilious vomiting to sense of fullness, upper abdominal discomfort, and weight loss depending upon the onset of presentation.5 Radiological imaging like Computed tomography (CT) helps clear visualization of duodenal compression besides confirming the diagnosis by measuring the aortomesenteric distance and angle.6 Medical management in form of refeeding and weight gain is the mainstay of treatment with the ultimate aim to regain the lost intraabdominal fat.7
SMA syndrome precipitating in the postoperative period of major emergency abdominal surgery is a much rarer event. We present a case of SMA syndrome in the early postoperative period in a young woman. The postoperative period was complicated by fungal septicemia and significant weight loss causing acute duodenal obstruction. The rare nature of the disease in the early postoperative period, which was managed successfully by non-operative therapy, is highlighted so that its awareness can lead to early diagnosis and management.
Case Presentation
A 36-year-old woman presented in the emergency room with a history of central abdominal pain for 3 days and complaints of abdominal fullness and vomiting for the last 2 days associated with non-passage of flatus and feces. She also gave a history of evening rise in temperature and non-productive cough for the past 3 months. She was receiving antitubercular treatment for pulmonary tuberculosis, which was diagnosed 3 months back. Upon examination, she was found to be in distributive shock with mild pallor and a body mass index (BMI) of 17.8 kg/m2. The abdomen was distended, tender with muscle guard, and peristaltic sounds were absent. A contrast-enhanced CT (CECT) scan of the whole abdomen showed pneumo-peritoneum with ascites and dilated bowel loops. She was taken up for an emergency exploratory laparotomy, and during surgery 3 l of foul-smelling enteric fluid was drained and two perforations were found in the terminal ileum 60 cm proximal to the ileocecal junction. The 5 cm segment bearing the perforations was resected, and a double-barrel ileostomy was fashioned. Postoperatively, her stoma started functioning within 48 h, she was allowed a soft diet by the fifth day and was advised on restarting the ATD. She developed a deep surgical site infection (SSI) on the seventh day, which was managed by antibiotics and regular dressings.
In the second week, she started developing recurrent bilious vomiting and a low-grade fever for which she was resuscitated with intravenous fluids, proton pump inhibitors, and prokinetics. She developed bilateral moderate pulmonary effusion and jaundice (total bilirubin 3.4 mg/dl), for which multiple percutaneous pleural taps were done, and she was started on second-line ATD. However, her bilious vomiting persisted even after stopping the first-line ATD. A gastroduodenoscopic examination revealed edematous but normal duodenal mucosa and a progressive luminal compromise until the third part (D3), beyond which the scope could not be negotiated suggestive of extrinsic compression. An attempt to negotiate a nasojejunal feeding tube beyond the D3 failed, and she was started on total parenteral nutrition. A CECT whole abdomen showed a distention of the proximal duodenum with air-fluid level and a transition point at the distal D3. There was no abnormal mural thickening, and the D4 and jejunal loops were found collapsed. The aorto-mesenteric angle was 16.5◦ (Figure 1) and the aorto-mesenteric distance was 6.38 mm (Figure 2), suggesting SMA syndrome. A trial of non-operative management was started due to her early postoperative status. She was nursed in the left lateral position with continuous nasogastric aspiration and parenteral nutritional support.
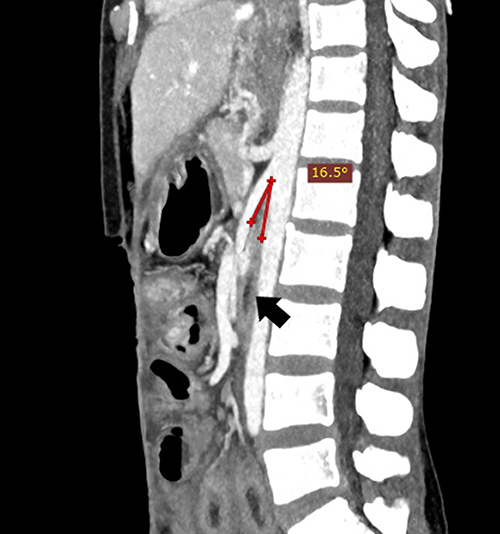 |
Figure 1 Aorto-mesenteric angle is 16.5◦. The compressed duodenum (D3) is marked with a black arrow. |
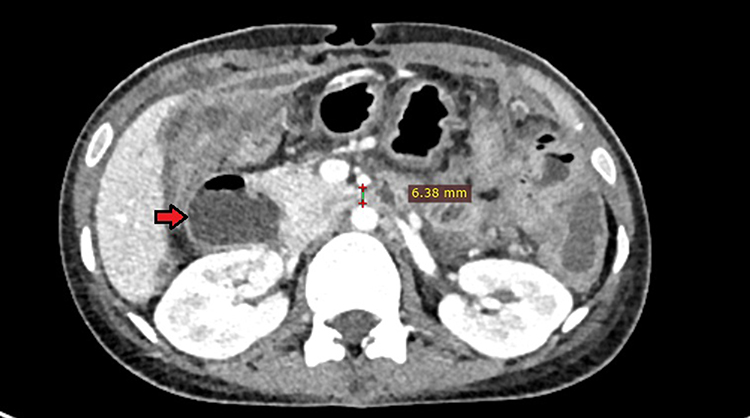 |
Figure 2 Aorto-mesenteric distance is 6.38 mm. Compression of the duodenum (D3) with distended proximal duodenum (D2) showing air-fluid level (red arrow). |
In the third postoperative week, she started developing features of septicemia, and hypotension. She was placed on vasopressor support for persistent hypotension and intravenous injection of Meropenem and Metronidazole for septicemia to which she did not respond adequately. Histopathological report of the resected intestinal segment showed areas of inflammatory infiltrates with fungal colonies, and the fungal culture was positive for Candida spp., which was treated with systemic antifungal agents. By the end of the third week, due to the subsidence of mucosal edema, a nasojejunal feeding (NJ) tube could be placed endoscopically beyond the narrowed segment, and tube feeding was started. Gradually over the next week, she responded to treatment, her vomiting subsided, she became afebrile, and started tolerating a liquid diet. After the fifth week, she started tolerating a normal diet by mouth and was discharged. She registered an increase in body weight by almost 3 kg at the end of the second month of follow-up.
