Back to Journals » Cancer Management and Research » Volume 17

Sunvozertinib Monotherapy in Advanced Lung Adenocarcinoma with EGFR Exon 20 Insertion and High PD-L1 Expression: A Case Report
Received 26 February 2025
Accepted for publication 31 August 2025
Published 18 September 2025 Volume 2025:17 Pages 2069—2076
DOI https://doi.org/10.2147/CMAR.S524920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Lu-Zhe Sun
Juan Zhou, Hui Han
Department of Oncology, Liaocheng People’s Hospital, Liaocheng City, Shandong Province, 252000, People’s Republic of China
Correspondence: Hui Han, Department of Oncology, Liaocheng People’s Hospital, No. 67, Dongchang West Road, Liaocheng City, Shandong Province, 252000, People’s Republic of China, Tel +86-13793058812, Email [email protected]
Abstract: As a key oncogenic driver in non–small-cell lung cancer (NSCLC), epidermal growth factor receptor (EGFR) exon 20 insertion mutations account for 2– 5% of EGFR‐mutated NSCLC cases and display marked heterogeneity. Conventional EGFR tyrosine kinase inhibitors (TKIs) are ineffective against these mutations. Sunvozertinib, an orally administered, potent, and highly selective EGFR-TKI, has been approved in China for second-line treatment of NSCLC harboring EGFR exon 20 insertion mutations. Historically, patients with EGFR exon 20 insertion and high programmed death-ligand 1 (PD-L1) expression often received combined immunotherapy and chemotherapy. In the present case report, we describe a patient who exhibited intolerance to first-line immunochemotherapy and was subsequently switched to sunvozertinib for maintenance therapy. This regimen yielded a prolonged progression-free survival, with manageable safety and tolerability profiles. These findings demonstrated that sunvozertinib could be a promising first-line treatment option for NSCLC patients with EGFR exon 20 insertion.
Keywords: EGFR exon 20 insertion, NSCLC, sunvozertinib, PD-L1
Introduction
Non-small cell lung cancer (NSCLC) is the most common histological type of lung cancer, accounting for approximately 85% of cases.1 The epidermal growth factor receptor (EGFR) mutation is one of the most prevalent driver mutations in NSCLC, with approximately 50% of non-squamous NSCLC patients harboring this mutation in Asia.2 It is acknowledged that in NSCLC, genetic mutations are associated with the efficacy of targeted therapies. EGFR tyrosine kinase inhibitors (EGFR-TKIs) show significant clinical benefit in EGFR exon 19 deletions (exon19-Del) and exon 21 L858R point mutations (exon21-L858R) and have already become the standard of care for these patients.3
The EGFR exon 20 insertion mutation, a distinct subtype of EGFR mutation, ranks as the third most common. Traditional EGFR-TKIs have shown limited efficacy in EGFR exon 20 insertion-positive NSCLC. Studies indicate that neither standard nor double-dose third-generation EGFR-TKIs provide significant clinical benefit for EGFR exon 20 insertion NSCLC patients.4 In China, there were no approved targeted therapies for EGFR exon 20 insertion NSCLC as a first-line treatment before 2025. According to the 2024 guidelines of the Chinese Society of Clinical Oncology (CSCO), such cases are treated as advanced or metastatic NSCLC without actionable driver mutations, and systemic chemotherapy is generally administered.5 According to data from the Flatiron Health database, as of May 2020, chemotherapy-based regimens are the most commonly used first-line treatments for such conditions.6 With the rise of immune checkpoint inhibitors, their combination with chemotherapy has become an option for patients with high programmed cell death ligand 1 (PD-L1) expression and EGFR exon 20 insertion mutations.7 Notably, approximately 24.1% of patients with EGFR exon 20 insertion NSCLC exhibit positive PD-L1 expression.8 EGFR exon 20 insertions may upregulate PD-L1 expression via downstream signaling pathways, such as the PI3K-AKT and MAPK pathways, contributing to an immunosuppressive tumor microenvironment.9 However, chemotherapy-based regimens show limited efficacy, and patients with EGFR exon 20 insertion mutations generally have worse prognosis than those with classic EGFR mutations,6 highlighting the need for more effective first-line treatments. In addition, compared with oral TKIs, intravenous chemotherapy-based regimens can lead to a higher incidence of adverse events (AEs), rendering some patients unable to tolerate treatment.10 Consequently, there remains a pressing need for improved therapeutic options for patients with EGFR exon 20 insertion mutation.
