Back to Journals » Infection and Drug Resistance » Volume 15
Successful Treatment of Relapsed Epstein–Barr Virus-Associated Hemophagocytic Lymphohistiocytosis After Allo-HSCT with PD-1 Blockade: A Case Report
Received 10 May 2022
Accepted for publication 7 July 2022
Published 13 July 2022 Volume 2022:15 Pages 3751—3756
DOI https://doi.org/10.2147/IDR.S372998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yubo Pi, Jingshi Wang, Zhao Wang
Department of Hematology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
Correspondence: Zhao Wang, Department of Hematology, Beijing Friendship Hospital, Capital Medical University, YongAn Road 95th Xicheng District, Beijing, 100050, People’s Republic of China, Tel +86-10-63138303, Email [email protected]
Background: Epstein–Barr virus-associated hemophagocytic lymphohistiocytosis (EBV-HLH) is a rare and aggressive disease with high mortality and poor prognosis. To date, allogeneic hematopoietic stem cell transplantation (allo-HSCT) remains the only way to cure EBV-HLH. However, relapse of EBV-HLH after allo-HSCT is common and remains a major challenge.
Case Presentation: A 22-year-old woman with persistent fever for a month presented to our center with EBV-HLH. After induction of remission using two cycles of the L-DEP (PEG-aspargase, liposomal doxorubicin, etoposide, and high-dose methylprednisolone) regimen, the patient underwent an human leukocyte antigen (HLA)-identical sibling allo-HSCT. However, she experienced disease relapse soon after the procedure, and none of the possible treatment options achieved a sustained response. Finally, she received a sintilimab injection and achieved complete resolution of EBV-HLH.
Conclusion: We summarize a case of relapsed EBV-HLH after allo-HSCT that was successfully treated with a programmed cell death protein-1 (PD-1) antibody. Further studies are needed to determine whether PD-1 blockade has therapeutic potential for relapsed EBV-HLH after allo-HSCT.
Keywords: Epstein–Barr virus, allogeneic hematopoietic stem cell transplantation, PD-1 antibody, graft-versus-host disease
Introduction
Hemophagocytic lymphohistiocytosis (HLH) is a life-threatening condition characterized by uncontrolled activation of immunocytes, resulting in excessive release of inflammatory cytokines. HLH can be divided into primary HLH and secondary HLH based on the presence or absence of underlying genetic defects. Common triggers of secondary HLH include infections, malignancies, and autoimmune diseases. Epstein–Barr virus (EBV) infection has been reported to account for approximately 70% of infection-related HLH, especially in the Asian population.1 In EBV-associated HLH (EBV-HLH), EBV infects T cells more often than it does natural killer (NK) cells and drives abnormal proliferation of T/NK-cell lineages.2 According to previous studies, EBV-HLH is a rare and aggressive disease with high mortality and poor prognosis in adults and adolescents with a 1-year survival rate of less than 30%.3,4
There is currently no unified evidence-based treatment for EBV-HLH in adults. The HLH-94 and HLH-04 regimens are most commonly used; however, approximately 30% of patients remain unresponsive.5,6 In adults and adolescents with refractory or relapsed EBV-HLH, the remission rate with HLH-94/HLH-04 regimens was only 46.43%.3 Alternative regimens, such as DEP (liposomal doxorubicin, etoposide, and high-dose methylprednisolone) and L-DEP (PEG-aspargase, liposomal doxorubicin, etoposide, and high-dose methylprednisolone), are proven to be effective, with an overall response rate of 72.7%–85.7%.7,8 Interestingly, it has been observed that the expression of programmed death protein-1 (PD-1) increased on the surface of CD8+ T cells, and PD-1 blockade immunotherapy could restore T-cell immune function in EBV-HLH patients.9 To date, allogeneic hematopoietic stem cell transplantation (allo-HSCT) remains the only way to cure EBV-HLH.3 Thus, relapse of EBV-HLH after allo-HSCT is a clinical dilemma, and there have been no large-scale studies with respect to corresponding treatments.
