Back to Journals » International Medical Case Reports Journal » Volume 16
Superficial Basal Cell Carcinoma on the Back Region Treated with a Combination of Cryotherapy and 5% Imiquimod Cream: A Case Report
Authors Sutedja EK ![]() , Elgianda GS, Sutedja E
, Elgianda GS, Sutedja E ![]() , Ruchiatan K
, Ruchiatan K
Received 23 February 2023
Accepted for publication 9 June 2023
Published 26 June 2023 Volume 2023:16 Pages 391—396
DOI https://doi.org/10.2147/IMCRJ.S409840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Eva Krishna Sutedja, Ghabrina Saraswati Elgianda, Endang Sutedja, Kartika Ruchiatan
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Eva Krishna Sutedja, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Tel +62222032426 ext. 3449, Fax +62222032426, Email [email protected]
Abstract: Basal cell carcinoma (BCC) is the most common skin malignancy, consisting of cells in the basal layer epidermis and its appendix. Superficial BCC is the second most common BCC subtype with a predilection on the trunk including the waist and can be treated with cryoimmunotherapy, a combination of cryotherapy and imiquimod cream. Herein, we report a case of superficial BCC in a 60-year-old woman which was triggered by short-wave diathermic (SWD) therapy on the waist one year previously. Superficial BCC was diagnosed based on clinical symptoms, a dermoscopy, and histopathology. The erythematous and hyperpigmented plaque on the waist had well-defined edges and bled easily. There were pseudopods, a blue-grey ovoid nest, haemorrhagic ulceration, and a deeply pigmented border with basaloid cells in the basal layer of the epidermis and palisade cells at the edges. The patient was treated with cryoimmunotherapy consisting of two cycles of a 30-second freeze time and a 5 mm margin, then two weeks later, 5% imiquimod cream was applied to the skin for five consecutive nights, followed by two days off for six cycles (six weeks). Follow-up at three months revealed clinical improvement with reduced lesion size, confirming that cryoimmunotherapy is an effective treatment for the management of superficial BCC with mild side effects.
Keywords: cryoimmunotherapy, superficial basal cell carcinoma, therapy
Introduction
Basal cell carcinoma (BCC) is a common skin malignancy, with a 65% incidence rate of epithelial tumors.1 This origin cell of BCC is still unclear and considered to arise from the basal layer of the epidermis, adnexal structures,2,3 or basal cells which differentiate to glandular cell.3 It is locally aggressive and usually grows slowly over several months to years.2 Clinical variants of BCC include nodular, superficial, morpheaform, pigmented, and fibroepithelioma of Pinkus (PEF), with the most frequently reported being nodular, superficial, and morpheaform.4 BCC generally appears on areas exposed to sunlight but in some rare cases, it is found on unexposed body parts including the trunk, buttocks, genitals, nails, axilla, areola, and soles. BCC that appears in unexposed areas is usually the superficial subtype which can be triggered by trauma, burns, cold exposure, radiotherapy, thermal radiation therapy, and photosensitive drugs.5
Therapeutic modalities for BCC include conventional surgical excision, Mohs micrographic surgery, destructive therapy (cryotherapy, carbon dioxide laser ablation, curettage, and electrodesiccation), radiation therapy, and topical therapy (imiquimod and fluorouracil).4 The choice of therapeutic modality is based on tumor size, anatomical location, tumor boundaries, BCC subtypes, and risk of recurrence,4,6 with low-risk BCCs treated by excision, electrodesiccation, curettage, and cryotherapy.6
The main goal of cryotherapy in BCC is to destroy the same amount of tissue as local excision, with a margin of 3 to 5 mm. Cryotherapy is performed in several cycles and treatment sessions are based on clinical response.7 It can be combined with imiquimod cream, known as cryoimmunotherapy,8 to increase tissue destruction. Cryoimmunotherapy is minimally invasive without causing significant damage to surrounding tissue and has been proven effective for superficial BCC lesions.8,9 MacFarlane et al conducted a study of 50 superficial BCC patients treated with cryoimmunotherapy for six weeks which yielded a good response with minimal side effects.9
There were 43 cases of BCC according to the outpatient medical records in the Dermatology and Venereology Polyclinic, General Hospital Dr Hasan Sadikin Bandung from 1 January 2019 to 30 July 2022. Herein, we report a case of superficial BCC on the back of a 60-year-old woman treated with a combination of cryotherapy and 5% imiquimod cream.
