Back to Journals » Psoriasis: Targets and Therapy » Volume 16
Sugary Drinks and High-Fat Foods are Associated with Poor Treatment Response in Psoriasis: A Prospective Study in Shanghai
Authors Song J ![]() , Luo Y, Zhang R, Gao X
, Luo Y, Zhang R, Gao X ![]() , Shen F, Cai R, Lu J, Xu H, Ma X, Li B, Jiang W, Wang R
, Shen F, Cai R, Lu J, Xu H, Ma X, Li B, Jiang W, Wang R ![]()
Received 15 April 2026
Accepted for publication 7 July 2026
Published 14 July 2026 Volume 2026:16 617180
DOI https://doi.org/10.2147/PTT.S617180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Enzo Errichetti
Jiankun Song,1,* Yue Luo,2,* Rui Zhang,3,* Xiangjin Gao,3 Fanlingzi Shen,3 Ruiqi Cai,4 Jinrong Lu,4 Haotian Xu,1 Xin Ma,2 Bin Li,2 Wencheng Jiang,2 Ruiping Wang3
1Central Laboratory, Shanghai Skin Disease Hospital, Institute of Dermatology, School of Medicine, Tongji University, Shanghai, 200443, People’s Republic of China; 2Traditional Chinese Medicine Dermatology Department, Shanghai Skin Disease Hospital, School of Medicine, Tongji University, Shanghai, 200443, People’s Republic of China; 3Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, Shanghai, 200443, People’s Republic of China; 4School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruiping Wang, Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, 1278 Baode Road, Jing’an District, Shanghai, 200443, People’s Republic of China, Email [email protected] Wencheng Jiang, Traditional Chinese Medicine Dermatology Department, Shanghai Skin Disease Hospital, School of Medicine, Tongji University, 1278 Baode Road, Jing’an District, Shanghai, 200443, People’s Republic of China, Email [email protected]
Purpose: While dietary factors are known to be associated with the development and progression of psoriasis, their effect on treatment efficacy remains unclear. Therefore, this study aimed to elucidate the influence of tea consumption, sugar drinks, and high-fat foods on the treatment response in psoriasis.
Patients and methods: We undertook a prospective cohort study comprising 559 patients with psoriasis from Shanghai Skin Disease Hospital between 2022 and 2024. Data on demographics, lifestyle (including tea, sugary drinks, and high-fat food consumption), and disease severity (PASI, BSA, PGA) were collected via structured questionnaires at baseline, week 4, and week 8. The primary endpoints were the proportions of patients achieving PASI 50 responses at week 8. Multivariable logistic regression was used to estimate odds ratios with 95% confidence intervals, adjusting for age, sex, BMI, smoking, alcohol, and treatment regimen. Data were analyzed using SAS 9.4 software.
Results: In the psoriasis cohort (mean age 48.5 years; 73.2% male), 37.1% and 68.7% of patients consumed sugar drinks and high-fat foods ≥ 2 times/week, respectively. Frequent sugar drinks consumption (≥ 4 times/week) was independently associated with significantly reduced odds of achieving PASI 50 (adjusted OR=0.24, 95% CI: 0.08– 0.75) and PASI 75 (adjusted OR=0.27, 95% CI: 0.07– 1.00) at week 8. Moderate intake of high-fat foods (2– 3 times/week) showed an inverse, borderline significant association with PASI 50 at week 4 (adjusted OR=0.68, 95% CI: 0.45– 1.00). Tea consumption showed a non-significant association with treatment response (e.g, week 8 PASI 50 adjusted OR=1.44, 95% CI: 0.88– 2.35), warranting further investigation in larger cohorts.
Conclusion: This study demonstrates that high consumption of sugar drinks and high-fat foods is associated with suboptimal treatment response in psoriasis. Tea consumption was not significantly associated with treatment outcomes, although further investigation with larger cohorts may be warranted. These findings highlight the importance of integrating dietary assessment and counseling into comprehensive psoriasis management.
