Back to Journals » Infection and Drug Resistance » Volume 19
Successful Rescue Therapy for Talaromycosis Complicated by Severe Acute Hepatorenal Failure with Hepatic Encephalopathy in an HIV/HCV-Coinfected Patient: A Case Report
Authors Zou J, Qin XY, Zhang MY, Han L ![]() , Jiang ZW, Song JW
, Jiang ZW, Song JW ![]() , Wang FS
, Wang FS
Received 16 March 2026
Accepted for publication 7 June 2026
Published 15 June 2026 Volume 2026:19 605910
DOI https://doi.org/10.2147/IDR.S605910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alberto Ospina Stella
Jun Zou,1,2 Xiao-Ying Qin,2,3 Meng-Yuan Zhang,4 Lin Han,5 Zhi-Wen Jiang,3 Jin-Wen Song,4,5 Fu-Sheng Wang1,5
1Department of Infectious Disease, Beijing Ditan Hospital Capital Medical University, Beijing, People’s Republic of China; 2Department of Infectious Disease, The Fourth People’s Hospital of Nanning, Nanning, People’s Republic of China; 3Guangxi Medical University, Nanning, People’s Republic of China; 4The Second School of Clinical Medicine, Southern Medical University, Guangzhou, People’s Republic of China; 5Senior Department of Infectious Diseases, the Fifth Medical Center of Chinese PLA General Hospital, National Clinical Research Center for Infectious Diseases, Beijing, People’s Republic of China
Correspondence: Jin-Wen Song, Senior Department of Infectious Diseases, the Fifth Medical Center of Chinese PLA General Hospital, National Clinical Research Center for Infectious Diseases, Beijing, People’s Republic of China, Email [email protected] Fu-Sheng Wang, Department of Infectious Disease, Beijing Ditan Hospital Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Background: Treatment of critically ill patients with Talaromyces marneffei (T. marneffei, TM) infection involving multiple organ dysfunction remains a major clinical challenge. As an important contributor to mortality among individuals with Acquired Immunodeficiency Syndrome (AIDS), talaromycosis remains associated with mortality rates of up to 30% even with appropriate antifungal therapy. Severe hepatic and renal impairment may restrict antifungal dosing and thus further compromise therapeutic efficacy. However, current clinical evidence regarding the management of Talaromyces marneffei infection complicated by hepatic encephalopathy and acute renal failure remains limited.
Case Presentation: A 39-year-old female with a newly identified hepatitis C virus (HCV) infection and newly diagnosed Human Immunodeficiency Virus (HIV) infection was admitted to our hospital because of recurrent fever and abdominal pain. Abdominal ultrasound revealed hepatosplenomegaly, while chest and abdominal computed tomography scan showed bilateral pulmonary nodular lesions, multiple enlarged intra-abdominal and retroperitoneal lymph nodes, and splenomegaly. On the second day after admission, quantitative real-time polymerase chain reaction analysis of blood detected a T. marneffei load of 1.7 × 106 copies/mL, and disseminated talaromycosis was subsequently confirmed by blood culture. The patient therefore started on antifungal treatment with liposomal amphotericin B (L-AmB) at 3 mg/kg per day. Shortly after treatment initiation, she developed hepatic encephalopathy and acute renal failure and was transferred to the intensive care unit for further management. With the artificial liver support therapy and continuous renal replacement therapy (CRRT), full-dose L-AmB was maintained, allowing the patient to successfully completed the induction therapy with L-AmB. Her liver and renal function ultimately normalized, and the patient remained clinically stable with no evidence of T. marneffei recurrence at the one-year follow-up.
Conclusion: Early recognition of hepatorenal failure and timely initiation of CRRT combined with artificial liver support within 24 hours are essential for maintaining the antifungal effect of full-dose L-AmB.