Case
A 60-year-old woman was referred by the Dermatovenereologist to the Tumor and Surgery Division of Dermatology and Venereology Department General Hospital Dr Hasan Sadikin Bandung with erythematous plaques accompanied by hyperpigmented plaques that bled easily on the waist which sometimes felt itchy.
The skin lesions first appeared approximately two years previously in the form of an erythematous plaque that bled easily and felt itchy in the middle of the waist. The patient was given topical medication by a general practitioner with no improvement. One year later, the skin lesion began to grow in the form of erythematous plaques accompanied by hyperpigmented plaques on the edges that were painful. Two months before admission, the preexisting skin lesions had increased in number and bled easily, so the patient went to the Dermatovenereologist and was referred to General Hospital Dr Hasan Sadikin. The patient had a history of SWD physiotherapy on the waist from 2019 to 2022 for bilateral knee osteoarthritis.
A physical examination revealed that the patient with body mass index 28 kg/m2 and had a solitary, irregularly shaped erythematous measuring 3.5 × 3 × 0.1 cm (Figure 1A) that was well defined, partially raised, dry, and located on the waist with hyperpigmented plaques (Figure 1B). Dermoscopic examination (Figure 2) showed pseudopods (black arrow), a blue-grey ovoid nest (red arrow), hemorrhagic ulcerations (yellow arrow), and deeply pigmented bordered (blue arrow) indicative of superficial BCC. Histopathological examination revealed stratified squamous epithelium, tumor mass at the basal layer (Figure 3) which consisted of round, oval, hyperplastic, condensed, and clustered cells with the tumor cells formed a palisading structure on the edges (red circle). The nuclei were pleomorphic and hyperchromatic with mitotic cell nuclei, and some cells contained melanin pigment. The histopathological findings supported the diagnosis of BCC. Two cycles of cryotherapy were utilised to treat the lesion with an open spray technique and liquid nitrogen cryogen (5 mm margin), followed by the application of 5% imiquimod cream on the lesion two week after cryotherapy, once per day for five consecutive nights two days apart for six weeks. The three-month follow-up revealed the skin lesion improved leaving hyperpigmented scars without new skin disorders.
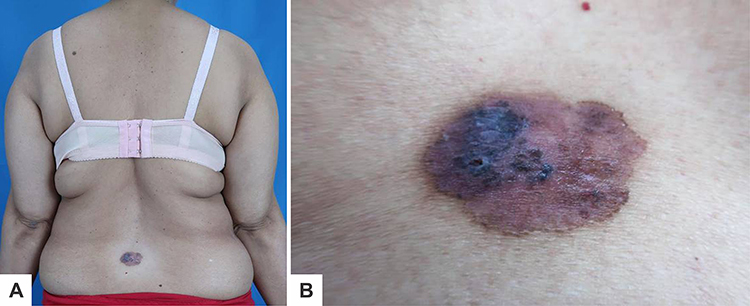 |
Figure 1 Dermatological examination showing: (A) A solitary lesion with an irregular shape on the waist (B) 3.5×3 x 0.1 cm of erythematous and hyperpigmented plaques. |
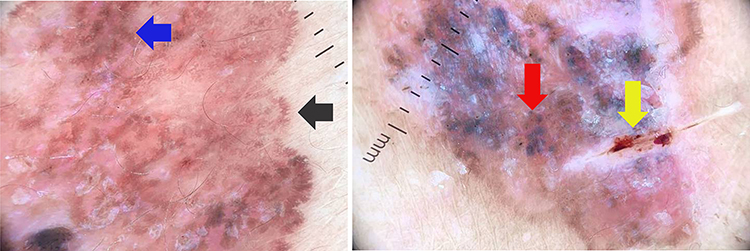 |
Figure 2 Dermoscopic examination showing pseudopods (black arrow), a blue-grey ovoid nest (red arrow), haemorrhagic ulcerations (yellow arrow), and a deeply pigmented border (blue arrow). |
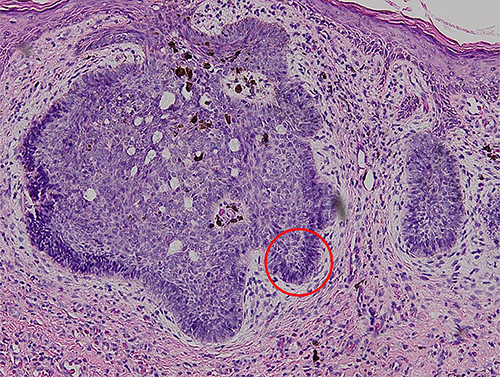 |
Figure 3 Histopathological examination showing that the tumor cells formed a palisading structure (red circle) (Hematoxylin-eosin stain, 100x magnification). |