Case Report
A 22-year-old woman with persistent fever for one month was admitted to our center on November 20, 2020. She was heavily treated with antibiotics before admission. Otherwise, the patient was previously considered healthy. Her routine work-up showed cytopenia in three lineages, hepatic insufficiency, increased levels of serum ferritin, elevated levels of soluble CD25 (sCD25), hepatomegaly, splenomegaly, and hemophagocytosis in the bone marrow. According to the HLH-2004 criteria, the patient was diagnosed with hemophagocytic lymphohistiocytosis. Further analysis of the underlying triggers revealed EBV infection, and there was no evidence of underlying immunodeficiency. Peripheral lymphocytes were sorted by flow cytometry, and quantitative polymerase chain reaction was performed on the sorted cells. The patient was confirmed to have EBV-HLH involving the NK cell lineage. After two cycles of L-DEP chemotherapy, the patient achieved complete remission of HLH. She underwent an HLA-identical sibling allo-HSCT using a VP16 + TBI/Cy conditioning regimen. Graft-versus-host disease (GVHD) prophylaxis included cyclosporine A (CsA), a short course of methotrexate, and mycophenolate mofetil. Both white blood cell (WBC) and platelet (PLT) engraftment occurred 11 days after allo-HSCT. EBV-DNA levels in the patient’s peripheral blood mononuclear cells (PBMCs) and plasma were monitored regularly and remained negative.
The EBV-DNA level in the patient’s PBMCs rose to 5.8×102 copies/mL 43 days after transplantation, whereas the EBV-DNA level in the patient’s plasma remained negative (<5.0×102 copies/mL). To eliminate EBV, the dosage of CsA was gradually tapered. The EBV-DNA level in the patient’s plasma and PBMCs rose to 9.9×102 copies/mL and 4.9×103 copies/mL, respectively, 53 days after transplantation. The patient developed intermittent fever and nausea without superficial lymph node enlargement. Further analysis demonstrated that EBV infection mainly involves the B cell lineage, without evident clonal B cell populations. Rituximab was administered intravenously at a dosage of 375 mg/m2. However, the EBV-DNA levels in PBMCs and plasma continued to rise, and EBV infection mainly involved the NK cell lineage, which indicated recurrence of the primary disease. Chimerism status was monitored regularly using polymerase chain reaction amplification of short tandem repeats, and the patient remained in complete donor chimerism.
The patient’s condition developed rapidly, presenting with high fever, nausea, hepatic insufficiency, cytopenia of two lineages, and elevated levels of ferritin and sCD25, 60 days after the procedure. We administered ruxolitinib (a selective inhibitor of Janus kinase 1 and 2) 10 mg twice daily to control the hyperinflammatory state, followed by donor lymphocyte infusion (DLI) 67 days after transplantation. After DLI, significant improvements in clinical and laboratory manifestations were observed; however, EBV-DNA levels in the patient’s PBMCs and plasma remained positive.
The patient showed signs of HLH recurrence again 81 days after transplantation and received two cycles of the DEP regimen in combination with DLI. However, the patient still experienced another episode of HLH recurrence during chemotherapy. The EBV-DNA level in the patient’s PBMCs was 6.1×103 copies/mL 101 days after transplantation, whereas the EBV-DNA level in the patient’s plasma was 4.3×104 copies/mL. As a last resort, sintilimab (a PD-1 monoclonal antibody; Suchow Xinda Biotechnology Co. Ltd., Suchow, China) was administered intravenously at a dose of 2 mg/kg on day 104. The patient’s fever, cytopenia, elevated liver enzymes, and increased serum ferritin and sCD25 levels returned to normal ranges. EBV-DNA levels in the patient’s PBMCs and plasma tested negative soon after sintilimab injection. An additional cycle of sintilimab was administered intravenously on day 118. The changes in EBV-DNA load throughout the treatment are shown in Figure 1. Changes in WBC and PLT counts and ferritin, sCD25, and alanine aminotransferase levels are shown in Figure 2.