Keywords: HIV/HCV/TM, hepatic encephalopathy, acute liver failure, liposomal amphotericin B, continuous renal replacement therapy, artificial liver support
Background
Talaromycosis is an invasive fungal disease caused by Talaromyces marneffei (T. marneffei, TM), the only thermally dimorphic fungus within the genus Penicillium. It is endemic throughout Southeast and South Asia, including southern China, northern Thailand, Malaysia, and Vietnam.1 The disease predominantly affects individuals with advanced Acquired Immunodeficiency Syndrome (AIDS) or an immunocompromised status.2–5 Typical clinical manifestations include fever, respiratory and gastrointestinal symptoms, hepatosplenomegaly, superficial lymphadenopathy, and characteristic umbilicated papules. Laboratory evaluation shows cytopenias and radiological evidence of pulmonary lesions.6–9 Although effective antifungal therapy can significantly reduce the risk of mortality, liver and kidney impairment can complicate antifungal administration.10 Elevated transaminases and renal impairment (e.g., an elevated urea-to-albumin ratio) have been identified as independent predictors of mortality.11–13 Severe hepatic or renal impairment may restrict antifungal dosing and thereby compromise treatment efficacy.14,15 Liver function impairment is common in T. marneffei infection; however, rapid deterioration leading to hepatic failure is rare.16,17 Currently, no clear guidelines exist regarding antifungal selection for patients with hepatic or renal failure, particularly those with hepatic encephalopathy.18 Herein, we reported the first case of successful treatment of disseminated T. marneffei infection in a patient with HIV/HCV coinfection complicated by severe hepatic and renal dysfunction and hepatic encephalopathy.
Case Description
A 39-year-old female living in Guangxi, China, was admitted to the Fourth People’s Hospital of Nanning on May 12, 2024, with recurrent fever and abdominal pain. The patient initially presented recurrent fever, followed by jaundice, progressive abdominal pain, and diarrhea. She had a history of intravenous drug use and had not received treatment for HCV infection. Abdominal computed tomography (CT) at the local hospital revealed multiple enlarged intraperitoneal and retroperitoneal lymph nodes and splenomegaly. She was diagnosed locally with AIDS, bacterial pneumonia and suspected of an invasive fungal infection. Meropenem and itraconazole were initiated, leading to the resolution of fever; however, abdominal symptoms persisted and oliguria developed. Given that she was HIV positive and suspected of having T. marneffei infection, she was transferred to our tertiary infectious disease center for further management. Physical examination showed marked jaundice, absence of palmar erythema and spider nevi, and mild abdomen distension with periumbilical tenderness. Suboptimal patient cooperation precludes a detailed palpation of the liver and spleen.
Laboratory investigations at admission showed markedly elevated white blood cell (WBC) count and C-reactive protein (CRP) levels, mild anemia, thrombocytopenia, and elevated creatinine and transaminase levels. The CD4+ T-lymphocyte count was 64 cells/μL and the HCV RNA load was 2.03 × 107 IU/mL (Table 1). Abdominal ultrasound confirmed hepatosplenomegaly. Chest-abdominal CT showed bilateral pulmonary nodular and multiple enlarged abdominal and retroperitoneal lymph nodes. Blood qPCR detected T. marneffei (1.7 × 106 copies/mL) on hospital day 2 (Figure 1B).