Discussion
In 2019, there were 4 million new cases of BCC worldwide and a retrospective study by Wibawa et al of 263 patients from 2014 to 2017 with skin cancer at Cipto Hospital Mangunkusumo reported that 66.9% of skin cancers were BCC.10 BCC generally occurs between 50 and 80 years and the incidence increases with age. It is more common in men than women with a ratio of 1.5–2:1.11 Herein, we reported the case of BCC in a 60-year-old woman.
BCC can be induced by environmental factors, such as exposure to ultraviolet (UV) light, ionisation, and chemical carcinogens,4 with trauma, burns, exposure to cold, radiotherapy, thermal radiation therapy, and photosensitive drugs also reported to be associated with BCC.5 Short-wave diathermic therapy (Marconi therapy) is an endogenous radiofrequency thermal therapy utilising high-frequency induced currents to treat chronic pain inflammation in musculoskeletal and neuralgia. In 1998 in Italy, Betti et al conducted a retrospective study of 76 BCC patients in the lumbosacral region showing that 14 patients with superficial BCC had a history of SWD therapy.12 The mechanism for the occurrence of BCC due to SWD therapy is still unknown.5 Our patient had SWD therapy one year before the skin disorder appeared, therefore, SWD therapy may be a risk factor for BCC in this case.
Typically about 75%13 BCC occurs on sun-exposed areas like the head and neck,4,13 but in rare cases, only about 10% BCC can also be found on unexposed areas including the trunk,13 genitals, nails, axillae, areola, and soles.4 BCC lesion in this current case was located on the lower back, consistent with the rare predilection of BCC. Generally, BCC lesions continue to enlarge slowly, are difficult to heal, bleed easily and may be accompanied by itching or asymptomatic. Based on the clinical symptoms, BCC is classified as nodular, morpheaform, infiltrative, pigmented, FEP, or superficial.14 There is a possible correlation between tumor location and histological subtype, some studies showed that unexposed areas such as the trunk and limbs display a predominantly superficial pattern, while those in sun exposed areas like the nose, neck and head, show mainly nodular pattern.8 Superficial type BCC is the second most common subtype with a prevalence of 10% to 30%.14,15 This disorder generally occurs in the fifth decade, with an increased incidence in women compared to other subtypes.15 The skin lesions are in the form of erythematous macules or plaques, with a diameter of several millimetres to 10 cm, well-defined, accompanied by slight scaling or superficial erosion, and often found on the trunk. It can occur as single or multiple lesions.2 In the current case report, it occurred as a solitary lesion in the form of an erythematous and hyperpigmented plaque in the middle of the waist, consistent with the clinical symptoms of superficial BCC.