 |
Figure 1 Changes in Epstein–Barr virus-deoxyribonucleic acid load in peripheral blood mononuclear cells and plasma throughout treatment. |
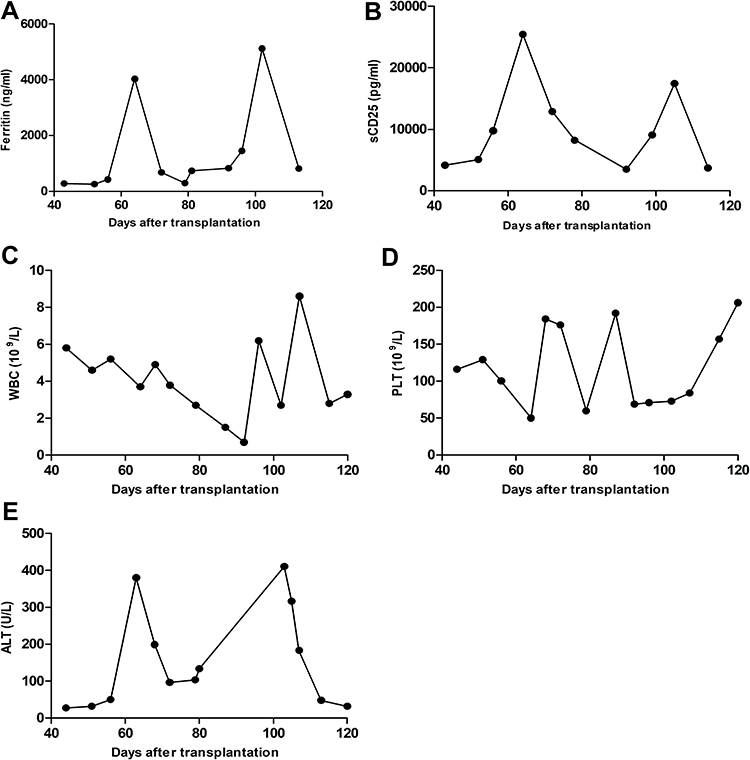 |
Figure 2 Changes in white blood cell and platelet counts and ferritin, soluble CD25, and alanine transaminase levels throughout treatment. (A) Ferritin level; (B) soluble CD25 level; (C) white blood cell count; (D) platelet count; (E) alanine transaminase level. |
The patient experienced occasional skin rashes, gastrointestinal infections, and pneumonia during follow-up, which were all controllable with anti-GVHD and anti-infective drugs. EBV-DNA levels in the PBMCs and plasma were monitored regularly and remained negative. Eight months after transplantation, the patient developed severe pneumonia, and blood culture confirmed Escherichia coli infection. Unfortunately, the patient discontinued treatment for financial reasons and eventually died.
Discussion
EBV is a double-stranded DNA virus that infects more than 90% of the world’s population. EBV cannot be eliminated from the body in cases of immunodeficiency. Active replication of EBV releases antigens that stimulate the immune system, causing excessive production of inflammatory cytokines and overactivation of immunocytes, which eventually leads to HLH.10 It accounts for approximately 70% of infection-related HLH, especially in the Asian population. EBV-HLH is a rare and aggressive disease with a high mortality rate and poor prognosis. Currently, the only way to eliminate EBV infection and improve the long-term survival of EBV-HLH patients is allo-HSCT. According to Gooptu et al,11 allo-HSCT using a reduced intensity regimen in combination with alemtuzumab (anti-CD-52 monoclonal antibody) achieved a favorable 3-year overall survival (OS) rate of 75% in adults with HLH, whereas another retrospective study of 87 adult HLH patients who underwent allo-HSCT revealed 3- and 5-year OS rate in 44% of the patients.12 Relapse of EBV-HLH after allo-HSCT is common and practically irremediable. It has been reported that all relapses are fatal.12