Discussion
SMA syndrome is an uncommon postoperative complication following surgery. Predisposing factors include debilitating illnesses such as malignancy, malabsorption syndromes, AIDS, trauma, and burns.2 It has been described in a variety of other disorders associated with profound weight loss, including bariatric surgery, spinal cord injury, paraplegia, drug abuse, prolonged bed rest, and anorexia nervosa.8,9 In the congenital variety, a short ligament of Treitz leads to a more cephalad position of the duodenojejunal angle, resulting in compression of the D3. Patients with mild incomplete obstruction may have only postprandial epigastric pain and early satiety, while those with more advanced obstruction may have severe nausea, bilious emesis, and weight loss. But acute presentations are rare. Abdominal CECT/MRI is the investigation of choice. The normal angle between the superior mesenteric artery and the aorta is between 38◦ and 65◦,10 and the aortomesenteric distance is normally 10 mm to 28 mm.11 An aorto-mesenteric angle of less than 20◦ and an aorto-mesenteric distance of less than 8 mm in adults is diagnostic of SMA syndrome.12 The reason believed to precipitate the condition is a rapid loss of the retroperitoneal fat pad that cushions the duodenum in the aorto-mesenteric angle.
Initially, patients are offered non-operative management and nursed in the left lateral position. Nutritional improvement, correction of fluid and electrolyte imbalance, and treatment of background disease, if any, are the cornerstones of medical management. Enteric nutrition via an NJ tube is usually preferred, but if such a tube cannot be negotiated, parenteral nutrition becomes an option. If patients do not improve, a surgical bypass should be done. Several surgical techniques have been described including mobilization of the ligament of Treitz and bringing down the DJ angle inferiorly (Strongs procedure) and drainage procedures such as gastrojejunostomy and duodenojejunostomy. Of these, duodenojejunostomy provides the best results.13 Given her recent postoperative status, our patient was managed conservatively with parenteral and then enteral nutrition, prokinetics, and proton pump inhibitors, and nutritional support. Fungal septicemia was diagnosed and promptly managed with systemic antifungal agents. It is a well-established practice now to send peritoneal fluid and biopsy for fungal cultures along with bacterial cultures.14
This report highlights two important issues about SMA syndrome. Although SMA syndrome commonly presents with a more protracted course of over months, it can present as an acute intestinal obstruction in the postoperative period,15 probably either due to adhesion formation and traction on the mesentery or due to rapid weight loss in the background of a low BMI. We believe the latter is the cause in the present case. The patient was already emaciated and underweight when she presented to our emergency. Tuberculosis itself causes loss of weight and as mentioned earlier, weight loss and loss of fat pads are known causes for precipitation of SMA syndrome. Due to illness and lack of nutrition, patient reached a critical limit, which manifested early in the post-operative period. Adhesive bowel obstruction is an implausible cause of SMA syndrome in the present case as the patient did not demonstrate any clinical or radiological evidence of adhesive bowel obstruction. Besides, duodenum being a retroperitoneal organ is unlikely to develop adhesions, especially in a case of ileal perforation.
Postoperative vomiting has several etiologies but SMA syndrome as a cause is not usually considered. Intractable postoperative bilious vomiting should arouse suspicion of the condition and a gastroduodenoscopy and a CT scan can diagnose the condition early. Secondly, medical management should always be an initial option in such cases. In the present case, due to her recent postoperative status, medical management was preferred. Over the next few weeks, medical management helped bring down her vomiting, correction of fluid-electrolyte imbalance, and improve her nutritional status. Therefore, it is likely that a similar approach should be effective in other cases of SMA syndrome also. Interestingly, no time duration has been defined beyond which medical management should be considered ineffective.16 Also, medical management has been shown to be ineffective in 50–75% of cases.17 Nevertheless, medical management can tide over acute conditions during which surgical outcomes can be challenging, as happened in the present case. When medical management fails or when definite indications for surgery exist such as in pancreatitis,15 surgical intervention is mandated.