Keywords: psoriasis, tea consumption, sugar drinks, high-fat foods, treatment outcome
Introduction
Psoriasis, a common immune‑mediated inflammatory skin disorder with a chronic relapsing course,1 affecting over 60 million individuals and imposing substantial physical, emotional, and psychosocial burdens.2 Its pathogenesis arises from a complex interplay of immunity, genetics, and environmental factors, with psychological stress, smoking, obesity, and alcohol commonly acting as external triggers that induce immune dysregulation and sustain an IL‑17/IL-23-mediated inflammatory cascade.3,4 Clinical severity and therapeutic response are primarily quantified using the Psoriasis Area and Severity Index (PASI),5,6 with treatment efficacy conventionally defined as the proportion of patients achieving PASI 50, PASI 75, or higher improvements from baseline.7–9
Treatment outcomes in psoriasis exhibit considerable heterogeneity,10 influenced by baseline disease characteristics, comorbidities, genetic predisposition, socioeconomic factors, and modifiable lifestyle behaviours such as smoking, alcohol consumption, and dietary patterns.11–15 Among these, diet has gained increasing attention as a key environmental factor that may modulate disease activity.16 Emerging clinical evidence further supports the dietary-psoriasis connection. Interventional studies have shown that low‑calorie or Mediterranean diets can improve PASI scores in overweight patients,17,18 while observational evidence suggests that psoriasis patients often consume excessive fatty foods, refined carbohydrates, and sugar‑sweetened beverages, a pro‑inflammatory profile that perpetuates both metabolic disturbances and cutaneous inflammation.19 Conversely, tea consumption, particularly green tea contains polyphenolic catechins that regulate inflammatory signalling and may confer anti‑psoriatic benefits.20
Despite growing interest, the evidence linking specific dietary components to objectively measured treatment response remains limited. Most existing studies are cross‑sectional or have small samples, short follow‑ups, and inconsistent dietary definitions. In particular, prospective data examining the association of sugary drinks, high‑fat foods, and tea consumption with standardised PASI endpoints are lacking. To address these evidence gaps, we established a prospective psoriasis cohort to evaluate the associations between intake of tea, sugary drinks, and high-fat foods with the attainment of PASI 50 and PASI 75 responses in psoriasis patients, with the aim of providing evidence to inform dietary intervention strategies in clinical practice.
Methods
Study Population
This prospective study based on a cohort of patients with psoriasis established at Shanghai Skin Diseases Hospital from 2022 to 2024. The diagnosis of psoriasis was in accordance with the Chinese clinical dermatology guidelines and international diagnostic standards. This study enrolled patients of either sex aged 18 years or older with psoriasis vulgaris who had no intention of relocating within the following year. Individuals were excluded if they were incapable of providing informed consent or presented with neurological or psychiatric disorders. The study protocol received approval from the Institutional Ethical Review Board of Shanghai Skin Disease Hospital (Approval No.2022–25) and was registered with the Chinese Clinical Trial Registry (ChiCTR2200066894). All procedures were conducted in strict compliance with the ethical principles of the Declaration of Helsinki.
Sample Size
We calculated the required sample size using the formula n=[μα2× p(1-p)]/δ2 and set p=30% (the prevalence of sugary drinks was 30%), α=0.05, δ=15% of p. A 10% non-response rate was also taken into account. Based on these parameters, a minimum of 399 psoriasis patients needed to be enrolled. Ultimately, 559 individuals with psoriasis were recruited and included in the final analysis.
Data Collection
Data for this study were collected via questionnaires administered by dermatologists during patient consultations. These instruments gathered information across the following domains: (1) demographic profiles, including sex, age, educational attainment, and body mass index (BMI); (2) lifestyle habits, such as smoking status, alcohol consumption, tea drinking, sugary drinks and high-fat foods; (3) psoriasis severity metrics, specifically Body Surface Area (BSA), Psoriasis Area and Severity Index (PASI), and Physician’s Global Assessment (PGA), evaluated at baseline, week 4, and week 8; and (4) therapeutic regimens, documenting the use of treatments like acitretin, methotrexate (MTX), and biologic agents. The questionnaire was developed through literature review and expert consultation, with dietary items adapted from validated food frequency questionnaires for Chinese populations. In a pilot test on 30 psoriasis patients, it demonstrated good reliability (Cronbach’s α=0.82) and content validity (CVI=0.88). To ensure consistent interpretation, interviewers provided standardised examples of each dietary category (as detailed in the Definitions and classifications section) before participants reported their consumption frequencies. All interviewers were uniformly trained and followed a standardised protocol to minimise variability.
Definitions and Classifications
In this study, dietary exposure variables were categorized as follows: tea consumption was defined as a binary variable (yes or no), the intake of sugary drinks (including cola, Sprite, sweetened milk tea, fruit-flavored juices and energy drinks) and high-fat foods (such as hamburgers, fried chicken, French fries, barbecued and creamy pastries) was classified into three groups based on weekly frequency: 0 or 1 time, 2 or 3 times, and ≥ 4 times.
Disease severity in psoriasis was assessed using several established metrics. The Psoriasis Area and Severity Index (PASI) was employed to quantify the severity of skin lesions, with scores ranging from 0 (indicating no disease) to 72 (most severe), where a higher score denotes more severe condition. The PASI 50 response and PASI 75 response were defined as an improvement of at least 50% and 75% from the baseline PASI score respectively, calculated using the formula: [(PASI at baseline - PASI at week t)/PASI at baseline] × 100%. The Body Surface Area (BSA) metric represents the percentage of affected skin area, ranging from 0% (best) to 100% (worst), with a higher percentage indicating greater severity. The Physician’s Global Assessment (PGA) reflects the clinician’s comprehensive evaluation of psoriasis severity, scored on a scale from 0 (best) to 5 (worst).