Recent studies have revealed that PD-1 is expressed on the surface of antigen-activated T cells in the setting of tumor or chronic viral infection.13 Interactions between PD-1 and PD-L1 transmit inhibitory signals to activated CD8+ T cells, which eventually leads to T-cell exhaustion. Hence, PD-1 blockade can restore the function of activated CD8+ T cells.14 Currently, PD-1/PD-L1 blockade is being used to treat hematological malignancies. According to recent studies, PD-1 blockade therapy has resulted in an overall response rates of 65.6%–71% in refractory and relapsed Hodgkin lymphoma (HL)15 and could also be a salvage treatment for EBV-positive non-Hodgkin lymphoma, especially for relapsed or refractory NK/T-cell lymphoma. PD-1 blockade has been reported to restore T-cell immune function in EBV-HLH patients.9 Interestingly, PD-1 blockade therapy could also improve the outcome of HL patients relapsing after allo-HSCT with a 1-year OS of 78.7%, and PD-1 blockade-associated GVHD occurred in 30% of all cases and remained responsive to conventional anti-GVHD treatments.16 However, PD-1 blockade was also reported to be associated with an elevated incidence of GVHD.17 Moreover, several secondary HLH cases due to PD-1 inhibition have been documented in patients with solid tumors.18
In this case, the patient relapsed soon after HLA-identical allo-HSCT and none of the conventional treatment options achieved a sustained response. As a last resort, sintilimab (a PD-1 monoclonal antibody) was administered, and EBV-DNA levels in the patient’s PBMCs and plasma rapidly became negative. Further enzyme-linked immunosorbent spot analysis revealed a significant improvement in the donor T cell immune response (Figure 3). As a result, EBV infection in the host was eliminated and hemophagocytic lymphohistiocytosis resolved. However, the efficacy, safety, underlying mechanism, indication, dosage, and timing of PD-1 blockade immunotherapy require further investigation in transplantation settings.
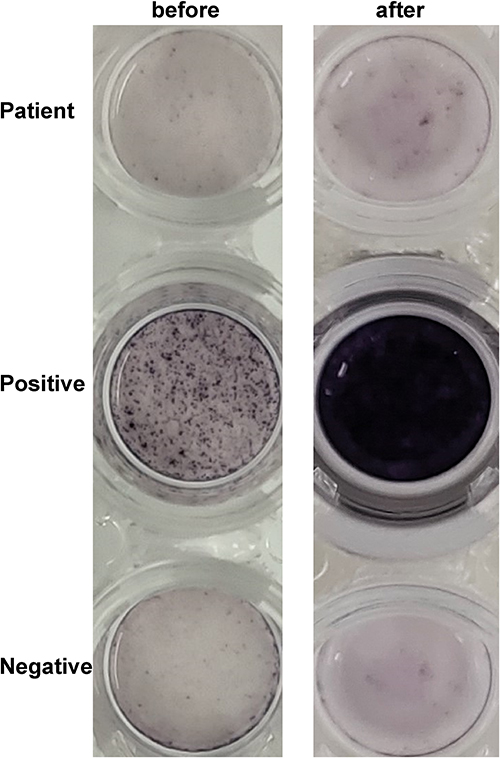 |
Figure 3 Changes in the donor T cell immune response monitored by enzyme-linked immunosorbent spot analysis before and after sintilimab injection. |
In conclusion, we report a case of relapsed EBV-HLH after allo-HSCT that was successfully controlled using PD-1 antibody. However, further studies are needed to determine whether PD-1 blockade has therapeutic potential for relapsed EBV-HLH after allo-HSCT.
Ethics Approval and Informed Consent
This report was approved by the ethics committee of Beijing Friendship Hospital.
The patient provided written informed consent and agreed to the publication of the case.
