")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 13
Successful Control of Hypoglycemia with Pasireotide LAR in a Patient with Inappropriate Insulin Secretion
Authors Rouland A , Bouillet B , Legris P, Simoneau I , Petit JM, Vergès B
Received 28 August 2020
Accepted for publication 26 November 2020
Published 5 February 2021 Volume 2021:13 Pages 33—37
DOI https://doi.org/10.2147/CPAA.S278978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Arthur E. Frankel
Alexia Rouland,1 Benjamin Bouillet,1,2 Pauline Legris,1 Isabelle Simoneau,2 Jean-Michel Petit,1,2 Bruno Vergès1,2
1Endocrinology Diabetics and Metabolic Disorders Department, Dijon University Hospital, Dijon, France; 2French National Health and Medical Research Body Unit, Lipid-Nutrition-Cancer-1231, University of Burgundy, Dijon, 21000, France
Correspondence: Alexia Rouland
Endocrinology Diabetics and Metabolic Disorders Department, Dijon University Hospital, 14 Rue Paul Gaffarel, Dijon, 21000, France
Email [email protected]
Introduction: Inappropriate insulin secretion could be due to several diseases. Nesidioblastosis is characterized by diffuse hyperplasia of pancreatic beta cells, causing organic hypoglycemia. No pancreatic lesions are found on the imaging of patients with this condition. Diazoxide is used as a first-line treatment but can be poorly tolerated because of its side effects, and therapeutic failure is possible. Somatostatin analogues have limited efficacy because of their poor affinity to somatostatin (SST) receptors. Pasireotide is a somatostatin analogue with a much higher affinity to SST receptors, especially SST5, and it could thus be more efficient for treating nesidioblastosis-related hypoglycemia.
Observation: A 56 years-old diabetic woman had symptoms of hypoglycemia, persistent after treatment’s withdrawal. A fasting test authentify an organic hypoglycemia, at 34mg/dL, a plasma insulin level at 6mUI/L above the 5 mU/L threshold, a C-peptide level at 1.9 ng/mL above the threshold of 0.6, and an insulin/C-peptide ratio 0.066, below the threshold of 1. No lesions were found on CT-scan or endoscopic ultrasound. Somatostatin receptor scintigraphy was also negative. Diazoxide and octreotide failed to improve the recurrence of hypoglycemia episodes. With pasireotide LAR, hypoglycemia disappeared and glycemia increased. Hyperglycemia was controlled with sitagliptin. The patient has now been treated with pasireotide LAR for two years, with no more episode of hypoglycemia until now.
Discussion: We present the first case of nesidioblastosis treatment with pasireotide LAR, with success. Patients diagnosed with nesidioblastosis and diazoxide-resistant hypoglycemia, or who experience difficulties with other treatments, could use pasireotide LAR in conjunction with glycemia monitoring, particularly if they are diabetic.
Keywords: nesidioblastosis, hypoglycemia, pasireotide LAR, diazoxide
Introduction
Hyperinsulinism can have several causes. Nesidioblastosis is a rare cause of hypoglycemia in adults that is characterized by diffuse hyperplasia of pancreatic beta cells.1 Clinical signs are similar to insulinoma, with hypoglycemia, especially during fasting. A 72 hours fasting test can be performed to confirm the presence of hypoglycemia with inadequate insulin and C-peptide secretion. Contrary to insulinoma, no pancreatic lesions are found with endoscopic ultrasound or other imaging techniques. Nesiodioblastosis can occur after bariatric surgery, especially after Roux-en-Y gastric by-pass, maybe because of an increase of post-operative GLP-1 secretion which can promote pancreatic beta cells hyperplasia.2
Treatment of inappropriate insulin secretion is not always simple. It is based firstly on dietary measures and on treatment with diazoxide. However, diazoxide can have poorly supported side effects, and therapeutic failure occurs in some cases. Somatostatin analogues (octreotide, lanreotide) can be used as a second-line treatment, even if their efficacy is limited because of their poor affinity to somatostatin (SST) receptors. Pasireotide is a somatostatin analogue with a much higher affinity to SST receptors, especially SST5, and is used mainly to treat Cushing’s disease and acromegaly. Pasireotide is also often responsible for the appearance or aggravation of diabetes, by lowering insulin secretion.3
Long-acting release pasireotide, pasireotide LAR, has been used successfully in two cases of malignant insulinoma.4,5 We report, for the first time, a patient with isolated nesidioblastosis who was successfully treated with pasireotide LAR.