In this study, age was divided into four groups: <35 years, 35–45 years, 46–60 years, and >60 years. Educational level was classified as primary school or below, secondary school, high school, or university and above. Monthly income was categorized as < 3,000, 3,000–5,000, 5,001–10,000 RMB, and >10,000 RMB. Body Mass Index (BMI) was derived from weight in kilograms divided by the square of height in meters and was classified according to Chinese criteria into three categories: <23.9 (normal or underweight), 24.0–28.0 (overweight), and >28.0 (obese).
Statistical Analysis
All statistical analyses were conducted using SAS version 9.4. Quantitative variables were summarized either as mean with standard deviation (SD) or as median with interquartile range (IQR). Group comparisons were performed using Student’s t-test or Mann–Whitney U-test. Qualitative variables were described using frequencies and percentages (%), with intergroup differences evaluated via the chi‑square test. To identify factors associated with treatment response (PASI 50 and PASI 75) at weeks 4 and 8, logistic regression models were employed to estimate odds ratios (ORs) along with their 95% confidence intervals (CIs). Forest tree figures were generated to visually present the variables linked to achieving PASI 50 at weeks 4 and 8, as well as PASI 75 at the same time points, respectively. In the present study, all statistical tests performed were two-tailed and a p-value of <0.05 was deemed to indicate statistical significance.
Results
Baseline Characteristics of the Study Population
This study enrolled 559 individuals diagnosed with psoriasis, all of whom completed the full 8‑week observation period without any dropouts. Of the total cohort, 409 (73.2%) identified as male and 150 (26.8%) as female. Their mean age stood at 48.5 years. Moreover, 79.1% of the participants were 35 years of age or older, and among them, 26.7% had reached above 60 years. Regarding socioeconomic status, over 48.1% of patients had attained university-level education or higher, and 21.8% reported a monthly income exceeding 10,000 RMB. In terms of lifestyle and clinical characteristics, 79.8% of participants were married, and 60% were classified as overweight or obese. The prevalence of smoking history was 45.4%, while 27.2% reported alcohol consumption. The median disease duration was 11 years (interquartile range [IQR]: 3.0–21.0). At baseline assessment, the median scores for disease severity measures were as follows: PASI 11.2 (IQR: 8.0–16.8), BSA 15.0 (IQR: 10.0–28.0), and PGA 2.7 (IQR: 2.0–3.0). Table 1 indicates that, relative to female patients, male had significantly higher frequencies of obesity, smoking, and alcohol use, along with more severe PASI and PGA scores (p < 0.01).
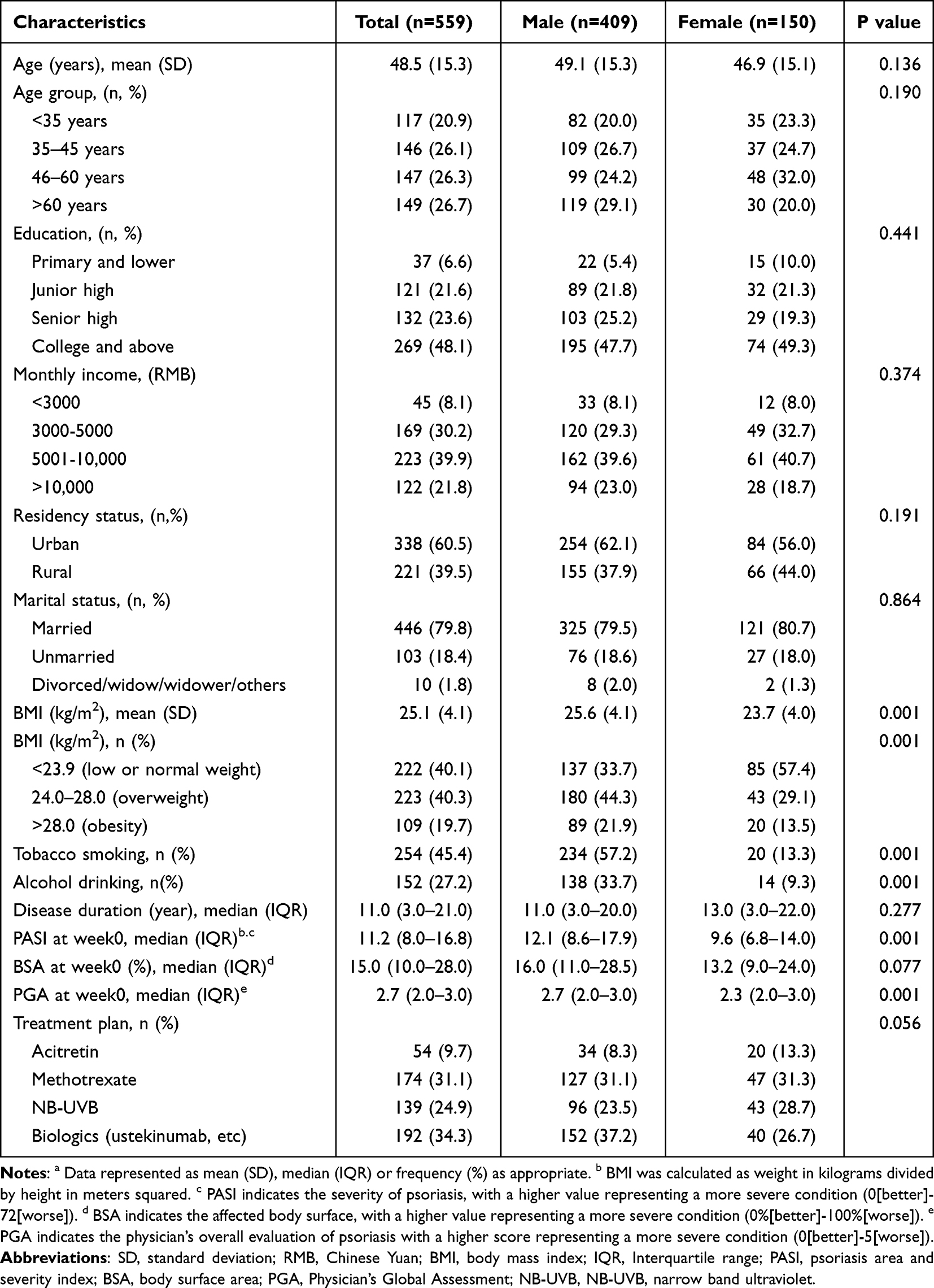 |
Table 1 The Baseline Demographic Features of Patients with Psoriasis a |
