Back to Journals » Lung Cancer: Targets and Therapy » Volume 17
Sunvozertinib in EGFR Exon 20 Insertion NSCLC: Approved but Not Available – Practical Dose Selection Considerations and Real-World Access Challenges
Authors Aldecoa KAT, Arter ZL ![]() , Ou SHI, Nagasaka M
, Ou SHI, Nagasaka M ![]()
Received 1 January 2026
Accepted for publication 18 May 2026
Published 28 May 2026 Volume 2026:17 592922
DOI https://doi.org/10.2147/LCTT.S592922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fengying Wu
Kim Abbegail Tan Aldecoa,1,2 Zhaohui Liao Arter,1,2 Sai-Hong Ignatius Ou,1,2 Misako Nagasaka1,2
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA
Correspondence: Misako Nagasaka, Department of Medicine, University of California Irvine School of Medicine, 101 The City Drive, Orange, CA, 92868, USA, Email [email protected]
Abstract: Sunvozertinib has emerged as one of the most promising tyrosine kinase inhibitors (TKIs) for previously treated non-small cell lung cancer (NSCLC) harboring epidermal growth factor receptor (EGFR) exon 20 insertion (exon20ins) mutations, a molecular subset with limited sensitivity to conventional EGFR TKIs and a persistent unmet need especially in the second-line setting. Regulatory approvals have occurred at different doses – 300 mg daily in China based on WU-KONG6 and 200mg daily in the United States based on WU-KONG1B – raising an important question regarding optimal dose selection in clinical practice. In this editorial, we outline the preclinical and clinical evidence supporting sunvozertinib’s approval, compare the efficacy and tolerability at 200mg versus 300mg, and discuss other emerging TKIs in this evolving treatment landscape. Finally, we highlight a critical paradox: despite FDA approval, sunvozertinib remains largely inaccessible to patients in the United States.
Keywords: sunvozertinib, TKI, NSCLC, exon20insertion, exon20ins, access challenges, WUKONG
Introduction
Epidermal growth factor receptor (EGFR) mutations are among the most clinically actionable drivers in non–small cell lung cancer (NSCLC), second to KRAS in prevalence.1 Classical EGFR sensitizing mutations, namely exon 19 deletions and L858R point mutations, are highly responsive to EGFR tyrosine kinase inhibitors (TKIs).2,3 In contrast, exon 20 insertions (exon20ins), which account for roughly 2% of NSCLC and 12% of EGFR mutations,1 have limited sensitivity to conventional TKIs and are associated with inferior clinical outcomes.4 Resistance stems from the unique spatial configuration of exon20ins mutations, including a modified kinase domain structure, a sterically hindered ATP-binding pocket, and considerable heterogeneity (>60 subtypes) of exon20ins.5
Therapeutic progress has been modest. Amivantamab, an EGFR and mesenchymal–epithelial transition factor (MET) bispecific antibody, is now approved as first line in combination with platinum-based chemotherapy for EGFR exon20ins NSCLC, with an overall response rate (ORR) of 73%,6 while ORR is 40% with amivantamab monotherapy in the second-line setting.7 However, its use is limited by significant skin toxicities6 and treatment options remain limited in the second-line setting. Sunvozertinib was purposely developed to address this gap. An earlier effort with the EGFR TKI mobocertinib, which received accelerated approval for platinum-pretreated NSCLC with EGFR exon20ins, was later withdrawn after EXCLAIM-2 trial failed to demonstrate superior PFS compared to chemotherapy.8
Sunvozertinib is a selective EGFR TKI that preferentially bind to different EGFR exon20ins (along with EGFR classical, T790M, and uncommon mutations) over wild-type inhibition. Its clinical trial program was named “WUKONG”, which may be viewed as symbolizing agility and innovation from the mythical monkey with supernatural powers, perhaps reflecting the developers’ ambition for sunvozertinib in this molecular subset. Sunvozertinib was first approved in China in 2023 (based on WU-KONG6 study) at a 300mg daily dose. It recently gained accelerated approval in the United States in July 2025 (based on WUKONG 1B study) at a 200mg daily dose for platinum pre-treated patients with locally advanced or metastatic NSCLC with exon20ins mutations. As sunvozertinib advances into the global Phase III evaluation in the first-line setting (WUKONG-28), the difference in approved dosing – 200mg in the United States and 300mg in China – makes it important to carefully examine the efficacy and safety profiles of both regimens to help define the most appropriate clinical use. Moreover, because sunvozertinib remains of limited real-world availability in the United States, discussion of other emerging TKIs in this setting is also relevant.