Case Report
A 56-year-old woman with a 2-year history of type 2 diabetes, treated with gliclazide 30 mg/d, presented with HbA1c at 6% and she described recent frequent hypoglycemic episodes. This led to the replacement of gliclazide by sitagliptin. However, hypoglycemic episodes continued during the 4 following months and their frequency increased, so sitagliptin was discontinued. At that time, HbA1c was at 5.7% (39mmol/mol). During the six following months, she continued to have very frequent hypoglycemic episodes that could occur at any time of day, and she had a total weight gain of 20 kg. In order to detect a possible organic cause of hypoglycemia, a 72 h fasting test was performed. The results showed, during hypoglycemia at 34 mg/dl (1.88mmol/L), a plasma insulin level 6mUI/L above the 3 mU/L threshold, C-peptide at 1.9 ng/mL above the 0.6 threshold, and an insulin/C-peptide ratio at 0.066, below the threshold of 1, which are all indicators of organic pancreatic hypoglycemia.6,7 Plasma pro-insulin levels were ranging between 3.72 and 4.5 pmol/L (normal ranges: 1.28–3.84). There was no kidney or liver failure. Cortisol was at 19µg/dL. No sulfonylureas were found in her blood during hypoglycemia. Anti-insulin antibodies were at 3% (<8). No pancreatic lesion was found on the abdominal CT scan or on several endoscopic ultrasounds, which were performed by experienced gastroenterologists. The somatostatin-receptor scintigraphy (Octreoscan®) was also negative. Insulinoma was therefore ruled out.
A treatment with diazoxide was started at an initial dose of 100 mg/d and increased up to 600 mg/d over the 9 following months after the patient’s consent has been obtained. Because the hypoglycemic episodes were persistent, the dose was uptitrated to 800 mg/d then to 900 mg/d, 9 months later. Despite, the high dose treatment with diazoxide, the patient experienced frequent episodes of hypoglycemia with elevated plasma insulin levels. For instance, during a hypoglycemic episode at 42 mg/L (2.33 mmol/L), plasma insulin level was at 17mUI/L, C-peptide at 4.4ng/mL, and pro-insulin at 10.87 pmol/L. Another endoscopic ultrasound did not find any pancreatic lesion.
Because of the persistent hypoglycemic episodes, the care team decided to initiate another treatment in addition to diazoxide. Long-acting octreotide at an initial dose of 20 mg every 4 weeks was uptitrated 6 months later to 30 mg every 4 weeks. Five months after the first uptitration of octreotide, the patient was still experiencing frequent hypoglycemic episodes with elevated plasma insulin levels. For instance, during a hypoglycemic event at 52 mg/dl (2.88 mmol/L), the patient’s plasma insulin level was 12mUI/L and C-peptide was 2.8ng/mL. Octreotide was therefore replaced by pasireotide LAR at a dose of 40 mg every 4 weeks, and the treatment with diazoxide was maintained (Figure 1). Very rapidly, the hypoglycemic events disappeared and glycemia increased, diazoxide was thus reduced to 600 mg/day and then discontinued 7 months later. At that time, because of high fasting blood glucose, ranging from 275 to 350 mg/dL (15.30 to 19.42 mmol/L) and an elevated HbA1c level of 8.8% (73mmol/mol), pasireotide LAR treatment was interrupted and an antidiabetic treatment with sitagliptin was introduced. The patient was hospitalized 2 months later for recurrent hypoglycemic episodes. Pasireotide LAR was reintroduced, 20 mg every 4 weeks, and sitagliptin treatment was maintained. Very shortly after reintroduction of pasireotide LAR, the hypoglycemic episodes disappeared. Twelve months later, because HbA1c was 7.5% (58mmol/mol), pasireotide LAR dose was downtitrated to 10 mg every 6 weeks (Figure 1). This patient has now been treated for 2 years with pasireotide LAR, with no recurrent hypoglycemia episodes, and her diabetes is well controlled with sitagliptin. We used continuous glucose monitoring recording recently to find out whether the patient presented asymptomatic hypoglycemias (Figure 2). No hypoglycemia was found on this record.