Dietary Consumption Patterns Among Psoriasis Patients
In this study, 29.8% of the 559 psoriasis patients consumed tea, 37.1% ingested sugary drinks at least twice per week, and 68.7% consumed high-fat food at least twice weekly. Stratified by gender, male patients demonstrated significantly higher prevalence across all three dietary categories compared to females: tea consumption was 34.2% in males versus 18.0% in females (P=0.001); sugary drinks intake 0 or 1 time/week was 60.1% in males versus 70.7% in females, ≥2 times/week was 39.8% in males versus 29.3% in females (P=0.015); and high-fat food consumption 0 or 1 time/week was 28.9% in males versus 38% in females, ≥2 times/week was 71.1% in males versus 62.0% in females (P=0.029) Table 2.
 |
Table 2 The Consumption of Tea, Sugary Drinks and High-Fat Food Among Patients with Psoriasis a |
Therapeutic Response in Psoriasis Patients at 4 and 8 Weeks of Treatment
At week 4, the PASI 50 and PASI 75 response rate were 41.1% and 13.6%, respectively. No statistically significant sex-based differences were found in PASI 50 response rates, PASI 75 response rates, or BSA scores (P > 0.05). By week 8, the response rate was 76.4% for PASI 50 and 46.5% for PASI 75, respectively. Female patients demonstrated significantly higher response rates than males for both PASI 50 (83.3% vs 73.8%, P=0.019) and PASI 75 (58.0% vs 42.3%, P=0.001). Additionally, median BSA scores were lower in females (2.0, IQR: 0.8–4.4) compared to males (3.5, IQR: 1.6–7.2), with all differences being statistically significant (P=0.024) Table 3.
 |
Table 3 The PASI, BSA and PGA at Week 4 and Week 8 Among Patients with Psoriasis a |
Factors Associated with Treatment Response in Psoriasis Patients
Analysis of factors influencing treatment response revealed several significant associations. Higher education level consistently predicted improved PASI 50 achievement at both week 4 (OR=2.17, 95% CI:1.01–4.67) and week 8 (OR=3.22, 95% CI:1.56–6.67). Female patients demonstrated better treatment outcomes, with significantly higher PASI 75 response at week 8 (OR=1.88, 95% CI:1.29–2.75). Negative predictors included advanced age, with patients >60 years showing reduced PASI 50 (OR=0.52, 95% CI:0.29–0.94) and PASI 75 (OR=0.46, 95% CI:0.28–0.76) responses. Smoking substantially compromised treatment efficacy for both PASI 50 (OR=0.23, 95% CI:0.15–0.35) and PASI 75 (OR=0.15, 95% CI:0.10–0.21) at week 8. Alcohol consumption similarly negatively affected PASI 50 (OR=0.36, 95% CI:0.24–0.54) and PASI 75 (OR=0.22, 95% CI:0.14–0.34) achievement. Other significant factors included obesity (BMI>28, OR=0.60 for PASI 75), longer disease duration (5–10 years, OR=0.68 for PASI 75), and marital status, with divorced/widowed patients showing higher PASI 75 rates at week 4 (OR=4.43, 95% CI:1.81–7.00) Figures 1 and 2.