Sunvozertinib Pre-Clinical Data
Sunvozertinib (developmental code DZD9008, marketed as Zegrovy) was developed by Dizal Pharmaceutical.9 The compound was rationally designed from the osimertinib scaffold (Figure 1). Similar to osimertinib, it preserves its irreversible covalent interaction with the cysteine-797 residue of EGFR to retain potency against classical sensitizing EGFR mutations. Its structure differs by replacing the rigid methylindole group in osimertinib with a more flexible anilinophenyl group. This modification enables binding within the sterically restricted ATP-binding pocket unique to exon20ins mutations.10
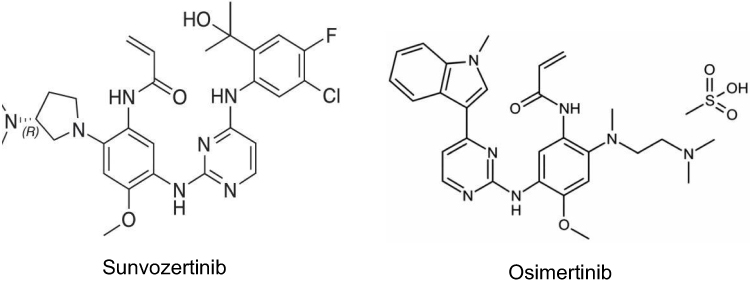 |
Figure 1 Structural comparison of sunvozertinib and osimertinib. Sunvozertinib, derived from the osimertinib scaffold, retains covalent binding to epidermal growth factor receptor (EGFR) cysteine-797 (Cys797) while incorporating a more flexible anilinophenyl group in place of the less flexible methylindole moiety of osimertinib, thereby facilitating accommodation within the sterically constrained ATP-binding pocket of exon 20 insertion mutations. |
Compared with osimertinib and other TKIs, sunvozertinib demonstrates 1.4 to 9.6 fold greater selectivity for ex20ins mutants than for wild-type EGFR.10 This higher selectivity improves the therapeutic index and reduces the frequency of toxicities (such as rash and diarrhea) that are common with earlier generation ex20ins TKIs. Preclinical studies also confirm CNS penetration and intracranial tumor activity in xenograft models. However, the drug should be avoided during pregnancy due to preclinical studies that have shown maternal toxicity and teratogenic effects.9–11
Pharmacodynamic Data
Data from the prescribing information reports that increasing sunvozertinib from 200mg (the approved dose) to 300 mg (1.5 times the approved dose) showed no clinically significant improvement in exposure–response relationships for ORR. No clinically significant QTc interval prolongations were observed at 300mg compared to 200mg.
Pharmacokinetic Data
Sunvozertinib reaches peak plasma concentration (Tmax) approximately 6 hours after oral administration. The drug can be taken with or without food. Sunvozertinib is a CYP3A4 substrate and concomitant use with strong or moderate CYP3A4 inducers or inhibitors should be avoided as they may decrease or increase systemic exposure, respectively. No clinically significant pharmacokinetic differences were observed in specific populations based on age (19–96 years), sex, race, body weight (30 to 118 kg), mild-to-moderate renal impairment (creatinine clearance 30–89mL/min), or mild-to-moderate hepatic impairment (bilirubin ≤upper limit of normal with AST≥ upper limit of normal or bilirubin >1-3x ULN with any AST).9
Clinical Studies
The clinical development program for sunvozertinib is named “WU-KONG”.