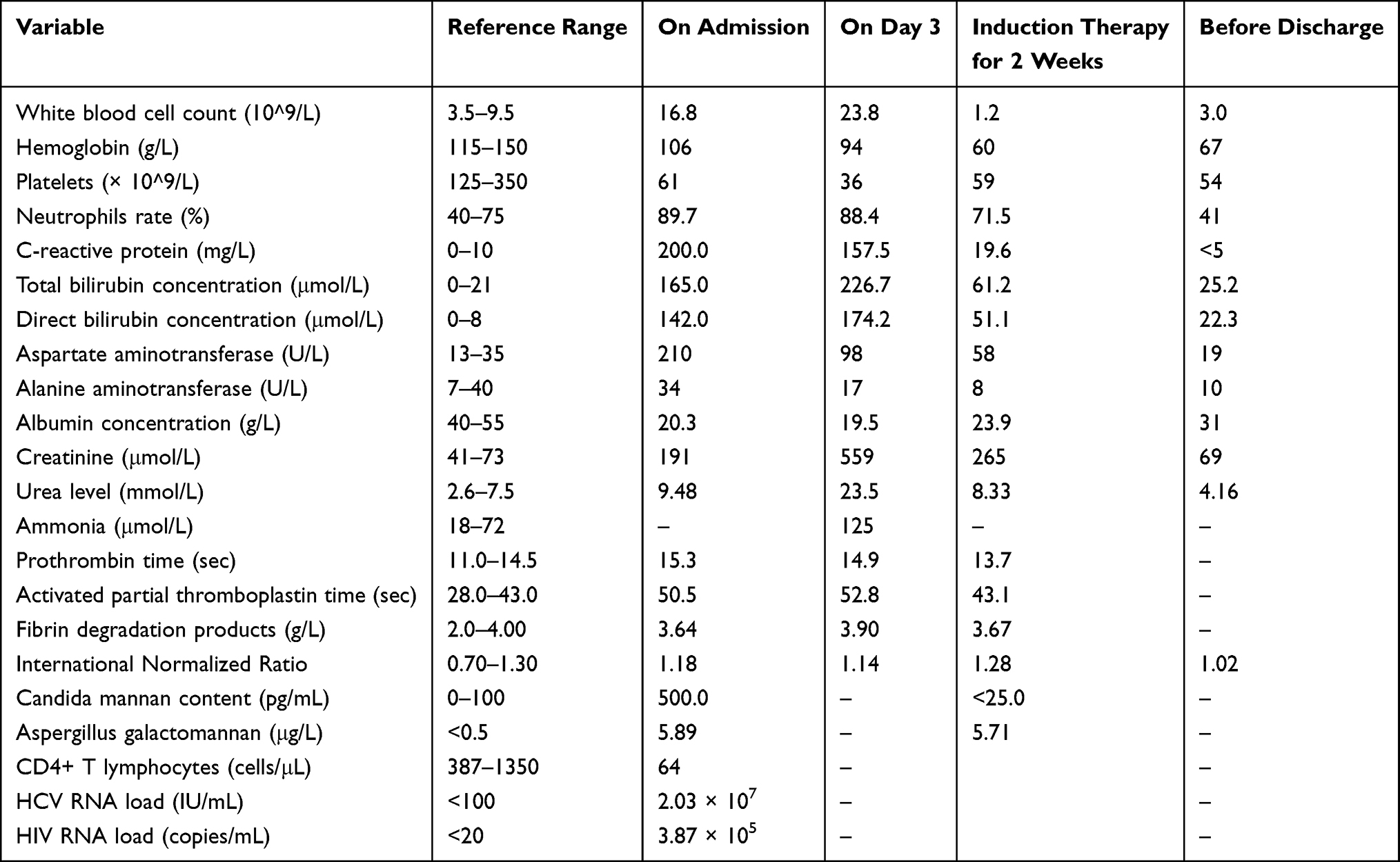 |
Table 1 Laboratory Findings |
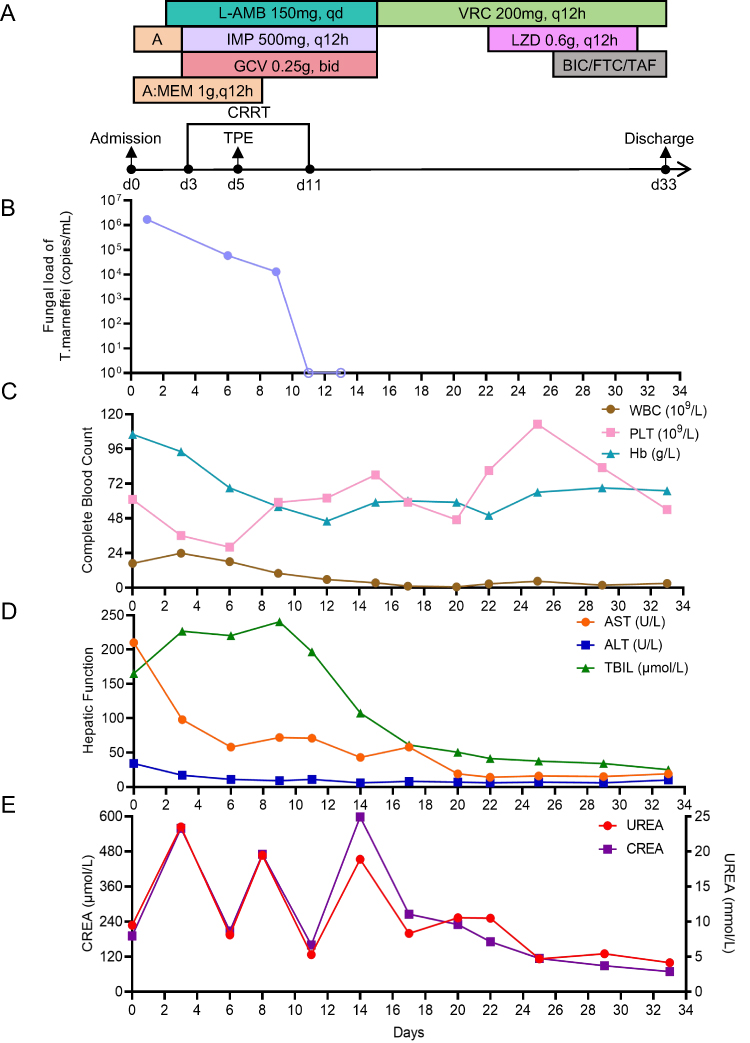 |
Figure 1 (A) Timeline of therapeutic interventions administered during hospitalization. Longitudinal dynamic of (B) T. marneffei fungal load, (C) complete blood counts, (D) liver function biomarkers, and (E) renal function indicators (creatine and urea). |
On admission, the patient was immediately empirically administered with liposomal amphotericin B (L-AmB, 3 mg/kg/day), meropenem (1 g q12h). The patient developed marked anuria (<30 mL/24h). By day 3, she developed worsening progressive disorientation, flapping tremor, and drowsiness, abdominal and back pain, severe fatigue, and nausea. Non-contrast cranial CT demonstrated no abnormal findings. These findings were consistent with acute-on-chronic liver failure-1 (ACLF-1), grade 2 hepatic encephalopathy. Repeated Laboratory tests showed worsening leukocytosis, progressive thrombocytopenia, elevated bilirubin, rising creatinine (559 μmol/L), urea (23.5 mmol/L), and hyperammonemia (125 μmol/L) (Table 1). NGS detected T. marneffei on hospital day 3 and blood culture confirmed T. marneffei infection on hospital day 6. The dynamics of laboratory indicators are shown in Figure 1C–E.
Therefore, the patient was diagnosed with disseminated talaromycosis complicated by stage 3 acute kidney injury and ACLF-1, grade 2 hepatic encephalopathy. High-flow noninvasive ventilation was initiated, antibacterial therapy was switched to imipenem‒cilastatin sodium (500 mg q12h), with full-dose L-AmB (3 mg/kg/day) continued throughout the treatment course, and voriconazole (200 mg bid) was added after 2 weeks of the original L-AmB regimen. Continuous renal replacement therapy (CRRT) combined with artificial liver plasma exchange therapy was administered, along with supportive care (Figure 1A). The patient achieved clinical stability and was discharged with a prescription for oral itraconazole (200 mg twice daily) for 10 weeks and bictegravir/emtricitabine/tenofovir alafenamide. She remained clinically stable without recurrence of T. marneffei infection during one year of follow up.