 |
Figure 1 Factors associated with achievement of PASI 50 at week 4 (A) and 8 (B) in patients with psoriasis in Shanghai. Bold text indicates statistical significance (P<0.05). Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index. |
 |
Figure 2 Factors associated with achievement of PASI 75 at week 4 (A) and 8 (B) in patients with psoriasis in Shanghai. Bold text indicates statistical significance (P<0.05). Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index. |
Association Between Dietary Patterns and Treatment Response in Psoriasis
In this study, sugary drinks and high-fat food demonstrated adverse effects on treatment outcomes (Table 4). Unadjusted and adjusted analyses of confounding factors consistently indicated that frequent sugary drinks (≥4 times/week) was associated with poorer treatment response. In the unadjusted model, sugary drinks consumption significantly reduced the likelihood of achieving PASI 50 (OR=0.30, 95% CI: 0.11–0.84) and PASI 75 (OR=0.27, 95% CI: 0.08–0.98) at week 8. After adjustment for age, gender, BMI, smoking, alcohol drinking, tea and high-fat food, the association remained significant for PASI 50 (OR=0.24, 95% CI: 0.08–0.75) and was consistent in direction for PASI 75 (OR=0.27, 95% CI: 0.07–1.00).
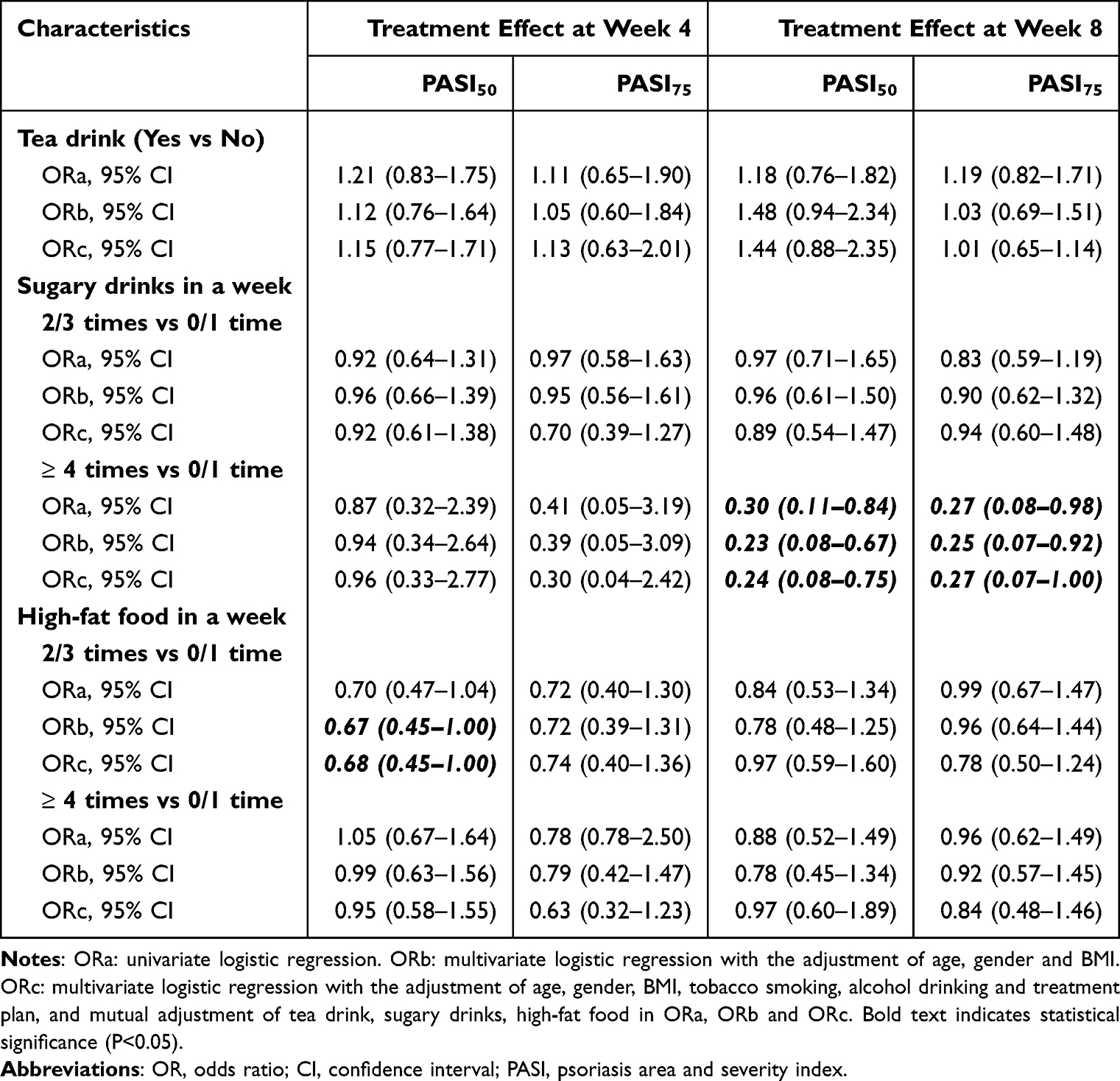 |
Table 4 Association Between Consumption of Tea, Sugary Drinks and High-Fat Food and Treatment Effect Among Patients with Psoriasis |
A borderline inverse association between high‑fat food consumption (2–3 times/week) and PASI 50 achievement was observed at week 4 in the fully adjusted model (OR=0.68, 95% CI: 0.45–1.00). However, this association was not sustained at week 8, where the corresponding ORs for the 2–3 times/week and ≥4 times/week groups were 0.97 (95% CI: 0.59–1.60) and 0.97 (95% CI: 0.60–1.89), respectively, with all confidence intervals crossing unity. In contrast, no statistically significant association was observed between tea consumption and treatment response across all models (eg, week 8 PASI 50, adjusted OR=1.44, 95% CI: 0.88–2.35). Although the point estimate suggested a potentially favorable direction, the wide confidence interval precludes definitive conclusions, and this possible association warrants further investigation in larger cohorts.