WU-KONG 1 (Phase 1/2, Global)
WU-KONG1 was initiated in 2019 as the first-in-human, open-label, multinational Phase I study of sunvozertinib as a second-line treatment in patients with EGFR exon20 insertion mutations. It was conducted globally across 17 centers in the United States, Australia, Taiwan, and Korea. The trial included two components: Part A (dose-escalation) and Part B (dose-expansion). A parallel phase I study, WU-KONG2, was conducted at 8 centers in China with a similar design. In the dose-escalation cohorts (Part A), patients received once-daily oral sunvozertinib at doses ranging from 50 mg to 400 mg. The drug was generally tolerated up to 400 mg, with dose-limiting toxicities observed at higher exposures, including grade 3 diarrhea at 300 mg and grade 3 cardiac arrhythmia at 400 mg.10 In the expansion cohorts (Part B) with WUKONG 1B, sunvozertinib was further evaluated at 200 mg and 300 mg once daily12 as discussed later in this article.
WU-KONG 6 (Phase 2, China)
A similar Phase II study, WU-KONG6, was conducted in 2021 as a single-arm, multicenter trial in China in which all enrolled patients received 300 mg daily. This trial reported an independent review committee (IRC)-assessed overall response rate (ORR) of 61% (median DOR 8.3 months) and provided the pivotal data leading to breakthrough therapy designations by both the United States FDA and the China National Medical Products Administration (NMPA) in 2022, with subsequent conditional approval in China in 2023.11
200mg vs 300mg: Efficacy and Tolerability
In July 2025, the FDA granted accelerated approval of sunvozertinib at 200 mg once daily for patients with EGFR exon20 insertion–mutant NSCLC previously treated with platinum chemotherapy, based on findings from the WU-KONG1B trial.13 In China, approval was granted at 300 mg following results from WU-KONG6,11 leading to differences in the approved dose across regions.
WU-KONG1B, a multinational phase II study, compared the efficacy and safety of 200 mg and 300 mg dosing. Confirmed ORRs were 45.9% at 200 mg and 47.2% at 300 mg (confirmed ORR 45.8% in the pooled 300 mg cohort), with no clinically meaningful difference between the two doses. Median PFS was also comparable (8.4 for 200mg vs 7.7 months for 300mg). DoR modestly favored 300mg (13.8 vs 11.1 months). Subgroup analyses indicated higher activity of 300 mg in patients with brain metastases (52.4% vs 28.6%) and in those previously exposed to amivantamab (41.7% vs 25%).12
Concurrently, the 300 mg dose was associated with substantially greater toxicity. Diarrhea was more frequent (82.9% vs 68.1%), with a higher incidence of grade ≥3 events (18% vs 2.2%). Rash occurred more often at 300 mg (47.7% vs 40.7%), although grade 3 cases were comparable across doses (4.5% vs 4.4%). Treatment modifications were more frequent with 300 mg – interruptions (49.5% vs 35.2%), reductions (38.7% vs 23.1%), and discontinuations (7.2% vs 4.4%). Discontinuations were mainly driven by interstitial lung disease (1.8% vs 0), pneumonitis (1.8% vs 0), and pneumonia (1.8% vs 0), while dose reductions were primarily due to diarrhea (9.9% vs 3.3%) and elevated CPK (7.2% vs 4.4%).12
Collectively, these data support the FDA’s decision to approve 200 mg as the U.S. label dose, achieving comparable efficacy with improved tolerability. Although the 300 mg regimen may be considered in specific subgroups (such as patients with brain metastasis and prior exposure to amivantamab), its use is limited by increased toxicity. The minimal gain in ORR (absolute difference 1.3%) does not appear to justify the increased toxicity, particularly in patients whom quality of life and tolerability are important considerations.