Sunvozertinib is an oral, irreversible, and selective EGFR-TKI targeting the EGFR exon 20 insertion as well as EGFR-sensitizing, T790M, and uncommon mutations with weak activity against wild-type EGFR.11 In August 2023, it received its first approval from the China’s National Medical Products Administration for second or later-line treatment in patients with locally advanced or metastatic NSCLC harboring EGFR exon 20 insertion mutations.12 In this study, we present a case with advanced pulmonary adenocarcinoma harboring EGFR exon 20 insertion mutation and high PD-L1 expression, who experienced intolerance to immune checkpoint inhibitors and chemotherapy. The patient was subsequently switched to sunvozertinib, resulting in prolonged progression-free survival (PFS). This case underscores the potential of sunvozertinib as first-line treatment for EGFR exon 20 insertion NSCLC and provides valuable insights for clinical practice.
Case Presentation
In February 2022, a 67-year-old male presented to our hospital with a complaint of cough lasting more than a month. Chest computed tomography (CT) (Figure 1) revealed the following: 1) a soft tissue mass in the left hilum and upper lobe of the left lung with mild enhancement (7.4 × 4.3 cm; Table 1); 2) enlarged lymph nodes in both lung hila and the mediastinum, the largest measuring 1.9 × 1.3 cm and exhibiting central low-density necrosis; 3) multiple nodules of varying sizes and scattered high-density spots throughout both lungs; and 4) evidence of multiple bone lesions affecting the bilateral ribs and thoracic spine. The patient had an Eastern Cooperative Oncology Group performance status of 1 and denied any smoking history or significant past medical history.
 |
Table 1 Longitudinal Changes in Serum Tumor Markers, Tumor Response, and Treatment Phases |
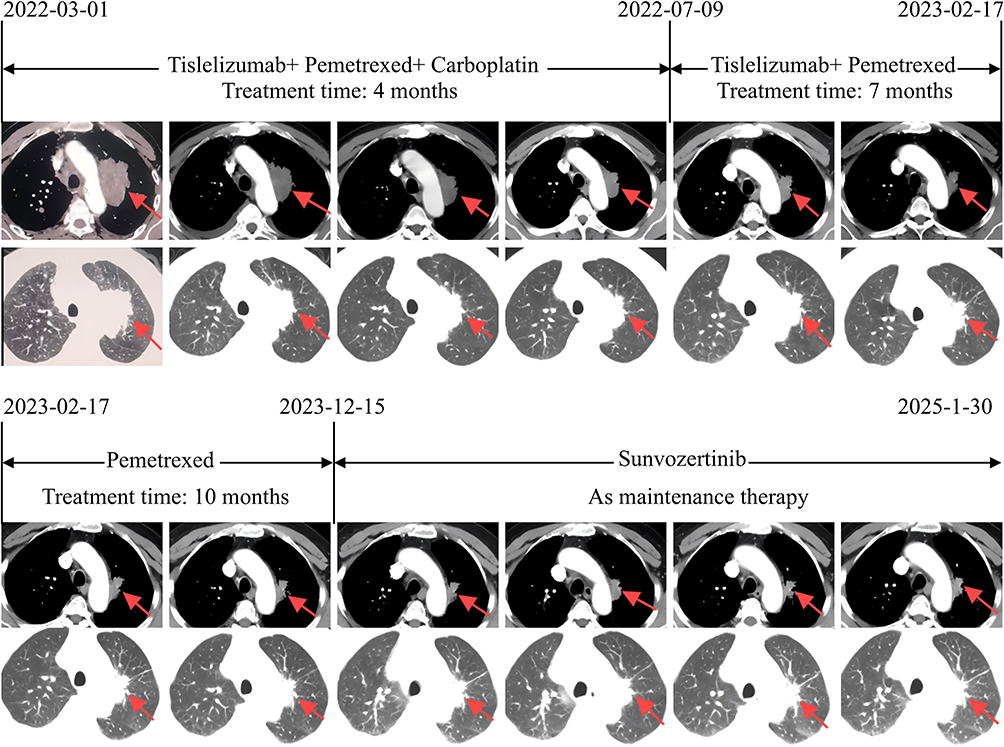 |
Figure 1 Tumor progression during treatment course revealed by consecutive Chest CT images (lesion in left upper lobe, red arrows). |
A biopsy of a left cervical lymph node was subsequently performed, and pathological examination confirmed the presence of adenocarcinoma originating from the lung. Tumor purity was assessed by a pathologist and confirmed to be above 30%, ensuring the adequacy of the sample for molecular profiling. Next-generation sequencing was carried out by Anhui Anlong Gene Technology Co., Ltd., revealing an EGFR exon 20 insertion (c.2315_2316ins3; p.P772delinsPH) with a mutation abundance of 22.4%. Immunohistochemical analysis further demonstrated strong PD-L1 expression (22C3 assay), with a tumor proportion score of 80% and a combined positive score of 80 (Figure 2). Based on imaging findings, including contrast-enhanced brain magnetic resonance imaging (MRI), superficial lymph node ultrasound, bone scintigraphy (ECT), and contrast-enhanced abdominal CT, the patient was staged as cT4N3M1c, corresponding to stage IVB according to the AJCC TNM staging system (8th edition). Brain MRI revealed no evidence of intracranial metastasis. Ultrasound identified multiple hypoechoic lesions in bilateral cervical and supraclavicular lymph nodes, indicative of nodal metastases. Bone scintigraphy demonstrated multiple irregular foci of increased radiotracer uptake in the skull, ribs, spine, and right scapula, consistent with extensive osseous metastases. Contrast-enhanced abdominal CT showed no hepatic or adrenal involvement. Positron emission tomography (PET)/CT was not performed due to financial constraints.