Discussion
Findings from this prospective cohort investigation indicate a link between dietary habits and psoriasis treatment outcome. Frequent consumption of sugary drinks was independently associated with significantly reduced odds of achieving PASI 50 and PASI 75 responses, even after comprehensive adjustment for potential confounders. A borderline inverse association for high‑fat food intake (2–3 times/week) was observed at week 4 (adjusted OR=0.68, 95% CI: 0.45–1.00), but this signal was not sustained at week 8. This temporal pattern may reflect the substantial rise in overall response rates from 41.1% at week 4 to 76.4% at week 8, whereby the relative contribution of dietary factors to residual disease activity could become less discernible as effective treatment predominates. In contrast, tea consumption was not significantly associated with treatment outcomes, with all confidence intervals crossing unity; the week 8 PASI 50 point estimate (OR=1.44) suggested a potential benefit, but wide confidence intervals preclude definitive conclusions. This null finding may be attributed to several methodological limitations, including a relatively low proportion of tea consumers (29.8%), resulting in limited statistical power, and the lack of differentiation between tea types (eg, green, black, oolong), which vary substantially in phytochemical composition, fermentation degrees, brewing practices, and bio-active compound extraction.20–23
Previous experimental studies have demonstrated that high‑fat and high‑sugar diets promote psoriasiform inflammation through multiple pathways, including enhanced IL‑17A‑producing γδ T cell accumulation, intestinal dysbiosis, and Treg dysfunction,24–26 while tea polyphenols exhibit anti‑inflammatory and antioxidant properties.27,28 These mechanistic insights provide a biological rationale for our epidemiological observations. However, given the observational nature of our study and the lack of direct molecular data, these mechanistic interpretations remain speculative and should be viewed as hypothesis‑generating rather than conclusive.
Our analysis further identified several significant non‑dietary determinants. Female patients showed more favourable outcomes, consistent with estrogen‑mediated modulation of T‑cell responses.29–31 Smoking and alcohol exerted negative effects,32–34 while higher education emerged as a positive predictor, possibly reflecting better health literacy and adherence.35,36
This study has several limitations. First, dietary intake was self‑reported, introducing potential recall bias. Second, the broad frequency categorisation and lack of portion‑size quantification may have introduced non‑differential misclassification, which typically attenuates effect estimates towards the null. Third, tea consumption was treated as binary, precluding dose‑response detection. Fourth, we lacked data on socioeconomic status, health awareness, overall dietary quality, physical activity, and comorbidities, raising the possibility of residual confounding—particularly for tea. Fifth, although we adjusted for treatment plan, the distinct expected response rates of biologics, MTX, and NB‑UVB may not be fully captured by categorical adjustment. Sixth, as a single‑center study, generalisability requires further validation. Finally, formal sensitivity analyses were not performed. Consequently, our findings should be interpreted as exploratory, and future studies with validated quantitative dietary tools, comprehensive covariate adjustment, and larger cohorts are warranted.
Notwithstanding these limitations, our findings possess notable clinical and public health significance. Dermatologists could incorporate brief dietary screening into routine consultations—asking about weekly consumption of sugary drinks and high‑fat foods—and offer simple replacement advice (eg, water or unsweetened tea instead of sugary drinks; lean protein instead of high‑fat processed foods). For patients with complex dietary patterns or metabolic comorbidities, referral to a registered dietitian may confer additional benefits. Integrating systematic dietary guidance into standard psoriasis care represents a viable, low‑cost approach to improving patient prognosis.
Conclusion
This study establishes frequent consumption of sugar drinks and high-fat foods as independent risk factors for suboptimal psoriasis treatment outcomes, while highlighting tea intake as a promising target for further investigation. These findings underscore the importance of addressing modifiable dietary habits within a comprehensive and individualized management approach for psoriasis.
Abbreviation
PASI, Psoriasis Area and Severity Index; SD, standard deviation; RMB, Chinese Yuan; BMI, body mass index; IQR, Interquartile range; PGA, Physician’s Global Assessment; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
The data supporting this study can be accessed by contacting Prof. Ruiping Wang ([email protected]). Inquiries should specify the research title and objectives for which the data are being requested.