An ongoing phase III global trial, WU-KONG28, is currently evaluating sunvozertinib as first-line therapy compared with platinum-based chemotherapy in patients with NSCLC and EGFR exon20 insertion mutations. If positive, this study could potentially move TKI into the frontline standard of care in treating EGFR exon20ins NSCLC.14
Beyond Clinical Data: The Prescriber’s Experience
Despite FDA approval, sunvozertinib remains largely unavailable to clinicians and patients in the United States. Dizal, the developer of the drug, lacks commercial presence or distribution network in the United States. With manufacturing based in China, distribution is further hindered by ongoing supply chain barriers and the current 2025 U.S.–China trade tariffs.15 Establishing a U.S.-based manufacturing facility appears unlikely in the near term. Until a distribution or commercialization agreement is secured, sunvozertinib will not reach U.S. pharmacy shelves.
For patients considering access through China, additional barriers exist. The approved U.S. dose is 200 mg once daily, whereas in China the approved dose is 300 mg, with only the 150 mg tablets available to be dispensed. This discrepancy makes cross-border procurement impractical.
These challenges risk blunting the momentum of sunvozertinib’s approval. If logistical barriers persist, there is a real possibility that competitor agents in development for exon20ins NSCLC may outpace sunvozertinib in adoption despite its solid clinical profile.
Emerging Contenders
Several novel TKIs are in development for EGFR exon20ins–mutant NSCLC and may represent potential competitors to sunvozertinib. Among these, furmonertinib and zipalertinib have also shown encouraging early results.