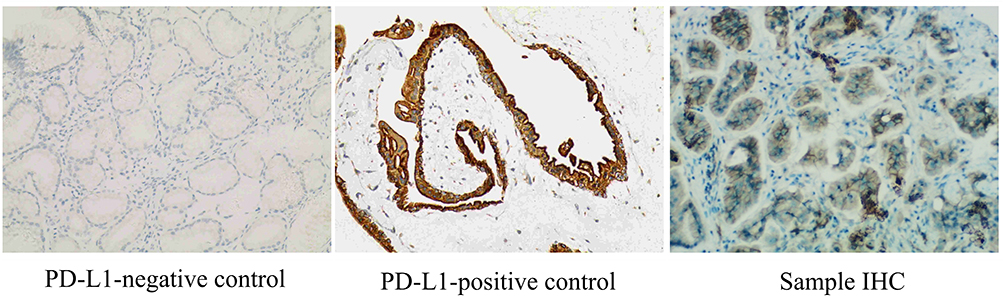 |
Figure 2 The expression level of PD-L1. Tumor proportion score (TPS) = PD-L1-positive tumor cell count / total viable tumor cell count × 100%; combined positive score (CPS) = PD-L1-positive cell count (tumor cells, lymphocytes, macrophages) / total viable tumor cell count × 100%. The scoring was performed simultaneously by two experienced pathologists, and any discrepancies were resolved by consensus. |
Treatment Course
On March 1, 2022, the patient began treatment with tislelizumab (200 mg on day 1, every 3 weeks), pemetrexed (500 mg/m² on day 1, every 3 weeks), and carboplatin (AUC = 5 on day 1, every 3 weeks), administered over six cycles. During the next 4 months, the tumor demonstrated continuous shrinkage, with the largest diameter decreasing from 7.4 cm to 4.9 cm. During this period, the patient experienced leukopenia (grade 1) according to CTCAE v5.0, which was managed with pegylated recombinant human granulocyte colony-stimulating factor (Qilu Pharmaceutical, Jinan, China).
On July 9, 2022, treatment was modified to maintenance therapy consisting of tislelizumab and pemetrexed for an additional 7 months. Tumor size continued to decrease, with the largest diameter reducing from 4.9 cm to 4.1 cm. However, the patient experienced leukopenia (grade 1), fatigue (grade 1), and diarrhea (grade 1) during this phase. These AEs were monitored periodically and managed symptomatically.
On February 17, 2023, due to persistent fatigue and diarrhea, tislelizumab was discontinued, and the patient transitioned to pemetrexed monotherapy for a duration of 10 months. Following this change, the fatigue and diarrhea resolved. However, the tumor size gradually increased from 4.1 cm to 4.4 cm. The disease remained stable and grade 1 leukopenia was observed.
In December 2023, the patient developed phlebitis (grade 1), resulting in difficulties with intravenous access. As a result, pemetrexed was discontinued. On December 15, 2023, treatment was switched to sunvozertinib at a daily oral dose of 300 mg. Following the change, the tumor continued to shrink from 4.4 cm to 3.8 cm. At the time of submission of this report, sunvozertinib has been administered for 13 months, with no evidence of disease progression. During this period, the patient has experienced grade 1 diarrhea and grade 1 paronychia, both of which improved with symptomatic management.