Ethics Approval and Consent to Participate
This study received approval from the Institutional Ethical Review Board of Shanghai Skin Disease Hospital (approval No. 2022-25). Prior to enrollment, written informed consent was secured from every participant. The trial was also registered with the Chinese Clinical Trial Registry (ChiCTR2200066894). All procedures were carried out in accordance with the principles of the Declaration of Helsinki.
Acknowledgment
We thank all dermatologists at Shanghai Skin Disease Hospital for their effort for data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82505585), the National Qi-Huang scholar (Grant Number: [2025] No.182), Clinical Research Plan of SHDC (SHDC2024CRX032), and Shanghai Municipal Health Commission Traditional Chinese Medicine Standard Research Project (2025BZ004).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Armstrong AW, Blauvelt A, Callis Duffin K, et al. Psoriasis. Nat Rev Dis Primers. 2025;11(1):45. doi:10.1038/s41572-025-00630-5
2. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–11. doi:10.1016/S0140-6736(20)32549-6
3. Zeng J, Luo S, Huang Y, Lu Q. Critical role of environmental factors in the pathogenesis of psoriasis. J Dermatol. 2017;44(8):863–872. doi:10.1111/1346-8138.13806
4. Shen F, Song Y, Qiang Y, et al. Tobacco smoking interacted with alcohol drinking could increase the failure of PASI75 achievement at week 8 among patients with psoriasis: findings based on a psoriasis cohort. Psoriasis. 2024;14:103–114. doi:10.2147/PTT.S484609
5. Reich K, Mrowietz U. Treatment goals in psoriasis. J Dtsch Dermatol Ges. 2007;5(7):566–574. doi:10.1111/j.1610-0387.2007.06343.x
6. Svoboda SA, Ghamrawi RI, Owusu DA, Feldman SR. Treatment goals in psoriasis: which outcomes matter most? Am J Clin Dermatol. 2020;21(4):505–511. doi:10.1007/s40257-020-00521-3
7. Ferris LK, Bagel J, Huang Y-H, et al. FRONTIER-2: a phase 2b, long-term extension, dose-ranging study of oral JNJ-77242113 for the treatment of moderate-to-severe plaque psoriasis. J Am Acad Dermatol. 2024;92(3):495–502. doi:10.1016/j.jaad.2024.10.076
8. Ritchlin CT, Coates LC, McInnes IB, et al. Bimekizumab treatment in biologic DMARD-naïve patients with active psoriatic arthritis: 52-week efficacy and safety results from the Phase III, randomised, placebo-controlled, active reference BE OPTIMAL study. Ann Rheum Dis. 2023;82(11):1404–1414. doi:10.1136/ard-2023-224431
9. Stein Gold L, Bhatia N, Tallman AM, Rubenstein DS. A phase 2b, randomized clinical trial of tapinarof cream for the treatment of plaque psoriasis: secondary efficacy and patient-reported outcomes. J Am Acad Dermatol. 2020;84(3):624–631. doi:10.1016/j.jaad.2020.04.181
10. Lee H-J, Kim M. Challenges and Future Trends in the Treatment of Psoriasis. Int J Mol Sci. 2023;24(17):13313. doi:10.3390/ijms241713313
11. Guo J, Zhang HY, Lin WR, Lu LX, Su J, Chen X. Signaling pathways and targeted therapies for psoriasis. Signal Transduction Tar. 2023;8(1):ARTN437. doi:10.1038/s41392-023-01655-6
12. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
13. Dand N, Mahil SK, Capon F, Smith CH, Simpson MA, Barker JN. Psoriasis and genetics. Acta Derm Venereol. 2020;100(3):adv00030. doi:10.2340/00015555-3384
14. Vesikansa A, Mehtälä J, Aaltonen J, Konttinen R, Tasanen K, Huilaja L. Healthcare resource utilization patterns in psoriasis patients using biologic and conventional treatments in Finland. Front Immunol. 2024;15:1374829. doi:10.3389/fimmu.2024.1374829
15. Minghui L, Changyong G, Runtian Z, Jianhong L, Lingling Y, Xi C. The association between dietary consumption habits and psoriasis: a two-sample Mendelian randomization study. Front Nutr. 2024;11:1405663. doi:10.3389/fnut.2024.1405663
16. Musumeci ML, Nasca MR, Boscaglia S, Micali G. The role of lifestyle and nutrition in psoriasis: current status of knowledge and interventions. Dermatol Ther. 2022;35(9):e15685. doi:10.1111/dth.15685
17. Perez-Bootello J, Berna-Rico E, de Aragon CAJ, et al. Mediterranean diet and patients with psoriasis: the MEDIPSO randomized clinical trial. JAMA Dermatol. 2025;161(12):1215–1223. doi:10.1001/jamadermatol.2025.3410