Furmonertinib is a third-generation small molecule EGFR TKI initially developed for EGFR T790M–mutant NSCLC and later repurposed at a higher daily dose (160mg, 240 mg) to target exon20ins, with minimal inhibitory activity against wild-type EGFR.16 In the phase Ib FAVOUR study, furmonertinib 240mg daily has an ORR of 46.2% in previously treated patients (n=28, comparable to the ORR of sunvozertinib (ORR 45.9%). Diarrhea occurred in 73% of patients (no grade 3), slightly higher than with sunvozertinib (68.1% at 200mg; with grade ≥3 at 2.2%),12,16 whereas rash was less frequent than sunvozertinib (23% vs 40.7% at 200mg). Hematologic adverse events were also more common with furmonertinib (43% vs. 30.8%); grade ≥3 were comparable (~4% in both groups).12,16 Limitations of the FAVOUR study include the higher dose requirement for exon20ins NSCLC, a relatively small patient population, shorter follow-up, and single-region cohort design, in contrast to the larger, multinational studies of sunvozertinib.12,16 Table 1 summarizes key differences among emerging tyrosine kinase inhibitors targeting EGFR exon20ins-mutated NSCLC. A phase III study (FURVENT) is ongoing to evaluate furmonertinib against platinum-based chemotherapy in the first-line setting (Table 2) 17
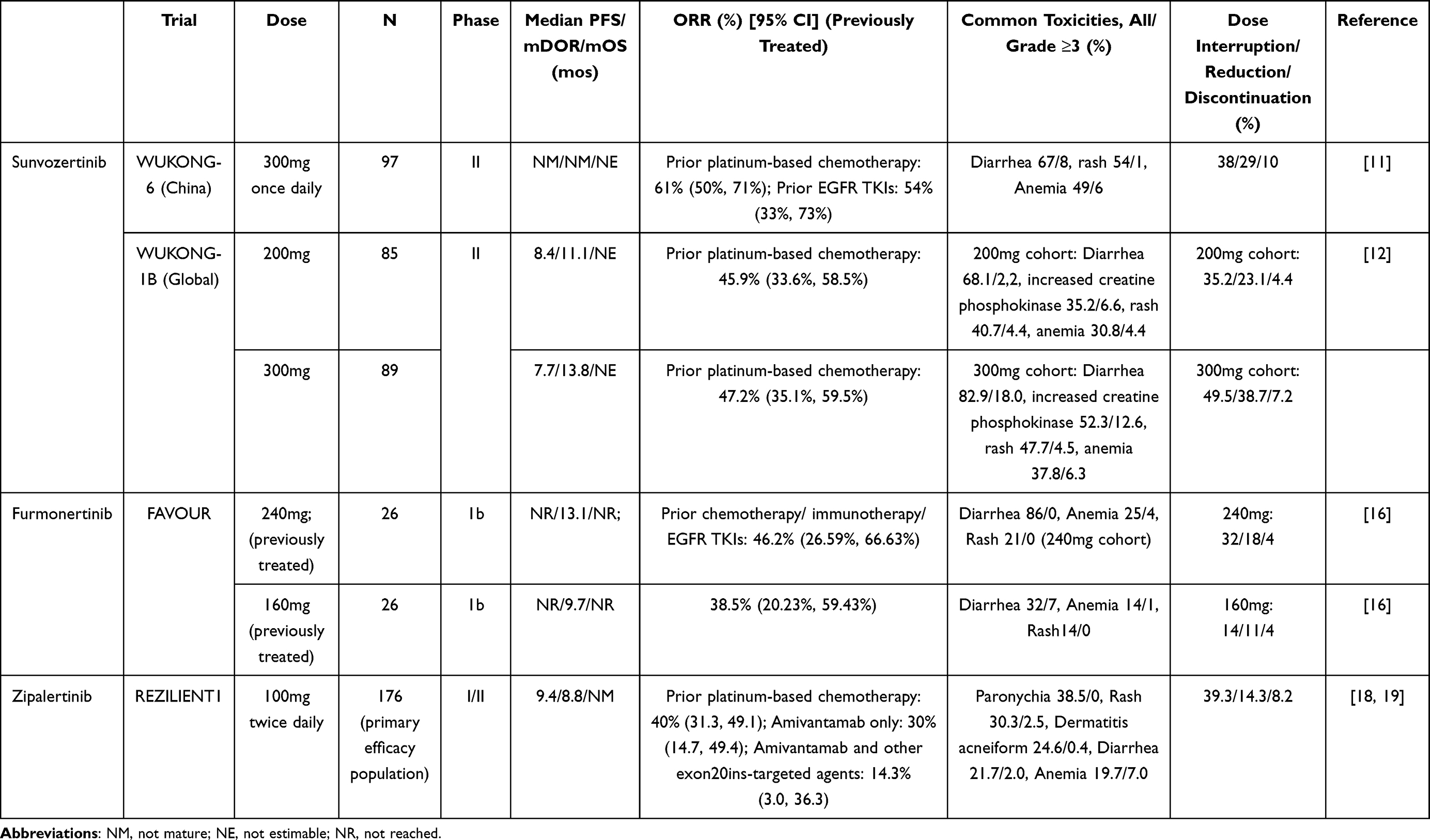 |
Table 1 Emerging Tyrosine Kinase Inhibitors for Epidermal Growth Factor Receptor (EGFR) Exon 20 Insertion-Mutated Non-Small Cell Lung Cancer (NSCLC) |
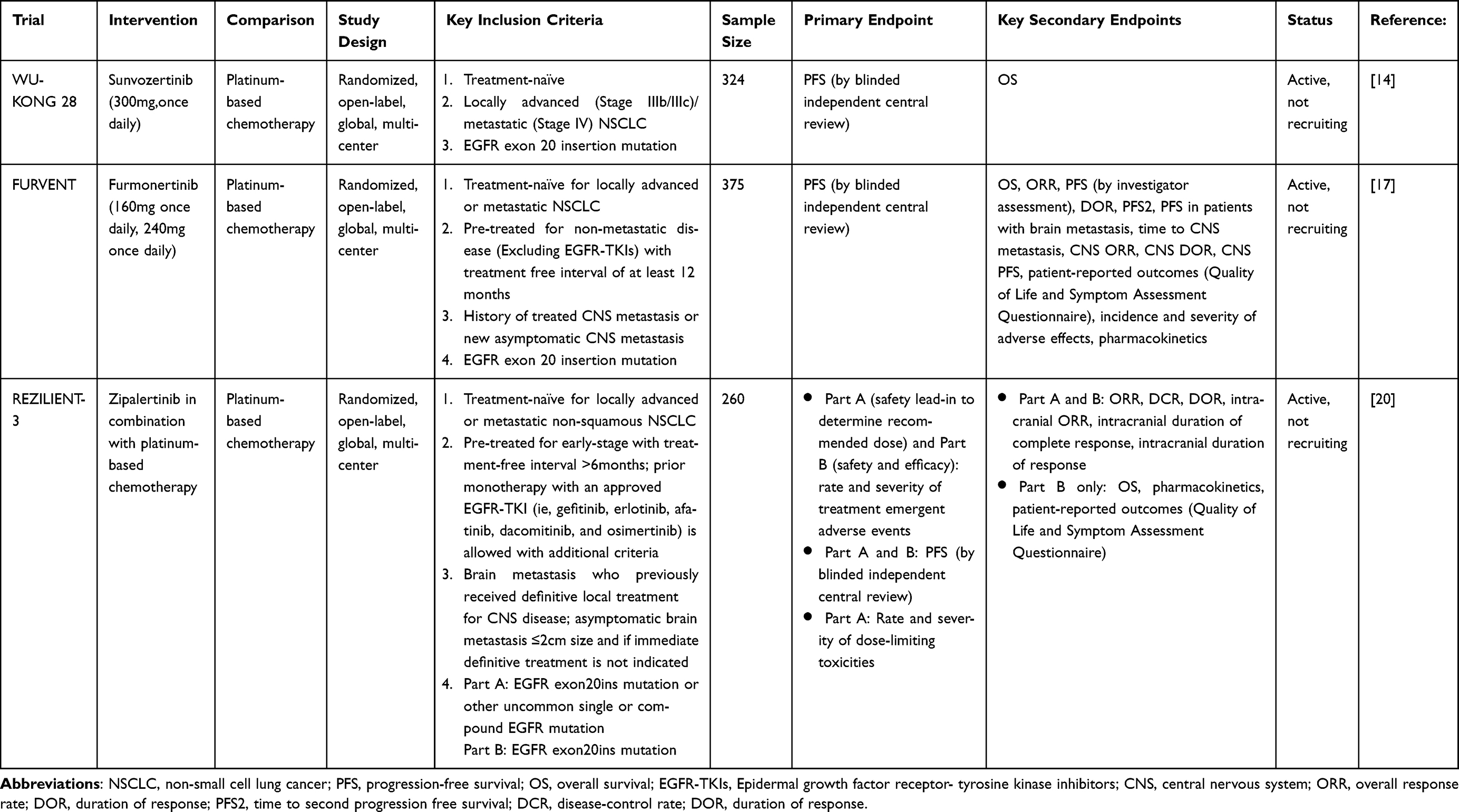 |