To date, the patient’s treatment has changed from immunotherapy combined with chemotherapy to maintenance with sunvozertinib, and the overall PFS has reached 34 months.
Discussion
NSCLC with EGFR exon 20 insertion predominantly affects never-smokers, females, individuals with adenocarcinoma, and those of Asian descent, with a notably younger age of onset. Recent advances in exploring new diagnostic and therapeutic strategies have informed the understanding and management of EGFR exon 20 insertion NSCLC.13–25 In terms of metastasis, the most common sites are the bone, brain, and liver.7 It was reported that approximately 39% of patients present with brain metastases at the time of diagnosis.26 Furthermore, patients with EGFR exon 20 insertion mutations generally have a poorer prognosis, with a PFS less than half of that of cases carrying classic EGFR mutations.6 Due to the unique structure, diverse subtypes, high malignancy, and substantial heterogeneity of these mutations, traditional treatments such as chemotherapy, immunotherapy, and first to third-generation EGFR-TKIs have shown limited efficacy for EGFR exon 20 insertion NSCLC.27,28 In this case, the patient exhibited sustained tumor shrinkage and a prolonged PFS of 34 months, highlighting the potential of sunvozertinib as a promising treatment option for EGFR exon 20 insertion-positive NSCLC.
Although patients with EGFR mutations typically exhibit reduced PD-L1 expression, a subset of patients with EGFR mutations show elevated PD-L1 expression.8 The optimal treatment approach for such cases remains a topic of ongoing debate. In relevant studies to date, data from the CHRYSALIS study (NCT02609776)29 demonstrated an objective response rate (ORR) of 40% for amivantamab as a later-line treatment, while the EXCLAIM study (NCT02716116)30 reported an ORR of 28% for mobocertinib in the post-line setting. Amivantamab and mobocertinib have been approved by the FDA for the treatment of EGFR exon 20 insertion mutations in NSCLC but were not available in China at the time the patient was admitted (March 2022), which necessitated the selection of alternative treatment options. According to the ASCO guidelines, for patients with EGFR exon 20 insertion mutations, clinicians may offer chemotherapy in conjunction with amivantamab as first-line therapy. In cases where amivantamab is unavailable, standard treatments aligned with non-driver alteration protocols should be considered.31 Considering the high expression of PD-L1 in this patient, treatment decisions were informed by the results of several immunotherapy studies, including: 1) KEYNOTE-024 (NCT02142738):32 Pembrolizumab monotherapy in patients with PD-L1 expression ≥50% yielded a median PFS of 10.3 months (95% confidence interval [CI], 6.7 months to not reached), significantly longer than the 6.0 months (95% CI, 4.2 to 6.2 months) achieved with chemotherapy alone (hazard ratio [HR]=0.50; 95% CI, 0.37 to 0.68 months; p<0.001); 2) KEYNOTE-189 (NCT02578680):33 Pembrolizumab in combination with chemotherapy resulted in a median PFS of 8.8 months (95% CI, 7.6 to 9.2 months) compared to 4.9 months (95% CI, 4.7 to 5.5 months) for chemotherapy alone (HR=0.52; 95% CI, 0.43 to 0.64 months; p<0.001); and 3) RATIONALE-304 (NCT03663205):34 The combination of tislelizumab and chemotherapy achieved a median PFS of 9.7 months versus 7.6 months with chemotherapy alone (HR=0.645; p=0.004). Notably, among patients with PD-L1 expression ≥50%, the HR was 0.308, indicating a markedly enhanced benefit within this subgroup. Based on the patient’s high PD-L1 expression and in accordance with available Chinese guidelines, the patient was treated according to the protocol for driver gene-negative NSCLC, using tislelizumab in combination with platinum-based chemotherapy. Subsequently, the patient was switched to tislelizumab plus single-agent chemotherapy or single-agent maintenance chemotherapy, continuing without disease progression. However, by December 2023, prolonged use of tislelizumab and pemetrexed led to AEs—such as fatigue, diarrhea, and phlebitis—prompting the patient to discontinue intravenous therapies. In this context, there was an urgent need for a drug with both efficacy and safety to maintain the benefits of treatment.