Discussion
According to the current guidelines, amphotericin B is the first-line treatment for systemic T. marneffei infections.19 However, amphotericin B deoxycholate (C-AmB) is associated with a wide range of adverse effects, including dose-dependent nephrotoxicity, acute infusion-related reactions, and electrolyte disturbances e.g., hypokalemia). These limitations have restricted its clinical application.14 We reported a case of HIV/HCV/TM complicated by stage 3 acute kidney injury, ACLF-1 and grade 2 hepatic encephalopathy and acute renal failure that was successfully managed with L-AmB combined with adjuvant therapy of artificial liver support system and CRRT. In the treatment of hepatorenal failure induced by severe infection, artificial liver support and CRRT serve as key measures to protect vital organs;20,21 however, the overall survival rate remains unsatisfactorily low. For instance, patients with liver failure complicated by hepatorenal syndrome present a considerably high mortality rate.22 In 2023, Liang Xu et al reported a renal transplant patient complicated with T. marneffei infection. Despite severe hepatorenal injury occurring during treatment, the patient recovered and was discharged after antifungal therapy with voriconazole and amphotericin B.23 In 2024, Shanshan Yang et al reported an HIV-negative patient infected with T. marneffei after renal transplantation. The patient still developed multiple organ dysfunction syndrome and hepatic encephalopathy despite amphotericin B deoxycholate antifungal treatment and died after treatment withdrawal.24 Although there is some experience with the use of L-AmB in patients undergoing CRRT treatment,25–27 its use in a patient with HIV/HCV/TM coinfection complicated by hepatic encephalopathy and acute renal failure has rarely been documented. L-AmB exhibits lower hepatic and renal toxicity, which ensures the efficacy and timeliness of antifungal therapy and ultimately contributes to a successful clinical outcome.
T. marneffei infection mainly involves the skin, lungs, liver, spleen, lymph nodes, and circulatory system.6 Central nervous system (CNS) involvement is rare but may cause meningitis or parenchymal lesions, leading to altered consciousness.28 When the CNS is involved, the disease progresses rapidly with an extremely high case fatality rate: most patients succumb within 10 days, and the overall case fatality rate stands at 81%.29 Even with appropriate antifungal therapy, the mortality rate in this population remains about 30%.30 Delayed antifungal therapy further compromises clinical outcomes.31 Furthermore, coinfection with viral hepatitis is associated with severe liver injury in people living with HIV.32 Both HIV and HCV can directly damage brain tissue through neurotoxicity and inflammation, which increases the risk of neurocognitive impairment or hepatic encephalopathy.33 Although the lumbar puncture was rejected, CNS invasion by T. marneffei could not be excluded. Many risk factors for death have been reported in patients with talaromycosis. Multiple studies have shown that elevated bilirubin, increased AST/ALT levels, decreased endogenous creatinine clearance rate, and low hemoglobin levels are associated with higher mortality in patients with HIV/TM coinfection. Factors related to renal impairment and liver dysfunction serve as independent prognostic risk factors.34,35 Generally, in cases of severe hepatic and renal impairment, consideration should be given to dose reduction, treatment interruption, or discontinuation in clinical practice.14 Given the benefit of rapidly controlling invasive fungi infection outweighed the risk of drug-induced liver injury, full-dose L-AmB was administered. The patient achieved rapid clinical remission, and hepatic and renal functions ultimately returned to normal. Therefore, aggressive antifungal treatment remains essential, even in the setting of hepatic and renal impairment. Antifungal therapy interruption or dose reduction due to concerns about potential drug toxicity should be avoided, as this may compromise therapeutic efficacy and result in poor prognosis.
Furthermore, active use of an artificial liver support system plays a vital role in the management of patients with liver failure, particularly in those with hepatic encephalopathy. Severe infection and liver failure can cause renal vasoconstriction and reduced renal perfusion, leading to acute kidney injury.36–38 After the patient developed oliguria and subsequent severe infection, rapid hepatic and renal failure occurred. With the support of artificial liver support system and CRRT, the patient was able to receive adequate and continuous L-AmB therapy for antifungal treatment, which successfully controlled the fungal infection and restored hepatic and renal function. For patients with sepsis-associated acute kidney injury, CRRT intervention within 12–24 hours can improve survival rate, shorten hospital stay and increase the recovery rate of renal function.20,39 Meanwhile, artificial liver therapy (plasma exchange) can eliminate infection-related inflammatory mediators and alleviate persistent multi-organ damage caused by systemic inflammatory response.21,40 This outcome highlights the indispensable role of supportive therapies such as artificial liver support system and CRRT in managing organ failure. Meanwhile, it also underscores the paramount importance of early identification and intervention for hepatic encephalopathy.