Table 2 Ongoing Phase III Clinical Trials Comparing Sunvozertinib, Furmonertinib and Zipalertinib |
Zipalertinib is another oral mutant-selective pyrimidine-based EGFR TKI similar to sunvozertinib. It demonstrates greater potency against exon20ins compared to wild-type EGFR, which reduces the frequency of EGFR-related toxicities.18 In the phase I/II REZILIENT-1 trial, it demonstrated an ORR of 40% in platinum-only pretreated patients (median DOR 8.8 mos) and 30% after prior amivantamab (median DOR 14.7mos), as outlined in Table 1. For comparison, sunvozertinib has reported an ORR 46% with DOR of 11.1 mos at 200mg dose in platinum-pretreated patients. The safety profile of zipalertinib showed rash (30.3%) and acneiform dermatitis (24.6%) at lower frequencies than sunvozertinib (40.7% at 200mg). Diarrhea occurred in 21.7% of patients, with grade ≥3 events in 2.0%, also lower than with sunvozertinib (68.1% at 200mg, with grade ≥3 at 2.2%).12,18,19 Treatment-related adverse events leading to discontinuation were almost similar between zipalertinib and sunvozertinib (8.2% vs 7.2% at 200mg), though treatment interruptions were higher with zipalertinib (39.3% vs. 23.1%).12,19 Both agents have demonstrated activity in patients with brain metastases; zipalertinib achieved an intracranial ORR of 30.9% (median DOR 8.3 months), while sunvozertinib reported an intracranial ORR of 28.6% with DOR of 8.4 months at 200 mg and higher ORR 52.4% with DOR of 7.7 months at 300 mg.12,19 Ongoing studies include the phase III REZILIENT-3 trial, evaluating zipalertinib in combination with platinum-based chemotherapy in the first-line setting for EGFR exon20ins NSCLC20 (Table 2).