18. Castaldo G, Rastrelli L, Galdo G, Molettieri P, Aufiero FR, Cereda E. Aggressive weight-loss program with a ketogenic induction phase for the treatment of chronic plaque psoriasis: a proof-of-concept, single-arm, open-label clinical trial. Nutrition. 2020;74:110757. doi:10.1016/j.nut.2020.110757
19. Hawkins P, Earl K, Tektonidis TG, Fallaize R. The role of diet in the management of psoriasis: a scoping review. Nutr Res Rev. 2024;37(2):296–330. doi:10.1017/S0954422423000185
20. Zheng X-Q, Zhang X-H, Gao H-Q, et al. Green tea catechins and skin health. Antioxidants. 2024;13(12):1506. doi:10.3390/antiox13121506
21. Frasheri L, Schielein MC, Tizek L, Mikschl P, Biedermann T, Zink A. Great green tea ingredient? A narrative literature review on epigallocatechin gallate and its biophysical properties for topical use in dermatology. Phytother Res. 2020;34(9):2170–2179. doi:10.1002/ptr.6670
22. Shen W, Ye Q, Zhang H, et al. A tea polyphenol-infused sprayable thermosensitive liposomal hydrogel for enhanced anti-inflammatory and antibacterial psoriasis treatment. J Funct Biomater. 2025;16(4):124. doi:10.3390/jfb16040124
23. Zheng X, Deng W, Wang X, Wu Z, Li C, Zhang X. Ameliorative effect of black tea extract on the skin of D-galactose-induced aging mice. Front Nutr. 2023;10:1275199. doi:10.3389/fnut.2023.1275199
24. Shi Z, Wu X, Yu S, et al. Short-term exposure to a Western diet induces psoriasiform dermatitis by promoting accumulation of IL-17A-producing γδ T cells. J Investigat Dermatol. 2020;140(9):1815–1823. doi:10.1016/j.jid.2020.01.020
25. Sivasami P, Elkins C, Diaz-Saldana PP, et al. Obesity-induced dysregulation of skin-resident PPARγ+ Treg cells promotes IL-17A-mediated psoriatic inflammation. Immunity. 2023;56(8). doi:10.1016/j.immuni.2023.06.021
26. Sonomoto K, Song R, Eriksson D, et al. High-fat-diet-associated intestinal microbiota exacerbates psoriasis-like inflammation by enhancing systemic γδ T cell IL-17 production. Cell Rep. 2023;42(7):112713. doi:10.1016/j.celrep.2023.112713
27. Zhang L, Huang Z, Xuan J, Yang L, Zhao T, Peng W. Anti-psoriatic activity of black, green and white tea extracts from Southeastern China. Molecules. 2024;29(6). doi:10.3390/molecules29061279
28. Rovaldi E, Di Donato V, Paolino G, et al. Epigallocatechin-gallate (EGCG): an essential molecule for human health and well-being. Int J Mol Sci. 2025;26(18):9253. doi:10.3390/ijms26189253
29. Zhang C, Dai X, Yin Z. Association between psoriasis and estrogen: a population-based study. J Am Acad Dermatol. 2025;93(4):1141–1143. doi:10.1016/j.jaad.2025.06.064
30. Wu H, Zeng L, Ou J, Wang T, Chen Y, Nandakumar KS. Estrogen acts through estrogen receptor-β to promote mannan-induced psoriasis-like skin inflammation. Front Immunol. 2022;13:818173. doi:10.3389/fimmu.2022.818173
31. Cassalia F, Lunardon A, Frattin G, Danese A, Caroppo F, Fortina AB. How hormonal balance changes lives in women with psoriasis. J Clin Med. 2025;14(2):582. doi:10.3390/jcm14020582
32. Qiang Y, Kuai L, Liu S, et al. Tobacco smoking negatively influences the achievement of greater than three-quarters reduction in psoriasis area and severity index after eight weeks of treatment among patients with psoriasis: findings from a prospective study. Tob Induc Dis. 2024;22. doi:10.18332/tid/184143
33. Näslund-Koch C, Skov L. Shedding light on the smoke: unravelling the impact of smoking cessation on psoriasis development. Br J Dermatol. 2024;191(2):157–158. doi:10.1093/bjd/ljae163
34. Wei J, Zhu J, Xu H, et al. Alcohol consumption and smoking in relation to psoriasis: a Mendelian randomization study. Br J Dermatol. 2022;187(5):684–691. doi:10.1111/bjd.21718
35. Larsen MH, Strumse YS, Andersen MH, Borge CR, Wahl AK. Associations between disease education, self-management support, and health literacy in psoriasis. J DermatolTreat. 2019;32(6):603–609. doi:10.1080/09546634.2019.1688233
36. Dressler C, Lambert J, Grine L, et al. Therapeutic patient education and self-management support for patients with psoriasis - a systematic review. J Dtsch Dermatol Ges. 2019;17(7):685–695. doi:10.1111/ddg.13840
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.