Dermoscopy can detect early-stage BCC and distinguish BCC subtypes with a sensitivity of 98.6% and a specificity of 99%.16 BCC consist of vascular structures (arborizing vessels and short fine telangiectasias), pigment-related structures (maple leaf-like areas, spoke-wheel areas, blue-grey nests and globules, in-focus dots, and concentric structures), and non-vascular and non-pigmented structures (ulcerations, multiple small erosions, shiny white-red structureless areas, and white streaks).16,17 The diagnosis of BCC is established if two conditions are met, the absence of pigmentation and the presence of one of the six BCC criteria (large blue-grey ovoid nests, multiple blue-grey dots/globules, maple leaf-like areas, spoke wheel areas, and arborising vessels).18 The main criteria for superficial BCC are shiny white to red areas, short fine telangiectasias, and small erosions on the lesion surface.17 The present case had blue-grey ovoid nests, hypopigmented areas, pseudopods, hemorrhagic ulcerations, red structureless areas, and leaf-like areas consistent with the superficial subtype BCC dermoscopy features.
Histopathological examination of excised tissue confirmed the diagnosis and estimate the risk of BCC recurrence.2 Through this examination can differentiated low-risk to high-risk subtype of BCC, provide an overview of excised margins, verify histological type, depth of invasion, lymphovascular invasion, and perineural involvement.18 Common histopathological BCC features include uniform proliferation of basaloid cells with hyperchromatic nuclei, and scanty cytoplasm. Morphologically, the basaloid cells resemble epidermal basal cells and have properties like follicular germ cells.2 Each BCC subtype has a different histopathological picture.15 In superficial type BCC, basaloid cells extend into the dermis from the basal epidermal layer and the peripheral layer shows prominent palisade cells.4 Histopathological examination of the current case revealed basaloid cells in the basal epidermal layer and palisade cells on the edges, consistent with the histopathological features of superficial BCC.
Bowen’s disease (BD) is one of the differential diagnoses of superficial BCC and occurs as pink to salmon-red patches or plaques that grow slowly, are well-defined and accompanied by white or yellow scales.19 BD typically occurs in sun-exposed areas and the dermoscopic appearance varies depending on the subtype but generally, glomerular vessels and scaly surfaces are observed.20 Histopathological examination is the gold standard for establishing the diagnosis of BD which is characterised by hyperkeratosis and parakeratosis in the epidermis, acanthosis with elongation and thickening of the rete ridges. Keratinocytes show intense mitotic activity, pleomorphism, and very large nuclei. The cells of the upper dermis were vacuolated with abundant eosinophilic cytoplasm.21 The patient in this case had the clinical features of BD but the lesion predilection did not match BD, so the differential diagnosis of BD was ruled out.
The main goal of skin cancer therapy is to remove the entire tumor to prevent recurrence, restore normal function, and provide good cosmetic results,6 so several factors need to be considered including patient age, tumor size, anatomical location, tumor boundaries, BCC subtype, and risk of recurrence.7 High-risk BCC is more than 2 cm in size, has a predilection in the middle of the face or ear, aggressive histopathological subtypes (infiltrative, sclerotic, and morpheaform), and a high recurrence rate from previous treatment. Low-risk BCCs are less than 1 cm, have a predilection for the torso or extremities, and non-aggressive histopathological subtypes (nodular and superficial).6 Thus can be treated with excision, electrodesiccation, curettage, and cryotherapy.19 Cryotherapy and topical therapies, such as imiquimod and 5-fluorouracil (5FU) can be used as alternatives to surgery are required.22 In a study by Gross et al, BCC treated with 5FU twice daily for 12 weeks showed a 90% cure rate.23