Summary and Perspective
Given the persistent unmet need in NSCLC harboring EGFR exon20ins mutations, the oral TKI sunvozertinib represents an important treatment option in the second-line setting. Current evidence suggests that the 200mg dose approved in the United States offers efficacy generally comparable to the 300mg dose approved in China, with a more favorable tolerability profile, although certain subgroups (eg. patients with brain metastasis and prior amivantamab exposure) may derive incremental benefit from the higher dose. Its clinical activity and tolerability support ongoing evaluation in the frontline setting, and phase III trials such as WU-KONG28 will be critical in defining its future role compared with platinum-based chemotherapy.
At the same time, the therapeutic landscape continues to evolve. Other emerging TKIs, such as furmonertinib and zipalertinib, have shown promising activity in EGFR exon20ins-positive NSCLC, although their Asia-based production similarly limits immediate access. Yet scientific progress alone is not sufficient. Despite FDA approval, sunvozertinib remains effectively out of reach for patients and clinicians in the United States. Ultimately, the future impact of these therapies will depend not only on efficacy and tolerability, but also on whether they can be delivered to patients in a timely and practical manner.
Cancer drugs are not a luxury; they are essential. Life-saving treatments should be on standby, ready for rapid deployment at the time of diagnosis, rather than delayed by regulatory or logistical hurdles. Oncology, perhaps more than any other field, sits at the crossroads of science, commerce, and international politics—where trade policy, nationalism, and global supply chains directly influence patient care. The case of sunvozertinib raises a broader question: how will current tariff structures affect the future availability of oncology therapeutics in the United States?
Disclosure
Zhaohui Liao Arter reports Advisory board from Jassen, from Rigel, from EMD Serono, from Taiho, from Catalyst, and from Boehringer Ingelheim., outside the submitted work. Sai-Hong Ignatius Ou reports personal fees from Pfizer, personal fees from Abbvie, personal fees from Bayer, stock ownership from MBrace Therapeutics, stock ownership from BlossomHIll Therapeutics, stock ownership from Lilly, stock ownership from Nuvalent, and stock options from Nuvation Bio, outside the submitted work; Misako Nagasaka reports personal fees from AstraZeneca, personal fees from Daiichi Sankyo, personal fees from Pfizer, personal fees from Lilly, personal fees from Genentech, personal fees from Regeneron, personal fees from Johnson and Johnson, personal fees from Mirati/BMS, personal fees from Takeda, personal fees, travel support from AnHeart/Nuvation Bio, personal fees from Caris Life Sciences, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Riess JW, Gandara DR, Frampton GM, et al. Diverse EGFR Exon 20 insertions and co-occurring molecular alterations identified by comprehensive genomic profiling of NSCLC. J Thorac Oncol. 2018;13(10):1560–8. doi:10.1016/j.jtho.2018.06.019
2. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
3. Sequist LV, Yang JC-H, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31(27):3327–3334. doi:10.1200/JCO.2012.44.2806
4. Bazhenova L, Minchom A, Viteri S, et al. Comparative clinical outcomes for patients with advanced NSCLC harboring EGFR exon 20 insertion mutations and common EGFR mutations. Lung Cancer. 2021;162:154–161. doi:10.1016/j.lungcan.2021.10.020
5. Vyse S, Huang PH. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduction Targeted Therapy. 2019;4(1):5. doi:10.1038/s41392-019-0038-9
6. Zhou C, Tang K-J, Cho BC, et al. Amivantamab plus Chemotherapy in NSCLC with EGFR Exon 20 insertions. N Engl J Med. 2023;389(22):2039–2051. doi:10.1056/NEJMoa2306441
7. Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR Exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: initial results from the CHRYSALIS Phase I study. J Clin Oncol. 2021;39(30):3391–3402. doi:10.1200/JCO.21.00662
8. Jänne PA, Wang B-C, Cho BC, et al. First-line mobocertinib versus platinum-based chemotherapy in patients with EGFR Exon 20 insertion–positive metastatic non–small cell lung cancer in the Phase III EXCLAIM-2 trial. J Clin Oncol. 2025;43(13):1553–1563. doi:10.1200/JCO-24-01269