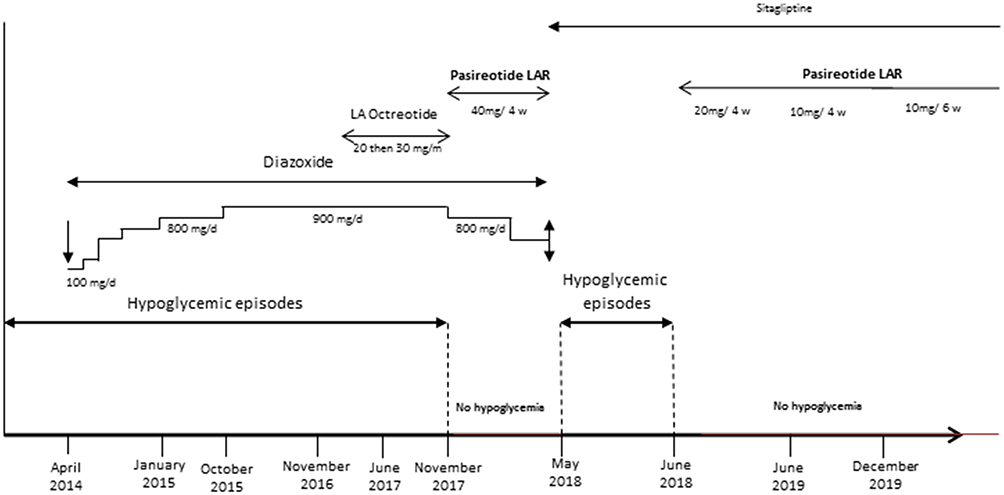 |
Figure 1 Treatments and recurrence of hypoglycemia over time. |
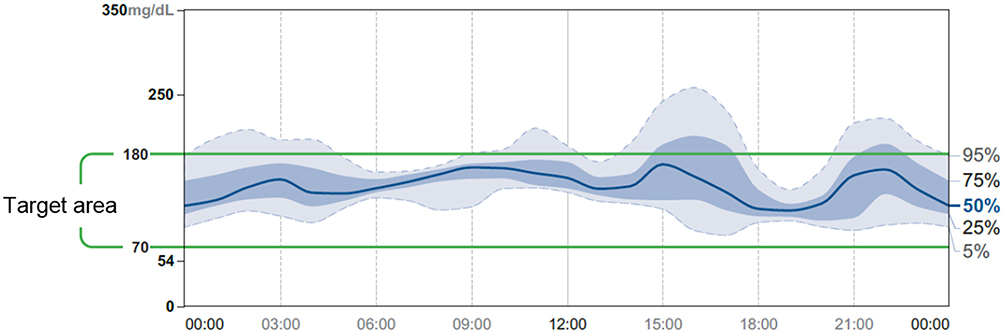 |
Figure 2 Glycemia during treatment with Pasireotide LAR. |
Discussion
We present here the first case of hyperinsulinism successfully treated with pasireotide LAR after failure of treatment with diazoxide and octreotide. In this patient, pasireotide LAR treatment completely resolved the patient’s hypoglycemia episodes since no glycemic episodes have occurred since the introduction of the treatment, 2 years ago.