In the PAPILLON Phase III trial (NCT04538664),35 amivantamab plus chemotherapy (carboplatin-pemetrexed) for advanced EGFR exon 20 insertion NSCLC demonstrated a median PFS of 11.4 months, compared with 6.7 months for chemotherapy alone (HR=0.40; 95% CI, 0.30–0.53; p<0.001). The ORR was 73% in the combination group compared to 47% with chemotherapy, highlighting a significant improvement in disease control. However, amivantamab was still unavailable in China at that time. In the EXCLAIM-2 phase III study (NCT04129502),36 mobocertinib monotherapy did not demonstrate superiority over chemotherapy in the first-line setting for EGFR exon 20 insertion NSCLC (median PFS of 9.6 months in both groups; HR=1.04; 95% CI, 0.77–1.39; p=0.803), leading to its withdrawal from the global market. In contrast, the WU-KONG6 study (NCT05712902)37 demonstrated that sunvozertinib monotherapy achieved an ORR of 61% and a median PFS of 6.5 months in previously treated NSCLC patients with advanced EGFR exon 20 insertion. The most common grade 3 or higher treatment-related AEs were elevated blood creatine phosphokinase (18 [17%] of 104 cases), diarrhea (8 cases [8%]), and anemia (6 cases [6%]). The most frequent serious treatment-related AEs included interstitial lung disease (5 cases [5%]), anemia (3 cases [3%]), vomiting (2 cases [2%]), nausea (2 cases [2%]), and pneumonia (2 cases [2%]).37 Based on these results, sunvozertinib was approved in China in August 2023, becoming the only targeted therapy for EGFR exon 20 insertion available in China at that time. Moreover, pooled data from the WU-KONG1/15 studies (NCT03974022; NCT05559645)38 showed promising efficacy of sunvozertinib in first-line setting of advanced EGFR exon 20 insertion NSCLC, with a confirmed ORR of 78.6% and a median PFS of 12.4 months. The safety profile was consistent with previous findings, with the most common treatment-emergent AEs being diarrhea, elevated creatine phosphokinase, and skin rash.38 Recently, CLN-081 (zipalertinib, NCT04036682) also showed encouraging activity, achieving a 41% partial response rate at 100 mg twice daily in heavily pretreated EGFR exon 20 insertion NSCLC patients, with a favorable safety profile.39 These studies demonstrated a promising efficacy and manageable safety profile, prompting us to use sunvozertinib as a maintenance therapy for our patient. As of the submission date for this report, sunvozertinib has been used for 13 months in the presented case, and the patient’s tumor has shown continued shrinkage and durable disease control, with no signs of progression.
The latest Chinese Expert Consensus recommends sunvozertinib as a preferred second-line therapy for advanced or metastatic EGFR exon 20 insertion NSCLC.40 However, no standardized first-line therapy is yet available in China. In patients who cannot tolerate or refuse chemotherapy and have a compromised performance status, sunvozertinib may be considered as a first-line treatment. In the present case, AEs from long-term use of immunotherapy and chemotherapy led to intolerance, prompting the discontinuation of these treatments. Sunvozertinib was subsequently used as a maintenance therapy, enabling the patient to maintain disease control. Compared with the PAPILLON trial, where the median PFS for the amivantamab plus chemotherapy arm was 11.4 months,35 our patient achieved an even longer PFS, highlighting the potential of sunvozertinib in the first-line management of advanced EGFR exon 20 insertion NSCLC.
For patients with concurrent EGFR mutations and high PD-L1 expression, the clinical benefit of combining immunotherapy with targeted therapy remains unclear, with concerns over increased immune-related AEs. The literature suggests that the combination of immunotherapy and targeted therapy can lead to an overall AE rate of up to 94.5%, with grade ≥3 events in 47.3% of cases.41 Notably, the incidence of interstitial lung disease is elevated, potentially due to the timing and sequence of drug administration. Several clinical trials—the CheckMate-012, KEYNOTE-021, and TATTON studies—failed to show clear survival benefits from combining or sequencing EGFR-TKIs with PD-1/PD-L1 inhibitors in advanced EGFR-mutant NSCLC, and instead reported high toxicity rates. In the TATTON trial, the incidence of interstitial lung disease reached 38% with osimertinib plus durvalumab, leading to early termination of enrollment and the premature closure of the Phase III CAURAL trial (NCT02143466; NCT02454933).42,43 In contrast, in our case, the patient initially benefited from immunotherapy combined with chemotherapy, but treatment was halted due to AEs. Ten months after tislelizumab treatment discontinuation, sunvozertinib was introduced, and during the period of treatment with sunvozertinib, only grade 1 diarrhea and paronychia were observed. These AEs are consistent with the known safety profile of sunvozertinib, with no severe toxicities such as interstitial lung disease. This suggests that a sufficient period between discontinuing immunotherapy and starting targeted therapy may mitigate the risk of severe toxicity. Hence, switching to sunvozertinib after a suitable washout period appears feasible and can yield sustained clinical benefits.