9. ZEGFROVY (sunvozertinib) [package insert]. U.S. Food and Drug Administration website. 2025.
10. Wang M, Yang JC-H, Mitchell PL, et al. Sunvozertinib, a selective EGFR inhibitor for previously treated non–small cell lung cancer with EGFR Exon 20 insertion mutations. Cancer Discov. 2022;12(7):1676–1689. doi:10.1158/2159-8290.CD-21-1615
11. Wang M, Fan Y, Sun M, et al. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, phase 2 trial. Lancet Respir Med. 2024;12(3):217–224. doi:10.1016/S2213-2600(23)00379-X
12. Yang JC-H, et al. Phase II dose-randomized study of sunvozertinib in platinum-pretreated non–small cell lung cancer with epidermal growth factor receptor Exon 20 insertion mutations (WU-KONG1B). J Clin Oncol. 2025;43(29):3198–208. JCO–25–00788.
13. Yang JC-H, Doucet L, Wang M, et al. A multinational pivotal study of sunvozertinib in platinum pretreated non-small cell lung cancer with EGFR exon 20 insertion mutations: primary analysis of WU-KONG1 study. J Clin Oncol. 2024;42(16_suppl):8513. doi:10.1200/JCO.2024.42.16_suppl.8513
14. A phase 3, open-label, randomized, multi-center study of DZD9008 versus platinum-based doublet chemotherapy as first-line treatment for patients with locally advanced or metastatic non-small cell lung cancer harboring epidermal Growth factor receptor Exon 20 insertion mutation. 2022.
15. Nagumo STAJ. Asian drugmakers’ shares hit as Trump announces 100% tariff. 2025.
16. Han B, Zhou C, Zheng W, et al. OA03.04 A phase 1b study of furmonertinib, an oral, brain penetrant, selective EGFR inhibitor, in patients with advanced NSCLC with EGFR Exon 20 INSERTIONS. J Thorac Oncol. 2023;18(11):S49. doi:10.1016/j.jtho.2023.09.033
17. Spira AI, Cho BC, Felip E, et al. FURVENT: phase 3 trial of furmonertinib vs chemotherapy as first-line treatment for advanced NSCLC with EGFR exon 20 insertion mutations (FURMO-004). J Clin Oncol. 2024;42(16_suppl):TPS8668–TPS8668. doi:10.1200/JCO.2024.42.16_suppl.TPS8668
18. Piotrowska Z, Tan DS-W, Smit EF, et al. Safety, tolerability, and antitumor activity of zipalertinib among patients with non–small-cell lung cancer harboring epidermal growth factor receptor Exon 20 insertions. J Clin Oncol. 2023;41(26):4218–4225. doi:10.1200/JCO.23.00152
19. Piotrowska Z, Passaro A, Nguyen D, et al. Zipalertinib in patients with epidermal growth factor receptor Exon 20 insertion-positive non–small cell lung cancer previously treated with platinum-based chemotherapy with or without amivantamab. J Clin Oncol. 2025;43(21):2387–2397. doi:10.1200/JCO-25-00763
20. Heymach JV, Yu HA, Besse B, et al. REZILIENT3: randomized phase III study of first-line zipalertinib plus chemotherapy in patients with EGFR exon 20 insertion-mutated NSCLC. Future Oncol. 2025;21(5):549–556. doi:10.1080/14796694.2025.2457294
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.