Limitations
Long-term follow-up beyond second post-operative month is a major limitation of the current case report. We do not have data regarding significant weight gain, recurrence of symptoms, completion of anti-tubercular drug treatment and stoma reversal.
Conclusion
SMA syndrome should be clinically suspected in postoperative patients with recurrent bilious vomiting and features of upper gastrointestinal obstruction. An abdominal CECT scan is diagnostic and should be done early during management. Initial medical management is effective and should be the first option unless there are compelling contraindications to it. Surgical management should be considered only after the failure of a trial of medical management in sick patients. Moreover, the underlying cause of weight loss and the precipitating factor for SMA syndrome should be addressed and treated to optimize the patient outcome.
Disclosure
The authors report no conflicts of interest in this work and no funding was received for the preparation and publication of the article. Written consent for publication was obtained from the patient. This article received Institutional Ethics Committee approval for publication.
References
1. Gthrie RH
2. Agarwal T, Rockall TA, Wright AR, Gould SW. Superior mesenteric artery syndrome in a patient with HIV. J R Soc Med. 2003;96(7):350–351. doi:10.1258/jrsm.96.7.350
3. Salem A, Al Ozaibi L, Nassif SMM, Osman RA, Al Abed NM, Badri FM. Superior mesenteric artery syndrome: a diagnosis to be kept in mind (Case report and literature review). Int J Surg Case Rep. 2017;34:84–86. doi:10.1016/j.ijscr.2017.03.018
4. Lee TH, Lee JS, Jo Y, et al. Superior mesenteric artery syndrome: where do we stand today? J Gastrointest Surg. 2012;16(12):2203–2211. doi:10.1007/s11605-012-2049-5
5. Rabie ME, Ogunbiyi O, Al Qahtani AS, Taha SB, El Hadad A, El Hakeem I. Superior mesenteric artery syndrome: clinical and radiological considerations. Surg Res Pract. 2015;2015:628705. PMID: 26347903; PMCID: PMC4549571. doi:10.1155/2015/628705
6. Waheed KB, Shah WJ, Jamal A, et al. Superior mesenteric artery syndrome: an often overlooked cause of abdominal pain! Saudi Med J. 2021;42(10):1145–1148. doi:10.15537/smj.2021.42.10.20210509
7. England J, Li N. Superior mesenteric artery syndrome: a review of the literature. J Am Coll Emerg Physicians Open. 2021;2(3):e12454. doi:10.1002/emp2.12454
8. Goitein D, Gagné DJ, Papasavas PK, et al. Superior mesenteric artery syndrome after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg. 2004;14(7):1008–1011. doi:10.1381/0960892041719626
9. Pentlow BD, Dent RG. Acute vascular compression of the duodenum in anorexia nervosa. Br J Surg. 1981;68(9):665–666. doi:10.1002/bjs.1800680918
10. Derrick JR, Fadhli HA. Surgical anatomy of the superior mesenteric artery. Am Surg. 1965;31:545–547.
11. Sapkas G, O’Brien JP. Vascular compression of the duodenum (cast syndrome) associated with the treatment of spinal deformities. A report of six cases. Arch Orthop Trauma Surg. 1981;98(1):7–11. doi:10.1007/BF00389703
12. Warncke ES, Gursahaney DL, Mascolo M, Dee E. Superior mesenteric artery syndrome: a radiographic review. Abdom Radiol. 2019;44(9):3188–3194. doi:10.1007/s00261-019-02066-4
13. Ylinen P, Kinnunen J, Höckerstedt K. Superior mesenteric artery syndrome. A follow-up study of 16 operated patients. J Clin Gastroenterol. 1989;11(4):386–391. doi:10.1097/00004836-198908000-00007
14. Jindal N, Arora S, Pathania S. Fungal culture positivity in patients with perforation peritonitis. J Clin Diagn Res. 2015;9(6):DC01–DC3. doi:10.7860/JCDR/2015/13189.6050
15. Claro M, Sousa D, Abreu da Silva A, Grilo J, Martins JA. Wilkie’s syndrome: an unexpected finding. Cureus. 2021;13(12):e20413. doi:10.7759/cureus.20413
16. Zaraket V, Deeb L. Wilkie’s syndrome or superior mesenteric artery syndrome: fact or fantasy? Case Rep Gastroenterol. 2015;9(2):194–199. doi:10.1159/000431307
17. Lorentziadis ML. Wilke’s syndrome. A rare cause of duodenal obstruction. Ann Gastroenterol. 2011;24(1):59–61.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.