To our knowledge, this is the first reported case of advanced HIV-associated T. marneffei disease complicated by HCV coinfection, in which the patient developed hepatic encephalopathy and acute renal failure but was successfully treated with L-AmB. This case provides valuable reference experience for the clinical management of HIV/HCV/TM patients presenting with severe complications such as hepatorenal failure and hepatic encephalopathy. Timely initiation of CRRT within 12–24 hours after the onset of oliguria/anuria can protect vital organs and create a therapeutic window for antifungal treatment. This strategy is critical for the safe administration of full-dose L-AmB and the ultimate successful control of fungal infection.
This case demonstrates that L-AmB has excellent pharmacological properties and serves as a viable therapeutic option for critically ill patients with HIV/TM co-infection complicated by hepatorenal failure. Early recognition of life-threatening complications and immediate initiation of CRRT combined with artificial liver support therapy within 24 hours is an effective measure to protect vital organs. Furthermore, dosage adjustment of L-AmB is unnecessary during CRRT, and its full-dose fungicidal effect is pivotal to rapid clinical recovery. Therefore, for patients with multiple risk factors presenting HIV/TM/HCV co-infection and concurrent hepatorenal failure, timely intervention with CRRT combined with artificial liver support should be administered, alongside antifungal therapy with L-AmB.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Statements and Informed Consent
This work was already approved by the Institutional Ethics Review Board of the Fourth People’s Hospital of Nanning ([2026]04). Written informed consent was obtained from the patient for the publication of this case report. Institutional approval from Institutional Ethics Review Board of the Fourth People’s Hospital of Nanning was required to publish the case details and was obtained.
Acknowledgments
We are grateful to the patient and the medical staff involved in the management of this patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Natural Science Foundation of China (82360623). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Vanittanakom N, Cooper CR, Fisher MC, Sirisanthana T. Penicillium marneffei infection and recent advances in the epidemiology and molecular biology aspects. Clin Microbiol Rev. 2006;19(1):95–7. doi:10.1128/CMR.19.1.95-110.2006
2. Wong SY, Wong KF. Penicillium marneffei Infection in AIDS. Patholog Res Int. 2011;2011:764293.
3. Höflich C, Sabat R, Rosseau S, et al. Naturally occurring anti-IFN-gamma autoantibody and severe infections with Mycobacterium cheloneae and Burkholderia cocovenenans. Blood. 2004;103(2):673–675. doi:10.1182/blood-2003-04-1065
4. Döffinger R, Helbert MR, Barcenas-Morales G, et al. Autoantibodies to interferon-gamma in a patient with selective susceptibility to mycobacterial infection and organ-specific autoimmunity. Clin Infect Dis. 2004;38(1):e10–4. doi:10.1086/380453
5. Wang F, Han R, Chen S. An overlooked and underrated endemic mycosis-talaromycosis and the pathogenic Fungus Talaromyces marneffei. Clin Microbiol Rev. 2023;36(1):e0005122. doi:10.1128/cmr.00051-22
6. Cao C, Xi L, Chaturvedi V. Talaromycosis (Penicilliosis) due to talaromyces (Penicillium) marneffei: insights into the clinical trends of a major fungal disease 60 years after the discovery of the pathogen. Mycopathologia. 2019;184(6):709–720. doi:10.1007/s11046-019-00410-2