Cryotherapy is a fast and low-cost freeze-thaw technique that destroys tissue by direct cell injury and statics in blood vessels.19 This technique provides a 94% to 99% cure rate for BCC,6 but its usage is limited to well-differentiated small, well-demarcated, superficial, and low-risk BCC subtypes.7,24 Cryotherapy is typically performed in one to two cycles with an average freeze time of 30 seconds and a maximum margin of 5 mm. The recurrence rate after cryotherapy is less than 8%7 and associated complications during and after treatment include local pain, extended healing time with increase risk for local infection, and poor cosmetic result (inflammatory hyperpigmentation, hypertrophic scarring, and tissue defect).24 To increase tissue destruction, cryotherapy can be combined with the administration of imiquimod cream, also known as cryoimmunotherapy. Early cryotherapy can destroy the stratum corneum and have a widening effect to increase tumor vascular permeability, thereby facilitating the penetration of imiquimod cream8 which acts as a 7-receptor agonist and provides anti-tumor effects through modifying the immune response and stimulating apoptosis in BCC cells. The effectiveness of imiquimod on BCC after 6 weeks of administration varies by 70% to 94% but can be accompanied by side effects in the form of itching, burning, and pain in the application area.25 In 2011, MacFarlane et al conducted a retrospective study of 50 superficial BCC patients treated with cryoimmunotherapy. The patients underwent two cycles of cryotherapy with a 5-second freeze, and 5 mm margin, and continued applying imiquimod cream one week after cryotherapy for five nights consecutively with a break of two days for six weeks. The recurrence after cryoimmunotherapy was 2% in post-therapy monitoring for 46.4 months with minimal side effects. A total of 17 patients underwent post-therapy repeat biopsies with 14 patients showing scar tissue and 3 patients showing elastosis.8
In this case report, the patient underwent cryoimmunotherapy consisting of two cycles of cryotherapy (30-second freeze time and 5 mm margin) and one week later, bullae were observed on the edges of the lesion which had collapsed leaving hyperpigmented macules (Figure 4B). Two weeks post cryotherapy, 5% imiquimod cream was applied for five nights consecutively two days apart for six weeks with no side effects reported. The three-month follow-up showed, that the BCC lesion changed between on 1st day before the cryotherapy (Figure 4A) into a hyperpigmented macule and reduced in size to 2.5 cm in diameter (Figure 4C). This patient had a relatively good response and prognosis due to the absence of evidence of metastases and no risk factors for recurrence.
 |
Figure 4 Comparison of skin lesions on observation: (A) 1st day before cryoimmunotherapy. (B) Bullae observed on the edge of the lesion 2 weeks after cryotherapy. (C) Clinical improvement with reduced lesion size and hyperpigmented macule 3 months after cryoimmunotherapy. |
Conclusion
BCC is a relatively common skin tumor with multifactorial aetiology and in rare cases, SWD therapy may be a risk factor for developing superficial BCC lesions. The combination of cryotherapy followed with the application of 5% imiquimod cream is an effective BCC treatment to reduce tumor size, especially for the superficial type. Long-term monitoring after cryoimmunotherapy is important for the detection of recurrence.
Ethic Statement
The publications of images were included in the patient’s consent for publication of the case. The case report has been approved by the institutional ethics committee of Dr. Hasan Sadikin General Hospital, Bandung, Indonesia (Ethical Clearance No.: LB.02.01/X.6.5/178/2023).
Consent for Publication
The patients provided written informed consent for the use of case details and images for publication and scientific purposes. Institutional approval was obtained to publish the case details.
Acknowledgments
The authors would like to thank the staff of the Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
The authors declare that this study has received no financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ogueta I, Fuentes CS, Madison A, Sandoval M. Basal cell carcinoma at an unusual location: case report. J Dermatol Cosmetol. 2018;2(1):60–61. doi:10.15406/jdc.2018.02.00040
2. Tanese K. Diagnosis and management of basal cell carcinoma. Curr Treat Options Oncol. 2019;20:1–13.
3. Tan SK, Ghanznawie M, Heenan PJ, Dosan R. Basal cell carcinoma arises from interfollicular layer of epidermis. J Oncol. 2018;2018:1–5. doi:10.1155/2018/3098940
4. Tang JY, Epstein EH, Oro AE. Basal cell carcinoma and basal cell nevus syndrome. In: Kang S, Amagai M, Bruckner AL, et al., editors. Fitzpatrick’s Dermatology.
5. Kim DP, Kus KJB, Ruiz E. Basal cell carcinoma review. Hematol Oncol Clin N Am. 2019;33(1):13–24. doi:10.1016/j.hoc.2018.09.004
6. Clebak KT, Miller MM, Croad J. Cutaneous cryosurgery for common skin conditions. Am Fam Physician. 2020;101(7):399–406.