A notable limitation of this case report is the absence of serial assessments of PD-L1 expression and EGFR exon 20 insertion variant allele frequencies across treatment stages. Such analyses would provide valuable insights into clonal evolution and biomarker dynamics in response to different therapies. Unfortunately, repeated tumor or liquid biopsies were not feasible in this case due to the patient’s declining performance status and clinical considerations. Additionally, no formal pharmacokinetic or pharmacodynamic considerations informed the 10-month washout period between tislelizumab discontinuation and sunvozertinib initiation, as no established guidelines currently exist for sequencing immunotherapy and EGFR-TKIs in EGFR-mutant NSCLC. Moreover, the unusually prolonged PFS observed in this patient may be influenced by the cumulative benefit of sequential therapies, rather than sunvozertinib monotherapy alone, limiting direct comparison with historical controls. Furthermore, post-progression biopsies or liquid biopsies were not performed due to the absence of progression during treatment with sunvozertinib. Notably, the risk of acquired resistance to sunvozertinib remains an important limitation to consider for long-term treatment, as mechanisms of resistance in EGFR exon 20 insertion NSCLC such as secondary EGFR mutations (eg, C797S) or bypass signaling pathways are still being elucidated. Furthermore, no analyses of tumor microenvironment features (eg, T-cell infiltration) or genomic correlates (eg, STK11/KEAP1 mutations) were performed to explain the high PD-L1 expression in this case, due to limited tissue availability. Future prospective studies with comprehensive biomarker monitoring, including post-progression molecular profiling and exploration of tumor microenvironment factors, are warranted to better understand these dynamics in EGFR exon 20 insertion-positive NSCLC.
Conclusions
To the best of our knowledge, this is the first report of an EGFR exon 20 insertion NSCLC patient with high PD-L1 expression who achieved durable disease control using sunvozertinib as a maintenance therapy after intolerance to immunochemotherapy. Remarkably, the patient maintained a prolonged PFS of nearly 3 years with manageable adverse effects. This outcome underscores the potential role of sunvozertinib as a promising first-line option for this challenging patient population and highlights the need for further investigation in prospective clinical trials (eg, WU-KONG28 [NCT05668988]).
Consent for Publication
The authors obtained informed consent from the patient for publication of the case details and any accompanying images. Institutional policy for approval by ethical committee was not required.
Acknowledgment
We thank Medjaden, Inc. for scientific editing of this paper.
Funding
No funding was used in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Melosky B, Kambartel K, Häntschel M, et al. Worldwide Prevalence of Epidermal Growth Factor Receptor Mutations in Non-Small Cell Lung Cancer: a Meta-Analysis. Mol Diagn Ther. 2022;26(1):7–18. doi:10.1007/s40291-021-00563-1
3. Zhou F, Guo H, Xia Y, et al. The changing treatment landscape of EGFR-mutant non-small-cell lung cancer. Nat Rev Clin Oncol. 2025;22(2):95–116. doi:10.1038/s41571-024-00971-2
4. Kwon CS, Lin HM, Crossland V, et al. Non-small cell lung cancer with EGFR exon 20 insertion mutation: a systematic literature review and meta-analysis of patient outcomes. Curr Med Res Opin. 2022;38(8):1341–1350. doi:10.1080/03007995.2022.2083326