7. Du Q, Tong CK. Talaromyces (Penicillium) marneffei infection. IDCases. 2018;13:e00428. doi:10.1016/j.idcr.2018.e00428
8. Supparatpinyo K, Khamwan C, Baosoung V, Nelson KE, Sirisanthana T. Disseminated Penicillium marneffei infection in Southeast Asia. Lancet. 1994;344(8915):110–113. doi:10.1016/S0140-6736(94)91287-4
9. Le T, Wolbers M, Chi NH, et al. Epidemiology, seasonality, and predictors of outcome of AIDS-associated Penicillium marneffei infection in Ho Chi Minh City, Viet Nam. Clin Infect Dis. 2011;52(7):945–952. doi:10.1093/cid/cir028
10. Weng Z, Lin Y, Dai W, et al. Clinical characteristics and prognosis of AIDS complicated with Talaromycosis marneffei infection: a single-center retrospective study. Infect Dis Ther. 2025;14(8):1935–1952. doi:10.1007/s40121-025-01198-z
11. Zhang Y, Gu K, Du W, Xu A. Risk factors and prediction model for mortality in HIV/Talaromyces marneffei co-infection: a retrospective cohort study. Heliyon. 2024;10(11):e32560. doi:10.1016/j.heliyon.2024.e32560
12. Wei F. Clinical Characteristics and Risk Factors in the Classification and Prognosis Evaluation of Talaromycosis: A Large Multicenter Retrospective Cohort Study. Guangxi Medical University; 2021.
13. Ying RS, Le T, Cai WP, et al. Clinical epidemiology and outcome of HIV-associated talaromycosis in Guangdong, China, during 2011-2017. HIV Med. 2020;21(11):729–738. doi:10.1111/hiv.13024
14. Hamill RJ. Amphotericin B formulations: a comparative review of efficacy and toxicity. Drugs. 2013;73(9):919–934. doi:10.1007/s40265-013-0069-4
15. Inselmann G, Inselmann U, Heidemann HT. Amphotericin B and liver function. Eur J Intern Med. 2002;13(5):288–292. doi:10.1016/S0953-6205(02)00065-1
16. Zaongo SD, Zhang F, Chen Y. An overview of diagnostic and management strategies for talaromycosis, an underrated disease. J Fungi. 2023;9(6):647. doi:10.3390/jof9060647
17. Yao Z, Pan Z, Li G, et al. Talaromycosis from Wuhan: two-case report and literature review. Front Cell Infect Microbiol. 2024;14:1347677. doi:10.3389/fcimb.2024.1347677
18. Thompson GR 3rd, Le T, Chindamporn A, et al. Global guideline for the diagnosis and management of the endemic mycoses: an initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology. Lancet Infect Dis. 2021;21(12):e364–e374. doi:10.1016/S1473-3099(21)00191-2
19. Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, Masur H. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the national institutes of health, and the HIV medicine association of the infectious diseases society of America. MMWR Recomm Rep. 2009;58(Rr–4):1–207; quizCE1–4.
20. Romagnoli S, Ricci Z, Ronco C. CRRT for sepsis-induced acute kidney injury. Current Opinion Crit Care. 2018;24(6):483–492. doi:10.1097/MCC.0000000000000544
21. Saliba F, Bañares R, Larsen FS, et al. Artificial liver support in patients with liver failure: a modified DELPHI consensus of international experts. Intensive Care Med. 2022;48(10):1352–1367. doi:10.1007/s00134-022-06802-1
22. Jung CY, Chang JW. Hepatorenal syndrome: current concepts and future perspectives. Clin Mol Hepatol. 2023;29(4):891–908. doi:10.3350/cmh.2023.0024
23. Xu L, Chen X, Yang X, et al. Disseminated Talaromyces marneffei infection after renal transplantation: a case report and literature review. Front Cell Infect Microbiol. 2023;13:1115268. doi:10.3389/fcimb.2023.1115268
24. Yang S, Lou L, Ma S, et al. Disseminated Talaromyces marneffei infection initially presenting as cutaneous and subcutaneous lesion in an HIV-Negative renal transplant recipient: a case report and literature review. BMC Infect Dis. 2024;24(1):473. doi:10.1186/s12879-024-09351-8