Pasireotide is a somatostatin analogue with a strong affinity for SST 1, 2, 3, and 5 receptors. Its affinity for SST 5 receptor especially is 39 fold higher than the affinity of octreotide. The somatostatin receptor subtype 5 (SST5) is more expressed in pancreatic β cells (87%) than in pancreatic β cells (44%) whereas the somatostatin receptor subtype 2 (SST2) is more expressed in pancreatic β cells (89%) than in pancreatic β cells (44%).8,9 Because pasireotide binds to both SST2 and SST5 receptors with the highest affinity to SST5, it induces a much more pronounced decrease in insulin secretion than in glucagon secretion.3 The high affinity of pasireotide for SST5 may partly explain why pasireotide increases glycemia more than octreotide in rats and humans.10,11 In addition, the pasireotide-induced reduction in insulin secretion is also due to the significant decrease in the secretion of incretins (GLP-1, GIP).3,10 It has been shown, in healthy control subjects, that a 7-day treatment with pasireotide induced a nearly total suppression of GLP-1 and GIP secretion.3 Because pasireotide decreases insulin secretion, it frequently induces diabetes.10,12,13 It has been shown that patients with preexisting glucose metabolism disorders were more at risk of developing diabetes on pasireotide.10,13 Since our patients had known type 2 diabetes, this could explain the rapid jump in glycemia levels in our patient after the initiation of pasireotide therapy.
Because pasireotide reduces the secretion of GLP-1 and GIP, the expert recommendations on the management of hyperglycemia in patients treated with pasireotide suggest using early DPP4 inhibitors than a GLP1 agonist to treat the pasireotide-induced diabetes.14,15 Indeed, DPP4 inhibitors and GLP1 analogues have been found effective to control hyperglycemia due to pasireotide treatment.10 This is what we observed also in our patient whose diabetes responded well to sitagliptin therapy.
Pasireotide LAR is a long-acting release formulation of pasireotide that is easy to use with only one injection per month. It is used to treat some chronic diseases such as acromegaly or Cushing’s disease. Pasireotide LAR has been used successfully in two cases of malignant insulinoma.4,5 In one case, diazoxide and octreotide LAR were not able to control hypoglycemia but treatment with pasireotide LAR resulted in near resolution of hypoglycemic events.4 In the other case, a patient with malignant insulinoma had frequent hypoglycemic events during treatment with everolimus and lanreotide, but these events almost completely resolved on pasireotide LAR.5 After distal pancreatectomy, short-acting pasireotide injected twice was able to significantly reduce hypoglycemic events in a patient with nesidioblastosis associated with neuroendocrine pancreatic adenomas.16 However, this case is somewhat different from ours because our patient had isolated nesidioblastosis without pancreatic adenomas and because we used, for the first time, long-acting release pasireotide LAR.
Our observations indicate that pasireotide LAR is an efficient treatment for hypoglycemic events in patients with nesidioblastosis. In addition, the monthly administration facilitates its long-term use. However, due to its rapid effect on insulin secretion, blood glucose should be monitored closely during the first weeks of treatment to detect hyperglycemia, more particularly in patients with preexisting type 2 diabetes.
Ethics and Consent
This case report did not require an institutional approval to be published. This patient gave us her informed written consent to publish this case report.
Acknowledgment
We thank Suzanne Rankin (Dijon University Hospital) for the English language revision.