5. Committee of Chinese Society of Clinical Oncology. CSCO Guideline of Non-Small Cell Lung Cancer 2024.
6. Bazhenova L, Minchom A, Viteri S, et al. Comparative clinical outcomes for patients with advanced NSCLC harboring EGFR exon 20 insertion mutations and common EGFR mutations. Lung Cancer. 2021;162:154–161. doi:10.1016/j.lungcan.2021.10.020
7. Pan B, Liang J, Shi H, Rao K, Guo W, Zhan C. Epidemiological characteristics and therapeutic advances of EGFR exon 20 insertion mutations in non-small cell lung cancer. Thorac Cancer. 2023;14(33):3247–3258. doi:10.1111/1759-7714.15127
8. Geng D, Guo Q, Huang S, Zhang H, Guo S, Li X. Clinical and molecular characteristics of epidermal growth factor receptor exon 20 insertion mutations in non-small-cell lung cancer. Clin Transl Oncol. 2022;24(2):379–387. doi:10.1007/s12094-021-02701-x
9. Lim JU, Jung J, Kim YW, et al. Targeting the Tumor Microenvironment in EGFR-Mutant Lung Cancer: opportunities and Challenges. Biomedicines. 2025;13(2):470. doi:10.3390/biomedicines13020470
10. Zhou S, Kishi N, Alerasool P, Rohs NC. Adverse Event Profile of Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors for Non-small Cell Lung Cancer: an Updated Meta-analysis. Target Oncol. 2024;19(4):547–564. doi:10.1007/s11523-024-01073-w
11. Wang M, Yang JC, Mitchell PL, et al. Sunvozertinib, a Selective EGFR Inhibitor for Previously Treated Non-Small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations. Cancer Discov. 2022;12(7):1676–1689. doi:10.1158/2159-8290.CD-21-1615
12. Yuan C, Yu JY, Zeng CX, et al. New advances in the treatment of EGFR exon20ins mutant advanced NSCLC. Am J Cancer Res. 2025;15(4):1852–1873. doi:10.62347/WTMU5537
13. Xu Y, Zeng Y, Xiao X, et al. Targeted Imaging of Tumor Associated Macrophages in Breast Cancer. Bio Integration. 2023;4(3):114. doi:10.15212/bioi-2022-0010
14. Xu H, Guo Z, Li M, et al. Copper-Based Nanomaterials for Image-Guided Cancer Therapy. BIO Integration. 2024;5(1):976. doi:10.15212/bioi-2024-0013
15. Guo Z, Saw PE, Jon S. Non-Invasive Physical Stimulation to Modulate the Tumor Microenvironment: unveiling a New Frontier in Cancer Therapy. BIO Integration. 2024;5(1):986. doi:10.15212/bioi-2024-0012
16. Mokashi A, Bhatia NM. Integrated Network Ethnopharmacology, Molecular Docking, and ADMET Analysis Strategy for Exploring the Anti-Breast Cancer Activity of Ayurvedic Botanicals Targeting the Progesterone Receptor. BIO Integration. 2024;5(1):970. doi:10.15212/bioi-2024-0066
17. Ji X, Tian X, Feng S, et al. Intermittent F-actin perturbations by magnetic fields inhibit breast cancer metastasis. Research. 2023;6:0080. doi:10.34133/research.0080
18. Tang J, He J, Guo H, et al. PTBP2-mediated alternative splicing of IRF9 controls tumor-associated monocyte/macrophage chemotaxis and repolarization in neuroblastoma progression. Research. 2023;6:0033. doi:10.34133/research.0033
19. X-f G, S-s G, Wang J, et al. Protective effect of mesenchymal stem cell-derived exosomal treatment of hippocampal neurons against oxygen-glucose deprivation/reperfusion-induced injury. World J Emerg Med. 2022;13(1):46. doi:10.5847/wjem.j.1920-8642.2022.015
20. Luo Z, Mei J, Wang X, et al. Voluntary exercise sensitizes cancer immunotherapy via the collagen inhibition-orchestrated inflammatory tumor immune microenvironment. Cell Rep. 2024;43(9):114697. doi:10.1016/j.celrep.2024.114697
21. Liao K, Gong L, Yang Y, et al. A comprehensive review of research progress in Chinese medicines for primary liver cancer treatment. Tradit Med Res. 2022;7(2):10. doi:10.53388/TMR20220207263
22. Zhang H, Lv G, Liu S, Liu D, Wu X. The artificial intelligence watcher predicts cancer risk by facial features. Tradit Med Res. 2022;7(1):
23. Xu S, Lu Z. Exploring FNDC4 as a biomarker for prognosis and immunotherapy response in lung adenocarcinoma. Asian J Surg. 2024;2024:1.
24. Liu X, Xi X, Xu S, et al. Targeting T cell exhaustion: emerging strategies in non-small cell lung cancer. Front Immunol. 2024;15:1507501. doi:10.3389/fimmu.2024.1507501
25. Lu Z, Xu S, Ye M, et al. Comparison of pembrolizumab plus chemotherapy versus concurrent or sequential radiochemotherapy in patients with driver mutation-lacking lung adenocarcinoma presenting with recurrent laryngeal nerve invasion leading to hoarseness. Am Soc Clin Oncol. 2024;2024:1.