25. Yu H, Luo ZK, Lu TT, et al. Diagnosis and treatment of Aspergillus terreus and Klebsiella pneumoniae coinfection following myocardial infarction: a case report and literature review. IDCases. 2025;41:e02301. doi:10.1016/j.idcr.2025.e02301
26. Li L, Li X, Xia Y, et al. Recommendation of antimicrobial dosing optimization during continuous renal replacement therapy. Front Pharmacol. 2020;11:786. doi:10.3389/fphar.2020.00786
27. Bellmann R, Egger P, Gritsch W, et al. Amphotericin B lipid formulations in critically ill patients on continuous veno-venous haemofiltration. J Antimicrob Chemother. 2003;51(3):671–681. doi:10.1093/jac/dkg139
28. Li YY, Dong RJ, Shrestha S, et al. AIDS-associated Talaromyces marneffei central nervous system infection in patients of southwestern China. AIDS Res Ther. 2020;17(1):26. doi:10.1186/s12981-020-00281-4
29. Le T, Chi NH, Ngo TKC, et al. AIDS-Associated Penicillium marneffei Infection of the central nervous system. Clin Infect Dis. 2010;51(12):1458–1462. doi:10.1086/657400
30. Le T, Kinh NV, Cuc NTK, et al; I.Investigators. A trial of itraconazole or amphotericin B for HIV-associated talaromycosis. N Engl J Med. 2017;376(24):2329–2340. doi:10.1056/NEJMoa1613306
31. Supparatpinyo K, Nelson KE, Merz WG, et al. Response to antifungal therapy by human immunodeficiency virus-infected patients with disseminated Penicillium marneffei infections and in vitro susceptibilities of isolates from clinical specimens. Antimicrob Agents Chemother. 1993;37(11):2407–2411. doi:10.1128/AAC.37.11.2407
32. Liu S, Zhou Y, Wang Y, et al. The correlated risk factors for severe liver damage among HIV-positive inpatients with abnormal liver tests. Front Med Lausanne. 2022;9:817370. doi:10.3389/fmed.2022.817370
33. Forton DM, Allsop JM, Main J, Foster GR, Thomas HC, Taylor-Robinson SD. Evidence for a cerebral effect of the hepatitis C virus. Lancet. 2001;358(9275):38–39. doi:10.1016/S0140-6736(00)05270-3
34. Qin Y, Zhou Y, Lu Y, et al. Multicentre derivation and validation of a prognostic scoring system for mortality assessment in HIV-infected patients with talaromycosis. Mycoses. 2021;64(2):203–211. doi:10.1111/myc.13206
35. Cen J, Huang J, Zeng W, Pan M, Qiu Y, Zhang J. Clinical features of HIV positive talaromycosis marneffei patients and development of a risk prediction model. Heliyon. 2023;9(9):e20068. doi:10.1016/j.heliyon.2023.e20068
36. Chen JJ, Lai PC, Lee TH, Huang YT. Blood purification for adult patients with severe infection or sepsis/septic shock: a network meta-analysis of randomized controlled trials. Crit Care Med. 2023;51(12):1777–1789. doi:10.1097/CCM.0000000000005991
37. Shimizu A, Ishii E, Masuda Y, et al. Renal inflammatory changes in acute hepatic failure-associated acute kidney injury. Am J Nephrol. 2013;37(4):378–388. doi:10.1159/000348567
38. Maiwall R, Singh SP, Angeli P, et al. APASL clinical practice guidelines on the management of acute kidney injury in acute-on-chronic liver failure. Hepatol Int. 2024;18(3):833–869. doi:10.1007/s12072-024-10650-0
39. Karkar A, Ronco C. Prescription of CRRT: a pathway to optimize therapy. Ann Intens Care. 2020;10(1):32. doi:10.1186/s13613-020-0648-y
40. Dong V, Karvellas CJ. Liver assistive devices in acute liver failure: current use and future directions, Best practice & research. Clin Gastroenterol. 2024;73:101964. doi:10.1016/j.bpg.2024.101964
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.