Disclosure
Alexia Rouland reports non-financial support from Novo Nordisk, Lilly, Vitalaire, Servier, and Novartis, outside the submitted work. Pauline Legris reports non financial support outside the submitted work from ALFASIGMA FRANCE and AMGEN SAS; no financial or non financial support from ASTRAZENECA, BAYER HEALTHCARE SAS, BOEHRINGER INGELHEIM FRANCE, EDWARDS LIFESCIENCE, FRESENIUS KABI FRANCE, IPSEN PHARMA, LILLY FRANCE SAS,MSD FRANCE, NOVARTIS PHARMA SAS, NOVO NORDISK, OTSUKA PHARMACEUTICAL FRANCE SAS, PFIZER SAS, ROCHE DIABETES CARE FRANCE, SANOFI AVENTIS FRANCE, SWEDISH ORPHAN BIOVITRUM, VITALAIR, and ZOLL MEDICAL FRANCE, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Jabri AL, Bayard C. Nesidioblastosis associated with hyperinsulinemic hypoglycemia in adults: review of the literature. Eur J Intern Med. 2004;15(7):407–410. doi:10.1016/j.ejim.2004.06.012
2. de Heide LJM, Laskewitz AJ, Apers JA. Treatment of severe postRYGB hyperinsulinemic hypoglycemia with pasireotide: a comparison with octreotide on insulin, glucagon, and GLP-1. Surg Obes Relat Dis. 2014;10(3):
3. Henry RR, Ciaraldi TP, Armstrong D, Burke P, Ligueros-Saylan M, Mudaliar S. Hyperglycemia associated with pasireotide: results from a mechanistic study in healthy volunteers. J Clin Endocrinol Metab. 2013;98(8):3446–3453. doi:10.1210/jc.2013-1771
4. Hendren NS, Panach K, Brown TJ, et al. Pasireotide for the treatment of refractory hypoglycaemia from malignant insulinoma. Clin Endocrinol (Oxf). 2018;88(2):341–343. doi:10.1111/cen.13503
5. Tirosh A, Stemmer SM, Solomonov E, et al. Pasireotide for malignant insulinoma. Hormones. 2016;15(2):271–276.
6. Lebowitz MR, Blumenthal SA. The molar ratio of insulin to C-peptide. An aid to the diagnosis of hypoglycemia due to surreptitious (or inadvertent) insulin administration. Arch Intern Med. 1993;153:650–655. doi:10.1001/archinte.1993.00410050082011
7. Okabayashi T, Shima Y, Sumiyoshi T, et al. Diagnosis and management of insulinoma. World J Gastroenterol. 2013;19:829–837. doi:10.3748/wjg.v19.i6.829
8. Kumar U, Sasi R, Suresh S, et al. Subtype-selective expression of the five somatostatin receptors (hSSTR1-5) in human pancreatic islet cells: a quantitative double-label immunohistochemical analysis. Diabetes. 1999;48(1):77–85. doi:10.2337/diabetes.48.1.77
9. Singh V, Brendel MD, Zacharias S, et al. Characterization of somatostatin receptor subtype-specific regulation of insulin and glucagon secretion: an in vitro study on isolated human pancreatic islets. J Clin Endocrinol Metab. 2007;92(2):673–680. doi:10.1210/jc.2006-1578
10. Vergès B. Effects of anti-somatostatin agents on glucose metabolism. Diabetes Metab. 2017;43(5):411–415. doi:10.1016/j.diabet.2017.05.003
11. Schmid HA, Brueggen J. Effects of somatostatin analogs on glucose homeostasis in rats. J Endocrinol. 2012;212(1):49. doi:10.1530/JOE-11-0224
12. Boscaro M, Bertherat J, Findling J, et al. Extended treatment of Cushing’s disease with pasireotide: results from a 2-year, Phase II study. Pituitary. 2014;17(4):320–326. doi:10.1007/s11102-013-0503-3
13. Colao A, Petersenn S, Newell-Price J, et al. A 12-month Phase 3 study of pasireotide in Cushing’s disease. N Engl J Med. 2012;366(10):914–924. doi:10.1056/NEJMoa1105743
14. Colao A, De Block C, Gaztambide MS, Kumar S, Seufert J, Casanueva FF. Managing hyperglycemia in patients with Cushing’s disease treated with pasireotide: medical expert recommendations. Pituitary. 2014;17(2):180–186. doi:10.1007/s11102-013-0483-3
15. Reznik Y, Bertherat J, Borson-Chazot F, et al. Management of hyperglycaemia in Cushing’s disease: experts’ proposals on the use of pasireotide. Diabetes Metab. 2013;39(1):34–41. doi:10.1016/j.diabet.2012.10.005
16. Schwetz V, Horvath K, Kump P, et al. Successful medical treatment of adult nesidioblastosis with pasireotide over 3 years. Medicine (Baltimore). 2016;95(14):e3272. doi:10.1097/MD.0000000000003272
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.