26. Cardona AF, Rojas L, Zatarain-Barrón ZL, et al. EGFR exon 20 insertion in lung adenocarcinomas among Hispanics (geno1.2-CLICaP). Lung Cancer. 2018;125:265–272. doi:10.1016/j.lungcan.2018.10.007
27. Meador CB, Sequist LV, Piotrowska Z. Targeting EGFR Exon 20 Insertions in Non-Small Cell Lung Cancer: recent Advances and Clinical Updates. Cancer Discov. 2021;11(9):2145–2157. doi:10.1158/2159-8290.CD-21-0226
28. Dorta-Suárez M, de Miguel M, Amor-Carro O, Calderón JM, González-Ortega M, Rodríguez-Abreu D. The state of the art of EGFR exon 20 insertions in non-small cell lung cancer: diagnosis and future perspectives. Cancer Treat Rev. 2024;124:102671. doi:10.1016/j.ctrv.2023.102671
29. Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer Progressing on Platinum Chemotherapy: initial Results From the CHRYSALIS Phase I Study. J Clin Oncol. 2021;39(30):3391–3402. doi:10.1200/JCO.21.00662
30. Zhou C, Ramalingam SS, Kim TM, et al. Treatment Outcomes and Safety of Mobocertinib in Platinum-Pretreated Patients With EGFR Exon 20 Insertion-Positive Metastatic Non-Small Cell Lung Cancer: a Phase 1/2 Open-label Nonrandomized Clinical Trial. JAMA Oncol. 2021;7(12):e214761. doi:10.1001/jamaoncol.2021.4761
31. Owen DH, Ismaila N, Ahluwalia A, et al. Therapy for Stage IV Non-Small Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2024.3. J Clin Oncol. 2025;43(10):e2–e16. doi:10.1200/JCO-24-02785
32. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
33. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
34. Lu S, Wang J, Yu Y, et al. Tislelizumab Plus Chemotherapy as First-Line Treatment for Locally Advanced or Metastatic Nonsquamous NSCLC (RATIONALE 304): a Randomized Phase 3 Trial. J Thorac Oncol. 2021;16(9):1512–1522. doi:10.1016/j.jtho.2021.05.005
35. Zhou C, Tang KJ, Cho BC, et al. Amivantamab plus Chemotherapy in NSCLC with EGFR Exon 20 Insertions. N Engl J Med. 2023;389(22):2039–2051. doi:10.1056/NEJMoa2306441
36. Jänne PA, Wang B-C, Cho BC, et al. First-Line Mobocertinib Versus Platinum-Based Chemotherapy in Patients With EGFR Exon 20 Insertion-Positive Metastatic Non-Small Cell Lung Cancer in the Phase III EXCLAIM-2 Trial. J Clin Oncol. 2025;2025:JCO2401269.
37. Wang M, Fan Y, Sun M, et al. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, Phase 2 trial. Lancet Respir Med. 2024;12(3):217–224. doi:10.1016/S2213-2600(23)00379-X
38. Yang JC, Wang M, Chiu C-H. Sunvozertinib as first-line treatment in NSCLC patients with EGFR Exon20 insertion mutations. Ann Oncol. 2023;34:S765. doi:10.1016/j.annonc.2023.09.2358
39. Piotrowska Z, Tan DS, Smit EF, et al. Safety, Tolerability, and Antitumor Activity of Zipalertinib Among Patients With Non-Small-Cell Lung Cancer Harboring Epidermal Growth Factor Receptor Exon 20 Insertions. J Clin Oncol. 2023;41(26):4218–4225. doi:10.1200/JCO.23.00152
40. Chinese Society of Clinical Oncology Non-small Cell Lung Cancer Committee. Chinese Expert Consensus on the Standardized Diagnosis and Treatment of Non‑small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations (2024 Edition). Zhongguo Fei Ai Za Zhi. 2024;27(7):485–494. doi:10.3779/j.issn.1009-3419.2024.102.27
41. Zhou X, Yao Z, Bai H, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitor-based combination therapies in clinical trials: a systematic review and meta-analysis. Lancet Oncol. 2021;22(9):1265–1274. doi:10.1016/S1470-2045(21)00333-8
42. Oxnard GR, Yang JC, Yu H, et al. TATTON: a multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann Oncol. 2020;31(4):507–516. doi:10.1016/j.annonc.2020.01.013
43. Yang JC, Shepherd FA, Kim DW, et al. Osimertinib Plus Durvalumab versus Osimertinib Monotherapy in EGFR T790M-Positive NSCLC following Previous EGFR TKI Therapy: CAURAL Brief Report. J Thorac Oncol. 2019;14(5):933–939. doi:10.1016/j.jtho.2019.02.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.