7. Krunic AL. Theoretical principle of immunocryosurgery. In: Pasquali P, editor. Cryosurgery a Practical Manual.
8. MacFarlane DF, Tal AKE. Cryoimmunotherapy: superficial basal cell cancer and squamous cell carcinoma in situ treated with liquid nitrogen followed by imiquimod. Arch Dermatol. 2011;147(11):1326–1327. doi:10.1001/archdermatol.2011.334
9. Zhang W, Zheng W, Jiang A, He Z, Shen X, Dong X. Global, regional and national incidence, mortality and disability-adjusted life-years of skin cancers and trend analysis from 1990 to 2019: an analysis of the global burden of disease study 2019. Cancer Med. 2021;10(14):4905–4922. doi:10.1002/cam4.4046
10. Wibawa LP, Andardewi MF, Krisanti IA, Arisanty R. The epidemiology of skin cancer at Dr. Cipto Mangunkusumo national central general hospital from 2014 to 2017. J Gen Proced Dermatol Venereol Indones. 2019;4(1):11–16. doi:10.19100/jdvi.v4i1.162
11. Mijuskovic ZP. Etiology and pathogenesis of basal cell carcinoma. Serbian J Dermatology Venereol. 2013;5(3):113–124. doi:10.2478/sjdv-2013-0009
12. Betti R, Inselvini E, Crosti C. Radiation and diathermic therapy as etiologic factors in basal cell carcinoma. J Eur Acad Dermatol Venerol. 1995;4:110–114. doi:10.1016/0926-9959(94)00066-9
13. Kikuchi M, Yano K, Kubo T, Hosokawa K, Yamaguchi Y, Itami S. Giant basal cell carcinoma affecting the lower abdominal, genital and bilateral inguinal region. Br J Plast Surg. 2002;55(5):445–448. doi:10.1054/bjps.2002.3869
14. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease association. J Am Acad Dermatol. 2019;16(60):303–318. doi:10.1016/j.jaad.2018.03.060
15. Dourmishev LA, Rusinova D, Botev I. Clinical variants, stages, and management of basal cell carcinoma. Indian Dermatol Online J. 2013;4(1):12–17. doi:10.4103/2229-5178.105456
16. Rito AW, Zalaudek I, Rudnicka L. Dermoscopy of basal cell carcinoma. Clin Exp Dermatol. 2018;43(3):241–247. doi:10.1111/ced.13387
17. Lallas A, Apalla Z, Loannides D, Argenziano G, Castagnetti F, Moscarella E. Dermoscopy in the diagnosis and management of basal cell carcinoma. Future Oncol. 2015;11(22):2975–2984. doi:10.2217/fon.15.193
18. Abdulkarim H, Ahmed R, Mohammed E, et al. Recurrent cutaneous basal cell carcinoma after surgical excision: a retrospective clinicopathological study. Ann Med Surg. 2022;78:1–5.
19. Akarsu S, Kamberoglu I. Cryotherapy for common premalignant and malignant skin disorder. In: Vereecken P, editor. Dermatologic Surgery and Procedures.
20. Rito AMW, Rudnicka L. Bowen’s disease in dermoscopy. Acta Dermatovenerol Croat. 2018;26(2):157–161.
21. Vijayasankar P, Karthikeyan K. Bowen’s disease. Indian Dermatol Online J. 2022;13(2):177–191. doi:10.4103/idoj.idoj_257_21
22. Scrutu LG, Petrica M, Grigore M, Avram A, Popescu I, Simionescu O. A conservative combined laser cryoimmunotherapy treatment vs. surgical excision for basal cell carcinoma. J Clin Med. 2022;11(12):1–13.
23. Gross K, Krixik L, Kricorian G. 5% 5-fluorouracil cream for the treatment of small superficial basal cell carcinoma: efficacy, tolerability, cosmetic outcome, and patient satisfaction. Dermatol Surg. 2007;33:433–439. doi:10.1111/j.1524-4725.2007.33090.x
24. Tchanque-Fussou CN, Eisen DB. A systematic review on the use of cryotherapy versus other treatment for basal cell carcinoma. Dermatol Online J. 2018;24(11):1–15.
25. Oldfield V, Keating GM, Perry CM. Imiquimod: in superficial basal cell carcinoma. Am J Clin Dermatol. 2005;6(3):195–200. doi:10.2165/00128071-200506030-00006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.