Acknowledgments
We thank all authors for their contributions to this work.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Maakaroun NR, Moanna A, Jacob JT, Albrecht H. Viral infections associated with haemophagocytic syndrome. Rev Med Virol. 2010;20(2):93–105. doi:10.1002/rmv.638
2. El-Mallawany NK, Curry CV, Allen CE. Haemophagocytic lymphohistiocytosis and Epstein-Barr virus: a complex relationship with diverse origins, expression and outcomes. Br J Haematol. 2022;196(1):31–44. doi:10.1111/bjh.17638
3. Lai W, Wang Y, Wang J, Wu L, Jin Z, Wang Z. Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in adults and adolescents-A life-threatening disease: analysis of 133 cases from a single center. Hematology. 2018;23(10):810–816. doi:10.1080/10245332.2018.1491093
4. Zeng X, Wei N, Wang Y, et al. [Treatment outcomes and prognostic analysis of 61 Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis]. Zhonghua Xue Ye Xue Za Zhi. 2015;36(6):507–510. Chinese. doi:10.3760/cma.j.issn.0253-2727.2015.06.013
5. Henter JI, Samuelsson-Horne A, Aricò M, et al. Treatment of hemophagocytic lymphohistiocytosis with HLH-94 immunochemotherapy and bone marrow transplantation. Blood. 2002;100(7):2367–2373. doi:10.1182/blood-2002-01-0172
6. Henter JI, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.21039
7. Wang J, Wang Y, Wu L, Zhang J, Lai W, Wang Z. PEG-aspargase and DEP regimen combination therapy for refractory Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. J Hematol Oncol. 2016;9(1):84. doi:10.1186/s13045-016-0317-7
8. Wang Y, Huang W, Hu L, et al. Multicenter study of combination DEP regimen as a salvage therapy for adult refractory hemophagocytic lymphohistiocytosis. Blood. 2015;126(19):2186–2192. doi:10.1182/blood-2015-05-644914
9. Liu P, Pan X, Chen C, et al. Nivolumab treatment of relapsed/refractory Epstein-Barr virus–associated hemophagocytic lymphohistiocytosis in adults. Blood. 2020;135(11):826–833. doi:10.1182/blood.2019003886
10. Janka G. Hemophagocytic lymphohistiocytosis: when the immune system runs amok. Klin Padiatr. 2009;221(5):278–285. doi:10.1055/s-0029-1237386
11. Gooptu M, Kim HT, Jacobsen ED, et al. Favorable outcomes following allogeneic transplantation in adults with hemophagocytic lymphohistiocytosis. Blood Adv. 2022. doi:10.1182/bloodadvances.2022007012
12. Machowicz R, Suarez F, Wiktor-Jedrzejczak W, et al. Allogeneic hematopoietic stem cell transplantation for adult HLH: a retrospective study by the chronic malignancies and inborn errors working parties of EBMT. Bone Marrow Transplant. 2022;57(5):817–823. doi:10.1038/s41409-022-01634-5
13. Xu-Monette ZY, Zhang M, Li J, Young KH. PD-1/PD-L1 blockade: have we found the key to unleash the antitumor immune response? Front Immunol. 2017;8(8):1597. doi:10.3389/fimmu.2017.01597
14. Nowicki TS, Hu-Lieskovan S, Ribas A. Mechanisms of resistance to PD-1 and PD-L1 blockade. Cancer J. 2018;24(1):47–53. doi:10.1097/PPO.0000000000000303
15. Kuzume A, Chi S, Yamauchi N, Minami Y. Immune-checkpoint blockade therapy in lymphoma. Int J Mol Sci. 2020;21:15. doi:10.3390/ijms21155456
16. Herbaux C, Gauthier J, Brice P, et al. Efficacy and tolerability of nivolumab after allogeneic transplantation for relapsed Hodgkin lymphoma. Blood. 2017;129(18):2471–2478. doi:10.1182/blood-2016-11-749556
17. Haverkos BM, Abbott D, Hamadani M, et al. PD-1 blockade for relapsed lymphoma post-allogeneic hematopoietic cell transplant: high response rate but frequent GVHD. Blood. 2017;130(2):221–228. doi:10.1182/blood-2017-01-761346
18. Thummalapalli R, Heumann T, Stein J, et al. Hemophagocytic lymphohistiocytosis secondary to PD-1 and IDO inhibition in a patient with refractory glioblastoma. Case Rep Oncol. 2020;13(2):508–514. doi:10.1159/000507281
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.